antimicrobial chemotherapeutic agents
DESCRIPTION
Antimicrobial Chemotherapeutic Agents. Drug Resistance. In the clinical context an organism is said to be resistant: If it is not killed or inhibited by drug concentrations readily attainable in the patient; this usually means blood and tissue concentrations. - PowerPoint PPT PresentationTRANSCRIPT

In the clinical context an organism is said to be resistant:
If it is not killed or inhibited by drug concentrations
readily attainable in the patient; this usually means blood
and tissue concentrations.
However, an organism resistant to these may of course
be sensitive to the higher concentrations attainable in
urine or by topical application.
Even the broadest of broad-spectrum antibacterial drugs
is ineffective against some bacterial genera, against some
species of other genera, and usually against some strains
of species that are in general sensitive to it.
ResistanceResistance
Inherent( non
specific)
Inherent( non
specific)AcquiredAcquired
Certain bacteria are, and as far as we know always have
been, more or less resistant to some antibiotics.
For example, gram-negative bacteria, especially
Ps. aeruginosa, are inherently resistant to a number of
antibiotics that are very effective against gram-positive
bacteria such as penicillin G, erythromycin, lincomycin…….
Inherent )non specific( Resistance
When a bacterial population adapts to the presence of
an antibiotic, sensitive cells are gradually replaced by
resistant cells as in the presence of antibiotic.
Resistant cells continue to grow at the expense of
sensitive cells.
When a new antibiotic is introduced into clinical
practice for the treatment of infections caused by
bacteria that are not inherently resistant to the drug,
the majority of infections respond to the new drug.
Acquired Resistance
But following months or years of continuous use,
resistant strains are reported.
The degree of resistance and the speed with which it
develops varies with:
The organism & The drug.
Generally, the development of acquired bacterial
resistance is common and must be usually expected
with some exceptions.
Streptococcus pyogenes has remained sensitive to
Penicillin G after 40 year's exposure to the drug.
Staph aureus develops slow or multisteps resistance to
penicillin, chloramphenicol and tetracycline.
While Mycobacterium tuberculosis and various
