bevel toric multicurve rigid gas-permeable lens for keratoconus
TRANSCRIPT

CLINICAL INVESTIGATION
Bevel toric multicurve rigid gas-permeable lens for keratoconus
Ryoji Yanai • Kiichi Ueda • Koh-Hei Sonoda
Received: 9 January 2012 / Accepted: 17 October 2012 / Published online: 7 December 2012
� Japanese Ophthalmological Society 2012
Abstract
Purpose To evaluate the efficacy and safety of Twinbel
bevel toric, a newly designed rigid gas-permeable (RGP)
lens with a toric bevel curvature, for keratoconus.
Methods A retrospective analysis of nine eyes of patients
with keratoconus who had been wearing RGP contact
lenses and were switched to Twinbel bevel toric at Yam-
aguchi University Hospital. Visual acuity and contrast
sensitivity were measured under photopic conditions.
Complaint symptoms were recorded as primary outcome
measures at follow-up visits. Efficacy and safety were
evaluated at 12 weeks after the switch to Twinbel bevel
toric or later.
Results Five eyes (55.6 %) showed an improvement in
visual acuity with Twinbel bevel toric compared with the
previous lens, whereas four eyes (44.4 %) maintained the
same visual acuity as before. The mean best corrected
visual acuity ± SD with Twinbel bevel toric was
0.01 ± 0.40 logMAR, significantly better (P = 0.044,
paired Student’s t test) than that (0.23 ± 0.51 logMAR)
with the previous lens. Contrast sensitivity and subjective
complaint scores did not differ significantly between
Twinbel bevel toric and the previous lens. No serious
complications of Twinbel bevel toric wear were observed.
Conclusions Fitting of Twinbel bevel toric improved
visual acuity in eyes affected by keratoconus, thus pro-
viding a viable alternative for management of such eyes.
Keywords Keratoconus multicurve design � Bevel toric
contact lens � Special lens � Rigid gas-permeable lens
Introduction
Keratoconus is a progressive noninflammatory disease of
the cornea characterized by thinning, ectasia, distortion and
increased curvature of the cornea [1–4]. The abnormal
curvature affects the refractive power of the cornea,
resulting in myopia or irregular astigmatism [5, 6]. Indi-
viduals with keratoconus in the advanced stage require a
rigid gas-permeable (RGP) contact lens to reduce distortion
and provide better vision [7–9]. Fitting of an RGP lens
improves visual acuity, and many such lenses have been
developed for management of keratoconus patients [8–19].
However, RGP lenses can cause discomfort as a result of
their small bevel width, which is necessitated by the dif-
ference in radius of curvature of the cornea between the
vertical and horizontal directions in advanced keratoconus
[20]. The small bevel results in reduced tear exchange and
induces corneal epithelial disorders and visual disturbance.
Although keratoplasty is the best treatment option for
patients with severe keratoconus, various postoperative
complications, including graft rejection or failure, astig-
matism, recurrence of keratoconus in the donor graft, and
development of cataracts, glaucoma, or acute hydrops, are
described [19, 21].
The Twinbel II contact lens (Sun Contact Lens Co., Ltd.,
