assessing problematic states in patients' narratives: the grid of problematic states
TRANSCRIPT
This article was downloaded by: [DUT Library]On: 05 October 2014, At: 02:10Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Psychotherapy ResearchPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/tpsr20
Assessing Problematic States in Patients' Narratives:The Grid of Problematic StatesAntonio Semerari , Antonino Carcione , Giancarlo Dimaggio , Maurizio Falcone , GiuseppeNicolò , Michele Procacci , Giorgio Alleva & Erhard MergenthalerPublished online: 23 Apr 2010.
To cite this article: Antonio Semerari , Antonino Carcione , Giancarlo Dimaggio , Maurizio Falcone , Giuseppe Nicolò , MicheleProcacci , Giorgio Alleva & Erhard Mergenthaler (2003) Assessing Problematic States in Patients' Narratives: The Grid ofProblematic States, Psychotherapy Research, 13:3, 337-353
To link to this article: http://dx.doi.org/10.1093/ptr/kpg032
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Psychotherapy Research 13(3) 337–353, 2003DOI: 10.1093/ptr/kpg032© 2003 Society for Psychotherapy Research
ASSESSING PROBLEMATIC STATES IN PATIENTS’NARRATIVES: THE GRID OF PROBLEMATIC STATES
Antonio SemerariAntonino CarcioneGiancarlo DimaggioMaurizio FalconeGiuseppe NicolòMichele ProcacciIII Centro di Psicoterapia Cognitiva, Training School in Cognitive Psychotherapy,
Rome
Giorgio AllevaUniversità Degli Studi La Sapienza, Rome
Erhard MergenthalerUniversität Ulm, Sektion Informatik in der Psychotherapie
This study is part of a research project headed by Antonio Semerari and Giuseppe Ruggeri. It is sup-ported by the National Project of Mental Health of the Istituto Superiore di Sanità, Rome, ContractNo. 96Q/T/23. Statistical analysis was performed by Antonio Camerlengo, Università La Sapienza, Rome.
Correspondence concerning this article should be addressed to Erhard Mergenthaler, Universität Ulm,Sektion Informatik in der Psychotherapie, Am Hochsträß 8, 89081 Ulm, Germany. E-mail: [email protected].
337
The authors present the theoretical background, development, and vali-dation of a new psychotherapy process rating tool: Grid of ProblematicStates (GPS). The GPS is based on Horowitz’s states of mind theory, whichdescribes recurrent patterns of experience and behavior. Meaningfulchanges in the observed states indicate therapeutic change. The GPS isdesigned for use with transcripts from psychotherapy sessions and focuseson narrative episodes within the patient dialogue. The GPS was appliedto a completely transcribed cognitive psychotherapy with a patient diag-nosed as mild major depressive. The authors demonstrated that the GPScould reliably assess disorganization and the development of stable con-struct clusters of thought themes, emotions, and somatic sensations. Theinterpretation of results is consistent with the patient’s clinical assessment.
In cognitive psychotherapy, therapists assess thoughts and images that precede, ac-company, and follow emotions and disturbing sensations. They also focus on theunderlying schema. Cognition is given an implicit primacy because it is easy to useclinically and, consequently, has been chosen as a practical choice rather than atheoretical option (Clark, 1995). However, this may not take into consideration suf-ficiently the effect of emotions and bodily states on cognitive processes and, therefore,bears the risk of overlooking important aspects of therapeutic change. If cognition,emotion, and sensation are actually integrated, a therapeutic change can occur through
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

338 SEMERARI ET AL.
either modification of beliefs or alteration of the emotional-somatic atmosphere, bothof which facilitate cognitive change.
An important contribution in understanding the relation among cognition, emo-tion, and bodily states has been made by the neuroscientist Antonio Damasio (1994,1999). According to his understanding, awareness of a feeling starts when mentalimages connect in specific brain circuits to the perception of bodily states. The brainconstantly is monitoring this process. Mental scenarios, therefore, are “marked” bymemories of positive or negative bodily states. This process of somatic marking is ofimportance for the “rationality” of decisions. This notion is supported by the obser-vation that individuals suffering from a lesion of the brain in specific areas and whohave lost the ability to experience emotions still maintain their ability to reason.However, they are incapable of carrying out suitable choices in everyday life. Ac-cording to Damasio, emotional-somatic marking is necessary. Otherwise, if emotionsare absent, the appropriate evaluation of the costs and benefits of an action will notbe possible. This, in turn, leads to an inability to reduce the nearly infinite set ofpossible future scenarios to a limited number of options. As emphasized by Greenbergand Safran (1987), in the psychotherapeutic realm, emotions allow us to act in anintegrated way, connecting cognition and action to memories of bodily states. Ac-cording to this view, normal as well as pathological behavior is connected to distinctmental states, each of them characterized by emotionally marked mental scenarios.Changing one of the elements in a scenario, in particular the emotional component,causes a change toward a different or altered scenario.
Horowitz’s (1987, 1991) states of mind theory is based on the concept of distinctmental states as a practical clinical construct. In his definition, a state of mind is “arecurrent pattern of experience and of behaviour that is both verbal and non-verbal.States are commonly recognised during a clinical interview because of changes infacial expression, intonation and inflection in speech, focus and content of verbalreports, degree of self-reflective awareness, general arousal, shifts in degree and natureof empathy, and other communicative qualities. . . . A state description may include,for behavioral form, the patterns noted in posture, facial expression, tone of voice,gestures, style of speech flow, dialect, deployment of gaze, and other physical signsof attention focus. These will often convey the emotional coloration of a given stateof mind. For verbal report, the specific thought contents, felt emotions as labeled inwords or described in images of bodily feelings, and other reported aspects of sub-jective experiences may be included” (1987, p. 27).
The main advantage of the states of mind theory is that Horowitz’s formulationsare easily adapted to various theoretical orientations, thus enabling the integrationof writings from authors with different backgrounds. With regard to empirical re-search, the issue is whether it possible to reliably identify different mental states insession material like audio- or videotapes and verbatim transcripts and to pinpointthe changes that occur in the course of the psychotherapeutic process. Horowitz andhis research group have developed tools to assess various types of states of mind(Horowitz, Milbrath, & Stinson, 1997), for example, the Positive State of Mind Scale(Horowitz, Adler, & Kegeles, 1988) a self-assessment instrument applied by the pa-tient him or herself. Using the Positive State of Mind Scale, patients rate, on a 5-pointscale for each of seven positive states of mind, how they have experienced themduring the preceding week. This scale can be used as a pre–post measure to controloutcome or during the treatment at various points to observe change. Another tool isfor use with videotapes. For consecutive segments of 30 s each, facial and expres-sive behavior (gesture) is rated as being a well-modulated, undermodulated, over-
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

ASSESSING PROBLEMATIC STATES 339
modulated, or shimmering state (Horowitz, Milbrath, Ewert, & Sonneborn, 1994).Finally, individualized descriptions of states of mind can also be collected at varioustimes in therapy based on transcripts. Indications of change are a decreasing fre-quency of dreaded and maladaptive states and the production of new states (Horowitz,1987).
The first case that we examined in the light of this theory—using verbatim tran-scripts—showed that the patient’s experience tended to be grouped into distinctproblematic mental states (Semerari, Dimaggio, Carcione, & Nicolò, 1997). This gaverise to the need to develop more systematically a text analytic tool for the empiricalassessment not only of individualized states but also for more general problematicstates as a grid of predefined constructs for the relevant domains.
