bone diseases dr derakhshandeh, phd. 2 dominant negative mutations dominant negative mutations:...
TRANSCRIPT

Bone Bone DiseasesDiseases
Dr Derakhshandeh, Dr Derakhshandeh, PhDPhD
2
Dominant negative Dominant negative mutationsmutations
Dominant negative mutations:Dominant negative mutations:antimorphic mutationsantimorphic mutations an altered gene product that acts an altered gene product that acts
antagonistically to the wild-type alleleantagonistically to the wild-type alleleThese mutations usually result in an These mutations usually result in an
altered molecular functionaltered molecular function (often inactive):(often inactive):DominantDominantor semi-dominant phenotypeor semi-dominant phenotype

3
Dominant negative Dominant negative mutationsmutationsIn humans:
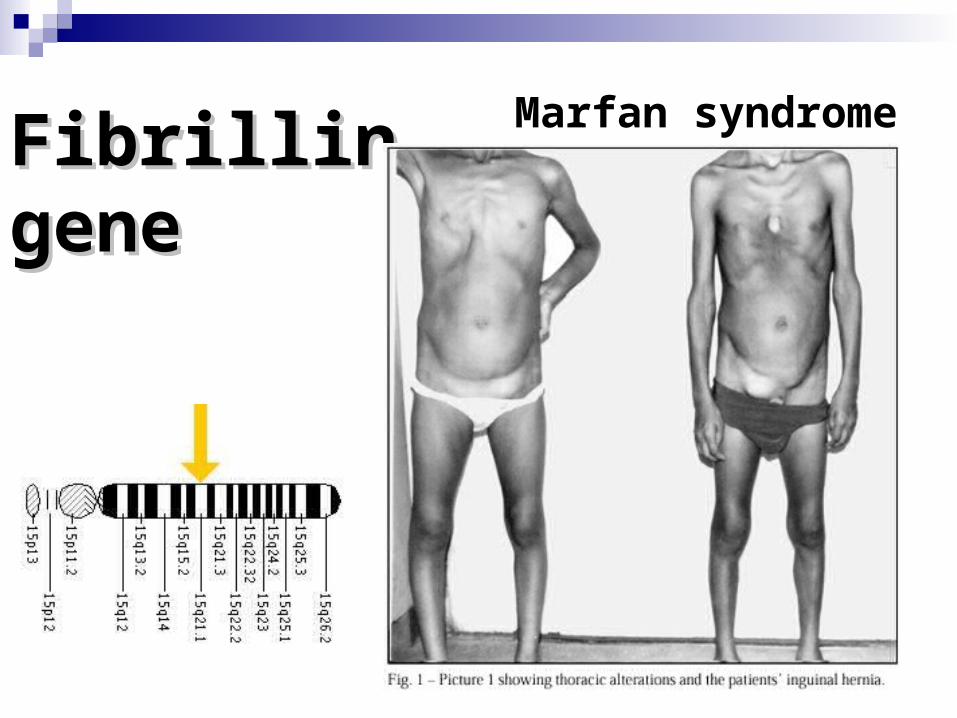
Marfan syndrome is an example of a dominant negative mutation
occurring in an autosomal dominant disease
the defective glycoprotein product of the fibrillin gene (FBN1): antagonizes the product of the normal allele
4
Fibrillin geneFibrillin geneMarfan syndrome
5
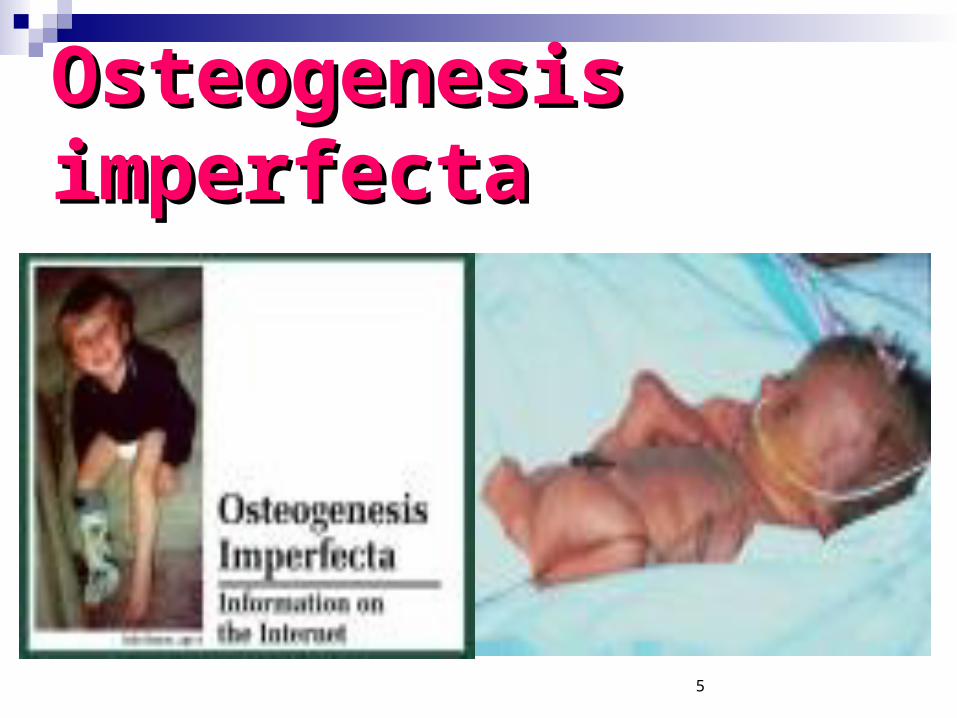
Osteogenesis Osteogenesis imperfectaimperfecta
6
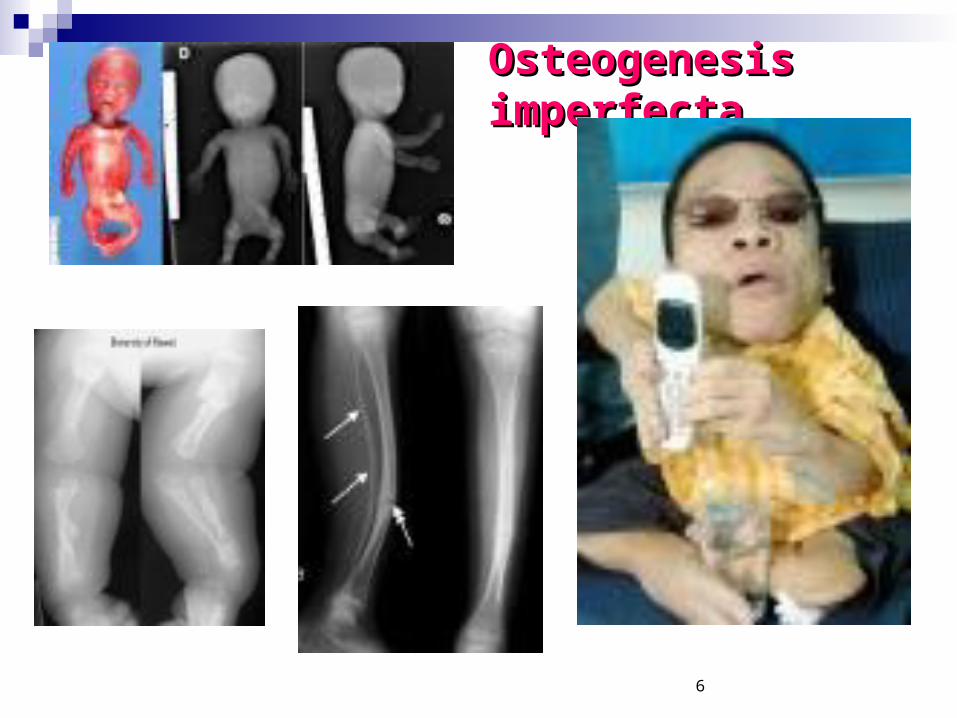
Osteogenesis Osteogenesis imperfectaimperfecta