Kyoto, Japan) has a multicurve design that incorporates a
flat base curve, steep first intermediate curve and flat sec-
ond intermediate curve. The designs of both the base curve
and the second intermediate curve contribute to the sta-
bility of lens centering. We previously showed that
Twinbel II is effective in improving visual acuity in eyes
R. Yanai (&) � K. Ueda � K.-H. Sonoda
Department of Ophthalmology, Yamaguchi University Graduate
School of Medicine, 1-1-1 Minami-Kogushi, Ube,
Yamaguchi 755-8505, Japan
e-mail: [email protected]
123
Jpn J Ophthalmol (2013) 57:199–205
DOI 10.1007/s10384-012-0216-6
with irregular astigmatism after penetrating keratoplasty
[22]. The Twinbel bevel toric lens (Sun Contact Lens) was
developed taking into account the unequal bevel width of
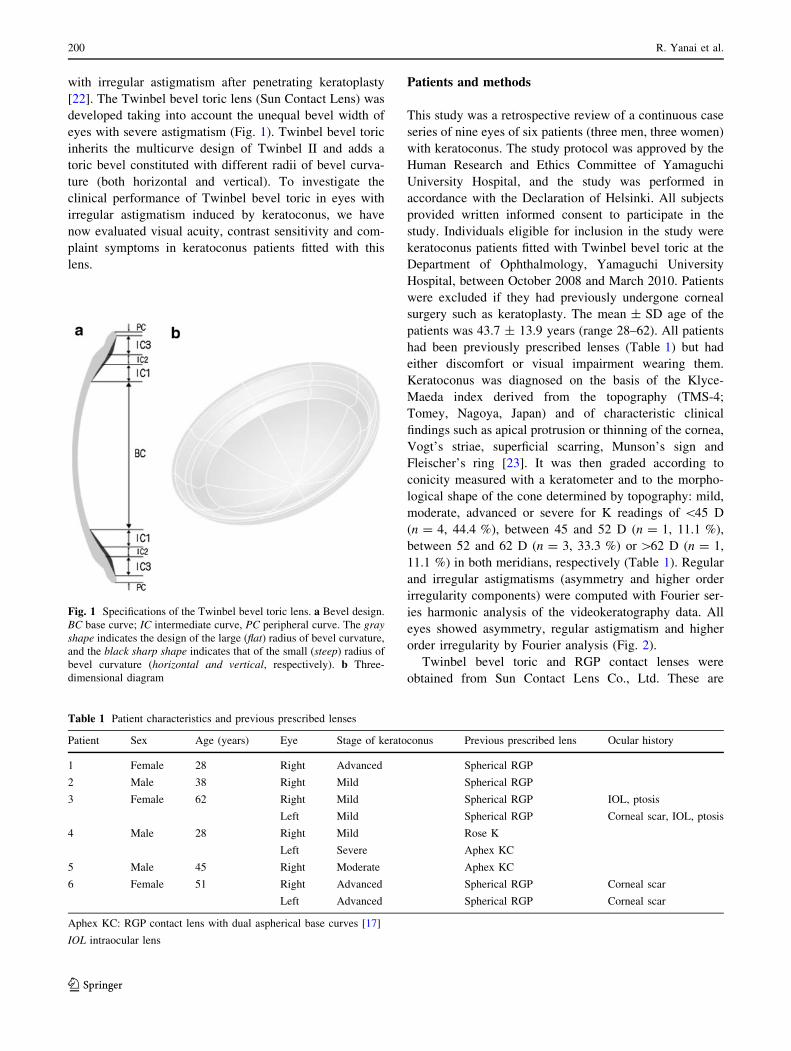
eyes with severe astigmatism (Fig. 1). Twinbel bevel toric
inherits the multicurve design of Twinbel II and adds a
toric bevel constituted with different radii of bevel curva-
ture (both horizontal and vertical). To investigate the
clinical performance of Twinbel bevel toric in eyes with
irregular astigmatism induced by keratoconus, we have
now evaluated visual acuity, contrast sensitivity and com-
plaint symptoms in keratoconus patients fitted with this
lens.
Patients and methods
This study was a retrospective review of a continuous case
series of nine eyes of six patients (three men, three women)
with keratoconus. The study protocol was approved by the
Human Research and Ethics Committee of Yamaguchi
University Hospital, and the study was performed in
accordance with the Declaration of Helsinki. All subjects
provided written informed consent to participate in the
study. Individuals eligible for inclusion in the study were
keratoconus patients fitted with Twinbel bevel toric at the
Department of Ophthalmology, Yamaguchi University
Hospital, between October 2008 and March 2010. Patients
were excluded if they had previously undergone corneal
surgery such as keratoplasty. The mean ± SD age of the
patients was 43.7 ± 13.9 years (range 28–62). All patients
had been previously prescribed lenses (Table 1) but had
either discomfort or visual impairment wearing them.
Keratoconus was diagnosed on the basis of the Klyce-
Maeda index derived from the topography (TMS-4;
Tomey, Nagoya, Japan) and of characteristic clinical
findings such as apical protrusion or thinning of the cornea,
Vogt’s striae, superficial scarring, Munson’s sign and
Fleischer’s ring [23]. It was then graded according to
conicity measured with a keratometer and to the morpho-
logical shape of the cone determined by topography: mild,
moderate, advanced or severe for K readings of \45 D
(n = 4, 44.4 %), between 45 and 52 D (n = 1, 11.1 %),
between 52 and 62 D (n = 3, 33.3 %) or [62 D (n = 1,
11.1 %) in both meridians, respectively (Table 1). Regular
and irregular astigmatisms (asymmetry and higher order
irregularity components) were computed with Fourier ser-
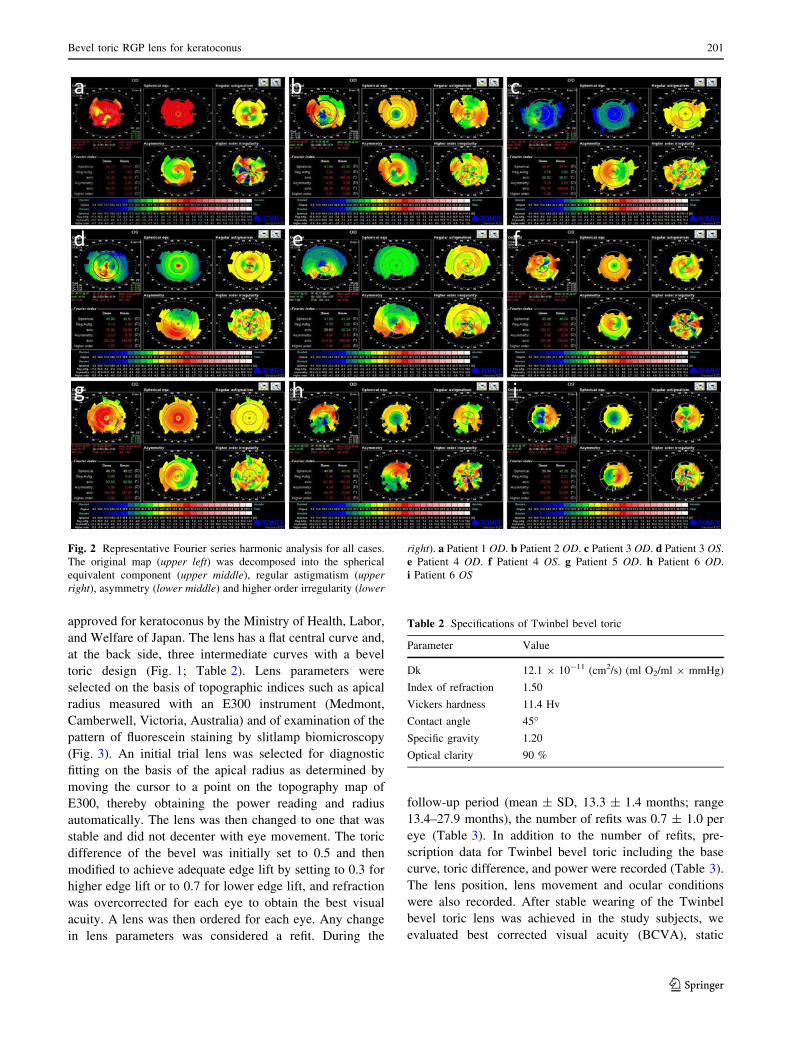
ies harmonic analysis of the videokeratography data. All
eyes showed asymmetry, regular astigmatism and higher
order irregularity by Fourier analysis (Fig. 2).