According to Horowitz’s definition, a mental state has both public and privatedimensions. The public dimension is what an observer can grasp externally throughmimic patterns and expressive behavior. The private dimension refers to thoughts,feelings, and somatic sensations that are typical for a given state. The concept ofproblematic states refers to this private dimension. Problematic states are global formsof subjective experience, some of them linked to psychological suffering. Their com-ponents are thought themes, emotions, sensations, and somatic phenomena. Theytend to be present in a form that is distinct and discontinuous, and they are sharedwith others through the report of narratives we also consider to be problematic states:those experiences that have not been felt subjectively to be painful but are relived ina rigid or compulsive way to avoid, either consciously or otherwise, other problem-atic states. Empirically, problematic states of mind can be assessed by analysis of thespoken word (e.g., with the analysis of session transcripts).
The aim of this article is to present the theoretical background and developmentof a rating tool for identifying problematic states in patient’s narrative material, espe-cially in the verbatim transcripts of tape-recorded sessions. We also present a samplestudy with a single case to illustrate the application and clinical relevance of themethod.
Grid of Problematic States (GPS) Rating Scale
General Aspects
The GPS rating scale was originally developed for use with session material inItalian, including a comprehensive manual with definitions and examples for judges(Carcione et al., 1999). In this article we present an English version of the GPS, whichhas not thus far been applied to English session material.
Starting from the idea that distinct mental states exist, it should be possible toidentify clearly observable instances for clusters within the domains of thought themes,emotions, and somatic sensations in the narrative material of patients during ses-sions from psychotherapeutic treatments. If such clusters remain stable over a sig-nificant period, this would signal that a patient has a stable way of living and describinghis or her subjective experience. The first step then in the construction of such aresearch tool was to compile a list of different thought themes, emotions and so-matic sensations, which, according to both our clinical experience and the literature,are important in psychotherapy. To trace a problematic state within or across therapysessions, we then need to identify the basic components—thought themes, emotionsand descriptions of sensations and somatic states—and to collapse them into mean-
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

340 SEMERARI ET AL.
ingful clusters. As in Kelly’s repertory grid (1955), the components of the GPS areorganized in the form of bipolar constructs built of positive and negative items (e.g.,missing care/receiving care). This allows us to trace not only variations across themesbut also oscillations along a negative–positive axis.
The definition of a problematic state is that at least one of the three domains ispresent in a given instance (e.g., just a thought theme but no emotion or somaticstate). In this way, with the GPS, we can overcome the problem that we might havewhen patients cannot integrate all elements of their subjective experience. By firstassessing how patients represent the domains of their subjective experience in theirown words, we can identify which domain is represented at any given point. Throughanalysis of the domains represented in the patients’ narratives, we can then observechanges in the modifications of the psychopathology.
Domains
The thought themes (Table 1, Constructs 1–19) were mainly derived from thecognitive psychotherapeutic literature. In particular, we referred to Bowlby’s (1969/1982, 1979) attachment theory and classical cognitive work on dominant themes indepression and anxiety (Beck, Rush, Shaw, & Emery, 1979; Ellis, 1962). We paidparticular attention to themes that are of particular importance for patients with per-sonality disorders following the Diagnostic and Statistical Manual of Mental Disor-ders (fourth edition; DSM-IV ) criteria (American Psychiatric Association, 1994) andcognitive psychotherapy-oriented authors (Young, 1994). Finally, a number of themesrepresent the concept of personal self-efficacy (Bandura, 1977).
The list of emotions (see Table 1, Constructs 20–29) was based on the set ofbasic emotions considered to be shared by all human beings. The studies to whichwe refer considered both the analysis of similarities in facial expressions in differentcultures and the observation of basic anatomical and neurophysiological mechanisms(Damasio, 1994; Ekman & Friesen, 1975; Frijda, 1986; Izard, 1977; Le Doux, 1996;Oatley & Johnson-Laird, 1987; Panksepp, 1982; Tomkins, 1962). We also drew onliterature about social emotions (Castelfranchi, 1988; Frijda; Heider, 1958; Lewis, 1992)and the tendency of an organism to react with variations in arousal and intensity(Frijda; Pribram & McGuinness, 1975; Toates, 1980). For a definition of boredom andemptiness, we also referred to Sartre’s (1939, 1943) phenomenological analyses.
The sensations and somatic states domain (see Table 1, Constructs 30–32) clas-sifies the way in which patients describe their subjectively perceived body and theintegrity of their state of consciousness. The lack of sense of cohesion/cohesionconstruct refers to alterations in the state of consciousness diagnosed in DSM-IV asdissociated disorders, in particular the phenomena found in depersonalization disor-der. Finally, (a) abulia, asthenia, weakness/feeling of vitality and strength, (b) un-controllable physical arousal/feeling of command and motor control, and (c) anyconstructs that indicate specific somatic manifestations refer to the way in which DSM-IV describes the perception of one’s body in somatization and conversion disorders.These are not included in the grid as predefined but are available to be used ad hocwhen they are important in a patient’s story.
Narrative Episodes
Narrative psychology (Bruner, 1986, 1990; Dimaggio & Semerari, 2001; Gonçalves,1995; Hermans & Kempen, 1993; Labov & Fanshel, 1977; Luborsky & Crits-Cristoph,
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

ASSESSING PROBLEMATIC STATES 341
1990; Mandler, 1984; Neimeyer, 1995, 2000; Sarbin, 1986; Spence, 1982; Villegas,1992; Villegas & Ricci, 1998) suggests a relationship between the narrative structureand different states of mind. Breaks in the continuity of the narrative structure, whichare signaled by changes in the aspects that provide the foundations for the story,ought to correspond to breaks in the continuity of states of mind and of subjectiveexperience. According to this view, patients organize their autobiographical memo-ries and discourse during therapy in the form of storytelling. Narratives form a modelof self-in-the-world and an instrument for action planning (Bruner, 1986, 1990). Tellingstories about one’s own life is one way for a speaker to let the recipient have accessto his or her interior states, to put “past experiences and ongoing life events intomeaningful units across time, themes and persons” (Mancuso & Sarbin, 1983). We,therefore, decided to use a narrative episode as scoring unit for the GPS rating scales.
TABLE 1. The 32 Constructs of the Grid of Problematic States Rating Scale
No Bipolar construct
t1 Missing care, missing help/received care, received helpt2 Denied care, denied help/lent care, lent helpt3 Distrust/trustt4 Failure/successt5 Refusal, exclusion, detachment/acceptance, belongingt6 Threat, danger, assault/assurance, feeling of being welcomet7 Moral degradation, chaos/harmony, ordert8 Injustice or unjustified caused harm/caused benefitst9 Feeling neglected, loneliness, loss/closeness, presencet10 Losing control/strong self-controlt11 To let go off oneself/good self-regulationt12 Death/lifet13 Detriment, suffered injustice/feeling of well-being, enjoying benefitst14 Negative judgment (received or foreseen)/positive judgment (received or
foreseen)t15 Low self-esteem/high self-esteemt16 Constraint/freedomt17 Transgression/to be in conformity with societies rulest18 Competition–negatively experienced/competition–positively experiencedt19 Low self-efficacy/high self-efficacye20 Fear, anxiety/calmnesse21 Sadness, depression/happiness, enthusiasme22 Lack of sexual interest/high sex drivee23 Disgust, dislike/niceness, attractivenesse24 Indifference, coldness/pity, tendernesse25 Contempt/admiration, emulatione26 Shame, embarrassment/easee27 Guilt/self-acceptance, feeling of being righte28 Anger/serenitye29 Emptiness, boredom/interest, curiositys30 Lack of sense of cohesion/cohesions31 Abulia asthenia, weakness/feeling of vitality and strengths32 Uncontrollable physical arousal/feeling of command and motor control
Note. The slash mark separates the negative from the positive items. t = thought theme; e = emotion; s= somatic state.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

342 SEMERARI ET AL.
The identification of narrative episodes within a therapy session is based on therules of story organization (narrative structure) and related aspects of syntax (Burke,1945). A description in narrative form might take into account a number of structuralcharacteristics typical for an autobiographical style: setting, characterization, plot,theme, and fictional goal (Neimeyer, 1995). With the term narrative episode, we referto the minimal narrative structure, or “micronarrative” to use the terminology of LynneAngus (Angus, Hardtke, & Levitt, 1996; Angus, Levitt, & Hardtke, 1999). Our instruc-tions for the identification of narrative episodes, therefore, largely follow those givenin the rating manual developed by Angus, Hardtke, and Levitt.
