biologic width: an important link between periodontics …jdsor.com/2016vol7-3/a7.pdf · biologic...
TRANSCRIPT

Biologic Width: An Important Link between Periodontics and Restorative Dentistry
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):125-130 125
JDSORJDSOR
Biologic Width: An Important Link between Periodontics and Restorative Dentistry1Pooja Mittal, 2RG Shiva Manjunath, 3Jaishree Garg, 4Ashish Agarwal, 5Himanshi Agarwal, 6Sana Khan
ABStRAct
A thorough understanding of the relationship between periodon-tal tissues and restorative dentistry is of utmost importance to ensure adequate form, function, esthetics, and comfort of the dentition. Most clinicians are familiar with the term biologic width, still confusion exists regarding its meaning and relevance to clinical procedures. An attempt has been made in this review article for the better understanding of the concept of biologic width and its implications in the maintenance of periodontal and restorative procedures. Lastly, we have discussed the various methods for the assessment of biologic width and surgical and non-surgical methods to correct it.
Keywords: Biologic width, Crown lengthening, Crown margins, Junctional epithelium, Periodontal surgery.
How to cite this article: Mittal P, Manjunath RGS, Garg J, Agarwal A, Agarwal H, Khan S. Biologic Width: An Important Link between Periodontics and Restorative Dentistry. J Dent Sci Oral Rehab 2016;7(3):125-130.
Source of support: Nil
Conflict of interest: None
INtRODUctION
Healthy periodontal tissues are the foundation for proper esthetics, function, and comfort to the patient. A healthy periodontium is a prerequisite for successful treatment outcome of all prosthetic and restorative treatment modalities. The interplay between periodontics and restorative dentistry is present at many fronts, including location of margins of restorations, crown contours, and response of the gingival tissues to restorations. As stated by Bryan, “We must keep constantly in mind that the dental restorations we make have a twofold purpose; the restoration of the tooth or teeth to function and the protec-tion of the supporting tissues from injury.”1 It is hence, evident that restorative procedures not only must con-sider the mechanical specifications, but also must fulfill the biologic requirement.
REVIEW ARTICLE
1,5,6Postgraduate Student, 2Professor and Head, 3,4Reader1-6Department of Periodontics and Implantology, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India
Corresponding Author: Pooja Mittal, Postgraduate Student Department of Periodontics and Implantology, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India, Phone: +919456455129 e-mail: [email protected]
10.5005/jp-journals-10039-1125
BIOLOGIc WIDtH
The term “biologic width” is familiar to most clinicians, still confusion exists regarding its meaning and relevance to clinical procedures. The biologic width is defined as the dimension of the soft tissue, which is attached to the portion of the tooth coronal to the crest of the alveolar bone. The research by Gargiulo et al,2 who described the dimensions and relationship of the dentogingival junction in humans, formed the basis of this term. Measurements made from the dentogingival components of 287 indi-vidual teeth from 30 autopsy specimens confirmed that there is an identifiable proportional relationship between the alveolar crest, the connective tissue attachment, the epithelial attachment, and the sulcus depth. Gargiulo et al reported the following mean dimensions: A sulcus depth of 0.69 mm, an epithelial attachment of 0.97 mm, and a connective tissue attachment of 1.07 mm. Based on this work, the biologic width is commonly stated to be 2.04 mm, which represents the sum of the epithelial and connective tissue measurements. It must, however, be considered that significant variations of dimensions were observed, particularly the epithelial attachment, which ranged from 1.0 to 9.0 mm. The connective tissue attach-ment was observed to be a relatively constant entity. Vacek et al3 also reported similar biologic width dimensions. On evaluation of 171 cadaver tooth surfaces, they observed mean measurements of 1.34 mm for sulcus depth, 1.14 for epithelial attachment, and 0.77 mm for connective tissue attachment. They also concluded that the connective tissue attachment was the most consistent measurement (Fig. 1).
