blended training for combat medics - nasa · blended training for combat medics ... • pressure...
TRANSCRIPT

123
Blended Training for Combat Medics
Jennifer Fowlkes1, Sandra Dickinson2
, and Todd Lazarus3
1CHI Systems, [email protected]
2 US Army Research Development & Engineering Command (RDECOM)SFC Paul Ray Smith Simulation & Training Technology Center (SnC)
3 University of Central FloridaInstitute for Simulation and Training
Abstract. Bleeding from extremity wounds is the number one cause of preventable death on thebattlefield and current research stresses the importance of training in preparing every Soldier to usetourniquets. HapMed is designed to provide tourniquet application training to combat medics andSoldiers using a blended training solution encompassing information, demonstration, practice, andfeedback. The system combines an instrumented manikin arm, PDA, and computer. The manikin armprovides several training options including stand-alone, hands-on skills training in which soldiers canexperience the actual torque required to staunch bleeding from an extremity wound and be timed ontourniquet application. This is more realistic than using a block of wood to act as a limb, which is oftenhow training is conducted today. Combining the manikin arm with the PDA allows instructors to providescenario based training. In a classroom or field setting, an instructor can specify wound variables suchas location, casualty size, and whether the wound is a tough bleed. The PDA also allows more detailedfeedback to be provided. Finally, combining the manikin arm with game-based technologies, the thirdcomponent, provides opportunities to build knowledge and to practice battlefield decision making. Notonly do soldiers learn how to apply a tourniquet, but when to apply a tourniquet in combat. The purpose ofthe paper is to describe the learning science underlying the design of HapMed, illustrate the trainingsystem and ways it is being expanded to encompass other critical life-saving tasks, and report onfeedback received from instructors and trainees at military training and simulation centers.
1.0 INTRODUCTION
Combat medics provide front line trauma careoften in the heat of a battle, with limitedresources, and under enormous stress. Inmodern warfare, medics serve as soldiers first,in keeping with the philosophy that "The bestmedicine on the battlefield is fire superiority't6]but must be able to transition to a medic rolequickly and decisively in accordance with thetactical situation. In these situations, medicsrespond to complex medical trauma. Mostinjuries on the battlefield are the result ofexplosions (from landmines and ImprovisedExplosive Devices) and gun shot wounds, eachof which presents challenges. Combat medicsmust not only understand the nature of warrelated injuries but also the implications forprocedures that will be effective. Moreover, asMazurek and Burgess [5] point out, decisions
regarding casualty treatment are made basednot only on the special knowledge of war-relatedinjuries, but also on the understanding of thetactical environment, current location, resourcesavailable, and own capabilities. Clearly, thereare significant training needs in regard tocombat medics
The purpose of this paper is to describe theHapMed training system which is aimed atfUlfilling at least some of the combat medictraining needs. HapMed was designed toprovide hands-on training to combat medics,addressing the three most common preventablepoint-of-injury deaths in combat: tourniquetapplication for hemorrhage control, needle chestdecompression to relieve tension pneumothorax(air trapped within the chest cavity resulting in acollapsed or compressed lung), and creating anairway (this is generally a preventive measure toensure a casualty airway remains open while
https://ntrs.nasa.gov/search.jsp?R=20100012846 2018-07-20T15:09:37+00:00Z
124
1.3 Challenge 3: Medics serve in low densityMOS assignments
Medics are one of the most common militaryoccupational specialties, yet perhaps 70% of
• complications that can arise when applying atourniquet
• differences among the different types oftourniquets.
Thus, training systems are needed that providehands-on training and support the acquisition ofthis type of knowledge.
1.2 Challenge 2: Tourniquets are Associatedwith Misinformation
Until recently, the tourniquets carried by soldierswere ineffective - they did not provide amechanical advantage that would help applyenough force to stop bleeding from a significantextremity wound and their narrow widthsresulted in excessive damage to limbs. As aresult, tourniquet use was shunned by civilianmedicine and myths abounded in both militaryand civilian sectors, some of which aresummarized in Table 1. Recent tourniquets,including the CAT and the Special OperationsForces Tourniquet greatly minimize or eliminatethese problems and recent research suggeststhey are highly effective [7]. Thus, our analysisindicated that hands-on training should besupplemented by didactic instruction thataddressed misconceptions surrounding the useof tourniquets.
