asthma - suli pharma · risk factors for severe acute asthma include 1- a history of previous...
TRANSCRIPT
Asthma
1
DEFINITION
• It is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role.
• Airflow Obstruction is often reversible either spontaneously or with treatment.
2
Aetiology
• The two main causes of asthma symptoms are airway hyperresponsiveness and bronchoconstriction.
• Hyperresponsiveness is an increased tendency of the airway to react to stimuli or triggers to cause an asthma attack.
• Bronchoconstriction is a narrowing of the airways that causes airflow obstruction.
3
Aetiology
Examples of asthma triggers • Environmental irritant causing seasonal asthma , like
pollen from grass &plant. • Allergen found in house dust, carpet, smoking,
fungi, and animal dander from cat &dog. • Food (egg, chocolate) . • Occupational factors (working environment) e.g
flour causing occupational asthma in bakers.
4
Aetiology
• Emotional stress • Physical activity ( exercise-induced
asthma) • Cold air • Drug induced asthma, including beta
blockers, aspirin and other nonsteroidal anti- inflammatory drugs.
5
6
Pathophysiology
Asthma can be classified according to the underlying pattern of airway inflammation with the presence or absence of eosinophils in the airways (eosinophilic vs. non- eosinophilic) into
1) Extrinsic asthma: known also as allergic asthma or eosinophilic asthma, mean the stimuli coming from external environment. It is more common in children associated with genetic predisposition and precipitated by known allergen.
7
2) Intrinsic asthma: Stimuli come from internal environment, developed in adulthood with symptoms triggered by non allergen factors such as viral infection.
• When asthma attacks related to allergies, the Ab (IgE) is formed after exposure to allergen (IgE formed in plasma cells in a no. of area in the body including the lung).
8
• IgE attach to the surface of mast cells in the lung tissue & through series of reactions allowing the mast cells to release the mediator of asthma, e.g. histamine,leukotrienes, prostaglandins , bradykinin, and prostaglandin-generating factor of anaphylaxis that attract eosinophils and neutrophils.
9
• Eosinophils release various inflammatory mediators such as leukotriene C4 (LTC4) and platelet-activating factor (PAF).
• all cause hypertrophy and hyperplasia of bronchial smooth muscle, mucus gland hypertrophy leading to excessive mucus production and airway plugging, airway oedema , acute bronchoconstriction and impaired mucociliary clearance .
10
Clinical manifestation
Wheezing
Dyspnea
Chest tightness
Less commonly coughs with production of a thick mucoid sputum
Cyanosis
Tachycardia
Agitation
11
Diagnosis
Lung function test
1-spirometer
• Measures the volume of air exhale against time
• Forced Expiratory Volume or (FEV1) is the amount of air exhale in the first second .
• Forced Vital Capacity or (FVC) is the total amount of air exhale until all air is expired .
• Reading is affected by age, gender and height.
12
2- peak flow meter
• by a peak flow meter, the patient can be self assessed for improvement or deterioration in the disease as well as the effectiveness of treatment.
• The peak flow meter measures peak expiratory flow (PEF) rate.
• Peak Expiratory Flow Rate (PEFR) is the maximum rate of air breathed out as hard as possible (after a full breath taken in).
13
Treatment of chronic asthma
Goal of therapy
• Maintain normal activity levels including exercise.
• Maintain near normal pulmonary function rate.
• Prevent chronic &troublesome symptoms e.g. coughing or shortness of breath).
• Prevent recurrent exacerbation of asthma.
• Avoid adverse effects from asthma medication.
14
Non- medical treatments
• Involves reduce exposure to pollen &allergen by keeping window closed during pollen season ,use air conditioner ,eliminate cigarettes smoking, prevent exercise in cold dry environment, better in warm moist area.
15
Treatment of chronic asthma • It depends upon frequency & severity of the
patient symptoms. The preferred route of administration of agents is used by inhalation. This allows the drugs to be delivered directly to the airways in smaller doses &with fewer SE than systemic route.
• Inhaled bronchodilators have a faster onset of action than systemic route .Treatment should be in stepwise according to severity of the case &response to current treatment.
