asfiksia perinatal
DESCRIPTION
perinatal. asfiksiaTRANSCRIPT
1
Birth asphyxiaDefinition and Causes
PETER G.J. NIKKELSDept. of Pathology UMC Utrecht,
the Netherlands
21st European Congress of PathologySeptember 08-13, 2007Istanbul, TURKEY
Symposium: Birth Asphyxia and Birth Trauma
2
Definition of perinatal asphyxia
What is asphyxia• Definition of the task force of the World Federation of
Neurology Group in 1993:Condition of impaired gas exchange leading, if it persists, to progressive hypoxemia and hypercapnia.
• Added suggestion in 1997:with a significant metabolic acidosis.
3
Perinatal asphyxia
• Criteria used in clinical practice:
– Apgar score (0-3 for > 5 minutes)
– arterial cord blood pH (pH < 7.0)
– base deficit (> -12 -16 mmoll/l)
– late decelerations on foetal monitoring or meconiumstaining
– delayed onset of respiration
– multiorgan involvement (brain, heart, kidney, etc.)
– necessity for resuscitation

4
Perinatal asphyxia• Many different criteria and different cut off points of the
criteria are used to define perinatal asphyxia.• Comparison between different studies difficult.
• Only severe acidemia has predictive value for long-term neurological injury
• A severe metabolic acidosis is associated with multiorgan complications (not a respiratory acidosis).
• Incidence:Umbilical artery base deficit > 12 mmoll/l 2%Umbilical artery base deficit > 16 mmoll/l 0.5%
5
