atypical amyloidosis with macroglossia
TRANSCRIPT

616-003.821 : 616. 313-007.61
ATYPICAL AMYLOIDOSIS WITH MACROGLOSSIA.
W. G. BARNARD, F. B. SMITH and J. L. WOODHOUSE. London County Council Central Histological Laboratory,
Dulwich Hospital and Royal Infirmary, Preston.
(PLATES LX.-LXII.)
THE association of an atypical amyloidosis with macroglossia was first described by Lubarsch (1929) and Pick (1931). The two cases here described showed the typical lesions-amyloid infiltration of the muscle of the tongue, cesophagus and heart and of the skeletal muscles and other connective tissues.
Case I. History. (J. L. W.).
A man aged 52 years, a worker in fancy leather, fist noticed a swelling of the tongue in J d y 1934. It was not associated with pain but did give rise to bouts of dyspncea. Septic teeth were extracted. His blood Wassermann, both at this time and subsequently, was negative. The swelling slowly progressed. In November 1935 the condition was considered to be either an cedematous or an angeiomatous lymphatic swelling. From this time he was treated a t intervals by radiotherapy. Two years later he was admitted to hospital complaining of rheumatism, bronchitis, anorexia and exhaustion. He looked ill and had prominent cheeks due to the lateral borders of the tongue extending beyond the alveolar borders; the tongue also protruded so that he was unable to close either his jaws or his lips. The submental region was prominent. The tongue was uniformly enlarged, almost completely immobile and abnormally pale. It was neither furred, ulcerated nor sore. The patient was thin and in various parts, especially over the right forearm, the deep fascia was granular, the granules averaging 2 mm. and being closely packed in the affected areas. His speech was dysarthric and he could only swallow fluids and semi-solids. His " rheumatism " was indefinite and appeared to be muscular rather than articular. The respiratory trouble was due t o chronic infection of the upper respiratory tract with nasal obstruction and embarrassment of respiration. This was more marked at night as he could not breathe easily through his mouth. No abnormality was detected in his urine (ward test only). There was never any complaint of dysuria or frequency and he was apyrexial until some 36 hours before his death when his temperature suddenly rose to about 102" F. He died in May 1937, 16 weeks after admission.
311
312 BARNARD, SMITH AND WOODHOUSE
Necropsy (J. L. W.)
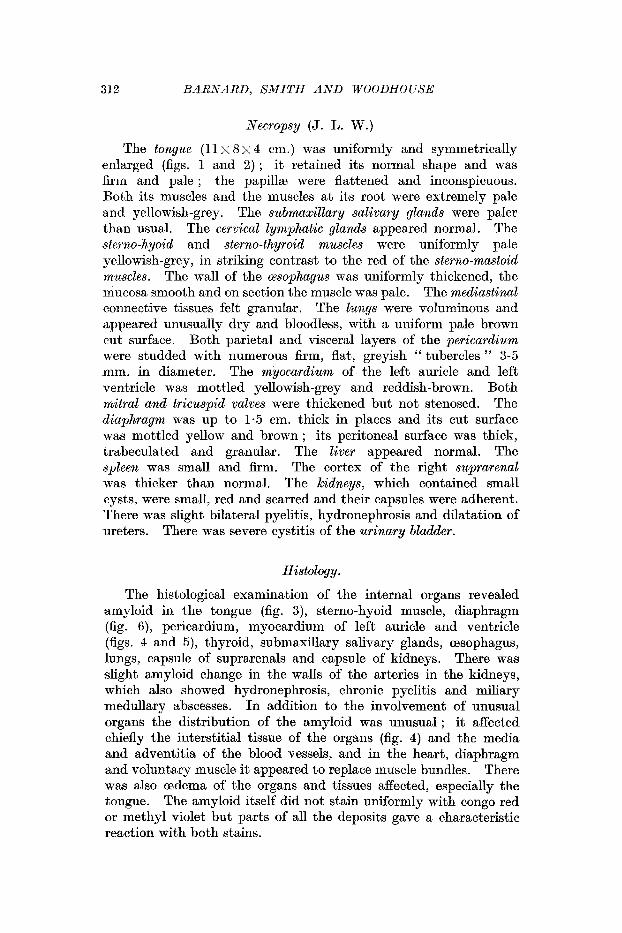
The tongue (11 x 8 x 4 em.) was uniformly and symmetrically enlarged (figs. 1 and 2) ; it retained its normal shape and was firm and pale ; the papilh were flattened and inconspicuous. Both its muscles and the muscles at its root were extremely pale and yellowish-grey. The submaxillary salivary glands were paler than usual. The cervical lymphatic glands appeared normal. The sterno-hyoid and sterno-thyroid muscles were uniformly pale yellowish-grey, in striking contrast to the red of the sterno-mastoid muscles. The wall of the @sophagus was uniformly thickened, the mucosa smooth and on section the muscle was pale. The mediastinal connective tissues felt granular. The lungs were voluminous and appeared unusually dry and bloodless, with a uniform pale brown cut surface. Both parietal and visceral layers of the pericardium were studded with numerous firm, flat, greyish " tubercles " 3-5 mm. in diameter. The myocardium of the left auricle and left ventricle was mottled yellowish-grey and reddish-brown. Both mitral and tricuspid valves were thickened but not stenosed. The diaphragm was up to 1.5 em. thick in places and its cut surface was mottled yellow and brown ; its peritonea1 surface was thick, trabeculated and granular. The liver appeared normal. The spleen was small and firm. The cortex of the right suprarenal was thicker than normal. The kidneys, which contained small cysts, were small, red and scarred and their capsules were adherent. There was slight bilateral pyelitis, hydronephrosis and dilatation of ureters. There was severe cystitis of the urinary bladder.
