arthroscopic evaluation of the synovial lining before and after open synovectomy of the knee joint...
TRANSCRIPT

Scand J Rheumatology 19: 193-201, 1990
Arthroscopic Evaluation of the Synovial Lining before and after Open Synovectomy of the Knee Joint in Patients with Chronic Inflammatory Joint Diseases
A. C. PAUS and J. A. PAHLE Oslo Sanitetsforening Rheumatism Hospiral, Oslo, Norway
Paus AC, Pahle JA. Arthroscopic evaluation of the synovial lining before and after open synovectomy of the knee joint in patients with chronic inflammatory joint diseases. Scand J Rheumatology 1990; 19: 193-201.
Twenty-eight patients with chronic inflammatory joint diseases had arthroscopy immedi- ately before synovectomy of the knee joint and 6 and 12 months postoperatively. In patients with moderate and/or severe synovitis of the knee joint all of the synovial membrane is involved in the disease process. Resynovitis (synovitis of the regenerated synovial membrane after synovectomy), however, is patchy and if biopsy should be indicated, arthroscopic guidance is advocated. Following synovectomy there is a recur- rence of mild synovitis of varying degree in some cases with an increase in resynovitis between 6 and 12 months. The level of synovitis at 12 months was, however, markedly less than at synovectomy (p<O.OI). Similar development was found both in histopathology and immunohistopathology after synovectomy. Arthroscopic examination of the synovial membrane in chronic inflammatory disease of the knee joints gives valuable information of the seventy and the longitudinal changes of synovitis. A simple method of scoring is described and is imperative when comparing patients or groups of patients and when doing longitudinal arthroscopic studies. The method was used both at arthroscopy and at subsequent synovectomy giving a highly significant correlation (p<O.OOI).
Key words: arthroscopy, chronic inflammatory joint diseases, rheumatoid arthritis, juve- nile rheumatoid arthritis, knee joint synovectomy. A . C. Paus, Oslo Sanitetsforening Rheumatism Hospital, Akersbakken 27, N-0172 Oslo I , Norway.
Arthroscopy is an established diagnostic method for disorders of the knee joint both in children and adults. There is some information in the literature about arthroscopy in rheumatic disease. There are studies where the value of synovial biopsy is discussed but with incomplete descriptions of the synovial membrane (1, 2, 3). Lindblad (4) has made a thorough arthroscopic description of the synovial membrane in various arthritides. The literature on arthroscopy in children (5 , 6, 7) concentrates on technical problems and diagnosis in connection with traumatology. Arthroscopy in children with rheumatic dis- eases has been described (8), but again with incomplete description of the synovial membrane.
It has not been possible to find any discussion in the literature of the arthroscopic findings following synovectomy.
When describing inflammatory changes of the synovial membrane, it is important to have a system which makes possible the comparison of different areas in one joint, comparison of different patients, longitudinal studies in each patient and groups of patients.
The aim of this study is t o compare the arthroscopic descriptions of the synovial lining immediately prior t o synovectomy with the findings at synovectomy, and 6 and 12 months following synovectomy. Further, in order to select areas for biopsies, it should be studied whether any particular area is liable to redevelop inflammatory changes.
13 -908143
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.

Scand J Rheumatology 19 194 A . C. Paus and J . A . Pahle
Parallel studies of the development of histopathology and irnmunohistopathology will be published separately (9, 10).
MATERIALS AND METHODS Patients The main criterium for selection of patients to this study, was the hospital’s indication for synovec- tomy of the knee joint. This is “synovitis without adequate effect of conservative treatment for six months or more, or danger of destruction of cartilage, bone or ligaments or danger of growth disturbances”. All the patients thus had active synovitis in the selected joint.
All patients admitted in 1985 for synovectomy of the knee joint were asked their consent to be included in the study. For patients under 18 years, both the patient and the parents had to consent. Children under 10 years of age were excluded from the study because of their difficulties in comprehending what consent involved and the possible technical problems with biopsies and photo- graphy at arthroscopy. There was no further selection. Thirty-three consecutive patients were asked their consent and 28 agreed. The patient characteristics are found in Table 1.