Perinatal asphyxia• However, metabolic acidosis determined at the time of
sampling does not necessarily reflect the severity of asphyxial exposure to the foetus.– Duration of asphyxia not known– Nature of insult not known (continuous or intermittent)
• Foetal response influences the importance of the asphyxial exposure.– Response: centralization of the foetal circulation
• (blood to brain, heart and adrenals)
• If hypoxia sustains: cardiovascular decompensation
6
Perinatal asphyxia
• Sustained hypoxia: cardiovascular decompensation: more severe brain damage, cardiac and renal dysfunction and respiratory complications.
• 2% of newborns has been exposed to an asphyxial event
• Majority of events is mild to moderate with little or no long-term significance
• Criteria used: cerebral, cardiac, renal and respiratory evaluation in first days after birth
7
Perinatal asphyxia
What is causing asphyxia?
Disturbed delivery of oxygen or an increased demand, transient or continuous, acute and/or chronic.
• Maternal factors• Maternal diseases• Maternal anaemia• Cigarette or drug abuse
• Multiple pregnancy (mono- or bichorionic)• Foetal factors• Placenta and umbilical cord problems
8
Perinatal asphyxiaA disturbed delivery of oxygen is often caused by placental
and/or umbilical cord pathology
9
Perinatal asphyxiaDelivery of oxygen in the placenta is by diffusion
Dependent on:
– Diffusion distance / Placental membrane distance