Histology.
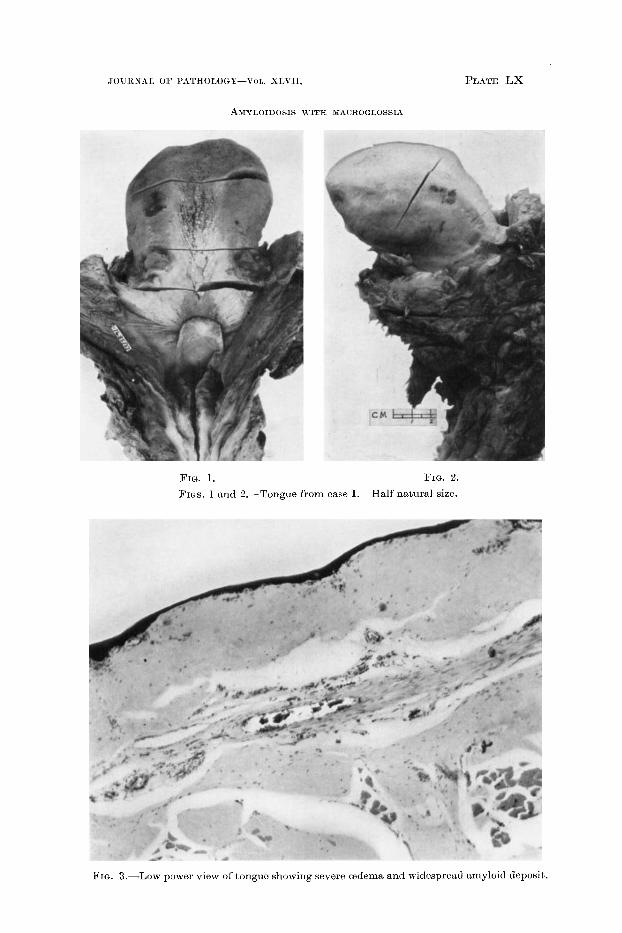
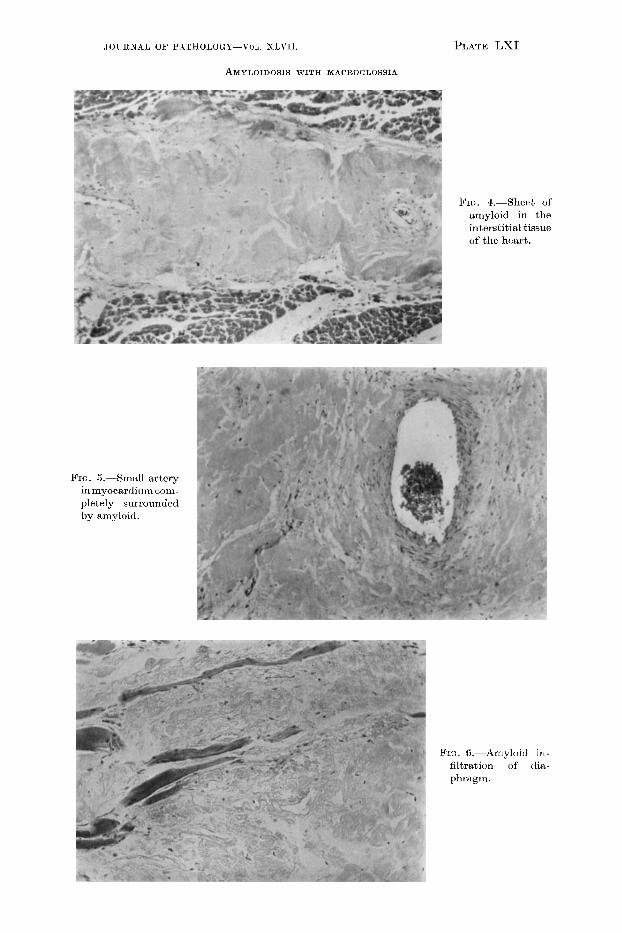
The histological examination of the internal organs revealed amyloid in the tongue (fig. 3), sterno-hyoid muscle, diaphragm (fig. 6), pericardium, myocardium of left auricle and ventricle (figs. 4 and 5), thyroid, submaxillary salivary glands, cesophagus, lungs, capsule of suprarenals and capsule of kidneys. There was slight amyloid change in the walls of the arteries in the kidneys, which also showed hydronephrosis, chronic pyelitis and miliary medullary abscesses. In addition to the involvement of unusual organs the distribution of the amyloid was unusual ; it affected chiefly the interstitial tissue of the organs (fig. 4) and the media and adventitia of the blood vessels, and in the heart, diaphragm and voluntary muscle it appeared to replace muscle bundles. There was also cedema of the organs and tissues affected, especially the tongue. The amyloid itself did not stain uniformly with congo red or methyl violet but parts of all the deposits gave a characteristic reaction with both stains.
JOURNAL Oh’ l’ATHOLOGT--T’or,. XLVI1.
AMYLOIDOSIS WITH MACROGLOSSIA
PLATE LX
FIG. 1. FIG. 2.
FICJS. I and -“.-Tongue from case I. Half natural size.
FIG. 3.-Low power view of tongue showing severe cedema and widespread arnyloid deposit.
J 0 UllNAL Oh' ~"~THOI,OC;Y--V(JL. XLVII.
AMYLOIDOSIS WITH MAGKOGLOSSIA
PLATE LXI
Fm. 4.-shert of aniyloid in the interstitial tissue of tlic h a r t .
FIG. S.-Small artory inmyocardium corn- pletely surrounded by amyloid.
PIG. G.--AmyIoid in- fihation of dia- phragm.
A M YLOIDOSIS W I T H MACROGLOSSIA 313
Case 11. (F. B. S.) History.
J. G. (36/1482), a married man aged 54, a furniture remover, was admitted to hospital complaining of asthenia, dyspncea and swelling of the legs, hands and scrotum for two months. A year previously he had injured the soft parts of the back, which was still slightly painful. Three years previously he had had pleurisy.