Table 1: Misinformation associated withttourmque use
Myth Current GuidanceIt is good to The tourniquet shouldoccasionally loosen a remain in place withtourniquet to allow the blood flowsome blood to get to completely stoppedthe damaged limb. until it can be removed.
Occasionally looseningthe tourniquet mayresult in death of thecasualty.
Once a tourniquet is A tourniquet canapplied the casualty remain in place forwill lose his or her several hours withoutlimb. causing major damage
to the limb.Tourniquets should Tourniquets should beonly be used as a last applied to extremityresort. wounds as soon as
tactically feasible.
medic is treating another soldier). The Army hasrecently enhanced training of these and relatedtasks within combat medic training programs,including the Tactical Combat Casualty Care(TC3) courses [1]. TC3 was developed inresponse to the growing recognition that medicalcare on the battlefield requires different skillsand mindsets compared to civilian approaches.
The design of HapMed was supported bycognitive engineering techniques includingfocused cognitive task analysis (CTA) to identifycritical cues, decisions, and strategies thatsupport task performance; observation ofcombat medic training; user feedback asprototypes and artifacts were developed; andtraining research. Our front end analysesrevealed several challenges in regard to combatmedic training [8]. Specifically, we facedchallenges in four areas.
1.1 Challenge 1: Need for Hands-on Training
Despite the recent changes in medic training(e.g., TC3), there are few opportunities toreceive hands-on practice. A well-practice skillsuch as tourniquet application may require atleast tens, and maybe hundreds, of trainingtrials, but there are few existing opportunities toget extensive hands-on practice. A commonapproach is to have .students apply a combatapplication (CAT) tourniquet to a 2x4 board.While students may learn procedural knowledgethis way, they do not receive tactile feedback onhow tight a tourniquet must be to stop bloodflow. This is a significant training need fortourniquet application as this quote suggests.
In the case of lower extremitywounds, which give rise to themost severe hemorrhagecontrolled by tourniquet, it hasbeen my observation, that toofew doctors, much less theirassistants, have a concept ofthe constricting pressurerequired about the thigh toabolish the flow of blood.(Emergency Treatment andResuscitation at the BattalionLevel by MAJ Meredith Mallory1954)
There are other related drawbacks to currenttraining. Students do not gain the knowledge of• how long it will take to apply a tourniquet;• the influence of the size of the casualty on
how long it will take to apply a tourniquet;

125
medics serve in low density assignments,meaning that they are assigned to infantry orarmor battalions and their numbers are smallcompared to other MOSs in their units. Oneconsequence is that training resources arelimited. Thus, training systems supportingmedics must be low cost, durable, and reliable.
1.4 Challenge 4: Combat medics must learnto perform under intense battlefield stress
During the CTA, the harsh realities and complexenvironment in which combat medics workbecame clear. Medics perform in environmentsdefined by intense time pressure, danger,complex and sometimes horrific injuries, and themany factors that impede or play a part intactical decision making including tactical,medical, interpersonal, and environmentalstressors. The importance of training medics towork effectively under these conditions wasreinforced through interviews with subject matterexperts and reviews of lessons learned.However, in examining existing curricula, wefound few opportunities to systematicallypractice combat medicine under these "fog ofwar" conditions. Lane training and fieldexercises provide immersive, realistic practice,yet there are a very limited number of theseopportunities. Moreover, in field exercises withtheir assigned units, it is often the case thatcombat medicine is not the primary focus oftraining and sometimes it is not addressed at all.
