bilateral stress fracture of the clavicle
TRANSCRIPT
Skeletal Radiol (1995) 24:613-616 Skeletal Radiology
Bilateral stress fracture of the clavicle
Emilio Calvo, M.D., Darlo Fermindez-Yruegas, M.D., Luis Alvarez, M.D., Jos~ C. de Lucas, M.D., Carlos Vallejo, M.D.
Department of Orthopaedic Surgery and Traumatology, Fundacidn Jim~nez Dfaz, Universidad Aut6noma, Madrid, Spain
Case report
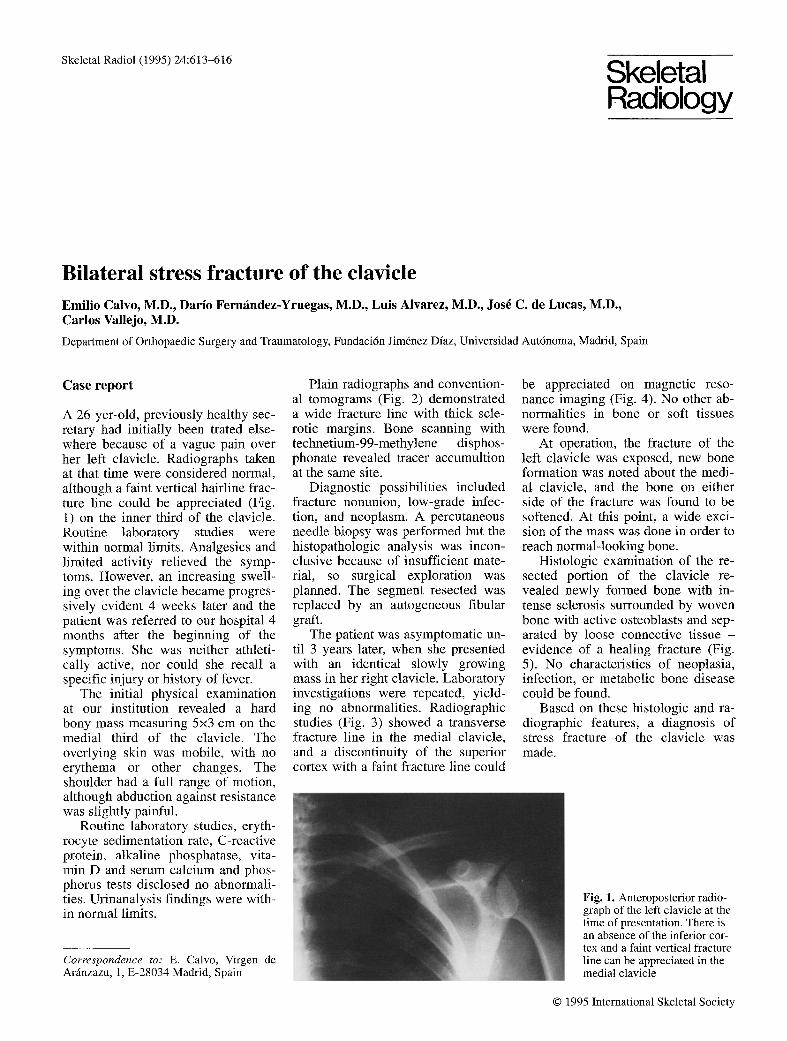
A 26-yer-old, previously healthy sec- retary had initially been trated else- where because of a vague pain over her left clavicle. Radiographs taken at that time were considered normal, although a faint vertical hairline frac- ture line could be appreciated (Fig. 1) on the inner third of the clavicle. Routine laboratory studies were within normal limits. Analgesics and limited activity relieved the symp- toms. However, an increasing swell- ing over the clavicle became progres- sively evident 4 weeks later and the patient was referred to our hospital 4 months after the beginning of the symptoms. She was neither athleti- cally active, nor could she recall a specific injury or history of fever,
The initial physical examination at our institution revealed a hard bony mass measuring 5x3 cm on the medial third of the clavicle. The overlying skin was mobile, with no erythema or other changes. The shoulder had a full range of motion, although abduction against resistance was slightly painful.