On examination the facies was distinctive by reason of painless swelling under the chin and thick lips ; the tongue was enlarged and its movements limited and speech was muffled ; the jaw dropped slightly to accommodate the tongue. Blood pressure lOS/SS; pulse 80; no pyrexia; urine normal but reduced in amount; blood urea 45 mg. per 100 c.c. ; Wassermann and Kahn reactions of blood serum negative ; hzmoglobin 60 per cent., colour index 1.1, moderate variability of red cells with a mean diameter of 7 .6 p, normal leucocytes. This suggestion of pernicious anzmia had not been investigated further when death occurred from heart failure and pulmonary cedema.
Abdomen much distended but not by free fluid.
Necrops y . Prominent features post mortem were (1) pulmonary cedema and
dilation of the right heart, ( 2 ) thickening of the ileum and esophagus and dilation of the ileum, (3) uniform enlargement of the tongue. Tongue is smooth and an inch longer and an inch deeper at the base than the average ; cut surface of mesial section glossy, pale and suggests cedema. Ileum thick, dilated and marked by ivory- yellow mottling and streaks visible through the serous coat. Thickening affects all coats, and, with the dilation, accounts for the swollen abdomen ; circumference of ileum varies from 4 to 5 inches. Gsophagus shows similar thickening and colour. Stomach and colon normal. Heart weighs 340 g. ; muscle pale and cloudy, with milky opacity under the pericardium. Distinctive features absent from other viscera.
Histology. Blocks were taken from the tongue (fig. 7 ) , heart muscle,
cesophagus, ileum (figs. 8 and 9), liver and kidneys and sections stained by hamalum and eosin, van Gieson’s stain, IKallory’s connective tissue stain, congo red, methyl violet and acetic acid, and crystal violet and acetic acid.