Identification of Narrative Episodes
A narrative episode can be initiated by the patient or the therapist through spe-cific interventions. It is made up of a story that the patient tells during a session aboutan event or a series of occurrences connected to each other. A narrative episode ischaracterized by a beginning, an unfolding, a space–time sequence, and coherentassociating links. A confused story, in which the components get mixed up withoutthe possibility of identifying a space–time order, therefore has to be excluded. Anarrative episode refers to particular components: the detailed description of emo-tions, physical sensations, and thoughts that patients give as they refers to whathappened. A narrative episode may concern (a) relationships with others; (b) rela-tionships between relevant others, even in the absence of the patient; (c) a dialogueor detailed thoughts regarding experiences (e.g., the story of how a symptom started,became acute and unbearable, and then disappeared at the end of the very sameday); and (d) fantasies. Dreams are scored in the same way as a narrative episodebut are analyzed as a separate category; each dream is considered a single unit. Anarrative episode cannot be interrupted. If, after having spoken on a different topic,the patient returns to the theme of an earlier reported narrative episode, this is con-sidered to be a new narrative episode.
A patient’s storytelling may contain different narrative episodes. The followingformal criteria are used to mark the boundaries between two or more adjacent nar-rative episodes: (a) the presence of a time marker that is inserted in the conversationand signals the action’s shift to a different period, (b) change in the scene of an ac-tion, (c) change (entry or exit) in the principal characters, (d) a clean break, withouta link, between the thought theme and the emotions that were dominant up to acertain point in the preceding narrative, and (e) change in the principal goal of anarrative episode.
When at least three of these five criteria are satisfied, judges should consider anarrative episode as being complete and should begin to identify a new narrativeepisode (e.g., change in time, different scene, and appearance of new character).
GPS Scoring Instructions
The scoring unit is the narrative episode. We used a 7-point Likert scale, whichrepresents both valence and intensity of the constructs. Scores from 1 to 3 indicate anegative valence, a score of 4 indicates the construct is not present, and scores of 5to 7 indicate a positive valence. The intensity of a construct depends on the numberof characteristics that are present. The extreme scores of 1 or 7 (high) are given if atleast two of three characteristics are present. If only one characteristic is present, the
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

ASSESSING PROBLEMATIC STATES 343
rating is 2 or 6 (medium). If none of the characteristics is present but the construct ismentioned in the narrative episode, the rating is 3 or 5 (low).
Characteristics for Thought Themes
Implausibility. These thought themes are, after commonsense reasoning, con-sidered to be unrealistic and not appropriate to the context in which the themeappears. For example, patients report themes describing missing help (negativeitem in Construct 1) in situations that the majority of observers would consider tobe very safe.
Generalization. A thought theme is considered to be highly pervasive when ittends to lead to a large number of inductive generalizations of the type “I will al-ways be rejected; the world is bad” or “I am simply the best.”
Emotionality. A thought theme has emotional content all over the course of annarrative episode or if at least one of Constructs 20 to 29 (emotion) is present withan extreme score of 1 or 7. For example, “I’m despairing because nobody is able tohelp me; I just get treated like an old tramp left to beg on the street.” Construct 1 isgeneralized and the emotionality is high, so the score is 1.
Characteristics for Emotions and for Sensations and Somatic States1
Intensity. An emotion or somatic state is considered to be intense when patients,from a subjective point of view, verbally emphasize their narration of an episode.Verbal indicators are the use of superlatives or diminutives, the type of adjectiveschosen, and also the use of strong figures of speech.
Influence. The influence of an emotion or somatic state on patients’ behavior isconsidered to be high when there is evidence in the narrative episode that it led toa particular action or that patients could not have carried out a different type ofbehavior even if they wanted to. Physical signs have to be taken into account.
Duration. The duration of an emotion or a somatic state is considered to be im-portant if most of the narrative episode is characterized by the patients. For example,an emotion fear/anxiety that causes flight and permeates an entire narrative episodewill score 1. An overbearing joy leading to the giving of presents will score 7.
Patient History
Maria, a 32-year-old woman, presented with weight loss (about 5 kg), diffi-culty falling asleep, significant mood depression, asthenia, abulia, and phobic–obsessive ideas fearing that she could become “mad” and kill someone. She wasalso afraid that she could die from suffocation. In the 2 years before she had three
1Emotions and somatic states are separate concepts. The former include an immediate evaluation ofthe meaning of an event, an appraisal, by a patient, whereas the latter do not, but they do have thecentrality of bodily experience as a common characteristic. For this reason, the rating criteria are thesame.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

344 SEMERARI ET AL.
spontaneous abortions, the cause of which remained unclear. Maria was convincedthat she would cause death to anyone who asked her to take care of him or her.She was afraid that if she had a child she would kill the child as soon he or sheneeded her help or care. In accordance with the DSM-IV criteria, she was diag-nosed as a mild major depressive with an overall functioning of 50/100. Maria wasoffered cognitive psychotherapy.
Material and Statistics
Maria’s 27 treatment sessions and an additional follow-up session were audio-recorded and transcribed following the psychotherapy transcription standards (Mergen-thaler, Freni, Giampieri, & Ferrari, 1998). As a unit for statistical analysis, we usedgroups of three sessions each rather than a fixed number of narrative episodes. Theseyielded nine phases plus one follow-up session. This allowed us to compare theGPS findings with other methods using the same type of unit (Nicolò et al., 2000,2001). The decision for a group size of three sessions meets two requirements: (a)an observation period long enough to produce sufficient data sufficient to perform astatistical analysis, within a period of therapy in which it can be hypothesized that apatient’s mental state is stable; and (b) a time window that is not too long (not morethan 1 month of therapy), so that we can precisely identify the moment when a changein content (assuming this occurs) might occur.
Exploratory Hypotheses
Because the nature of this study was to demonstrate the applicability of the GPSrating scale, we decided to stay with an exploratory hypothesis. We expect to findstable clusters of thought themes, emotions, sensations, and somatic sensations inthe initial phase of the therapy and before a possible therapeutic change.
Results
Before the study two judges were trained for the identification of narrative epi-sodes and for rating the GPS using 25 sessions from three different therapies. The judgesscored the 27 sessions independently and noted on each transcript the episode’s run-ning number, its beginning, and its end. Of the narrative episodes, the second judgeidentified 93% of the episodes identified by the first judge. In addition, the first judgeidentified 89% of the episodes identified by the second judge.2 The average size of anarrative episode (measured in terms of number of lines on which both judges agreed)was 27.4 lines. The median difference in numbers of transcript lines for the onset of anarrative episode was 6 lines or less, whereas for the offset there was a difference ofup to 10 lines. A consensus judge made the final decision as to whether there was anarrative episode and when it started and ended. There were a total of 229 narrativeepisodes, 25.4 on average for each of the nine groups of sessions, varying from aminimum of 11 (fourth period) to a maximum of 41 (first period).
