atorvastatin is more effective than pravastatin in preventing recurrent cardiac events
Post on 25-Nov-2016
214 views
TRANSCRIPT

ARTICLE IN PRESS
Evidence-Based Healthcare & Public Health (2004) 8, 296–297
KEYWORDAcute corosyndrome;LDL;AtorvastatPravastatinSecondarypreventionCardiovascdiseases;Randomisecontrolled
1744-2249/$ - sdoi:10.1016/j.e
$Abstractedcoronary syndro
www.elsevier.com/locate/ebhph
EVIDENCE-BASED CLINICAL PRACTICE
Atorvastatin is more effective than pravastatin inpreventing recurrent cardiac events$
Snary
in;;
;ular
dtrial
ee front matter & 2004hbc.2004.08.007
from: Cannon CP, Braumes. New England Jou
Summary
Question What are the effects of high-dose atorvastatin compared with standard-dose pravastatin in people with acute coronary syndrome?
Study design Double-blind randomised controlled trial.
Main results High-dose atorvastatin significantly reduced the combined risk ofdeath or major cardiovascular events compared with standard-dose pravastatin at 2years (reduction in risk: 16%, 95%CI 5 to 26%). High-dose atorvastatin alsosignificantly reduced risk of revascularisation, unstable angina, death or myocardialinfarction compared with pravastatin (see Results table). There were no significantdifferences in risk of stroke between groups. High-dose atorvastatin produced lowermedian LDL-cholesterol levels compared with pravastatin (atorvastatin vs. pravas-tatin: 62mg/dL n 95mg/dL, p ¼ o0:001). People with LDL-cholesterol levels4125mg/dL responded better to atorvastatin than people with lower LDL-cholesterol levels (reduction in hazard ratio for LDL-cholesterol 4125mg/dL nLDL-cholesterol o125mg/dL: 34% n 7%, p ¼ 0:02).
Authors’ conclusions High-dose atorvastatin is more effective than standardtherapy for people with acute coronary syndrome. The study indicates that optimallevels of low-density lipoprotein are lower than previously predicted.& 2004 Elsevier Ltd. All rights reserved.
Study parameters
Question
What are the effects of high-dose atorvastatin compared with standard-dose pravastatin in people withacute coronary syndrome?
Study design
Double-blind randomised controlled trial.
Setting
349 centres in 8 countries; November 2000 to December 2001.
Elsevier Ltd. All rights reserved.
nwald E, mccabe CH et al. Intensive versus moderate lipid lowering with statins after acuternal of Medicine 2004; 350: 1495–1504.
ARTICLE IN PRESS
EVIDENCE-BASED CLINICAL PRACTICE 297
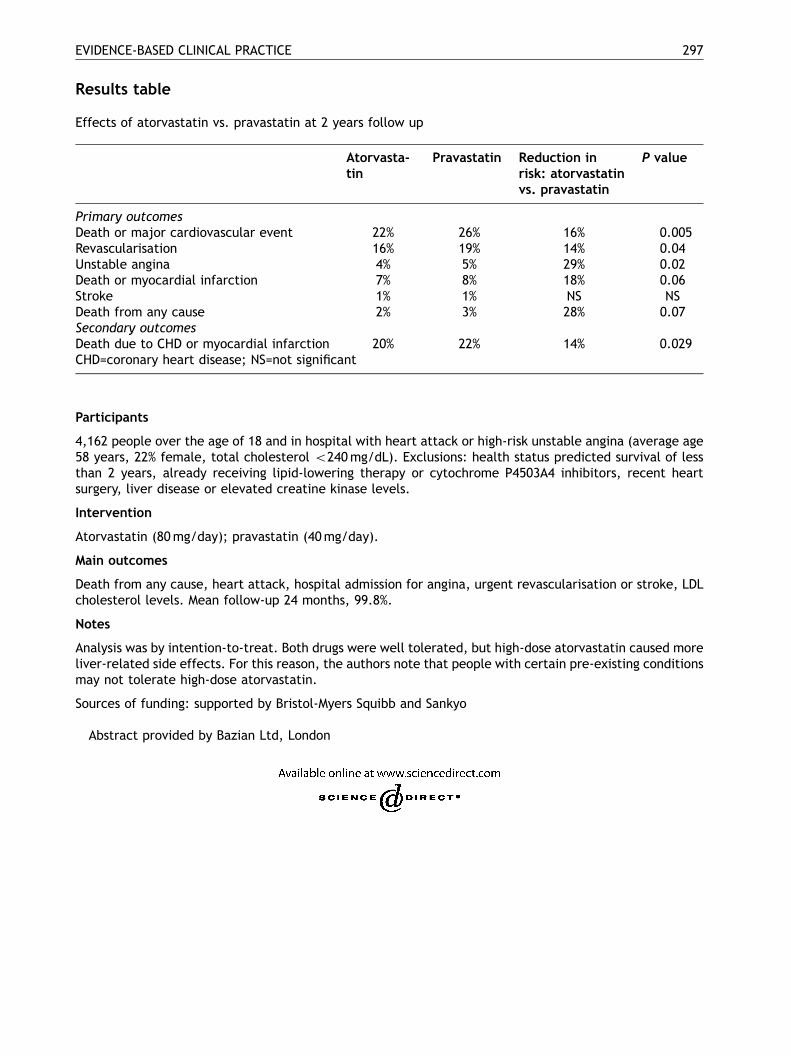
Results table
Effects of atorvastatin vs. pravastatin at 2 years follow up
Atorvasta-tin
Pravastatin
Reduction inrisk: atorvastatinvs. pravastatinP value
Primary outcomes
Death or major cardiovascular event 22% 26% 16% 0.005 Revascularisation 16% 19% 14% 0.04 Unstable angina 4% 5% 29% 0.02 Death or myocardial infarction 7% 8% 18% 0.06 Stroke 1% 1% NS NS Death from any cause 2% 3% 28% 0.07 Secondary outcomes Death due to CHD or myocardial infarction 20% 22% 14% 0.029 CHD=coronary heart disease; NS=not significantParticipants
4,162 people over the age of 18 and in hospital with heart attack or high-risk unstable angina (average age58 years, 22% female, total cholesterol o240mg/dL). Exclusions: health status predicted survival of lessthan 2 years, already receiving lipid-lowering therapy or cytochrome P4503A4 inhibitors, recent heartsurgery, liver disease or elevated creatine kinase levels.
Intervention
Atorvastatin (80mg/day); pravastatin (40mg/day).
Main outcomes
Death from any cause, heart attack, hospital admission for angina, urgent revascularisation or stroke, LDLcholesterol levels. Mean follow-up 24 months, 99.8%.
Notes
Analysis was by intention-to-treat. Both drugs were well tolerated, but high-dose atorvastatin caused moreliver-related side effects. For this reason, the authors note that people with certain pre-existing conditionsmay not tolerate high-dose atorvastatin.
Sources of funding: supported by Bristol-Myers Squibb and Sankyo
Abstract provided by Bazian Ltd, London