application form the british school al...
TRANSCRIPT

APPLICATION FORM THE BRITISH SCHOOL AL KHUBAIRAT
PO Box 4001, Abu Dhabi, UAE. Tel: +971 2 446 2280 Fax: +971 2 446 1915 Email: [email protected] Website: www.britishschool.sch.ae
FOR OFFICE USE ONLY Application received by HAND/EMAIL/FAX on: __ / ____ /20______
Assessment: YES/NO Date: __________ Time: ______ Year Applied For: _____ Registration No: ______
Sibling Info: Applied/Offered/Registered ___________ Age Appropriate: ______ Class Admitted: _____
To ensure that your child’s application is processed efficiently, please complete this form in CAPITALS, as fully as
possible. Please note that applications cannot be processed unless ALL sections of the Application Form are completed. If a section does not apply, please mark as 'N/A' (ie not applicable) thus indicating that the information in the section has
been noted.
THE CHILD AND SPONSOR’S NAME MUST BE AS DETAILED IN PASSPORT
1. CHILD’S DETAILS
First name Middle name Surname
Date of birth (dd/mm/yyyy)
Place of birth Nationality
Boy Girl
Religion Muslim Christian Other
1st language (ie language spoken at home)
Other languages Fluent in English
YES NO
Date of prospective entry (dd/mm/yyyy)
Year Group for which entry is sought
Previous application to BSAK YES NO Date of previous application
(dd/mm/yyyy)
2. CURRENT SCHOOLING OR PRE-SCHOOL All applications from Nursery upwards must include a copy of your child's latest school/nursery report. NB. A reference will be requested from your child’s current school.
Name of current school Country
Headmaster’s/Principal’s name Tel Email
Date of entry Date of leaving Year/Grade on leaving
Will Transfer Certificate indicate that the above mentioned year has been
completed? YES NO
Is it possible that your child requires special educational support? YES NO
Does your child receive special educational support at their current school? YES NO
If yes please specify:
The school reserves the right to withdraw the place offered before or after admission in the light of
incomplete disclosure.
Has your child encountered any difficulties at his/her previous school?
YES NO
If yes please give details: PTO
FO R OFF ICE US E
Result: ACCEPT / DECLINE