2For the evaluation of the level of agreement we used a procedure similar to that used by Luborsky andCrits-Cristoph for relationship episodes (see an example in Crits-Cristoph et al., 1999).
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4
ASSESSING PROBLEMATIC STATES 345
Problematic States
Three trained raters, all of them clinically experienced therapists, scored the 229narrative episodes on a session-by-session basis. Raters were rotated so that none ofthem scored two consecutive sessions. To check the reliability of the raters, all 12narrative episodes occurring during the 10th session of another patient were used todetermine the level of agreement. The interrater reliability among the three raterswas assessed using the intraclass correlation coefficient (Shrout & Fleiss, 1979). Ascore of .64 was achieved for the single measure intraclass correlation and .84 forthe average measure intraclass correlation.
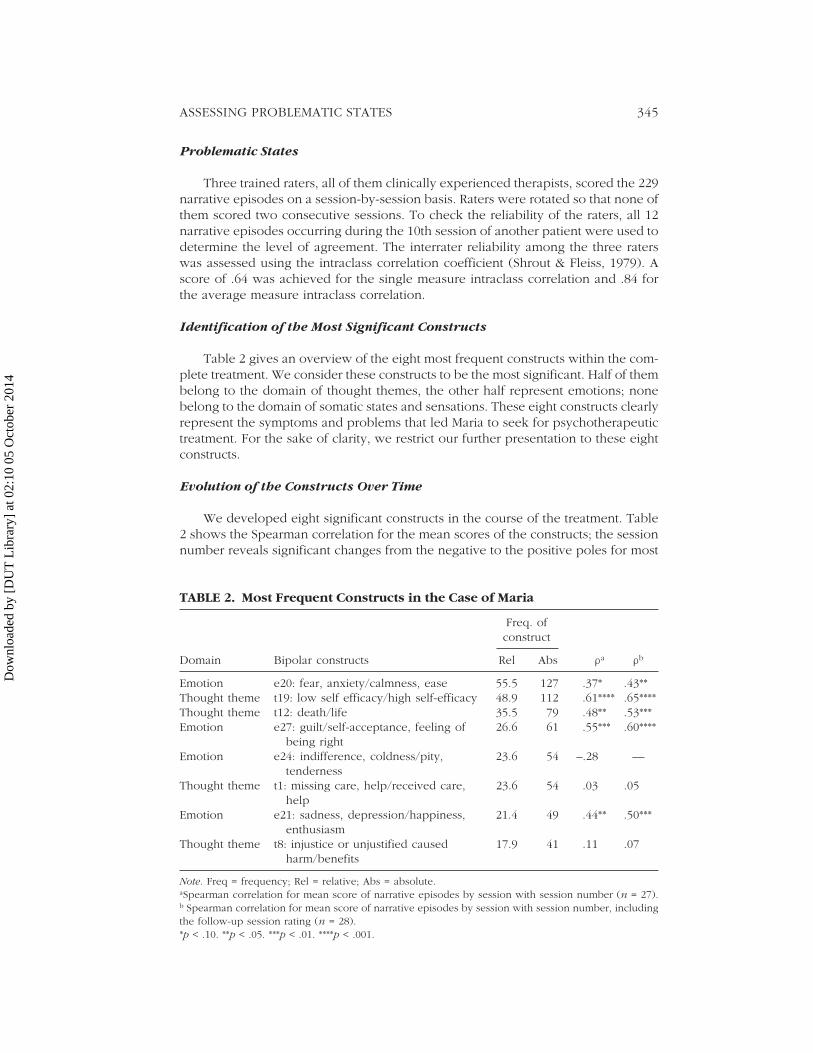
Identification of the Most Significant Constructs
Table 2 gives an overview of the eight most frequent constructs within the com-plete treatment. We consider these constructs to be the most significant. Half of thembelong to the domain of thought themes, the other half represent emotions; nonebelong to the domain of somatic states and sensations. These eight constructs clearlyrepresent the symptoms and problems that led Maria to seek for psychotherapeutictreatment. For the sake of clarity, we restrict our further presentation to these eightconstructs.
Evolution of the Constructs Over Time
We developed eight significant constructs in the course of the treatment. Table2 shows the Spearman correlation for the mean scores of the constructs; the sessionnumber reveals significant changes from the negative to the positive poles for most
TABLE 2. Most Frequent Constructs in the Case of Maria
Freq. ofconstruct
Domain Bipolar constructs Rel Abs ra rb
Emotion e20: fear, anxiety/calmness, ease 55.5 127 .37* .43**Thought theme t19: low self efficacy/high self-efficacy 48.9 112 .61**** .65****Thought theme t12: death/life 35.5 79 .48** .53***Emotion e27: guilt/self-acceptance, feeling of 26.6 61 .55*** .60****
being rightEmotion e24: indifference, coldness/pity, 23.6 54 –.28 —
tendernessThought theme t1: missing care, help/received care, 23.6 54 .03 .05
helpEmotion e21: sadness, depression/happiness, 21.4 49 .44** .50***
enthusiasmThought theme t8: injustice or unjustified caused 17.9 41 .11 .07
harm/benefits
Note. Freq = frequency; Rel = relative; Abs = absolute.aSpearman correlation for mean score of narrative episodes by session with session number (n = 27).b Spearman correlation for mean score of narrative episodes by session with session number, includingthe follow-up session rating (n = 28).*p < .10. **p < .05. ***p < .01. ****p < .001.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4
346 SEMERARI ET AL.
of the constructs. Including the follow-up session, this finding remains stable or evengets stronger.
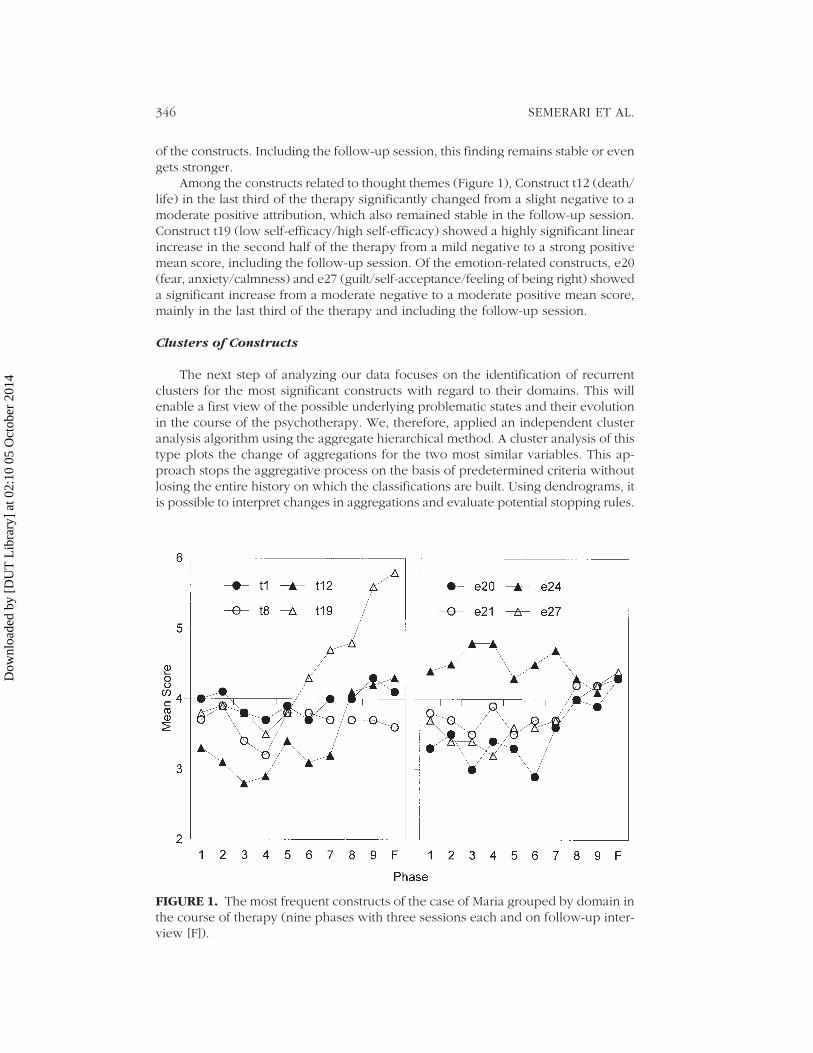
Among the constructs related to thought themes (Figure 1), Construct t12 (death/life) in the last third of the therapy significantly changed from a slight negative to amoderate positive attribution, which also remained stable in the follow-up session.Construct t19 (low self-efficacy/high self-efficacy) showed a highly significant linearincrease in the second half of the therapy from a mild negative to a strong positivemean score, including the follow-up session. Of the emotion-related constructs, e20(fear, anxiety/calmness) and e27 (guilt/self-acceptance/feeling of being right) showeda significant increase from a moderate negative to a moderate positive mean score,mainly in the last third of the therapy and including the follow-up session.
