arteriovenous fistulas in elderly hemodialysis patients ... · journal of clinical nephrology and...
TRANSCRIPT
Cite this article: Forauer AR, Bazylewicz M, Reilley MJ, Kristine A. Giffin BS (2015) Arteriovenous Fistulas in Elderly Hemodialysis Patients: Evaluation of Post-Intervention Patency of Percutaneous Transluminal Angioplasty (PTA). J Clin Nephrol Res 2(2): 1023.
Central Journal of Clinical Nephrology and Research
*Corresponding authorAndrew R. Forauer, Interventional Radiology, Dartmouth-Hitchcock Medical Center, One Medical Center Drive, Lebanon, NH 03756, Tel: 603-650-4477; Fax: 603-650-5455; Email:
Submitted: 22 September 2015
Accepted: 20 November 2015
Published: 23 November 2015
ISSN: 2379-0652
Copyrighta© 2015 Forauer et al.
OPEN ACCESS
Short Communication
Arteriovenous Fistulas in Elderly Hemodialysis Patients: Evaluation of Post-Intervention Patency of Percutaneous Transluminal Angioplasty (PTA)Andrew R. Forauer*, Michael Bazylewicz, Matthew J. Reilley and Kristine A. Giffin BSDepartment of Radiology, Dartmouth-Hitchcock Medical Center, Lebanon
INTRODUCTIONAs the generation born between 1946 and 1964- the so-called
“baby boomers”- ages, a similar trend of increasing age is reflected in the chronic kidney disease patient population. According to the U.S. Renal Data System (USRDS), one out of six patients in 2013 was age seventy-five years or older [1]. Studies that have examined the psychosocial impact of hemodialysis on elderly patients’ quality of life have failed to demonstrate a consistently negative effect [2-4]. Evaluations of vascular accesses, and specifically arteriovenous (AV) fistula patency, have often been contradictory [5-8]. It is logical to postulate that co-morbidities in this patient group, such as diabetes and cardiovascular disease, may adversely affect the maturation and natural history of vascular accesses [9].Older patients cannot simply be assumed to respond identically to interventions performed in patients twenty, thirty or more years younger.
Percutaneous interventions are crucial to the maintenance of AV access patency in order to minimize disruptions to the
delivery of optimal renal replacement therapy [10]. There is no clear consensus on the role of patient age in AV access outcomes. The purpose of this study was to compare the post-intervention patency of percutaneous transluminal angioplasty (PTA) of AV fistula stenoses in an elderly population, defined as age seventy-five years or older, with those of a control group of younger patients.
METHODSThe Institution’s Committee for the Protection of Human
Subjects approved this study plan and data collection adhered to Health Insurance Portability and Accountability Act(HIPAA) regulations. It was retrospective and no individual patient consent for study inclusion was required.
The study population was obtained from an institutional quality assurance hemodialysis database. Patients aged seventy-five years or older who received hemodialysis via an autologous vein AV fistula were identified, and36 elderly patients (mean
Abstract
Purpose: The purpose of this study is to examine whether there is a difference in post-intervention patency of arteriovenous fistulas (AVF) after percutaneous transluminal angioplasty (PTA) in elderly vs. younger patients.
Materials & Methods: Data was collected on 72 patients: 36 elderly patients (age 75 years or older) and 36 younger (control) patients between the ages of 40 and 60 years. Demographic & clinical data was collected in both groups. Primary patency, primary-assisted patency, and secondary patency were determined. In addition, post intervention primary patency was recorded for each PTA procedure performed. Kaplan-Meier survival curves, logistic regression models, and Cox-proportional-hazards regression models were applied to determine whether patency in the elderly differed significantly from the younger end- stage renal disease(ESRD) population and what variables, if any, affected patency.
Results: Elderly patients were more likely to have cardiovascular disease, have anticoagulants prescribed and have a reduced ejection fraction. There was no significant difference between the groups in terms of primary patency (p=0.98), primary assisted patency (p=0.63) or secondary patency (p=0.89). Time on hemodialysis (HD) before AVF placement had no significant effect on the outcomes of primary patency (p=0.51), primary assisted patency (p=0.61), or secondary patency (p=0.94). There was no significant difference between the groups in terms of post-interventional primary patency of angioplasty (p=0.83).
