biliary tree infection, liver abscess and hepatitis a
DESCRIPTION
Biliary Tree Infection, Liver Abscess and Hepatitis A. OCTOBER 2005. Acute cholecystitis Cholangitis Liver abscess Hepatitis All cause jaundice. } Viral. Biliary Tree Infection. Bacterial Bacterial/Protozoan. Cholecystitis. Hepatitis / Liver abscess. Cholangitis. Jaundice. - PowerPoint PPT PresentationTRANSCRIPT

Biliary Tree Infection, Liver Biliary Tree Infection, Liver Abscess and Hepatitis AAbscess and Hepatitis A
OCTOBER 2005
Biliary Tree InfectionBiliary Tree Infection
Acute cholecystitis Cholangitis Liver abscess Hepatitis
All cause jaundice
}Viral
Bacterial
Bacterial/Protozoan
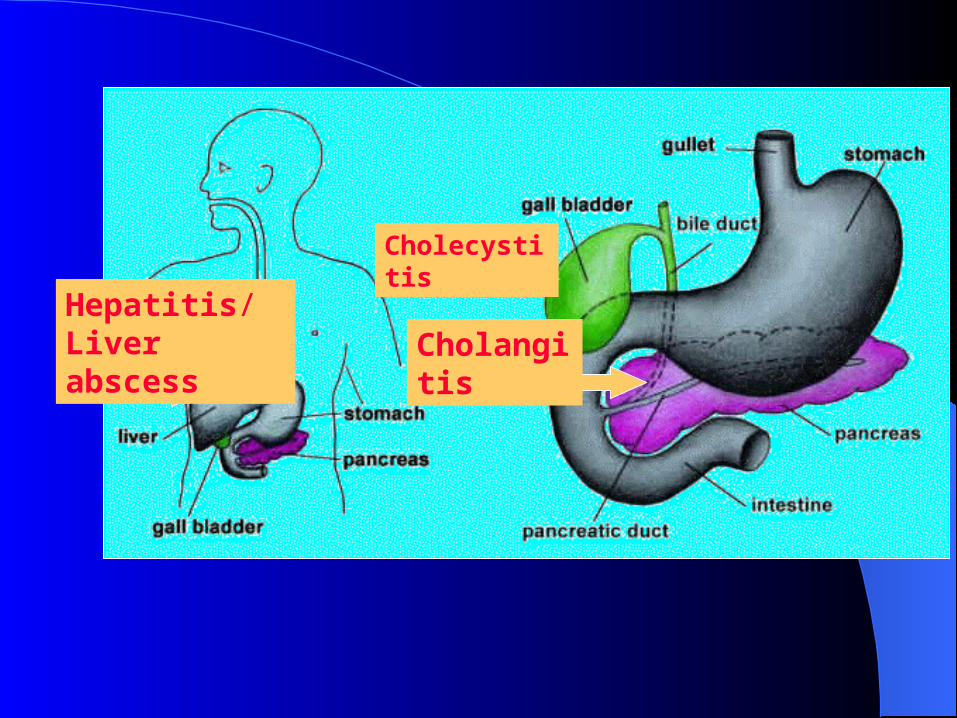
Cholecystitis
Hepatitis/Liver abscess Cholangitis

JaundiceJaundice
= hyperbilirubinaemia due to various causes
Can be due to conjugated or unconjugated bilrubin
Classically presents with yellow eyes, skin, pale stools and dark urine
May have a hepatomegaly, pruritus Can be due to obstructive (tumour,
gallstones) or non obstructive causes (hepatitis, alcoholic hepatitis, haemolysis)


Sclera Sclera

BilirubinBilirubin
Bilrubin is bound to albumin in blood delivered to liver, conjugated to sugar
residues to make it water solublesecreted in bileOnce in gut bilirubin reduced to
urobilinogen (by bacterial flora) urobilinogen is required (indirectly) to give
stools characteristic colour

BilirubinBilirubin
If this process is blocked:
less bilirubin ends up in bile more in blood and therefore more ends up
in urine So stools lose their pigment (pale) and excess bilirubin in blood exits
through urine giving it dark colour