organisms develops sudden or one step resistance to
Streptomycin.
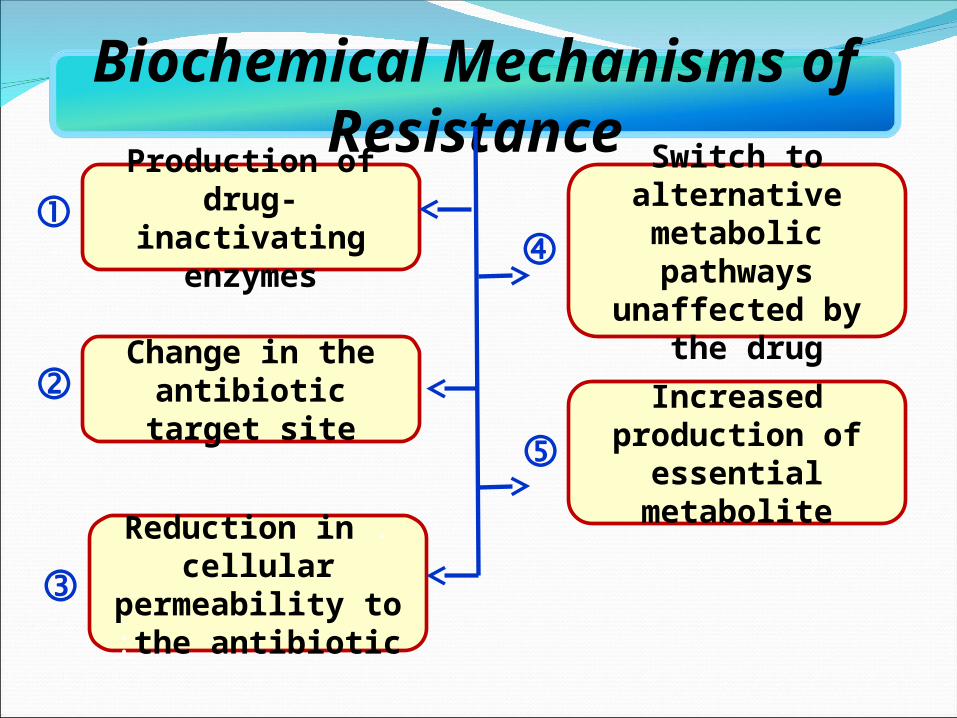
Biochemical Mechanisms of
ResistanceProduction of drug-
inactivating enzymes
Change in the antibiotic target site
.Reduction in cellular permeability to the
antibiotic:
Switch to alternative metabolic pathways
unaffected by the drug:
Increased production of essential metabolite
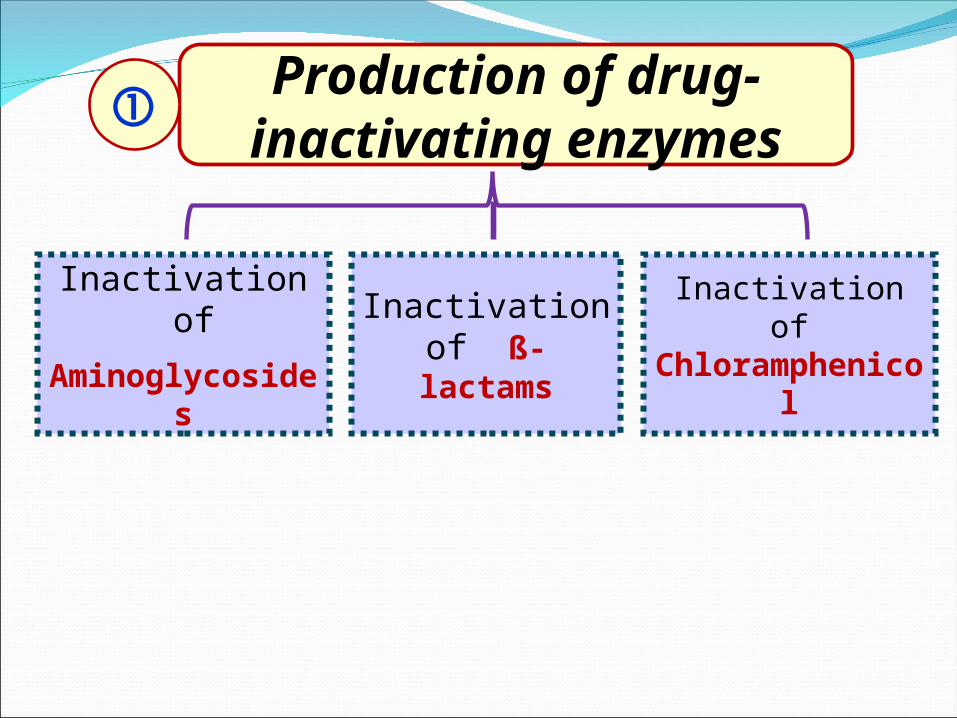
Production of drug-inactivating enzymes
Inactivation of
Aminoglycosides
Inactivation of ß-lactams
Inactivation of Chloramphenicol
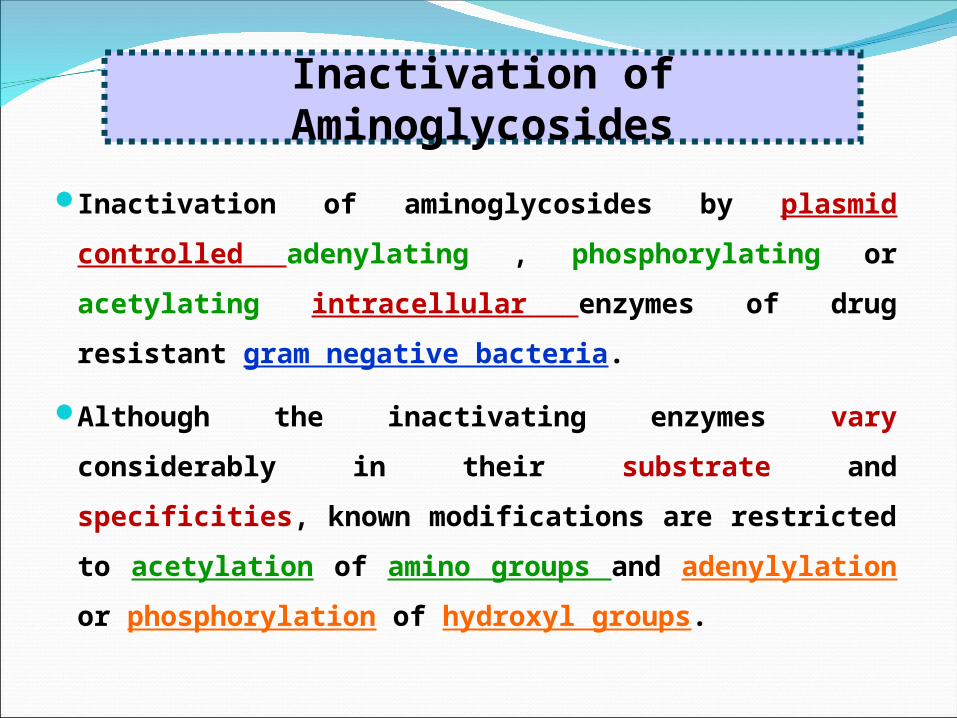
Inactivation of aminoglycosides by plasmid controlled
adenylating , phosphorylating or acetylating intracellular
enzymes of drug resistant gram negative bacteria.
Although the inactivating enzymes vary considerably in
their substrate and specificities, known modifications are
restricted to acetylation of amino groups and
adenylylation or phosphorylation of hydroxyl groups.
Inactivation of Aminoglycosides
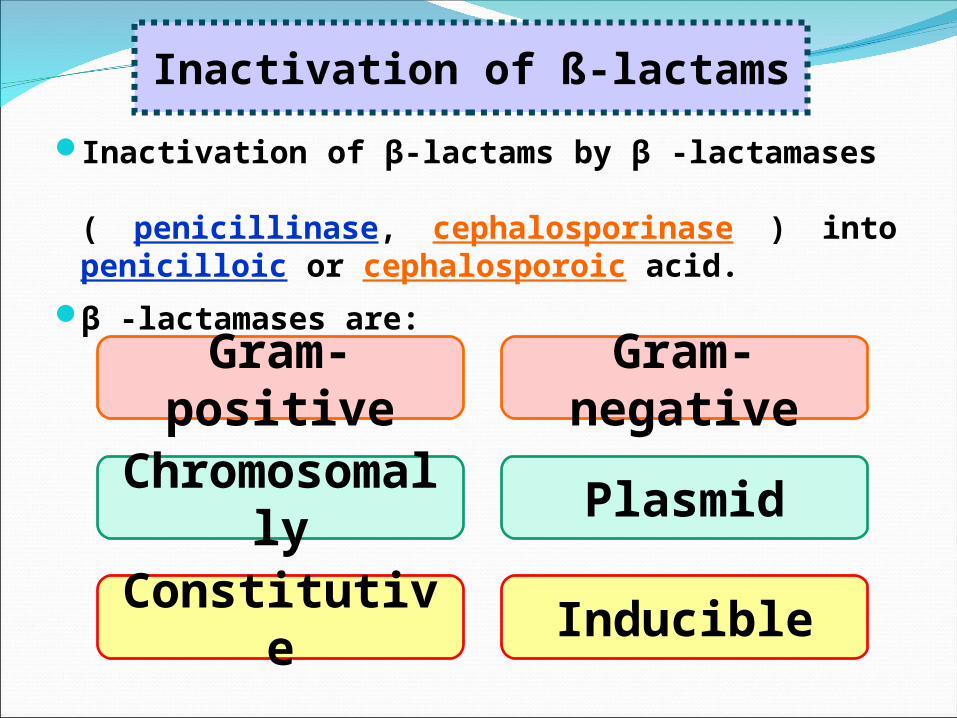
Inactivation of β-lactams by β -lactamases ( penicillinase, cephalosporinase ) into penicilloic or cephalosporoic acid.
