blood substitutes artificial oxygen carriers: perfluorocarbon emulsions
TRANSCRIPT
Blood substitutesArtificial oxygen carriers: perfluorocarbon emulsionsDonat R Spahn
Mini-review R93
IntroductionArtificial oxygen carriers aim at improving oxygen trans-port and oxygen unloading to the tissue. Artificial oxygencarriers may thus be used as an alternative to allogeneicblood transfusions or to improve tissue oxygenation andfunction of organs with marginal oxygen supply. Thepresent article describes the currently evaluated perfluo-rocarbon emulsions, in order to summarize their efficacy,discuss potential side effects and illustrate potentialfuture applications.
Background of perfluorocarbon emulsionsPerfluorochemicals are chemically inert synthetic mole-cules that consist primarily of carbon and fluorine atoms,and are clear, colourless liquids. They have the ability tophysically dissolve significant quantities of many gasesincluding oxygen and carbon dioxide. Perfluorochemicalsare hydrophobic, and are therefore not miscible with water.Perfluorochemicals thus have to be emulsified for intra-venous use. With sophisticated technology, it is possible togenerate a stable perfluorocarbon emulsion with excep-tionally small particles (median diameter <0.2µm) [1].
First-generation perfluorocarbon emulsions as well asRussian or Chinese products have been described in a pre-vious review [1]. Western development of second-genera-tion perfluorocarbon emulsions has focused on linearperfluorocarbon molecules such as perfluorooctyl bromide(C8F17Br, also referred to as perflubron), perfluorodecylbromide (C10F21Br) and perfluorodichlorooctane(C8F16Cl2) [1]. Using solely 3.6%w/v egg yolk phospho-lipid, Alliance Pharmaceutical Corporation (San Diego,California, USA) developed a concentrated (60%w/v) andstable perfluorocarbon emulsion, Oxygent, which is com-posed of 58%w/v perfluorooctyl bromide and 2%w/v per-fluorodecyl bromide, with an average particle size of0.16–0.18µm diameter. Hemagen/perfluorocarbon (StLouis, Missouri, USA) developed another concentrated(40% v/v) perfluorocarbon emulsion, Oxyfluor, using per-fluorodichlorooctane, egg yolk phospholipid and triglyc-erid with an average particle size of 0.22–0.25µm diameter.
After intravenous administration, the droplets of the per-fluorocarbon emulsion are taken up by the reticuloen-dothelial system (RES). This uptake into the RES
RES = reticuloendothelial system; ANH = acute normovolemic haemodilution.
Perfluorocarbon emulsions are being clinically evaluated as artificial oxygencarriers to reduce allogeneic blood transfusions or to improve tissueoxygenation. Perfluorocarbon emulsions are efficacious in animal experiments,and in humans they are well tolerated and at least as successful to reversephysiologic transfusion triggers than autologous blood. Perfluorocarbonemulsions may be used in the future in the concept of augmented acutenormovolaemic haemodilution. In this concept relatively low preoperativehaemoglobin levels are targeted during preoperative normovolaemichaemodilution and a perfluorocarbon emulsion is given to augment oxygendelivery during surgery when low endogenous haemoglobin levels are expected.The autologous blood is subsequently retransfused in the postoperative periodwhen the patient’s oxygenation is provided primarily by the endogenoushaemoglobin. Additional uses of perfluorocarbon emulsions will includetreatments of diseases with compromised tissue oxygenation such as cerebral ormyocardial ischaemia, air embolism and emergency or trauma surgery as long asno allogeneic blood is available.
Address: Institut für Anästhesiologie,UniversitätsSpital, Zürich, Switzerland
Correspondence: Donat R Spahn, M.D., Professorof Anesthesiology, Institut für Anästhesiologie,UniversitätsSpital, Rämistrasse 100, CH-8091Zürich, Switzerland. Tel: (41) 1 255 26 96;fax: (41) 1 255 44 09;e-mail: [email protected]
Keywords: artificial oxygen carriers,perfluorocarbon emulsion, acute normovolaemichaemodilution, blood transfusion, bloodconservation
Received: 16 August 1999Accepted: 6 September 1999Published: 24 September 1999
Crit Care 1999, 3:R93–R97
The original version of this paper is the electronicversion which can be seen on the Internet(http://ccforum.com). The electronic version maycontain additional information to that appearing inthe paper version.
