assessment of premature ejaculation …€¦ · 2 assessment of premature ejaculation and erectile...
TRANSCRIPT

2
ASSESSMENT OF
PREMATURE EJACULATION
AND ERECTILE
DYSFUNCTION
Dr Michael Gillman
St Andrews Hospital Wickham Terrace Spring Hill
Mater Private Clinic, South Brisbane
Shore St West Medical Centre, Cleveland

3
Disclosure Slide
Advisor Lilly Australia Cialis
Advisor Pfizer Australia Viagra / Caverject
Advisor Bayer Levitra
Advisor Andrology Australia Erectile Dysfunction Board
Advisor Janssen Cilag Priligy
Advisor Sanofi Adventis Xatral
Advisor CSL / Astellis Flomaxtra
4
Premature Ejaculation
• A common sexual disorder
• Usually affects younger couples
• May accommodate problem with second attempt while still young enough to have a short refractory period
• Higher levels of intercourse related anxiety
• Greater patient and partner impairment in intercourse satisfaction
• Greater impairment in relationship satisfaction
Premature Ejaculation (PE)
• ISSM definition of PE:
– intravaginal ejaculatory latency time (IELT) <1 min
– inability to delay ejaculation- lack of control
– negative impact on man and partner- distress
• either lifelong or acquired (often associated with erectile
dysfunction)
• psychological and physiological components
Diagnof Premature Ejaculation
McMahon et al, 2008
Time to
ejaculation
Inability to
delay
ejaculation
Negative
personal
consequences + +
7
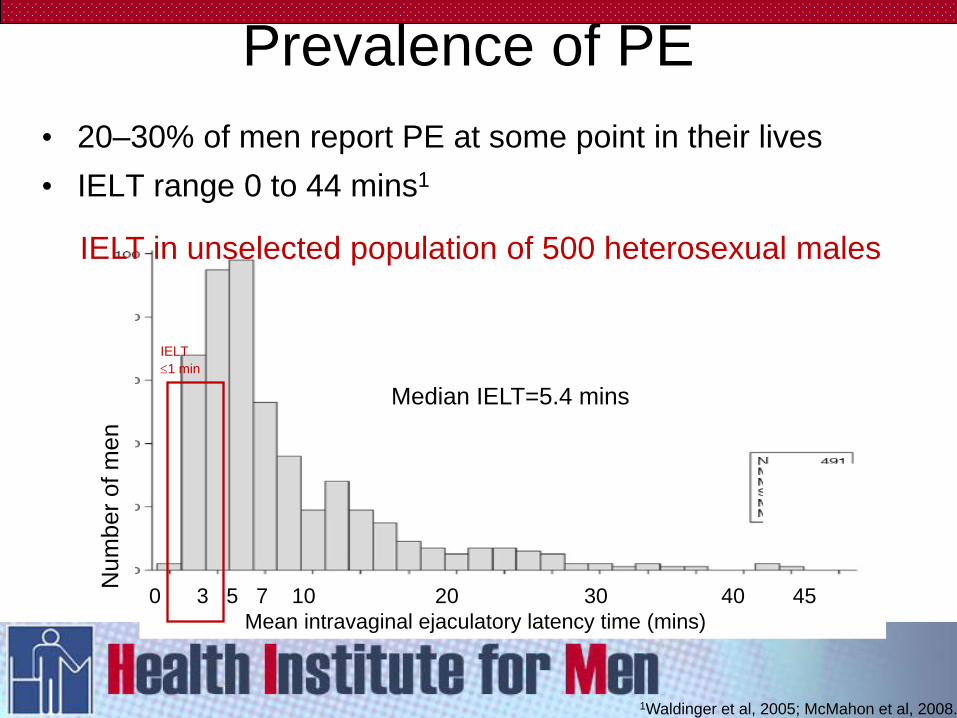
• 20–30% of men report PE at some point in their lives
• IELT range 0 to 44 mins1
1Waldinger et al, 2005; McMahon et al, 2008.