Twinbel bevel toric and RGP contact lenses were
obtained from Sun Contact Lens Co., Ltd. These are
Fig. 1 Specifications of the Twinbel bevel toric lens. a Bevel design.
BC base curve; IC intermediate curve, PC peripheral curve. The grayshape indicates the design of the large (flat) radius of bevel curvature,
and the black sharp shape indicates that of the small (steep) radius of
bevel curvature (horizontal and vertical, respectively). b Three-
dimensional diagram
Table 1 Patient characteristics and previous prescribed lenses
Patient Sex Age (years) Eye Stage of keratoconus Previous prescribed lens Ocular history
1 Female 28 Right Advanced Spherical RGP
2 Male 38 Right Mild Spherical RGP
3 Female 62 Right Mild Spherical RGP IOL, ptosis
Left Mild Spherical RGP Corneal scar, IOL, ptosis
4 Male 28 Right Mild Rose K
Left Severe Aphex KC
5 Male 45 Right Moderate Aphex KC
6 Female 51 Right Advanced Spherical RGP Corneal scar
Left Advanced Spherical RGP Corneal scar
Aphex KC: RGP contact lens with dual aspherical base curves [17]
IOL intraocular lens
200 R. Yanai et al.
123
approved for keratoconus by the Ministry of Health, Labor,
and Welfare of Japan. The lens has a flat central curve and,
at the back side, three intermediate curves with a bevel
toric design (Fig. 1; Table 2). Lens parameters were
selected on the basis of topographic indices such as apical
radius measured with an E300 instrument (Medmont,
Camberwell, Victoria, Australia) and of examination of the
pattern of fluorescein staining by slitlamp biomicroscopy
(Fig. 3). An initial trial lens was selected for diagnostic
fitting on the basis of the apical radius as determined by
moving the cursor to a point on the topography map of
E300, thereby obtaining the power reading and radius
automatically. The lens was then changed to one that was
stable and did not decenter with eye movement. The toric
difference of the bevel was initially set to 0.5 and then
modified to achieve adequate edge lift by setting to 0.3 for
higher edge lift or to 0.7 for lower edge lift, and refraction
was overcorrected for each eye to obtain the best visual
acuity. A lens was then ordered for each eye. Any change
in lens parameters was considered a refit. During the
follow-up period (mean ± SD, 13.3 ± 1.4 months; range
13.4–27.9 months), the number of refits was 0.7 ± 1.0 per
eye (Table 3). In addition to the number of refits, pre-
scription data for Twinbel bevel toric including the base
curve, toric difference, and power were recorded (Table 3).
The lens position, lens movement and ocular conditions
were also recorded. After stable wearing of the Twinbel
bevel toric lens was achieved in the study subjects, we
evaluated best corrected visual acuity (BCVA), static
Fig. 2 Representative Fourier series harmonic analysis for all cases.
The original map (upper left) was decomposed into the spherical
equivalent component (upper middle), regular astigmatism (upperright), asymmetry (lower middle) and higher order irregularity (lower
right). a Patient 1 OD. b Patient 2 OD. c Patient 3 OD. d Patient 3 OS.
e Patient 4 OD. f Patient 4 OS. g Patient 5 OD. h Patient 6 OD.
i Patient 6 OS
Table 2 Specifications of Twinbel bevel toric
Parameter Value
Dk 12.1 9 10-11 (cm2/s) (ml O2/ml 9 mmHg)
Index of refraction 1.50
Vickers hardness 11.4 Hv
Contact angle 45�Specific gravity 1.20
Optical clarity 90 %
Bevel toric RGP lens for keratoconus 201
123
contrast sensitivity and subjective symptoms. BCVA and
static contrast sensitivity were measured with both Twinbel
bevel toric and the previously prescribed lens. Static con-
trast sensitivity was measured with the use of a contrast
grating with internal illumination and a contrast luminance
of 85 cd/m2 (CSV 1000; Vector Vision, Dayton, OH,
USA). The test presents four rows of sine-wave gratings
with spatial frequencies of 3, 6, 12 and 18 cycles/degree at
2.5 m; sensitivity levels range from 0.7 to 2.08, 0.91 to
2.29, 0.61 to 1.99 and 0.17 to 1.55 log units, respectively.