16
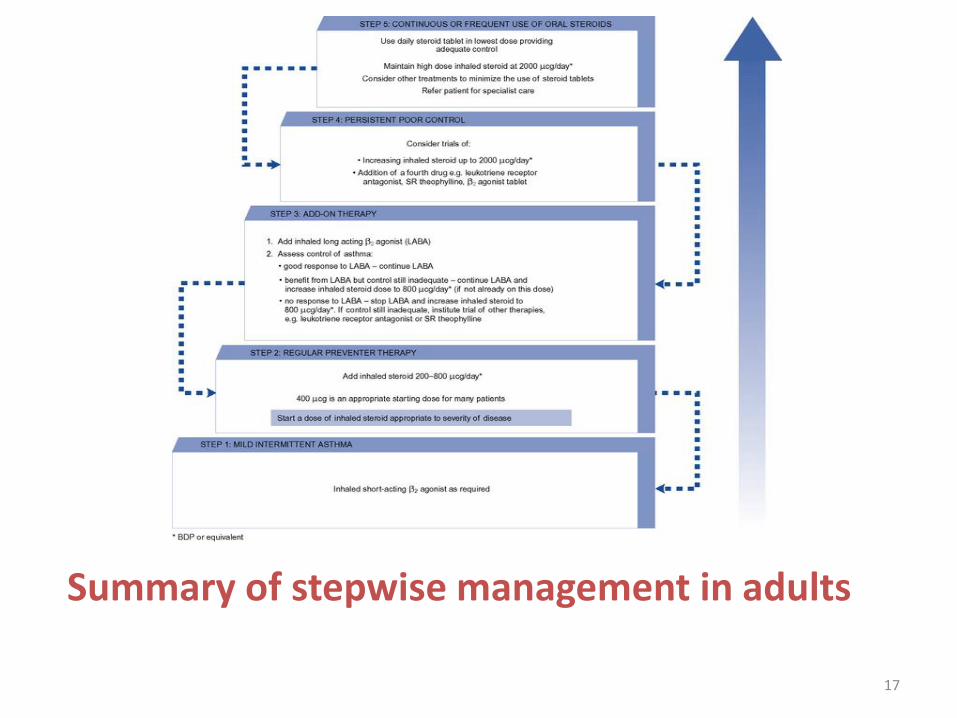
Summary of stepwise management in adults
17
Short acting ß2 agonist: • They are the mainstay of asthma management.
Salbutamol and Terbutaline are selective ß2-agonist and have few ß1- mediated SE, particularly cardiotoxicity.
• ß2-receptors present in myocardial tissue, so cardiovascular stimulation result in tachycardia and palpitation when such drug used in high doses.
18
• It produces bronchodilation by relaxing bronchial smooth muscle through activation of cyclic adenosine monophosphate CAMP( increase cellular level of CAMP )i.e. it activates adenylcyclase ,the enzyme responsible for the conversion of ATP----- CAMP.
19
• Inhaled short acting ß2-agonist is the first line agent in management of asthma, used as required for symptomatic relief of shortness of breath & wheezing .
• The onset of action of short acting B2 agonist is rapid within 5 minutes &reaches maximal effect in 15-30 minutes, duration of action in 4-6 hours.
20
Corticosteroids Inhaled corticosteroids( Beclometasone diproprionate or budesonide, ciclesonide, fluticasone and mometasone) • Steroid inhaler can reverse bronchospasm which
doesn't respond to short acting ß 2-agonist.It indicated in the severe form of chronic asthma. Maximum dose used is 1.5-2mg a day.
• Local adverse effects from ICSs include oropharyngeal Candidiasis and dysphonia that are dose dependent. The use of a spacer device can decrease oropharyngeal deposition and thus decrease the incidence and severity of local side effects.
21
• Systemic adverse effects can occur with any of the ICSs given in a sufficiently high dose include growth suppression in children, osteoporosis, and adrenal insufficiency and crisis.
22
Oral corticosteroids
• Oral corticosteroids (prednisolone) can control symptoms not achieved with maximum dose of inhaled bronchodilators & steroids .
• Patient on continuous oral steroids, should be placed on short acting agent & should placed on the lowest dose possible mainly single morning dose to minimize adrenal suppression.
23
Long Acting inhaled B2 Agonist
• long acting B2 Agonist: e.g. salmeterol and formoterol used twice daily.
• They have long duration of action therefor should not be used for acute of asthma.
• Patients need to be counseled to continue to use their short acting inhaled B2 agonist for acute exacerbations while receiving the long acting inhaled B2 agonists.
24
Oral B2 agonist ((tab.or syrup)
• Oral rout has slow onset of action and side effects are more pronounced with the oral therapy such as tachycardia and hand tremor.
25
Methylxanthin (Theophylline )
• For treatment of chronic asthma a slow released forms should be used. It is useful as a single night time dose for nocturnal symptoms.
• Theophyline has a narrow therapeutic index.
• The clearance of theophyline is effected by many factors like cigarettes ,viral pneumonia ,heart failure, corpulmonale & liver cirrhosis .The clearance also affected in patients taking enzyme inhibitor drug like cimetidine or enzyme inducer drugs like phenytoin.