2.0 HAPMED TRAINING SYSTEM
Our solution to the challenges we uncoveredduring our front end analyses was to design anddevelop a blended training solution. By blendedsolution we mean incorporating complementarytraining interventions linked to the challenges ortraining needs discussed above. The HapMedtraining system, currently in prototype form,includes an instrumented manikin arm to providehands-on skills training for tourniquetapplication, a PDA that wirelessly controls thearm to provide scenario-based training; andgame based didactic instruction to further buildknowledge and skills required of medics on thebattlefield. Finally, we performed trainingresearch from which we determined that hapticand audio stimili can be combined inexpensivelyto serve as surrogate stressors. Thesecomponents are described below.
2.1 HAPMED Manikin Arm for TourniquetTraining
The HapMed manikin arm, pictured in Figure 1,was designed to provide stand-alone, hands-onskills training (as well as interact with the othersystem components) in which trainees canexperience the actual torque required to staunchbleeding from an extremity wound and be timedon tourniquet application [4]. The featuresdesigned into the arm were based on theessential cues for tourniquet applicationidentified from the CTA. The hardwarecomponents were based on our assessment oflow cost technologies that could be sufficientlyruggedized. In the current design of theprototype,• Bleeding is depicted through LED arrays
clustered at four different locations to representfour possible wound areas. Wound sites can beselected by the trainee or instructor.• Pressure sensors within the arm gauge the
amount of pressure being applied via atourniquet (or through other source of pressuresuch as squeezing with the hands at pressurepoints). The sensors were calibrated from dataobtained from surgical applications oftourniquets. (e.g., [3])• As the tourniquet is tightened, LED lights
on the arm indicate to the trainee that thebleeding is being slowed by the tourniquet.When the trainee has tightened the tourniquetenough, per amount of torque needed on anactual human, the red lights turn to greenindicating that the bleeding has beensuccessfully stopped.• A timer on the arm shows the number of
seconds that it took to stop the bleeding.• If a tourniquet is loosened once having
been applied, the "bleeding" will begin again(and the timer will start again).
Figure 1: HapMed manikin arm prototype.• A pulse can be felt that weakens as the
tourniquet is applied.• The arm will respond realistically to almost
any tourniquet. This provides a tool to be used

126
by medical personnel to try out or comparedifferent tourniquets.• The arm can be affixed to a full body
manikin or to a wall (see Figure 3).
During the course of development a great dealof feedback was obtained from the combatmedic community regarding the arm. Inaddition, we conducted a more formal try outwith a National Guard unit during which the armwas incorporated into combat medic and combatlifesaver training. This work has resulted in thedesign of a system suitable for use by themilitary.
2.2 HapMed PDA
The sensitivity of the pressure sensors on theHapMed arm can be manipulated throughwireless connections so that different body sizescan be simulated, a feature that we incorporatedinto a PDA interface. The HapMed PDAprovides a portable and intuitive interface tospecify training scenario parameters such aswound location, casualty size, and whether thewound will require more than one tourniquet--these are all distinctions a medic or combatlifesaver needs to know when applying atourniquet in combat. The PDA also providesperformance feedback to trainees. Specifically,the PDA shows the location of the tourniquet(s)applied to the arm and indicates whether theyhave been placed correctly (2-4 inches abovethe wound site), the amount pressure beingapplied relative to the amount of bleeding, timeto control bleeding, and status of the casualty.Finally, the PDA provides prompts that can beused by an instructor to facilitate discussionabout the variables important in tourniquetapplication. The PDA can be used by aninstructor to control the manikin arm in aclassroom or in the field as part of lane training.
Figure 2 shows one of the PDA screens. Figure3 shows an instructor using the PDA towirelessly control the arm during combat medictraining. Our usability evaluations showed thatinstructors could easily and immediately use thePDA. Much of the feedback we obtainedpertained to additional controls and features thatinstructor's would like to see incorporated intothe PDA.