3. OTHER FACTORS
Are there any musical, artistic or sporting achievements that you wish to make us aware of?
Are there any family circumstances which you feel we should be aware of?
4. MEDICAL HISTORY
Allergies Physical limitations
Previous illness (which could affect his/her activities)
Other
5. SIBLINGS Siblings registered at BSAK
YES NO
Name Class
Name Class
Siblings applied for BSAK* YES NO
Name Year Group
Name Year Group
*Would you be willing to accept one place at BSAK? YES NO
6. DETAILS OF CHILD’S SPONSOR (FATHER/MOTHER)
Surname First name Middle name
Title (Mr/Mrs/Dr/HE) Nationality Place of birth
P O Box Home tel Mobile Employer
Email Religion Muslim Christian Other
7. DETAILS OF SPOUSE (WIFE/HUSBAND)
Surname First name Middle name
Title (Mr/Mrs/Dr/HE) Nationality Place of birth
P O Box Home tel Mobile Employer
Email Religion Muslim Christian Other
To apply for entry to The British School Al Khubairat for my above mentioned child, I understand that all fees are non-refundable and non-transferable. I declare that I am the child's parent/legal guardian and
that, to the best of my knowledge and belief, all information given is correct and complete. I am aware that you will contact my child’s current school for a reference.
Signed ___________________________________________________ Date ______________________
Please see checklist and information sheet for details of other documents to accompany this application form.
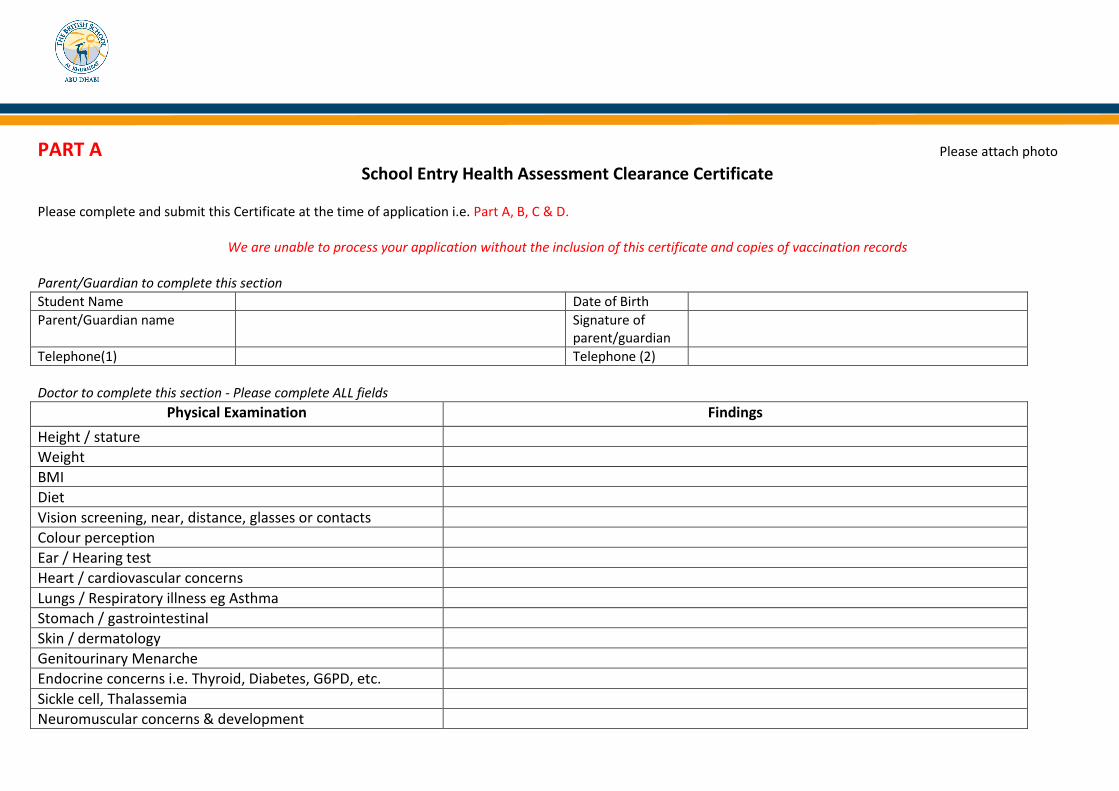
PART A Please attach photo
School Entry Health Assessment Clearance Certificate Please complete and submit this Certificate at the time of application i.e. Part A, B, C & D.
We are unable to process your application without the inclusion of this certificate and copies of vaccination records
Parent/Guardian to complete this section
Student Name Date of Birth
Parent/Guardian name
Signature of parent/guardian
Telephone(1) Telephone (2)
Doctor to complete this section - Please complete ALL fields
Physical Examination Findings
Height / stature
Weight
BMI
Diet
Vision screening, near, distance, glasses or contacts
Colour perception
Ear / Hearing test
Heart / cardiovascular concerns
Lungs / Respiratory illness eg Asthma
Stomach / gastrointestinal
Skin / dermatology
Genitourinary Menarche
Endocrine concerns i.e. Thyroid, Diabetes, G6PD, etc.
Sickle cell, Thalassemia
Neuromuscular concerns & development

