body fat as a predictor of the antihypertensive effect of nifedipine
TRANSCRIPT

journal o/ Internal Medicine 1995: 237: 169-173
Body fat as a predictor of the antihypertensive effect of nifedipine
G. STQA-BIRKETVEDT, E. THOM,* J. AARBAKKEt & J. FLORHOLMEN From the lnstitute o/ Clinical Medicine and tInstitute of Medical Biology. University of Trornso. Tromso. and 'Medstat Research Incorporated. Lillestrom. Norwau
Abstract. Staa-Birketvedt G, Thom E, Aarbakke J, Florholmen J (Institute of Clinical Medicine, and Institute of Medical Biology, University of Tromsa, Tromsa, and Medstat Research Incorporated, Lillestram, Norway). Body fat as a predictor of the antihypertensive effect of nifedipine. J Intern Med 1995; 237: 169-73.
Objective. The aim of this study was to investigate the relationship between the blood pressure response and body fat in patients treated with the calcium entry blocker nifedipine. Subjects. Forty untreated subjects with moderate hypertension completed the study. Interventions. Height, weight, body mass index (BMI) and body fat (measured by near infrared spectro- photometry using Futrex 5000) were measured before the start of the study. Based on blood pressure measurements before and 30 min after one capsule of 10 mg nifedipine, the patients were allocated to treatment with 10 mg nifedipine daily in the re- sponder group (reduction in diastolic blood pressure 2 10 mmHg) and with 20 mg nifedipine daily in the
non-responder group. Finally, the blood pressure was measured after 1 week. Results. Twelve patients were classified as responders and 28 patients as non-responders. The responder/ non-responder groups were comparable with respect to the blood pressure readings initially and to age, whereas the non-responders had higher weight (P < 0.01) and BMI (P < 0.01), more body fat (P < 0.01) and were smaller in height (P < 0.01). After 1 week no additional antihypertensive effect was observed in either group. The blood pressure re- duction was negatively correlated to the body fat mass in kilogrammes (P < 0.05 for systolic and P < 0.01 for diastolic blood pressure) in the responder group but not in the non-responder group, whereas no significant correlations were found to BMI in either group. Conclusion. Our data indicate that the body fat can be used to predict the antihypertensive effect of nifedipine.
Keywords: body composition, calcium entry blocker, hypertension, spectrophotometry.
Introduction Obesity is common in hypertensive subjects. How- ever, the implication of this for the antihypertensive response is poorly understood. It has been shown that obese hypertensive patients have higher cardiac output and lower total peripheral resistance com- pared to lean subjects with the same level of arterial hypertension [ l , 21. Therefore, from a theoretical point of view, a beta-blocker with effects on the cardiac output [3] and not a calcium entry blocker with effects on the peripheral resistance [4] should be preferable in obese hypertensive subjects. However, only little clinical documentation has been presented to support this hypothesis [5].
In clinical practice, drug dosage is frequently adjusted according to the total body weight or the body mass index (BMI). However, BMI only reflects the relative overweight, i.e. it does not take into account the body composition in terms of body fat, lean body mass and water. In recent years a number of methods have been developed for estimating body fat [6]. The hydrostatic method with underwater weighing and measurements of total body potassium and total body water are usually considered to be the reference methods for measuring the body fat mass and body free fat mass [7]. Moreover, in recent years computerized tomography has often been used for body fat mass measurements. However, these are complex, time consuming and expensive methods
169
170 G. ST0A-BIRKETVEDT et al.
[6]. Among the new non-invasive methods intro- duced in the last decade, near infrared spectro- photometry has been shown to be a safe and simple method for measurements of body fat [8] with good precision [6], and especially convenient for use in general practice [9].
Nifedipine is a widely used calcium antagonist for the treatment of cardiovascular diseases. The effect of one capsule of 10 mg will give a maximum hypo- tensive effect after only 30 min [lo]. Whether the antihypertensive effect of nifedipine is influenced by overweight and obesity has not been settled.