Routine laboratory studies, eryth- rocyte sedimentation rate, C-reactive protein, alkaline phosphatase, vita- min D and serum calcium and phos- phorus tests disclosed no abnormali- ties. Urinanalysis findings were with- in normal limits.
Correspondence to: E. Calvo, Virgen de Ar~nzazu, 1, E-28034 Madrid, Spain
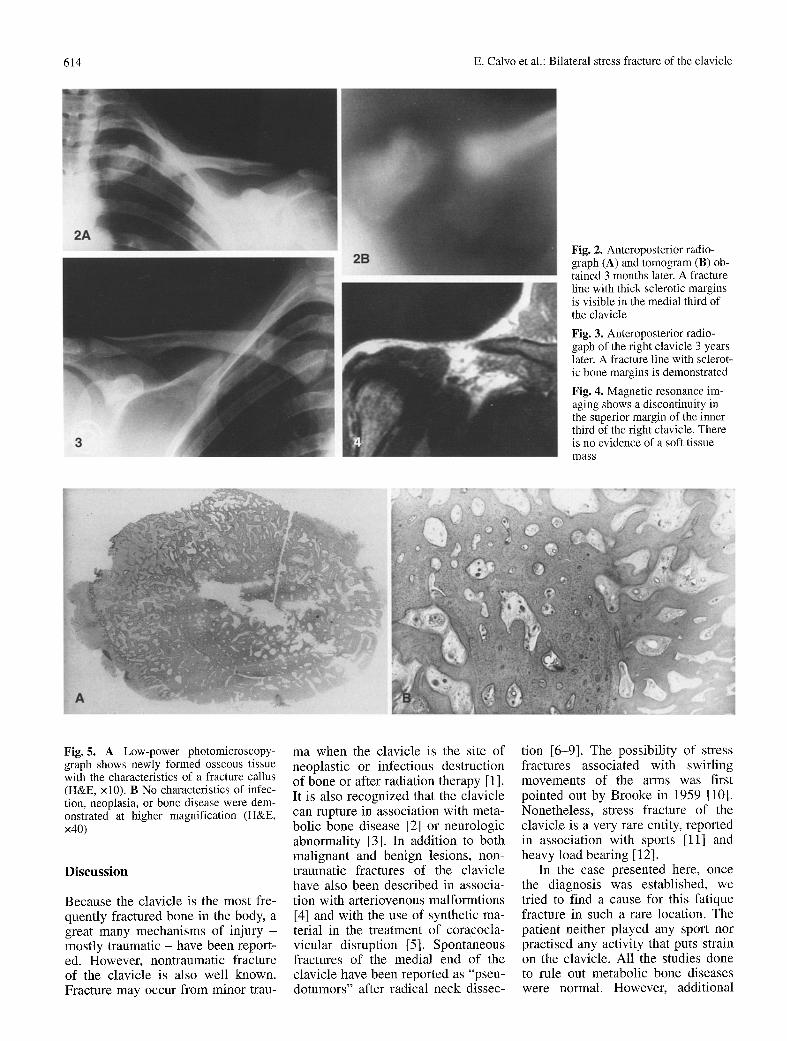
Plain radiographs and convention- al tomograms (Fig. 2) demonstrated a wide fracture line with thick scle- rotic margins. Bone scanning with technetium-99-methylene disphos- phonate revealed tracer accumultion at the same site.
Diagnostic possibilities included fracture nonunion, low-grade infec- tion, and neoplasm. A percutaneous needle biopsy was performed but the histopathologic analysis was incon- clusive because of insufficient mate- rial, so surgical exploration was planned. The segment resected was replaced by an autogeneous fibular graft.
The patient was asymptomatic un- til 3 years later, when she presented with an identical slowly growing mass in her right clavicle. Laboratory investigations were repeated, yield- ing no abnormalities. Radiographic studies (Fig. 3) showed a transverse fracture line in the medial clavicle, and a discontinuity of the superior cortex with a faint fracture line could
be appreciated on magnetic reso- nance imaging (Fig. 4). No other ab- normalities in bone or soft tissues were found.