– Maternal blood flow
– Foetal blood flow
– Placental perfusion
– Surface area
– Metabolic activity of the placenta(placenta uses 50% of oxygen delivered to the foetus)
10
Perinatal asphyxiaDisturbed oxygen delivery, acute and/or chronic
1. Not enough or loss of placental parenchyma
2. Diffusion distance too large between maternal and foetal circulation
3. Disturbance in the connection between foetus and placenta, umbilical cord pathology
4. Miscellaneous, e.g. blood loss
Increased demand , acute and/or chronic
1. Diabetes mellitus
2. Infection
11
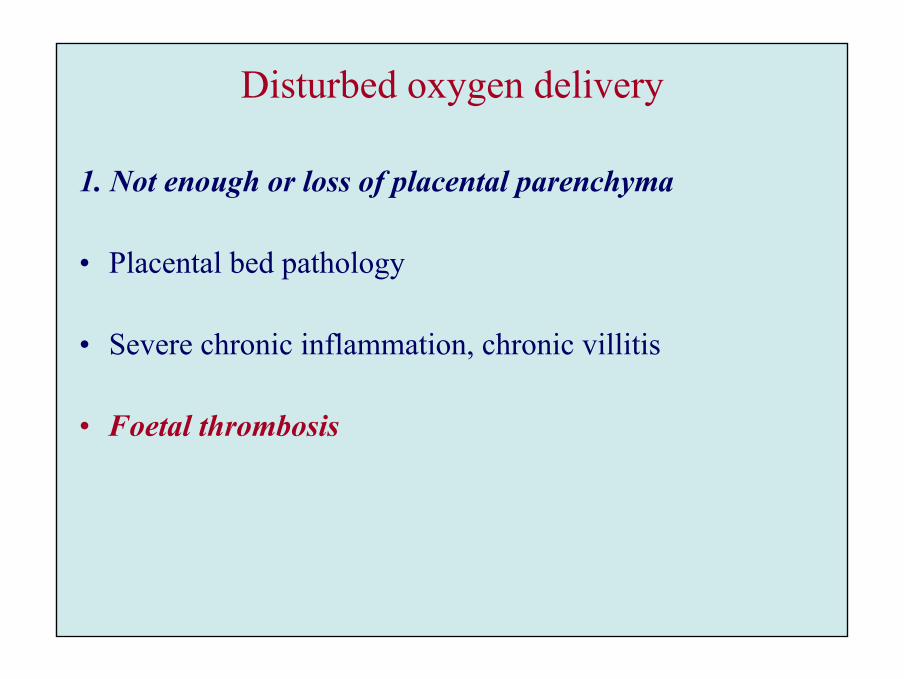
Disturbed oxygen delivery
1. Not enough or loss of placental parenchyma
• Placental bed pathology
• Severe chronic inflammation, chronic villitis
• Foetal thrombosis
12
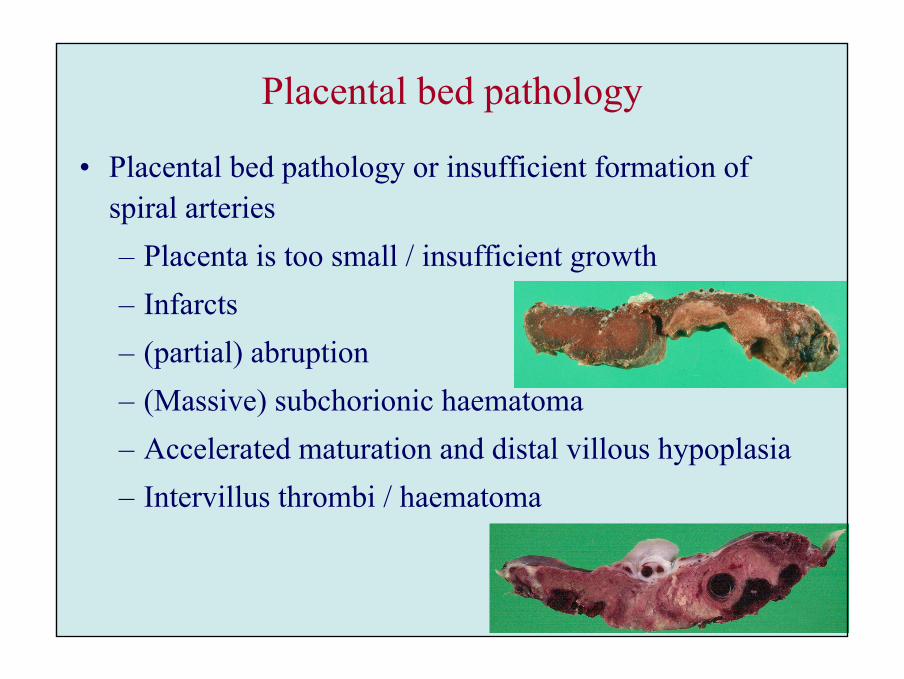
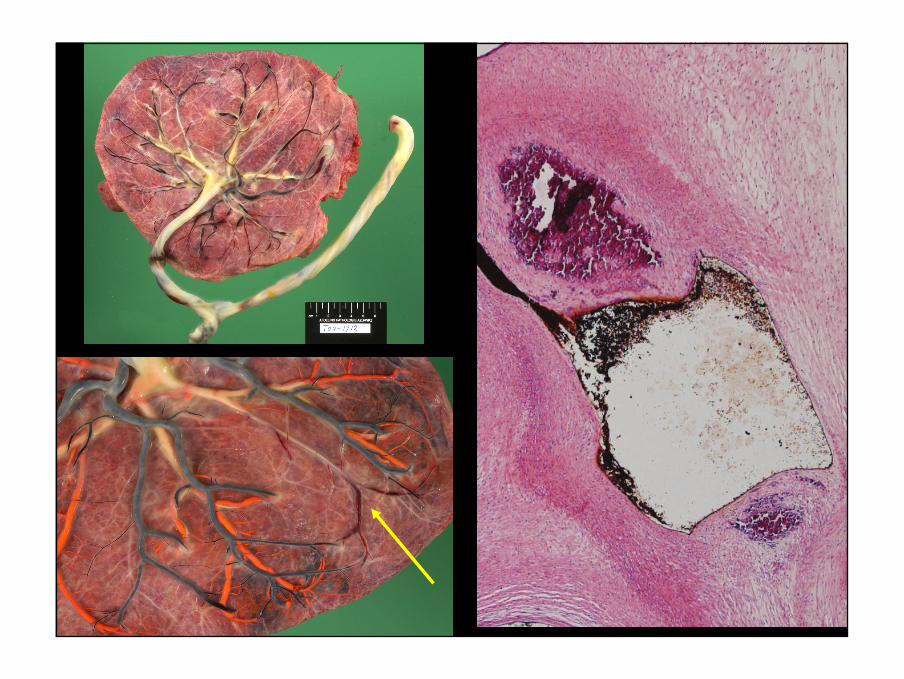
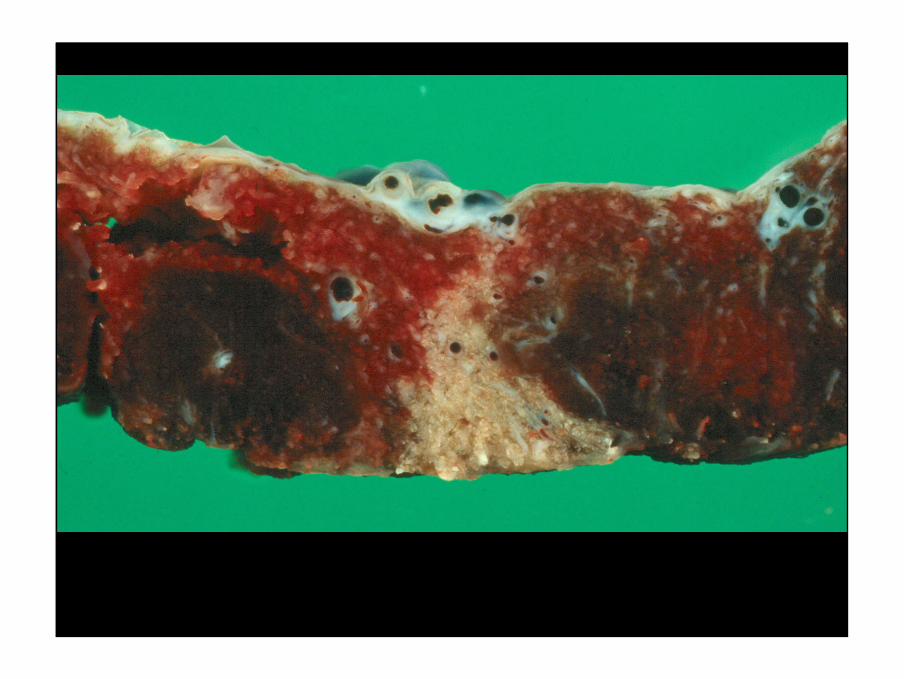
Placental bed pathology
• Placental bed pathology or insufficient formation of spiral arteries– Placenta is too small / insufficient growth– Infarcts– (partial) abruption– (Massive) subchorionic haematoma– Accelerated maturation and distal villous hypoplasia– Intervillus thrombi / haematoma
13
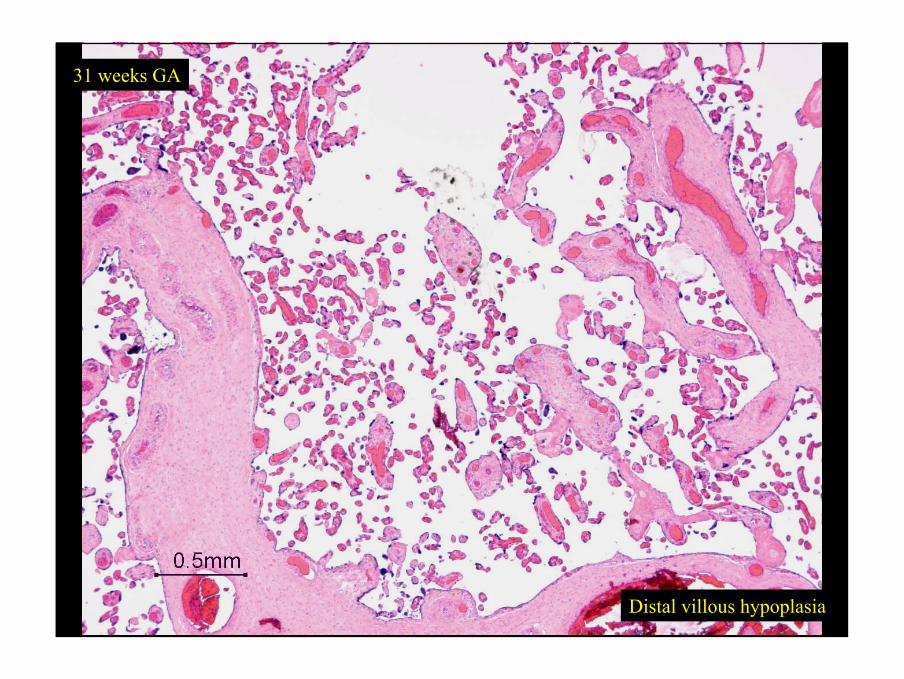
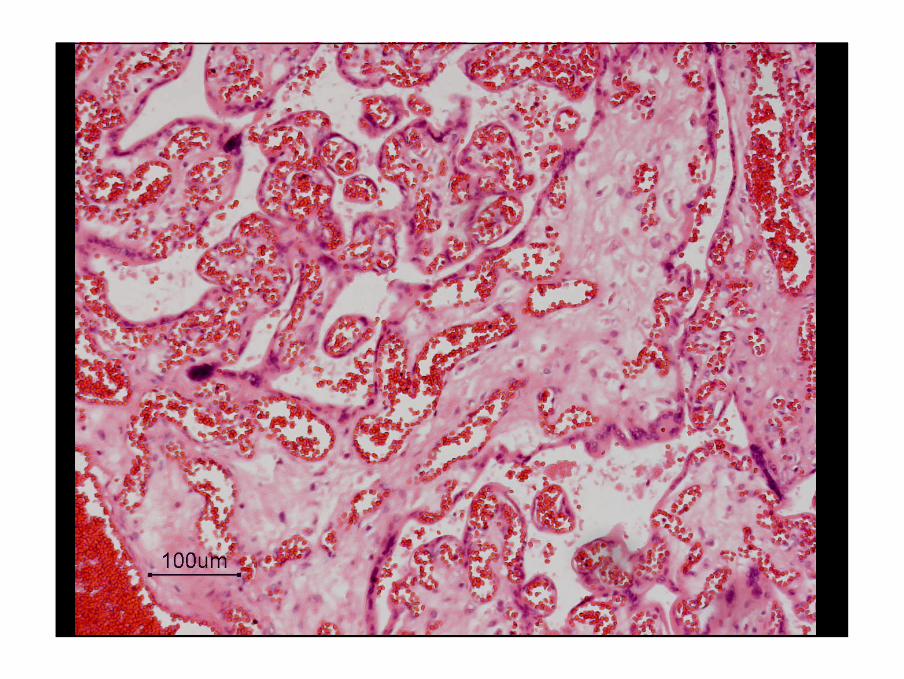
Placental bed pathologyAccelerated maturation histology• Premature formation of terminal villi with syncytio-
