aortic stenosis. introduction etiology/classification etiology/classification pathophysiology...
TRANSCRIPT
Aortic StenosisAortic Stenosis
IntroductionIntroduction
Etiology/ClassificationEtiology/Classification PathophysiologyPathophysiology Clinical ManifestationsClinical Manifestations EvaluationEvaluation ManagementManagement
Obstruction to left Obstruction to left ventricular outflowventricular outflow ValvularValvular
• Calcific/DegenerativeCalcific/Degenerative• BiscuspidBiscuspid• RheumaticRheumatic• CongenitalCongenital
SupravalvularSupravalvular• Uncommon. Occurs as part of a congenital syndrome or Uncommon. Occurs as part of a congenital syndrome or
from lipid deposits in severe familial hyperlipidemiasfrom lipid deposits in severe familial hyperlipidemias SubvalvularSubvalvular
• CongenitalCongenital• Fibromuscular membrane present in the LVOTFibromuscular membrane present in the LVOT• Pathogenesis not completely understoodPathogenesis not completely understood
Hypertrophic CardiomyopathyHypertrophic Cardiomyopathy
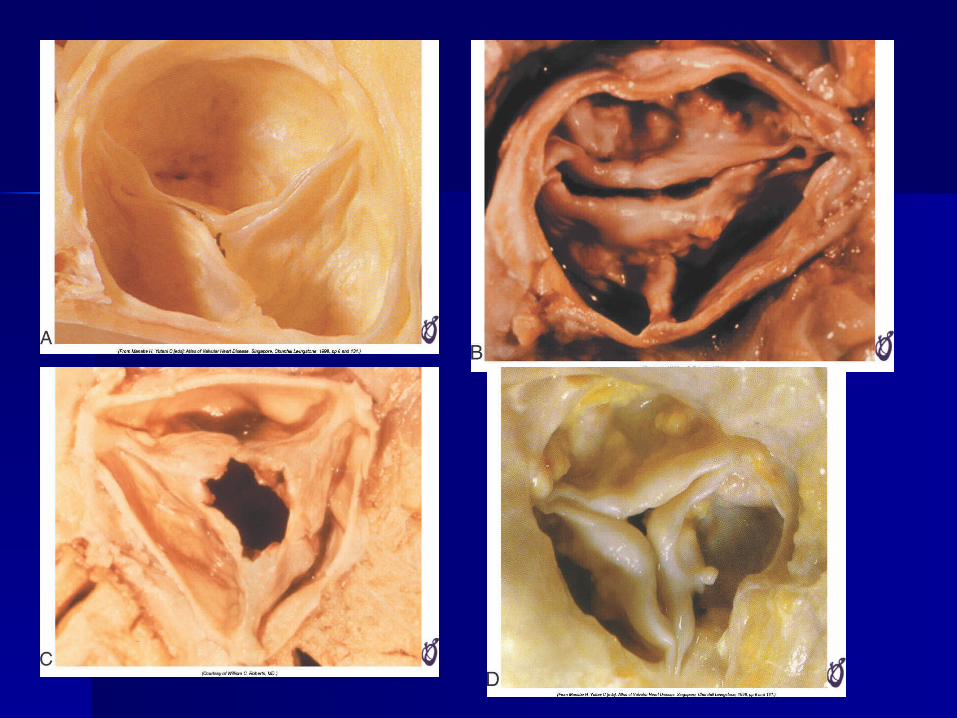
Valvular Aortic Valvular Aortic StenosisStenosis Calcific/DegenerativeCalcific/Degenerative
• Most commonMost common• Normal trileaflet valve develops “age-related” calcificationNormal trileaflet valve develops “age-related” calcification• Presents later in life (age 70-85)Presents later in life (age 70-85)
Bicuspid valveBicuspid valve• Present in 1-2% of the populationPresent in 1-2% of the population• More prevalent in men (70-80% of cases)More prevalent in men (70-80% of cases)• Usually presents at a younger age (45-65)Usually presents at a younger age (45-65)
RheumaticRheumatic• Preferentially involves the mitral valve, so Rheumatic AS Preferentially involves the mitral valve, so Rheumatic AS
diagnosed when occurs concurrently with mitral valve diseasediagnosed when occurs concurrently with mitral valve disease CongenitalCongenital
• Typically unicuspid valve with single eccentric orificeTypically unicuspid valve with single eccentric orifice Ochronosis with alkaptonuriaOchronosis with alkaptonuria
• Anyone?Anyone?
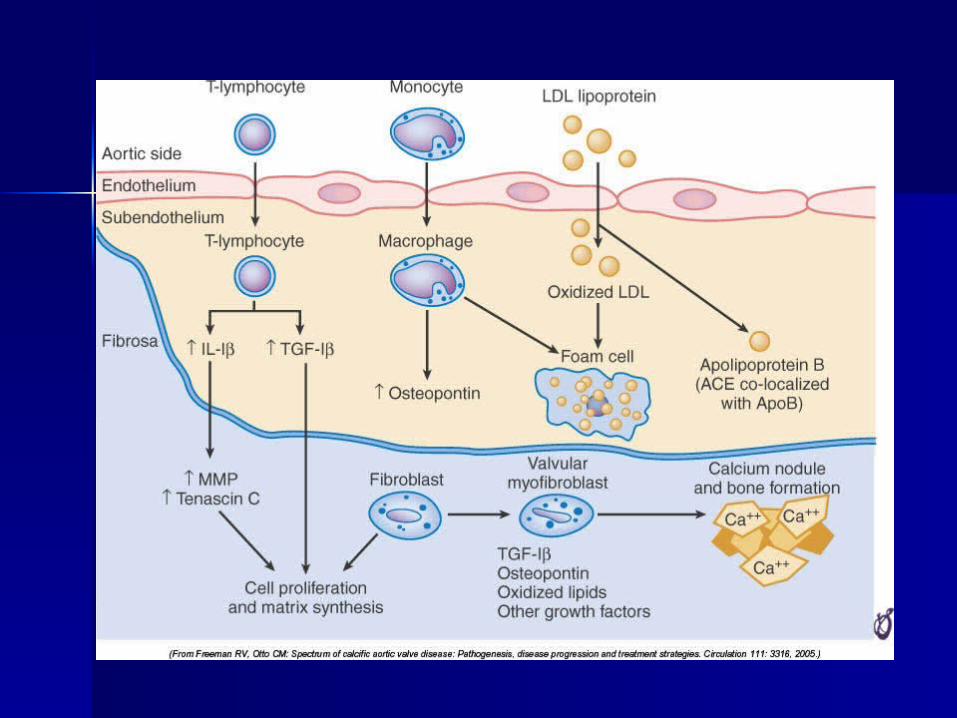
Calcific/Degenerative Calcific/Degenerative ASAS Active disease processActive disease process “Rather than representing a degenerative and
unmodifiable process, valvular aortic stenosis is an active process initiated at least in part by mechanical injury, mediated by lipid infiltration and a chronic inflammatory reaction, and further characterized by accumulation of extracellular matrix secreted primarily by resident valve fibroblasts as a response to inflammatory injury.” (Circulation 1994;90:844-53)
Evidence that hemodynamic stress plays a role, as calcium deposition occurs on the aortic side of the valve where turbulence and shear stress are high.