Patients were asked to provide details concerning foreign
body sensation, dryness, blurriness, lens dislocation and
overall performance in order to compare the subjective
complaints for Twinbel bevel toric with those for the pre-
viously prescribed lens. The subjective complaints were
rated according to a six-point ordinal scale for analysis.
Efficacy and safety were evaluated at 12 weeks or later
after the switch to Twinbel bevel toric.
Data are presented as mean ± SD. Statistical analysis of
visual acuity was performed after conversion to logMAR
units. Differences in BCVA, contrast sensitivity and
symptom scores between Twinbel bevel toric and the ori-
ginal contact lens were assessed with the paired Student’s
t test. A P value of \0.05 was considered statistically
significant.
Results
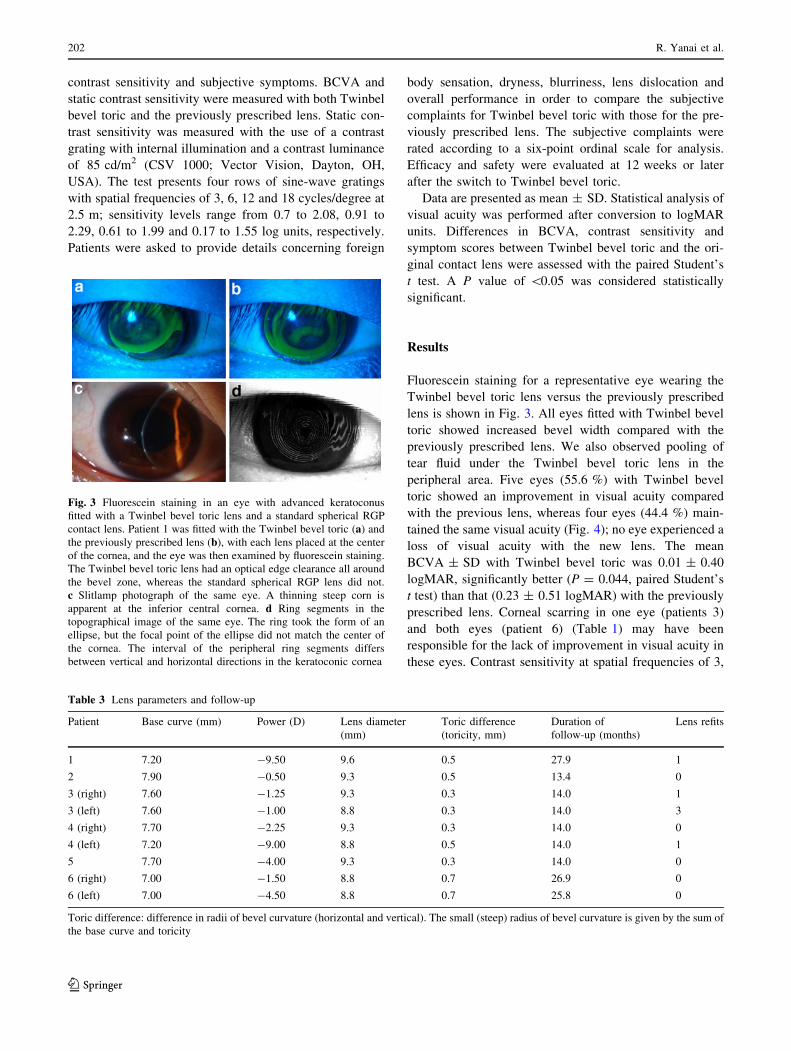
Fluorescein staining for a representative eye wearing the
Twinbel bevel toric lens versus the previously prescribed
lens is shown in Fig. 3. All eyes fitted with Twinbel bevel
toric showed increased bevel width compared with the
previously prescribed lens. We also observed pooling of
tear fluid under the Twinbel bevel toric lens in the
peripheral area. Five eyes (55.6 %) with Twinbel bevel
toric showed an improvement in visual acuity compared
with the previous lens, whereas four eyes (44.4 %) main-
tained the same visual acuity (Fig. 4); no eye experienced a
loss of visual acuity with the new lens. The mean
BCVA ± SD with Twinbel bevel toric was 0.01 ± 0.40
logMAR, significantly better (P = 0.044, paired Student’s
t test) than that (0.23 ± 0.51 logMAR) with the previously
prescribed lens. Corneal scarring in one eye (patients 3)
and both eyes (patient 6) (Table 1) may have been
responsible for the lack of improvement in visual acuity in
these eyes. Contrast sensitivity at spatial frequencies of 3,
Fig. 3 Fluorescein staining in an eye with advanced keratoconus
fitted with a Twinbel bevel toric lens and a standard spherical RGP
contact lens. Patient 1 was fitted with the Twinbel bevel toric (a) and
the previously prescribed lens (b), with each lens placed at the center
of the cornea, and the eye was then examined by fluorescein staining.