Median IELT=5.4 mins
IELT in unselected population of 500 heterosexual males
IELT
1 min
0 3 5 7 10 20 30 40 45
Mean intravaginal ejaculatory latency time (mins)
Num
ber
of m
en
Prevalence of PE
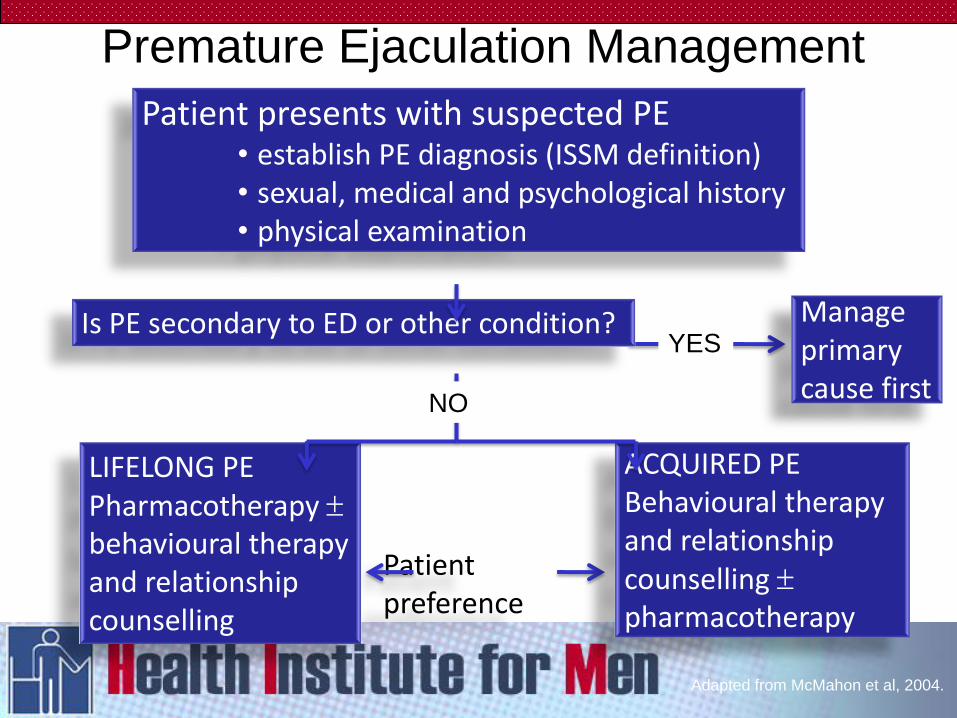
Premature Ejaculation Management
YES Manage primary cause first
Patient preference
Adapted from McMahon et al, 2004.
Patient presents with suspected PE • establish PE diagnosis (ISSM definition) • sexual, medical and psychological history • physical examination
LIFELONG PE Pharmacotherapy behavioural therapy and relationship counselling
NO
ACQUIRED PE Behavioural therapy and relationship counselling pharmacotherapy
Is PE secondary to ED or other condition?
PE pharmacotherapy:
• serotonin and 5-HT receptors are involved in ejaculation1,2
1. Donatucci, 2006. 2. Giuliano & Clement, 2006. 3. Dapoxetine Product Information. Janssen-Cilag: 2009.
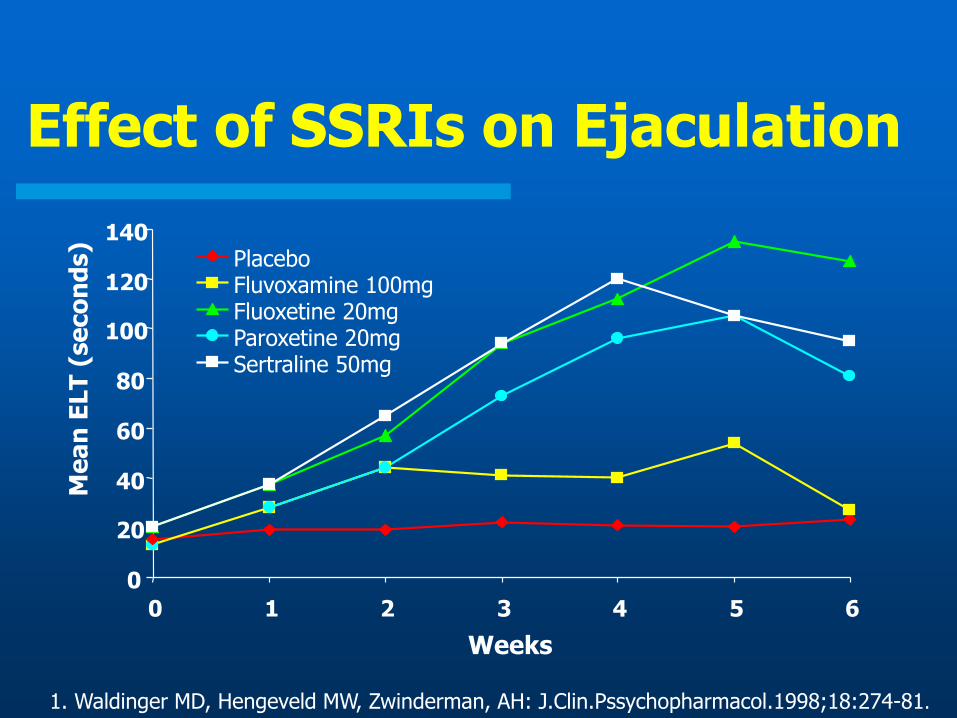
Effect of SSRIs on Ejaculation
1. Waldinger MD, Hengeveld MW, Zwinderman, AH: J.Clin.Pssychopharmacol.1998;18:274-81.
0
20
40
60
80
100
120
140
0 1 2 3 4 5 6
Weeks
Me
an
ELT
(se
co
nd
s)
Placebo Fluvoxamine 100mg Fluoxetine 20mg Paroxetine 20mg Sertraline 50mg
• Effective
• Daily paroxetine - 8.8 fold increase in IELT
• “On demand” clomipramine – 4.6 fold increase
• Safe
• Usually well tolerated
• Minor, self limiting adverse effects of SSRIs ...
• Fatigue, yawning, mild nausea, loose stools or perspiration
Effective, Safe, Well Tolerated …
13
PE management plan and follow-up
Management plan
Involve patient and partner
• partner may influence choice of management
Consider SSRI treatment in combination with behavioural
therapy
Follow up
4 weeks or 6 doses after starting therapy; check…
• efficacy
• dose titration
• side effects
1. Dapoxetine Product Information. Janssen-Cilag: 2009.
Summary Premature Ejaculation (PE)
• PE is common and distressing
• Behavioural therapies are effective in some cases
• If lifelong PE requires pharmacological treatment
• Combined medical and psychological treatment is most
effective strategy for PE
16
ASSESSMENT OF ERECTILE
DYSFUNCTION
Dr Michael Gillman
St Andrews Hospital Wickham Terrace Spring Hill
Mater Private Clinic, South Brisbane
Shore St West Medical Centre, Cleveland
17
IMPOTENCE
Impotence is the inability to
achieve or sustain an erection
sufficient for the sexual needs
of the man or his partner
18
ERECTILE DIFFICULTIES
40% at age 40
50% at age 50
60% at age 60
70% at age 70
Do Men Really Care???
How many of your male patients book
appointments to discuss erection problems

20
21
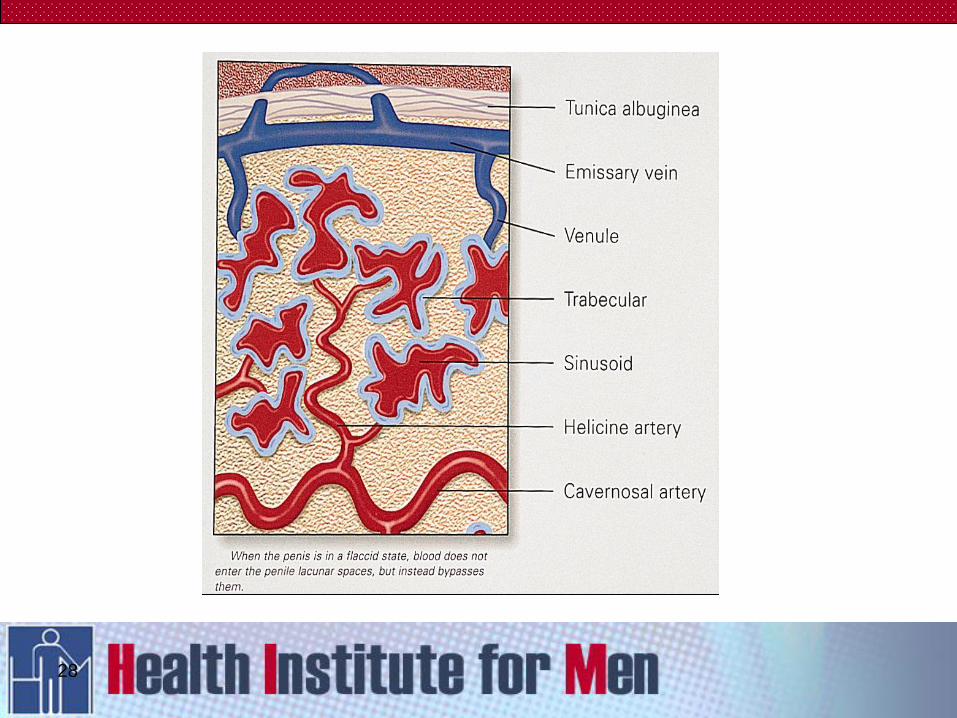
23
Erectile Dysfunction
History – Main Points
Duration of onset of problem.