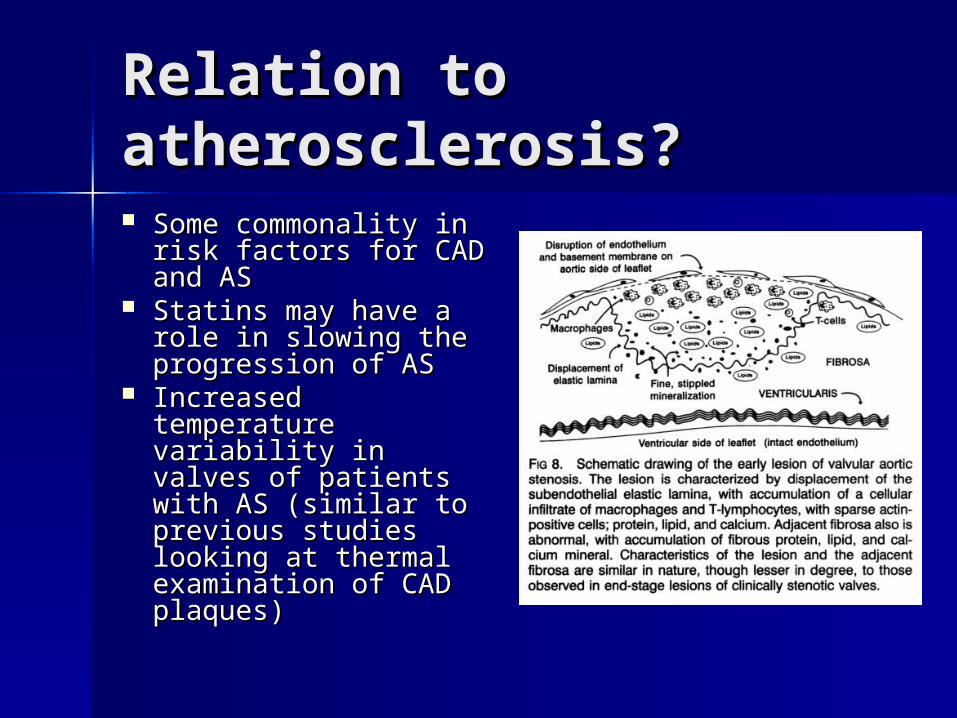
Relation to Relation to atherosclerosis?atherosclerosis? Some commonality in Some commonality in
risk factors for CAD risk factors for CAD and ASand AS
Statins may have a Statins may have a role in slowing the role in slowing the progression of ASprogression of AS
Increased Increased temperature temperature variability in valves of variability in valves of patients with AS patients with AS (similar to previous (similar to previous studies looking at studies looking at thermal examination thermal examination of CAD plaques)of CAD plaques)
NormalNormal
Normal anatomy: three thin cusps Normal anatomy: three thin cusps with unrestricted systolic openingwith unrestricted systolic opening
Normal area 3-4 cmNormal area 3-4 cm²² Normal opening produces 2cm Normal opening produces 2cm
leaflet separationleaflet separation Normal velocity: approx 1 m/sNormal velocity: approx 1 m/s
PathophysiologyPathophysiology
Aortic sclerosis produces thickening of the Aortic sclerosis produces thickening of the valves, but no obstruction to outflowvalves, but no obstruction to outflow
When stenosis develops, the functional area When stenosis develops, the functional area of the valve decreases and causes a of the valve decreases and causes a measurable obstruction of outflowmeasurable obstruction of outflow
Concentric LVH develops with normal Concentric LVH develops with normal chamber sizechamber size
Diastolic dysfunction due to increased Diastolic dysfunction due to increased myocardial cell mass and interstitial fibrosismyocardial cell mass and interstitial fibrosis