Therefore, we decided to carry out a clinical study investigating the possibly relationship between blood pressure response and body fat in patients with newly diagnosed moderate hypertension receiving nifedipine for one week. We conclude that body fat is useful to predict the antihypertensive effect of the drug.
Material and methods Forty patients (30 females and 10 males) with moderate hypertension were included in the study. Moderate hypertension was defined as a diastolic pressure 100 mmHg on three different occasions measured in the sitting position, with at least two weeks between each reading. The patients did not have any concomitant disease, and their hyper- tension was diagnosed at the first visit to the general practitioner’s office. Informed consent was obtained from each patient.
The patients rested for at least 5 min with the arm unconstricted and supported on a table at the level of the heart before measurement. The largest cuff that fitted the upper arm was used. For each patient all measurements were performed at the same time of the day. Disappearance of sound (Korotkoff V) was recorded as the diastolic level.
Stature was measured on a portable stadiometer to an accuracy of kO.5 cm with the patient barefoot, feet together, and head in the upright position [9]. Body mass was measured on a balance beam medical scale to the nearest 0.1 kg. Body mass index was obtained by dividing body mass by the square of the stature (kg m-’). Frame size was estimated from elbow diameter according to published tables [ l 11.
Body composition was determined with near infrared (NIR) technique (Futrex 5000: Futrex Inc. Gaithersburg, WA, USA) [8]. The NIR method is based on the principle that the degree of infrared
absorption is related to the composition of the substance through which the energy is passing. During the measurement, a ‘light wand’ emits low- level energy at 940 and 950 nm and a silicon detector measures the intensity of the re-emitted light expressed as optical density at 940 nm and 950 nm. This method is sensitive for light absorption in both subcutaneous and intramuscular fat. After calibration with the manufacturer-provided optical Teflon (Kett Electric Laboratory, Tokyo, Japan), the ‘light wand’ is placed at the midpoint of the bicep. The instrument is calibrated for measurements from this position. The calculated body fat mass takes into account the body weight and height of the subject 16, 91.
The patients were given one capsule of nifedipine (10 mg AdalatB) together with 200 ml of water immediately after having their blood pressure measured in the sitting position. Thirty minutes after the drug intake, the blood pressure was remeasured using the same procedure as described above. The responder group (see below) continued with the same dose of nifedipine, whereas in the non-re- sponder group the nifedipine dose was increased to 20 mg daily. After one week the blood pressure was controlled in both groups.
A responser is defined as having a diastolic blood pressure reduction of 10 mmHg or more, and a non- responder as having a diastolic blood pressure reduction less than 10 mmHg, all based on the measurements before and 30 min after the intake of 10 mg nifedipine.
Statistical methods
A two-sided paired t-test with a significant level of 5% was applied in comparing the two groups. Regression analyses were performed using the method of least squares fit.