vascular membranes• Stem villi with aspect normal for pregnancy duration• Distal villous hypoplasia with long slender villi and
increased space between villi
• Hyperchromasia of trophoblast• Increased syncytial knotting
14
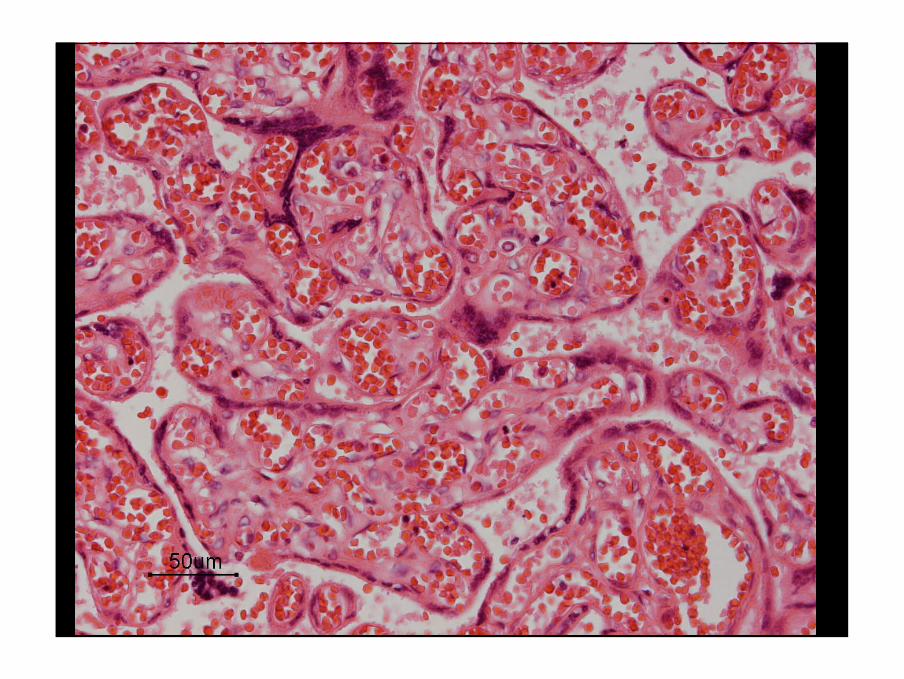
Distal villous hypoplasia
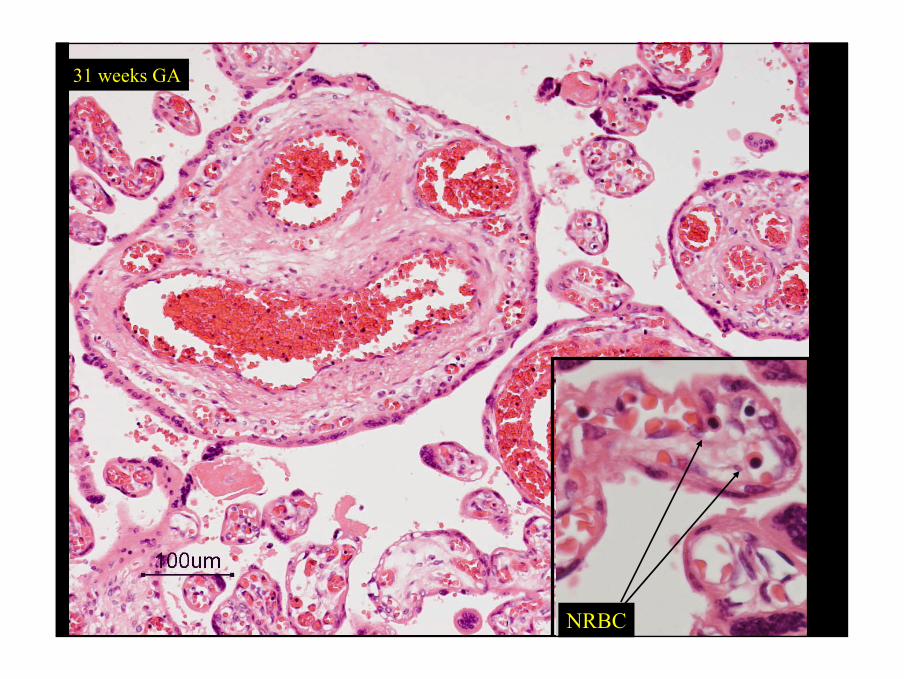
31 weeks GA
15
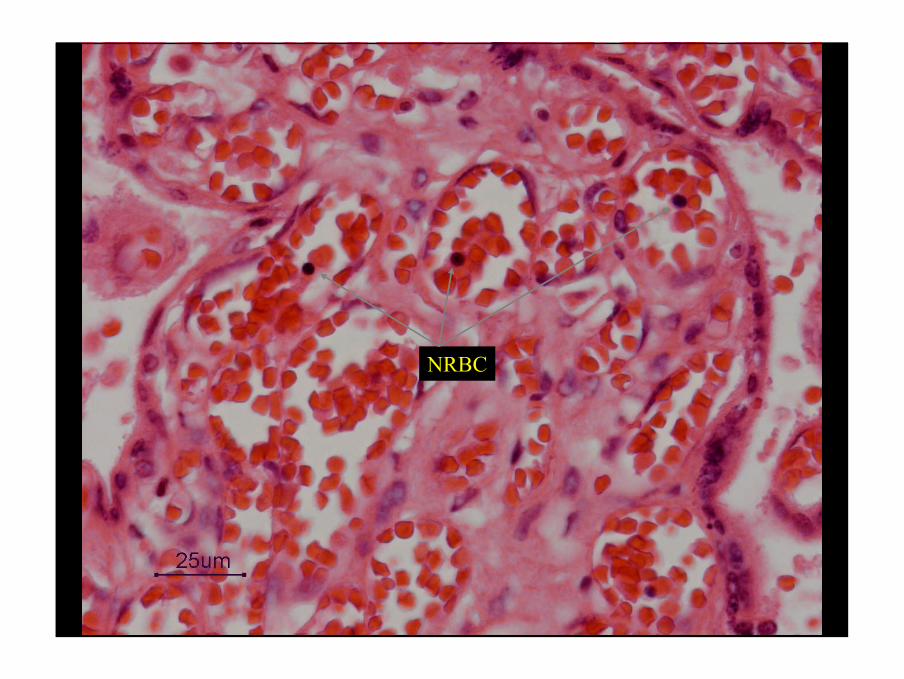
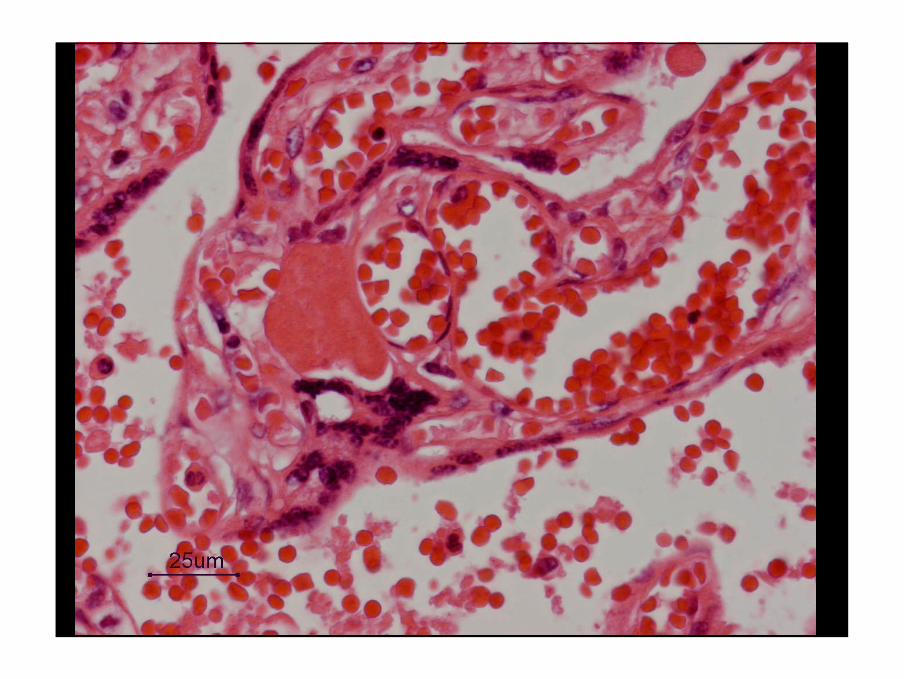
NRBC
31 weeks GA
16
Disturbed oxygen delivery
1. Not enough or loss of placental parenchyma
• Placental bed pathology
• Severe chronic inflammation, chronic villitis
• Foetal thrombosis
17
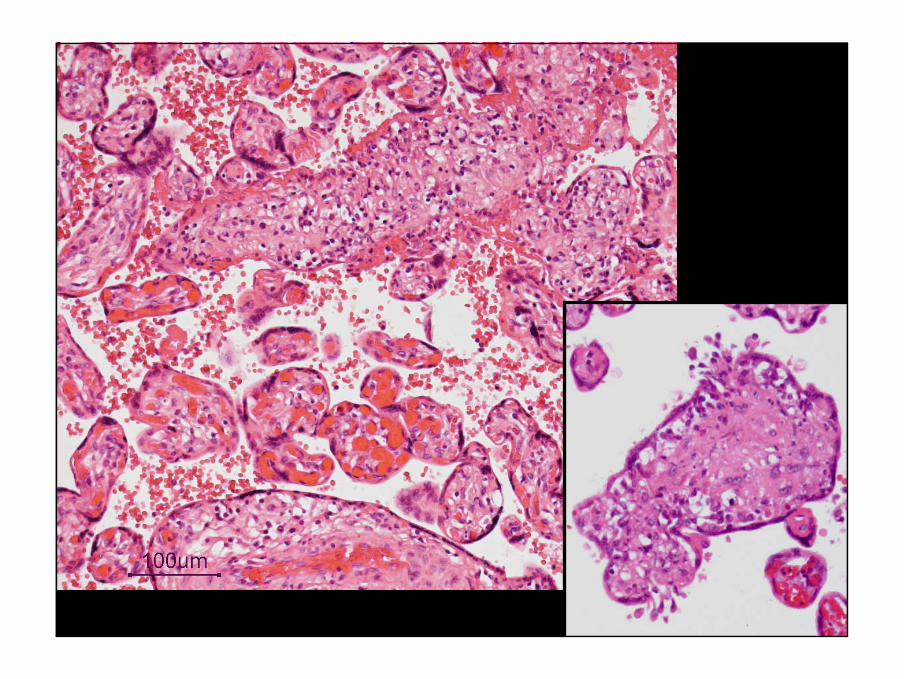
Loss of placental parenchyma
Severe chronic villitis
• Destruction of villi, less mature villi
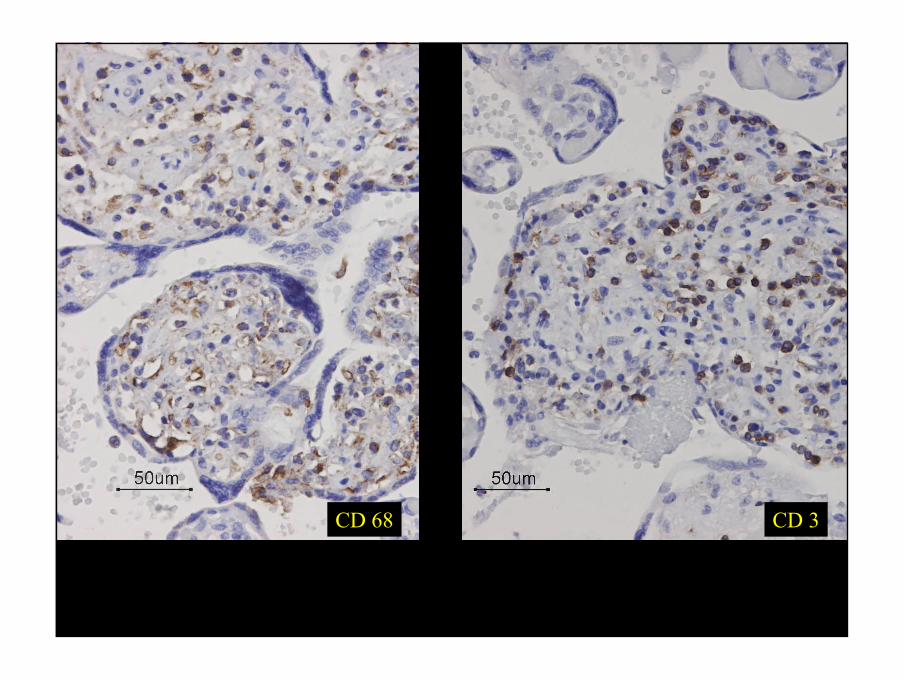
• Infiltrate with macrophages and T-cells
• High recurrence risk of IUGR and IUFD
– Recently some case reports with favourable outcome after treatment with corticosteroids and antithrombotics
Boog et al. J Gynecol Obstet Biol Reprod (Paris). 2006 Jun;35(4):396-404. [Combining corticosteroid and aspirin for the prevention of recurrent villitis or intervillositis of unknown etiology]
18
19
CD 3CD 68
20
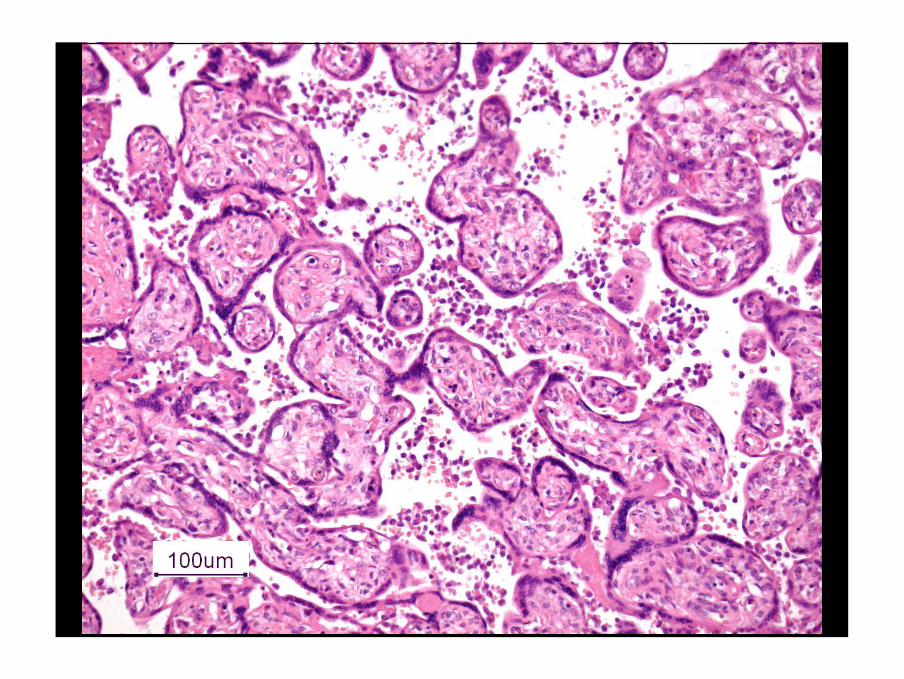
”Loss of placental parenchyma”
Chronic intervillositis
• Massive histiocytic infiltrate in maternal compartment
• Perinatal mortality 29%, IUGR 77%
• High recurrence risk of abortion, IUGR and IUFD