Conclusion: Comparison between younger and older patient populations with arteriovenous fistulas showed no difference in primary, primary assisted, secondary, or post-interventional primary patency. This study supports the hypothesis that AVF patency after intervention does not differ between younger & older patient populations.
Central
Forauer et al. (2015)Email:
J Clin Nephrol Res 2(2): 1023 (2015) 2/5
age 80 years, range 75-90; 23 males, 13 females) comprised the study group. A control group (n=36, mean age 52.9 years, range 40-60; 21 males, 15 females)was randomly selected by choosing every fifth patient between the ages of 40 – 60 years from an alphabetical, database-generated list of individuals who met the same access criteria as above. Data for each patient in both groups was collected over the same time period. The patient age in both groups used was the age at which the AVF was created. The data examined was related to angioplasty performed in a dysfunctional but patent AV fistula.
Demographic data collected included age, gender, and tobacco use. Clinical data and the presence or absence of the following co-morbid medical conditions was recorded: diabetes, hypertension, atherosclerotic cardiovascular disease (ASCVD), cardiac ejection fraction, and use of anticoagulant or antiplatelet medications. ASCVD, for the purpose of this study, was defined as including coronary, cerebrovascular, or peripheral vascular distributions. If available, the left ventricular ejection fraction measured by either echocardiogram or cardiac catheterization within six months of AV fistula creation was recorded. The length of time on dialysis was calculated for each patient, defined as the number of days from the start date of hemodialysis to the date of AV fistula creation. This data was entered into a spreadsheet software program (Excel, Microsoft, Redmond, WA).Hemodialysis access-specific data included AV fistula location, date of access creation, and dates of PTA or percutaneous thrombectomy.
The post-intervention (post-PTA) patency was defined as the time beginning from a percutaneous intervention on the access until the next intervention in accordance with published standards [11,12]. Accepted definitions of primary, primary-assisted, and secondary patency were used [11,12].
Statistical analysis
Comparison of discreet (demographic or clinical) variables was performed using Chi-square analysis. Continuous variables were compared using a Student’s t-Test.
Kaplan-Meier curves were generated to calculate and compare the post-intervention patency as well as primary, primary assisted, and secondary patencies. Statistical analysis software package R (v2.9.2, www.r-project.org ) was used to conduct data processing and analysis. All groups were tabulated from censored data, and overall post-intervention patency of AV fistulas after PTA in elderly vs. younger patients was calculated using the Kaplan-Meier method. Curves were compared using Log Rank test. The effects of clinical and demographic factors were controlled for using the Cox-proportional hazards regression model. Statistical significance was established as a P value of .05 or less.
RESULTSThe study group was comprised of 36 elderly patients (mean
age 80 years, range 75-90; 23 males, 13 females). The control group had 36 patients (mean age 52.9 years, range 40-60; 21 males, 15 females). The two groups did not differ in their gender composition, the incidence of tobacco use, prevalence of diabetes, or hypertension. More ASCVD (P= .0007) and use of antiplatelet or anticoagulant medications (P=.017) was observed in the
elderly patient group. An ejection fraction as measured by either echocardiogram or cardiac catheterization within six months of AV fistula creation averaged 52% in the study group and 63% in the younger control group (P=.03). The length of time on hemodialysis at the time of AV fistula creation was significantly different between the two groups: elderly group: 360 days, control group: 220 days (P=.013). A summary of the presence of co-morbidities in presented in the (Table 1).