Fig. 1: Biologic width4
Pooja Mittal et al
126
VIOLAtION OF BIOLOGIc WIDtH
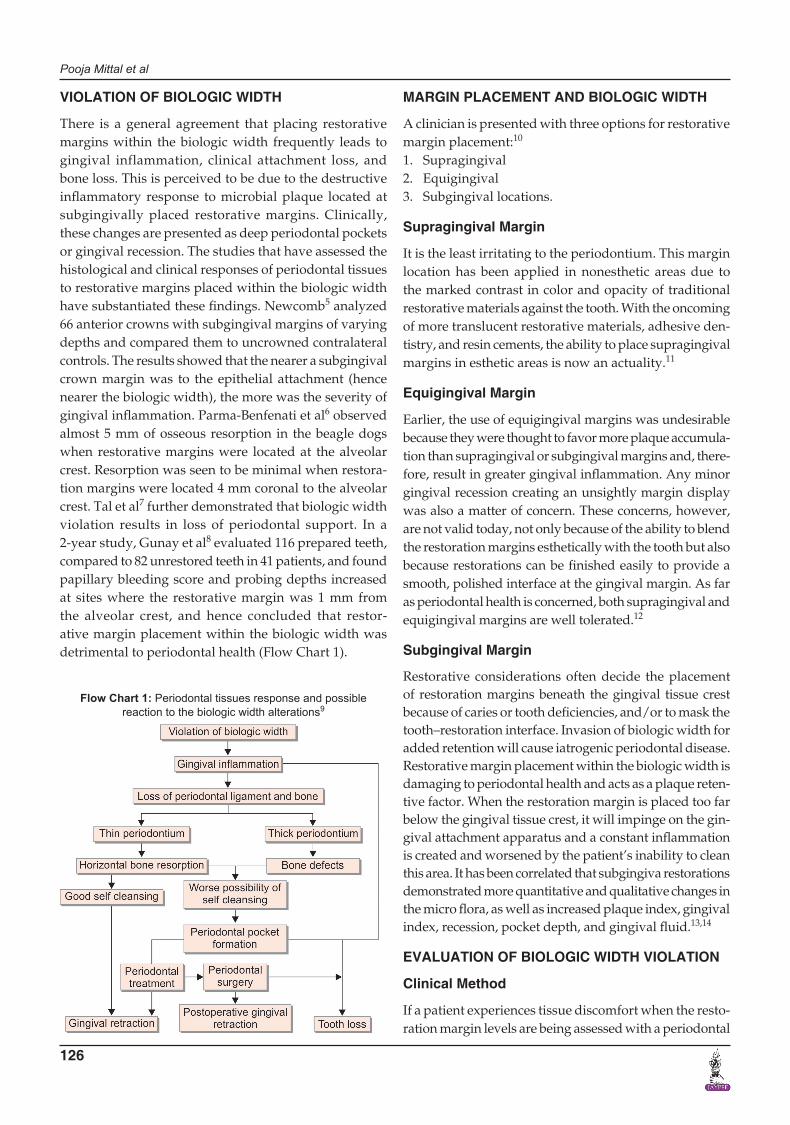
There is a general agreement that placing restorative margins within the biologic width frequently leads to gingival inflammation, clinical attachment loss, and bone loss. This is perceived to be due to the destructive inflammatory response to microbial plaque located at subgingivally placed restorative margins. Clinically, these changes are presented as deep periodontal pockets or gingival recession. The studies that have assessed the histological and clinical responses of periodontal tissues to restorative margins placed within the biologic width have substantiated these findings. Newcomb5 analyzed 66 anterior crowns with subgingival margins of varying depths and compared them to uncrowned contralateral controls. The results showed that the nearer a subgingival crown margin was to the epithelial attachment (hence nearer the biologic width), the more was the severity of gingival inflammation. Parma-Benfenati et al6 observed almost 5 mm of osseous resorption in the beagle dogs when restorative margins were located at the alveolar crest. Resorption was seen to be minimal when restora-tion margins were located 4 mm coronal to the alveolar crest. Tal et al7 further demonstrated that biologic width violation results in loss of periodontal support. In a 2-year study, Gunay et al8 evaluated 116 prepared teeth, compared to 82 unrestored teeth in 41 patients, and found papillary bleeding score and probing depths increased at sites where the restorative margin was 1 mm from the alveolar crest, and hence concluded that restor-ative margin placement within the biologic width was detrimental to periodontal health (Flow Chart 1).