Liver EnzymesLiver Enzymes
Some are a better measure of hepatocellular damage e.g. Alanine aminotransferase (ALT), Aspartate aminotransferase (AST)
This can be due to hepatitis, drugs, alcohol, toxins etc
Others are a better measure of obstruction e.g. Alkaline phosphatase, serum bilirubin
This can be due to cholecystitis, cholangitis, tumours, gall stones
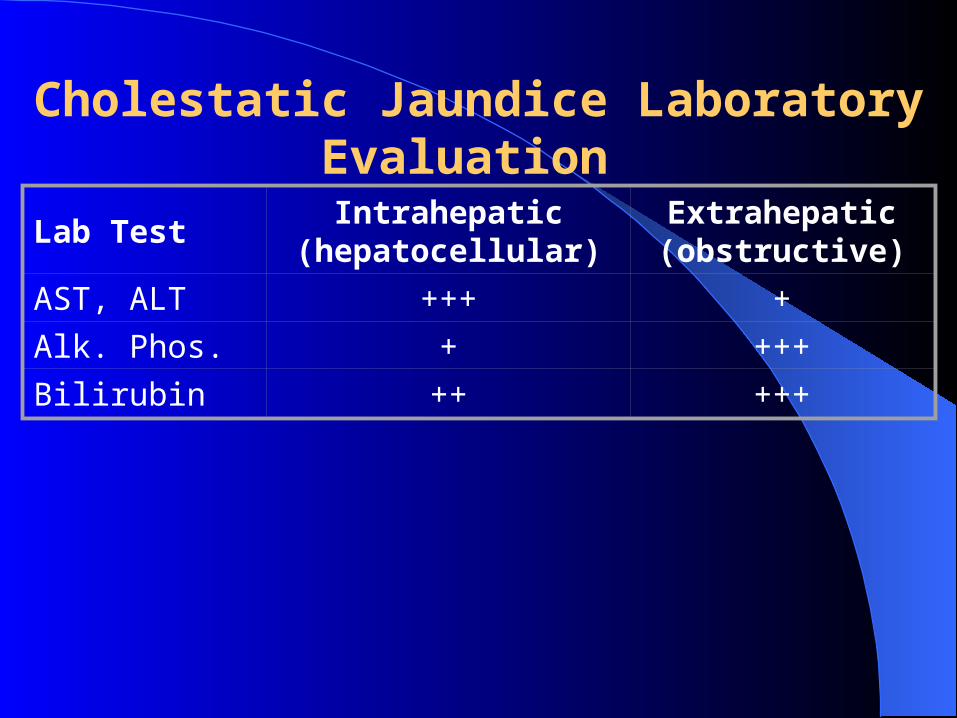
Cholestatic Jaundice Laboratory Evaluation
Lab TestIntrahepatic
(hepatocellular)Extrahepatic(obstructive)
AST, ALT +++ +
Alk. Phos. + +++
Bilirubin ++ +++

Acute CholecystitisAcute Cholecystitis
Acute inflammation of gallbladderAffects 10% of Western populationOf these only 1/5 symptomaticOf these, 1-3% develop cholecystitis,
i.e. ~ 1/2500 of general pop)Does not always involve infection
Acute CholecystitisAcute CholecystitisPathogenesis
Gall stones 90% due to Obstruction of cystic duct e.g. by
stones, biliary sludge, tumour or scarring Necrosis 20% of cases involve infection with normal bowel
flora (E. coli, Klebsiella, Enterococcus spp., Bacteroides spp., Clostridia spp.)
In developing countries, ascariasis worm major cause

ClassificationClassificationOEDEMAOEDEMA plus CONGESTIONFOCAL NECROSIS
SUPPURATION
GANGRENE
PERFORATION
INTRAMURAL
INTRALUMINAL
PERI-CHOLECYSTIC
LOCALISED
FREE

Gall StonesGall Stones
Gall stones can consist of bile salt, cholesterol or be mixed

Prostaglandins mediate inflammatory response, vicious circle

Acute CholecystitisAcute Cholecystitis
Clinical Features
Nausea, vomiting, fever Constant pain in right upper quadrant of abdomen Murphy’s sign (pain preventing full inspiration during
subhepatic palpation) +/- jaundice +/- palpable gall bladder Temperature Said to occur classically in women who are “fair, fat and forty
with four children” but can occur in anybody If infection occurs, may have signs of septicaemia (worse
prognosis) or peritonitis if perforation occurs