Atrial contraction plays an important role in Atrial contraction plays an important role in filling of the left ventricle in ASfilling of the left ventricle in AS
Loss of appropriately timed atrial contraction Loss of appropriately timed atrial contraction could cause clinical deteriorationcould cause clinical deterioration
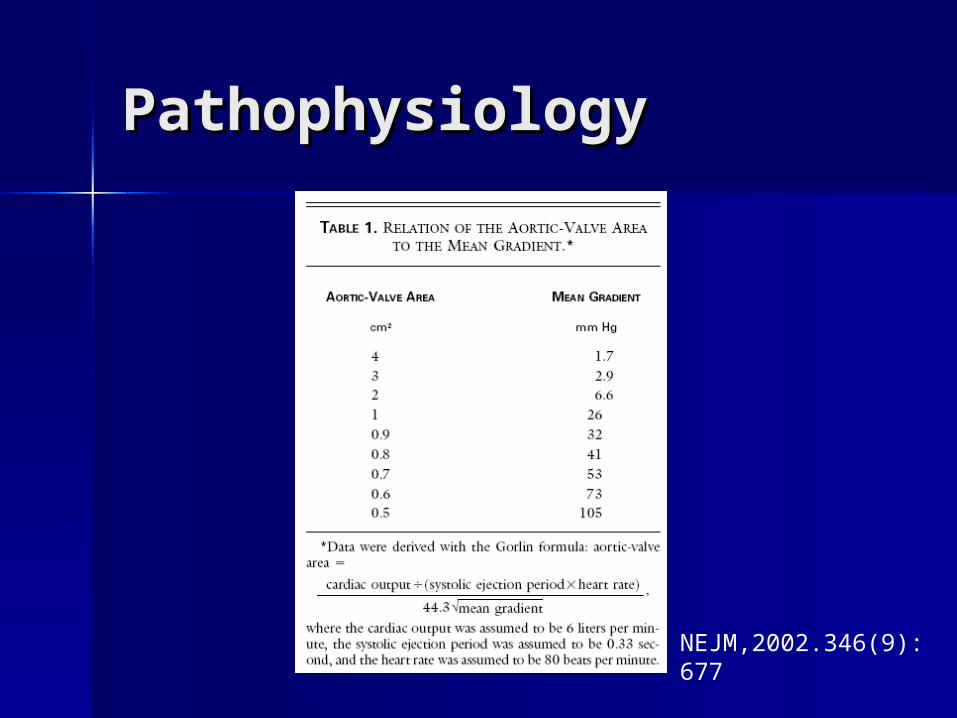
PathophysiologyPathophysiology
NEJM,2002.346(9): 677
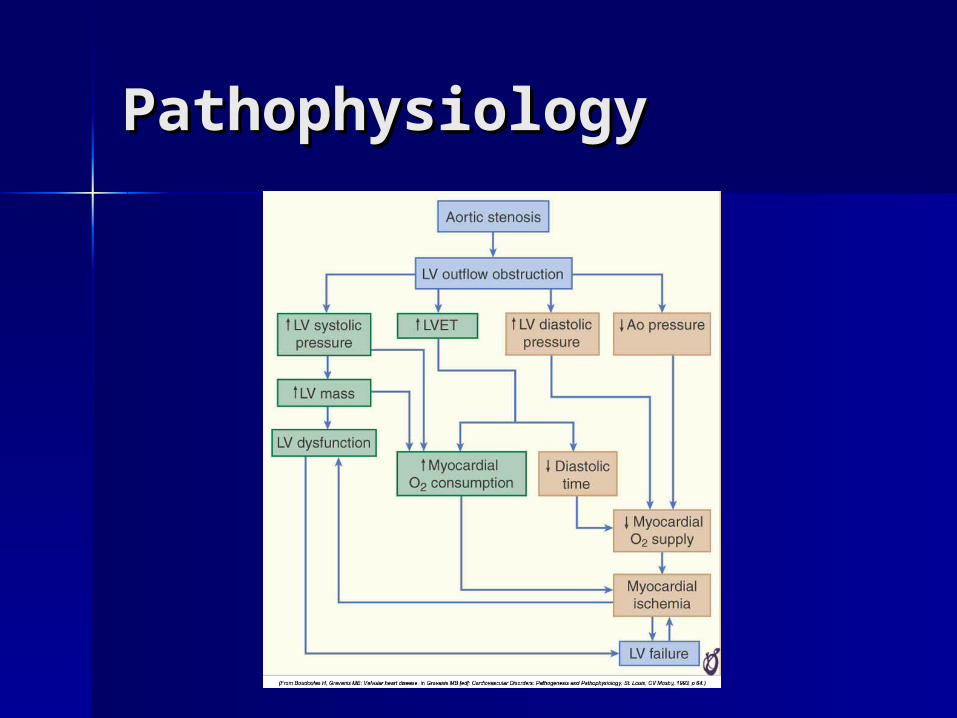
PathophysiologyPathophysiology
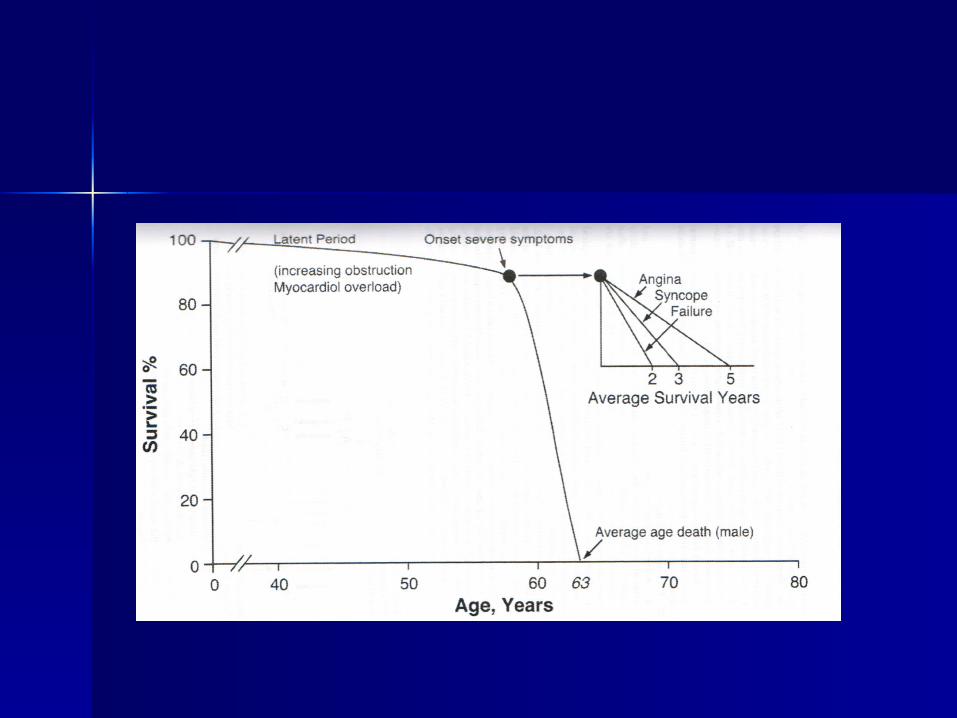
SymptomsSymptoms
Asymptomatic (long latency period)Asymptomatic (long latency period) Decrease in exercise toleranceDecrease in exercise tolerance FatigueFatigue DyspneaDyspnea AnginaAngina SyncopeSyncope Heart FailureHeart Failure
Signs (Physical Exam)Signs (Physical Exam)
Loud, late-peaking systolic murmurLoud, late-peaking systolic murmur Radiation to the carotidsRadiation to the carotids Single or paradoxically split S2Single or paradoxically split S2 Delayed and Diminished carotid Delayed and Diminished carotid
upstroke (Pulsus parvus et tardus)upstroke (Pulsus parvus et tardus) Low output states may affect intensity Low output states may affect intensity
of the murmur and carotid upstrokeof the murmur and carotid upstroke
Associated increase in GI bleeding Associated increase in GI bleeding from angiodysplasiafrom angiodysplasia
EKG and CXREKG and CXR
Left ventricular hypertrophy (85 Left ventricular hypertrophy (85 percent of patients)percent of patients)
Left atrial abnormality (80 Left atrial abnormality (80 percent)percent)
Rounding of the left ventricular Rounding of the left ventricular border with dilatation of the border with dilatation of the ascending aortaascending aorta