MARGIN PLAcEMENt AND BIOLOGIc WIDtH
A clinician is presented with three options for restorative margin placement:10
1. Supragingival2. Equigingival3. Subgingival locations.
Supragingival Margin
It is the least irritating to the periodontium. This margin location has been applied in nonesthetic areas due to the marked contrast in color and opacity of traditional restorative materials against the tooth. With the oncoming of more translucent restorative materials, adhesive den-tistry, and resin cements, the ability to place supragingival margins in esthetic areas is now an actuality.11
Equigingival Margin
Earlier, the use of equigingival margins was undesirable because they were thought to favor more plaque accumula-tion than supragingival or subgingival margins and, there-fore, result in greater gingival inflammation. Any minor gingival recession creating an unsightly margin display was also a matter of concern. These concerns, however, are not valid today, not only because of the ability to blend the restoration margins esthetically with the tooth but also because restorations can be finished easily to provide a smooth, polished interface at the gingival margin. As far as periodontal health is concerned, both supragingival and equigingival margins are well tolerated.12
Subgingival Margin
Restorative considerations often decide the placement of restoration margins beneath the gingival tissue crest because of caries or tooth deficiencies, and/or to mask the tooth–restoration interface. Invasion of biologic width for added retention will cause iatrogenic periodontal disease. Restorative margin placement within the biologic width is damaging to periodontal health and acts as a plaque reten-tive factor. When the restoration margin is placed too far below the gingival tissue crest, it will impinge on the gin-gival attachment apparatus and a constant inflammation is created and worsened by the patient’s inability to clean this area. It has been correlated that subgingiva restorations demonstrated more quantitative and qualitative changes in the micro flora, as well as increased plaque index, gingival index, recession, pocket depth, and gingival fluid.13,14
EVALUAtION OF BIOLOGIc WIDtH VIOLAtION
clinical Method
If a patient experiences tissue discomfort when the resto-ration margin levels are being assessed with a periodontal
Flow Chart 1: Periodontal tissues response and possible reaction to the biologic width alterations9
Biologic Width: An Important Link between Periodontics and Restorative Dentistry
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):125-130 127
JDSOR
probe, it is a good indication of the extension of margin into the attachment and a biologic width violation. The biologic width violation presents the following signs: Chronic progressive gingival inflammation around the restoration, bleeding on probing, localized gingival hyperplasia with minimal bone loss, gingival recession, pocket formation, clinical attachment loss, and alveolar bone loss. Gingival hyperplasia is most frequently found in altered passive eruption and subgingivally placed restoration margins.11
