basic life support for healthcare providers · basic life support for healthcare providers basic...
TRANSCRIPT

BASIC LIFE SUPPORT FOR HEALTHCARE PROVIDERSBASIC LIFE SUPPORT FORHEALTHCARE PROVIDERS
2015 2015
Immediately resume CPR starting with compressions.
Continue for 2 minutes
Immediately resume CPR starting with compressions.
Continue for 2 minutes
Start Compressions
Compress the chest fast (almost 2 per second)Push hard / Ensure full chest recoil /
Minimize interruptions
Breaths
If unable to perform breaths, do continuous compressions until equipment arrives
Give 1 Shock
Monophasic – 360JBiphasic – 120 - 360J
Paediatric – 4J/kg
Attach AED / Defib immediately
Shock Advised(VF/VT)
No Shock Advised(PEA/Asystole)
• No Pulse or not sure• Pulse rate <60 in children and infants
• Give rescue breaths
• Adult: every 6 seconds• Child: every 5 seconds• Infant: every 4 seconds
• Reassess continuously
Has pulse but no effective breathing
• Place in recovery position • Check for continued breathing• Reassess continuously
Has pulse and breathing
Continue until AED / Defib arrives
ANALYSE RHYTHM
www.resuscitationcouncil.co.za
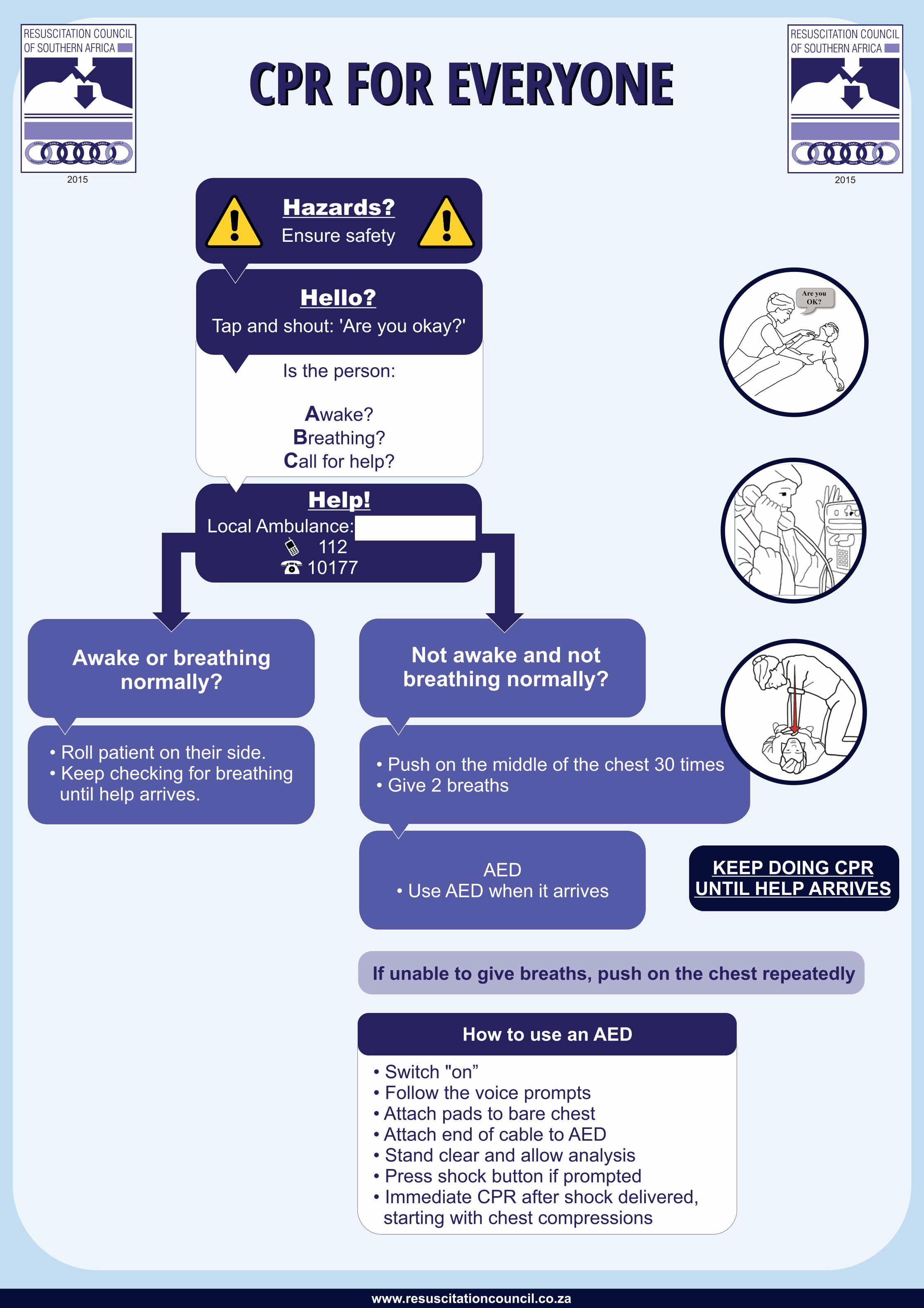
CPR FOR EVERYONECPR FOR EVERYONE
2015 2015
Not awake and not breathing normally?