At operation, the fracture of the left clavicle was exposed, new bone formation was noted about the medi- al clavicle, and the bone on either side of the fracture was found to be softened. At this point, a wide exci- sion of the mass was done in order to reach normal-looking bone,
Histologic examination of the re- sected portion of the clavicle re- vealed newly formed bone with in- tense sclerosis surrounded by woven bone with active osteoblasts and sep- arated by loose connective tissue - evidence of a healing fracture (Fig. 5). No characteristics of neoplasia, infection, or metabolic bone disease could be found.
Based on these histologic and ra- diographic features, a diagnosis of stress fracture of the clavicle was made.
Fig. 1. Anteroposterior radio- graph of the left clavicle at the time of presentation. There is an absence of the inferior cor- tex and a faint vertical fracture line can be appreciated in the medial clavicle
�9 1995 International Skeletal Society
614 E. Calvo et al.: Bilateral stress fracture of the clavicle
Fig. 2. Anteroposterior radio- graph (A) and tomogram (B) ob- tained 3 months later. A fracture line with thick sclerotic margins is visible in the medial third of the clavicle
Fig. 3. Anteroposterior radio- gaph of the right clavicle 3 years later. A fracture line with sclerot- ic bone margins is demonstrated
Fig. 4. Magnetic resonance im- aging shows a discontinuity in the superior margin of the inner third of the right clavicle. There is no evidence of a soft tissue mass
Fig. 5. A Low-power photomicroscopy- graph shows newly formed osseous tissue with the characteristics of a fracture callus (H&E, xl0). B No characteristics of infec- tion, neoplasia, or bone disease were dem- onstrated at higher magnification (H&E, x40)
Discuss ion
Because the clavicle is the most fre- quently fractured bone in the body, a great many mechanisms of injury - mostly traumatic - have been report- ed. However, nontraumatic fracture of the clavicle is also well known. Fracture may occur from minor trau-
ma when the clavicle is the site of neoplastic or infectious destruction of bone or after radiation therapy [1]. It is also recognized that the clavicle can rupture in association with meta- bolic bone disease [2] or neurologic abnormality [3]. In addition to both malignant and benign lesions, non- traumatic fractures of the clavicle have also been described in associa- tion with arteriovenous malformtions [4] and with the use of synthetic ma- terial in the treatment of coracocla- vicular disruption [5]. Spontaneous fractures of the medial end of the clavicle have been reported as "pseu- dotumors" after radical neck dissec-
tion [6-9]. The possibility of stress fractures associated with swirling movements of the arms was first pointed out by Brooke in 1959 [10]. Nonetheless, stress fracture of the clavicle is a very rare entity, reported in association with sports [11] and heavy load bearing [12].