EchocardiographyEchocardiography
QualitativeQualitative• 2D imaging of valve anatomy (number of 2D imaging of valve anatomy (number of
leaflets)leaflets)• Calcification/thickening, valve openingCalcification/thickening, valve opening• Left ventricular functionLeft ventricular function• Chamber size, wall thicknessChamber size, wall thickness
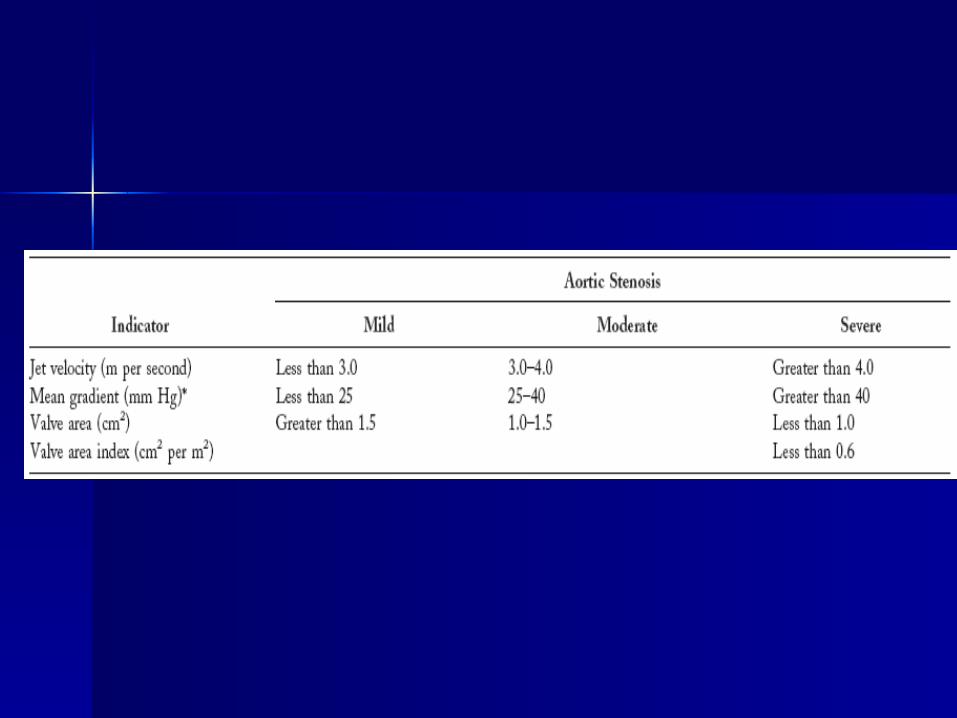
QuantitativeQuantitative• Peak aortic valve velocityPeak aortic valve velocity• Mean and maximum pressure gradientsMean and maximum pressure gradients• Aortic valve area (continuity equation)Aortic valve area (continuity equation)• Ratio of outflow tract to aortic jet velocityRatio of outflow tract to aortic jet velocity
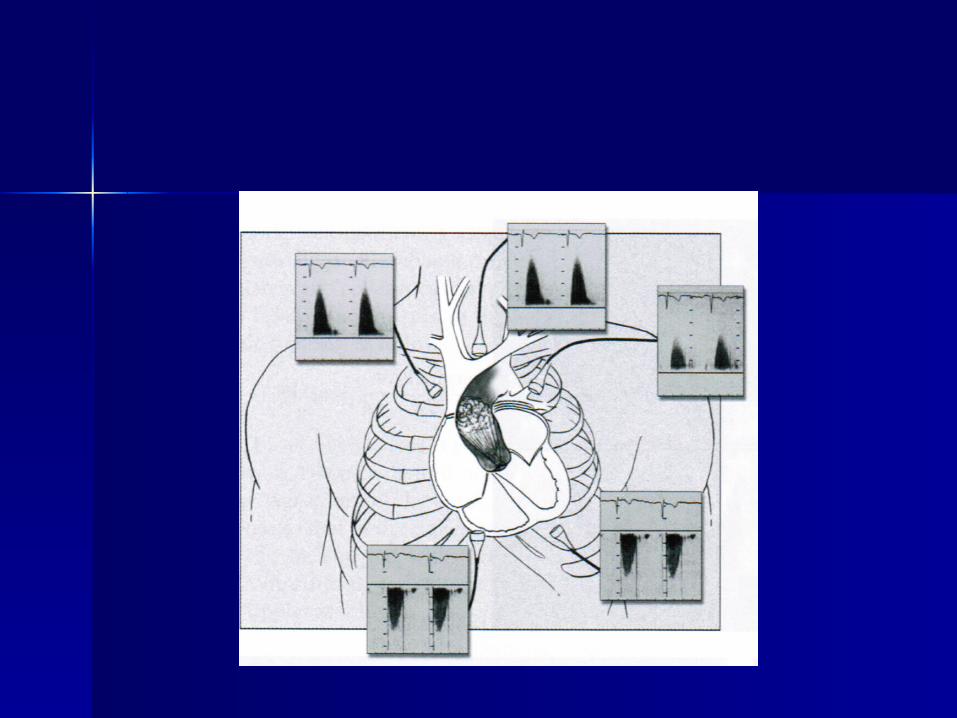
Quantitative Doppler Quantitative Doppler AssessmentAssessment Dedicated non-imaging transducerDedicated non-imaging transducer
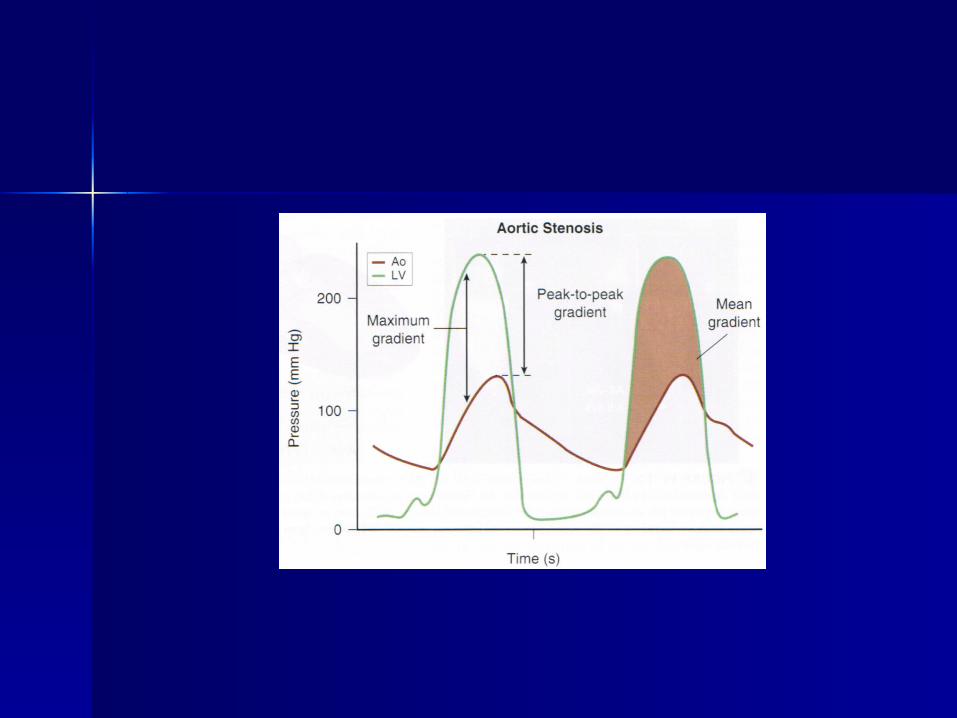
Maximum pressure gradient using the Maximum pressure gradient using the simplified Bernoulli equationsimplified Bernoulli equation
∆∆Pmax = 4(Vmax)²Pmax = 4(Vmax)²
Mean pressure gradient obtained from Mean pressure gradient obtained from planimetry of the Doppler envelope; computer planimetry of the Doppler envelope; computer integrates velocity data to provide mean valueintegrates velocity data to provide mean value
Mean pressure gradient can also be estimated Mean pressure gradient can also be estimated from published regression equations (for from published regression equations (for native valve AS):native valve AS):
∆∆Pmean = (∆Pmax/1.45) + 2mmHgPmean = (∆Pmax/1.45) + 2mmHg