• Push on the middle of the chest 30 times• Give 2 breaths
Awake or breathing normally?
• Roll patient on their side.• Keep checking for breathing until help arrives.
AED• Use AED when it arrives
Local Ambulance:....................112
10177
Ensure safety
Tap and shout: 'Are you okay?'
Is the person:
Awake?
Breathing?
Call for help?
How to use an AED
• Switch "on”• Follow the voice prompts• Attach pads to bare chest• Attach end of cable to AED• Stand clear and allow analysis• Press shock button if prompted• Immediate CPR after shock delivered, starting with chest compressions
If unable to give breaths, push on the chest repeatedly
KEEP DOING CPRUNTIL HELP ARRIVES
www.resuscitationcouncil.co.za

ADVANCED CARDIAC ARREST ALGORITHM
Adult and Paediatric
ADVANCED CARDIAC ARREST ALGORITHM
Adult and Paediatric2015 2015
Start Compressions
Compress the chest fast (almost 2 per second)
Push hard / Ensure full chest recoil /
Minimize interruptions
Attempt 2 breaths at 1 breath/second(with if available) after every 30 compressions
Continue until AED / Defib arrives
BreathsIf unable to perform breaths, do continuous compressions until equipment arrives
Attach AED / Defib immediately
• No Pulse or not sure• Pulse rate <60 in
children and infants
• Give rescue breaths
• Adult: every 6 seconds• Child: every 5 seconds• Infant: every 4 seconds
• Reassess continuously
Has pulse but no effective breathing
• Place in recovery position • Check for continued breathing• Reassess continuously
Has pulse and breathing
Contributory Causes:• Hypoxia• Hypovolaemia• Hypothermia• Hydrogen ion (Acidosis)• Hypo- / Hyperkalaemia• Hypoglycaemia• Tension Pneumothorax• Tamponade (Cardiac)• Toxins• Trauma• Thrombosis (Coronary)• Thrombosis (Pulmonary)
High Quality CPR:• Compression rate 100 – 120 per minute• Avoid excessive ventilation; 1 breath every 6 seconds if advanced airway • Rotate compressors every 2 minutes• Consider capnography and arterial monitoring
Advanced Considerations:Correct contributory causes• Obtain IV/IO access, take ABG/VBG• Give high levels of Fi and consider •
advanced airway if requiredContinuous chest compressions •
after advanced airway in placeConsider Adrenaline and •
antiarrhythmics:Adrenaline 1mg every 3 - 5 min •
(0.01mg/kg in paed)Amiodarone 300mg followed by •
150mg (5mg/kg in paed) or if not available Lignocaine 1.5mg/kg initial,
followed by 0.5mg/kg (max 3mg/kg)
Immediately resume CPR starting with compressions.
Continue for 2 minutes
Give 1 Shock
Monophasic – 360JBiphasic – 120-360J
Paediatric – 4J/kg
Shock Advised(VF/VT)
Immediately resume CPR starting with compressions.
Continue for 2 minutes
No Shock Advised(PEA/Asystole)
ANALYSE RHYTHM
Additional considerations:1) VA ECMO might be considered in appropriate centres when available;
2) Ultrasound can be considered as a diagnostic and procedural tool where training and resources exist.