β -lactamases are:
Inactivation of ß-lactams
Gram-positive Gram-negative
Chromosomally Plasmid
Constitutive Inducible
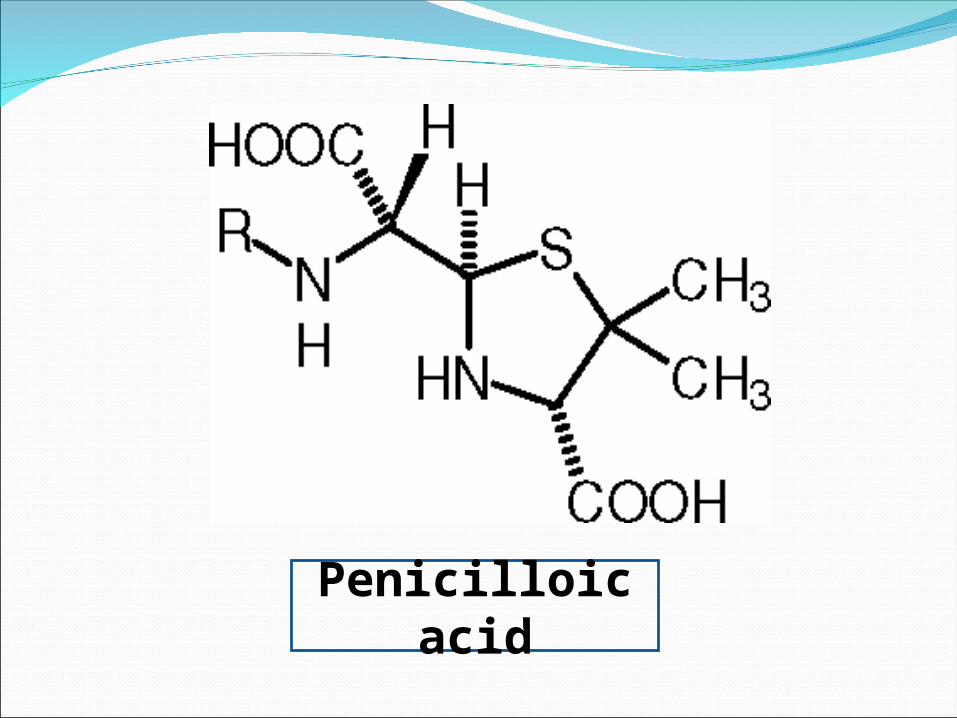
Penicilloic acid
The synthesis of gram positive β-lactamase is induced by
the antibiotic themselves and is released extracellularly
and destroy antibiotic in the external environment.
Most strains of gram-negative cells, by contrast,
synthesize β-lactamases constitutively. i.e. continuously
and are not released into the external environment (cell-
bound or intracellular).
Chromosomally-mediaied β-lactamases of gram negative
hydrolyze cephalosporins more rapidly than penicillins and
are inhibited by cloxacillin but not by clavulanic acid.
However, those of Aeromonas spp. and
Klebsiella spp. are more active against
penicillins and not inhibited by cloxacillin.