Quantitative Quantitative AssessmentAssessment Pressure gradients are dependent on Pressure gradients are dependent on
volume flow rates in addition to valve volume flow rates in addition to valve narrowingnarrowing
Differences in stroke volume can lead Differences in stroke volume can lead to inaccurate assessment of stenosis to inaccurate assessment of stenosis severityseverity
Coexisting AI will have a high Coexisting AI will have a high transaortic pressure gradienttransaortic pressure gradient
Patients with LV systolic dysfunction or Patients with LV systolic dysfunction or coexisting MR may have low coexisting MR may have low transaortic pressure gradienttransaortic pressure gradient
Quantitative Quantitative AssessmentAssessment
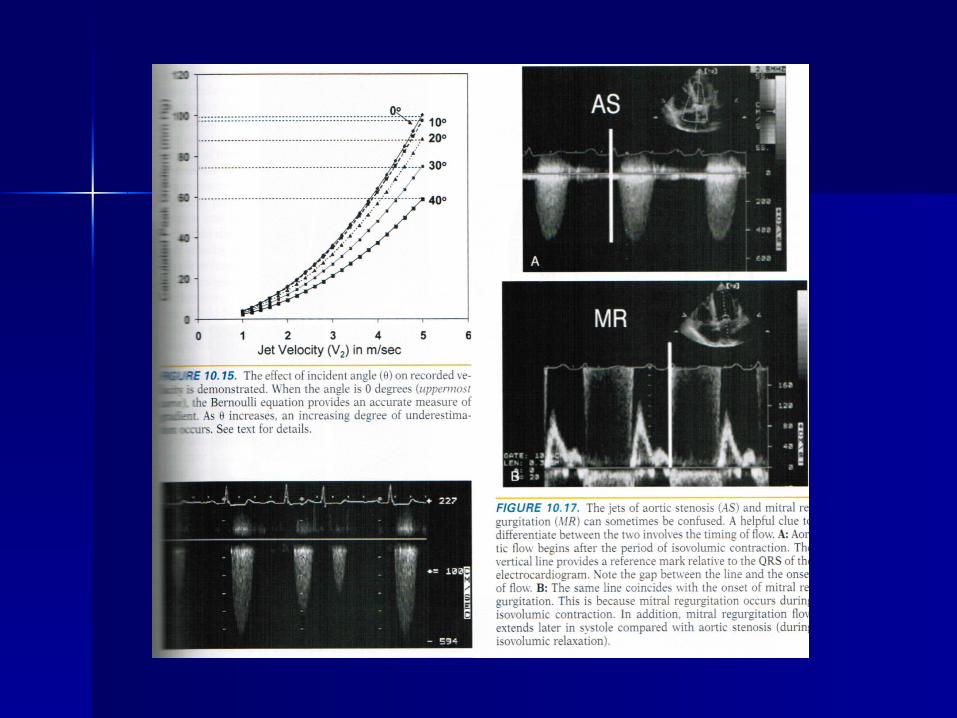
Quality ControlQuality Control
Angle Angle θθ should be as close to zero should be as close to zero degrees as possible, significant errors degrees as possible, significant errors in measurement when greater than 20 in measurement when greater than 20 degreesdegrees
Mistaken identity (MR jet)Mistaken identity (MR jet) Locating highest velocity signalsLocating highest velocity signals Recognize differences in reported data Recognize differences in reported data
(peak instantaneous gradient vs peak-(peak instantaneous gradient vs peak-to-peak gradient)to-peak gradient)
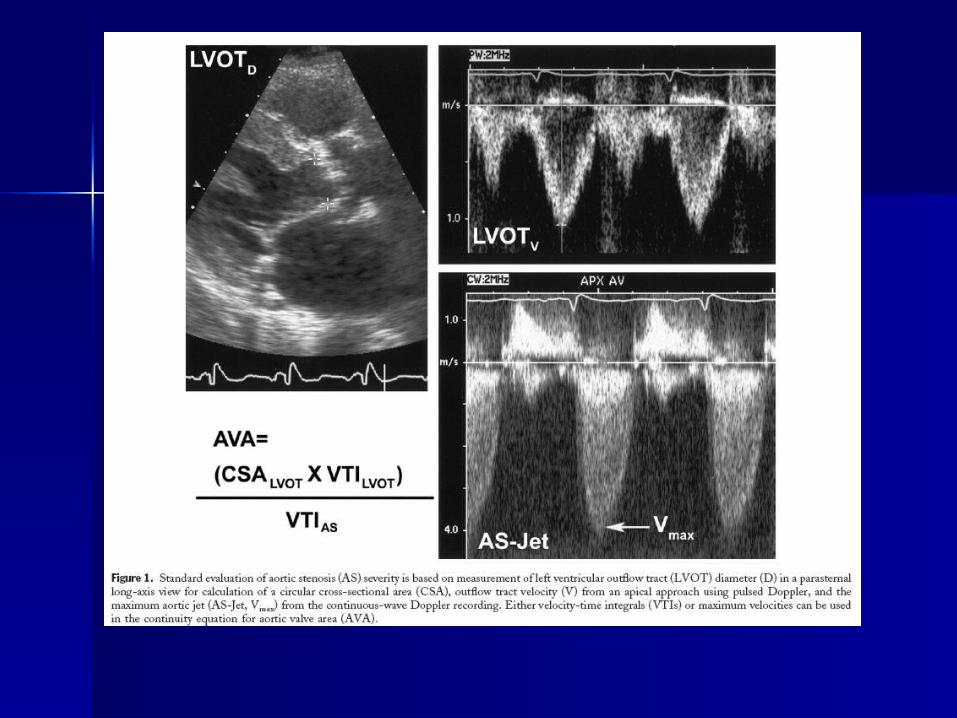
Continuity Equation Continuity Equation Valve AreaValve Area Use principle of continuity of flow to calculate valve area; Use principle of continuity of flow to calculate valve area;
not affected by changes in SV (as when increased in AI and not affected by changes in SV (as when increased in AI and decreased SV with LV dysfunction)decreased SV with LV dysfunction)