In the case presented here, once the diagnosis was established, we tried to find a cause for this fatique fracture in such a rare location. The patient neither played any sport nor practised any activity that puts strain on the clavicle. All the studies done to rule out metabolic bone diseases were normal. However, additional
E. Calvo et al.: Bilateral stress fracture of the clavicle 615
A
c X y
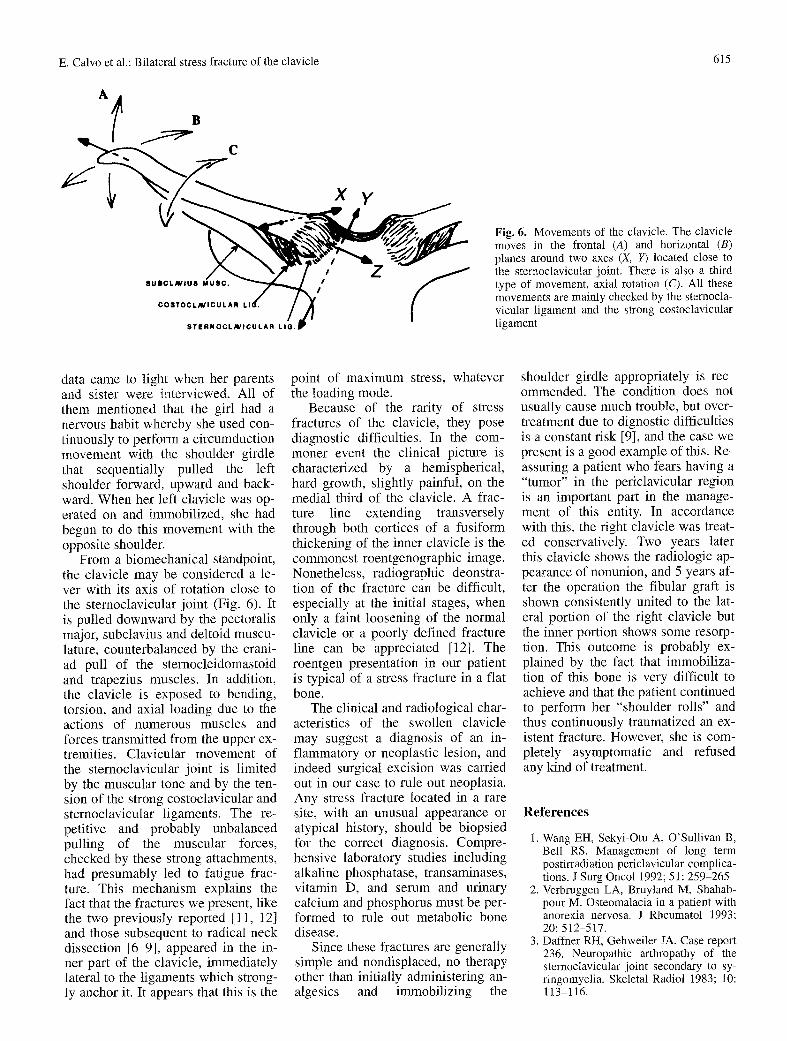
Fig. 6. Movements of the clavicle. The clavicle moves in the frontal (A) and horizontal (B) planes around two axes (X, I7) located close to the sternoclavicular joint. There is also a third type of movement, axial rotation (C). All these movements are mainly checked by the sternocla- vicular ligament and the strong costoclavicular ligament
data came to light when her parents and sister were interviewed. All of them mentioned that the girl had a nervous habit whereby she used con- tinuously to perform a circumduction movement with the shoulder girdle that sequentially pulled the left shoulder forward, upward and back- ward. When her left clavicle was op- erated on and immobilized, she had begun to do this movement with the opposite shoulder.
From a biomechanical standpoint, the clavicle may be considered a le- ver with its axis of rotation close to the sternoclavicular joint (Fig. 6). It is pulled downward by the pectoralis major, subclavius and deltoid muscu- lature, counterbalanced by the crani- ad pull of the sternocleidomastoid and trapezius muscles. In addition, the clavicle is exposed to bending, torsion, and axial loading due to the actions of numerous muscles and forces transmitted from the upper ex- tremities. Clavicular movement of the sternoclavicular joint is limited by the muscular tone and by the ten- sion of the strong costoclavicular and sternoclavicular ligaments. The re- petitive and probably unbalanced pulling of the muscular forces, checked by these strong attachments, had presumably led to fatigue frac- ture. This mechanism explains the fact that the fractures we present, like the two previously reported [11, 12] and those subsequent to radical neck dissection [6-9], appeared in the in- ner part of the clavicle, immediately lateral to the ligaments which strong- ly anchor it. It appears that this is the
point of maximum stress, whatever the loading mode.
Because of the rarity of stress fractures of the clavicle, they pose diagnostic difficulties. In the com- moner event the clinical picture is characterized by a hemispherical, hard growth, slightly painful, on the medial third of the clavicle. A frac- ture line extending transversely through both cortices of a fusiform thickening of the inner clavicle is the commonest roentgenographic image. Nonetheless, radiographic deonstra- tion of the fracture can be difficult, especially at the initial stages, when only a faint loosening of the normal clavicle or a poorly defined fracture line can be appreciated [12]. The roentgen presentation in our patient is typical of a stress fracture in a fiat bone.