www.resuscitationcouncil.co.za

BRADYCARDIA MANAGEMENT ALGORITHM
BRADYCARDIA MANAGEMENT ALGORITHM
2015 2015
Alternatives• Transvenous pacing
• High dose Insulin (1 U/kg if BB or CCB)• Glucagon (if BB or CCB overdose)
ADRENALINE(0.05μg/kg/min 0.5 μg/kg/min
infusion)OR
TRANSCUTANEOUS PACING
ATROPINE(Exclude Hypoxia/Hypothermia/
Head injury)
0.5 mg IV bolusCan repeat every 3 - 5 minutes,
up to 3 mg
BRADYCARDIAHR < 60/min despite effectiveoxygenation and ventilation
IF UNSTABLE
START CPR1 Rescuer = 30 compressions : 2 breaths2 Rescuers = 15 compressions : 2 breaths
ADRENALINE0.1 ml/kg IV of 1:10 000 dilution(Max - 1 mg) every 3 - 5 minutes
ATROPINE0.02 mg/kg IV if vagal tone or
1° AV blockMaximum 0.5mg
CONSIDER PACING
BRADYCARDIAHR < 50/min
IF UNSTABLE
SIGNS OF INSTABILITY• Hypotension
• Acutely altered mental state• Signs of shock
• Ischaemic chest discomfort• Acute heart failure
ECG RHYTHMRun rhythm strip to confirm dysrhythmia
12 lead ECG if possibleIdentify and treat underlying causes
DRIPEstablish IV access
CIRCULATIONAssess pulse, blood pressure and
perfusionAttach ECG monitor, pulse oximeter and vital signs monitor if available
BREATHINGAdminister oxygen if required. Target Saturation 94-98%
Ventilate if necessary
AIRWAYOpen, maintain and protect as necessary
* BB = Beta Blockers* CCB = Calcium Channel Blockers
SPECIALIST MEDICAL ADVICE SHOULD BE SOUGHT
WHENEVER POSSIBLE
ADULT PAEDIATRIC
Look for and treat contributory causes
of Bradycardia
• Hypoxia• Hypothermia• Head Injury
• Hyperkalaemia• Heart Block
• Hydrogen Ion (Acidosis)• Hypotension
• Toxins(e.g. organophosphates)
• Theraputic Agents (e.g. beta blocker overdose/
calcium channel blocker overdose)
www.resuscitationcouncil.co.za

TACHYCARDIA MANAGEMENT ALGORITHM
TACHYCARDIA MANAGEMENT ALGORITHM
2015 2015
AMIODARONE150 mg in 5% D/W over 10 minutes
IV (15 mg/min) then 1 mg/min infusion
Alternatives (esp irregular rhythms)
• BB or CCB
ADENOSINE (NOT if varying R-R intervals /
Atrial fibrillation)6 mg IV rapidly, then 12mg IV
after 1 - 2min prn
AlternativesIce water applied to face
Coughing / Breath-holdingCarotid Sinus Massage (C/I if bruits,
CVS disease, elderly)
VAGAL STIMULATION(NOT if varying R-R intervals /
Atrial fibrillation)Preferable: Valsalva (Modified)
NARROW COMPLEX TACHYCARDIA
(Supraventricular Tachycardia)HR > 150/min with QRS < 0.12 sec
Alternatives (esp irregular rhythms)
• BB or CCB
Consider (if Torsades de Pointes):• Defibrillation (Asynchronous)
• Magnesium (2g IV over 10min)• Correct Electrolytes and consider
toxins/drugs
AMIODARONE150 mg in 5% D/W over 10min IV (15 mg / min), then 1 mg / min infusion
WIDE COMPLEXTACHYCARDIA
(Ventricular Tachycardia)Generally HR > 150/min with