The Twinbel bevel toric lens had an optical edge clearance all around
the bevel zone, whereas the standard spherical RGP lens did not.
c Slitlamp photograph of the same eye. A thinning steep corn is
apparent at the inferior central cornea. d Ring segments in the
topographical image of the same eye. The ring took the form of an
ellipse, but the focal point of the ellipse did not match the center of
the cornea. The interval of the peripheral ring segments differs
between vertical and horizontal directions in the keratoconic cornea
Table 3 Lens parameters and follow-up
Patient Base curve (mm) Power (D) Lens diameter
(mm)
Toric difference
(toricity, mm)
Duration of
follow-up (months)
Lens refits
1 7.20 -9.50 9.6 0.5 27.9 1
2 7.90 -0.50 9.3 0.5 13.4 0
3 (right) 7.60 -1.25 9.3 0.3 14.0 1
3 (left) 7.60 -1.00 8.8 0.3 14.0 3
4 (right) 7.70 -2.25 9.3 0.3 14.0 0
4 (left) 7.20 -9.00 8.8 0.5 14.0 1
5 7.70 -4.00 9.3 0.3 14.0 0
6 (right) 7.00 -1.50 8.8 0.7 26.9 0
6 (left) 7.00 -4.50 8.8 0.7 25.8 0
Toric difference: difference in radii of bevel curvature (horizontal and vertical). The small (steep) radius of bevel curvature is given by the sum of
the base curve and toricity
202 R. Yanai et al.
123
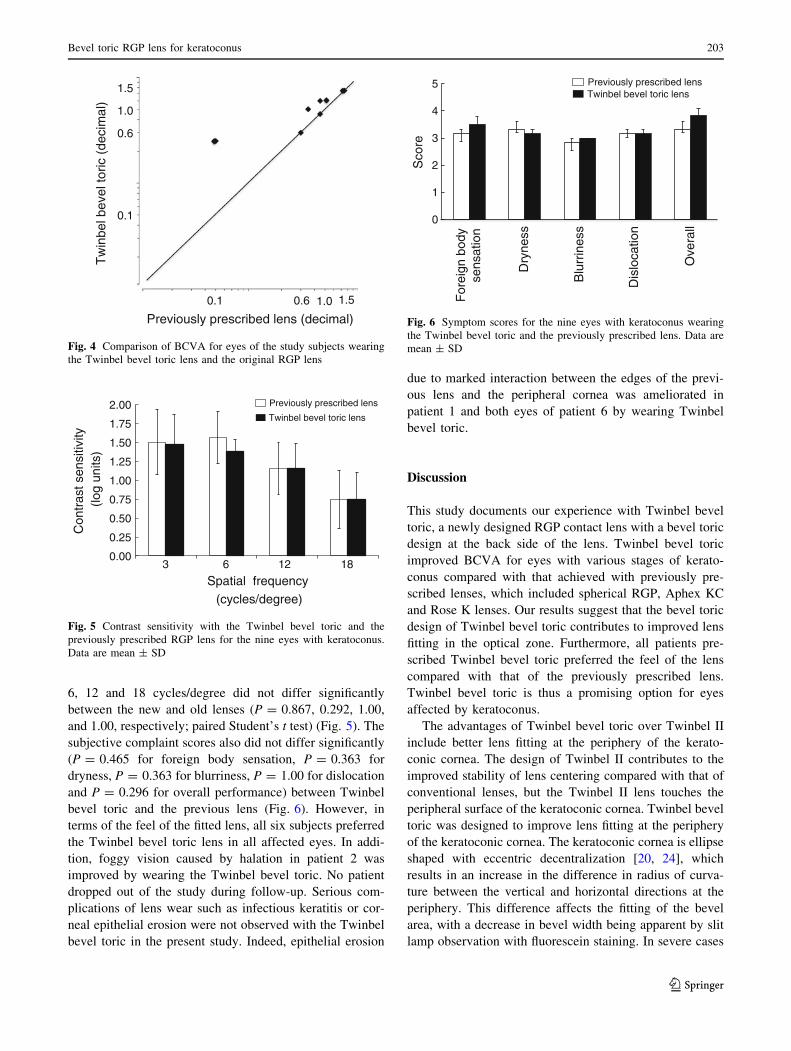
6, 12 and 18 cycles/degree did not differ significantly
between the new and old lenses (P = 0.867, 0.292, 1.00,
and 1.00, respectively; paired Student’s t test) (Fig. 5). The
subjective complaint scores also did not differ significantly
(P = 0.465 for foreign body sensation, P = 0.363 for
dryness, P = 0.363 for blurriness, P = 1.00 for dislocation
and P = 0.296 for overall performance) between Twinbel
bevel toric and the previous lens (Fig. 6). However, in
terms of the feel of the fitted lens, all six subjects preferred
the Twinbel bevel toric lens in all affected eyes. In addi-
tion, foggy vision caused by halation in patient 2 was
improved by wearing the Twinbel bevel toric. No patient
dropped out of the study during follow-up. Serious com-
plications of lens wear such as infectious keratitis or cor-
neal epithelial erosion were not observed with the Twinbel
bevel toric in the present study. Indeed, epithelial erosion
due to marked interaction between the edges of the previ-
ous lens and the peripheral cornea was ameliorated in
patient 1 and both eyes of patient 6 by wearing Twinbel
bevel toric.