– Recently some case reports of favorable outcome aftertreatment with corticosteroids and antitrombotics
Boog et al. J Gynecol Obstet Biol Reprod (Paris). 2006 Jun;35(4):396-404. [Combining corticosteroid and aspirin for the prevention of recurrent villitis or intervillositis of unknown etiology]
21
22

23
CD 68 CD 3
24
Disturbed oxygen delivery
1. Not enough or loss of placental parenchyma
• Placental bed pathology
• Severe chronic inflammation, chronic villitis
• Foetal thrombosis

25
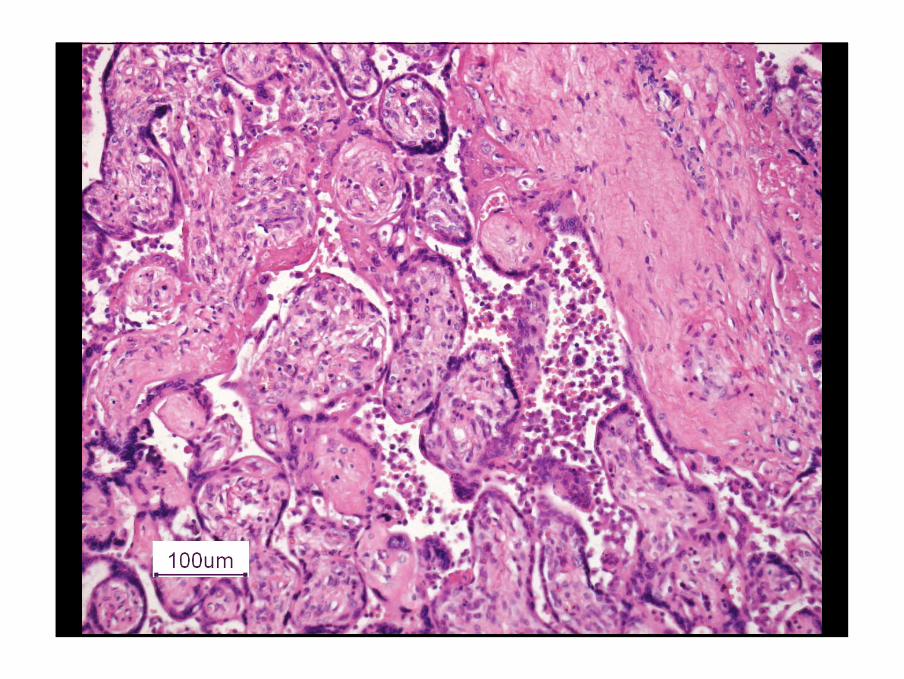
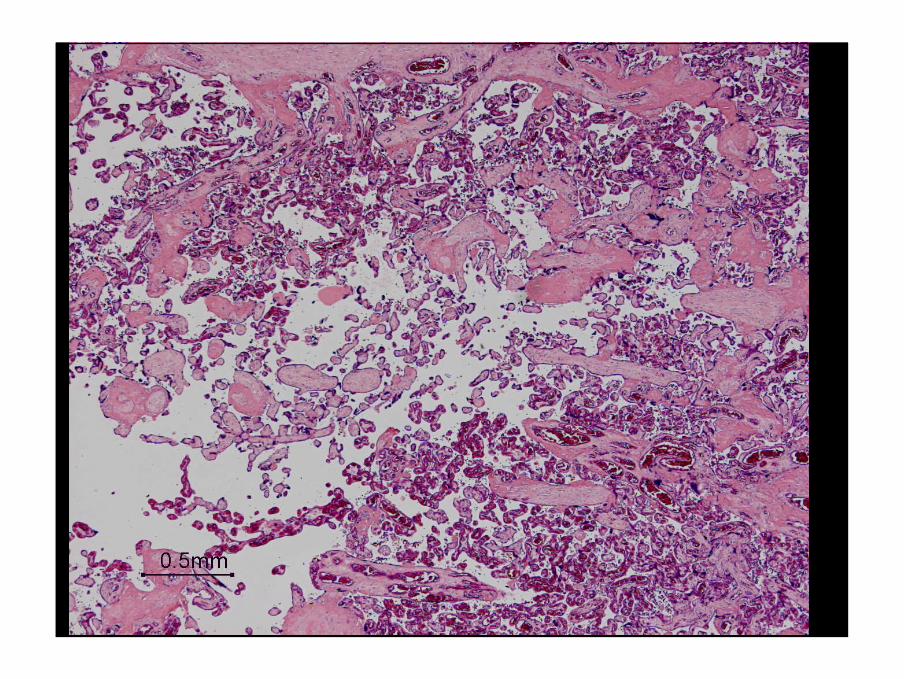
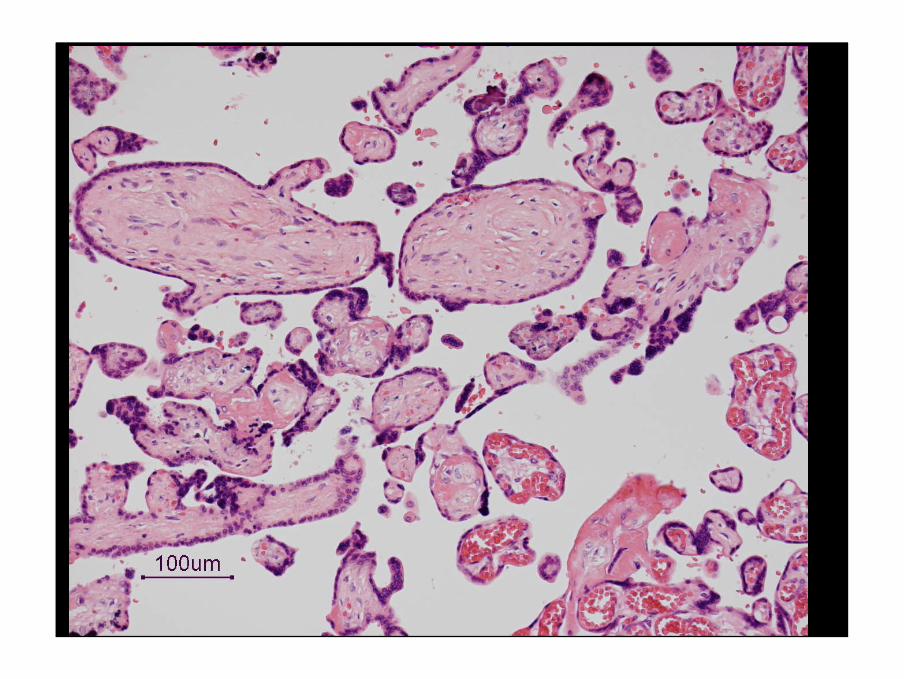
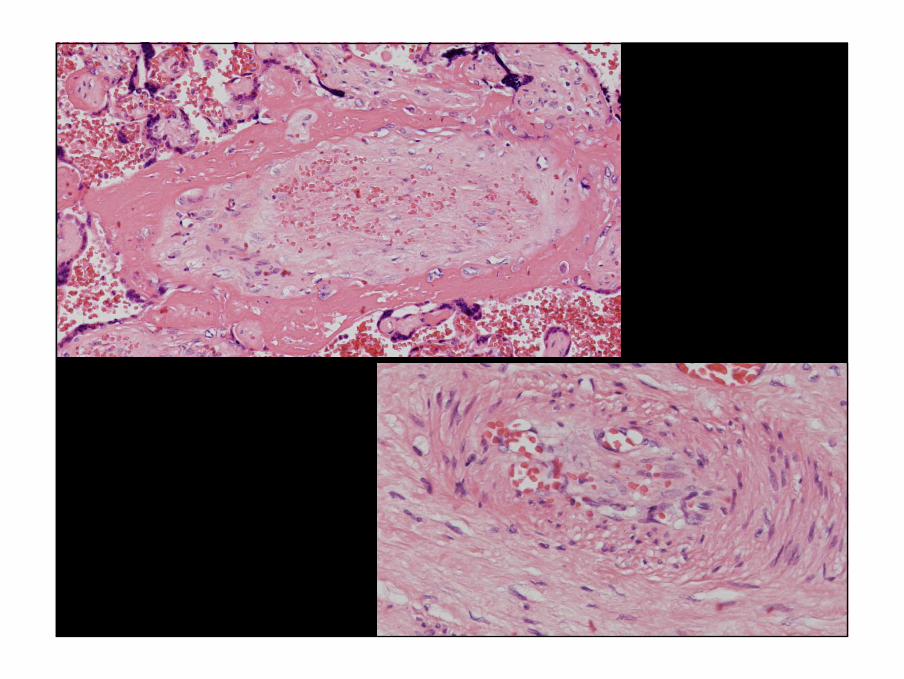
Loss of parenchyma, foetal trombosis
• Groups of avascular villi
• Histology similar as in IUFD
• Incidence
– Normal placenta’s 2%
– Placenta’s with overcoiled cord 20%
– Pre-eclampsia 20-30%
– Macrosomia without DM 30-40%
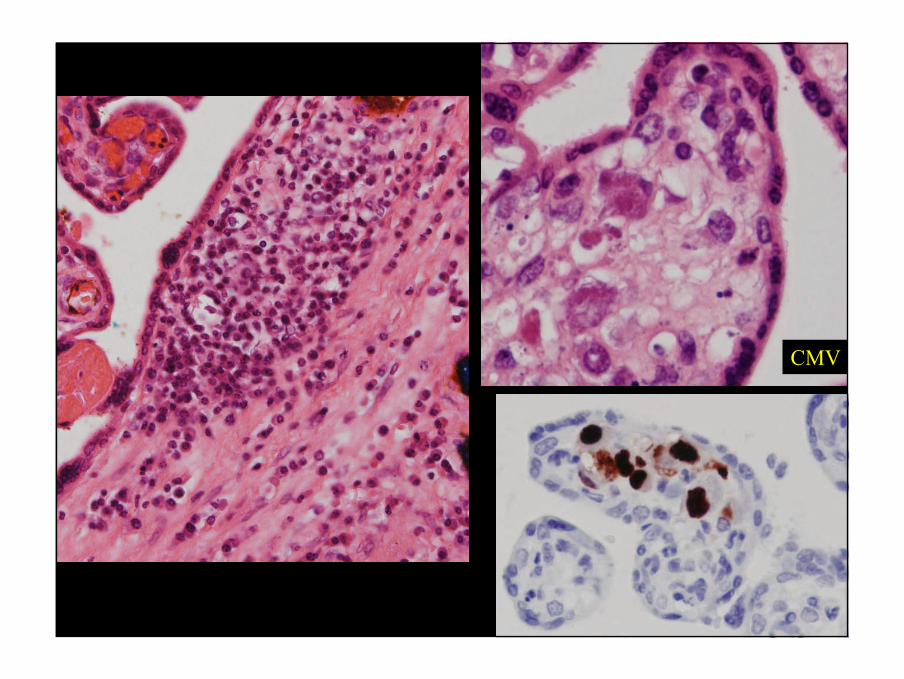
• Occasionally in association with CMV or trombophiliadisorder
26
27
28
29
30
31
CMV
32
Perinatal asphyxiaDisturbed oxygen delivery:
1. Not enough or loss of placental parenchyma
2. Diffusion distance too large between maternal and foetal circulation
3. Disturbance in the connection between foetus and placenta, umbilical cord pathology
4. Miscellaneous, e.g. blood loss
Increased demand
1. Diabetes mellitus
2. Infection
33
Disturbed oxygen delivery
2. Diffusion distance too large between maternal and
foetal circulation