© Current Science LtdPrint ISSN 1364-8535 Online ISSN 1466-609X
determines the intravascular half life [1–3]. Intravascularhalf life is dose-dependent, and for Oxygent was found tobe 9.4±2.2h for a dose of 1.8g/kg [4]. After the initialuptake of the perfluorocarbon emulsion into the RES thedroplets are slowly broken down, and the perfluorocarbonmolecules are taken up in the blood again (bound to bloodlipids) and transported to the lungs, where the unalteredperfluorocarbon molecules are finally excreted via exhala-tion. At present no metabolism of fluorocarbon moleculesis known in humans [1–3].
Safety profileOxygent and Oxyfluor both underwent extensive safetytesting. The results of most of these studies are not pub-lished in the scientific literature, but they form the basisfor regulatory authorities to allow clinical testing. Commonside effects such as delayed febrile reaction and flu-likesymptoms seem to be related to the normal activity ofphagocytic cells of the RES. The magnitude of these sideeffects depend on the particle size of the emulsion. Smallerparticles (0.1–0.2µm diameter) appear to be less detectablefor the RES than larger particles (>0.2µm diameter) andcause only mild temperature increases and mild flu-likesymptoms in relatively few individuals [1,3,5].
Once in the RES, excretion depends on vapor pressureand lipid solubility of flourocarbons. Elimination half-timeis 3–4 days for perfluorooctyl bromide and 8 days for per-fluorodichlorooctane. Because flourocarbon molecules areinert to biochemical degradation, they diffuse back intothe blood where they dissolve in plasma lipids. Theselipids transport the perfluorocarbon molecules to the lungswhere they are excreted by exhalation.
At higher doses (1.7g/kg Oxyfluor, 1.8g/kg Oxygent) a tran-sient decrease in platelet count was observed 2–3 days afterdosing, with recovery by 7–14 days [1,6]. With Oxygent,however, the decrease in platelet count was mild (10–20%)and no drug-related effects on platelet function wereobserved. Furthermore, plasmatic coagulation was not com-promised and template bleeding time was not prolonged by1.8g/kg Oxygent [1,6]. In addition, there was no comple-ment activation [7]; no suppression of humoral or cell-medi-ated immune function; no haemodynamic effects orvasoconstriction; no changes in liver, lung or renal function;and no clinically relevant effects on blood chemistry [1].
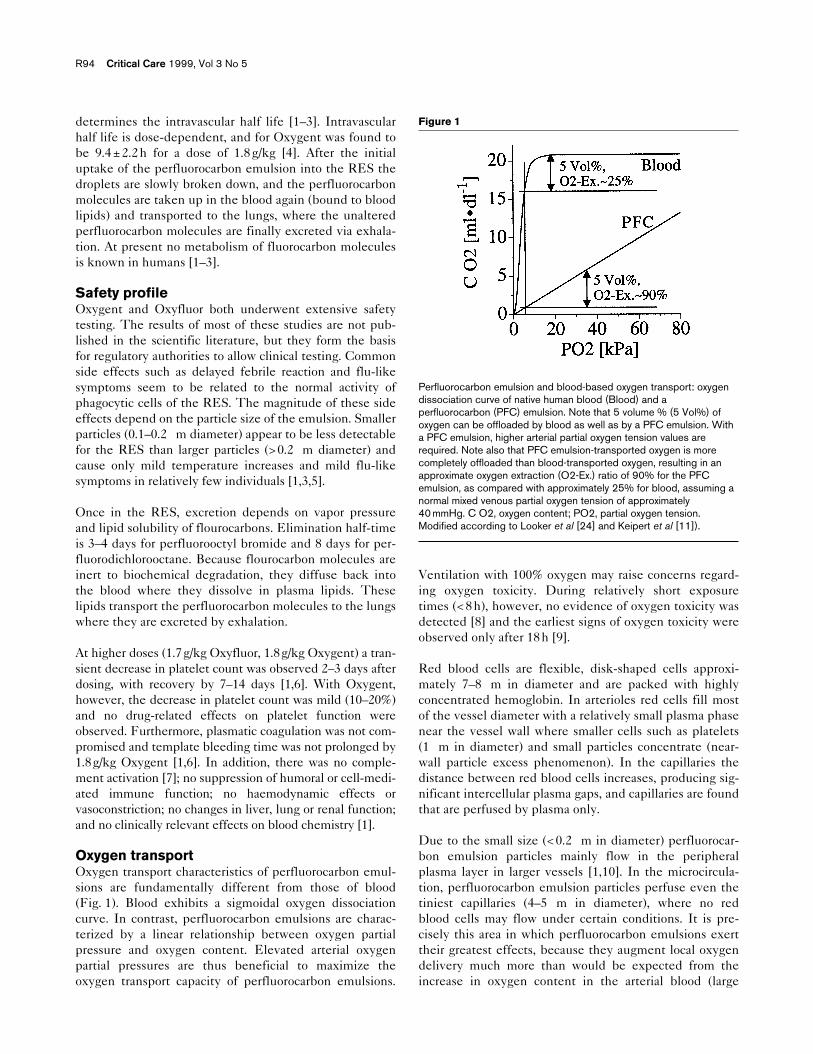
Oxygen transportOxygen transport characteristics of perfluorocarbon emul-sions are fundamentally different from those of blood(Fig. 1). Blood exhibits a sigmoidal oxygen dissociationcurve. In contrast, perfluorocarbon emulsions are charac-terized by a linear relationship between oxygen partialpressure and oxygen content. Elevated arterial oxygenpartial pressures are thus beneficial to maximize theoxygen transport capacity of perfluorocarbon emulsions.