7
DefinitionDefinition
Osteogenesis imperfecta:a congenital (present from birth) condition of abnormal fragility of the bones

8
CollagenFibrillin in EM

9
Collagen in most tissues and organs is most plentiful in:
dermisTendonCartilageand bone
as a scaffolding for our bodies Controls cell shape broken bones regenerate and wounds heal

10
Collagens the fibrous protein constituent:
Insolubleextracellular glycoprotein found in all animals the most abundant proteins in the
human body
11
Primary Structure of Collagens
The basic unit of collagens:a polypeptide consisting of the
repeating sequence (Glycine (Gly) - X - Y)n
X is often Proline (Pro) and Y is often hydroxyproline

12
Procollagen Type I
The most common form of fibrillar collagen
It is a major constituent of: boneand skin
consists of a heterotrimer of: two alpha1(I) and one alpha2(I) chains

13
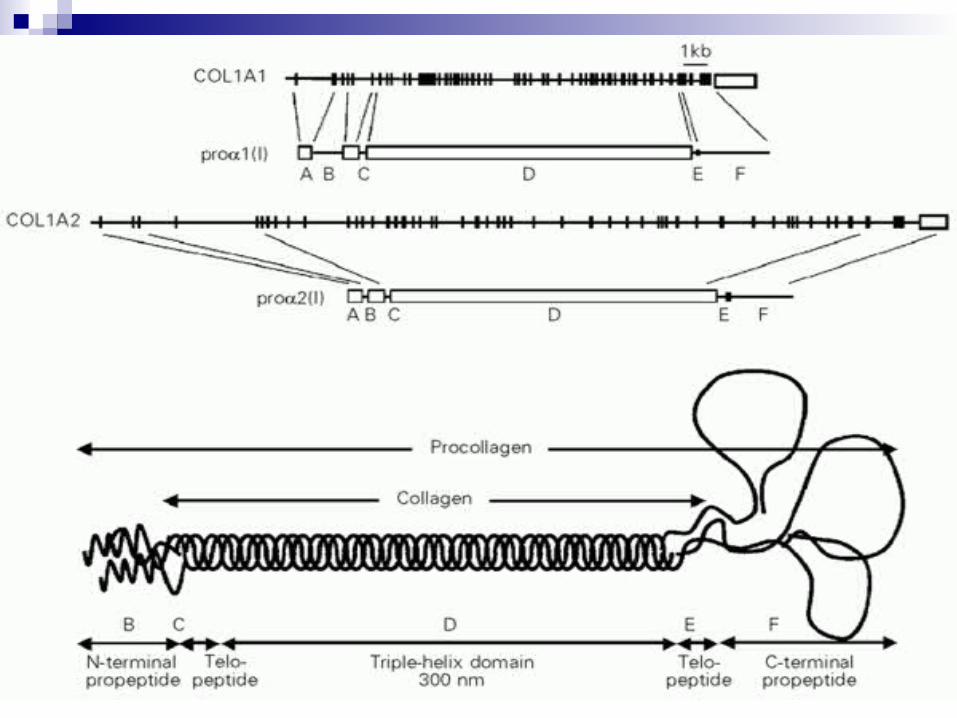
Tertiary Structure
14
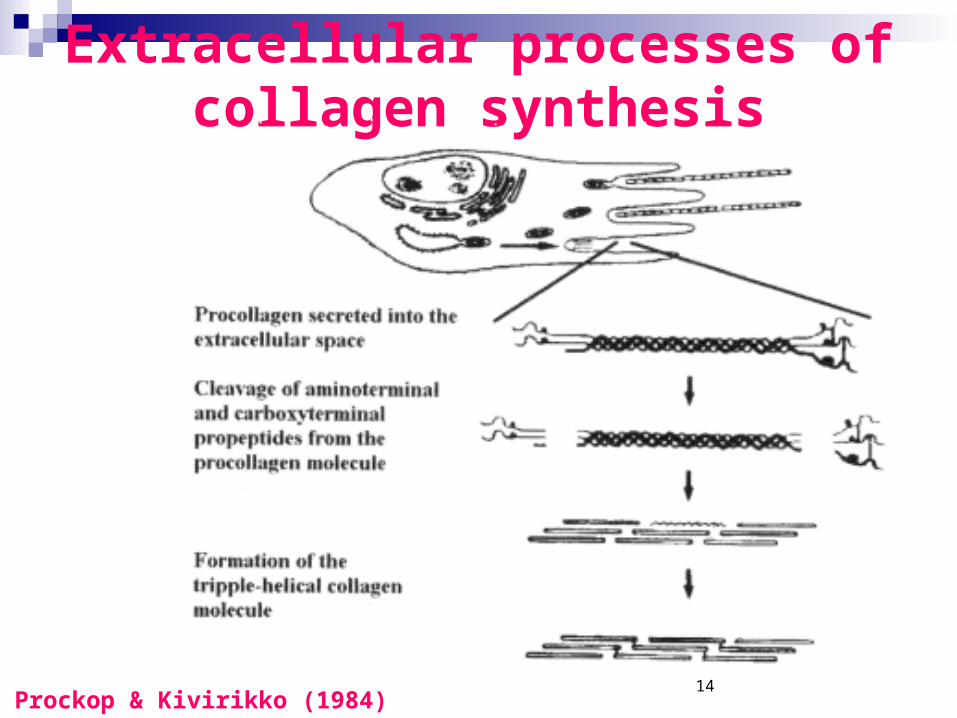
Extracellular processes of collagen synthesis
Prockop & Kivirikko (1984)

15
GeneticGenetic OI, TYPE I
OSTEOGENESIS IMPERFECTA WITH BLUE SCLERA
Gene map locus 17q21.31-q22, 7q22.1
OI type I phenotype can be produced by mutation in either the COL1A1 gene or the COL1A2 gene
16
Osteogenesis imperfecta type I
1:10 000 dominantly inherited (AD) Connective tissue disorder characterized mainly by bone fragility blue sclera 'functional null' alleles of COL1A1 on
chromosome 17 or COL1A2 on chromosome 7
lead to reduced amounts of normal collagen I

17
What is the official name of the COL1A1 gene?
The official name of this gene is:
“collagen, type I, alpha 1”
COL1A1 is the gene's official symbol
18