Of the 28 patients included in the study, 4 did not want any further arthroscopies after synovec- tomy. Of the remaining 24 patients, arthroscopy was done in 19 patients 6 months and 23 patients 12 months after synovectomy.
Equipment The arthroscopic equipment was Carl Storz Arthroscope with 5 mm sheath, a Stryker Camera and a Carl Storz TTL-Computer flash unit. Equipment used for photography was Olympus OM-2 attached to Carl Storz objective (593-T2), Kodak Ektachrome ASA 400 film and Olympus Record Data Back 2, for imprinting number and date on each photograph.
Classification The knee joint was divided into 5 areas, posterior, intercondylar, medial and lateral gutter and the suprapatellar pouch. The synovial membrane was described according to the macroscopic severity of the dominant inflammatory changes in each area and given a score from 1 to 4:
Grade 1 = No signs of synovitis. Grade 2 = Moderate hyperemia, no villous proliferation (Fig. 1 u) . Grade 3 = Moderate hyperemia, moderate villous proliferation (Fig. 1 b ) . Grade 4 = Moderate to severe hyperemia with massive villous proliferation (Fig. 1 c ) .
Despite a bloodless field the increased vasculature of the synovial membrane was easy to observe, both the increased number of vessels and the change of colour due to capillary hyperaemia.
The villous changes are described as moderate and massive. The moderate changes reflects villi smaller in size with less oedema and not as numerous as seen in the massive changes.
Arthroscopy Epidural or general anaesthesia was used both for the first and subsequent arthroscopies. A bloodless field was always used and lasted on average 45 min (30-80 min).
The routine port of entry was anterolateral, just lateral to the lateral margin of patellar tendon. A continuous flow of Ringer solution (17) was used with inflow through the arthroscope and with a separate outflow through a cannula lateral in the suprapatellar pouch. A probe was used to obtain complete examination of the joint (18) and was introduced through an anteromedial entry 2 cm medial to the medial margin of the patellar tendon above the medial meniscus. The quality and quantity of synovial fluid was observed. The findings were classified and recorded by one surgeon only (A. C. P.).
Four to eight photographs of the synovial lining were taken at each arthroscopic examination. All details observed at the preoperative arthroscopy were recorded before the synovectomy was
started, to prevent the operative findings from influencing the recording.
Synouectomy In direct connection with the preoperative arthroscopy, synovectomy was performed using the same anaesthesia. Radical synovectomy was done by “four quadrant resection” through two longitudinal parapatellar incisions according to the method described by Mori (19, 20). All pannus growth on the articular cartilages was carefully removed and all marginal erosions were cleansed for synovial tissue. Total meniscectomy (both menisci) was performed in all patients.
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.