The thickening of the tongue, cesophagus and ileum is due to amyloid infiltration in the form of (1) uniform deposits in the capillaries and small arteries (fig. 7 ) , ( 2 ) nodal deposits in the interstitial framework and perivascular sheaths of the larger arteries, (3) replacement of most of the striped niuscle of the tongue and much of the striped and unstriped muscle of the cesophagus and ileum (figs. 8 and 9), (4) interstitial and vascular infiltration in the heart, but muscle fibres normal, (5) scanty deposits in portal vessels of liver, but kidneys normal.
314 BARNARD, SMITH -4ND WOODHOUSE
Discussion.
After the histological examination had shown the true nature of the condition in the first case, the patient’s wife was seen and she volunteered the information that at about the same time as the enlargement of the tongue was noticed her husband complained of pain and heaviness in his legs. When walking he had to rest a while every now and then but when these symptoms had passed off he could continue. This intermittent claudication was noted by Parkes Weber in the first case described in this country (Parkes Weber et al., 1937). The diagnosis of their case was made on operation material removed from an enlarged tongue. In addition to their own they discuss 10 cases culled from the literature. In all these cases the distribution of the amyloid is similar, the media and adventitia of the arteries and the interstitial tissue of organs being chiefly affected. As far as the interstitial tissue is concerned the appearance is that which would be found if the organ had been infiltrated by a coagulable fluid which had coagulated. The muscle bundles are separated by the intervening amyloid deposit ; they atrophy and finally disappear so that they seem to have been replaced by amyloid material. There is no obvious inflammatory focus in these cases comparable to that found in the more usual cases of generalised amyloidosis. Nothing is known as to its cause nor as to any factors which might influence its development.
We have to thank Sir Frederick Menzies, Dr Roberts and Dr Rayner for permission to publish and make use of the notes in these cases.
REFERENCES.
LUBARSCH, 0. . . . . . Arch. path. Anut., 1929, cclxxi. 867. PICK, L. . . . . . . Klin. Wschr., 1931, x. 1515. WEBER, F. PARKES, CADE, S., Quart. J . Med., 1937, vi. 181.
STOTT, A. W., AND PULVER- TABT, R. J. V.
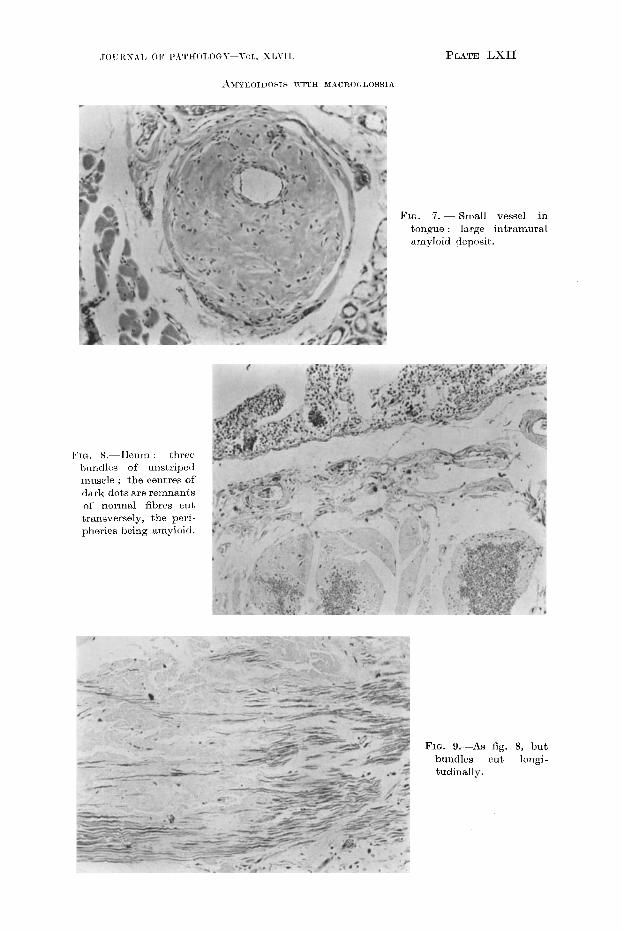
PLATE LXII
FIG. 7. - Rniall vessel in tonque : large intramural amyloirl deposit.
FIG. 8.-Ilcurn : three hundlcs of unstriped muscle : the centres of dark dots are remnants of normd fibres cut transversely, the peri- pheries being amyloid.
FIG. 9.-As fig. 8, but bundles cut longi- tudinally.