Acute CholecystitisAcute Cholecystitis
Diagnosis Based on Clinical Features and
Investigations
Radiological findings US, PFA,
Lab findings, increased WCC, ESR, CRP

Acute CholecystitisAcute Cholecystitis

Radiological Investigations
Ultrasound scan – can reveal stones, oedema of gall bladder wall, fluid around gall bladder
Plain film of abdomen (X-ray) shows stones in 10%, may show air level in emphesymatous cholecystitis
If US unclear, Scintigraphy used. Inject radiolabelled HIDA which is secreted in bile. Failure of appearance in gallbladder within 1-2 hours is a sign of blockage
CT may also be useful
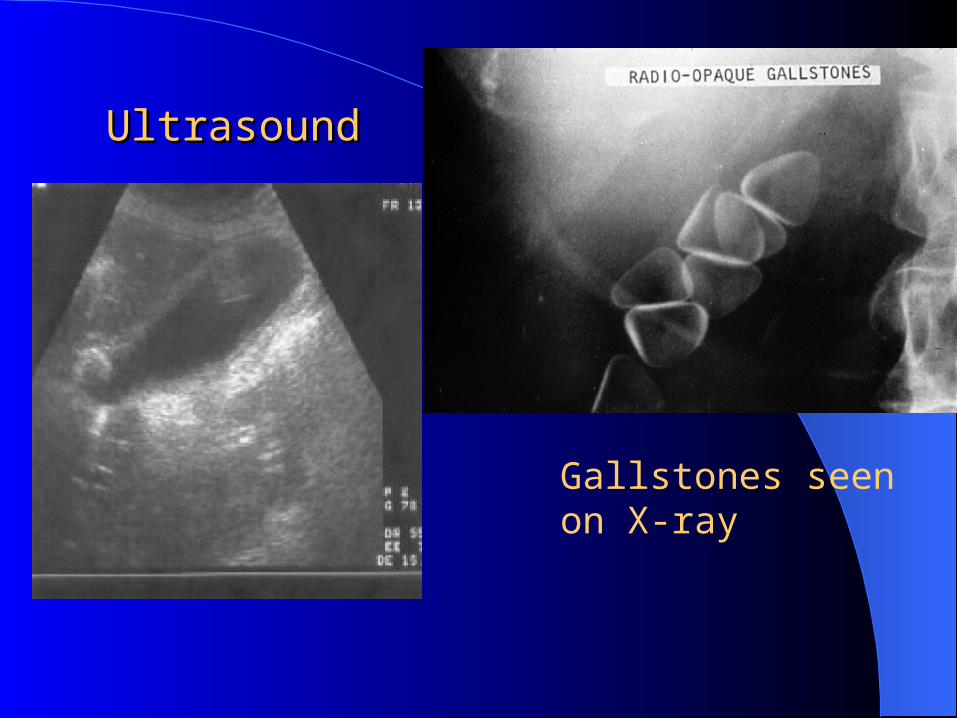
UltrasoundUltrasound
Gallstones seen on X-ray

PFA findings in Emphysematous Cholecystitis

Organsims InvolvedOrgansims Involved
Usually mixed, derived from bowel floraEnterobacteriaceae 68%Enterococci 14%Bacteroides spp. 10%Clostridium sp. 7%

Acute CholecystitisAcute Cholecystitis
Complications
Perforation, necrosis gangrene, suppuration
Abscess formation Septicaemia Peritonitis
Acute CholecystitisAcute Cholecystitis
Treatment Most respond to conservative management, gallstones
falls back into gall bladder, cystic duct empties and symptoms resolve
Rest gall bladder – no food, IV fluids, pain relief as required
Indomethacin to reduce prostaglandin effects If systemic signs or no improvement after 12-24 hours
give Antibiotics, usually:– Co-Amoxiclav or Ampicillin, Ciprofloxacin or
Gentamicin , and Metronidazole– Piperacillin/Tazobactam (Tazocin)

Acute CholecystitisAcute Cholecystitis
Treatment About 20% require emergency surgery These are patients with deterioration in
condition,perforation with peritonitis, suspected pericholecystic abscess or emphysematous cholecystitis
Many others will require surgery but timing of surgery is a matter of debate
Cholecystectomy = removal of gallbladder, can be done as an open or laparoscopic procedure