Seizure, convulsion, epilepsy, concussion history
Musculoskeletal system (including vertebral column alignment) Flat feet, neck back injuries, past concussion
Speech and language development as age appropriate
Sleep problems
Toileting concerns
Emotional behaviour difficulties
Has received care from the following specialists in the past or present, please provide details: Speech therapist, occupational therapist, physiotherapist, educational psychologist, psychiatrist, counsellor
Allergies to foods, animals, bees, jellyfish, medication: Please specify… Experienced anaphylaxis?
Last dental appointment and outcome
List all medication currently taken and medication required for regular school and related school activities i.e. sports
Does this child have any special health or educational needs which could affect his / her education: yes / no? If yes, please provide details
Past surgeries / operations
Past or present concerns for TB, hepatitis or other communicable illnesses etc.
Other past / present concerns. Please specify…
Referral indicated after today’s assessment: yes / no? Please specify…
Doctor’s Name (Print) :
Doctor’s Signature:
Doctor’s / Clinic Email : Doctor’s / Clinic Telephone:
Doctor’s / Clinic Stamp:

PART B
Immunisation Status All schools in the UAE are mandated to hold immunisation records on all children from birth to present.
Doctor’s Reference: Kindly review this student’s immunisation history and immunise as appropriate. Please also attach immunisation details for school health records. Students entering Year 1 or Year 11 will be offered immunisations at school in line with those offered through the Abu Dhabi Ambulatory School Health Department programme. It is the parents’ responsibility to ensure immunisations are up to date prior to commencing school.
Unless there is a reliable vaccination history, individuals should assume to be unimmunised and a full course of immunisations planned
Individuals coming to the UAE part way through their immunisation schedule should be transferred onto the UAE schedule and immunised as appropriate for age
If the primary course has been started but not completed, continue where left off- no need to repeat doses or restart course
Planned catch up immunisations schedule with minimum number of visits and within a minimum possible timescale - aim to protect individuals in shortest time possible
See link for UAE schedule 2013>(http://www.haad.ae/HAAD/LinkClick.aspx?fileticket=gX0cyy7oStY%3D&tabid=183
Doctor’s Immunisation Clearance please tick A or B
A) I certify that this child is adequately or age appropriately immunised in accordance with the UAE schedule
B) I certify that I have reviewed this child’s Immunisation Status and have recommended the following immunisations:
1. 3. 2. 4.
Scheduled Appointment date: Doctors Name: Doctors Signature: Clinic stamp: Telephone / Email contact details:

Deferred Immunisations
If immunisations have been deferred on medical, ethical or religious reasons, please sign below. I have been advised by my doctor at this time to decline or defer the vaccination(s) recommended for my child. I know that failure to follow the recommendations about vaccination may endanger the health or life of my child and others with whom my child might come into contact. I know that I may readdress this issue with my child’s doctor or nurse at any time and that I may change my mind and accept vaccination for my child any time in the future.
Parent/Guardian full name: Parent/Guardian signature:
Date:

PART C Consent for Prescription Medication during the School Day or Related School Activities
(to be completed, signed and stamped by Licensed Physician) Link: http://www.haad.ae/HAAD/LinkClick.aspx?fileticket=rJGicUPp-Bw%3d&tabid=820
Student Name (First, Middle, Last) Date of Birth (Day/Month/Year)
Health condition for which the medication is prescribed: Name of medication:
Dose:
This medication should be continued until:
Route for administering the medication: By mouth Injection Topical Inhalation Other : (please specify)………………………………………………..
What time does medication need to be given at school: ………………………………………..AM ……………………………………….PM
Any precautions that school personnel need to know?
Any contraindications that school personnel need to know?
What are possible reactions/side effects?
What should be done in the event of reaction/side effect?
Check appropriate box below: I authorise this student to self-administer the above medication The above medication can only be administered by a HAAD Licensed School Nurse
Name, address, phone number of Healthcare Provider
Signature of the treating physician prescribing the medication
Parent/Guardian to complete I understand it is my responsibility to send the medication to school in the original pharmacy container labelled with my child’s name, treating physician’s instructions/care plan and any other documentation to assist in the safe administration of the specified medications. Parent/Guardian full name: Parent/Guardian signature: Date:

PART D SCHOOL HEALTH RECORD Consent and Declaration
Please note that the following consents are valid for the duration of time that your child attends BSAK, unless you inform the school otherwise in writing or by telephoning the school nurse directly.
Print Child’s Name
Date of Birth
As the parent / guardian of the child above I give my consent to the following: 1. Consent for Emergency Treatment
Should your child require prompt medical treatment you will be contacted and asked to collect your child from school. In the event of
a serious emergency, an ambulance will be called immediately. You will be contacted and advised to meet at the Hospital; the nearest hospital is Sheikh Khalifa Medical City on 24th Street near Karama Compound. I consent to my child receiving medical emergency care as advised by the licensed healthcare provider at the time.
I consent that my child may receive the emergency care as outlined above. Parents Name (Print): ________________________________________________________
Parents Signature ________________________________________________________
Date ________________________________________________________
2. School Declaration The school requires parents to disclose of any health and special educational needs at the time of the application. Failure to do so may result in the parent meeting additional costs through support or loss of a school place. The school reserves the right to withdraw the place offered before or after admission in the light of incomplete disclosure.
I have understood and agree to the above conditions.
Parents Name (Print): ________________________________________________________
Parents Signature ________________________________________________________
Date ________________________________________________________
3. Consent for the Administration of Paracetamol and First Aid In the event of your child developing discomfort from dental, menstruation, muscular or mild cold symptoms, without fever, the
school nurse may, after assessment, wish to administer age-appropriate Paracetamol to your child No alternative would be offered Students with fever are referred home for care All students who receive medication are monitored and you will be duly notified of any new concerns Minor first aid treatments including topical application of antihistamine and antiseptic products
I consent to my child being given Paracetamol and First Aid, should it be considered necessary, by the Licensed School Nurse.
Parents Name (Print): ________________________________________________________
Parents Signature ________________________________________________________
Date ________________________________________________________
4. School Health Screening The Health Authority of Abu Dhabi (HAAD) mandates that all children are screened annually for health concerns, this includes a simple vision, height, weight, body mass index (BMI). Parents of children identified with a possible concern will be contacted by the school nurse. Results of screening are not shared with students. All results are recorded in your child’s school health record and transferred to HAAD as mandated. For further information regarding school health screening, refer to the HAAD website http://www.haad.ae
I consent to my child being included in the mandated HAAD health screening as outlined above. Parents Name (Print): ________________________________________________________
Parents Signature ________________________________________________________
Date ________________________________________________________