Results In the whole group of patients there was a slight and non-significant reduction of the blood pressure from 168.4/110.3 (13.8/9.21) before to 161.7/105.0 (27.0/10.5) mmHg (systolic/diastolic blood press- ure, mean * SD) 30 min after 10 mg nifedipine. Based on the blood pressure measurement before and at 30 min, 12 patients were classified as responders with a significant reduction, and 28 as non- responders with a non-significant reduction of the blood pressure. The background data for the two
BODY FAT AS PREDICTOR OF EFFECT OF NIFEDIPINE 171
Table 1 Age and anthrophometric parameters in the responder/non-responder groups
Classification
Responders Non-responders Parameter (n = 12) (n = 28) P-value
Age (years)
Male/female Height (cms)
Body weight (kgs)
(kg m-') Body mass index
Body fat (%)
Body fat (kg)
Mean SD Min-max
Mean SD Min-max Mean SD Min-max Mean SD Min-max Mean SD Min-max Mean SD Min-max
58.7 15.1 32-80 3/10
173.8 10.7
80.3 17.1
26.3 3.3
26.0 4.6
19.3-3 6.2 21.0
6.0
156-1 93
51-107
19.4-30.6
9.8-30.0
52.0 15.3 P = 0.22 26-78
7/20 P = 1.0 166.3
17.7 P = 0.04
97.0 22.6 P = 0.01 65-165 34.8
157-192
6.3 P < 0.01 2 5.8-52.8 39.5
3 3.9-48.1 38.6
3.2 P < 0.01
7.5 P < 0.01 24.4-78.2
Table 2 Systolic and diastolic blood pressures before and after intake of nifedipine
Classification
Blood pressure Blood pressure at start after 30 min (mmHg) (mmHg)
Responders Mean 169.6/110.0 ( n = 1 2 ) SD 20.519.5
Min-rnax 145 .0-200.0/ 100.0-130.0
Non-responders Mean 167.9/110.4 (n = 28) SD 11.5/9.6
Min-max 145.0-1 8 5 .O/ 100.0-140.0
*Significant difference from the values at start.
154.2/95.8* 14.916.3
130.0-180.0/ 90.0-110.0
165.0/109.0 11.0/9.5
145.0-185.0/ 100.0-140.0
groups of patients are listed in Table 1. The responder/non-responder groups are comparable with respect to age, sex and blood pressure readings initially, whereas the non-responders had higher weight and BMI, more body fat and were lower in height compared to the responders (Table 1 and Table 2). The overlap between the lowest value in the non-responder group and the highest value in the responder group was 65-107,25.8-30.6,33.9-36.2 and 24.4-30 for body weight in kilogrammes, BMI in kg m-2 and body fat in per cent and in kilogrammes, respectively.
After one week with 10 mg nifedipine daily in the responder group or 20 mg nifedipine daily in the
40
30
..2 z a 20 m UY
10
0
10 15 20 25 30
Fat weight
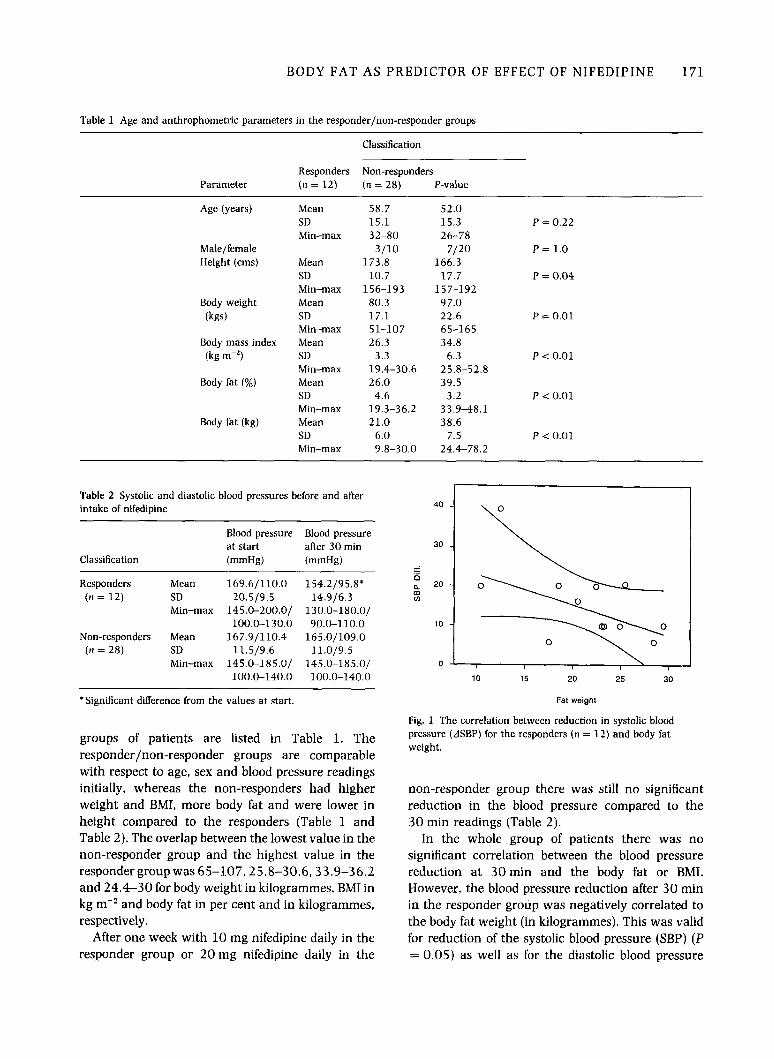
Fig. 1 The correlation between reduction in systolic blood pressure (ASBP) for the responders (n = 12) and body fat weight.