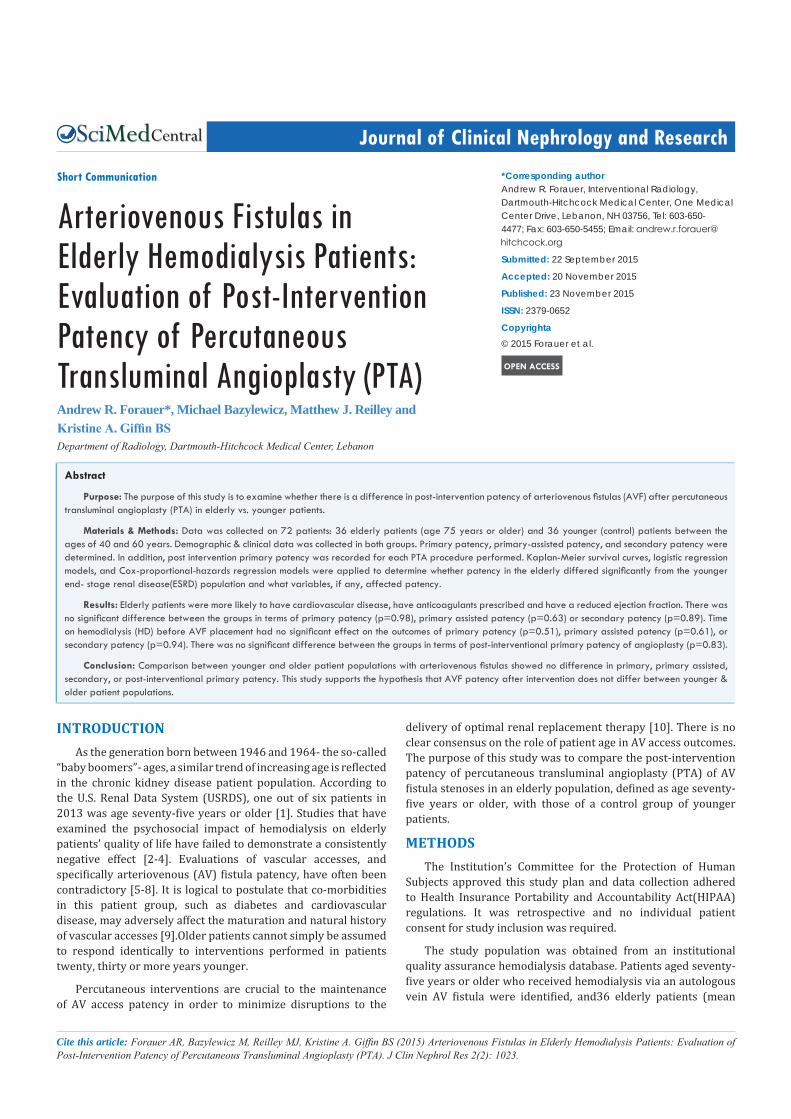
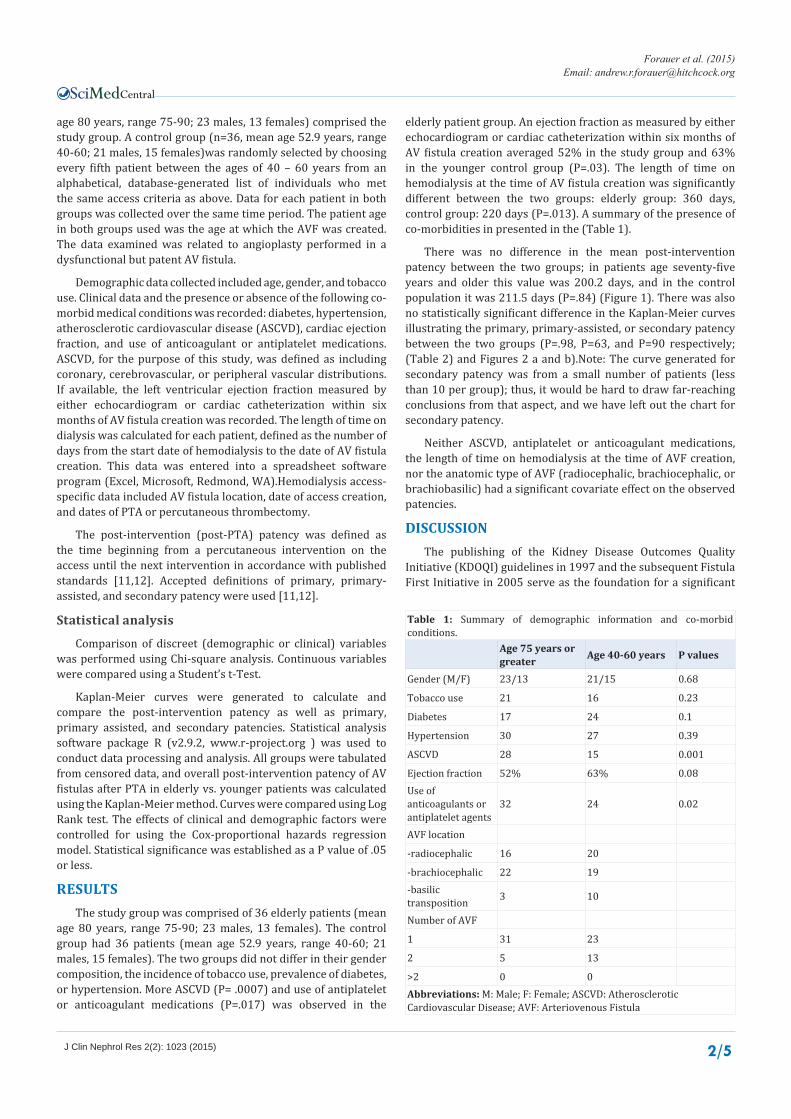
There was no difference in the mean post-intervention patency between the two groups; in patients age seventy-five years and older this value was 200.2 days, and in the control population it was 211.5 days (P=.84) (Figure 1). There was also no statistically significant difference in the Kaplan-Meier curves illustrating the primary, primary-assisted, or secondary patency between the two groups (P=.98, P=63, and P=90 respectively; (Table 2) and Figures 2 a and b).Note: The curve generated for secondary patency was from a small number of patients (less than 10 per group); thus, it would be hard to draw far-reaching conclusions from that aspect, and we have left out the chart for secondary patency.
Neither ASCVD, antiplatelet or anticoagulant medications, the length of time on hemodialysis at the time of AVF creation, nor the anatomic type of AVF (radiocephalic, brachiocephalic, or brachiobasilic) had a significant covariate effect on the observed patencies.
DISCUSSIONThe publishing of the Kidney Disease Outcomes Quality
Initiative (KDOQI) guidelines in 1997 and the subsequent Fistula First Initiative in 2005 serve as the foundation for a significant
Table 1: Summary of demographic information and co-morbid conditions.
Age 75 years or greater Age 40-60 years P values
Gender (M/F) 23/13 21/15 0.68
Tobacco use 21 16 0.23
Diabetes 17 24 0.1
Hypertension 30 27 0.39