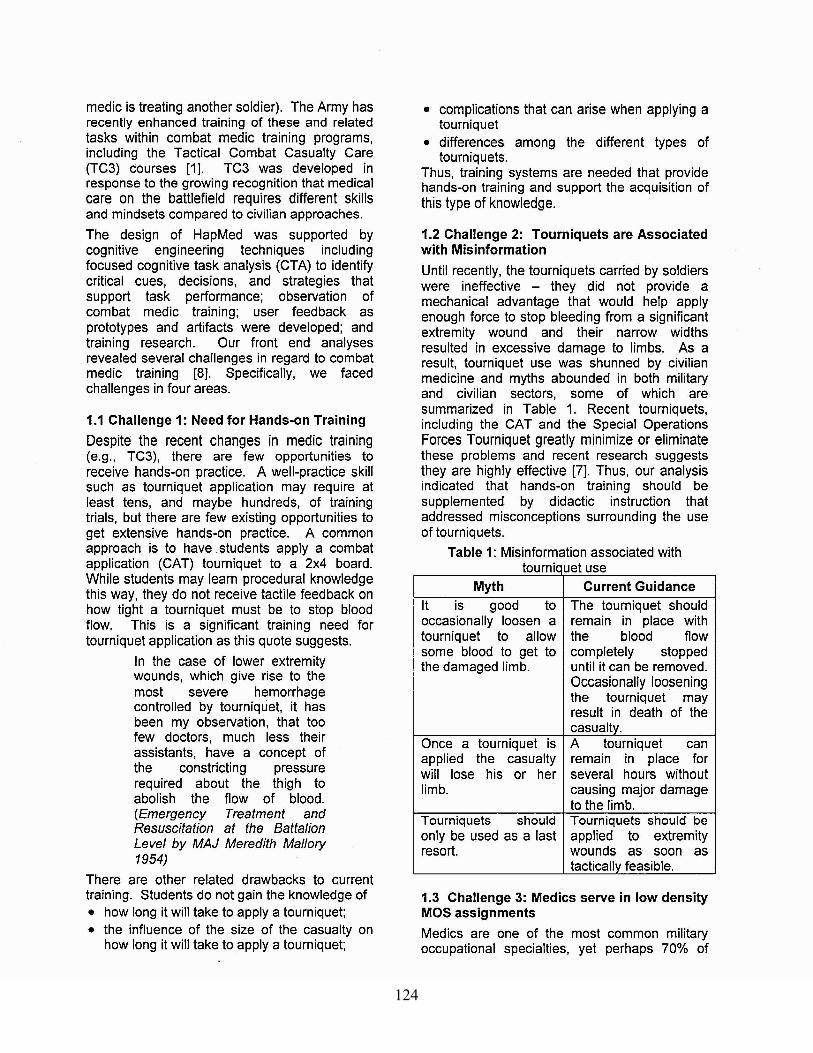
2.3 Game-based Training
A computer-based training framework wasdesigned that would allow trainees to accessgame-based training modules, combat medic
stories, and demonstrations that would interactwirelessly with the manikin arm. The gamebased training modules were the componentsthat we initially developed for the HapMedprototype. These included training modulesfocused on myths associated with tourniquetapplications and identification of injuries suitablefor tourniquets (screen for which is shown inFigure 4). In addition, a scenario-baseddecision making exercise was created. To
Figure 2: HapMed PDA scenario control screen.
Figure 3: Instructor using the PDA.
127
enhance the training, each of the trainingmodules sets the stage for the trainee throughan advanced organizer, provides performanceperformance feedback, and concludes with aguided reflection exercise. The game-basedinstruction has, thus far, received the leastattention in terms of validation work. We intendto evaluate the effectiveness of the game-basedtraining format compared to more traditionalmethods for information presentation in futurework.
Figure 4: Card sort game-based trainingmodule screen.