Bone Sounding
The biologic width can be identified by probing to the bone level under local anesthesia (referred to as “sound-ing to bone”) and subtracting the sulcus depth from the resulting measurement. If this measurement is less than 2 mm at one or more location, biologic width violation can be a confirmed diagnosis. This measurement must be done on teeth with healthy gingival tissues and should be repeated on more than one tooth to ensure accurate assessment, and reduce individual and site variations.12
Radiographic Evaluation
Interproximal violations of biologic width can be assessed radiographically. However, for the mesiofacial and disto-facial line angles of teeth, radiographs are not diagnostic
because of tooth superimposition. Galgali and Gontiya15 have described a new innovative parallel profile radio-graphic (PPR) technique to measure the dimensions of the dentogingival unit. The PPR technique could be used to measure both length and thickness of the dentogingival unit with accuracy, as it was simple, concise, noninvasive, and a reproducible method.16
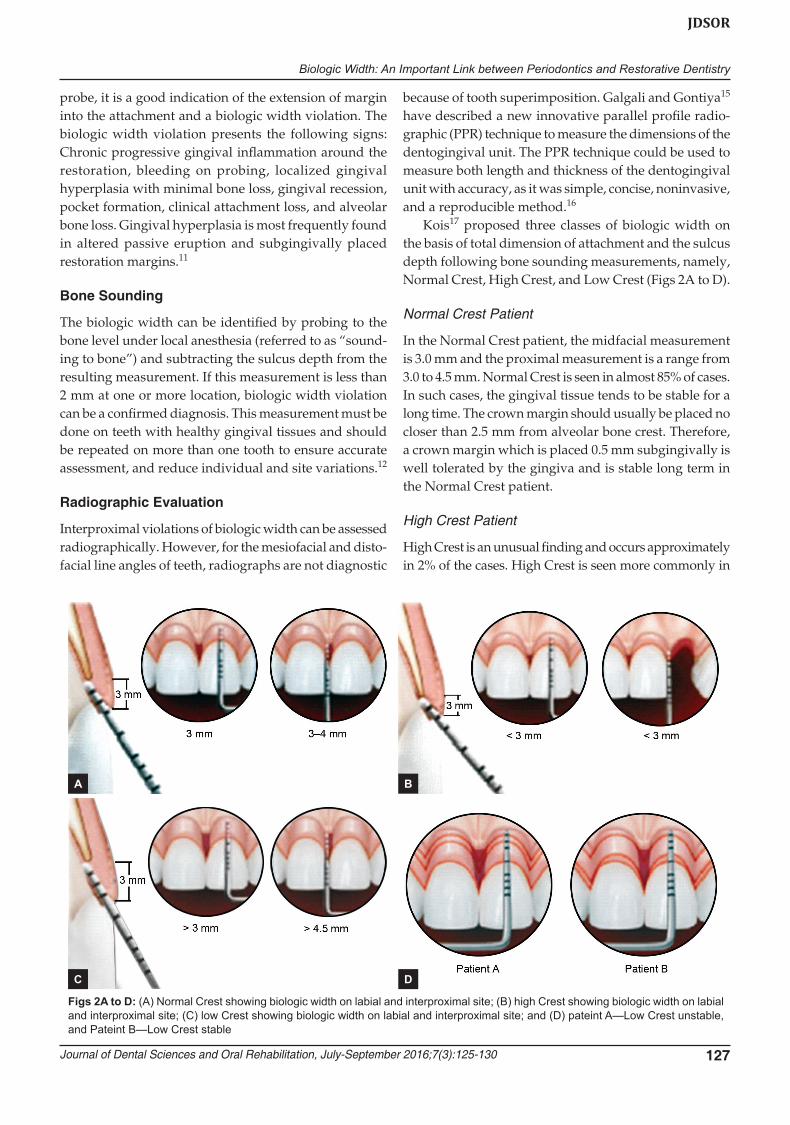
Kois17 proposed three classes of biologic width on the basis of total dimension of attachment and the sulcus depth following bone sounding measurements, namely, Normal Crest, High Crest, and Low Crest (Figs 2A to D).
Normal Crest Patient
In the Normal Crest patient, the midfacial measurement is 3.0 mm and the proximal measurement is a range from 3.0 to 4.5 mm. Normal Crest is seen in almost 85% of cases. In such cases, the gingival tissue tends to be stable for a long time. The crown margin should usually be placed no closer than 2.5 mm from alveolar bone crest. Therefore, a crown margin which is placed 0.5 mm subgingivally is well tolerated by the gingiva and is stable long term in the Normal Crest patient.
High Crest Patient
High Crest is an unusual finding and occurs approximately in 2% of the cases. High Crest is seen more commonly in
Figs 2A to D: (A) Normal Crest showing biologic width on labial and interproximal site; (B) high Crest showing biologic width on labial and interproximal site; (C) low Crest showing biologic width on labial and interproximal site; and (D) pateint A—Low Crest unstable, and Pateint B—Low Crest stable
A B
C D
Pooja Mittal et al
128
a proximal surface adjacent to an edentulous site. In the High Crest patient, the midfacial measurement is less than 3.0 mm and the proximal measurement is also less than 3.0 mm. In this situation, generally impossible to place an intracrevicular margin because the margin will be too close to the alveolar bone, resulting in a biologic width impingement and chronic inflammation.