Discussion
This study documents our experience with Twinbel bevel
toric, a newly designed RGP contact lens with a bevel toric
design at the back side of the lens. Twinbel bevel toric
improved BCVA for eyes with various stages of kerato-
conus compared with that achieved with previously pre-
scribed lenses, which included spherical RGP, Aphex KC
and Rose K lenses. Our results suggest that the bevel toric
design of Twinbel bevel toric contributes to improved lens
fitting in the optical zone. Furthermore, all patients pre-
scribed Twinbel bevel toric preferred the feel of the lens
compared with that of the previously prescribed lens.
Twinbel bevel toric is thus a promising option for eyes
affected by keratoconus.
The advantages of Twinbel bevel toric over Twinbel II
include better lens fitting at the periphery of the kerato-
conic cornea. The design of Twinbel II contributes to the
improved stability of lens centering compared with that of
conventional lenses, but the Twinbel II lens touches the
peripheral surface of the keratoconic cornea. Twinbel bevel
toric was designed to improve lens fitting at the periphery
of the keratoconic cornea. The keratoconic cornea is ellipse
shaped with eccentric decentralization [20, 24], which
results in an increase in the difference in radius of curva-
ture between the vertical and horizontal directions at the
periphery. This difference affects the fitting of the bevel
area, with a decrease in bevel width being apparent by slit
lamp observation with fluorescein staining. In severe cases
Previously prescribed lens (decimal)
Tw
inbe
l bev
el to
ric (
deci
mal
)
0.1 1.0 1.5
0.1
1.0
1.5
0.6
0.6
Fig. 4 Comparison of BCVA for eyes of the study subjects wearing
the Twinbel bevel toric lens and the original RGP lens
0.00
0.25
0.50
0.75
1.00
1.25
1.50
1.75
2.00
Spatial frequency(cycles/degree)
Previously prescribed lens
Twinbel bevel toric lens
Con
tras
t sen
sitiv
ity(lo
g un
its)
3 6 12 18
Fig. 5 Contrast sensitivity with the Twinbel bevel toric and the
previously prescribed RGP lens for the nine eyes with keratoconus.
Data are mean ± SD
0
1
2
3
4
5
Sco
re
For
eign
bod
y se
nsat
ion
Dry
ness
Blu
rrin
ess
Dis
loca
tion
Ove
rall
Previously prescribed lens Twinbel bevel toric lens
Fig. 6 Symptom scores for the nine eyes with keratoconus wearing
the Twinbel bevel toric and the previously prescribed lens. Data are
mean ± SD
Bevel toric RGP lens for keratoconus 203
123

of keratoconus, the peripheral cornea in the flatter meridian
direction makes marked contact with the edges of the lens,
often resulting in the development of corneal epithelial
disorders [25]. Such inadequate fitting also reduces tear
volume under the lens at the bevel zone and results in a
sensation of discomfort. The steep bevel of the Twinbel
bevel toric fits the steeper meridian at the peripheral cor-
nea, whereas its flat bevel also fits with the flatter meridian
at the peripheral cornea. The rotation of Twinbel bevel
toric is often observed during continuous rapid blinking,
but the orientation of the lens returns immediately to an
adequate position and is stable during normal blinking. In
the present study, all keratoconus patients were satisfied
with the fit of the Twinbel bevel toric and did not drop out
of the study before the final visit. Our experience thus
suggests that Twinbel bevel toric should be a clinical
option for fitting in keratoconus.
In this study, mean BCVA was improved by the switch
to Twinbel bevel toric, with no patients showing a decrease
in BCVA. Although in 44.4 % of cases BCVA was not
improved by the Twinbel bevel toric, all of these eyes with
the exception of one with a corneal scar showed a BCVA of
[0.9. These cases had, therefore, likely already achieved
maximum visual acuity with the previous lens. These
observations suggest that the Twinbel bevel toric was
effective for correction of both irregular and regular
astigmatism induced by corneal irregularity in keratoconus.
Although mean BCVA was improved by the Twinbel bevel
toric compared with that achieved with the previous lens,
the small number of subjects in the present study means
that further studies are needed to confirm that this lens can
to improve the quality of vision including BCVA. Contrast
sensitivity was not significantly improved by the Twinbel
bevel toric, which is consistent with the results of previous
studies with RGP lenses in keratoconus [26–28].
Foggy vision associated with halation in patient 2 was
improved by the Twinbel bevel toric. This patient had com-
plained of the same symptoms while wearing both conven-
tional and special lenses, including Rose K and Aphex KC, for
more than 10 years. Although we had attempted to respond to
the complaint, changing the base curve, size, power or the
design of the lens all proved ineffective. The improvement in
fitting at the peripheral cornea with the Twinbel bevel toric
may have facilitated exchange of tear fluid and reduced the
feeling of discomfort. Among the eyes with mild keratoconus
in the present study, only this case needed a toricity of 0.5 mm
for the Twinbel bevel toric, whereas the others required a
toricty of 0.3 mm (Tables 1, 3). This case suggests the
importance of lens fitting at the peripheral cornea in mild
keratoconus, especially when it is symptomatic, even in the
absence of significant objective findings.