Quality of all erections ( Spontaneous and
sexual )
Relationship issues
Previous Treatments including Newspaper
Commercial Clinics
24
Erectile Dysfunction
History – Main Points
>70% have an organic component
Assume that most men have both
Organic and Psychogenic
25
Psychogenic
Mainly Performance anxiety
Relationship Difficulties
Financial Difficulties
etc
26
27
28
Diabetes Hypertension
The Deadly Quartet
Obesity Dyslipidemia
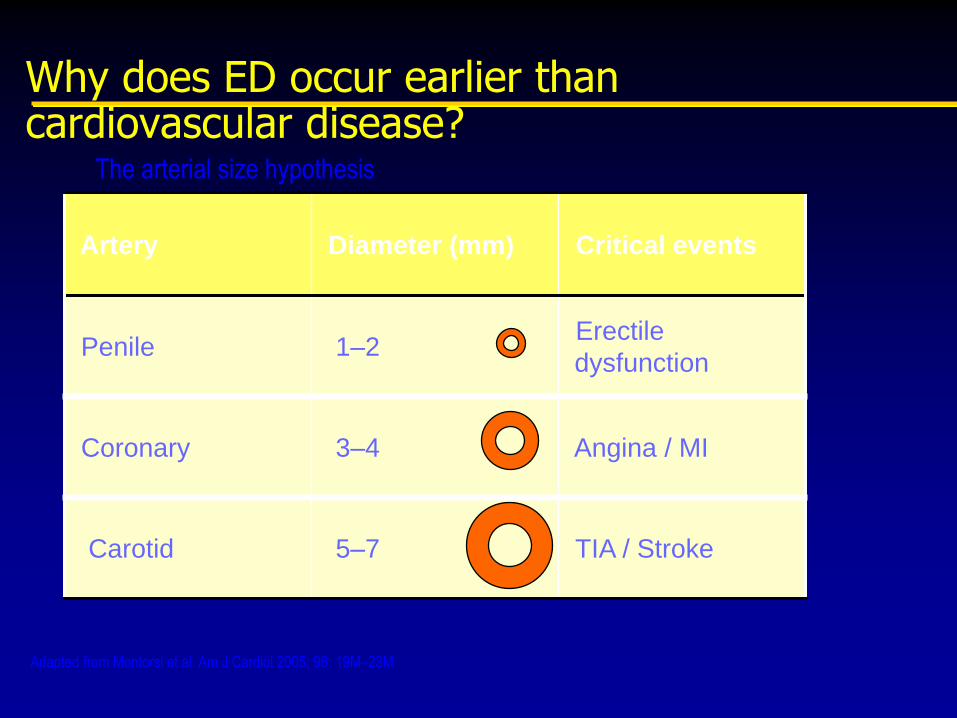
Why does ED occur earlier than cardiovascular disease?