19

20
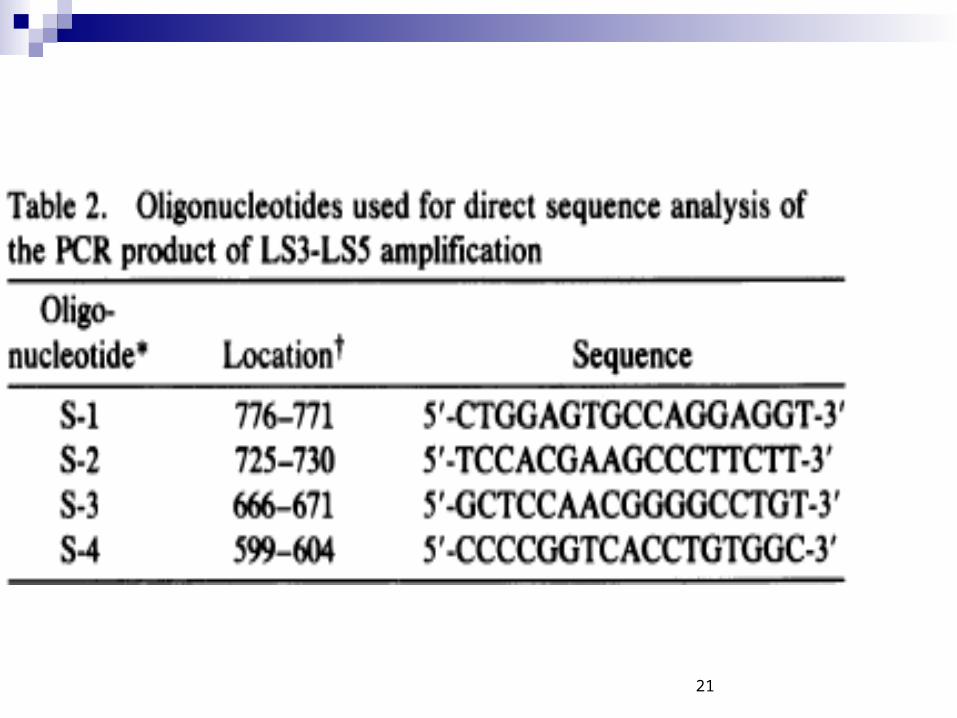
21
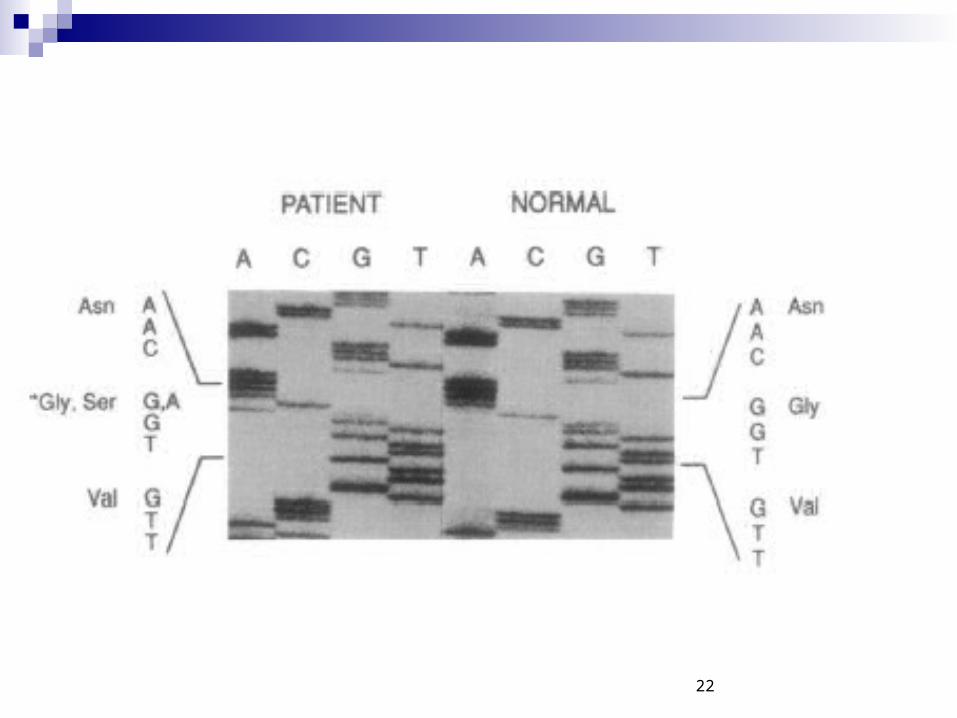
22
23
Glycine Serin
24
What conditions are related to the COL1A1 gene?
Ehles-Donlos syndrome (AD)
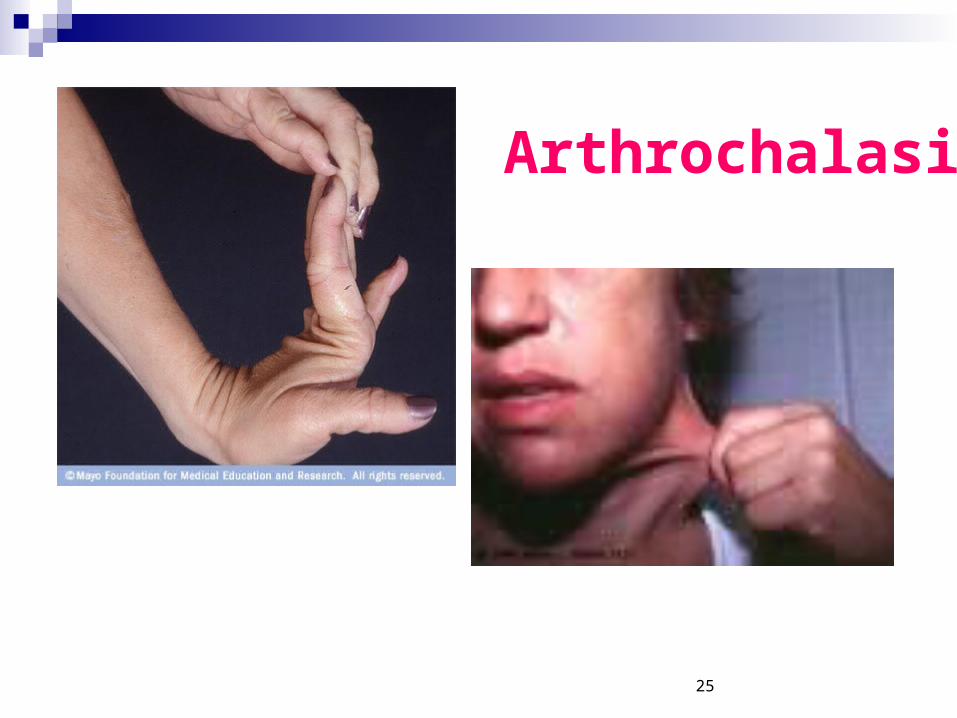
Arthrochalasia:
(Short stature, Hyper elasticity of skin, AR, Problem with healing, N-Terminal defect
caused by mutations in the COL1A1/2 gene
25
Arthrochalasia