Ventilation with 100% oxygen may raise concerns regard-ing oxygen toxicity. During relatively short exposuretimes (<8h), however, no evidence of oxygen toxicity wasdetected [8] and the earliest signs of oxygen toxicity wereobserved only after 18h [9].
Red blood cells are flexible, disk-shaped cells approxi-mately 7–8µm in diameter and are packed with highlyconcentrated hemoglobin. In arterioles red cells fill mostof the vessel diameter with a relatively small plasma phasenear the vessel wall where smaller cells such as platelets(1µm in diameter) and small particles concentrate (near-wall particle excess phenomenon). In the capillaries thedistance between red blood cells increases, producing sig-nificant intercellular plasma gaps, and capillaries are foundthat are perfused by plasma only.
Due to the small size (<0.2µm in diameter) perfluorocar-bon emulsion particles mainly flow in the peripheralplasma layer in larger vessels [1,10]. In the microcircula-tion, perfluorocarbon emulsion particles perfuse even thetiniest capillaries (4–5µm in diameter), where no redblood cells may flow under certain conditions. It is pre-cisely this area in which perfluorocarbon emulsions exerttheir greatest effects, because they augment local oxygendelivery much more than would be expected from theincrease in oxygen content in the arterial blood (large
R94 Critical Care 1999, Vol 3 No 5
Figure 1
Perfluorocarbon emulsion and blood-based oxygen transport: oxygendissociation curve of native human blood (Blood) and aperfluorocarbon (PFC) emulsion. Note that 5 volume % (5 Vol%) ofoxygen can be offloaded by blood as well as by a PFC emulsion. Witha PFC emulsion, higher arterial partial oxygen tension values arerequired. Note also that PFC emulsion-transported oxygen is morecompletely offloaded than blood-transported oxygen, resulting in anapproximate oxygen extraction (O2-Ex.) ratio of 90% for the PFCemulsion, as compared with approximately 25% for blood, assuming anormal mixed venous partial oxygen tension of approximately40 mmHg. C O2, oxygen content; PO2, partial oxygen tension.Modified according to Looker et al [24] and Keipert et al [11]).

vessel with red blood cells) [1]. Another important aspectthat determines the efficacy of perfluorocarbon emulsionsis the fact that all oxygen carried by the perfluorocarbon isin the dissolved state, resulting in a higher oxygen partialpressures in the microcirculation and thereby augmentingthe driving pressure for the diffusion of dissolved oxygeninto the tissue.