2.4 Stress Training
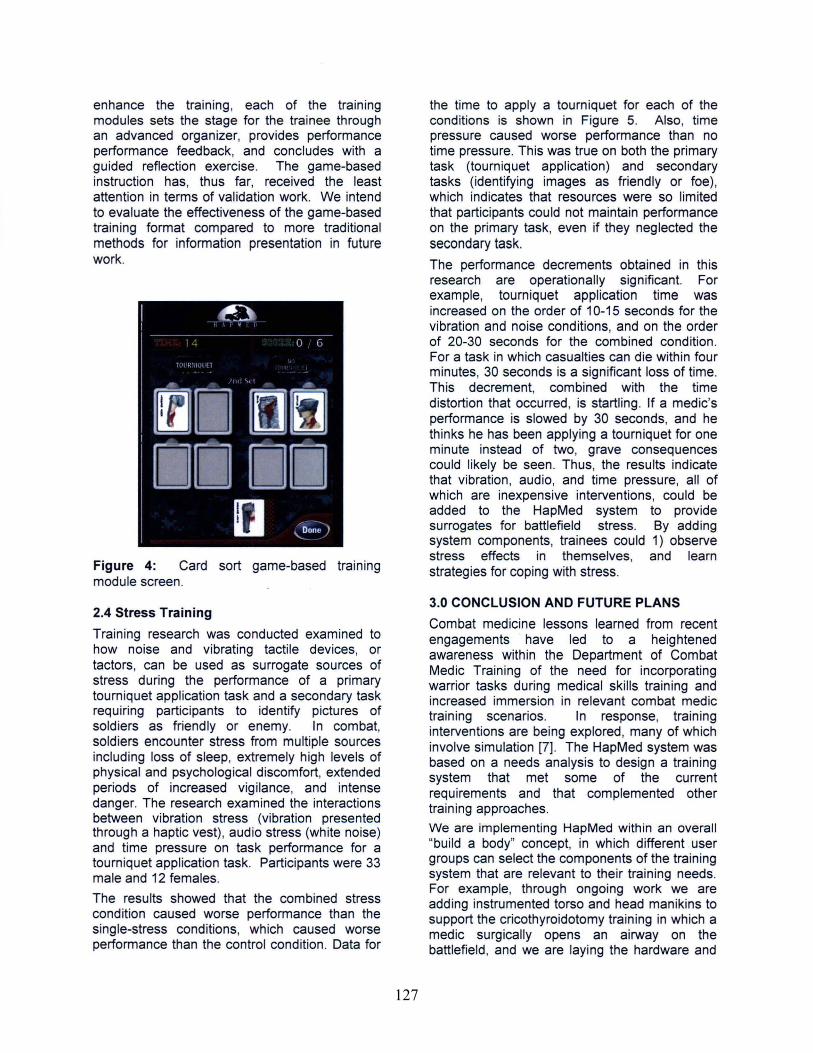
Training research was conducted examined tohow noise and vibrating tactile devices, ortactors, can be used as surrogate sources ofstress during the performance of a primarytourniquet application task and a secondary taskrequiring participants to identify pictures ofsoldiers as friendly or enemy. In combat,soldiers encounter stress from multiple sourcesincluding loss of sleep, extremely high levels ofphysical and psychological discomfort, extendedperiods of increased vigilance, and intensedanger. The research examined the interactionsbetween vibration stress (vibration presentedthrough a haptic vest), audio stress (white noise)and time pressure on task performance for atourniquet application task. Participants were 33male and 12 females.
The results showed that the combined stresscondition caused worse performance than thesingle-stress conditions, which caused worseperformance than the control condition. Data for
the time to apply a tourniquet for each of theconditions is shown in Figure 5. Also, timepressure caused worse performance than notime pressure. This was true on both the primarytask (tourniquet application) and secondarytasks (identifying images as friendly or foe),which indicates that resources were so limitedthat participants could not maintain performanceon the primary task, even if they neglected thesecondary task.
The performance decrements obtained in thisresearch are operationally significant. Forexample, tourniquet application time wasincreased on the order of 10-15 seconds for thevibration and noise conditions, and on the orderof 20-30 seconds for the combined condition.For a task in which casualties can die within fourminutes, 30 seconds is a significant loss of time.This decrement, combined with the timedistortion that occurred, is startling. If a medic'sperformance is slowed by 30 seconds, and hethinks he has been applying a tourniquet for oneminute instead of two, grave consequencescould likely be seen. Thus, the results indicatethat vibration, audio, and time pressure, all ofwhich are inexpensive interventions, could beadded to the HapMed system to providesurrogates for battlefield stress. By addingsystem components, trainees could 1) observestress effects in themselves, and learnstrategies for coping with stress.