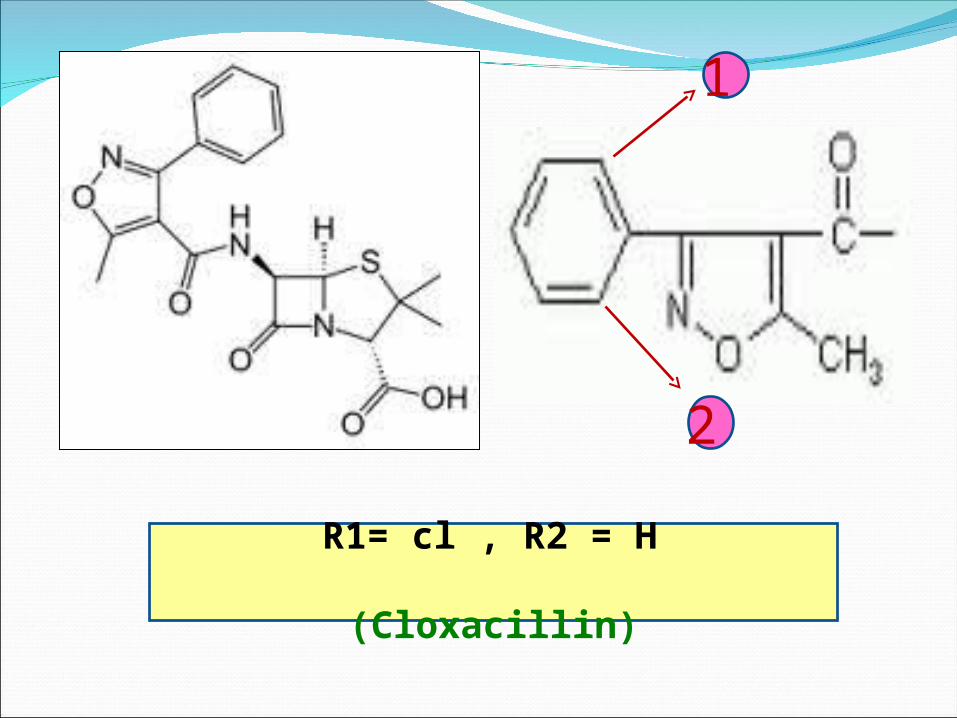
1
2
R1= cl , R2 = H (Cloxacillin)
Inducible types are found in microorganisms such as
Pseudomonas spp., Proteus and other gram
negative bacteria but infrequently in E. coli in which, as
many enterobacter species, constitutive types could be
isolated.
Different types of plasmid-mediated β-lactamases were
isolated.
TEM type enzymes are present in almost all gram
negative bacteria.
These enzymes were first isolated from E. coli strains
isolated, in Athens, from a young girl called Temoniera
and was referred to as TEM enzyme.
Electrophoretically different type was then isolated
from Pseudomonas aeruginosa (TEM-2).
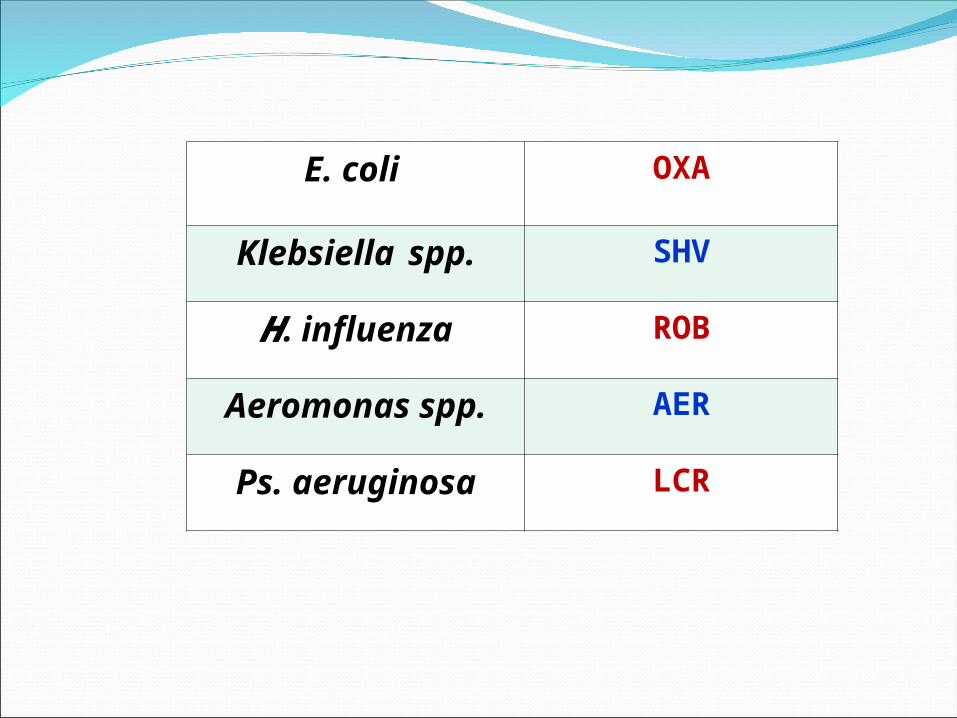
OXAE. coli
SHVKlebsiella spp.