CholangitisCholangitis
continuous, varying degrees of inflammation and /or infection involving hepatic and common bile duct (mucosa continuous) More severe entities are ascending cholangitis and acute obstructive suppurative cholangitis.
Pathogenesis Essentially obstruction of the common bile duct
due to stones, parasites, surgery, leading to increased pressure, oedema, congestion, necrosis and proliferation of bacteria.
Definition

Ascending CholangitisAscending Cholangitis
Signs and Symptoms Previous history of gall bladder disease, acute onset of Charcot's triad
– RUQ pain, – fever & rigors– Jaundice
Treatment Antibiotics e.g.Co-Amoxiclav or Ampicillin ,+Ciprofloxacin
or Gentamicin ,+ metronidazole or Piperacillin-tazobactam+/-Ciprofloxacin
Decompression by endoscopy(ERCP), radiological stenting or surgical drainage
Delay in treatment can result in septicaemia, liver abscess

Liver AbscessLiver Abscess
Liver is a very vascular organ, receiving blood from systemic and portal circulation
Bile drainage also provides route of bacterial entry especially when obstruction occurs
Usually Kuppfer cells lining hepatic sinusoids clear bacteria to prevent infection

Liver AbscessLiver Abscess
Source FrequencyBiliary tract disease 60%
Portal venous system from GIT 24%
Arterial seeding from systemic bacteremia
15%
Contiguous spread e.g. from gall bladder
4%
Other causes include trauma and secondary infection also
crytogenic
Liver abscess can be pyogenic or amoebic

Liver AbscessLiver Abscess
Untreated pyogenic liver abscess is uniformly fatal
Appropriate antibiotic Tx and drainage reduces mortality to 5-30%
Abscess can be single or multiple( due to biliary disease)Right lobe being bigger is more
commonly involved

Liver AbscessLiver Abscess
Clinical Features Fever, chills for several days or weeks Spiking temperatures with ascending
cholangitis Malaise Anorexia Weight loss +/- referred pain to right shoulder

Liver AbscessLiver Abscess
Clinical Findingshepatomegaly+/- tendernessReduced breath sounds on right hand
sideHepatic friction rubJaundice in 25%

Most Common Causative Organisms
Usually mixed aerobes and anaerobes, type often corresponds to source:
Gram negative bacilli from GIT e.g E.coli, Klebiella sppStreptococcus milleri from GITBacteroides, Fusobacterium and other anaerobes from GITS. aureus from haematogenous spread Entamoeba histolyticaFungal abscesses e.g. C. albicans in patients with prolonged
antibiotic exposure, transplants, immunocompromised patients

Liver AbscessLiver Abscess
InvestigationsFBC: anaemia, raised WBCsRaised CRP and ESRRaised liver enzymes esp Alk PhosBlood culturesCulture abscess fluidRadiology: CT or ultrasound

Liver AbscessLiver Abscess
TreatmentPercutaneous drainage of abscess
under CT or US guidanceIf this fails – surgical drainageException is Entamoeba histolytica
which responds to metronidazole without surgery
CT/US to monitor Tx

Liver AbscessLiver Abscess
Antibiotic Treatment depends on culture results: Ampicillin+Gentamicin + metronidazole or
Piperacillin-tazobactam Clindamycin, Flucloxacillin for sensitive
Staphylococci Amphotericin B for fungi Entamoeba histolytica – metronidazole Usually for 1-4 months

Causes of HepatitisCauses of HepatitisInfectious Bacterial
Leptospirosis
Syphillis
Tuberculosis
Parasitic
Toxoplasmosis
Amoebiasis
Viral
Hepatitis Viruses A, B,C, D, E, G
Epstein Barr
Cytomegalovirus
Herpes Simplex
Varicella Zoster
Coxsackievirus
Rubella
Yellow Fever
Noninfectious
Alcohol
Drugs

Hepatitis VirusesHepatitis Viruses
Types A to GNo relation to each other, simply
infect same organViral hepatitis can also be caused by
other viruses e.g. EBV, CMV and HSV
Hepatitis AHepatitis A
Hepatitis A - HistoryHepatitis A - History
“Catarrhal jaundice” recognised in ancient China, Greece and Rome Hippocrates
Epidemic in Minorca in 1745
McDonald first to suggest viral cause in 1907