non-responder group there was still no significant reduction in the blood pressure compared to the 30 min readings (Table 2).
In the whole group of patients there was no significant correlation between the blood pressure reduction at 30min and the body fat or BMI. However, the blood pressure reduction after 30 min in the responder group was negatively correlated to the body fat weight (in kilogrammes). This was valid for reduction of the systolic blood pressure (SBP) (P = 0.05) as well as for the diastolic blood pressure
172 G. STQA-BIRKETVEDT et al.
30
25 "2 = 0 a 20 0 m
15
10
10 15 20 25 30
Fat weight
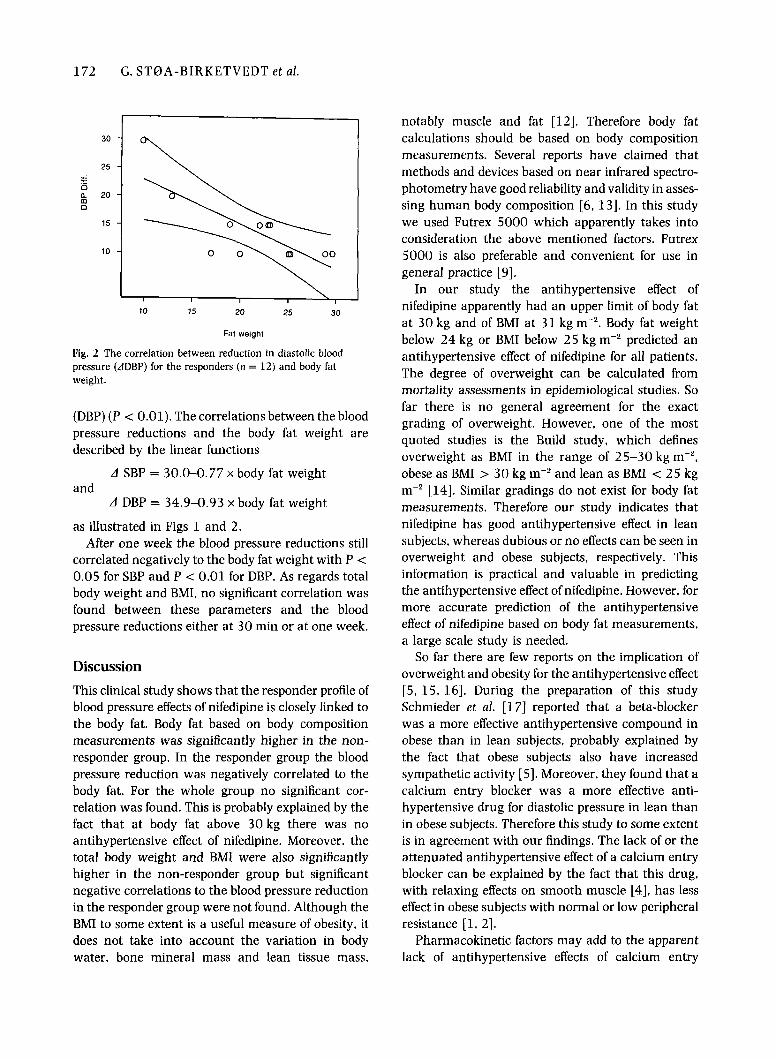
Pig. 2 The correlation between reduction in diastolic blood pressure (ADBP) for the responders (n = 12) and body fat weight.