PART D
الـسجل الـصحي للطـالـب
الموافقة واإلقــرار
من خالل االتصال لية تكون سارية المفعول خالل الوقت الذي يحضر فيه الطفل الى مدرسة الجالية في الخبيرات مالم يتم إبالغ المدرسة خطيا بخالف ذلك أو يرجى العلم بأن الموافقات التا
مباشرة بالممرضة في المدرسة.
تاريخ الوالدة اسم الطالب
:لى مايليبصفتي ولي أمر/ الوصي على الطفل المذكور أعاله فإنني أوافق ع
الموافقة على العالج في الحاالت الطارئة .1
رئة الخطرة يتم استدعاء في حال تتطلب األمر إعطاء الطفل عالجا طبيا بشكل فوري سوف يتم اإلتصال بكم والطلب منكم اصطحاب الطفل من المدرسة. وفي الحاالت الطا
حضور الى المستشفى، علما أن المستشفى األقرب إلينا هي مدينة الشيخ خليفة الطبية في الشارع الرابع سيارة اسعاف على الفور. عندها يتم االتصال بكم والطلب منكم ال
حية المفوض في ذلك الوقت.والعشرين قرب مجمع الكرامة. وعليه، فإنني أوافق على أن يتلقى طفلي الرعاية الطبية الطارئة المطلوبة التي نصح بها مزود الرعاية الص
لقي طفلي الرعاية الطارئة وفق ما هو موضح أعاله.أوافق على ت
)طباعة(: ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــاسم الوالدين
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ توقيع الوالدين:
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ التاريخ:
إقـــرار الـمـدرســة .2
لى تكبد تكاليف إضافية لوالدين اترجو المدرسة من الوالدين اإلفصاح عن أية مشاكل صحية وتربوية خاصة في وقت تقديم طلبات التسجيل. علما أن عدم القيام بذلك قد يعرض ا
يجة اإلفصاح غير الكامل.من خالل تقديم خدمات المساندة أو الى فقدان المقعد في المدرسة. هذا وتحتفظ المدرسة بحقها بسحب المقعد المتاح قبل أو بعد القبول نت
لقد اطلعت على الشروط أعاله وأوافق عليها
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ)طباعة(: ــــــــــــــــــــــاسم الوالدين
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ توقيع الوالدين:
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ التاريخ:
وتقديم اإلسعافات األولية له باراسيتامولالموافقة على إعطاء الطالب دواء ال .3
ب الممرضة في المدرسة في حال كان الطالب يعاني من آالم في أسنانه أو آالم مصاحبة للدورة الشهرية أو آالم في العضالت أو أعراض رشح خفيف بدون حمى، قد تطل
باراسيتامول للطالب تتوافق مع عمره. بعد تقييم الحالة إعطاء جرعة
ال يتم تقديم أي عالج بديل
.يتم إرجاع الطالب الذين يعانون من الحمى الى البيت للرعاية
.يتم مراقبة كافة الطالب الذين تلقوا عالجا ويتم إبالغكم حسب األصول بأية مستجدات بهذا الشأن
وية المضادة للهيستامين واألدوية المطهرة. تتضمن اإلسعافات األولية االستعمال الموضعي لألد
أوافق على أن يتم إعطاء طفلي الباراسيتامول وإجراء اإلسعافات األولية له، في حال اقتضت الضرورة ذلك، من قبل ممرضة المدرسة المرخصة
ـــــــــــــــــــــ)طباعة(: ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــاسم الوالدين
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ توقيع الوالدين:
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ التاريخ:
الفحص الصحي في المدرسة .4
(. BMI)أبوظبي القيام بإجراء فحص لكافة األطفال سنويا فيما يتعلق بصحتهم وهذا يتضمن إجراء فحص بسيط للنظر والطول والوزن ومؤشر كتلة الجسم -ة الصحةتتطلب هيئ
ن نتائج الفحص ال يجري مشاركتها مع وعليه، سوف يتم االتصال بأولياء أمور األطفال الذين يتم تشخيص حالة محتملة لهم من قبل ممرضة المدرسة. إضافة الى ذلك، فإ
أبوظبي وفق ما هو مطلوب. ولمزيد من المعلومات فيما يتعلق بالفحص الطبي -الطالب، بحيث يتم تدوين كافة النتائج في سجل الطالب الصحي ومن ثم إحالته الى هيئة الصحة
www.haad.aeأبوظبي على الموقع االلكتروني: -في المدرسة، يرجى مراجعة هيئة الصحة
أبوظبي وفق ما هو موضح أعاله -أوافق على أن يخضع طفلي الى الفحص الصحي المطلوب من قبل هيئة الصحة
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ )طباعة(: اسم الوالدين
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ الوالدين: توقيع
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ التاريخ:

Dear Prospective Parents School Website & Publications Photographs of pupils at work, school outings and special events are included on the website and in publications. Including images of pupils on the school website and publications can be motivating for the pupils involved and provide a good opportunity to promote the work of the school. However, the school has a duty of care towards pupils which means that we would never include the full name of a pupil alongside an image. Most of the photographs show pupils in groups engaged in an activity. We realise that some parents may not wish their child’s photograph to appear on the website, therefore please complete the slip below and return it along with your application form. Yours sincerely
Mrs Elaine Rawlings Acting Head
School Website & Publications
We do not object to our child’s photograph appearing on the school website/publications □ or
We do object to our child’s photograph appearing on the school website/publications □
* please tick one option Name of Child Class Name of Child Class Name of Child Class Signature Date