QRS > 0.12 sec
ECG RHYTHMRun rhythm strip to confirm dysrhythmia
12 lead ECG if possibleIdentify and treat underlying causes
SIGNS OF INSTABILITY• Hypotension
• Acutely altered mental state• Signs of shock
• Ischaemic chest discomfort• Acute heart failure
TACHYCARDIAHR > 150/min * See Paed Rates
SYNCHRONISED CARDIOVERSION
Consider procedural sedation
Start with 100J initially(monophasic or biphasic)
UNSTABLE
DRIPEstablish IV access
CIRCULATIONAssess pulse, blood pressure and
perfusionAttach ECG monitor, pulse oximeter and vital signs monitor if available
BREATHINGAdminister oxygen if required. Target Saturation 94 - 98%
Ventilate if necessary
AIRWAYOpen, maintain and protect as necessary
STABLE
Paediatric start 0.5 - 1J/kgthen 2J/kg (Max 4J/kg)
Paediatric Drug DosesAdenosine 0.1mg / kg rapidly
followed by 0.2mg / kg
Amiodarone 5mg / kgover 20 - 60min (max 300mg)
Magnesium 50 mg / kg
SPECIALIST MEDICAL ADVICE SHOULD BE SOUGHT
WHENEVER POSSIBLE
* BB = Beta Blockers* CCB = Calcium Channel Blockers
* Paediatric Tachycardia Rates
QRS < 0.08sec
QRS > 0.08 sec
www.resuscitationcouncil.co.za
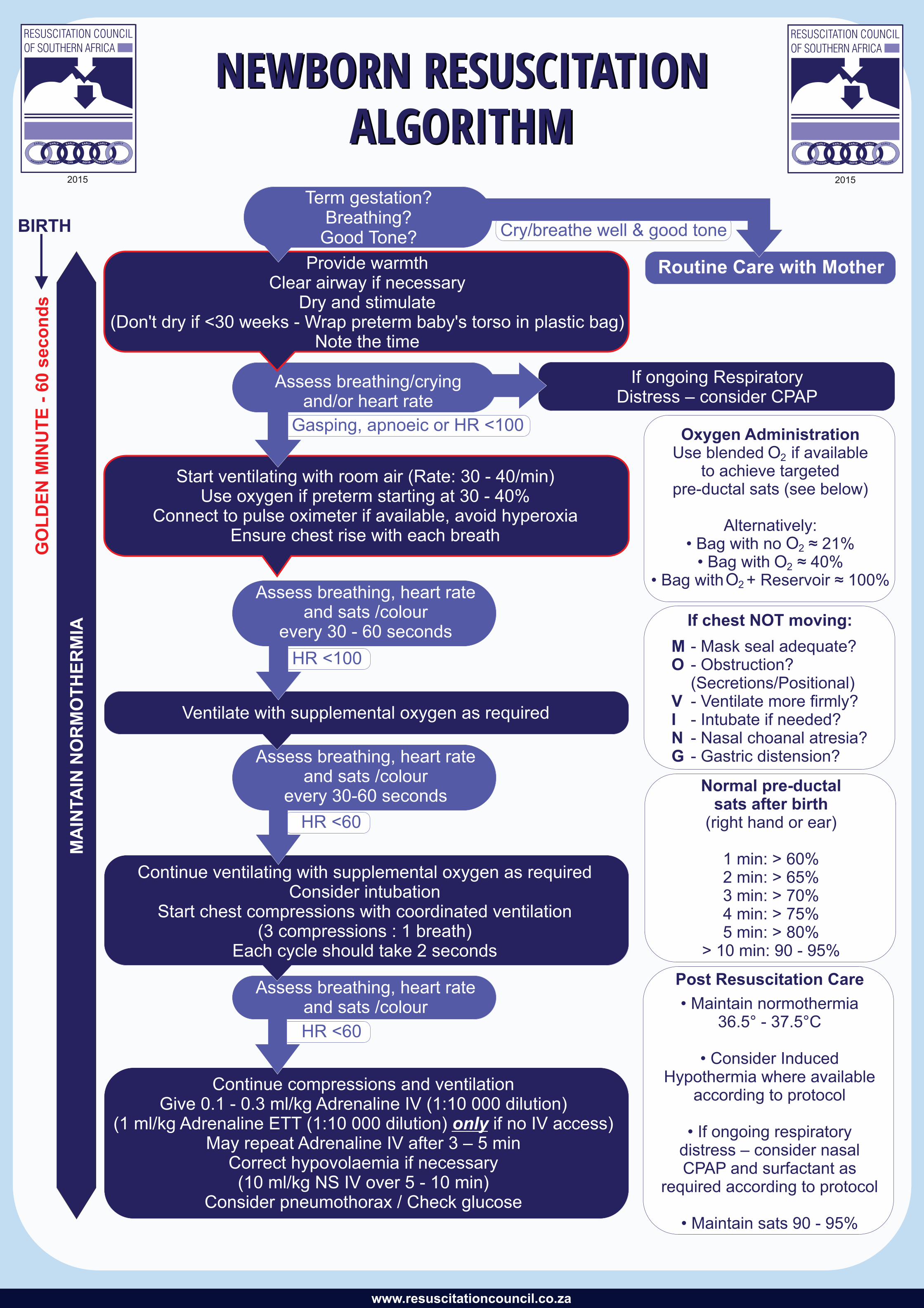
NEWBORN RESUSCITATION ALGORITHM
NEWBORN RESUSCITATION ALGORITHM
2015 2015
www.resuscitationcouncil.co.za
NEWBORN RESUSCITATION ALGORITHM
NEWBORN RESUSCITATION ALGORITHM
2015 2015
www.resuscitationcouncil.co.za
Continue compressions and ventilation Give 0.1 - 0.3 ml/kg Adrenaline IV (1:10 000 dilution)
(1 ml/kg Adrenaline ETT (1:10 000 dilution) only if no IV access)May repeat Adrenaline IV after 3 – 5 min
Correct hypovolaemia if necessary (10 ml/kg NS IV over 5 - 10 min)
Consider pneumothorax / Check glucose
HR <60
Assess breathing, heart rateand sats /colour
Continue ventilating with supplemental oxygen as required Consider intubation
Start chest compressions with coordinated ventilation(3 compressions : 1 breath)
Each cycle should take 2 seconds
HR <60
Assess breathing, heart rateand sats /colour
every 30-60 seconds
HR <100
Assess breathing, heart rateand sats /colour
every 30 - 60 seconds
Start ventilating with room air (Rate: 30 - 40/min)Use oxygen if preterm starting at 30 - 40%
Connect to pulse oximeter if available, avoid hyperoxia Ensure chest rise with each breath
Ventilate with supplemental oxygen as required
Provide warmthClear airway if necessary
Dry and stimulate (Don't dry if <30 weeks - Wrap preterm baby's torso in plastic bag)
Note the time
Assess breathing/crying and/or heart rate
Gasping, apnoeic or HR <100
MA
INTA
IN N
OR
MO
TH
ER
MIA
If ongoing Respiratory Distress – consider CPAP
BIRTH
GO
LD
EN
MIN
UT
E -
60 s
eco
nd
s
Cry/breathe well & good tone
Term gestation?Breathing?