Scand J Rheumatology 19
Table I. Patient characteristics at synovectomy
Arthroscopic evaluation of the synovial lining 195
RA" J R A ~ PsA' Sum
No. of patients Malelfemale Oligo-Ipoly-articular disease Mean age in years
Disease duration in years
Knee joint involvement in years
Hematology Hgb (g/lOO ml) ESR (mm) CRP (mg/l) WCC (1000) Thrombocytes (1000) Waalers reaction (No. of patients with positive tests 364)
Functional capacityd Colorado knee score' Ritchie's clinical score! Morning stiffness (min)
( fSD)
( fSD)
(kSD)
Clinical scores
Present medication (No. of patients) None NSAIDs Antimalaria Gold D-penicillamine Cytostatic drugs Steroids
6 19 3 28 016 2/17 211 4/24
1316 47 (k11.0) 15 ( f4 .9) 24 (f5.8) 23 (f14.5)
8.5 (54.3) 8.6 ( f4 .5) 7.3 (f3.3) 8.1 (54.3)
2.6 ( f2 .0) 7.8 ( f4 .4) 5.9 (k4.6) 6.5 (k4.6)
11.5 ( f5 .4) 12.1 (k1.0) 13.8 ( f l .O) 12.2 ( f1 .3) 31 (512.3) 18 (211.4) 14 (f12.1) 21 (f13.0) 26 (f12.0) 6 (k7.0) 5 (54.5) 9 ( f l l . 4 ) 5.3 (k2.2) 6.5 (k1.6) 4.8 ( f3 .3) 6.1 ( f2 .1)
4 3 0 7 347 ( f61 ) 332 ( f83 ) 322 (577) 334 (k78)
2.2 ( f0 .4) 1.7 ( f0 .4) 2.3 (20.5) 1.9 (f0.5) 70 (f lO.8) 88 ( f9 .5 ) 70 (f13.6) 82 (k13.4) 7.3 (k3.5) 3.1 ( f2 .3) 4.0 (k3.6) 4.1 ( f3 .2)
23 (526) 24 ( f43 ) 7 (54.7) 22 (k38)
0 0 0 0 6 12 3 21 0 5 0 5 1 2 0 3 0 1 0 1 1 4 0 5 1 4 0 5
RA = classical or definite rheumatoid arthritis (1 1).
PsA = psoriatic arthropathy (13). Steinbrocker 1949 (14).
' Geens, 1969 (15). Ritchie, 1968 (16).
' JRA =juvenile rheumatoid arthritis (12).
The operative findings of the synovial lining were classified and recorded using the same score system as for arthroscopy and by the same surgeon (A. C. P.).
Statistics
The results are given as arithmetic mean and standard deviation (SD). Analysis of differences between 5 different sites in the joint and between the 3 different sets of tests taken at baseline, at 6 and at 12 months postoperatively were performed on individual developments using Friedman's non parametric tests or Spearman's rank correlation test.
RESULTS
Zntraarticular variations The findings at arthroscopy prior to synovectomy and at synovectomy were compared. There was a highly statistically significant correlation (p<O.OOl) . At the preoperative
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.

Scand J Rheumatology 19 196 A . C. Paus and J . A . Pahle
Fig. I a . Grade 2 synovitis.
Fig. I b. Grade 3 synovitis.
Fig. I c . Grade 4 synovitis.
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.
Scand J Rheumatology 19 Arthroscopic evaluation of the synovial lining 197 ~~
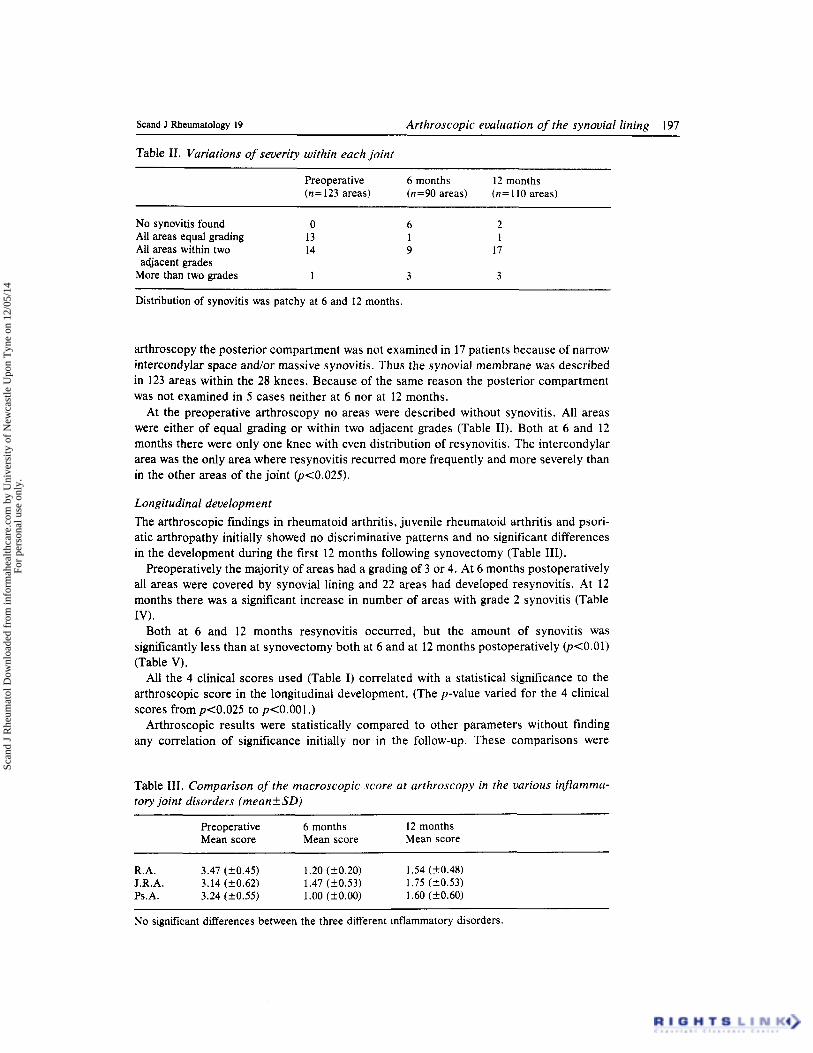