Low Crest Patient
In the Low Crest patient group, the midfacial measurement is greater than 3.0 mm and the proximal measurement is greater than 4.5 mm. Low Crest occurs approximately in 13% of the cases. Traditionally, the Low Crest patient has been described as more susceptible to recession secondary to the placement of an intrasulcular crown margin. When retraction cord is placed subsequent to the crown prepara-tion; the attachment apparatus is routinely injured. As the injured attachment heals, it tends to heal back to a Normal Crest position, resulting in gingival recession.
Low Crest, Stable or Unstable
Low Crest attachment is actually more complex because all Low Crest patients do not react the same way to an injury to the attachment. Some Low Crest patients are susceptible to gingival recession while others have a quite stable attach-ment apparatus. The difference lies on the basis of the depth of the sulcus, which can have a wide range. For example, if patient A is bone sounded, the midfacial distance from the gingival crest to the alveolar crest is 5.0 mm, while patient B is bone sounded and the measurement is again 5.0 mm. They are not the same in spite of both being Low Crest. However, they are not the same. Patient A has a 3.0-mm sulcus and a 2.0-mm attachment (i.e., epithelium and con-nective tissue). In contrast, Patient B has a 1.0-mm sulcus and a 4.0-mm attachment (i.e., epithelium and connective tissue) (Fig. 2D). Patient A has 3.0 mm of unsupported tissue from the base of the sulcus to the gingival crest. This amount of unsupported gingival tissue tends to be unstable, and this patient is susceptible to gingival reces-sion. However, Patient B has a more substantial attachment apparatus (4.0 mm) and has a significantly shallower sulcus (1.0 mm). This patient has far less susceptibility to gingival recession. Patient A is classified as an Unstable Low Crest because the patient is more susceptible to gingival reces-sion. Patient B is classified as a Stable Low Crest because this patient reacts more like a Normal Crest patient and is not as susceptible to gingival recession.
Based on the sulcus depth the following three rules can be employed to place intracrevicular margins:1. If the sulcus probes 1.5 mm or less, the restorative
margin could be easily placed 0.5 mm below the gingival crest.
2. If the sulcus probes more than 1.5 mm, the restorative margin can be placed in half the depth of the sulcus.
3. If the sulcus is greater than 2 mm, gingivectomy could be performed to lengthen the tooth and create a 1.5 mm sulcus. Then the patient can be treated as per rule 1.15,18
cORREctION OF BIOLOGIc WIDtH VIOLAtION
Various methods have been advocated for the correction of biologic width violation:
Surgical crown Lengthening
Crown lengthening, as defined by Allen in 1993, is a sur-gical procedure aimed at exposing more tooth structure for restorative and/or esthetic reasons.19
Indications
Inadequate clinical crown for retention due to extensive caries, subgingival caries or tooth fracture, root perfora-tion, or root resorption within the cervical one-third of the root in teeth with adequate periodontal attachment.• Short clinical crowns• Placement of subgingival restorative margins• Unesthetic gingival levels• Altered/delayed passive eruption• Teeth with excessive occlusal wear or incisal wear• Teeth with inadequate interocclusal space for proper
restorative procedures due to supraeruption• Restorations which violate the biologic width• In conjunction with tooth requiring hemisection or
root resection.20
Contraindications
Deep caries or fracture requiring excessive bone removal.• Unesthetic outcomes after surgery• Tooth with improper crown–root ratio• Nonrestorable teeth• Tooth with increased risk of furcation involvement
post surgery.20
External Bevel Gingivectomy
Gingivectomy is a very successful and predictable sur-gical procedure for reconstruction of biologic width; however, it can be used only in situations with hyper-plasia or pseudopockets (>3 mm of biologic width) and presence of adequate amount of keratinized tissue.21
Internal Bevel Gingivectomy
Reduction of pocket depth and exposure of coronal tooth structure in the absence of a sufficient zone of attached

Biologic Width: An Important Link between Periodontics and Restorative Dentistry
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):125-130 129
JDSOR
gingiva with or without the need for correction of osseous abnormalities requires internal bevel gingivectomy.12
Apical Repositioned Flap Surgery
The apically positioned flap technique with/without bone recontouring (resection) may be used to expose sound tooth structure. It can be done in case of fracture or caries.12
Indication
Crown lengthening of multiple teeth in a quadrant or sextant of the dentition, root caries, and fractures.