Good Tone?
Oxygen AdministrationUse blended if available
to achieve targeted pre-ductal sats (see below)
Alternatively:• Bag with no ≈ 21%
• Bag with ≈ 40%• Bag with + Reservoir ≈ 100%
Normal pre-ductal sats after birth
(right hand or ear)
1 min: > 60%2 min: > 65%3 min: > 70%4 min: > 75%5 min: > 80%
> 10 min: 90 - 95%
Post Resuscitation Care
• Maintain normothermia36.5° - 37.5°C
• Consider InducedHypothermia where available
according to protocol
• If ongoing respiratory distress – consider nasalCPAP and surfactant as
required according to protocol
• Maintain sats 90 - 95%
If chest NOT moving:
- Mask seal adequate?- Obstruction?(Secretions/Positional)- Ventilate more firmly?- Intubate if needed?- Nasal choanal atresia?- Gastric distension?
MO
VING

POST CARDIAC ARREST CARE(Return of Spontaneous Circulation)
Circulatory ControlMaintain and monitor perfusion
• Initially target SBP > 90 mmHg (MAP > 65 mmHg)• Urine output
• Lactate levels
Advanced monitoring• Monitor HR, BP, capillary refill
• Consider appropriate fluid administration• Consider inotrope infusion
Breathing Support• If required ventilate every 6 seconds
• Target normoxia; oxygen saturation at 94 - 98%• Target normocarbia (C 35 – 45 mmHg)
• Apply protective lung ventilation when appropriate
Airway Management• Open and maintain• Intubate if required
• Use capnography when available
Suggested Initial Ventilation• Tidal Vol of 6 ml/kg (ideal weight) • PEEP of ≥ 5 cmH • Target pH of > 7.20)
Inotrope AdministrationStart Adrenaline at 0.05μg/kg/min and titrate to effect
Differential DiagnosisSearch for contributory causes
Hypoxia • Hypovolaemia •
Hypo/hyperkalaemia • Hydrogen ion imbalance (Acidosis) •
Hypoglycaemia •Hypothermia •
• Tension pneumothorax• Tamponade• Thrombosis (coronary)• Thrombosis (pulmonary)• Toxins and drugs• Trauma
Evaluation• 12 lead ECG (including right-sided ECG)
• Coronary angiography if arrest of suspected cardiac origin• Early Reperfusion if indicated (especially STEMI or LBBB)
• Continuous ECG monitoring• Haemodynamic monitoring
• Appropriate Laboratory investigations
'Freezing' (Targeted Temperature Management) Using established cooling strategies and existing protocols
• Maintain a constant targeted T° between 32 - 36°C for > 24 hours• Monitor glucose, electrolytes (especially K, Ca, Mg, Po�),
and Haemodynamic status• Rewarm at 0.25°C per hour
• Avoid rebound hyperthermia (T° > 37.5°C)
Glucose Control• Maintain blood glucose at
8 - 10 mmol/l • Avoid hypoglycaemia
Head / Neuro Evaluation• Treat seizures aggressively• Consider EEG monitoring• Consider brain imaging
• Delay prognostication for at least 72 hours post normothermia
UNRESPONSIVE
RESPONSIVE
A
B
C
D
E
F G
H
POST CARDIAC ARREST CARE(Return of Spontaneous Circulation)
2015 2015
www.resuscitationcouncil.co.za