The process of contact lens fitting for eyes affected by
advanced keratoconus is complicated and challenging for
both the patient and the fitter. Although various new
therapies have been developed [29–40], contact lenses
remain the most effective means for achieving good vision
in such eyes. If the keratoconic cornea becomes too scarred
or too steep to tolerate a contact lens, corneal transplan-
tation is indicated. There was no significant obvious cor-
relation between lens parameters such as base curve,
diameter and toricity and the stage of keratoconus in the
present study (Tables 1, 3). However, a larger toricity
([0.5 mm) tended to be needed in eyes with advanced
keratoconus. These data suggest that the Twinbel bevel
toric might be more effective in eyes with larger differ-
ences in radii of curvature at the periphery.
Another important factor with regard to contact lens
wear in keratoconus patients is the safety of wearing the
lens for extended periods [41]. The number of hours each
day that a contact lens is worn tends to be greater for
keratoconus patients than for other individuals because of
the lack of any other way to correct their vision. Moreover,
given that the onset of keratoconus occurs during puberty,
lens wearing can be required over most of a lifetime. The
safety of contact lens wear in terms of corneal health is thus
an important issue in patients with keratoconus.
One of the major objectives of the present study was to
determine the safety and efficacy of the bevel toric lens
design for eyes affected by keratoconus. A multitude of
lenses has been developed for patients with this condition
[8–19]. However, no previous study has examined a bevel
toric lens, designed to improve bevel width and tear
exchange efficacy, in such patients. Although we did not
measure the exchange of tear fluid in the subjects of the
present study, we did observe pooling of tear fluid under
the Twinbel bevel toric lens in all studied eyes. Tear
exchange and oxygen supply are essential for glucose
metabolism in corneal epithelial cells. The demonstrated
efficacy of the Twinbel bevel toric for improvement of
vision in keratoconus patients suggests that it might also be
suitable for eyes with irregular or strong astigmatism, such
as those affected by pellucid marginal degeneration or
those subjected to keratoplasty, refractive surgery or cor-
neal injury.
Acknowledgments This study was supported by a grant from the
Japanese Eye Bank Association (to R.Y.).
References
1. Krachmer JH, Feder RS, Belin MW. Keratoconus and related
noninflammatory corneal thinning disorders. Surv Ophthalmol.
1984;28:293–322.
2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:
297–319.
3. Kim H, Joo CK. Measure of keratoconus progression using
Orbscan II. J Refract Surg. 2008;24:600–5.
204 R. Yanai et al.
123
4. Haque S, Jones L, Simpson T. Thickness mapping of the cornea
and epithelium using optical coherence tomography. Optom Vis
Sci. 2008;85:E963–76.
5. Ye P, Tang K, Hofbauer J, Weissman BA. A case report of
keratoconus with regular astigmatic topography. Eye Contact
Lens. 2007;33:203–6.
6. Nakagawa T, Maeda N, Kosaki R, Hori Y, Inoue T, Saika M,
et al. Higher-order aberrations due to the posterior corneal surface
in patients with keratoconus. Invest Ophthalmol Vis Sci.
2009;50:2660–5.
7. Jinabhai A, Radhakrishnan H, O’Donnell C. Visual acuity and
ocular aberrations with different rigid gas permeable lens fittings
in keratoconus. Eye Contact Lens. 2010;36:233–7.
8. Betts AM, Mitchell GL, Zadnik K. Visual performance and
comfort with the Rose K lens for keratoconus. Optom Vis Sci.
2002;79:493–501.
9. Jain AK, Sukhija J. Rose-K contact lens for keratoconus. Indian J
Ophthalmol. 2007;55:121–5.
10. Ozkurt YB, Sengor T, Kurna S, Evciman T, Acikgoz S, Haboglu
M, et al. Rose K contact lens fitting for keratoconus. Int Oph-
thalmol. 2008;28:395–8.
11. Szczotka-Flynn LB, Patel S. Menicon Z rigid gas permeable
lenses for keratoconus and irregular corneas: a retrospective case
series. Eye Contact Lens. 2008;34:254–60.
12. Hu CY, Tung HC. Managing keratoconus with reverse-geometry
and dual-geometry contact lenses: a case report. Eye Contact
Lens. 2008;34:71–5.
13. Erdurmus M, Yildiz EH, Abdalla YF, Hammersmith KM,
Rapuano CJ, Cohen EJ. Contact lens related quality of life in
patients with keratoconus. Eye Contact Lens. 2009;35:123–7.
14. Bilgin LK, Yilmaz S, Araz B, Yuksel SB, Sezen T. 30 years of
contact lens prescribing for keratoconic patients in Turkey.
Contact Lens Anterior Eye. 2009;32:16–21.
15. Mandathara Sudharman P, Rathi V, Dumapati S. Rose K lenses for
keratoconus—an Indian experience. Eye Contact Lens. 2010;36:220–2.
16. Schornack MM, Patel SV. Scleral lenses in the management of
keratoconus. Eye Contact Lens. 2010;36:39–44.