Artery Diameter (mm) Critical events
Penile 1–2 Erectile
dysfunction
Coronary 3–4 Angina / MI
Carotid 5–7 TIA / Stroke
Adapted from Montorsi et al. Am J Cardiol 2005; 96: 19M–23M
The arterial size hypothesis
31
Examination
Examination
BP
Height Weight and waist circumference
Penile shaft for fibrosis
Testicles
Vascular system AAA, peripheral
pulses
? Prostate with informed consent
32
Investigations
E/LFTs
HDL/LDL
Testosterone ( LH and PRL if low )
TSH
Urine WTU
?PSA
33
34
Testosterone and ED ??
– Low testosterone is an uncommon cause of ED
– However PDE 5 inhibitors do not work as well in the presence of low testosterone
– Free Androgen Index, Bioavailable Index and Free Testosterone are unreliable and generally not used
– “best of a bad bunch” is two morning sample serum testosterone levels
35
TREATMENT
Counselling
Viagra Cialis, Levitra, Uprima ( Not Yet Available )
Intracavernosal Injections ( Caverject and Combinations)
Trans-urethral Agents (MUSE) ( Not currently available)
Topiglans ( Not yet available )
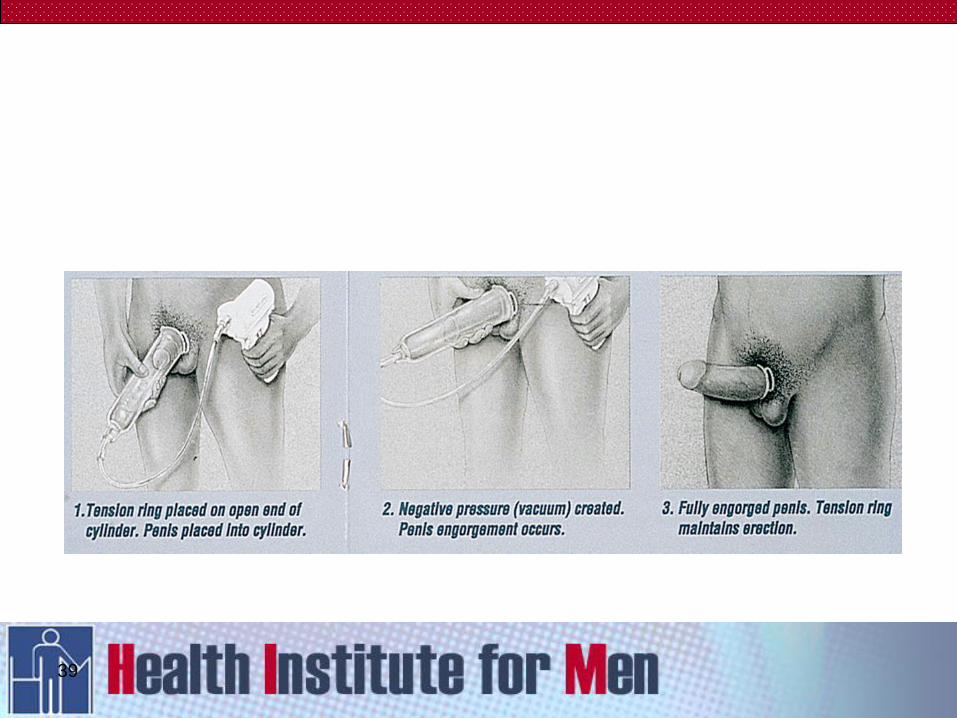
Vacuum Devices
Penile implants
Testosterone
Vascular Surgery ( Selected Cases Only )
36
VACUUM DEVICES
38
39
INTRACAVERNOSAL
INJECTIONS
41
SELF INJECTION THERAPY (cont)
Side effects
scarring
priapism
bruising
pain
Follow up
at one month, then every six months
as appropriate
42
43
44
PRIAPISM
Prolonged erection not associated with
sexual stimulation
After 24 hours may have irreversible
cavernosal damage resulting in
permanent erectile dysfunction
Must have action plan
Not usual with PDE5 inhibitors alone

INTRACAVERNOSAL
IMPLANTS
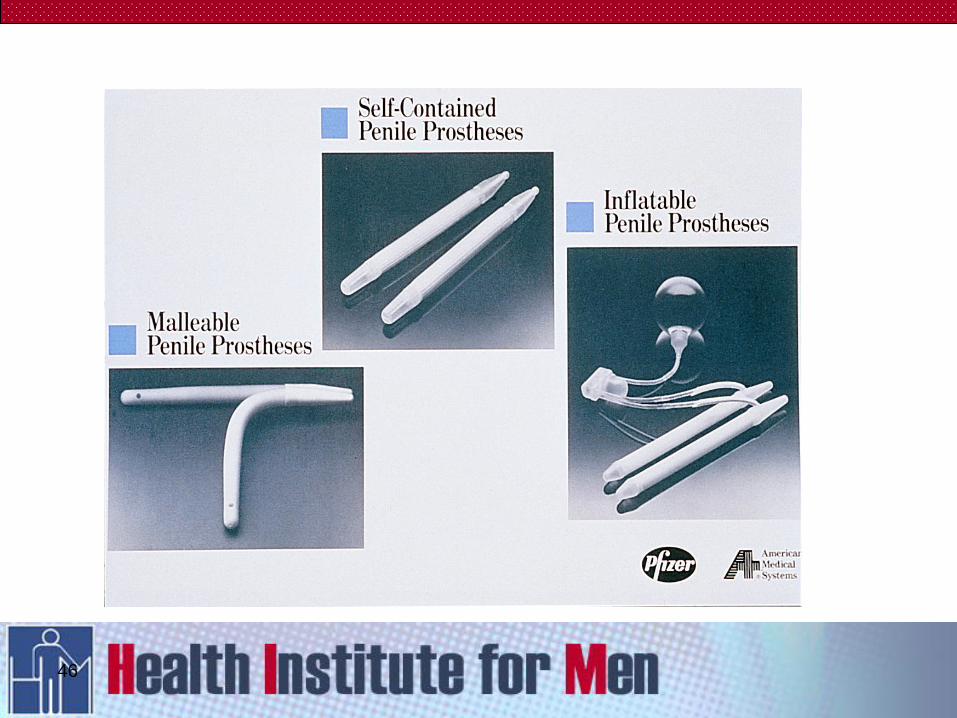
46
47
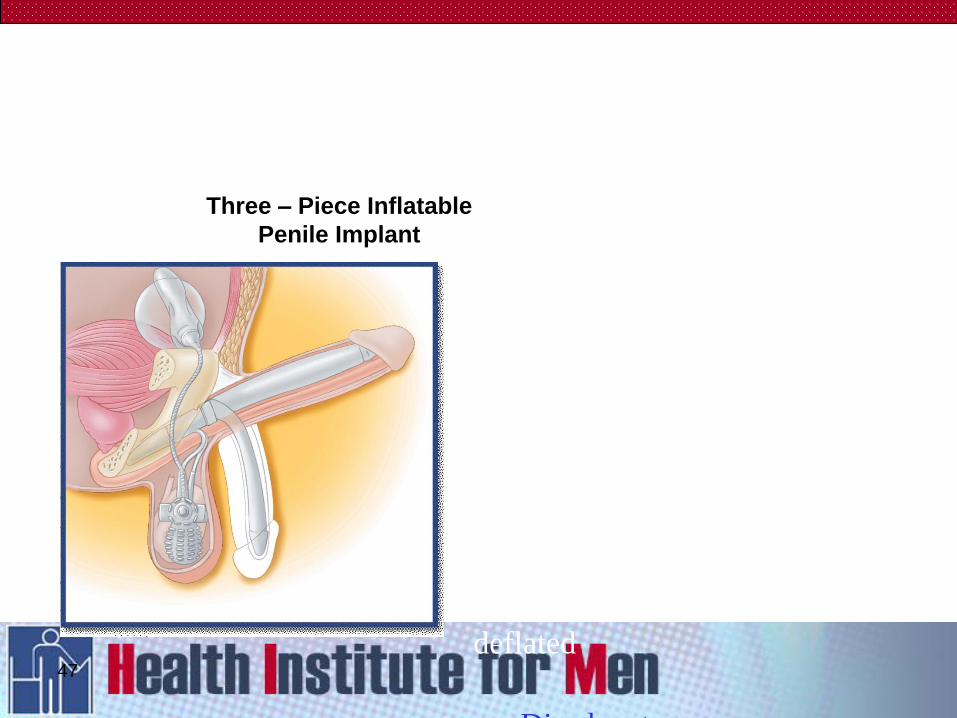
Three – Piece Inflatable
Penile Implant
Simple to use
Totally concealed within body
Acts and feels like a natural
erection
Provides fullness and girth
expansion
Softer and more flaccid when
deflated
Disadvantages
Requires some manual
dexterity
Possibility of malfunction
Possibility of leakage
48
PDE5’s ARE
DISCOVERED!!!!!!