Preclinical efficacy of second-generationperfluorocarbon emulsionsA perflubron emulsion (Oxygent) was assessed in a varietyof haemodilution studies. Keipert et al [11] applied perflu-bron emulsion in dogs after acute normovolemic haemodi-lution (ANH) at a haematocrit of 10%. With theapplication of Oxygent, cardiac output tended to increaseand a massive rise in mixed venous oxygen partial pres-sure and mixed venous saturation was observed. The per-centage of metabolized oxygen that originated fromendogenous haemoglobin decreased with the applicationof Oxygent, indicating that the oxygen transported byOxygent is preferentially metabolized, due to its excellentoxygen unloading characteristics [11].
An increase in mixed venous oxygen partial pressure indi-cates improvement in global oxygenation status [12],rather than shunting of oxygen from arterioles directly intovenules (i.e. oxygen bypassing the microcirculation). Thisview is substantiated by a study that demonstrated anincrease of oxygen consumption in a maximally working,in-situ gastrocnemius muscle preparation in anesthetizedand haemodiluted dogs after Oxygent administration [12].It is also substantiated by the fact that increases in mixedvenous oxygen partial pressure are generally associatedwith an Oxygent-dependent improvement in tissue oxy-genation, as demonstrated in the heart, brain, muscle, gutand liver [13,14]. Furthermore, Holman et al [15] testedOxygent in severely haemodiluted dogs undergoing car-diopulmonary bypass. Dogs treated with increasing dosesof Oxygent survived cardiopulmonary bypass progres-sively better than did control animals.
Oxygent may also be beneficial as an adjunct to resuscita-tion. In a porcine model of near fatal haemorrhage,Oxygent treatment in addition to standard resuscitationdecreased mortality from 43 to 13% [16]. Infusion of oxy-genated Oxygent into the aortic arch also improvedoutcome in another resuscitation model [17].
Mixed venous oxygen partial pressure was higher inOxygent-treated animals after ANH to a haemoglobin of7g/dl than in control animals [14,18], and measures of leftventricular systolic and diastolic contractile function werefound to be improved after Oxygent administration at ahaemoglobin level of 3g/dl [19]. This might be explainedby an augmented oxygen delivery through very narrowcapillaries where Oxygent particles may penetrate better
than the relatively large red blood cells, and therebyimprove local tissue oxygenation more than red blood cells[1]. These studies thus indicate that Oxygent indeedtransports and unloads oxygen into the areas where it isneeded most.
Clinical efficacy of second-generationperfluorocarbon emulsionsOxygent has also been used in humans [6,20,21,22]. ANHto a haemoglobin concentration of approximately 9g/dl wasperformed [20]. During surgery Oxygent (0.9g/kg) wasadministered when a blood transfusion was deemed neces-sary by the anaesthesiologist, which occurred at a haemo-globin concentration of approximately 8g/dl. Mixed venousoxygen tension and mixed venous oxygen saturation bothincreased significantly after Oxygent administration, andcardiac output was stable. Although only relatively littleoxygen was transported by perflubron emulsion (approxi-mately 1%), 5% of the metabolized oxygen was transportedby Oxygent, again indicating that Oxygent-transportedoxygen is preferentially metabolized [11,20].
Recently, the results of two large prospective randomizedmulticenter studies on the use of Oxygent in orthopaedicand genitourinary surgery were presented [21,22]. In theorthopaedic study [21], 147 patients undergoing hipreplacement and spine surgery were haemodiluted preop-eratively to a hemoglobin level of 9g/dl. After the patientshad reached a predefined transfusion trigger, they wererandomized into four groups: standard of care (retransfu-sion of 450 ml autologous blood at an unchanged fractionalinspired oxygen of 0.4); Oxygent (0.9 or 1.8g/kg) withcolloid to a total 450ml with ventilation with an fractionalinspired oxygen of 1.0; and infusion of 450ml colloid withventilation with an fractional inspired oxygen of 1.0.Oxygent (1.8g/kg) was most successful in reversing trans-fusion triggers in 97% of patients, as compared with 60%in the control group. The duration of transfusion triggerreversal in the Oxygent 1.8g/kg group was significantlylonger (80min) than in the control and colloid groups (55and 30min, respectively). In the study that including 109patients undergoing genitourinary surgery [22], similarresults were achieved. Thus, physiologic transfusion trig-gers may be treated at least as successfully with Oxygentas with autologous blood of colloids. This illustrates theremarkable potency of Oxygent to deliver readily availableoxygen to those areas in the body in which the extraoxygen is needed most.