Viral Hepatitis - HistoryViral Hepatitis - History
Deliberate transmission to human volunteers in Germany in 1942
Jaundice committee 1943, One(serum) has incubation period 60-160 Hep B and another feacal oral route , I.P shorter Hep A identified
Mid 1970`s- new serological test for Hepatitis B did not explain all cases-nonA-nonB now Hepatitis C (1989) but sporadic and community acquired Hep E also described
Rizzetto 1977 described Hep D while working on Hep B
Other causes of jaundice complicated early understanding and were separated into “infectious hepatitis” and “serum hepatitis”

Hepatitis A - ClassificationHepatitis A - Classification
Picornaviridae of which there are 3 genera: – Rhinovirus (Rhinoviruses)– Enteroviruses (Polio, coxsackie, echo and
enteroviruses)– Hepatavirus (Hepatitis A)
RNA virus, ss + RNA (7.5 kb) Only one serotype Non-enveloped 27-28 nm icosahedral structure

Hepatitis A Virus (HAV)Hepatitis A Virus (HAV)
First isolated in 1979Natural host: humanStable: heat and acid-resistantInactivated by high temperature,
formalin, chlorine

Hepatitis A – Life CycleHepatitis A – Life Cycle
Infected material ingestedAbsorbed through stomach or small
intestineReplicates in liverSecreted into bileExcreted into stool or reabsorbedSpread: Faecal-oral route

HAV Life CycleHAV Life Cycle

Hepatitis AHepatitis A
Robust virus:stable after incubation at 56oCLasts for years at –20oCIn dried form at room temperature
can last for several weeksKilled by boiling for 5 minutes

Hepatitis AHepatitis A
Therefore steaming shellfish probably insufficient
Survives for days/months in live oysters, waste water, soil
Stable at pH 3Resistant to diethyl ether, chloroform
and 50% trichlorotrifluorethane

Hepatitis AHepatitis A i.e. tough organism which, because of its ability to
survive, is easily transmitted
Therefore meticulous care is needed when handling clinical specimens
Destroyed by: – Boiling– Autoclaving– Chlorine– Iodine– Radiation– formaldehyde

HAV EpidemiologyHAV Epidemiology
Man is natural host Worldwide distribution Late Autumn , early Winter Virus spread in feces Virus contaminates
– Water: drinking, bathing; washing food– Food: shellfish and other filter feeders – Hands: personal hygiene; contaminated water

Hepatitis A - EpidemiologyHepatitis A - Epidemiology CDC 10,600 cases in USA/2001, 22% hospitalised, ~
100 deaths/yr
Over last 40 years average age of infection increasing due to improved sanitation, detection and prevention
Approx 10% of children and 40% of adults will have IgG
Highest rate of seropositivity in Africa, Asia and South America
But epidemiology is changing with improved hygiene and increasing travel

Hepatitis A - EpidemiologyHepatitis A - Epidemiology
High risk groups include:– Contacts of recently infected individuals– Foreign travellers (esp visitors to Third world)– Military personnel– Male homo/bisexuals– IV drug abusers– Those living in poverty or in institutions– Childcare and sewage workers– Recognised Foodborne or water outbreaks

Unknown 44.5% Personal
contact 24%
Day Care 15.1%
Injecting drug use 2.4%
International travel 5.5%
Homosexual men 3.8%
Outbreaks 4.7%
Prevalence of Risk Factors in Patients with HAV

Hepatitis A - EpidemiologyHepatitis A - Epidemiology
Mortality about 2% in elderly, about 0.02% in normal population
Also higher in those with coincidental liver disease
Hepatitis A in Ireland: 112 cases in 2001NO chronic carrier state

Hepatitis A IrelandHepatitis A Ireland


Hepatitis A - TransmissionHepatitis A - Transmission
Faecal-oral spread, shed in faeces 2-3 weeks before jaundice and 1 week after
Close person-to-person contact poor hygiene, foodborne or waterborne
outbreaks e.g. faecal contamination of food such as Oysters or by food handler
Via shared needles/blood transfusions (rare)
How is HAV different from How is HAV different from foodborne bacteria?foodborne bacteria?
Does not replicate in infected food
Virus remains stable for long periods of time in a wide range of conditions, e.g. in one outbreak, the virus survived for > 1 year in frozen fruit