17. Yanai R, Ueda K, Nishida T. Retrospective analysis of vision cor-
rection and lens tolerance in keratoconus patients prescribed a contact
lens with dual aspherical curves. Eye Contact Lens. 2010;36:86–9.
18. Kang YS, Park YK, Lee JS, Lee SU, Shin JH, Han YS, et al. The
effect of the YK lens in keratoconus. Ophthalmic Physiol Opt.
2010;30:267–73.
19. Barnett M, Mannis MJ. Contact lenses in the management of
keratoconus. Cornea. 2011;30:1510–6.
20. Zadnik K, Steger-May K, Fink BA, Joslin CE, Nichols JJ,
Rosenstiel CE, et al. Between-eye asymmetry in keratoconus.
Cornea. 2002;21:671–9.
21. Oshida T, Fushimi N, Sakimoto T, Sawa M. Acute hydrops in a
host cornea after penetrating keratoplasty for keratoconus. Jpn J
Ophthalmol. 2011;55:418–9.
22. Yanai R, Ishida Y, Ueda K, Nishida T. Use of multi-curved rigid
contact lenses for irregular astigmatism after penetrating kera-
toplasty. J Jpn Contact Lens Soc. 2007;49:166–70.
23. Romero-Jimenez M, Santodomingo-Rubido J, Wolffsohn JS. Ker-
atoconus: a review. Contact Lens Anterior Eye. 2010;33:157–66.
24. Wilson SE, Lin DT, Klyce SD, Reidy JJ, Insler MS. Rigid contact
lens decentration: a risk factor for corneal warpage. CLAO J.
1990;16:177–82.
25. Moon JW, Shin KC, Lee HJ, Wee WR, Lee JH, Kim MK. The
effect of contact lens wear on the ocular surface changes in
keratoconus. Eye Contact Lens. 2006;32:96–101.
26. Negishi K, Kumanomido T, Utsumi Y, Tsubota K. Effect of
higher-order aberrations on visual function in keratoconic eyes
with a rigid gas permeable contact lens. Am J Ophthalmol.
2007;144:924–9.
27. Marsack JD, Parker KE, Pesudovs K, Donnelly WJ 3rd, Apple-
gate RA. Uncorrected wavefront error and visual performance
during RGP wear in keratoconus. Optom Vis Sci. 2007;84
:463–70.
28. Wei RH, Khor WB, Lim L, Tan DT. Contact lens characteristics
and contrast sensitivity of patients with keratoconus. Eye Contact
Lens. 2011;37:307–11.
29. Chan CC, Wachler BS. Reduced best spectacle-corrected visual
acuity from inserting a thicker Intacs above and thinner Intacs
below in keratoconus. J Refract Surg. 2007;23:93–5.
30. Thebpatiphat N, Hammersmith KM, Rapuano CJ, Ayres BD,
Cohen EJ. Cataract surgery in keratoconus. Eye Contact Lens.
2007;33:244–6.
31. Tomalla M, Cagnolati W. Modern treatment options for the
therapy of keratoconus. Contact Lens Anterior Eye. 2007;30:
61–6.
32. Shetty R, Kurian M, Anand D, Mhaske P, Narayana KM, Shetty
BK. Intacs in advanced keratoconus. Cornea. 2008;27:1022–9.
33. Elsahn AF, Rapuano CJ, Antunes VA, Abdalla YF, Cohen EJ.
Excimer laser phototherapeutic keratectomy for keratoconus
nodules. Cornea. 2009;28:144–7.
34. Abdalla YF, Elsahn AF, Hammersmith KM, Cohen EJ. Synerg-
Eyes lenses for keratoconus. Cornea. 2010;29:5–8.
35. Espandar L, Meyer J. Keratoconus: overview and update on
treatment. Middle East Afr J Ophthalmol. 2010;17:15–20.
36. Pesando PM, Ghiringhello MP, Di Meglio G, Romeo S. Treat-
ment of keratoconus with Ferrara ICRS and consideration of the
efficacy of the Ferrara nomogram in a 5-year follow-up. Eur J
Ophthalmol. 2010;20:865–73.
37. Yu JO, Gundel RE. Use of Acular LS in the pain management of
keratoconus: a pilot study. Optom Vis Sci. 2010;87:125–30.
38. Izquierdo L Jr, Henriquez MA, McCarthy M. Artiflex phakic
intraocular lens implantation after corneal collagen cross-linking
in keratoconic eyes. J Refract Surg. 2011;27:482–7.
39. Kang SY, Park YK, Song JS, Kim HM. Anterior stromal puncture
for treatment of contact lens-intolerant keratoconus patients.
Graefes Arch Clin Exp Ophthalmol. 2011;249:89–92.
40. Sedaghat M, Ansari-Astaneh MR, Zarei-Ghanavati M, Davis SW,
Sikder S. Artisan iris-supported phakic IOL implantation inpatients with keratoconus: a review of 16 eyes. J Refract Surg.
2011;27:489–93.
41. Yildiz EH, Diehl GF, Cohen EJ, Hammersmith KM, Laibson PR,
Rapuano CJ. Demographics of patients older than 50 years with
keratoconus. Eye Contact Lens. 2009;35:309–11.
Bevel toric RGP lens for keratoconus 205
123