50
51
52
53
Oral Agents
Needs sexual stimulation to work
Allow time
On demand or daily dosing
Tailor management to individual
couple Cost
Convenience
Efficacy
Side effects
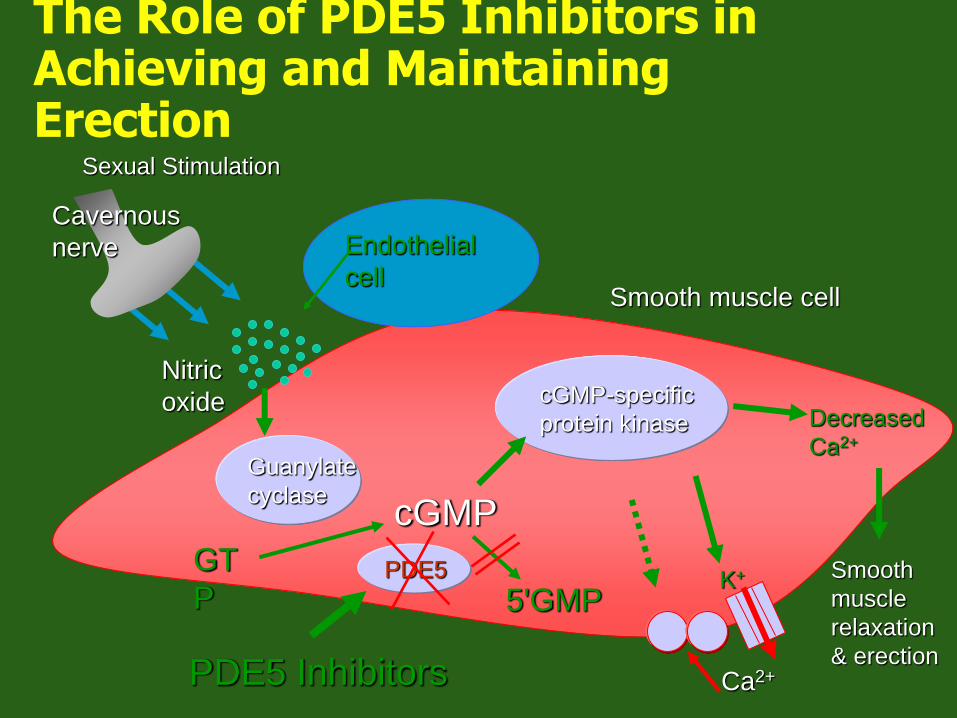
The Role of PDE5 Inhibitors in Achieving and Maintaining Erection
cGMP-specific
protein kinase
Endothelial
cell
Guanylate
cyclase
GT
P
cGMP
K+
Ca2+
Decreased
Ca2+
Smooth
muscle
relaxation
& erection
Nitric
oxide
Smooth muscle cell
5'GMP PDE5
Cavernous
nerve
Sexual Stimulation
PDE5 Inhibitors
CHANCE OF A
“CURE”????
56
CAVERNOSAL HYPOXIA
Aging effects on the corporal
vasculature supply (hyperlipidaemia,
hyperglycaemia etc.) cause hypoxic
changes
Transforming Growth Factor TGF-B(1)
is inhibited by prostaglandin
PGE(1&2) suppress collagen
synthesis in human fibroblast
cultures
57
CAVERNOSAL HYPOXIA
(cont)
An imbalance between PGE and
TGF-B(1) in the corpora due to
hypoxia, may cause increased
extracellular matrix deposition,
inhibition of smooth muscle growth,
and eventually fibrosis
PGE may have a role in the
management of cavernosal fibrosis
58
Main Points
Take a good history
Ask at risk patients about sexual
function
Offer patients a range of options
Discuss pros and cons of each
Ensure they use product effectively
59
They do grow on trees!
60