Future uses of perfluorocarbon emulsionsOptimal use of perfluorocarbon emulsions in the futuremay consist of a combination of ANH preoperatively withapplication of an artificial oxygen carrier such as a perfluo-rocarbon emulsion during the operation, a proceduretermed ‘augmented ANHSM’ [Roth DJ, Keipert PE,Faithfull NS, Zuck TF, Riess JG: Facilitated oxygen
Mini-review Perfluorocarbon emulsions Spahn R95
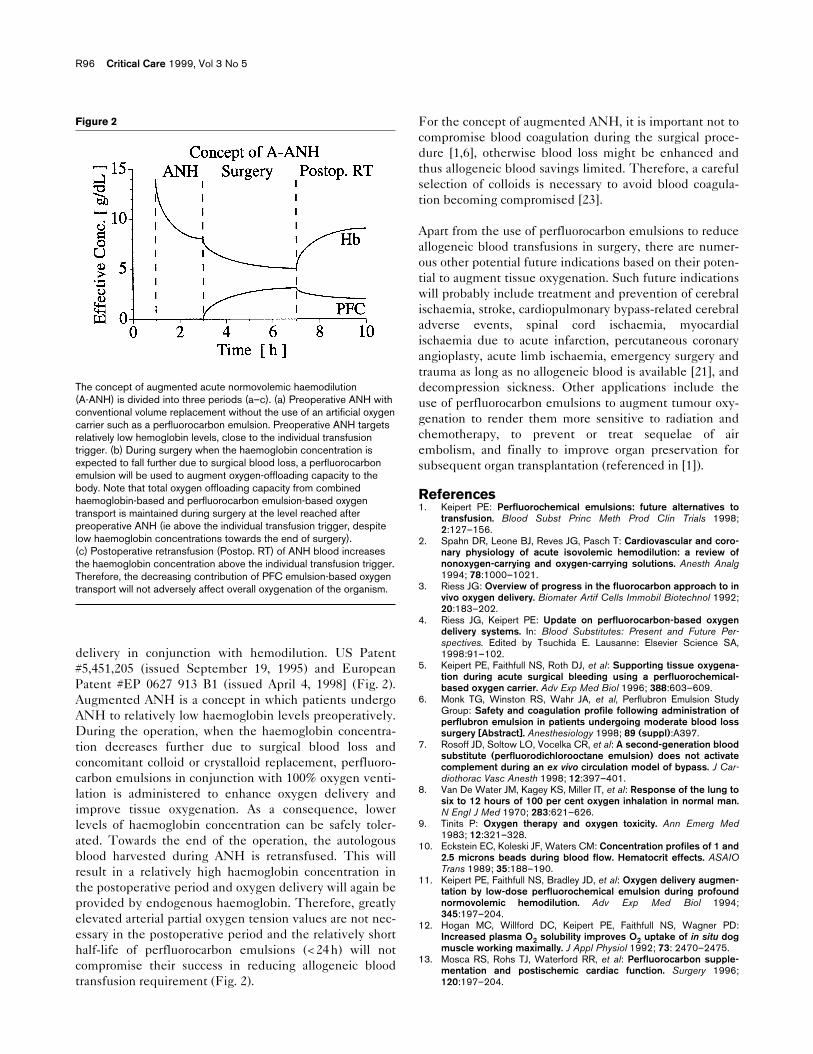
delivery in conjunction with hemodilution. US Patent#5,451,205 (issued September 19, 1995) and EuropeanPatent #EP 0627 913 B1 (issued April 4, 1998] (Fig. 2).Augmented ANH is a concept in which patients undergoANH to relatively low haemoglobin levels preoperatively.During the operation, when the haemoglobin concentra-tion decreases further due to surgical blood loss andconcomitant colloid or crystalloid replacement, perfluoro-carbon emulsions in conjunction with 100% oxygen venti-lation is administered to enhance oxygen delivery andimprove tissue oxygenation. As a consequence, lowerlevels of haemoglobin concentration can be safely toler-ated. Towards the end of the operation, the autologousblood harvested during ANH is retransfused. This willresult in a relatively high haemoglobin concentration inthe postoperative period and oxygen delivery will again beprovided by endogenous haemoglobin. Therefore, greatlyelevated arterial partial oxygen tension values are not nec-essary in the postoperative period and the relatively shorthalf-life of perfluorocarbon emulsions (<24h) will notcompromise their success in reducing allogeneic bloodtransfusion requirement (Fig. 2).