Clusters of Constructs
The next step of analyzing our data focuses on the identification of recurrentclusters for the most significant constructs with regard to their domains. This willenable a first view of the possible underlying problematic states and their evolutionin the course of the psychotherapy. We, therefore, applied an independent clusteranalysis algorithm using the aggregate hierarchical method. A cluster analysis of thistype plots the change of aggregations for the two most similar variables. This ap-proach stops the aggregative process on the basis of predetermined criteria withoutlosing the entire history on which the classifications are built. Using dendrograms, itis possible to interpret changes in aggregations and evaluate potential stopping rules.
FIGURE 1. The most frequent constructs of the case of Maria grouped by domain inthe course of therapy (nine phases with three sessions each and on follow-up inter-view [F]).
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4
ASSESSING PROBLEMATIC STATES 347
From the class of aggregation algorithms, we chose the VarClus method3 (Harman,1976), which is available in the Statistical Analysis System-8 package.
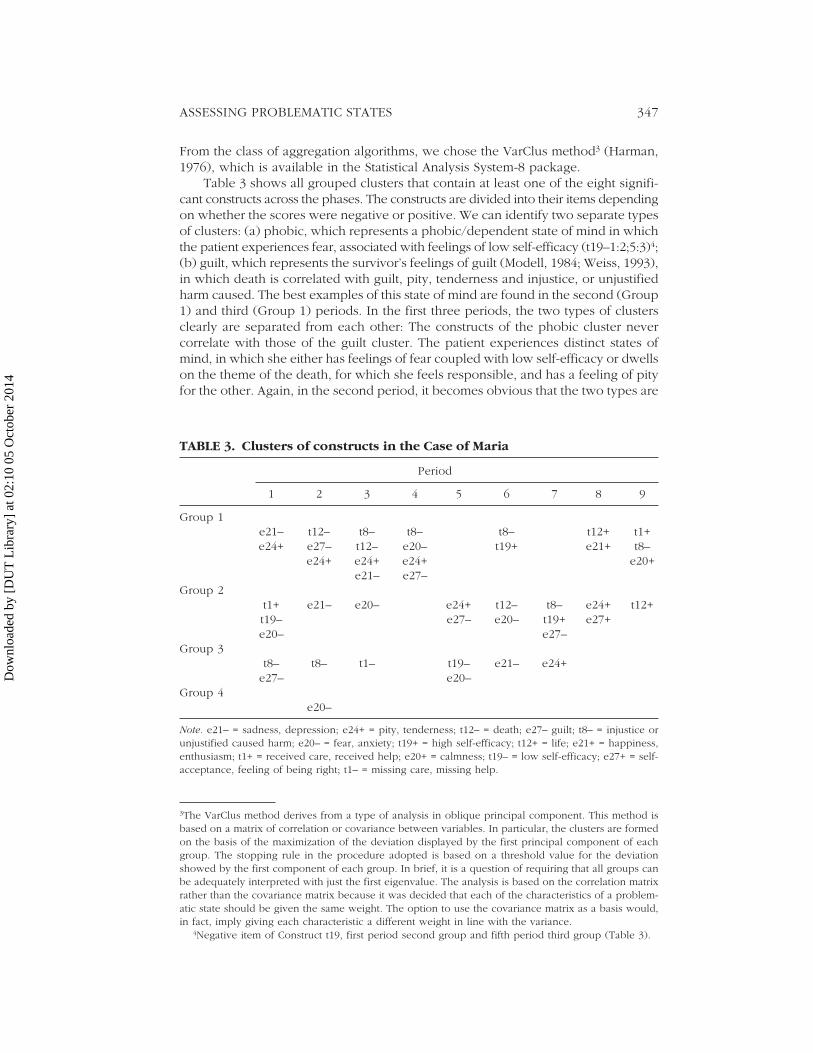
Table 3 shows all grouped clusters that contain at least one of the eight signifi-cant constructs across the phases. The constructs are divided into their items dependingon whether the scores were negative or positive. We can identify two separate typesof clusters: (a) phobic, which represents a phobic/dependent state of mind in whichthe patient experiences fear, associated with feelings of low self-efficacy (t19–1:2;5:3)4;(b) guilt, which represents the survivor’s feelings of guilt (Modell, 1984; Weiss, 1993),in which death is correlated with guilt, pity, tenderness and injustice, or unjustifiedharm caused. The best examples of this state of mind are found in the second (Group1) and third (Group 1) periods. In the first three periods, the two types of clustersclearly are separated from each other: The constructs of the phobic cluster nevercorrelate with those of the guilt cluster. The patient experiences distinct states ofmind, in which she either has feelings of fear coupled with low self-efficacy or dwellson the theme of the death, for which she feels responsible, and has a feeling of pityfor the other. Again, in the second period, it becomes obvious that the two types are
3The VarClus method derives from a type of analysis in oblique principal component. This method isbased on a matrix of correlation or covariance between variables. In particular, the clusters are formedon the basis of the maximization of the deviation displayed by the first principal component of eachgroup. The stopping rule in the procedure adopted is based on a threshold value for the deviationshowed by the first component of each group. In brief, it is a question of requiring that all groups canbe adequately interpreted with just the first eigenvalue. The analysis is based on the correlation matrixrather than the covariance matrix because it was decided that each of the characteristics of a problem-atic state should be given the same weight. The option to use the covariance matrix as a basis would,in fact, imply giving each characteristic a different weight in line with the variance.
4Negative item of Construct t19, first period second group and fifth period third group (Table 3).
TABLE 3. Clusters of constructs in the Case of Maria
Period
1 2 3 4 5 6 7 8 9
Group 1e21– t12– t8– t8– t8– t12+ t1+e24+ e27– t12– e20– t19+ e21+ t8–
e24+ e24+ e24+ e20+e21– e27–
Group 2t1+ e21– e20– e24+ t12– t8– e24+ t12+t19– e27– e20– t19+ e27+e20– e27–
Group 3t8– t8– t1– t19– e21– e24+
e27– e20–Group 4
e20–
Note. e21– = sadness, depression; e24+ = pity, tenderness; t12– = death; e27– guilt; t8– = injustice orunjustified caused harm; e20– = fear, anxiety; t19+ = high self-efficacy; t12+ = life; e21+ = happiness,enthusiasm; t1+ = received care, received help; e20+ = calmness; t19– = low self-efficacy; e27+ = self-acceptance, feeling of being right; t1– = missing care, missing help.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

348 SEMERARI ET AL.
exclusive: The first group displays the survivor’s feelings of guilt, and the fourth grouprepresents the phobic type.