Table 11. Variations of severity within each joint
Preoperative 6 months 12 months (n= 123 areas) (n=90 areas) (n= 110 areas)
No synovitis found 0 6 2 All areas equal grading 13 1 1 All areas within two 14 9 17
More than two grades 1 3 3 adjacent grades
Distribution of synovitis was patchy at 6 and 12 months.
arthroscopy the posterior compartment was not examined in 17 patients because of narrow intercondylar space and/or massive synovitis. Thus the synovial membrane was described in 123 areas within the 28 knees. Because of the same reason the posterior compartment was not examined in 5 cases neither at 6 nor at 12 months.
At the preoperative arthroscopy no areas were described without synovitis. All areas were either of equal grading or within two adjacent grades (Table 11). Both at 6 and 12 months there were only one knee with even distribution of resynovitis. The intercondylar area was the only area where resynovitis recurred more frequently and more severely than in the other areas of the joint (p<0.025).
Longitudinal development The arthroscopic findings in rheumatoid arthritis, juvenile rheumatoid arthritis and psori- atic arthropathy initially showed no discriminative patterns and no significant differences in the development during the first 12 months following synovectomy (Table 111).
Preoperatively the majority of areas had a grading of 3 or 4. At 6 months postoperatively all areas were covered by synovial lining and 22 areas had developed resynovitis. At 12 months there was a significant increase in number of areas with grade 2 synovitis (Table IV) .
Both at 6 and 12 months resynovitis occurred, but the amount of synovitis was significantly less than at synovectomy both at 6 and at 12 months postoperatively (pCO.01) (Table V).
All the 4 clinical scores used (Table I) correlated with a statistical significance to the arthroscopic score in the longitudinal development. (The p-value varied for the 4 clinical scores from ~ ~ 0 . 0 2 5 to p<O.OOl.)
Arthroscopic results were statistically compared to other parameters without finding any correlation of significance initially nor in the follow-up. These comparisons were
Table 111. Comparison of the macroscopic score at arthroscopy in the various injlamma- tory joint disorders (meanfSD)
Preoperative 6 months 12 months Mean score Mean score Mean score
R.A. 3.47 (f0.45) 1.20 (f0.20) 1.54 (k0.48) J.R.A. 3.14 (k0.62) 1.47 (f0.53) 1.75 (k0.53) Ps.A. 3.24 (k0.55) 1.00 (kO.00) 1.60 (f0.60)
No significant differences between the three different inflammatory disorders.
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.

