arthroscopic distal clavicle resection from a bursal approach
TRANSCRIPT
Arthroscopic Distal Clavicle Resection From a Bursal Approach
William N. Levine, M.D., O. Alton Barron, M.D., Ken Yamaguchi, M.D., Roger G. Pollock, M.D.,Evan L. Flatow, M.D., and Louis U. Bigliani, M.D.
Summary: We retrospectively reviewed 117 consecutive patients who underwentarthroscopic acromioclavicular joint (ACJ) arthroplasties. Only patients whounderwent ACJ arthroplasties from a bursal approach in conjunction withsubacromial decompression were included. Patients with isolated ACJ arthrosistreated with resection of the distal clavicle from a superior approach, isolatedimpingement with only undersurface distal clavicle debridement, prior surgery, orother shoulder pathology were excluded. Twenty-four patients met these rigidcriteria for inclusion in the study. After an arthroscopic subacromial decompres-sion, the distal clavicle was visualized and resected through a standard bursalapproach. In addition, an anterosuperior portal was used in 50% of the patients toconfirm adequate clavicle resection. Postoperative follow-up averaged 32.5months (range, 24 to 70 months). Preoperative and postoperative pain were ratedsubjectively on a 5-point scale (1, incapacitating pain; 5, no pain). Operativereports and postoperative radiographs were reviewed to determine technical factorsthat may have influenced outcome. Seventeen patients had excellent results (71%),4 good (16.5%), and there were 3 failures (12.5%). Average preoperative painrating was 1.8 and was improved to 4.3 postoperatively. The average amount ofclavicle resection was only 5.4 mm. Given smooth, even, and complete boneremoval, the amount of bone resected did not correlate with outcome. Arthroscopicdistal clavicle resection performed in conjunction with subacromial decompressiongave excellent results, comparable to isolated ACJ procedures. In this series,additional use of an anterosuperior portal for more direct shaver placement andcomplete ACJ viewing allowed consistent bone resection and excellent results in ahigh percentage of patients.Key Words: Distal—Clavicle—Excision—Bursal—Approach.
Acromioclavicular joint (ACJ) pain is a com-mon cause of shoulder complaints, and resection
of the outer end of the clavicle has been a reliabletreatment for recalcitrant cases.1-6 This can be per-formed from a superior approach in isolated ACJdisease, such as distal clavicle osteolysis or post-
traumatic arthritis of the AC joint.7-9 Results of thisprocedure have been quite satisfactory and equivalentto results of open resection of the distal clavicle.7,8
However, ACJ pathology can also occur in conjunctionwith impingement syndrome. If an enlarged ACJcontributes to impingement, then an undersurfacedebridement with removal of inferior osteophytes isperformed.10,11
If the ACJ is an independent source of pain (asevidenced by preoperative ACJ tenderness, pain withcross-body adduction, and/or a confirmatory ACJinjection), a distal clavicle excision should be includedas part of the treatment. In fact, a common cause of
From The Shoulder Service, New York Orthopaedic Hospital,Columbia-Presbyterian Medical Center, New York, New York,U.S.A.
Address correspondence and reprint requests to Evan L. Flatow,M.D., 161 Ft. Washington Ave, New York, NY 10032, U.S.A.
r 1998 by the Arthroscopy Association of North America0749-8063/98/1401-1523$3.00/0
52 Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 14, No 1 (January-February), 1998: pp 52–56

failure following isolated subacromial decompressionis persistent ACJ pain.12-14
We undertook the current study to assess our resultsof bursal-approach distal clavicle excision in conjunc-tion with arthroscopic subacromial decompression.Specific attention was given to technical factors thatmay lead to a successful outcome.
MATERIALS AND METHODS
We retrospectively reviewed 117 consecutive pa-tients who underwent arthroscopic ACJ arthroplasties.Only patients with bursal approaches performed inconjunction with subacromial decompressions wereincluded. Patients with isolated ACJ arthrosis treatedwith resection of the distal clavicle from a superiorapproach, isolated impingement with only undersur-face distal clavicle debridement, prior surgery, or othershoulder pathology (e.g., labral tears or partial thick-ness rotator cuff tears) were excluded. Twenty-fourpatients met these rigid criteria for inclusion in thestudy.
All patients had failed a minimum of 6 months ofnonoperative treatment including nonsteroidal anti-inflammatory medications, physical therapy, activitymodification, and a confirmatory acromioclavicularjoint injection.