• Massive perivillous fibrin deposition /gitter infarct
• Defective placental maturation
34
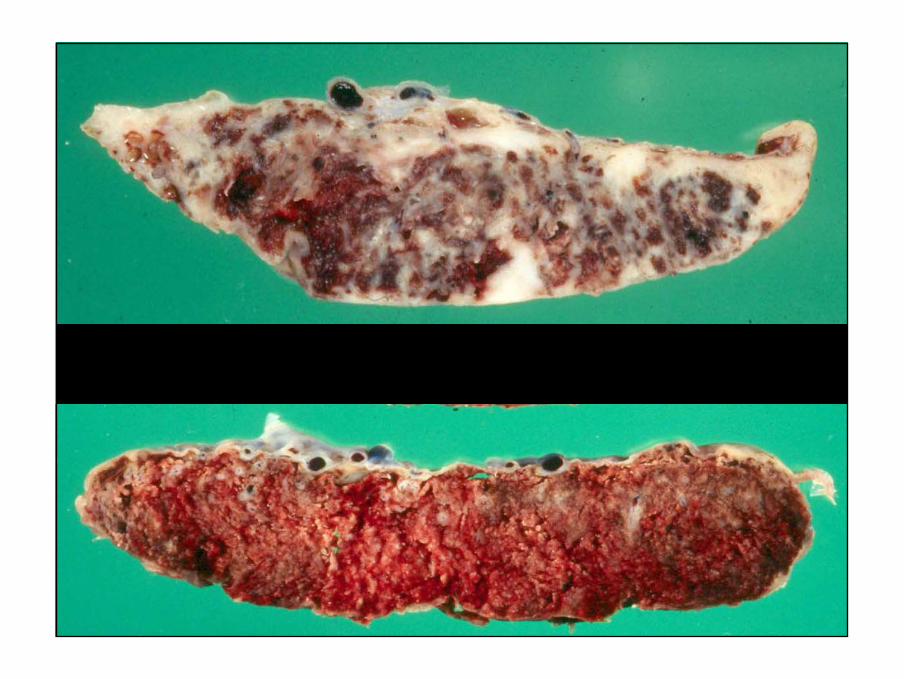
Diffusion distance too long, fibrin
Gitter infarct, maternal floor infarct
• Massive perivillous fibrin deposition
• High recurrence risk
• High risk of IUGR and IUFD
• Sometimes associated with VUE
35
36
37
38
Disturbed oxygen delivery
2. Diffusion distance too large between maternal and
foetal circulation
• Massive perivillous fibrin deposition /gitter infarct
• Defective placental maturation
39
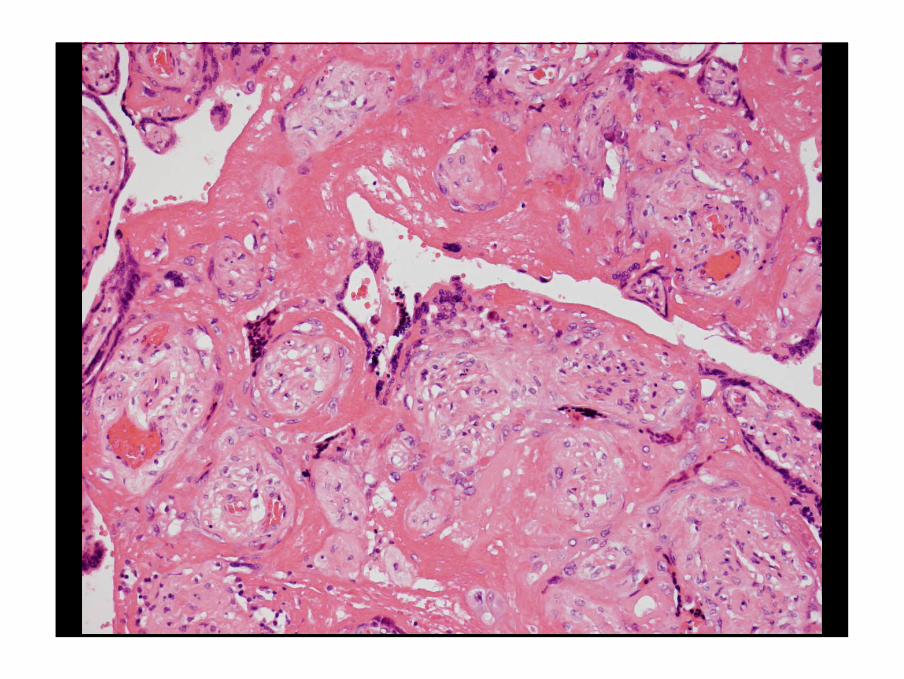
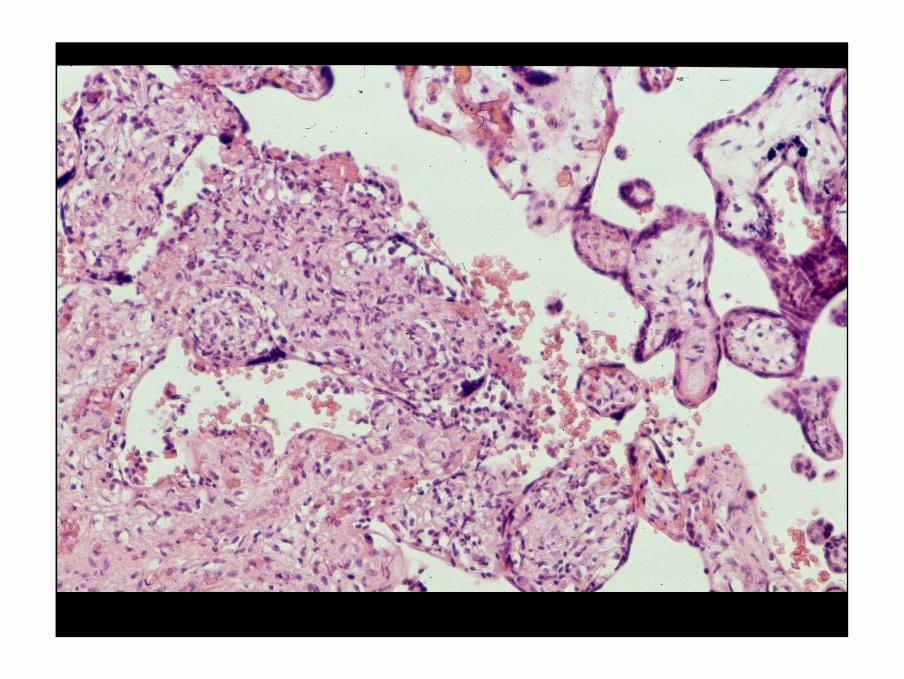
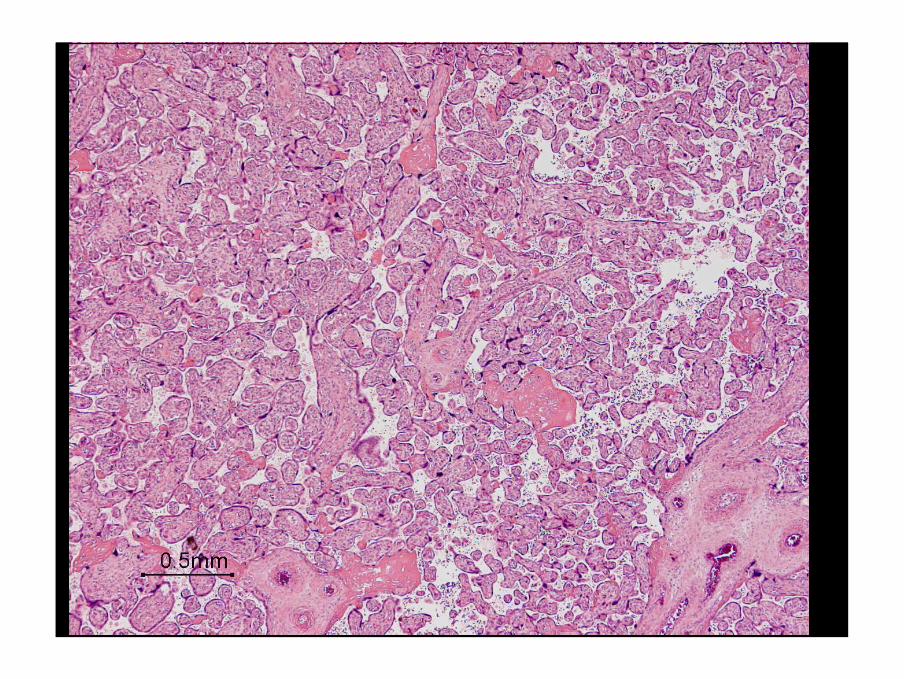
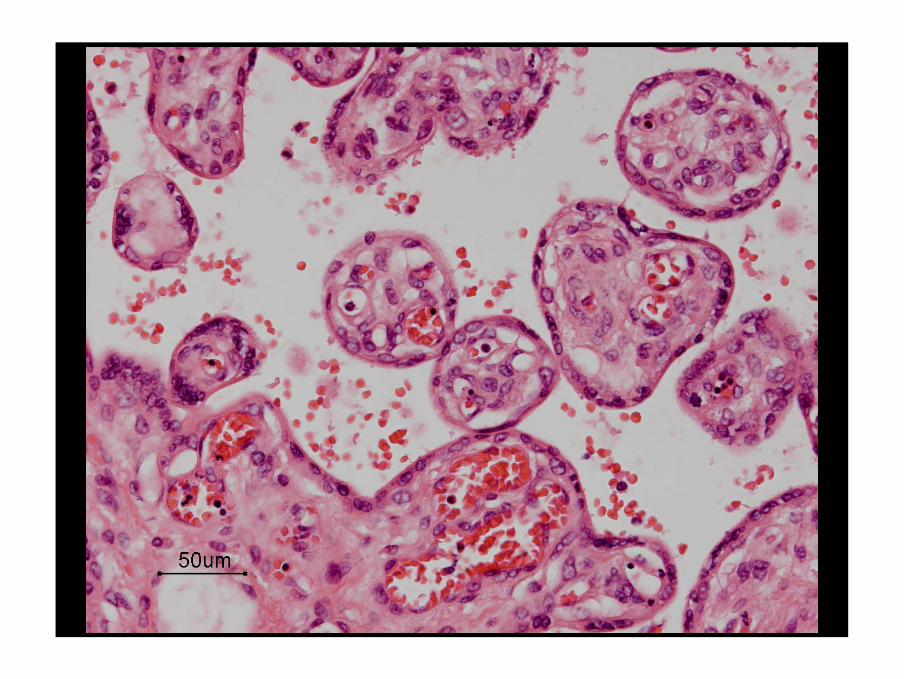
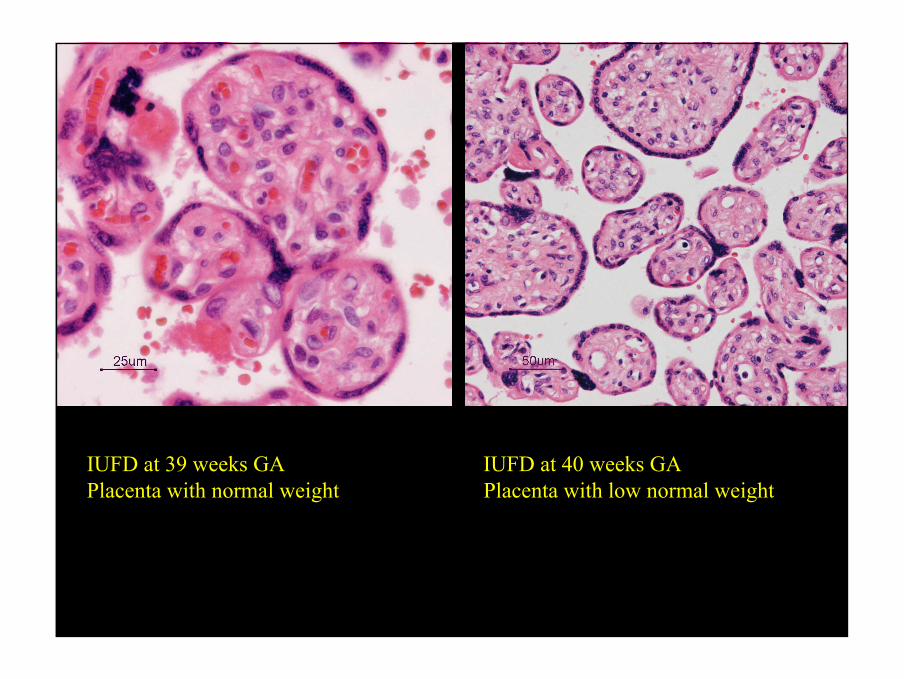
Diffusion distance too long, maturation
Defective placental maturation
• Absence of terminal villi, no syncytio-vascularmembranes
• Occurs after 35-36 weeks GA
• No IUGR
• Severe hypoxia and increase of NRBC’s at the end of pregnancy
Stallmach et al. Rescue by birth: defective placental maturation and late fetal mortality. Obstet Gynecol. 2001 Apr;97(4):505-9.
40
41
42
IUFD at 39 weeks GA IUFD at 40 weeks GAPlacenta with normal weight Placenta with low normal weight
43
Perinatal asphyxiaDisturbed oxygen delivery:
1. Not enough or loss of placental parenchyma
2. Diffusion distance too large between maternal and foetal circulation