Contraindication
Apically repositioned flap surgery should not be used during surgical crown lengthening of a single tooth in the esthetic zone.
Apically Repositioned Flap without Osseous Resection
This procedure is employed when there is no adequate width of attached gingiva and there is a biologic width of more than 3 mm on multiple teeth.
Apical Repositioned Flap with Osseous reduction
This technique is used when there is inadequate zone of attached gingiva and the biologic width is less than 3 mm. The alveolar bone is reduced by ostectomy and osteo-plasty, to expose the required tooth length in a scalloped fashion and to follow the required contour of the overlying gingiva.22 Elavarasu et al,23 in a report on surgical crown lengthening with apical repositioned flap with bone resec-tion performed in the fractured maxillary anterior teeth region, showed satisfactory results both in terms of esthetic as well as functional (restoring biologic width) outcomes.
Forced tooth Eruption
Heithersay24 and Ingber first suggested the use of “forced eruption” to treat “nonrestorable” or previously “hopeless” teeth. According to Starr, two concepts of forced eruption have been proposed: (i) Forced eruption with minimal osseous resection and (ii) forced eruption combined with fiberotomy.
Forced Eruption with Minimal Osseous Resection12
Indication
Crown lengthening at sites where removal of attachment and bone form adjacent teeth must be avoided.
Contraindication
The forced eruption technique employs the use of fixed orthodontic appliances. Thus, in patients who have only a few teeth remaining, an alternative approach for crown lengthening has to be selected.
Forced tooth Eruption with Fibrotomy
If fibrotomy is performed along with the forced tooth eruption procedure, the crestal bone and the gingival margin are maintained at their pretreatment location, and the tooth–gingiva interface at adjacent teeth is unaltered.25 Fibrotomy is performed with scalpel at 7 to 10 day inter-vals during the forced eruption to sever the supracrestal connective tissue fibers, thereby preventing the crestal bone from following the root in coronal direction.
Indication
Crown lengthening at sites where it is important to main-tain the location of the gingival margin at adjacent teeth.
Contraindication
Fibrotomy should not be used at teeth associated with angular bone defects, ectopically erupting tooth.
cONcLUSION
The health of the periodontal tissues is dependent on properly fabricated and placed restorations. Incorrectly placed restoration margin and unadapted restoration vio-lates the biologic width. Margin placement deep below the gingival margin often leads to a more pronounced plaque-induced inflammatory response. If restorative margins need to be placed near the alveolar crest, crown-lengthening surgical procedure or orthodontic extru-sion should be considered to provide adequate tooth structure while simultaneously assuring the integrity of the biologic width. Repeated maintenance visits, patient cooperation, and motivation are important for improved success of restorative procedures with a good periodontal health.
REFERENcES
1. Bryan AW. Restorations contributing to the injury of the sup-porting structures. J Am Dent Assoc 1927 Aug;14(8):1486-1489.
2. Gargiulo AW, Wentz F, Orban B. Dimensions and relations of the dentogingival junction in humans. J Periodontol 1961 Jul;32(3):261-267.
3. Vacek JS, Gher ME, Assad DA, Richardson AC, Giambarresi LI. The dimensions of the human dentogingival junction. Int J Periodontics Restorative Dent 1994 Apr;14(2):154-165.
4. Padbury A Jr, Eber R, Wang H-L. Interactions between the gingiva and the margin ofrestorations. J Clin Periodontol 2003 May;30(5):379-385.