ASCVD 28 15 0.001
Ejection fraction 52% 63% 0.08Use of anticoagulants or antiplatelet agents
32 24 0.02
AVF location
-radiocephalic 16 20
-brachiocephalic 22 19-basilic transposition 3 10
Number of AVF
1 31 23
2 5 13
>2 0 0Abbreviations: M: Male; F: Female; ASCVD: Atherosclerotic Cardiovascular Disease; AVF: Arteriovenous Fistula
Central
Forauer et al. (2015)Email:
J Clin Nephrol Res 2(2): 1023 (2015) 3/5
Days 0 90 180 365 730 Patients over 75 27 26 18 11 5 Patients 40-60
28 27 19 11 5
Figure 1 Post-interventional (Post-PTA) Patency. Kaplan-Meier curves for post-PTA patency for patients aged 75 years or older (solid line) and the control group, age 40 – 60 years old (dashed line). There was no significant difference between the curves (p=.84); mean patency was 200.2 days (elderly group) and 211.5 days (control group).
Days 0 90 180 365 730 1095 Patients over 75 36 33 25 14 8 6 Patients 40 - 60 36 31 27 16 9 4
Days 0 90 180 365 730 1095 Patients over 75 27 19 17 13 6 3 Patients 40-60 28 23 19 16 8 4
Figure 2 Kaplan-Meier curves for Primary Patency (2a) and Primary-Assisted Patency (2b).There was no significant difference between those patients age 75 years & older (solid line) and the younger, control group between the ages of 40 and 60 years (dashed line). The p values were .98 and .63respectively.
Table 2: Primary, primary-assisted, secondary, and post-intervention patencies of the two patient groups. Patency is reported in days.