A change in this overall figure starts with the fourth period: The links betweenthe main clusters and their predominant components loosen and tend to split up:death (t12–) and guilt (e27–) separate, and there is no longer any cluster that theyshare. Maria now experiences the theme of death and the feelings of guilt in differ-ent states of mind. She no longer perceives herself as having been the cause of deathfor her loved ones. Death during the central period of the therapy is now experi-enced with fear and anxiety (e20–6:2). Guilt (e27–) is now clustered with Injustice(t8–4:1;6:2). Again, in the seventh period, we can observe an important change: Guilt(e27–) is now associated with thoughts of high self-efficacy (t19+7:2), and the pa-tient manages to master this sensation. The concept of fear and the thoughts of deathare no longer present throughout the remainder of the therapy.
In the eighth period, Maria’s psychological change becomes more and moreapparent. A new mental state has arisen in which the concept of fear/calmness hasneutralized (M = 4.0), and the theme of death has turned to the opposite pole: life(t12+8:1). Guilt has been transformed into self-acceptance (e27–8:2) without beingassociated with any specific construct from the thought theme domain.
Finally, in the ninth period, the alteration of the phobic cluster type has stabi-lized: Maria feels that she receives care and help (t1+9:1), and fear has changed intocalmness (e20+9:1). The thought theme life (t12+9:2) becomes neutralized with re-gard to the significant construct from the domain of emotions.
None of the constructs belonging to the domain of sensations and somatic stateswas among the eight most frequent. In the cluster analysis, lack of sense of cohesion(s30–) was present in Periods 1, 5, 7, and 9 but did not cluster in any significant waywith the constructs presented here. The received care and help (t1+1:2) and lowself-efficacy (t19–) constructs are associated with fear and anxiety (e20–1:2) in thefirst phase. At the end of the therapy received care and help is associated with calm-ness (e20+9:1). The concept of injustice or unjustified caused harm/caused benefits(t8) was present in almost every phase (except 5 and 8) with its negative item andmostly accompanied with negative emotions.
Discussion
During the course of the therapy, it is possible to identify distinct types of prob-lematic states: (a) phobic dependent and (b) survivor’s feelings of guilt. These statesremain exclusive during the first three time periods. From the fourth period onward,death and guilt split. Both clusters undergo similar modifications, as indicated by theinversion in polarity of the constituting items from negative to positive. In the phobic-dependent cluster, there is an evolution toward a less intense fear, which in the endbecomes calmness. In the cluster of the survivor’s guilt feeling type, we can see first aseparation between guilt and death themes (the patient no longer claims to have killedher loved ones), and then an inversion in the polarity of the constructs, with deathbecoming life and guilt becoming self-acceptance. Furthermore, received care and help,which was associated with fear and anxiety at the beginning of the therapy in combi-nation with low self-efficacy, is associated with calmness at the end of the therapy.However, there also seems to be an unresolved topic. The concept of injustice orunjustified caused harm/caused benefits (t8) was present in almost every phase (ex-cept 5 and 8) with its negative item and mostly accompanied with negative emotions.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

ASSESSING PROBLEMATIC STATES 349
Conclusions
The application of the GPS scales and their evaluation in the case of Maria hasgiven results that are consistent with Horowitz’s hypothesis: From the narratives pro-duced by the patient during sessions, it was possible to identify consistent clusters ofconstructs signaling the existence of distinct mental states, which were experiencedwith subjective suffering. These clusters remained unaltered and separated from eachother during the first three periods of therapy (nine sessions). Subsequently, thepatient’s psychological experience began to change. In particular, the therapy re-sulted in a shift in thought themes and emotions from a negative to a positive pole.This is a development typical and desired for a successful therapy with patients mainlyaffected by syndromes on Axis I of the DSM-IV.
The presence of clusters that are stable over time can be ascribed to variouscauses. It may simply be that the theory of mental states is correct. Alternatively, it ispossible that the therapist mainly has elicited narratives about themes believed to beimportant for this treatment. What cannot be concluded from this single case studyis whether Horowitz’s theory is valid in general or just for specific syndromes as inthe case of Maria. The next step in testing the theory will be to extend the analysisto other individual cases and to compare the results with the respective psychopatho-logical diagnoses.
The single case presented here in the light of problematic states of mind high-lights some of the potential uses of the GPS rating scale. It supports the notion thatthere are distinct states of mind that can become identified as problematic states. Italso was possible to show how these states evolve during the psychotherapeuticprocess. The GPS, therefore, can be used as a tool to assess the focus of a therapyand to evaluate the process. We expect that the application of the GPS to a wideclinical population will allow the verification of the existence of at least three typesof psychotherapeutic change. First, there is a problematic state present, and it canbe identified. During therapy it is seen to disappear or there is a turnaround in thepolarities of the elements, from positive to negative. Furthermore, it is possible thatother constructs, which change its overall meaning, may appear within it. Second,after an initial situation of fragmentation and disorganization, in which it is not pos-sible to identify recognizable and stable states of mind, one passes to states that aremore coherent and complete. Third, certain patients are poor at narrating. A prob-lematic state exists, but there is not a sufficient variety of states of mind. During asuccessful therapy, one may see new states of mind appearing or states that are al-ready present expanding.
Our analytic tool, if compared with other methods present in clinical literature,has a number of advantages as well as disadvantages. By considering, as we do, theindividual elements (emotions, thought themes, somatic states) present in a narra-tive, without hypothesizing links of cause and effect between them, it is possible toachieve a description of the state of mind of a patient that is formulated with a verylow degree of theoretical inference. In other words, we do not need to hypothesizea preexisting schema-type structure, as in the Core Conflictual Relationship Theme(Luborsky & Crits-Cristoph, 1990) or in Weiss’s method for the analysis of the un-conscious pathogenic beliefs that hamper the pursuit of an individual’s plans (Weiss,1993; Weiss, Sampson, & the Mount Zion Psychotherapy Research Group, 1986). Forthese methods, there is the risk of not considering as significant those elements fromsubjective experience that, although carrying weight in a patient’s life, do not getidentified by these research methods. For example, a patient may talk about the
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

350 SEMERARI ET AL.
evolution of an emotion over time or about a somatic state that is dissociated fromother elements of his or her mental life, which is not included in a schema, such aswish, other’s response, self’s response type. These states of mind correspond tothe most primitive forms of subjective experience that Stiles, Meshot, Anderson,and Sloan (1992) defined as warded-off, unwanted thoughts or vague awareness.Our method isolates the subjective components of experiences from the ongoinginterpersonal process, which constitutes, without doubt, a limitation. The methodsmentioned, on the contrary, pick up the level of interpersonal experience. Anadvantage of our method is that it is possible to observe not just the organizationof knowledge but also its disorganization. Patients suffering from borderline anddissociative disorders often relate their lives in a confused, fragmented, and dis-connected manner (Liotti, 2000). In these cases, it sometimes can be arbitrary topick out a single interpersonal schema or a single pathogenic belief and explain adisorder on this basis. With our method it is possible to observe the disorganiza-tion that is present in these patients (e.g., there is no formation of stable constructclusters) and to determine whether a therapy is helping narratives become moreintegrated: The hypothesis is that during a therapy it will be possible to see theformation of clusters that are stable over time.
References
American Psychiatric Association. (1994). Diag-nostic and statistical manual of mental disor-ders (4th ed.). Washington, DC: Author.