For the concept of augmented ANH, it is important not tocompromise blood coagulation during the surgical proce-dure [1,6], otherwise blood loss might be enhanced andthus allogeneic blood savings limited. Therefore, a carefulselection of colloids is necessary to avoid blood coagula-tion becoming compromised [23].
Apart from the use of perfluorocarbon emulsions to reduceallogeneic blood transfusions in surgery, there are numer-ous other potential future indications based on their poten-tial to augment tissue oxygenation. Such future indicationswill probably include treatment and prevention of cerebralischaemia, stroke, cardiopulmonary bypass-related cerebraladverse events, spinal cord ischaemia, myocardialischaemia due to acute infarction, percutaneous coronaryangioplasty, acute limb ischaemia, emergency surgery andtrauma as long as no allogeneic blood is available [21], anddecompression sickness. Other applications include theuse of perfluorocarbon emulsions to augment tumour oxy-genation to render them more sensitive to radiation andchemotherapy, to prevent or treat sequelae of airembolism, and finally to improve organ preservation forsubsequent organ transplantation (referenced in [1]).
References1. Keipert PE: Perfluorochemical emulsions: future alternatives to
transfusion. Blood Subst Princ Meth Prod Clin Trials 1998;2:127–156.
2. Spahn DR, Leone BJ, Reves JG, Pasch T: Cardiovascular and coro-nary physiology of acute isovolemic hemodilution: a review ofnonoxygen-carrying and oxygen-carrying solutions. Anesth Analg1994; 78:1000–1021.
3. Riess JG: Overview of progress in the fluorocarbon approach to invivo oxygen delivery. Biomater Artif Cells Immobil Biotechnol 1992;20:183–202.
4. Riess JG, Keipert PE: Update on perfluorocarbon-based oxygendelivery systems. In: Blood Substitutes: Present and Future Per-spectives. Edited by Tsuchida E. Lausanne: Elsevier Science SA,1998:91–102.
5. Keipert PE, Faithfull NS, Roth DJ, et al: Supporting tissue oxygena-tion during acute surgical bleeding using a perfluorochemical-based oxygen carrier. Adv Exp Med Biol 1996; 388:603–609.
6. Monk TG, Winston RS, Wahr JA, et al, Perflubron Emulsion StudyGroup: Safety and coagulation profile following administration ofperflubron emulsion in patients undergoing moderate blood losssurgery [Abstract]. Anesthesiology 1998; 89 (suppl):A397.
7. Rosoff JD, Soltow LO, Vocelka CR, et al: A second-generation bloodsubstitute (perfluorodichlorooctane emulsion) does not activatecomplement during an ex vivo circulation model of bypass. J Car-diothorac Vasc Anesth 1998; 12:397–401.
8. Van De Water JM, Kagey KS, Miller IT, et al: Response of the lung tosix to 12 hours of 100 per cent oxygen inhalation in normal man.N Engl J Med 1970; 283:621–626.
9. Tinits P: Oxygen therapy and oxygen toxicity. Ann Emerg Med1983; 12:321–328.
10. Eckstein EC, Koleski JF, Waters CM: Concentration profiles of 1 and2.5 microns beads during blood flow. Hematocrit effects. ASAIOTrans 1989; 35:188–190.
11. Keipert PE, Faithfull NS, Bradley JD, et al: Oxygen delivery augmen-tation by low-dose perfluorochemical emulsion during profoundnormovolemic hemodilution. Adv Exp Med Biol 1994;345:197–204.