APPLICATION AND ADMITTANCE PROCEDURES FOR ALL APPLICANTS The UAE Ministry of Education requires ALL the following documentation to be supplied to the school BEFORE ENTRY. Please supply the following documents along with a completed application form; the only documents that will be excused are the UAE Residence Visa and Emirates ID card if you are not yet resident in the Emirates.
Please ensure you submit the originals and copies of the following documents or the application will not be accepted. Applications for entry cannot be accepted until ALL the required paperwork has been supplied. 1. BIRTH CERTIFICATE * Original and colour photocopy Applicant’s original Birth Certificate (BC) plus a colour copy.* Applicants born in South American/African/Eastern European/Asian and Middle Eastern countries must have their BC attested by the Ministry of Health in the issuing birth country and UAE Ministry of Foreign Affairs. Applicants born in a GCC country must have their BC attested by the Ministry of Health in the issuing birth country. Applicants born in the UAE need only supply their Arabic BC. BCs not in English must be translated into English or Arabic. 2. PASSPORT PHOTOS 3 per applicant 3. PASSPORTS * Original and colour photocopy Sponsor’s original passport including valid UAE Residence Visa, plus colour copy* Applicant’s original passport including valid UAE Residence Visa, plus colour copy*
4. EMIRATES ID CARD
Colour copy front and back or stamped completed copy of ID card application form.
5. SCHOOL REPORTS Please note that the school will request a confidential school report from the current school.
True copy of previous academic year or 2 most recent mid-term reports accepted. Applicants requiring Learning Support must also submit external reports ie Ed Psych, OT.
6. TRANSFER CERTIFICATE (for all new Year 1 students upwards, plus all new FS2 students who have already attended school)
Original only, faxed and emailed copies not accepted. Please refer to attached samples. Only required if you accept a place for your child/ren.
The Transfer Certificate (TC) is only required when the child has been offered a place. It should be completed in English by the previous school, on official headed paper and bear the school stamp/seal. Students transferring from South America/Africa/Middle East and Asia must have their TC attested by the Ministry of Education, Ministry of Foreign Affairs and UAE Embassy before relocating to Abu Dhabi. Students transferring from a GCC country must have their TC attested by the Ministry of Education in the issuing country. Students transferring from within the UAE are issued with an Arabic Transfer Certificate by the former school which is stamped at the Education Zone in the Emirate concerned. Students transferring from another school in Abu Dhabi are not required to provide a TC as their records will be electronically transferred by the outgoing school. 7. VISA LETTER TO BE SUPPLIED BY SPONSOR COMPANY ~
A sample letter is attached. This is only required in the absence of a valid residence visa.
8. BSAK’S WEBSITE PERMISSION FORM Please tick one of the options 9. BSAK’S SCHOOL HEALTH CERTIFICATE AND CONSENT AND DECLARATION FORM
Please attach an up to date vaccination record to the completed school health certificate and consent and declaration form
Notes:
* The original Birth Certificate (of applicant) and passports (of applicant and sponsor) must be presented for
checking at the time of application and will be returned immediately.
~ If the UAE residence visa of the sponsor or the applicant has not been issued, the applicable passport (with a photocopy) showing the arrival stamp must be presented instead. In such a case, a letter from the employer
of the sponsor must also be submitted confirming that the visa application is being processed. This letter must refer to the child by name. When the relevant visa has been issued, a copy must be provided to the school immediately.
Your child’s application is only valid for 1 year. If a place is not secured within the year you will need to reapply
for the next academic year.
NB: Fees are Non-Transferable and Non-Refundable