Angus, L., Hardtke, K., & Levitt, H. (1996). Thenarrative process coding system manual: Re-vised edition. North York, Ontario, Canada:York University.
Angus, L., Levitt, H., & Hardtke, K. (1999). Thenarrative processes coding system: Researchapplications and implications in psychotherapy.Journal of Clinical Psychology, 55, 1255–1270.
Bandura, A. (1977). Self efficacy: Towards a uni-fying theory of behavior change. PsychologicalReview, 84, 191–215.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G.(1979). Cognitive therapy of depression. NewYork: Guilford Press.
Bowlby, J. (1979). The making and breaking ofaffective bonds. London: Tavistock.
Bowlby, J. (1982). Attachment and loss. Volume I(2nd ed.). London: Hogarth Press. (Originalwork published 1969)
Bruner, J. (1986). Actual minds, possible worlds.Cambridge, MA: Harvard University Press.
Bruner, J. (1990). Acts of meaning. Cambridge,MA: Harvard University Press.
Burke, K. (1945). A grammar of motives. NewYork: Prentice Hall.
Carcione, A., Dimaggio, G., Falcone, M., Nicoló,G., Procacci, M., & Semerari, A. (1999). Manualeper l’utilizzazione della griglia degli stati prob-lematici [Handbook for the use of the Grid ofProblematic States]. Unpublished.
Castelfranchi, C. (1988). Che figura. Emozioni e
immagine sociale. [What’s a shame, emotionsand social image]. Bologna: Il Mulino.
Clark, D. A. (1995). Perceived limitations of stan-dard cognitive therapy: A consideration of ef-forts to revise Beck’s theory and therapy. Journalof Cognitive Psychotherapy, 9, 153–172.
Crits-Cristoph, P., Connolly, M. B., Shappell, S.,Elkin, I., Krupnick, J., & Sotsky, S. (1999). In-terpersonal narratives in cognitive and interper-sonal psychotherapies. Psychotherapy Research,9, 22–35.
Damasio, A. R. (1994). Descartes error: Emotion,reason and the human brain. New York:Putnam.
Damasio, A. R. (1999). The feeling of what hap-pens. Body and emotion in the making of con-sciousness. New York: Harcourt Brace.
Dimaggio, G., & Semerari, A. (2001). Psychopatho-logical narrative forms. Journal of ConstructivistPsychology, 14, 1–23.
Ekman, P., & Friesen, W. V. (1975). Unmaskingthe face. Englewood Cliffs, NJ: Prentice Hall.
Ellis, A. (1962). Reason and emotion in psycho-therapy. New York: Lyle-Stuart.
Frijda, N. H. (1986). The emotions. London: Cam-bridge University Press.
Gonçalves, O. F. (1995). Cognitive narrative psy-chotherapy: The hermeneutic construction ofalternative meanings. In M. J. Mahoney (Ed.),Cognitive and constructivist psychotherapies(pp. xx–xx). New York: Springer.
Greenberg, L. S., & Safran, J. D. (1987). Emotionin psychotherapy: Affects and the process ofchange. New York: Guilford Press.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

ASSESSING PROBLEMATIC STATES 351
Harman, H. H. (1976). Modern factor analysis (3rded.). Chicago: University Press.
Heider, F. (1958). The psychology of interpersonalrelationship. New York: Wiley.
Hermans, H. J. M., & Kempen, H. J. K. (1993). Thedialogical self. Meaning as movement. San Di-ego: Academic Press.
Horowitz, M. J. (1987). States of mind. Configu-rational analysis of individual psychology (2nded.). New York London: Plenum.
Horowitz, M. J. (1991). States, schemas, and con-trol: General theories for psychotherapy inte-gration. J Psychotherapy Integration, 2, 85–102.
Horowitz, M. J., Adler, N., & Kegeles, S. (1988). Ascale for measuring the occurrence of positivestates of mind. Psychosomatic Medicine, 50,477–483.
Horowitz, M. J., Milbrath, C., Ewert, M., &Sonneborn, D. (1994). Clinical patterns of statesof mind in psychotherapy. American Journalof Psychiatry, 151, 1767–1770.
Horowitz, M. J., Milbrath, C., & Stinson, C. H.(1997). Assessing personality disorders. In H. H.Strupp, L. M. Horowitz, & M. J. Lambert (Eds.),Measuring patient changes in mood, anxiety andpersonality disorders (pp. 401–432). Washington,DC: American Psychological Association.
Izard, C. E. (1977). Human emotions. New York:Plenum.
Kelly, G. (1955). The psychology of personal con-structs. New York: Norton.
Labov, W., & Fanshel, D. (1977). Therapeutic dis-course: Psychotherapy as conversation. NewYork: Academic Press.
Le Doux, J. (1996). The emotional brain. NewYork: Simon & Schuster.
Lewis, M. (1992). Shame. The exposed self. NewYork: Free Press.
Liotti, G. (2000). Disorganized attachment mod-els of borderline pathology and evolutionarypsychotherapy. In P. Gilbert & K. Bailey (Eds.),Genes on the couch: Explorations in evolution-ary psychotherapy (pp. 232–256). Hove, En-gland: Brunner-Routledge.
Luborsky, L., & Crits-Christoph, P. (1990). Under-standing transference: The CCRT method. NewYork: Basic Books.
Mancuso, J. C., & Sarbin, T. R. (1983). The self-narrative in the enactment of roles. In T. R.Sarbin & K. Scheibe (Eds.), Studies in socialidentity (pp. 233–253). New York: Praeger.
Mandler, J. (1984). Scripts, stories, and scenes:Aspects of schema theory. Hillsdale, NJ: Erlbaum.
Mergenthaler, E., Freni, S., Giampieri, E., & Ferrari,R. (1998). Regole standardizzate di trascrizionedelle sedute di psicoterapia [Psychotherapy tran-scription standards]. Ricerca in Psicotherapia, 1,29–46.
Modell, A. H. (1984). Psychoanalysis in a new con-text. New York: International University Press.
Neimeyer, R. A. (1995). Client-generated narra-tives in psychotherapy. In R. A. Neimeyer & M.J. Mahoney (Eds.), Constructivism in psycho-therapy. Washington, DC: American Psychologi-cal Association.
Neimeyer, R. A. (2000). Narrative disruptions inthe construction of the self. In R. A. Neimeyer& J. D. Raskin (Eds.), Constructions of disorder(pp. 207–242).Washington, DC: American Psy-chological Association.
Nicoló, G., Mergenthaler, E., Pontalti, I., Semerari,A., Carcione, A., & Catania, D. (2000). Analisidei patterns di Emozione-Astrazione in untrattamento cognitivista: Risultati preliminari[Analysis of emotion-abstraction patterns in acognitive psychotherapy: Preliminary results].Psicoterapia, 6, 67–72.
Nicoló, G., Pontalti, I., Catania, D., Carcione, A.,Dimaggio, G., & Semerari, A. (2001, March).Evaluation of therapeutic cycle model, prob-lematic mental state metacognitive function incognitive psychotherapy: analysis of four psy-chotherapy treatments. Paper presented at themeeting of the Society for Psychotherapy Re-search European Congress, Leiden.
Oatley, K., & Johnson-Laird, P. N. (1987). Towardsa cognitive theory of emotions. Cognition andEmotion, 1, 29–48.
Panksepp, J. (1982). Toward a general psychobio-logical theory of emotions. Behavioral andBrain Sciences, 5, 407–467.
Pribram, K. H., & McGuinness, D. (1975). Arousal,activation, and effort in the control of attention.Psychological Review, 82, 116–149.
Sarbin, T. R. (1986). The narrative as a root meta-phor for psychology. In T. R. Sarbin (Ed.), Nar-rative psychology: The storied nature of humanconduct (pp. 1–27). New York: Praeger.