ROBH. influenza
AERAeromonas spp.
LCRPs. aeruginosa
Inactivation of chloramphenicol by chloramphenicol
acetyl transferase (CAT).
Usually they are a plasmid-mediated enzymes which are
inducible type in gram-positive bacteria but constitutive
in gram-negative bacteria.
These enzymes acetylates the OH groups in the side chain
of the drug.
Inactivation of chloramphenicol
Replacement of the terminal - OH group of this side
chain, which is normally the first to be acetylated by an
inert fluorine atom, yields a chloramphenicol derivative
that is not susceptible to attack by CAT.
Change in the antibiotic target site
Chromosomal
Resistance to
Aminoglycosides
Resistance to
Erythromycin
Resistance- to some
Penicillins
Resistance to
Sulfonamides &
Trimethoprim
It is associated with the loss or alteration of a specific
protein in the 30S subunit of the bacterial ribosome that
serve as a binding site in the susceptible organisms.
Chromosomal Resistance to Aminoglycosides
Resistance to Erythromycin
It is associated with alteration, of its receptor on the
5OS subunit of the ribosome.
Resistance- to some penicillins due to loss or alteration
of Penicillin Binding Proteins (PBPs).
Resistance- to some Penicillins
Resistance to Sulfonamides & Trimethoprim
Occurs by alteration of the tetrahydropteroat
synthetase and tetrahydrofolate reductase,
respectively, that have a much higher affinity for
PABA than these drugs.
Bacterial cells altering the permeability of their cell
membrane making it difficult for antimicrobials to enter.
This type of resistance is found in bacteria resistant to:a. Polymyxins.b. Tetracyclines.c. Amikacin & some aminoglycosides.Streptococci have a natural permeability barrier to
aminoglycosides. This can be partly overcome by combination with cell wall
active drug, e.g. (penicillin).
Reduction in cellular permeability to the
antibiotic
The organism develop an altered metabolic pathway
that bypasses the reaction inhibited by the drug
e.g. some sulfonamide-resistant bacteria do not
require extra-cellular PABA but, like mammalian cells,
can utilize preformed folic acid.
Switch to alternative metabolic pathways unaffected by the
drug:
That is competitively antagonized by the drug in
sensitive cells e.g. resistance to sulfonamides may be
associated with high level of bacterial synthesis of
PABA.
Increased production of essential metabolite
:
The origin of drug resistance
Non Genetic Origin
Genetic Origin
This involves metabolically inactive cells or loss of target sites.
a.Most antimicrobial agents act effectively only on replicating cells.
• Mycobacteria survive for many years in tissue yet are restrained by the host's defenses and do not multiply.
• Such persisting organisms are resistant to treatment and cannot be eradicated by drugs.
• When they start to multiply they are fully susceptible to the drugs.
Non Genetic Origin
b. Loss of a particular target structure, often induced by
the drug, may result in antimicrobial resistance.
• Exposure of some gram-positive bacteria to penicillin
results in the formation of cell lacking cell wall
(i.e. L-forms).
• These cells then are penicillin resistant, having lost the
structural target site of the drug.