All patients had gradually progressive pain referableto the subacromial bursa and ACJ. All patients hada positive impingement sign, and all but one hadboth pain on palpation of the ACJ and with cross-body adduction. All patients had an AC injection tocorroborate the clinical findings. An anesthetic injec-tion was placed in the subacromial space first, and ifresidual pain was then eliminated with a separateACJ injection, a distal clavicle resection was thenplanned.
After a standard arthroscopic acromioplasty usinganterolateral and posterolateral bursal portals (Fig 1),the undersurface of the ACJ was cleared of soft tissues.While viewing from the bursa, a burr was broughtin from a portal anterior to the ACJ and the distalclavicle was resected. To confirm full resection, thescope could be moved to the anterior operativeportal to view the distal clavicle. This allowed a lessdistorted view of the posterosuperior corner of thedistal clavicle.
Preoperative and postoperative pain were ratedsubjectively on a 5-point scale (1, incapacitating pain;5, no pain). Patients were rated as excellent (no pain),good (minimal pain), and failure (all others). Opera-tive reports and postoperative radiographs were re-
viewed to determine technical factors which may haveinfluenced outcome.
OPERATIVE TECHNIQUE
The operative technique used has been previouslydescribed15 but will be briefly reviewed here. Follow-ing the arthroscopic subacromial decompression, local-ization of the ACJ is facilitated by placing a needlethrough the joint from above and visualizing it in thesubacromial space below. Electrocautery is used toclearly demarcate the distal clavicle and minimizebleeding. Great care is used in this step to avoidunnecessary disruption of the supporting ligamentsand capsule. A burr of known dimensions (usually 5 to6 mm) is then used to resect the distal claviclebeginning inferiorly. The clavicle is brought down intothe subacromial space with manual pressure fromabove to facilitate resection of the superior portion ofthe distal clavicle. Use of a superior portal is oftenhelpful to assure even resection. The arthroscope
FIGURE 1. Anterolateral and posterolateral bursal portals (x)shown as well as additional AC portals that are used as needed.
53ARTHROSCOPIC AC RESECTION: BURSAL APPROACH

should be placed in the bursal, anterior and superior (ifused) portal to best confirm an even, smooth resection.
RESULTS
Twenty-four patients underwent arthroscopic acro-mioplasty with a bursal-approach distal clavicle exci-sion in this series. There were 14 men and 10 womenwith 15 dominant and 9 nondominant shoulders in-volved. The average age at the time of surgery was 55years, with a range of 30 to 80 years. The averagefollow-up in this series was 32.5 months, with a rangeof 24 to 70 months.
Preoperative range of motion was normal in mostpatients with average forward elevation of 170° (range,80° to 180°), average external rotation of 63° (range,40° to 90°), and internal rotation to the T7 vertebrallevel (range, T6-L4). In all patients, postoperativerange of motion was equal to or better than thepreoperative values.
Preoperative radiographs showed degenerativechanges in 65% of the AC joints (Fig 2). Thirty percentof the AC joints were normal on routine radiographsand there was 1 patient with superior subluxation ofthe distal clavicle (type II AC separation). Approxi-mately 50% of the patients with degenerative ACJshad inferiorly protruding osteophytes.