26
–The mutations in the COL1A1/2 gene
–instruct the cell to leave out a part of the pro-alpha1(I) chain that contains a segment used to attach one molecule to another
–When this part of the protein is missing, the structure of type I collagen is compromised
–Tissues that are rich in type I collagen:
•such as the skin, bones, and tendons, are affected by this change
27
OI Type I
Osteogenesis imperfecta is the most common disorder
Mutations: inactivate one of the two copies of the COL1A1/2 gene:
28
OI Type I
•The mutated copy of the gene does not produce any pro-alpha1/2(I) collagen chains
•Because only one copy of the gene:
•cells from people with this disorder make only half of the normal amount of type I collagen:
•which results in bone fragility and other symptoms

29
OI Type II- caused by mutations in the COL1A1/2 gene
Many different types of mutations in the COL1A1/2 gene: can cause osteogenesis imperfecta type II
These mutations range: from missing pieces of the COL2A1/2 gene
to amino acid substitutionsin which the amino acid glycine is replaced by another amino acid in the protein strand
C-terminal
30
OI Type II Sometimes one end of the gene
(called the C-terminus) is altered which interferes with the
association of the protein strands All of these changes prevent the
normal production of mature type I collagen
which results in this severe condition, type II osteogenesis imperfecta

31
OI Type III- caused by mutations in the COL1A1/2 gene Mutations in the COL1A1/2 gene may
result: unusable for collagen production Other mutations cause the amino acid
glycine to be replaced by a different amino acid in the pro-alpha1(I) chain
inhibits the essential interaction between protein chains

32
type III osteogenesis imperfecta
inability of the altered procollagen strands
These alterations negatively affect tissues that are rich in type I collagensuch as the skin, bones, teeth
(Dentinogenesis imperfecta), and tendons
33
OI Type (IV)
caused by mutations in the COL1A1/2 gene
Several different types of mutations in the COL1A1/2 gene cause osteogenesis imperfecta type IVmissing pieces of the COL1A1/2 geneor changes in base pairs
formation of the mature triple-stranded collagen molecule

34
OI Position effect (5’/3’-
Mutation)
Protein effect (Gly)
Chain effect (aI/aII)

35
Where is the COL1A1 gene located?
Cytogenetic Location: 17q21.3-q22.1 Molecular Location on chromosome
17
36
CLINICAL FEATURESCLINICAL FEATURES
Osteogenesis imperfecta:
Characterized chiefly by multiple bone fractures, usually resulting from minimal trauma
Affected individuals have blue sclerae, normal-near normal teeth, and normal or near-normal stature
37
CLINICAL FEATURESCLINICAL FEATURES
Osteogenesis imperfecta:
Fractures are rare in the neonatal period;
fracture tendency is constant from childhood to puberty
Often increases following menopause in women and after the sixth decade in men
38
CLINICAL FEATURESOI
39
CLINICAL FEATURES Fractures:
heal rapidly with evidence of a callus formation
and, with good orthopedic care, without deformity
Hearing loss;occurs in about 50% of familiesbeginning in the late teens to profound deafness, by the end of the fourth to fifth decade