LV outflow tract diameterLV outflow tract diameter• Measured on 2D PSLA midsystolic imageMeasured on 2D PSLA midsystolic image• Presume a circular shapePresume a circular shape• Measure diameter (D), one-half of measured is radius (r)Measure diameter (D), one-half of measured is radius (r)• Area = Area = ллr²r²
LVOT VTILVOT VTI• Pulsed Doppler from apical approach, position sample just Pulsed Doppler from apical approach, position sample just
proximal to the stenotic valveproximal to the stenotic valve Aortic jet VTIAortic jet VTI
• Continuous-wave Doppler from the window that yields the Continuous-wave Doppler from the window that yields the highest signalhighest signal
For clinical use, may simplify by substituting maximum For clinical use, may simplify by substituting maximum velocities for velocity-time integrals (Otto)velocities for velocity-time integrals (Otto)
Velocity RatioVelocity Ratio
Define “normal” valve area for the Define “normal” valve area for the individual as the cross-sectional area individual as the cross-sectional area of the outflow tractof the outflow tract
The increase in velocity from outflow The increase in velocity from outflow tract to aortic jet reflects stenosis tract to aortic jet reflects stenosis severity regardless of sizeseverity regardless of size
Actual AVA Actual AVA / “normal” AVA ≈ (V lvot / V Ao) / “normal” AVA ≈ (V lvot / V Ao)
Ratio of 1 indicates little obstruction, Ratio of 1 indicates little obstruction, 0.5 half normal and 0.25 one-fourth 0.5 half normal and 0.25 one-fourth normal value.normal value.