The clinical and radiological char- acteristics of the swollen clavicle may suggest a diagnosis of an in- flammatory or neoplastic lesion, and indeed surgical excision was carried out in our case to rule out neoplasia. Any stress fracture located in a rare site, with an unusual appearance or atypical history, should be biopsied for the correct diagnosis. Compre- hensive laboratory studies including alkaline phosphatase, transaminases, vitamin D, and serum and urinary calcium and phosphorus must be per- formed to rule out metabolic bone disease.
Since these fractures are generally simple and nondisplaced, no therapy other than initially administering an- algesics and immobilizing the
shoulder girdle appropriately is rec- ommended. The condition does not usually cause much trouble, but over- treatment due to dignostic difficulties is a constant risk [9], and the case we present is a good example of this. Re- assuring a patient who fears having a "tumor" in the periclavicular region is an important part in the manage- ment of this entity. In accordance with this, the right clavicle was treat- ed conservatively. Two years later this clavicle shows the radiologic ap- pearance of nonunion, and 5 years af- ter the operation the fibular graft is shown consistently united to the lat- eral portion of the right clavicle but the inner portion shows some resorp- tion. This outcome is probably ex- plained by the fact that immobiliza- tion of this bone is very difficult to achieve and that the patient continued to perform her "shoulder rolls" and thus continuously traumatized an ex- istent fracture. However, she is com- pletely asymptomatic and refused any kind of treatment.
References
1. Wang EH, Sekyi-Otu A, O'Sullivan B, Bell RS. Management of long term postirradiation periclavicular complica- tions. J Surg Oncol 1992; 51:259-265
2. Verbrnggen LA, Bruyland M, Shahab- pour M. Osteomalacia in a patient with anorexia nervosa. J Rheumatol 1993; 20: 512-517.
3. Daffner RH, Gehweiler JA. Case report 236. Neuropathic arthropathy of the sternoclavicular joint secondary to sy- ringomyelia. Skeletal Radiol 1983; 10: 113-116.

616 E. Calvo et al.: Bilateral stress fracture of the clavicle
4. Mnaymneh W, Vargas A, Kaplan J. Pathologic fracture of the clavicle caused by arteriovenous malformation. Clin Orthop 1980; 148: 256-258.
5. Dust WN, Lenczer AM. Stress fracture of the clavicle leading to nonunion sec- ondary to coracoclavicular reconstruc- tion with Dacron. Am J Sports Med 1989; 17: 128-129.
6. Cummings CW, First R. Stress fracture of the clacivle after radical neck dissec- tion. Case report. Plast Reconstr Surg 1975; 55: 366-367.
7. Fini-Storchi O, LoRusso D, Agostini V.
"Pseudotumors" of the clavicle subse- quent to radical neck dissection. J Lar- yngol Otol 1985; 99: 73-83.
8. Ord RA, Langdon JD. Stress fracture of the clavicle: a rare late complication of radical neck dissection. J Maxillofac Surg 1985; 14: 281-284.
9. Strauss M, Bushey M J, Chung C, Baum S. Fractures of the clavicle fol- lowing radical neck dissection or post- operative radiotherapy: a case report and review of the literature. Laryngo- scope 1982; 92: 1304-1307.
10. Brooke R. Jive fracture of the first rib. J
11.
12.
Bone Joint Surg B 1959; 41 B: 370- 371. Paul RP, Ahonen A, Virtama P, Aho A, Ekfors T. F-18 Fluorodeoxyglucose: its potential differentiating between stress fracture and neoplasia. Clin Nucl Med 1989; 14: 906-908. Kaye JJ, Nance EP, Green NE. Fatigue fracture of the medial aspect of the clavicle: an academic rather than athlet- ic injury. Radiology 1982; 144: 89- 90.