12. Hogan MC, Willford DC, Keipert PE, Faithfull NS, Wagner PD:Increased plasma O2 solubility improves O2 uptake of in situ dogmuscle working maximally. J Appl Physiol 1992; 73: 2470–2475.
13. Mosca RS, Rohs TJ, Waterford RR, et al: Perfluorocarbon supple-mentation and postischemic cardiac function. Surgery 1996;120:197–204.
R96 Critical Care 1999, Vol 3 No 5
Figure 2
The concept of augmented acute normovolemic haemodilution(A-ANH) is divided into three periods (a–c). (a) Preoperative ANH withconventional volume replacement without the use of an artificial oxygencarrier such as a perfluorocarbon emulsion. Preoperative ANH targetsrelatively low hemoglobin levels, close to the individual transfusiontrigger. (b) During surgery when the haemoglobin concentration isexpected to fall further due to surgical blood loss, a perfluorocarbonemulsion will be used to augment oxygen-offloading capacity to thebody. Note that total oxygen offloading capacity from combinedhaemoglobin-based and perfluorocarbon emulsion-based oxygentransport is maintained during surgery at the level reached afterpreoperative ANH (ie above the individual transfusion trigger, despitelow haemoglobin concentrations towards the end of surgery).(c) Postoperative retransfusion (Postop. RT) of ANH blood increasesthe haemoglobin concentration above the individual transfusion trigger.Therefore, the decreasing contribution of PFC emulsion-based oxygentransport will not adversely affect overall oxygenation of the organism.
14. Habler OP, Kleen MS, Hutter JW, et al: Hemodilution and intra-venous perflubron emulsion as an alternative to blood transfu-sion: effects on tissue oxygenation during profound hemodilutionin anesthetized dogs. Transfusion 1998; 38:145–155.
15. Holman WL, Spruell RD, Ferguson ER, et al: Tissue oxygenationwith graded dissolved oxygen delivery during cardiopulmonarybypass. J Thorac Cardiovasc Surg 1995; 110:774–785.
16. Stern SA, Dronen SC, McGoron AJ, et al: Effect of supplemental per-fluorocarbon administration on hypotensive resuscitation of severeuncontrolled hemorrhage. Am J Emerg Med 1995; 13:269–275.
17. Manning JE, Batson DN, Payne FB, et al: Selective aortic arch perfu-sion during cardiac arrest: enhanced resuscitation using oxy-genated perflubron emulsion, with and without aortic archepinephrine. Ann Emerg Med 1997; 29:580–587.
18. Habler OP, Kleen MS, Hutter JW, et al: Effects of hyperoxic ventila-tion on hemodilution-induced changes in anesthetized dogs.Transfusion 1998; 38:135–144.
19. Habler OP, Kleen MS, Hutter JW, et al: Iv perflubron emulsionversus autologous transfusion in severe normovolemic anemia:Effects on left ventricular perfusion and function. Res Exp Med1998; 197:301–318.
20. Wahr JA, Trouwborst A, Spence RK, et al: A pilot study of the effectsof a perflubron emulsion, AF 0104, on mixed venous oxygentension in anesthetized surgical patients. Anesth Analg 1996; 82:103–107.
21. Spahn DR, van Bremt R, Theilmeier G, et al: Perflubron EmulsionStudy Group: Perflubron emulsion delays blood transfusion inorthopedic surgery. Anesthesiology 1999; in press.
22. Monk TG, Winston RS, Wahr JA, et al, Perflubron Emulsion StudyGroup: Perflubron emulsion is more effective than blood for trans-fusion trigger reversal [Abstract]. Anesth Analg 1998; 86(suppl):S142.
23. Egli GA, Zollinger A, Seifert B, et al: Effect of progressive haemodi-lution with hydroxyethyl starch, gelatin and albumin on bloodcoagulation. An in vitro thrombelastography study. Br J Anaesth1997; 78:684–689.
24. Looker D, Abbott-Brown D, Cozart P, et al: A human recombinanthaemoglobin designed for use as a blood substitute. Nature 1992;356:258–260.
Mini-review Perfluorocarbon emulsions Spahn R97