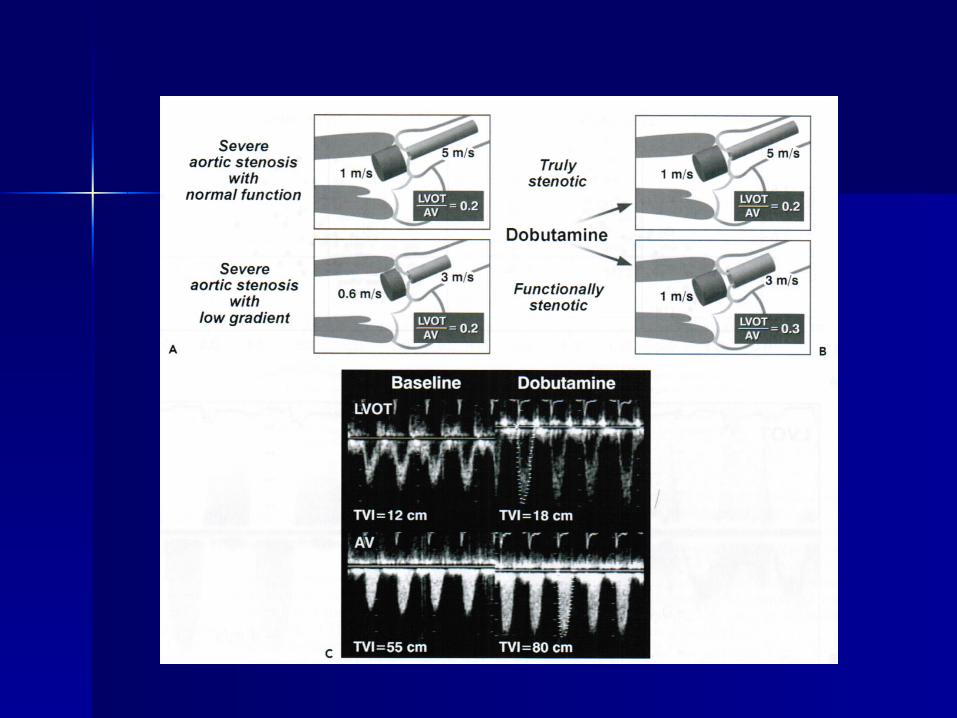
Low gradient with LV Low gradient with LV dysfunctiondysfunction At very low flow rates, valve opening may be inhibited At very low flow rates, valve opening may be inhibited
leading to an underestimation of aortic valve arealeading to an underestimation of aortic valve area May be difficult to distinguish severe AS with low-May be difficult to distinguish severe AS with low-
pressure gradient due to low SV from mild-moderate pressure gradient due to low SV from mild-moderate stenosis with reduced Ao valve opening due to low stenosis with reduced Ao valve opening due to low flow.flow.
Dobutamine echocardiography can help distinguishDobutamine echocardiography can help distinguish• Infuse 5mcg/kg/min in 5 mcg increments every 3 minutes Infuse 5mcg/kg/min in 5 mcg increments every 3 minutes
until LVOT velocity or TVI reaches a normal value (usually until LVOT velocity or TVI reaches a normal value (usually at 15-20 mcg/kg/min)at 15-20 mcg/kg/min)
True severe AS will have a fixed valve areaTrue severe AS will have a fixed valve area Consider severe if valve area < 1cm2 or > 30mmHG Consider severe if valve area < 1cm2 or > 30mmHG
gradient with dobutaminegradient with dobutamine Also used to assess inotropic reserve (increase in SV > Also used to assess inotropic reserve (increase in SV >
20% with dobutamine infusion)20% with dobutamine infusion) Class IIa (B)Class IIa (B)
Natural History of Natural History of ProgressionProgression Aortic jet velocity: 0.3 m per Aortic jet velocity: 0.3 m per
second per yearsecond per year Increase in mean gradient Increase in mean gradient
pressure of 7mmHg per yearpressure of 7mmHg per year Decrease in valve area of 0.1cmDecrease in valve area of 0.1cm² ²
per yearper year
(JACC Vol 48 (3): e1-148.)(JACC Vol 48 (3): e1-148.)

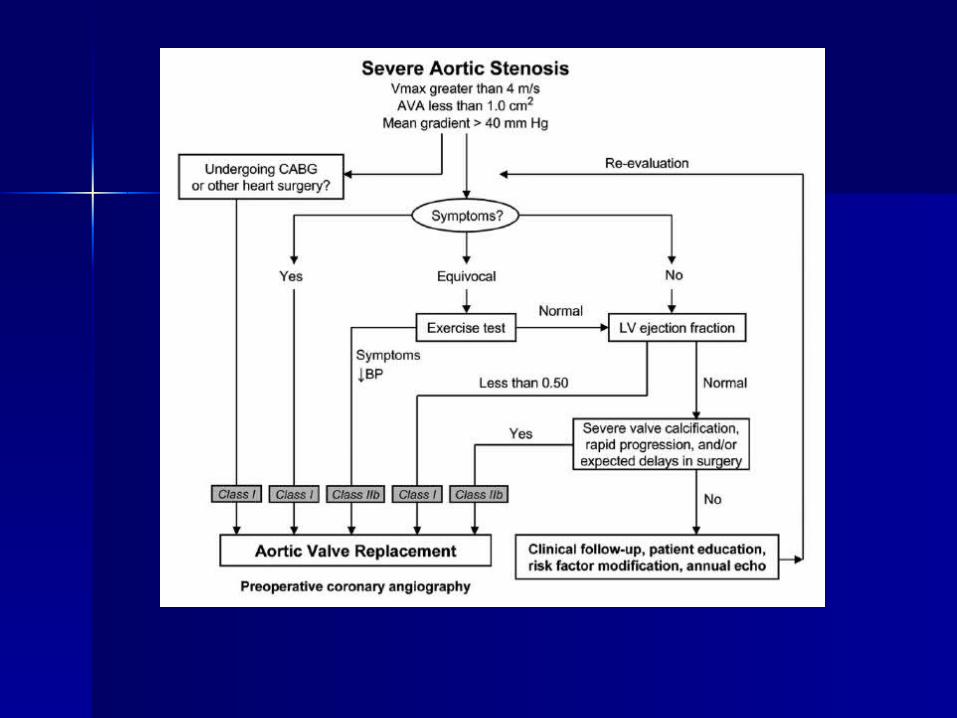
ManagementManagement
Presence of absence of symptomsPresence of absence of symptoms Severity of stenosisSeverity of stenosis Status of the left ventricleStatus of the left ventricle Presence of comorbiditiesPresence of comorbidities
Follow-up ExamsFollow-up Exams
An optimal schedule for repeated medical examinations has not been defined.