198
Table IV. Changes of the synovial lining decided according to the severity of the injlam- matory changes
A . C. Paus and J . A . Pahle Scand J Rheumatology 19
Preoperative 6 months 12 months (n = 123 areas) (n=90 areas) (n=110 areas)
Grade 1 0 64 (72%) 46 (42%) Grade 2 15 (12%) 22 (24%) 52 (47 %) Grade 3 65 (53%) 4 (4%) 12 (11%) Grade 4 43 (35%) 0 0
The number of areas with resynovitis increased significantly between 6 and 12 months @<0.01), but did not reach preoperative levels.
calculated on the individual development for each patient regarding disease duration, period of knee joint involvement prior to synovectomy, whatever drugs the patients were treated with, laboratory results like CRP, ESR, white cell counts, thrombocytes, hemoglo- bin, sex and age.
Table V. The individual development of the mean arthroscopic score
Patient No. Preoperative 6 months 12 months Diagnosis
2 3 4 6 7 8 9
10 11 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31
4.00 2.75 4.00 4.00 4.00 4.00 2.80 2.75 4.00 2.40 3 .OO 4.00 3.00 2.75 3.50 2.75 3.25 3.25 3.75 3.50 2.60 2.75 3.00 3.00 3.20 2.25 3.00 3.00
- 1 .oo
1.40 1.40 1 .oo
-
- - 1.40 1.40 - - 1.20 1.25 1 .oo I .oo 1 S O 1.75 1 .oo 2.00 1.20 1 .oo 2.20 -
- - 1.20 1.75
1 .oo 1 .oo
2.20 1.40 1.40 1.20 2.20 1.75 I .25 1.20 2.00 1.20 1.80 2.25
2.50 1.20 1.60 2.25 2.20 1.75
1.40
-
-
-
- - 2.20 2.20
PsA RA JRA JRA RA RA JRA JRA JRA JRA PsA JRA JRA JRA JRA PsA RA JRA RA JRA JRA JRA RA JRA JRA JRA JRA JRA
~ ~~ ~ ~
Significantly less synovitis both 6 and 12 months after synovectomy @<0.01), despite an increase between 6 and 12 months.
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.

Scand J Rheurnatology 19 Arthroscopic evaluation of the synovial lining 199
DISCUSSION
The method of classification of synovitis was simple to use. This classification encom- passes the great variety of changes that is seen in the synovitis in chronic inflammatory joints. Villi may be threadlike or coarse edematous polyplike structures as described by Watanabe (21). The increased vascularity is clearly visualized as well as the various amounts of fibrin deposits. Lindblad’s classification (4) includes the same parameters even though with different values. Our aim was to find a system of classification which both was easy to use and without to many variables. This simple system of classification standard- ized the description of the synovial membrane at arthroscopy and at synovectomy and made comparison between different patients and longitudinal study of each patient possi- ble.
The identical findings at the preoperative arthroscopy and at synovectomy is taken as an indication of the accuracy of the arthroscopy. The scores at 6 and 12 months are therefore considered to reflect the changes of the synovial lining without methodical errors of importance.
The method of selection of patients ensured active synovitis of moderate to severe grade present in the joint at preoperative arthroscopy. The inflammatory changes of the synovial lining were then evenly distributed. If biopsies should be required at this stage, blind biopsies may be adequate. Both the documentation of others (4) and our postoperative findings describes a variance in the degree of inflammation of the synovial lining. Arthros- copically guided biopsies will therefore be of more value both early in the disease and in the postoperative follow-up.
Lindblad (4) describes that synovitis starts in the synovial lining adjacent to cartilage in previously healthy patients. This could not be demonstrated in our study, possibly because all preoperative arthroscopies were performed in knee joints with moderate or severe general synovitis where all the synovial lining was involved.
At 6 months the synovial lining had regenerated completely in all cases but resynovitis varied considerably in severity. The intercondylar area was more frequently and more severely involved than other areas. It may be claimed that it is difficult to remove all synovitis within this area at surgery which then would explain the early resynovitis. This area was, however, meticulously cleansed for all synovial lining and we therefore do not consider the surgical procedure as the cause of more pronounced resynovitis in the intercondylar area. Arthroscopy of all knee joints with chronic inflammatory disease should therefore specifically consider the intercondylar area. If biopsy should be indicated at this later stage, arthroscopical guidance would help in achieving representative biopsies of inflamed areas.