40
CLINICAL FEATURES Radiologically:
wormian bones are common but bone morphology is generally normal at birth
Vertebral body morphology: in the adult is normal initiallybut often develops the classic 'cod-fish' appearance
41
EYESEYES Individuals with OI type I
have distinctly blue sclera which remain intensely blue throughout life
The intensity of the blue fades with time: that these individuals may have sclerae of normal hue by adult life
42
EYESEYES
Hartikka et al. (2004) found that:
patients with COL1A1 mutations more frequently had blue sclerae than those with COL1A2 mutations
43
CARDIOVASCULARCARDIOVASCULARMitral valve prolapse occurred in 18% (3 times the prevalence in unaffected relatives)
44
EARSEARS In likely heterogeneous groups of
patients with OI: about half of affected individuals
have hearing loss that begins during the second
decade as a conductive loss
Audiometry showed hearing loss in 25 patients (59.5%)
45
EARSEARS Hartikka et al. (2004) reported: No correlation was found between
the mutated gene or mutation type and hearing pattern
The authors interpreted this to mean that the basis of hearing loss in OI is complex
and that it is a result of multifactorial
46
Causes, incidence, and risk Causes, incidence, and risk factorsfactors
All four types of OI are caused by defects in the amount or
structure of Type 1 collagen
an important part of the bone matrix

47
Causes, incidence, and risk Causes, incidence, and risk factorsfactors
The defect may be inherited in an autosomal dominant pattern from an affected parent
This means that an affected parent, who carries a single gene for the disorder
has a 50% chance of having children with the disorder
Any child who inherits this gene will be affected
48
PreventionPrevention
Genetic counseling: is recommended for
prospective parents if one or both are affected by this disorder
49
SymptomsSymptoms OI:
• all of the bones are abnormally weak• The severity of the abnormality varies
enormously from Type II OI• which is usually lethal in infancy (or even
before birth) • Type I OI, which may be so mild that the
diagnosis is not made, even in adulthood
50
SymptomsSymptoms
• The three classic symptoms of OI includes:
• fragile bones• early hearing loss• and whites of the eyes that
appear bluish (blue sclerae)

51
SymptomsSymptoms• not all people with OI will have
blue sclerae or hearing loss
• All do have fragile bones, but not all people with OI actually ever break a bone
penetrance of hearing loss is clearly age-dependent (Garretsen and Cremers, 1991)

52
SKINSKIN Skin elasticity OI type I increased elasticity
in comparison to the type III patients
53
INHERITANCEINHERITANCE Paternal age effect: for increased risk of new mutations
has been documented although it appears to be
considerably lower than, for example, in Achondroplasia
Blumsohn et al. (2001) confirmed the presence of a small paternal age effect in apparently sporadic OI
54
CLINICAL FEATURESOII
55
OSTEOGENESIS IMPERFECTA OSTEOGENESIS IMPERFECTA CONGENITA,CONGENITA,
NEONATAL LETHAL FORMNEONATAL LETHAL FORMOSTEOGENESIS IMPERFECTA, OSTEOGENESIS IMPERFECTA, TYPE IITYPE IIOIOI
Gene map locus Gene map locus 17q21.31-q22, 7q22.1
56
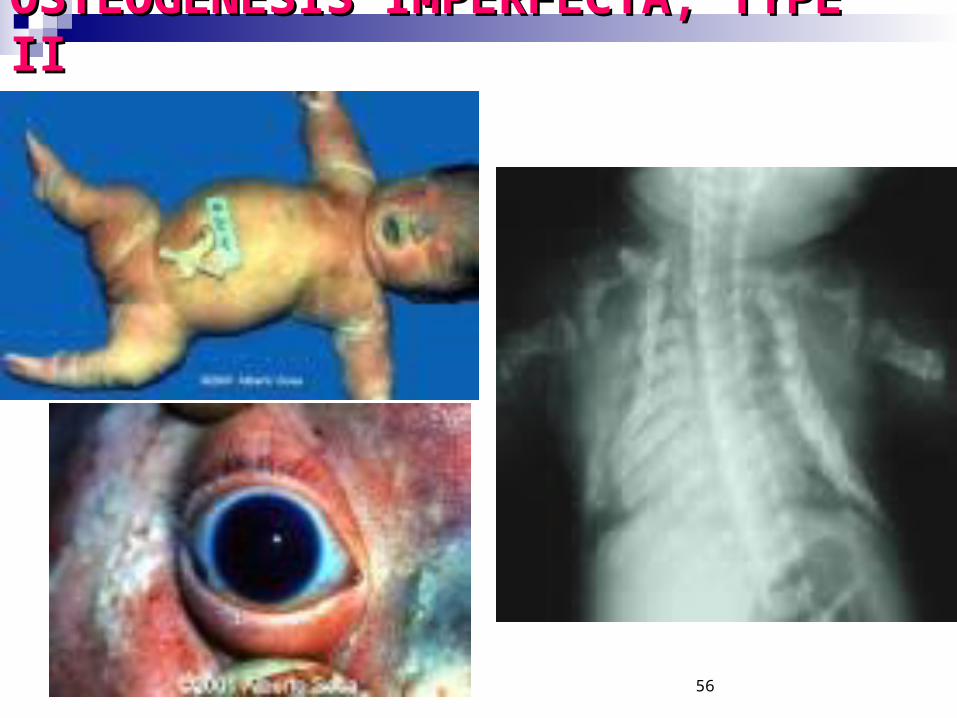
OSTEOGENESIS IMPERFECTA, OSTEOGENESIS IMPERFECTA, TYPE IITYPE II
57
Osteogenesis imperfecta, type II:
the most severe form of the disorder Infants with the disorder:
have soft, fragile bones that may appear bent or crumpled
Bones are easily brokenand multiple fractures can occur even
before birthThe chest is narrow with short ribs and underdeveloped
lungs