An annual history and physical examination on patients with asymptomatic AS of any degree is reasonable.
Annual echocardiogram for severe AS (Class I, LOE: B) An essential component of each visit is patient education
about the expected disease course and symptoms. Because the rate of progression varies considerably,
clinicians often perform an annual echocardiogram every year which may be appropriate.
In patients with moderate AS, serial studies performed every 1 to 2 years are satisfactory. Mild AS, serial studies can be performed every 3 to 5 years (Class I, LOE: B).
Echocardiograms should be performed more frequently if there is a change in signs or symptoms.
Cardiac Cardiac CatheterizationCatheterization Class I
1. Coronary angiography is recommended before AVR in patients with AS at risk for CAD (Level of Evidence: B)
2. Cardiac catheterization for hemodynamic measurements is recommended for assessment of severity of AS in symptomatic patients when noninvasive tests are inconclusive or when there is a discrepancy between noninvasive tests and clinical findings regarding severity of AS. (Level of Evidence: C)
3. Coronary angiography is recommended before AVR in patients with AS for whom a pulmonary autograft (Ross procedure) is contemplated and if the origin of the coronary arteries was not identified by noninvasive technique. (Level of Evidence: C)
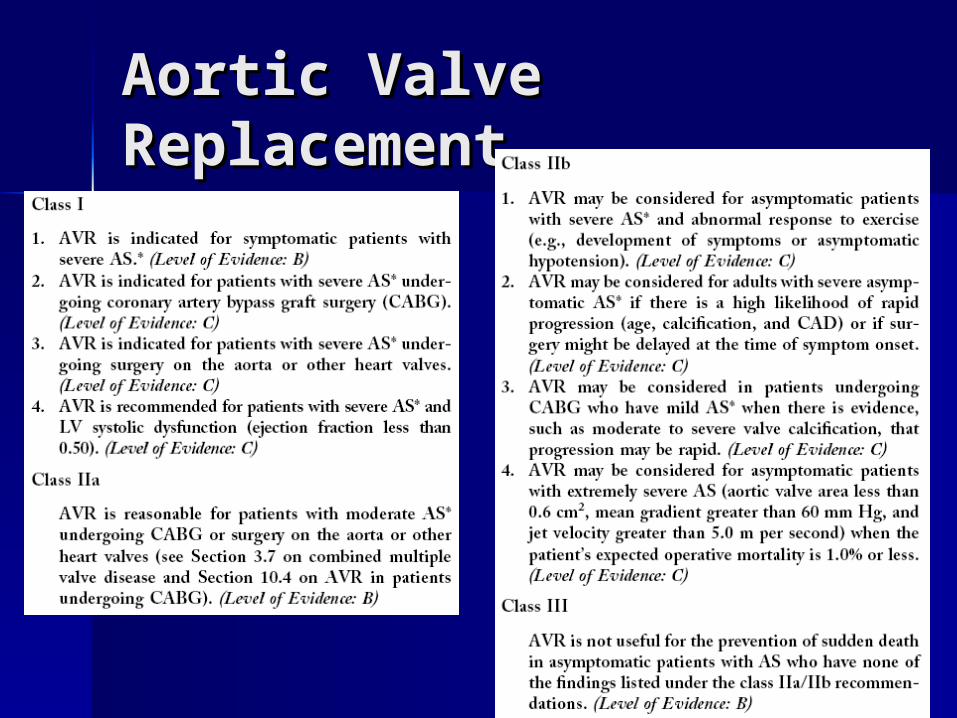
Aortic Valve Aortic Valve ReplacementReplacement
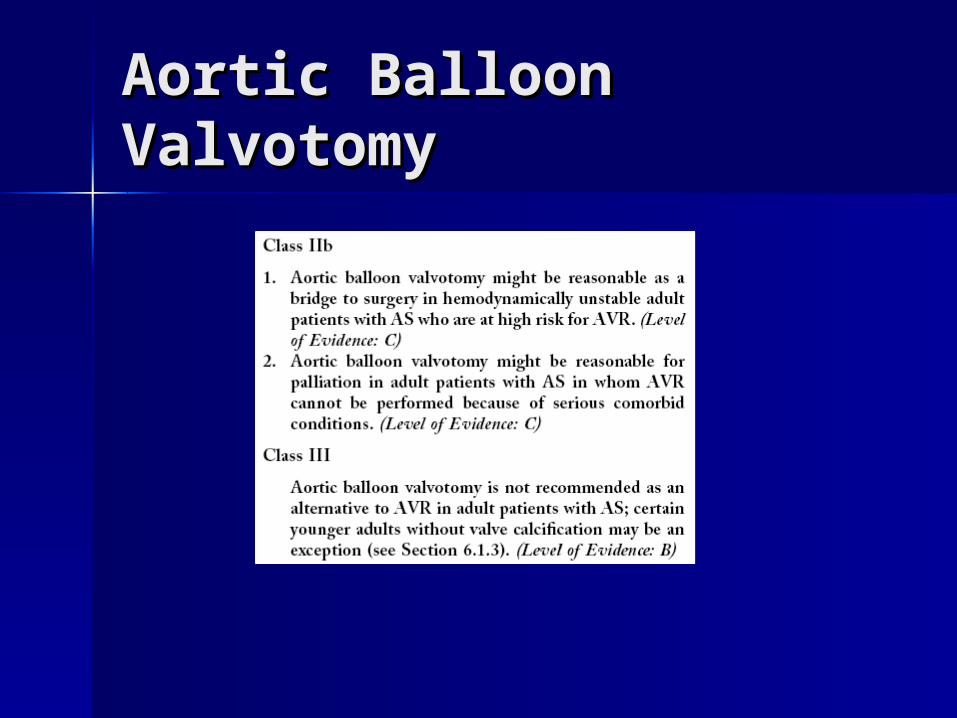
Aortic Balloon Aortic Balloon ValvotomyValvotomy