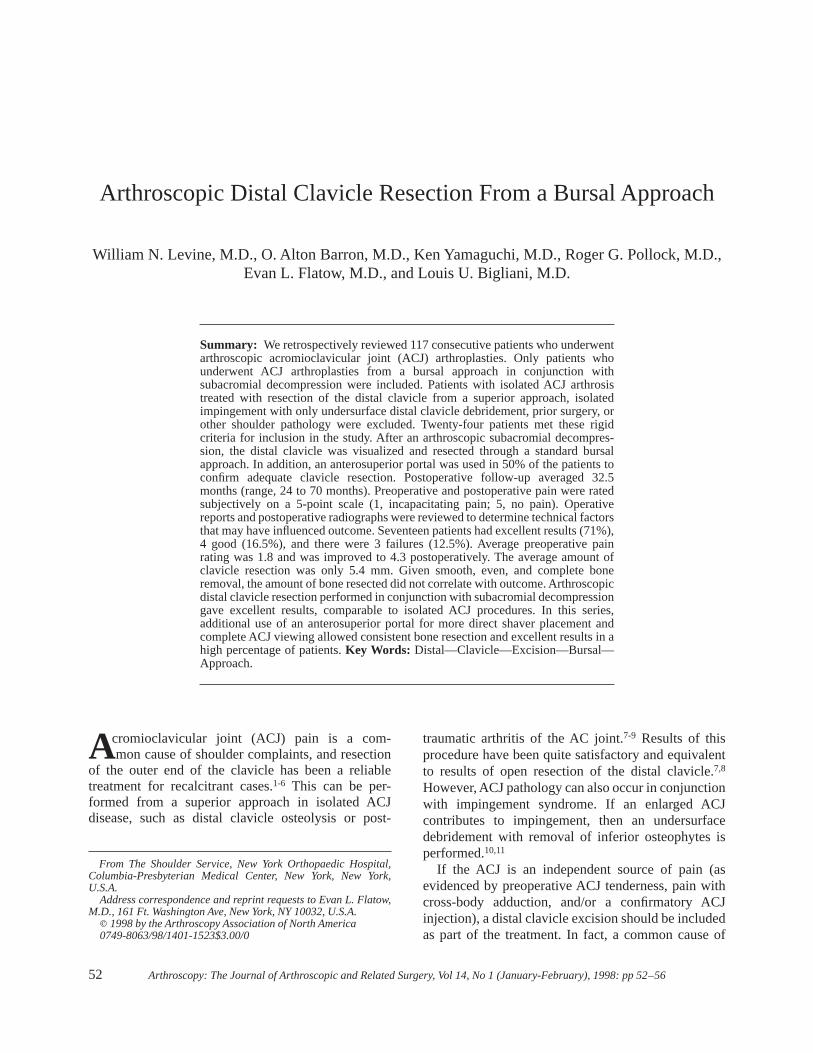
Review of postoperative radiographs recorded anaverage distal clavicle resection of 5.4 mm (range, 3 to10 mm) (Fig 3). There were no cases of heterotopicbone formation. Two cases showed retained bone: 1superior and 1 posteroinferior.
Overall, 17 patients achieved excellent results (71%),4 good (16.5%), and there were 3 poor results (12.5%).The average postoperative pain score improved to 4.3postoperatively (range, 1 to 5). The average preopera-tive pain score was 1.8 (range, 1 to 3). All patientsreturned to their preoperative activity level with resolu-tion of symptoms in the majority.
COMPLICATIONS
There were no infections and no arthroscopic portalhealing complications, and there was no keloid orfistula formation. There were 3 failures in this study.One was in the patient with a type II AC separation,which we now consider a contraindication to thisprocedure.15,16 This patient as well as 1 additionalfailure had uneven bone resection as noted above. Thethird failure was in a patient who had persistent,significant pain postoperatively. No intraoperative tech-nical factors could be elucidated to explain the pain.
DISCUSSION
Open resection of the distal clavicle was introducedindependently by Gurd and Mumford in 1941.3,4
Subsequent reports have documented consistent, satis-factory results with this procedure.1,5,6,17,18In addition,it has been advocated in rotator cuff surgery as one partof the reconstructive procedure.12,13,19The complica-tions following open distal clavicle excision includecosmesis of the incision, as well as postoperative
FIGURE 2. Preoperative AP ra-diograph showing a degenera-tive ACJ.
54 W. N. LEVINE ET AL.
weakness.1,5,20Arthroscopic AC arthroplasty was intro-duced to attempt to avoid some of these concerns.
In a cadaveric study, Gartsman et al.21 showed thatarthroscopic distal clavicle resection could reliably beperformed and bony resection was comparable to opentechniques. Using quantitative radiographic analysis,Flatow and coworkers7 documented comparable boneresection with arthroscopic and open techniques. Sub-sequent clinical studies have shown that the results areexcellent and reliable.8,16,22-24In isolated ACJ pathol-ogy, we have preferred a direct approach that does notintroduce bleeding and bone debris into the subacro-mial bursa.7,8 However, the group presented in thisstudy had impingement syndrome as well as ACJpathology and, therefore, were not suitable candidatesfor a direct approach. Arthroscopic resection of thedistal clavicle from a bursal approach yielded 87.5%excellent and good results. Success was not correlatedto the amount of bone resected but instead to technicalsuccess in achieving a smooth, even resection of bone.