58
Osteogenesis imperfecta, type IIAffected infants: have short bowed arms and legs; and
unusually soft skull bones
Characteristic facial features include a small, narrow nose and a dark blue tint to the part of the eyeball that is usually white
Most infants with this condition are stillborn or die shortly after birth, usually from respiratory problems. A few children have lived from several months to a few years

59
CLINICAL FEATURESOIII
60
OSTEOGENESIS IMPERFECTA,
TYPE IIIOI Gene map locus
17q21.31-q22, 7q22.1
The causative mutation in most cases lies in one of the genes for type I collagen, COL1A1 or COL1A2

61
TYPE III OI
62
TYPE III OI People with the disorder are much shorter than
average because the condition prevents bones from growing
normally. Spinal curvature (scoliosis) and bone abnormalities often become progressively
worse during childhood but tend to stabilize during adolescence These complications may shorten a person's lifespan
by affecting heart and lung function Other signs and symptoms include a light blue tint to
the part of the eyeball that is usually white , brittle and discolored teeth, loose joints, and, in some cases, hearing loss.
63
Gene TherapyGene Therapy Chamberlain et al. (2004)
used adeno-associated virus vectors
to disrupt mutant COL1A1 collagen genes
in mesenchymal stem cells, from individuals with severe OI
demonstrating successful gene targeting in adult human stem cells
64
CLINICAL FEATURESOI IV

65
OSTEOGENESIS IMPERFECTA, TYPE IV
OI, TYPE IVOSTEOGENESIS IMPERFECTA WITH NORMAL SCLERAE
Gene map locus 17q21.31-q22
66
OSTEOGENESIS IMPERFECTA, TYPE
IV
67
HypothesisHypothesismore than one broken bone occurring in a single episode (multiple) present at birth occuring after only minor trauma a minority of people with OI never break a bone deformed or short extremities (such as leg deformities or arm deformities) deafness (conductive hearing loss may occur in adults)

68
HypothesisHypothesisShort stature tooth abnormalities low nasal bridge easy bruising bowed legs
69
Signs and tests A physical examination may confirm the presence
of fractures, deformities, and other symptoms. Bone X-rays may show multiple healed fractures. Once the specific molecular diagnosis is known,
family members can be tested by a DNA blood test. DNA testing on prenatal chorionic villus samples
(CVS) can make the diagnosis during pregnancy. Severe OI is visible on prenatal ultrasound as early
as 16 weeks.
70
Osteomyelitis

71
Osteomyelitis
Procedure Osteomyelitis is an acute or
chronic bone infection, usually caused by bacteria or by fungus
72
Causes, incidence, and risk factors Osteomyelitis
The infection that causes osteomyelitis:
often is in another part of the body and spreads to the bone via the blood
Affected bone may have been predisposed to infection because of recent trauma
In children: the long bones are usually affected In adults: the vertebrae and the pelvis (hip)
are most commonly
73
Osteomyelitis Risk factors are recent trauma,
diabetes, hemodialysis, and intravenous drug abuse. People who have had their spleen removed are also at higher risk for osteomyelitis
The incidence of osteomyelitis is 2 in 10,000 people.
74
Prevention
Prompt and complete treatment of infections is helpful
High-risk people should see a health care provider promptly if they have signs of an infection anywhere in the body
75
Symptoms Pain in the bone
Local swelling redness and warmth Fever General discomfort, uneasiness, or ill
feeling
76
Achondroplasia

77
Achondroplasia
Definition An inherited disorder of bone
growth that causes the most common
type of dwarfism
78
Achondroplasia
its characteristic normal to large-sized head
shortened arms and legs (especially the upper arm)
a normal-sized trunk and waddling gait

79
Achondroplasia Achondroplasia is inherited as an
(AD) trait However, the majority of cases,
approximately 80%, appear as spontaneous mutations
If one parent has Achondroplasia, the infant has a 50% chance of inheriting the disorder
If both parents have the condition, the infant's chances of being affected increase to 75%