Gil & Katone (22) conclude that arthroscopy is useful not only for diagnosis of disease, but also in observing natural evolution of its lesions. Jackson (23) concludes that arthros- copy in the management of arthritis in the knee, makes possible early detection of pathology.
Our conclusion is in agreement with these authors that arthroscopy gave valuable information about the early development of resynovitis following synovectomy.
Already at 6 months following synovectomy resynovitis occurs even though no areas in any patients had a grade 4 synovitis and only very few areas had grade 3 synovitis. However, it is disturbing to note that already at 12 months there was a statistically significant increase both in distribution and severity of resynovitis. Clinical improvements consist primarily of better function and relief of pain. Our findings at 12 months show that this improvement is not synonymous with the disease being removed. Whether the resynovitis after synovectomy is as aggressive and destructive as if the knee joint had been
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.

Scand J Rheumatology 19 200 A . C. Paus and J . A . Pahle
treated conservatively cannot be evaluated, but retrospective studies on the effect of knee joint synovectomy suggest a delay in the destructive patterns (24, 25, 26).
It must be emphasized that this study does not give any answers to the question of the value of synovectomy as compared to other kinds of treatments. We have not performed similar studies on conservatively treated patients, and the patients included in the study has a too short follow-up period.
The groups of patients with different inflammatory joint disorders are small and there is no statistical differences between these groups in our study. The results were statistically similar whether calculated for each group separately or for the total number of patients as one group. Our impression is that synovitis is a non-specific response of the synovial lining and that irrespective of etiology synovitis presents with the same macroscopic changes.
Our conclusions are that the synovial membrane is fully regenerated at 6 months and that resynovitis occurs already 6 months following synovectomy and increases between 6 and 12 months. It did not reach the preoperative severity within this short observation period. This finding correlates positively with the clinical results.
The inflammatory response of the synovial lining seems to be nonspecific, and arthros- copy is a good method of verifying the severity of the disease but not to discriminate between the various chronic inflammatory disorders. Arthroscopic guidance is advocated to help achieving representative biopsies of inflamed areas. A method of describing the inflammatory changes using a score scale is introduced and is of importance both when comparing groups of patients and longitudinal studies of each patient.
ACKNOWLEDGEMENTS
The authors want to acknowledge the Research Fellowship and the economical support given by Norman and Leon Hess’ Foundation for Rheumatological Research. The authors want to thank E. Fginstelien for the invaluable help with statistical data. We also owe our gratitude to Inger Lise Wollan who has done the secretarial work. Further we owe our thanks to the medical staff in the rheumatolo- gical ward and the operating theater. Without their help this study would have been impossible.
REFERNCES 1 . 2.
3 .
4. 5.
6. 7.
8.
9.
10.
1 1 .
Kogstad 0. Arthroscopy. Tidsskr Nor Laegeforen 1977; 25: 128C-2. McGinty JB. Arthroscopy. Kelley WN, Harris ED, Ruddy S, Sledge CB. Textbook of rheumatol- ogy, 2nd ed. W. B. Saunders Company, 1985; 640-8. Paus A, Pahle JA. The value of arthroscopy in the diagnosis and treatment of patients with juvenile rheumatoid arthritis. Ann Chir Gynaecol 1986; 75: 168-71. Lindblad S , Hedfors E. Intraarticular variation in synovitis. Arthritis Rheum 1985; 28: 977-86. Bergstrgim R, Gillquist J , Lysholm J, Hamberg P. Arthroscopy of the knee in children. J Pediatr
Zive I, Carrol NC. The role of arthroscopy in children. J Pediatr Orthop 1982; 2: 243-7. Suman RK, Stother IG, Illingworth G. Diagnostic arthroscopy of the knee in children. J Bone Joint Surg 1984; 66B: 4: 535-7. Rydholm U. Arthroscopy of the knee in juvenile chronic arthritis. Scand J Rheumatol 1986; 15:
Paus AC, Refsum S, Fgirre 0. Histopathologic changes of arthroscopic synovial biopsies before and after synovectomy in patients with chronic inflammatory joint diseases. Scand J Rheumatol (in press). Paus AC, Mellbye 0, Fgirre @. Irnmunhistopathologic findings in synovial biopsies before and after synovectomy in patients with chronic inflammatory joint diseases and their relation to clinical evaluation. Scand J Rheumatol (submitted). Ropes MW, Bennett GA, Cobb S, Jacox R, Jessar RA. Revision of diagnostic criteria for rheumatoid arthritis. Bull Rheum Dis 1958: 0: 175-6.