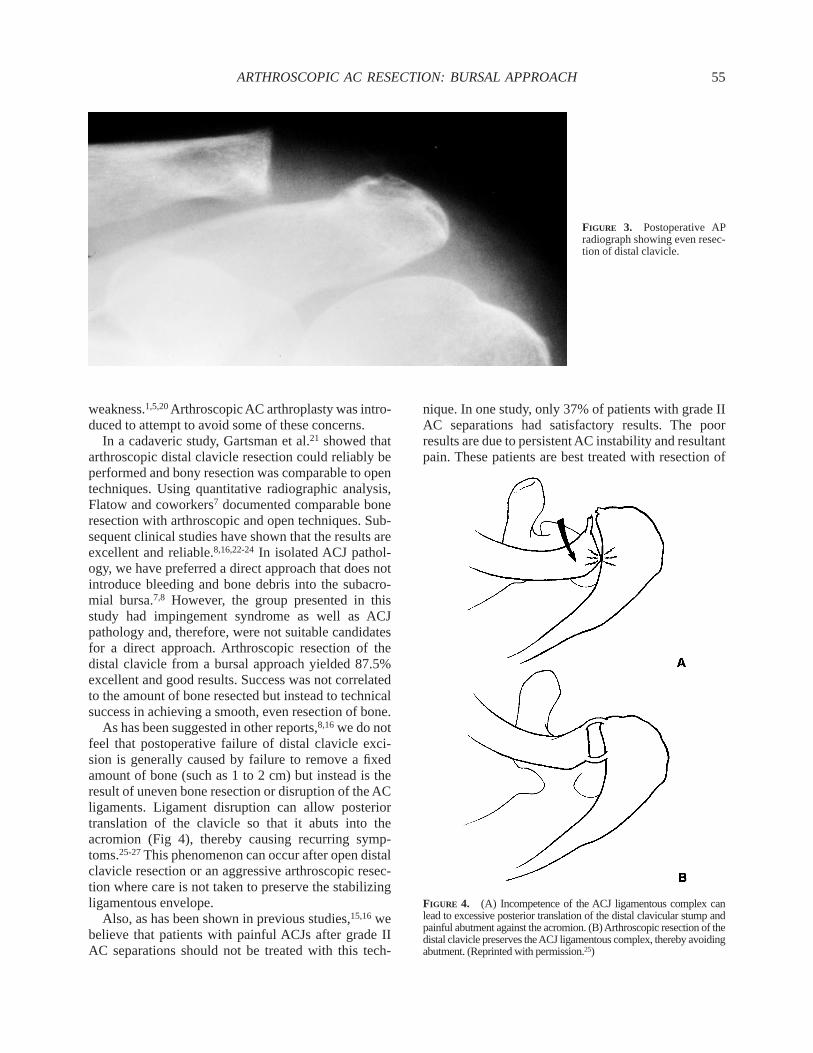
As has been suggested in other reports,8,16we do notfeel that postoperative failure of distal clavicle exci-sion is generally caused by failure to remove a fixedamount of bone (such as 1 to 2 cm) but instead is theresult of uneven bone resection or disruption of the ACligaments. Ligament disruption can allow posteriortranslation of the clavicle so that it abuts into theacromion (Fig 4), thereby causing recurring symp-toms.25-27This phenomenon can occur after open distalclavicle resection or an aggressive arthroscopic resec-tion where care is not taken to preserve the stabilizingligamentous envelope.
Also, as has been shown in previous studies,15,16webelieve that patients with painful ACJs after grade IIAC separations should not be treated with this tech-
nique. In one study, only 37% of patients with grade IIAC separations had satisfactory results. The poorresults are due to persistent AC instability and resultantpain. These patients are best treated with resection of
FIGURE 3. Postoperative APradiograph showing even resec-tion of distal clavicle.
FIGURE 4. (A) Incompetence of the ACJ ligamentous complex canlead to excessive posterior translation of the distal clavicular stump andpainful abutment against the acromion. (B)Arthroscopic resection of thedistal clavicle preserves theACJ ligamentous complex, thereby avoidingabutment. (Reprinted with permission.25)
55ARTHROSCOPIC AC RESECTION: BURSAL APPROACH

the ACJ joint and distal clavicle stabilization (modifiedWeaver-Dunn procedure).
In summary, arthroscopic distal clavicle excisionfrom a bursal approach yields predictable, reliableresults in the majority of patients. Care should be takento resect an even amount of bone and preserve thesupporting capsular and ligamentous structures of theACJ to maintain stability. The amount of bone resecteddid not correlate with results and in fact, we nowrecommend resecting much less bone (5 to 7 mm) thanearlier reports.