Primary Patency Primary-assisted patency Secondary Patency Post-intervention Patency
Age 75 yrs& older 298 663 701 200
Age 40-60 yrs 373 469 522 211
P-value 0.98 0.63 0.89 0.84

Central
Forauer et al. (2015)Email:
J Clin Nephrol Res 2(2): 1023 (2015) 4/5
effort to promote autologous AV fistula creation in chronic kidney disease patients approaching hemodialysis [13,14]. This emphasis has increased the percentage of patients receiving hemodialysis via this route in the United States from 28% in 2000 to well over 50% by 2010 [15].
This evolution in vascular access strategy is not without controversy. The reported rates of primary AV fistula failure range from 20% to 34.5% in all age groups prior to the current emphasis placed on fistula creation [9,16-18]. Failure rates as high as 40% have been reported in elderly patients [19]. The drive to create fistulas may have unintended consequences; some report an increase in catheter placements for those patients whose fistulas fail to mature adequately for use [20]. PTA is an accepted and crucial technique in maintaining AV access patency; however, there is a monetary cost associated with the increased volume of post-surgical procedures to promote maturity or treat access dysfunction [21-23]. One author observed that 42% of AV fistulas required at least one intervention to become mature, and this was in a practice environment that employed an aggressive preoperative screening program [22]. Given the increasing efforts to create AV fistulas in all patient age groups, the use of angioplasty will accordingly increase as well. It will be important to determine if there are clinical settings that will have lower success rates in order to use available resources wisely or properly formulate alternate treatment strategies.
The emphasis on fistula creation, coupled with the aging hemodialysis population, has resulted in more elderly patients having autologous vein accesses created. The subjective belief that elderly patients tolerate hemodialysis poorly is not necessarily supported by the literature. As early as 1979, one report focusing on patients receiving hemodialysis over the age of eighty concluded that: “Despite the relatively brief mean survival of elderly patients undergoing dialysis, many patients appear to do very well, with survival beyond five years.” [24]. Mortality is increased in older patients, particularly over age 80 years; however it is increased across all age groups of patients undergoing hemodialysis [3,25,26]. Studies investigating the psychological quality of life in elderly patients on dialysis have not shown significant differences when comparing them with age-matched individuals not on hemodialysis [3]. Further, even in the presence of impaired day-to-day activity, the degree of life satisfaction may not necessarily correlate with the physical limitations of typical three-times-per-week hemodialysis [27].
Early series reporting the outcomes of PTA in AV fistulas did not focus on a specific age group. In fact, the descriptive statistics of patient age provided vary from series to series with some reporting only a mean age, others merely an age range. Series presenting surgical outcomes of AV fistula, such as primary and secondary patency, indicate that patient age has no definite negative effect [5-7]. One series of 243 patients divided into groups less than seventy years of age, between 70 and 79 years, and those over the age of eighty, found no differences in primary or secondary AV access patency [28].
In our study, we observed that patient age had no negative effect on the outcome of PTA in treating AVF stenoses. Common medical co-morbidities can play a key role in the vascular biology of AVF inflow arteries and, potentially, outflow veins. Increasing
age can be associated with a higher incidence of diabetes, ASCVD, and hypertension; these are among the factors identified with AVF failure [29]. We did not observe this in our patient population. No difference was found in the incidence of diabetes mellitus (DM) or hypertension between our two groups. In addition, though the incidence of ASCVD was higher in our elderly group, multivariate analysis did not indicate a significant adverse contribution. It seems that cardiovascular risk factors may not impact surgical patency rates or the success of endovascular interventions in the elderly patient population [30].
Furthermore, Kaplan-Meier analysis revealed no difference in the primary, primary-assisted, or secondary patency rates in elderly versus younger patient groups. These observations lead us to conclude that once an elderly patient’s AVF is mature and has demonstrated adequate function, their access responds to PTA as well as a younger control group with no significant difference in post-intervention patency.
As a retrospective study, this project was subject to the inherent limitations of accuracy and documentation of archived, historical clinical information. The actual numbers of patients in each group was small, but the statistical results demonstrated are convincing in terms of similar outcomes. The authors focused on those patients whose AV fistulas were mature and functioning; an evaluation of the number of elderly patients who underwent AV fistula creation was not the subject of the project, and therefore, the primary failure rate of AV fistulas created in our institution’s population was not assessed.