26
Methylxanthines may produce bronchodilation through numerous mechanisms, including
1- inhibition of phosphodiesterase thereby increasing cAMP levels and inhibition of calcium ion influx into smooth muscle.
3- prostaglandin antagonism.
4- stimulation of endogenous catecholamines.
5- inhibition of release of mediators from must cells and leukocytes.
27
Side effects of theophylline
Side effects of theophylline is related to its serum concentration level.
The mild side effects such as nausea &vomiting are seen at concentrations as low as 13 mg /L, but are more common over 20mg/L.
cardiac effect tachycardia & arrhythmias are usually seen at conc .of 40 mg /L .
CNS effect like irritability ,insomnia &seizure occur when serum level greater than 50mg/L.
28
• Therefore the dose of theophylline should adjusted to keep the plasma level within a therapeutic range of 10-20 mg / L .
• Theophylline are available in injection, tablets &syrup dosage form.
29
Sodium cromoglicate and Nedocromil sodium • Sodium Cromoglicate and Nedocromil sodium are
pharmacologically similar. • They are classified as must cell stabilizers, and the
principal difference appears to be potency, with 4 mg nedocromil by MDI equivalent to 10 mg Sodium cromoglicate membrane stabilizer.
• It is effective in exercise induced asthma . • Cough and wheeze have been reported following
inhalation of each, and bad taste and headache following nedocromil are reported.
30
Leukotriene receptor antagonists
• leukotriene receptor antagonists, e.g. Montelukast& Zafirlukast (oral form ).
• less effective than long acting B2 agonist in controlling asthma when added to inhaled corticosteroid.
• It is effective in aspirin-induced asthma.
• Side effects of leukotriene receptor antagonist include headache, diarrhea, dizziness. Rarely acute hepatitis associated with zafirlukast.
31
Anti-IgE monoclonal antibodies
• Omalizumab is the first anti- IgE antibody approved for the treatment of asthma not well controlled on high dose of inhaled corticosteroid.
• Omalizumab is administered subcutaneously and has a slow absorption rate; peak serum concentration is achieved in 3 to 14 days.
32
Severe acute asthma
Is a dangerous condition that needs hospitalization &immediate emergency treatment.
It occurs when bronchospasm progressed to a state where the patient is breathless at rest &has a degree of cardiac stress (the patient can not lie down).
Breathing can become rapid >30breaths / min, the patient becomes fatigue, cyanosed & confused.
33
Risk factors for Severe acute asthma include
1- A history of previous severe asthma exacerbation ( e.g. hospitalizations, intubations, or hypoxic seizures).
2- Complicating illness ( e.g. cardiac disease, diabetes, or psychosis)
3- Use of more than two canisters per month of short acting inhaled B2 agonist.
4- Current intake of oral corticosteroids or recent withdrawal from oral corticosteroids.
34
The primary therapy of acute exacerbation is pharmacologic which includes inhaled short acting B2 agonists and, depending on the severity, systemic corticosteroids and o2.
- B2 agonists
An inhaled ß2-agonist is considered the first choice for acute asthma due to its potency &rapidity of action.
ß2-agonist is administered by metered dose inhaler . With severe symptoms ,nebulizers are preferable than inhalers (they permit a high dose).
35
• High doses of inhaled B2 agonist therapy can produce hypokalemia, hyperglycemia, tachycardia, and cardiac dysrhythmias.
- Oxygen Oxygen is administered to achieve an oxygen
saturation of 92% or more. - Corticosteroids Oral corticosteroids also given in acute attack. During
exacerbation of asthma, a short course of high dose can be used.
Intravenous hydrocortisone should only be require if the patient cannot take oral medication.
36
- Aticholinergics
If life threating features are present nebulized salbutamol with ipratropium are recommended.
37
Alternative therapies Methylxanthin (Aminophylline)
A loading dose of Aminophylline can be given by i.v. rout over a period of 20-40 minute in order to give serum level of 10mg / L, followed by constant infusion of the drug.
Magnesium sulfate
Magnesium sulfate is a moderately potent bronchodilator is similar to theophylline, producing relaxation of smooth muscle and central nervous system depression.
The adverse effects of magnesium sulfate include hypotension, facial flushing, sweating, nausea, and respiratory depression.
Patients have required dopamine to treatment.
38
Ketamine
Ketamine has been recommended for rapid induction of anesthesia in patients with asthma who require intubation and mechanical ventilation.
Adverse effects of ketamine include an increase in heart rate, arterial blood pressure, cerebral blood flow because of sympathetic effects and delirium.
39