• When these organisms revert to their bacterial parent
forms resuming cell wall production, they are again
fully susceptible to penicillin.
Most drug-resistant microbes emerge as a result of genetic change and subsequent selection processes by antimicrobial drugs.
Genetic Origin
The mechanisms by which geneticchange occur are:
Chromosomal
Resistance
Extra Chromosom
al Resistance
This develops as a result of mutation in a gene locus
that controls susceptibility to a given antimicrobial drug.
The presence of the drug serves as a selecting
mechanism to suppress susceptible organisms and favor
the growth of drug resistant mutant.
Spontaneous mutation occurs at a frequency of 10 7 to
10 12.
Chromosomal Resistance
Chromosomal mutants are most commonly resistant by
virtue of a change in a structural receptor for a drug as
in bacterial resistance to erythromycin, lincomycin,
aminoglycosides and others by alteration of their target
site in susceptible cells.
Prevention of the emergence of resistant mutants is one
of the main indications for the clinical use of
combinations of drugs.
But provided that the mechanisms of action of the two
drugs are unrelated.
Therefore if both drugs are given in adequate dosage,
the risk of the emergence of a resistant strain is very
much less than if either is used alone.
Extra Chromosomal Resistance
Plasmids
Transposons
Bacteria often contain extra chromosomal DNA units
known as plasmids.
Some of which alternate between being free and being
integrated into the chromosome.
R factors are a class of plasmids that carry genes for
resistance to one and often several antimicrobial drugs
and heavy metals.
Plasmids
Plasmid genes for antimicrobial resistance often control
the formation of enzymes that inactivate the
antimicrobial drugs such as β-lactamases, CAT and
enzymes that inactivates aminoglycosides; or enzymes