Based on our observations, the post-intervention patency of autologous AV fistulas following PTA is not affected by the age of the patient. Furthermore, age alone should not be viewed as a limitation to the use of PTA in the maintenance of vascular access patency in patients with advanced chronic kidney disease. Similar standards for technical success and patency rates across all patient age groups should therefore be achievable.
REFERENCES1. United States Renal Data System
2. Kutner NG, Brogan D, Hall WD, Haber M, Daniels DS. Functional impairment, depression, and life satisfaction among older hemodialysis patients and age-matched controls: a prospective study. Arch Phys Med Rehabil. 2000; 81: 453-459.
3. Lamping DL, Constantinovici N, Roderick P, Normand C, Henderson L, Harris S, et al. Clinical outcomes, quality of life, and costs in the North Thames Dialysis Study of elderly people on dialysis: a prospective cohort study. Lancet. 2000; 356: 1543-1550.
4. Moranne O, Couchoud C, Vigneau C. PSPA Study Investigators. Characteristics and treatment course of patients older than 75 years, reaching end-stage renal failure in France: The PSPA study. J Gerontol A Biol Sci Med Sci. 2012; 67: 1394-1399.
5. Golledge J, Smith CJ, Emery J, Farrington K, Thompson HH. Outcome of primary radiocephalic fistula for haemodialysis. Br J Surg, 1998; 86: 211-216.
6. Lok CE, Oliver MJ, Su J, Bhola C, Hannigan N, Jassal S. Arteriovenous fistula outcomes in the era of the elderly dialysis population. Kidney Int. 2005; 67: 2462-2469.
7. Weale AR, Bevis P, Neary WD, Boyes S, Morgan JD, Lear PA, et al. Radiocephalic and brachiocephalic arteriovenous fistula outcomes in

Central
Forauer et al. (2015)Email:
J Clin Nephrol Res 2(2): 1023 (2015) 5/5
Forauer AR, Bazylewicz M, Reilley MJ, Kristine A. Giffin BS (2015) Arteriovenous Fistulas in Elderly Hemodialysis Patients: Evaluation of Post-Intervention Patency of Percutaneous Transluminal Angioplasty (PTA). J Clin Nephrol Res 2(2): 1023.
Cite this article
the elderly. J Vasc Surg. 2008; 47: 144-150.
8. Lazarides MK, Georgiadis GS, Antoniou GS, Staramos DN. A meta-analysis of dialysis access outcome in elderly patients. J Vasc Surg. 2007; 45:420-426.
9. Feldman HI, Joffe M, Rosas SE, Burns JE, Knauss J, Brayman K. Predictors of successful arteriovenous fistula maturation. Am J Kidney Dis. 2003; 42:1000-1012.
10. K/DOQI Clinical Practice Guidelines for Vascular Access. Am J Kidney Dis 2006; 48: 177-247.
11. Sidawy, AN, Gray R, Besarab A, et al. Recommended standards for reports dealing with arteriovenous hemodialysis accesses. J Vasc Surg, 2002; 35:603-610.
12. Gray RJ, Sacks D, Martin LG, et al. Reporting standards for percutaneous interventions in dialysis access. J Vasc Interv Radiol, 2003; 14: 433-442.
13. K/DOQI Clinical Practice Guidelines for Vascular Access. Am J Kidney Dis. 1997; 30: 137-240.
14. h t t p : / / w w w . c m s . h h s . g o v / a p p s / m e d i a / p r e s s / r e l e a s e .asp?Counter1386.
15. http://www.fistulafirst.org/home .
16. Winsett OE, Wolma FJ. Complications of vascular access for hemodialysis. South Med J. 1985; 78: 513-517.
17. Fitzgerald JT, Schanzer A, Chin AI, McVicar JP, Perez RV, Troppmann C. Outcomes of upper arm arteriovenous fistulas for maintenance hemodialysis access. Arch Surg, 2004; 139: 201-208.
18. Schild AF, Glenn M, Livingstone J, Alfieri K, Raines J. Maturation and failure rates in a large series of arteriovenous dialysis access fistulas. Vasc Endovascular Surg. 2004; 38: 449-453.