3. Disturbance in the connection between foetus and placenta, umbilical cord pathology
4. Miscellaneous, e.g. blood loss
Increased demand
1. Diabetes mellitus
2. Infection
44
Disturbed oxygen delivery
3. Disturbance in the connection between foetus and placenta, umbilical cord pathology
• Too short, too long
• Knots
• Strangulation
• Thrombosis
• Haemangioma
• Meconium induced necrosis
• Coiling
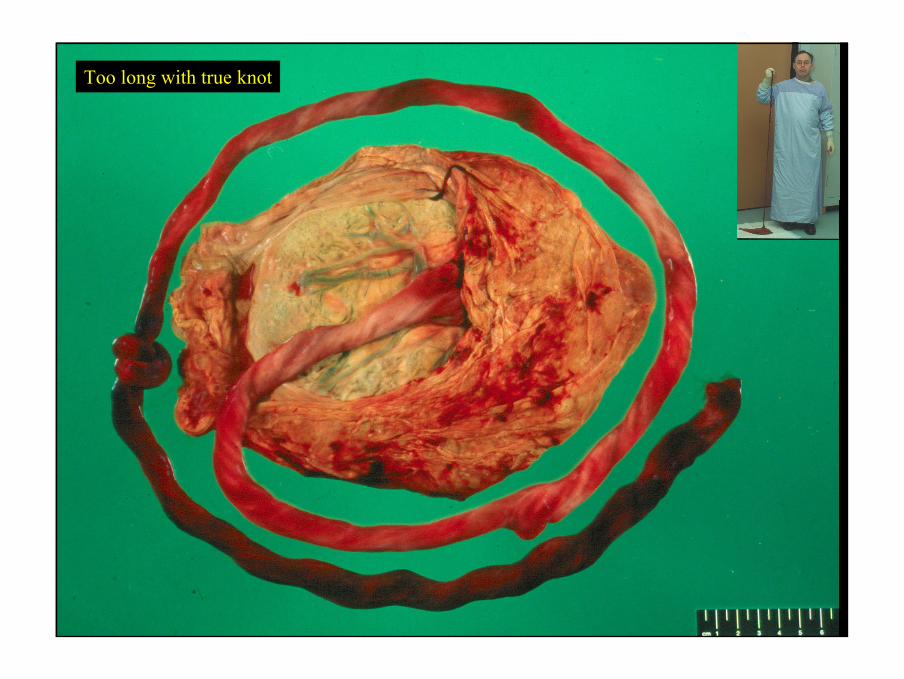
45
Too long with true knot
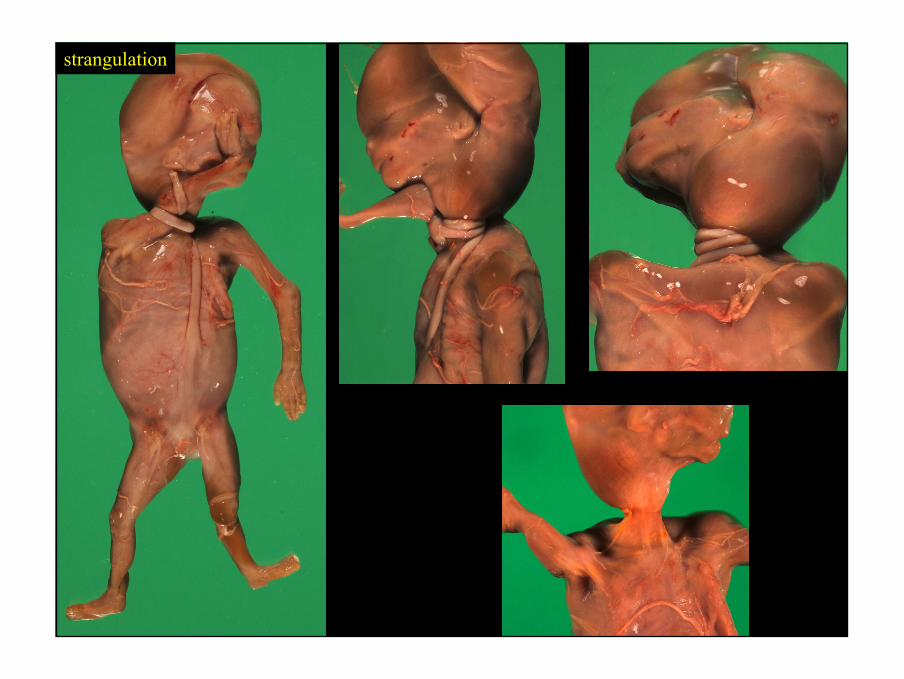
46
strangulation
47
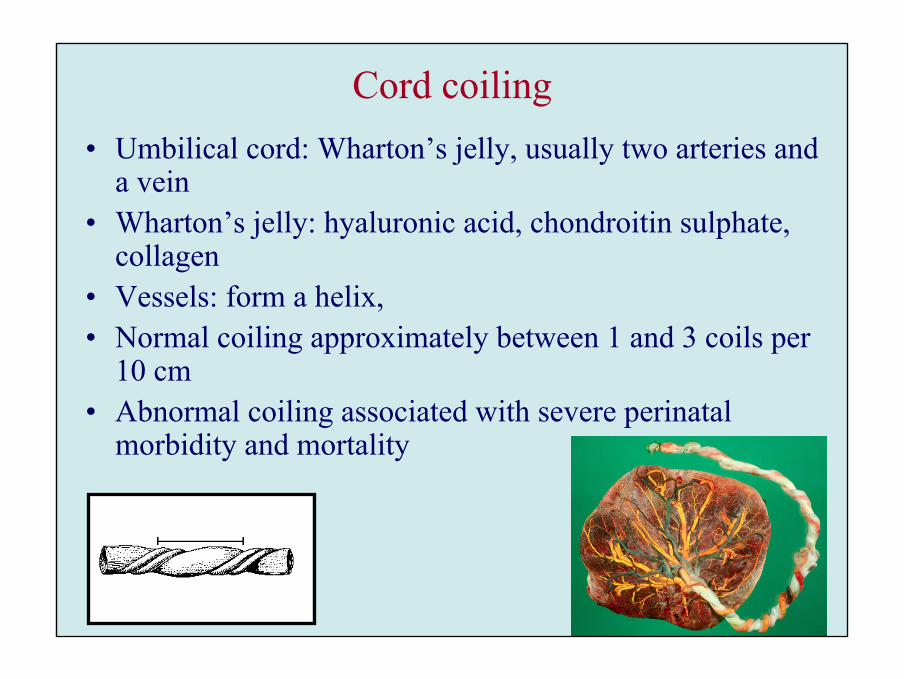
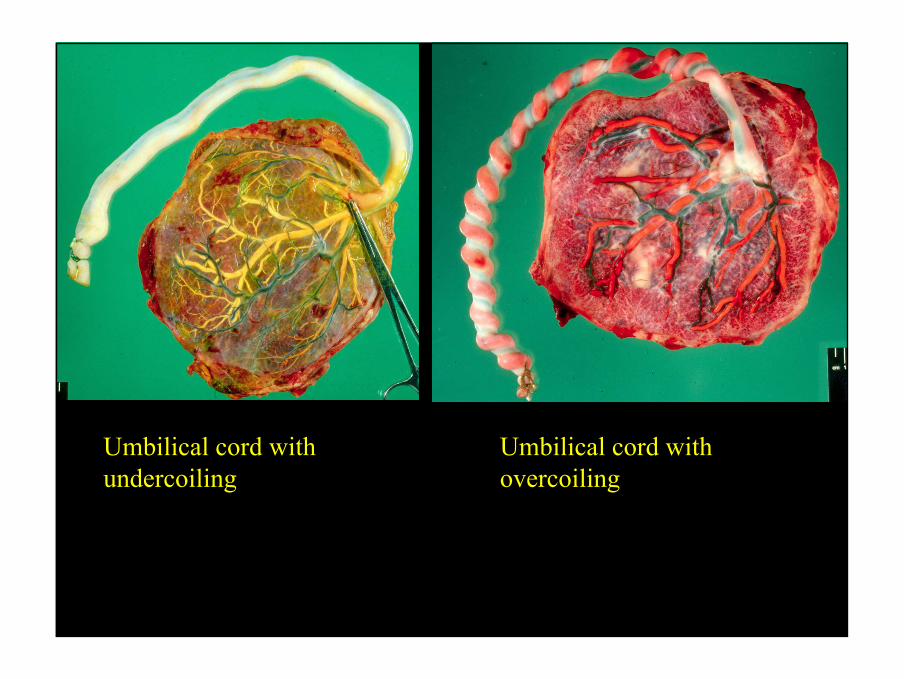
Cord coiling• Umbilical cord: Wharton’s jelly, usually two arteries and
a vein• Wharton’s jelly: hyaluronic acid, chondroitin sulphate,
collagen• Vessels: form a helix,• Normal coiling approximately between 1 and 3 coils per
10 cm• Abnormal coiling associated with severe perinatal
morbidity and mortality
48
Umbilical cord withundercoiling
Umbilical cord withovercoiling
49
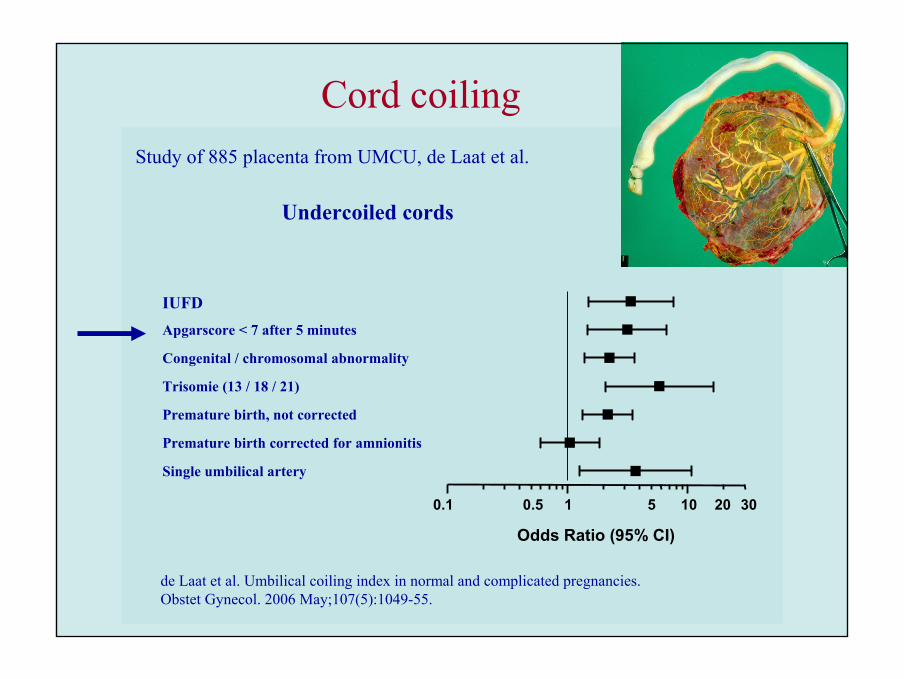
Cord coiling
0.1 1 10
Single umbilical artery
Premature birth corrected for amnionitis
Premature birth, not corrected
Trisomie (13 / 18 / 21)
Congenital / chromosomal abnormality
Apgarscore < 7 after 5 minutes
IUFD
Odds Ratio (95% CI)
20 300.5 5
Undercoiled cords
Study of 885 placenta from UMCU, de Laat et al.
de Laat et al. Umbilical coiling index in normal and complicated pregnancies.Obstet Gynecol. 2006 May;107(5):1049-55.