REFERENCES
1. Cook FF, Tibone JE. The Mumford procedure in athletes: anobjective analysis of function.Am J Sports Med1988;16:97-100.
2. Grimes DW, Garner RW. The degeneration of the acromiocla-vicular joint: Treatment by resection of distal clavicle.OrthopRev1980;9:41-44.
3. Gurd FB. The treatment of complete dislocation of the outerend of the clavicle: A hitherto undescribed operation.Ann Surg1941;63:1094.
4. Mumford EB. Acromioclavicular dislocation: A new operativetreatment.J Bone and Joint Surg1941;23:799-801.
5. Petersson CJ. Resection of the lateral end of the clavicle: a 3 to30 year follow-up.Acta Orthop Scand1983;54:904-907.
6. Worcester JN, Green DP. Osteoarthritis of the acromioclavicu-lar joint. Clin Orthop1968;58:69-73.
7. Flatow EL, Cordasco FA, Bigliani LU. Arthroscopic resectionof the outer end of the clavicle from a superior approach: Acritical quantitative, radiographic assessment of bone removal.Arthroscopy1992;8:55-64.
8. Flatow EL, Duralde XA, Nicholson GP, Pollock RG, BiglianiLU. Arthroscopic resection of the distal clavicle with a superiorapproach.J Shoulder and Elbow Surg1995;4:41-50.
9. Johnson LL.Diagnostic and surgical arthroscopy.St. Louis:CV Mosby, 1981.
10. Ellman H. Arthroscopic subacromial decompression: Analysisof one- to three-year results.Arthroscopy1987;3:173-181.
11. Esch JC, Ozerkis LR, Helgager JA, Kane N, Lilliott N.
Arthroscopic subacromial decompression: Results according tothe degree of rotator cuff tear.Arthroscopy1988;4:241-249.
12. Neer CS II: Impingement lesions.Clin Orthop 1983;173:70-77.
13. Neer CS II.Shoulder reconstruction.Philadelphia: WB Saun-ders, 1990.
14. Penny JN, Welsh RP: Shoulder impingement syndromes inathletes and their surgical management.Am J Sports Med1981;9:11-15.
15. Bigliani LU, Nicholson GP, Flatow EL. Arthroscopic resectionof the distal clavicle.Orthop Clin North Am1993;24:133-141.
16. Gartsman GM. Arthroscopic resection of the acromioclavicularjoint. Am J Sports Med1993;21:71-77.
17. Taylor GM, Tooke M. Degeneration of the acromioclavicularjoint as a cause of shoulder pain.J Bone and Joint Surg Br1977;59:507.
18. Weaver JK, Dunn HK. Treatment of acromioclavicular injuries,especially complete acromioclavicular separation.J Bone andJoint Surg Am1972;54:1187-1194.
19. Neviaser TJ, Neviaser RJ, Neviaser JS, Neviaser JS. Thefour-in-one arthroplasty for the painful arc syndrome.ClinOrthop1982;163:107-112.
20. Daluga DJ, Dobozi W. The influence of distal clavicle resectionand rotator cuff repair on the effectiveness of anterior acromio-plasty.Clin Orthop1989;247:117-123.
21. Gartsman GM, Combs AH, Davis PF, Tullos HS. Arthroscopicacromioclavicular joint resection: An anatomical study.Am JSports Med1991;19:2-5.
22. Kay SP, Ellman H, Harris E. Arthroscopic distal clavicleexcision: technique and early results.Clin Orthop1994;301:181-184.
23. Snyder SJ, Banas MP, Karzel RP. The arthroscopic Mumfordprocedure: An analysis of results.Arthroscopy1995;11:157-164.
24. Tolin BS, Snyder SJ. Our technique for the arthroscopicMumford procedure.Orthop Clin North Am1993;24:143-151.
25. Flatow EL. The biomechanics of the acromioclavicular, sterno-clavicular, and scapulothoracic joints. In: Heckman, ed.,Instruc-tional course lectures.American Academy of OrthopaedicSurgeons, 1993;237-246.
26. Fukuda K, Craig EV, An K, Cofield RH, Chao EY. Biomechan-ical study of the ligamentous system of the acromioclavicularjoint. J Bone and Joint Surg Am1986;68:434-439.
27. Salter EG, Nasca RJ, Shelley BS. Anatomical observations onthe acromioclavicular joint and supporting ligaments.Am JSports Med1987;15:199-206.
56 W. N. LEVINE ET AL.