Sartre, J. P. (1939). Esquisse d’une théorie phéno-menologique des émotions [Sketch for a theory ofemotions]. Paris: Hermann.
Sartre, J. P. (1943). L’Etre et le néant [Being andnothingness]. Paris: Gallimard.
Semerari, A., Dimaggio, G., Carcione, A., & Nicolò,G. (1997). Disturbi somatici e sintonia interper-sonale. Uno studio attraverso la “Griglia di Valuta-zione degli Stati Problematici” [Narrative episodesand grid of problematic states method descrip-tion and manual.] Psicoterapia, 6/7, 117–132.
Shrout, P. E., & Fleiss, J. L. (1979). Intraclass cor-relations: Uses in assessing rater reliability. Psy-chological Bulletin, 86, 420–428.
Spence, D. P. (1982). Narrative truth and histori-cal truth. New York: Norton.
Stiles, W. B., Meshot, C. M., Anderson, T. M., &Sloan, W. W. (1992). Assimilation of problem-atic experiences: The case of John Jones. Psy-chotherapy Research, 2, 81–101.
Toates, F. M. (1980). Animal behavior: A systemapproach. Chichester, England: Wiley.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

352 SEMERARI ET AL.
Tomkins, S. S. (1962). Affect, imagery and con-sciousness, Vol. I. New York: Springer.
Villegas, M. (1992). Análisis del discurso terapeutico[Analysis of therapeutic discourse]. Revista dePsicoterapia, 10–11, 23–66.
Villegas, M., & Ricci, M. (1998). El discurso onirico:Aplicacion de las tecnicas de analisis textual a lossueños en psicoterapia [Dream discourse: Anapplication of text analysis techniques to dreamsin psychotherapy]. Revista de Psicoterapia, 34–35, 31–92.
Weiss, J. (1993). How psychotherapy works? NewYork: Guilford Press.
Weiss, J., Sampson, H., & Mount Zion Psycho-therapy Research Group. (1986). The psycho-analytic process: Theory, clinical observationand empirical research. New York: GuilfordPress.
Young, J. E. (1994). Cognitive therapy for per-sonality disorders: A schema focused approach,revised. Sarasota, FL: Professional ResourcePress.
ZusammenfassungIn diesem Artikel stellen die Autoren den theoretischen Hintergrund, die Entwicklung und die Validierungeiner neuen Ratingskala für psychotherapeutische Prozesse–Grid of Problematic States (GPS)–vor. Er beruhtauf der ‘“States of Mind”-Theorie von Horowitz, die stets wiederkehrende verbale sowie auch nonverbaleErfahrungs- und Verhaltensmuster beschreibt. Bedeutungsvolle Änderungen in den beobachteten Statesweisen gleichzeitig auf therapeutische Veränderung hin. Der GPS wurde zur Anwendung auf Transkriptevon psychotherapeutischen Gesprächen entworfen und ist auf Berichtsepisoden im narrativen Materialdes Patienten gerichtet. In einer ersten Validierung wurde der GPS auf eine vollständig transkribiertekognitive Psychotherapie bei einer depressiven Patientin angewendet. Es konnte gezeigt werden, dasssowohl die Disorganisation als auch die Entwicklung stabiler Konstrukt-Cluster von Gedankengängen,Emotionen und somatischen Wahrnehmungen zuverlässig mit dem GPS erfasst werden können. Die In-terpretation der Ergebnisse ist konsistent mit einer klinischen Bewertung des Falles.
RésuméLes auteurs présentent le fond théorique, le développement, et la validation d’un nouvel instrument decodage du processus psychothérapeutique : Grille d’Etats Problématiques (GPS). La GPS est basée sur lathéorie des états d’esprit de Horowitz qui décrit des patterns récurrents d’expérience et de comportement.Des changements substantiels des états observés indiquent un changement thérapeutique. La GPS estconçue pour des transcriptions de séances de psychothérapie et cible sur des épisodes narratifs dans ledialogue d’un(e) patient(e). Nous avons appliqué la GPS pour une psychothérapie cognitive entièrementtranscrite avec une patiente au diagnostic de dépression majeure modérée. Nous avons démontré que laGPS permettait d’évaluer de manière fidèle la désorganisation, et que le développement de clusters stablesde thèmes de pensée, d’émotions et de sensations somatiques pouvait être évalué de façon fiable.L’interprétation des résultats est consistante avec l’évaluation clinique de la patiente.
ResumenLos autores presentan la fundamentación, el desarrollo y la validación teórica de una nueva herramientapara evaluar el proceso psicoterapéutico: la Grilla de estados problemáticos (GPS). El GPS se basa enla teoría de los estados de la mente de Horowitz que describe patrones recurrentes de experiencia ycomportamiento. Cualquier cambio significativo en los estados observados indica cambio terapéutico.El GPS está diseñado para usar con transcripciones de sesiones psicoterapéuticas y focaliza los episodiosnarrativos habidos en el diálogo con el paciente. Hemos aplicado el GPS a la transcripción completa deuna psicoterapia cognitiva de un paciente diagnosticado como depresivo mayor leve. Demostramosque el GPS podía evaluar confiablemente tanto la desorganización como el desarrollo de grupos establesde constructos de pensamientos temáticos, de emociones y de sensaciones somáticas. La interpretaciónde los resultados es consistente con la evaluación clínica del paciente.
ResumoOs autores apresentam os fundamentos teóricos, o desenvolvimento e a validação de um novo instru-mento de avaliação do processo psicoterapêutico: a Grelha de Estados Problemáticos (GEP). A GEP ébaseada na teoria dos estados mentais de Horowitz, que descreve padrões recorrentes de experiênciase comportamentos. As alterações significativas nos estados observados indicam mudanças terapêuticas.A GEP foi concebida para ser utilizada com transcrições de sessões psicoterapêuticas e foca-se emepisódios narrativos contidos no diálogo do paciente. Aplicámos a GEP a uma transcrição completaduma psicoterapia cognitiva com um paciente diagnosticado com depressão major leve. Demonstrámos
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4

ASSESSING PROBLEMATIC STATES 353
que a GEP poderia avaliar com fidelidade a desorganização e o desenvolvimento de agrupamentosestáveis de temas de pensamento, emoções e sensações somáticas. A interpretação dos resultados éconsistente com as avaliações clínicas dos pacientes.
SommarioGli autori presentano I riferimenti teorici, lo sviluppo e la validazione di un nuovo strumento divalutazione del processo psicoterapeutico: la Griglia degli Stati Problematici (GPS). La GPS (Griglia degliStati Problematici) è basata sulla teoria degli Stati Mentali di Horowitz, che descrive pattern ricorrenti diesperienze e comportamenti. Cambiamenti significativi negli stati osservati segnalano il cambiamentoterapeutico. La GPS è studiata per essere applicata a trascrizioni di sedute di psicoterapia e si focalizzasugli episodi narrativi presenti all’interno del dialogo del paziente. Abbiamo applicato la GPS a trascrizioniintegrali di psicoterapia cognitiva in pazienti con diagnosi di depressione maggiore di grado lieve.Dimostriamo che la GPS potrebbe valutare in modo attendibile la disorganizzazione e che l’evoluzionedi cluster di costrutti stabili di temi di pensiero, emozioni e sensazioni somatiche potrebbero esserevalutati affidabilmente con la GPS stessa. L’interpretazione dei risultati è risultata coerente con lavalutazione clinica del paziente.
Received November 11, 1999Revision received July 25, 2002
Accepted September 26, 2002
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 0
2:10
05
Oct
ober
201
4