80
Genetics of Achondroplasia 99% of the affected individuals:
a single point mutation in the Fibroblast Growth Factor
Receptor gene3 (FGFR 3)located on chromosome 4glycine is substituted for
arginine at codon 380 of FGFR 3
81
Such a mutation results: in an abnormal cartilage and fibrous connecting tissue formation
Therefore, not only bones, but the ligaments, tendons and muscles of the patient with Achondroplasia are affected
82
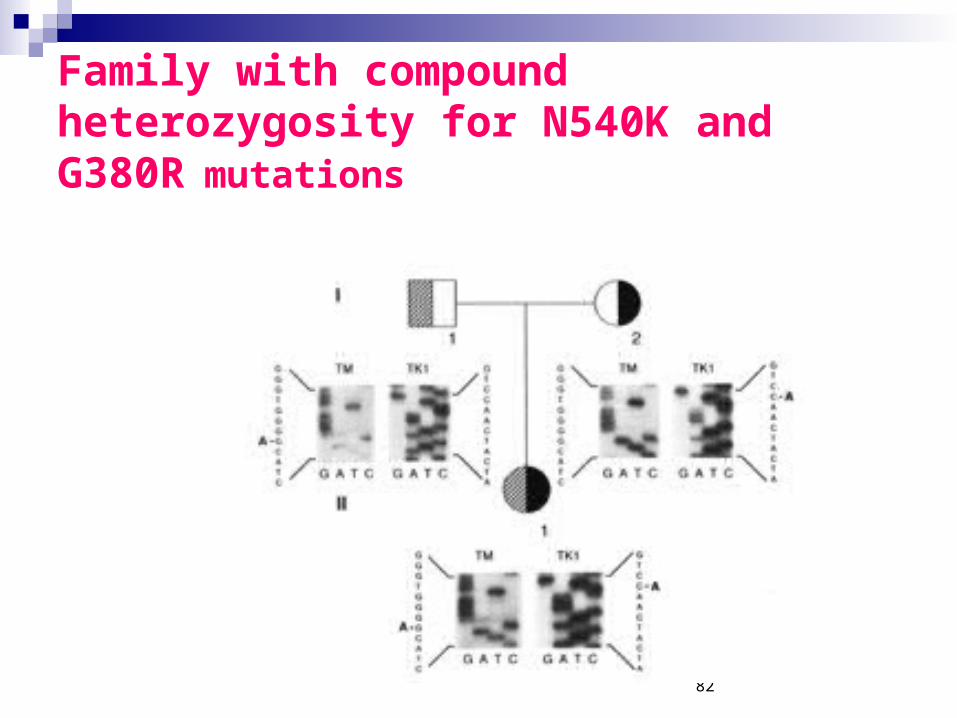
Family with compound heterozygosity for N540K and G380R mutations
83
Prevention Genetic counseling may be
helpful for prospective parents: when one or both have
achondroplasia Because achondroplasia arises as
a spontaneous mutation:absolute prevention is not possible

84
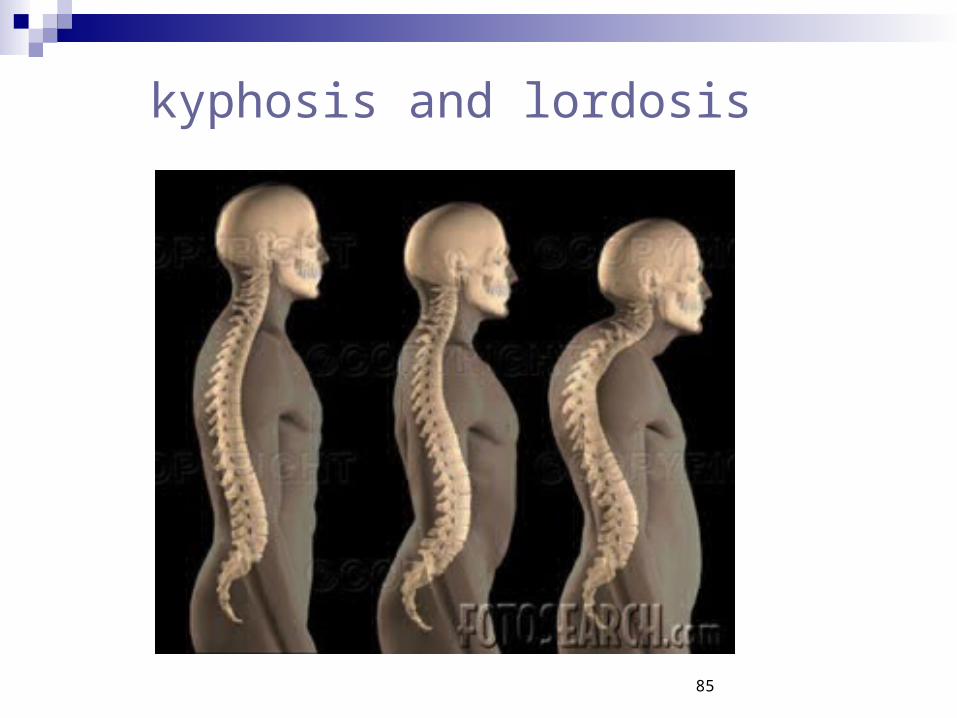
Symptoms at birth: Short stature short limbs large appearing head Skeletal (limb) abnormality Abnormal hand appearance with persistent space between the
long and ring fingers marked kyphosis and lordosis (spine
curvatures)
85
kyphosis and lordosis
86
Symptoms Waddling gait prominent forehead (frontal bossing) increased inward curve of lower back increased outward curve of upper back
making back appear slightly hunched (kyphosis)
head appears disproportionately large for body
bowed legs