50
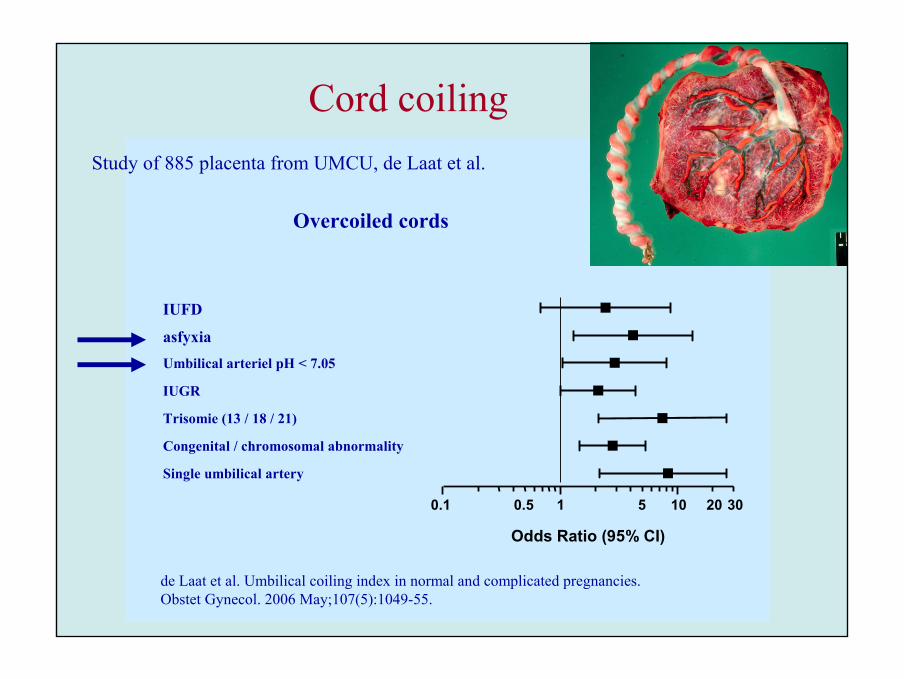
Cord coiling
1 100.1
Single umbilical artery
Congenital / chromosomal abnormality
Trisomie (13 / 18 / 21)
IUGR
Umbilical arteriel pH < 7.05
asfyxia
IUFD
Odds Ratio (95% CI)
20 300.5 5
Overcoiled cords
de Laat et al. Umbilical coiling index in normal and complicated pregnancies.Obstet Gynecol. 2006 May;107(5):1049-55.
Study of 885 placenta from UMCU, de Laat et al.
51
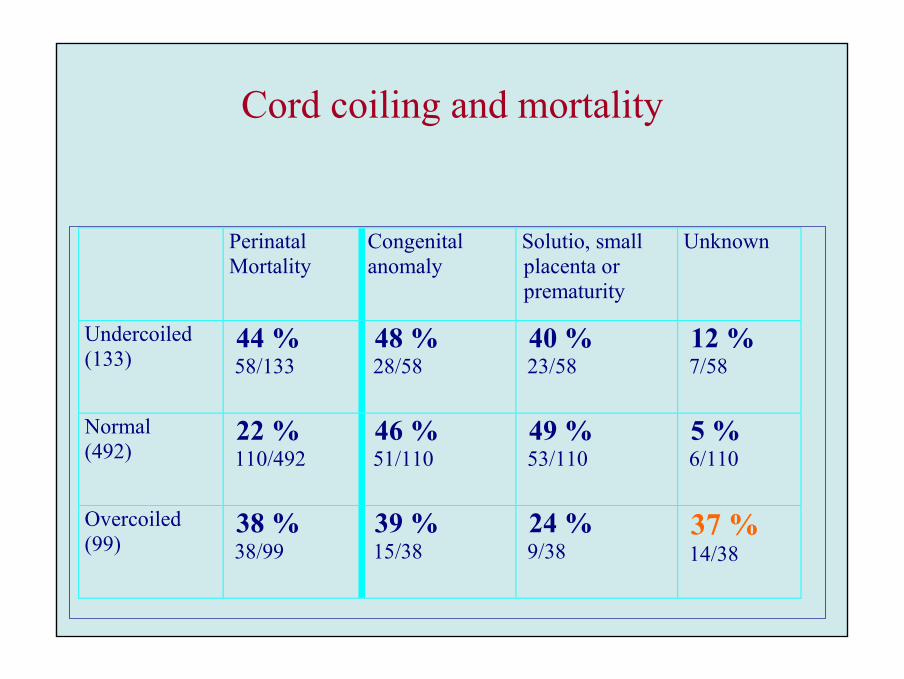
Perinatal Mortality
Congenital anomaly
Solutio, small placenta or prematurity
Unknown
Undercoiled (133)
44 % 58/133
48 % 28/58
40 % 23/58
12 % 7/58
Normal (492)
22 % 110/492
46 % 51/110
49 % 53/110
5 % 6/110
Overcoiled (99)
38 % 38/99
39 % 15/38
24 % 9/38
37 % 14/38
Cord coiling and mortality
52
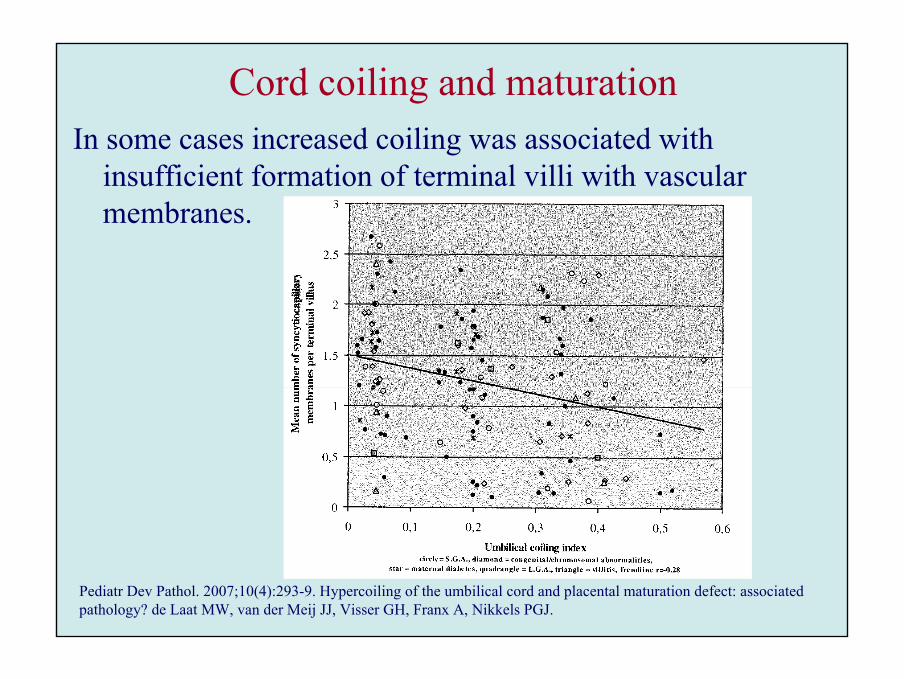
Cord coiling and maturationIn some cases increased coiling was associated with
insufficient formation of terminal villi with vascular membranes.
Pediatr Dev Pathol. 2007;10(4):293-9. Hypercoiling of the umbilical cord and placental maturation defect: associated pathology? de Laat MW, van der Meij JJ, Visser GH, Franx A, Nikkels PGJ.
53
Perinatal asphyxiaDisturbed oxygen delivery:
1. Not enough or loss of placental parenchyma
2. Diffusion distance too large between maternal and foetal circulation
3. Disturbance in the connection between foetus and placenta, umbilical cord pathology
4. Miscellaneous, e.g. blood loss
Increased demand
1. Diabetes mellitus
2. Infection
54
Perinatal asphyxiaDisturbed oxygen delivery:
1. Not enough or loss of placental parenchyma
2. Diffusion distance too large between maternal and foetal circulation
3. Disturbance in the connection between foetus and placenta, umbilical cord pathology
4. Miscellaneous, e.g. blood loss
Increased demand
1. Diabetes mellitus
2. Infection

55
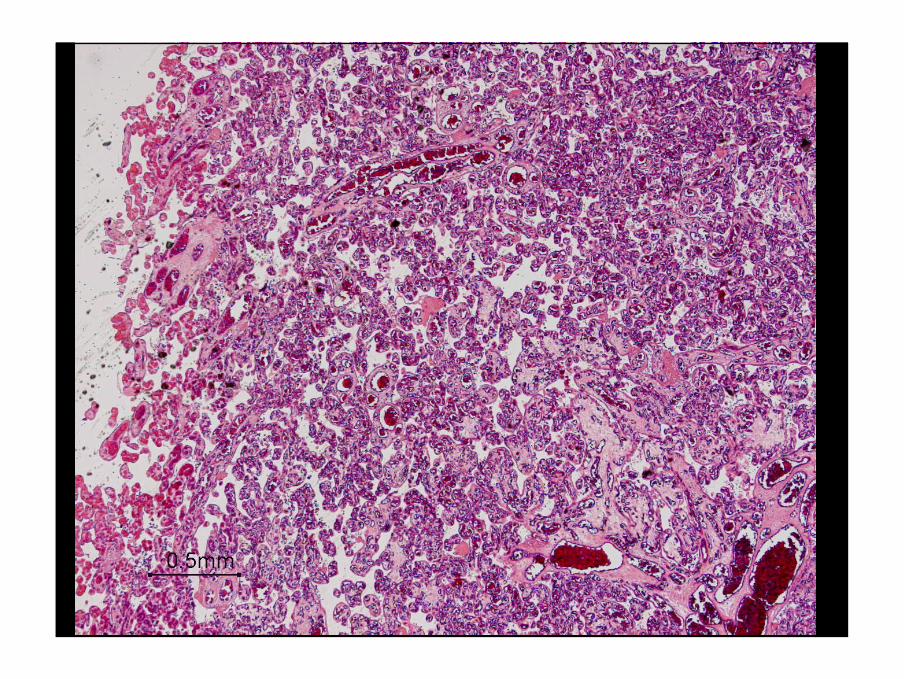
Increased demandDiabetes mellitus
Placental abnormalities associated with DM
• decreased maturation with decreased formation of terminal villi
• groups of immature villi and hydropic villi can be found
• increase of NRBCs
• other DM associated abnormalities are chorangiosis and fibrinoid necrosis of villous stroma
• (Less optimal delivery of oxygen by maternal hemoglobin)
56
57
58
59
NRBC
60
61
Perinatal asphyxiaDisturbed oxygen delivery:
1. Not enough or loss of placental parenchyma
2. Diffusion distance too large between maternal and foetal circulation
3. Disturbance in the connection between foetus and placenta, umbilical cord pathology
4. Miscellaneous, e.g. blood loss
Increased demand
1. Diabetes mellitus
2. Infection
62
63
HAVE FUN WITH YOUR PLACENTASPETER NIKKELS