(DBP) (P < 0.01). The correlations between the blood pressure reductions and the body fat weight are described by the linear functions
A SBP = 30.0-0.77 x body fat weight and
A DBP = 34.9-0.93 x body fat weight
as illustrated in Figs 1 and 2. After one week the blood pressure reductions still
correlated negatively to the body fat weight with P < 0.05 for SBP and P < 0.01 for DBP. As regards total body weight and BMI, no significant correlation was found between these parameters and the blood pressure reductions either at 30 min or at one week.
Discussion This clinical study shows that the responder profile of blood pressure effects of nifedipine is closely linked to the body fat. Body fat based on body composition measurements was significantly higher in the non- responder group. In the responder group the blood pressure reduction was negatively correlated to the body fat. For the whole group no significant cor- relation was found. This is probably explained by the fact that at body fat above 30 kg there was no antihypertensive effect of nifedipine. Moreover, the total body weight and BMI were also significantly higher in the non-responder group but significant negative correlations to the blood pressure reduction in the responder group were not found. Although the BMI to some extent is a useful measure of obesity, it does not take into account the variation in body water, bone mineral mass and lean tissue mass,
notably muscle and fat [12]. Therefore body fat calculations should be based on body composition measurements. Several reports have claimed that methods and devices based on near infrared spectro- photometry have good reliability and validity in asses- sing human body composition [6, 131. In this study we used Futrex 5000 which apparently takes into consideration the above mentioned factors. Futrex 5000 is also preferable and convenient for use in general practice [9].
In our study the antihypertensive effect of nifedipine apparently had an upper limit of body fat at 30 kg and of BMI at 31 kg m-'. Body fat weight below 24 kg or BMI below 25 kg m-' predicted an antihypertensive effect of nifedipine for all patients. The degree of overweight can be calculated from mortality assessments in epidemiological studies. So far there is no general agreement for the exact grading of overweight. However, one of the most quoted studies is the Build study, which defines overweight as BMI in the range of 25-30 kg m-', obese as BMI > 30 kg m-' and lean as BMI < 25 kg m-' [14]. Similar gradings do not exist for body fat measurements. Therefore our study indicates that nifedipine has good antihypertensive effect in lean subjects, whereas dubious or no effects can be seen in overweight and obese subjects, respectively. This information is practical and valuable in predicting the antihypertensive effect of nifedipine. However, for more accurate prediction of the antihypertensive effect of nifedipine based on body fat measurements, a large scale study is needed.
So far there are few reports on the implication of overweight and obesity for the antihypertensive effect [5, 15, 161. During the preparation of this study Schmieder et al. [17] reported that a beta-blocker was a more effective antihypertensive compound in obese than in lean subjects, probably explained by the fact that obese subjects also have increased sympathetic activity [5]. Moreover, they found that a calcium entry blocker was a more effective anti- hypertensive drug for diastolic pressure in lean than in obese subjects. Therefore this study to some extent is in agreement with our findings. The lack of or the attenuated antihypertensive effect of a calcium entry blocker can be explained by the fact that this drug, with relaxing effects on smooth muscle [4], has less effect in obese subjects with normal or low peripheral resistance [ l . 21.
Pharmacokinetic factors may add to the apparent lack of antihypertensive effects of calcium entry

BODY FAT AS PREDICTOR OF EFFECT OF NIFEDIPINE 173
blockers. Nifedipine is highly lipophilic and should exhibit increased distribution volume in obese subjects since drugs with sufficiently high lipid solubility may tend to accumulate preferentially and extensively in adipose tissue deposits [18]. However, the impact of pharmacokinetic factors for any in- terference of the antihypertensive effect of nifedipine in obese subjects awaits further studies.