HAV PathogenesisHAV Pathogenesis Incubation period 15-50 days weeks, depends on
infective dose Replication: liver (hepatocytes and Kuppfer’s cells);
peak viraemia 10-12 days after infection (appearance of HAV in serum and feces)
Virus released into bile and stool Virus does not induce cytopathic effects Damage to liver is immune mediated, thought to be
via cell-mediated immune response Histology is similar to hepatitis B virus infection, portal
inflammation but less focal necrosis

Hepatitis A - Clinical FeaturesHepatitis A - Clinical Features
In Western world tends to be symptomatic In Third world, often asymptomatic and subclinical Majority of infected children are
asymptomatic(70%), majority of adults have symptoms(70% jaundice)
symptoms and severity of illness increase with age
Flu-like illness Jaundice, hepatomegaly, splenomegaly Usually uneventful recovery

Symptoms of patients with Hepatitis A
Symptom Reported Ranges (%)
Jaundice (Yellow Eyes) 40-80
Dark urine 68-94
Fatigue/Lassitude 52-91
Loss of appetite 42-90
Abdominal pain/discomfort 37-65
Light-coloured stools 52-58
Nausea or vomiting 26-87
Fever or chilliness 32-73
Headache 26-73
Arthralgias 11-40
Myalgia 15-52

Clinical Course of HAV InfectionClinical Course of HAV Infection Incubation phase: 15-50 days, i.e. can infect others
before symptoms develop
Preicteric phase– Abrupt appearance– Fever, fatigue, nausea, loss of appetite, abdominal pain
leading to Icteric phase (jaundice)
Icteric phase – Symptoms lessen– Jaundice, dark urine
Convalescent phase– Complete recovery 99% of cases

Clinical Diagnosis of HAVClinical Diagnosis of HAV
Discrete onset of symptoms
History
Jaundice

Lab Findings in HAV InfectionLab Findings in HAV Infection
Elevated serum aminotransferase levels (ALT and AST elevated)
Alkaline Phosphatase only mildly elevated (elevation is a sign of cholestasis)
Mild lymphocytosisIncrease in prothrombin time bad signSpecific Ig tests for Diagnosis by ELISA

Hepatitis A - DiagnosisHepatitis A - Diagnosis
Anti HAV IgM appears just before jaundice and remains elevated for 4/12 up to 6 months(ELISA)
IgG levels used to determine immune status
Virus culture for diagnosis not an option as it is slow, difficult and expensive
Positive RT-PCR and/or antigen test

Complications of HAVComplications of HAV
Fulminant Hepatitis– 1-3/1000 cases; 80% mortality– Extensive necrosis of the liver– Includes hepatic encephalopathy
Relapsing hepatitis ~ 12%– 4-15 weeks after initial symptoms– Biochemical changes only in some patients
Cholestatic hepatitis– Total blockage/suppression of bile – High bilirubin levels

Complications of HAVComplications of HAV
NO CHRONIC INFECTION
NO CARRIER STATE
VERTICAL TRANSMISSION RARE

Hepatitis A – TreatmentHepatitis A – Treatment
Symptomatic Tx (e.g. rehydration, antiemetics)
Immune serum globulin– Given before or early in incubation phase
(effective within 2 weeks of exposure)
Contact tracing Those with fulminant hepatitis and hepatic
failure occasionally require transplant

Hepatitis A – PreventionHepatitis A – Prevention
Adequate sanitation, disrupt Faecal-oral spread
Good hygieneEffective (inactivated) vaccine availableImmunoglobulins also available for
passive protection

HAV VaccineHAV Vaccine No adverse reactions but not used in those < 2 yrs of
age Recommended for:
– international travelers to endemic areas (effective 4 weeks after administration)
– Homo/bisexual men– I.v. drug users– Persons with coagulopathies, chronic liver disease (including
hepatitis C)– Those who regularly receive blood products– Persons at occupational risk (sewage workers, those in mental
institutions , consider in certain Health care workers groups)– Contacts of known cases

HAV ImmunityHAV ImmunityInfected > Vaccinated > passive IgG Tx
Infection provides lifelong immunity
Vaccination thought to be largely sufficient and should provide immunity for at least 10 years, probably longer(2 doses, o and 6-12 months later) e.g Havrix and Vapta
Passive Immunization with IgG provides protection for about 5 months and straight away

HAV SummaryHAV Summary