3.0 CONCLUSION AND FUTURE PLANS
Combat medicine lessons learned from recentengagements have led to a heightenedawareness within the Department of CombatMedic Training of the need for incorporatingwarrior tasks during medical skills training andincreased immersion in relevant combat medictraining scenarios. In response, traininginterventions are being explored, many of whichinvolve simulation [7]. The HapMed system wasbased on a needs analysis to design a trainingsystem that met some of the currentrequirements and that complemented othertraining approaches.
We are implementing HapMed within an overall"build a body" concept, in which different usergroups can select the components of the trainingsystem that are relevant to their training needs.For example, through ongoing work we areadding instrumented torso and head manikins tosupport the cricothyroidotomy training in which amedic surgically opens an airway on thebattlefield, and we are laying the hardware and

128
software foundations to support nasopharyngealand needle chest decompression training. Asthese components are added, we plan tocontinue the evaluation research efforts todetermine training system effectiveness, identifyusability issues, and identify useful trainingniches such as was accomplished through thestress research. We believe a blended trainingsolution, providing opportunities for information,demonstration, practice and feedback, in aninexpensive training suite, will be one key to theeffectiveness of the HapMed system.
4.0 REFERENCES
1. Butler et al. (2008). Tactical combatcasualty care for 2007. Section I: Evolvingconcepts and battlefield experience. Journalof Special Operations Medicine. Trainingsupplement to Volume 8 (4).
2. Fowler, S. Smith, B. & Litteral, D. (2005). ATC3 Gamebased Simulation for CombatMedic Training. Proceedings of theInterservicellndustry Training, Simulation &Education Conference. Orlando, FL.
3. Klenerman L. & Hulands G.H. (1979).Tourniquet pressure for the lower limb. JBone Joint Surg, 61 B:124.
4. Lazarus, T.; Martin, G.A.; Nayeem, R.,Fowlkes, J. & Riddle, D. (2008). E-MA T: TheExtremities Multiple Application Trainer forHaptics-based Medical Training. Paperpresented at the Virtual Reality Conference,2008.
5. Mazurek, M.T. & Burgess, A.R. (2006)Moderator's summary: Stabilization of longbones. Journal of the American Academy ofOrthopaedic Surgeons, 14, S113-S117.
6. Parsons, D. (2004). Tourniquets:Lifesavers on the battlefield. Journal ofSpecial Operations Medicine, 4(4), 51-53.
7. Richey, S.L. (2007). Tourniquets for thecontrol of traumatic hemorrhage: a review ofthe literature. World Journal of EmergencySurgery 2. Retrieved 8/20/09 fromhttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2151 059
8. Riddle, D. L., Fowlkes, J., Lazarus, T.,Martin, G., Daly, J., & Fowler, S. (2006).Integrating instructional strategies andhaptic technologies to enhance the trainingefficacy of an Army 91W (Combat Medic)medical skills training simulation.Proceedings of the Human Factors andErgonomics Society 4£fh Annual Meeting[CDROM]. San Francisco, California:HFES.
ACKNOWLEDGEMENTSThe authors would like to express our thanks toRetired Lieutenant Colonel Donald L. Parsons,PA-C, with the Department of Combat MedicTraining, Fort Sam Houston, TX, for sogenerously sharing his time and expertise, forhis efforts to ensure the HapMed team receivesquality domain knowledge to support 91W10instruction.
70 ~---------------------------,
60 +----------------------
10
o
Q)
Ei=
-Q)~
.!2'c:; _ 50 +-----------------------o III~ 't:I 40 +------------------------~5~ ~ 30 +---------c:r:'"0-20-
Baseline Vibration Audio Combined
Figure 5: R~sults from the stress research.