SAMPLE TRANSFER LETTER – TRANSFERRING FROM ANY OTHER COUNTRY AT THE END OF THE ACADEMIC YEAR
Please ask your child/ren’s current school to type this template on the School’s letterhead,
showing the full name and address, including country and telephone number of school.
TO WHOM IT MAY CONCERN
1. Name : 2. Date of Birth : dd/mm/yyyy 3. Place of Birth : 4. Date of Admission : dd/mm/yyyy 5. Class of Admission : 6. Last Year/Grade Attended : (equivalent to Year _____ in the English curriculum) 7. Date of Leaving : dd/mm/yyyy 8. Reason for Leaving : 9. Completed Year _____ and has been promoted to Year ______ for the Academic Year 2015/2016.
(NOTE: Point 9 is only applicable at the end of an academic year i.e. June for Northern Hemisphere and December for Southern Hemisphere. If your child is transferring mid academic year, please delete point 9).
Signature of Headmaster/Principal: Date: dd/mm/yyyy (PLEASE INCLUDE THE SCHOOL STAMP)
Parents should note that without this letter it will not be possible to legally register your child
in school or with the Ministry of Education in Abu Dhabi.
Students transferring from South America/Africa/Middle East and Asia must have their Transfer Certificate attested (stamped) by:
the Ministry of Education of the country in which the previous school is situated; that country's Ministry of Foreign Affairs; and
the U.A.E. Embassy. If there is no U.A.E. Embassy in the country concerned go to the Embassy of your Nationality
Students transferring from a GCC country must have their Transfer Certificate attested (stamped) by:
the Ministry of Education of the country in which the previous school is situated.

SAMPLE VISA LETTER TO BE SUPPLIED BY SPONSOR'S EMPLOYER
Please ask the sponsor’s new employer to type the following on the Sponsor Company’s letterhead, showing the full name, address, email and telephone number of the Company in the UAE
Version 1 (if Sponsor has his/her own Residence Visa) Date The British School Al Khubairat P O Box 4001 Abu Dhabi UAE Dear Registrar This is to certify that Mr/Mrs _________________ is employed with our company and his/her Residence Visa has been obtained. We are currently processing the Residence Visa for his/her child(ren) namely: (Each child's name to be listed) and we will forward these when available. Yours sincerely Authorised Company Representative ________________________________________________________________________________________________ Version 2 (if Sponsor does not yet have Residence Visa) Date The British School Al Khubairat P O Box 4001 Abu Dhabi UAE Dear Registrar This is to certify that Mr/Mrs ___________________ is employed with our company in the position of ______________. We are currently processing the Residence Visa for him/her and his/her child(ren) namely: (Each child's name to be listed) and we will forward these when available. Yours sincerely Authorised Company Representative

CHECKLIST FOR SUPPORTING DOCUMENTATION
1 Applicant’s Birth Certificate and copy
i) BC issued by the birth country of the applicant
ii) UAE Arabic Birth Certificate, if the applicant is born in the UAE
iii) Attestation of BC if child born in Africa/Asian/Arab/Eastern European & South American Countries by Embassy and Ministry of Foreign Affairs
iv) Attestation of BC if child born in a GCC country by the Ministry of Health in the country of birth
v) Legal translation of BC into English/Arabic
2 3 passport photos of applicant
3 i) Applicant’s passport and copy
ii) Applicant’s UAE Residence Visa / Diplomatic ID and copy
iii) Sponsor’s passport and copy
iv) Sponsor’s UAE Residence Visa / Diplomatic ID and copy
v) Change of name deed if applicant’s name differs to BC
4 Copy of Emirates ID card (front and back) or copy of stamped application form if ID card not yet received
5 Company letter (if visa under process)
6 School report ( Nursery – Year 12)
i)
Mid Year Applications for Year 7 Copy of MIDYIS Data Test if available Applications for Year 8 – Year 10 Copy of MIDYIS Data Test if available
ii)
Year 12 Applications Latest two school reports Predicted GCSE results Mock results when received Reference letter from current school Provisional list of A level options
iii)
Educational Psychologist report and IEP for students with Special Educational Needs
7 BSAK’s website permission form
8 BSAK’s school health certificate plus up to date vaccination record
9 Transfer Certificate (only required if we offer a place and if transferring from a school outside Abu Dhabi)
i) Original Transfer Certificate in English or Arabic
ii) Attestation of T/C for students coming from Africa/Asia/Middle East & South America
iii) Arabic T/C (transfers within UAE)
iv) No Objection Letter from parents if student is repeating the year at BSAK.