Pooja Mittal et al
130
5. Newcomb GM. The relationship between the location of subgingival crown margins and gingival inflammation. J Periodontol 1974 Mar;45(3):151-154.
6. Parma-Benfenati S, Chiesa A, Ritt A, Di Fulvio W. Gingi-voplasty. G Stomatol Ortognatodonzia 1986 Oct-Dec;5(4): 57-58.
7. Tal H, Soldinger M, Dreiangel A, Pitaru S. Periodontal responseto long-term abuse of the gingival attachment by supracrestal amalgam restorations. J Clin Periodontol 1989 Nov;16(10):654-659.
8. Gunay H, Seeger A, Tschernitschek H, Geurtsen W. Placement of preparation line and periodontal health – A prospective 2 year clinical study. Int J Periodontics Restorative Dent 2000 Apr;20(2):173-181.
9. Planciunas L, Puriene A, Mackeviciene G. Surgical length-ening of the clinical tooth crown. Stomatologija 2006;8(3): 88-95.
10. Nugala B, Santosh Kumar BB, Sahitya S, Krishna PM. Biologic width and its importance in periodontal and restorative dentistry. J Conserv Dent 2012 Jan-Mar;15(1):12-17.
11. Jorgic-Srdjak K, Plancak D, Maricevic T, Dragoo MR, Bosnjak A. Periodontal and prosthetic aspect of biological width part I: Violation of biologic width. Acta Stomatol Croat 2000;34:195-197.
12. Khuller N, Sharma N. Biologic width: evaluation and correc-tion of its violation. J Oral Health Community Dent 2009;3: 20-25.
13. Valderhaug J, Birkeland JM. Periodontal conditions in patients 5 years following insertion of fixed prostheses. Pocket depth and loss of attachment. J Oral Rehabil 1976 Jul;3(3):237-243.
14. Newman MG, Takei H, Klokkevold PR. Carranza’s clinical periodontology. 10th ed. Philadelphia: Saunders, Elsevier Publishing; 2006. p. 1050-1069.
15. Galgali SR, Gontiya G. Evaluation of an innovative radio-graphic technique – parallel profile radiography – to deter-mine the dimensions of the dentogingival unit. Indian J Dent Res 2011 Mar-Apr;22(2):237-241.
16. Kois J. Altering gingival levels: the restorative connection, Part 1: Biologic variables. J Esthetic Restorative Dent 1994 Jan;6(1):3-9.
17. Kois JC. The restorative-periodontal interface: Biological parameters. Periodontol 2000 1996 Jun;11:29-38.
18. Freeman K, Bebermeyer R, Moretti A, Koh S. Single-tooth crown lengthening by the restorative dentist: A case report. J Greater Houston Dent Soc 2000;2:14-16.
19. Allen EP. Surgical crown lengthening for function and esthetics. Dent Clin North Am 1993 Apr;37(2):163-180.
20. Jorgic-Srdjak K, Dragoo MR, Bosnjak A, Plancak D, Filipovic I, Lazic D. Periodontal and prosthetic aspect of biological width part II: Reconstruction of anatomy and function. Acta Stomat Croat 2000;34:441-444.
21. Smukler H, Chaibi M. Periodontal and dental considerations in clinical crown extension: a rationale basis for treatment. Int J Periodontics Restorative Dent 1997 Oct;17(5):464-477.
22. Pontoriero R, Carnevale G. Surgical crown lengthening: a 12-month clinical wound healing study. J Periodontol 2001 Jul;72(7):841-848.
23. Elavarasu S, Kermani K, Thangakumaran S, Jeyaprakash GS, Maria R. Apically repositioned flap in reconstruction of muti-lated teeth. JIADS 2010;1:63-66.
24. Heithersay GS. Combined endodontic-orthodontic treatment of transverse root fractures in the region of the alveolar crest. Oral Surg Oral Med Oral Pathol 1973 Sep;36(3):404-415.
25. Felippe LA, Monteiro Junior S, Vierira LC, Araujo E. Reestab-lishing biologic width with forced eruption. Quintessence Int 2003 Nov-Dec;34(10):733-738.