Orthop 1984; 4: 542-5.
109-1 2.
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.

Scand J Rheumatology 19
12. Brewer EJ Jr, Bass J, Baum J, Cassidy JT, Fink C, Jacobs J, Hanson V, Levinson JE, Schuller J , Stillman JS. Current proposed revision JRA criteria. Arthritis Rheum 1977; 20: 195-9.
13. Wright V. Psoriatic arthritis. In: Copman’s textbook of the rheumatic diseases (ed. Scott J. Edinburgh). London: New York, 1978: 537-50.
14. Steinbrocker 0, Traeger CH, Batterman RC. Therapeutic criteria in rheumatoid arthritis. JAMA 1949; 140: 659.
15. Geens S, Clayton ML, Leidholt JD, Smyth CJ, Bartholomew BA. Synovectomy and debridement of the knee in rheumatoid arthritis. J Bone Joint Surg 1969; 51A: 62642.
16. Ritchie DM, Boyle JA, McInnes JM, Jasani MK, Dalakos TG, Grieveson P, Buchanan WW. Clinical studies with an articular index for the assessment of joint tenderness in patients with rheumatoid arthritis. Q J Med 1968; 147: 393406.
17. Reagan BF, McInerey VK, Treadwell BV, Zarins B, Mankin HJ. Irrigating solutions for arthros- copy. J Bone Joint Surg 1983; 65A: 629-31.
18. Paus A, Fasting OJ, Hareide A, Gjengedal E. Arthroscopic diagnosis. Tidsskr Nor Legeforen 1985; 105: 669-70.
19. Mori M. Surgery of rheumatoid arthritis of the knee joint. Rheumatism 1964; 20: 3542 . 20. Mori M. A review of knee joint synovectomy in rheumatoid arthritis with theoretical and
21. Watanabe M, Takeda S , Ikeuchi H. Atlas of arthroscopy. Berlin: Springer-Verlag, 1979: 113-21. 22. Gil JR, Katona G. Arthroscopy as a means of diagnosis and research. Review of 80 arthroscopies.
23. Jackson RW. The role of arthroscopy in management of the arthritic knee. Clin Orthop 1974; 101:
24. Dummer U, Tillmann K. Comparative evaluation of partial and subtotal synovectomies of the
25. Souter WA. Present attitudes on timing of surgical interventions in the treatment of rheumatoid
26. Paus AC, Teigland J, @stensen H. Synovectomy of the knee joint in patients with chronic
Arthroscopic evaluation of the synovial lining 201
technical considerations. Ann Chir Gynaecol 1985; Suppl 198: 74: 4C-7.
Exerpta Medica 1967; 209: 209-15.
28-35.
knee joint in rheumatoid arthritis. Reconstr Surg Traumat 1981; 18: 8-15.
disease. Ann Chir Gynaecol 1985; 74: Suppl 198: 19-25.
inflammatory joint diseases. Scand J Rheumatol 1990 (in press).
Received 15 August 1989 Received in revised form 13 November 1989
Scan
d J
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le U
pon
Tyn
e on
12/
05/1
4Fo
r pe
rson
al u
se o
nly.