In conclusion, the body fat apparently attenuates the antihypertensive effect of nifedipine. Measure- ments of body fat based on near infrared spectro- photometry can probably be a feasible method in general practice for predicting the antihypertensive effect of nifedipine.
References Messerli FH. Sundgaard-Riise K. Reisin ED. Dreslinski GR. Ventura HO. Oigman W et a/. Dimorphic cardiac adaptation to obesity and arterial hypertension. Ann Intern Med 1983: 99:
Messerli FH. Sundgaard-Riise K. Reisin ED, Dreslinski GR. Dunn FG. Frohlich ED. Disparate cardiovascular effects of obesity and arterial hypertension. A m ] Med 1983: 74:
Prichard BNCM. Hypotensive action of pronetholol. Br Med ] 1964: 1: 1227. Messerli FH. Oren S. Grossmann E. Effects of calcium channel blockers on systemic hemodynamics in hypertension. Am ] Med 1988: 8 4 (Suppl. 3B): 8-12. Tuck ML. Obesity, the sympathetic nervous system. and essential hypertension. Hgpertension 1992 : 19 (Suppl. 1):
Lukaski HC. Methods for the assessment of human body composition: traditional and new. Am Clin Nutr 1987; 46:
75 7-6 1.
808-1 2.
67-77.
537-56.
7 Sjnstrem L. Impact of body weight. body composition, and adipose tissue distribution on morbidity and mortality. In: Stunkard AJ. Wadden TA. eds. Obesity. 2nd edn. New York: Raven Press, 1993; 13-41.
8 Conway JM. Norris KH, Bodwell CE. A new approach for the estimation of body composition: infrared interactance. Am ] Clin Nutr 1984: 40: 1123-30.
9 Stna-Birketvedt G. Thorn E. The effect of modest physical exercise in the treatment of overweight. Tidsskr Nor Lageloren
10 Olivari MT. Bartorelli C. Polese A, Fiorentini C. Moruzzi P. Guazzi M. Treatment of hypertension with nifedipine. a calcium antagonistic agent. Circulation 1979 : 59: 1056.
11 Frisancho RA. Flegel PN. Elbow breadth as a measure of frame size for US males and females. Am ] Clin Nutr 1983: 37: 3 1 1 4 .
1 2 Heitmann BL. Evaluation of body fat estimated from body mass index. skinfolds and impednnce. A comparative study. Eur ] Clin Nutr 1990: 44: 831-7.
1 3 Sohlstrom A, Forslund A, Sjodin A, Forsum E. Evaluation of simple methods to estimate total body fat in healthy women. Scand Med Sci Sports 1992; 2: 207-11.
1 4 Society of Actuaries and Association of Life Insurance Medical Directors. Build Study. Chicago: Recording and Statistical Corp.. 1979.
15 Galletti F. Fasano ML. Ferrara LA, Groppi A. Montagna M. Mancini M. Obesity and beta-blockcrs: influence of body fat on their kinetics and cardiovascular effects. / Clin Pharrnacol
16 MacMahon SW. MacDonald GJ. Bernstein L. Andrews G. Blacket RB. Comparison of weight reduction with metoprolol in treatment of hypertension in young overweight patients. Lancet 1985: 1233-6.
1 7 Schmieder RE, Gatzka C. Schachinger H. Schobel H. Ruddel H. Obesity as determinant for response to antihypertensive treatment. BM] 1993: 307: 537-40.
1 8 Abernethy DR, Greenblatt DJ. Phmnacokinetics of drugs in obesity. Clinical Pharmacokinetics 1982 : 7: 108-24.
1992: 112: 3781-3.
1989: 29: 212-6.
Received 18 April 1994, accepted 16 August 1994.
Correspondence: G. Stoa-Buketvedt. Institute of Clinical Medicine, University of Tromsn. 9037 Tromso, Norway.