that determine the active transport of tetracyclines
across the cell membrane, and for others.
The drug resistance (R) genes are often part of highly
mobile short DNA sequences known as transposons
(Transposable elements or jumping genes) that is able
to move, from one position to another, between one
plasmid and another or between a plasmid and
a portion of the bacterial chromosome within a
bacterial cell.
Transposons
Thus, transposons are able to insert themselves into
many different genomic sites with no homology with
them.
Simple transposons (IS) only carry information
concerned with the insertion function.
Simple transposons (IS) (i.e. insertion sequences) have
no known effects beyond transposition and
inactivation of the gene (or operon) into which they may
insert.
Complex or composite transposons (Tn) contain
additional genetic material unrelated to transposition,
such as drug-resistance genes.
Such as penicillin, kanamycin, streptomycin,
sulfonamides, tetracyclines, chloramphenicol ,and
trimethoprim.
Mechanisms of Transmission of Genetic Material and Plasmids
Transduction
Transformation
Conjugation
Transposition
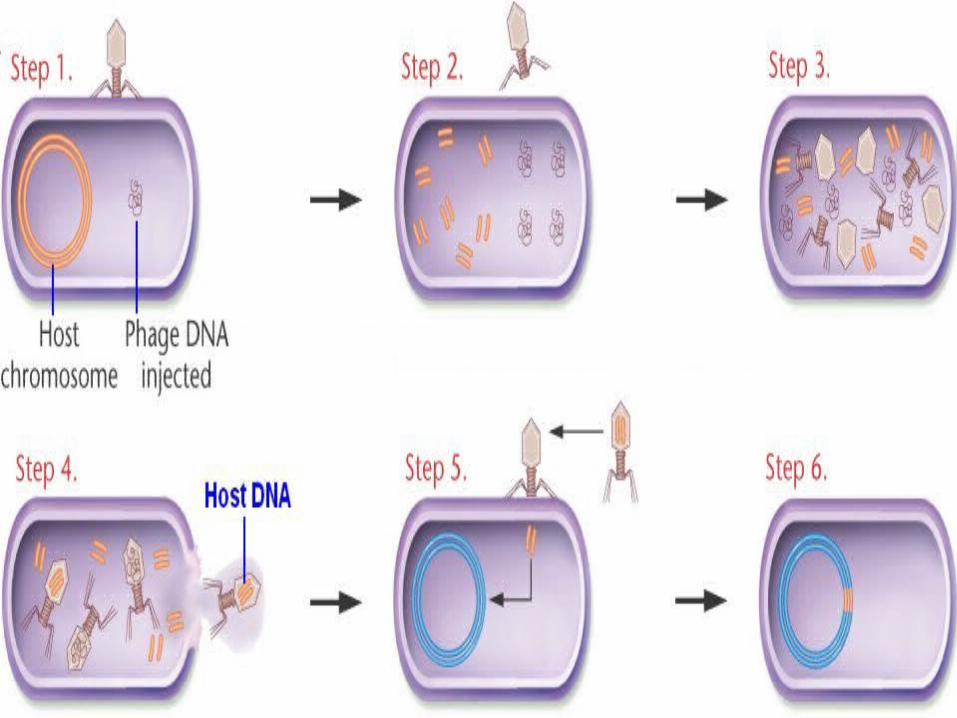
This is the main mechanism for transmission of antibiotic
resistance between gram-positive cocci, and occurs in
other bacterial groups.
Plasmid DNA is enclosed in a bacteriophage and
transferred by the virus to another bacterium of the same
species e.g. the plasmid carrying the gene for β-lactamase
production can be transferred from a penicillin-resistant
to a susceptible staphylococcus if carried by a suitable
bacteriophage.
Transduction
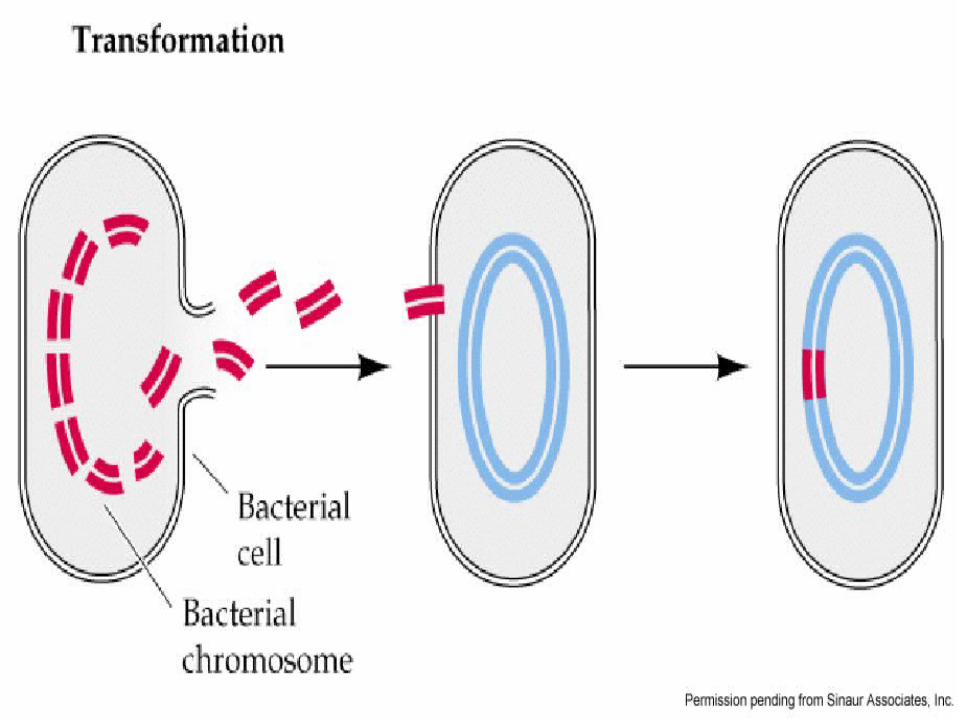
Naked DNA passes from one cell of a species to another
cell, thus altering its genotype.
This can occur through laboratory manipulation and
perhaps spontaneously.
Transformation
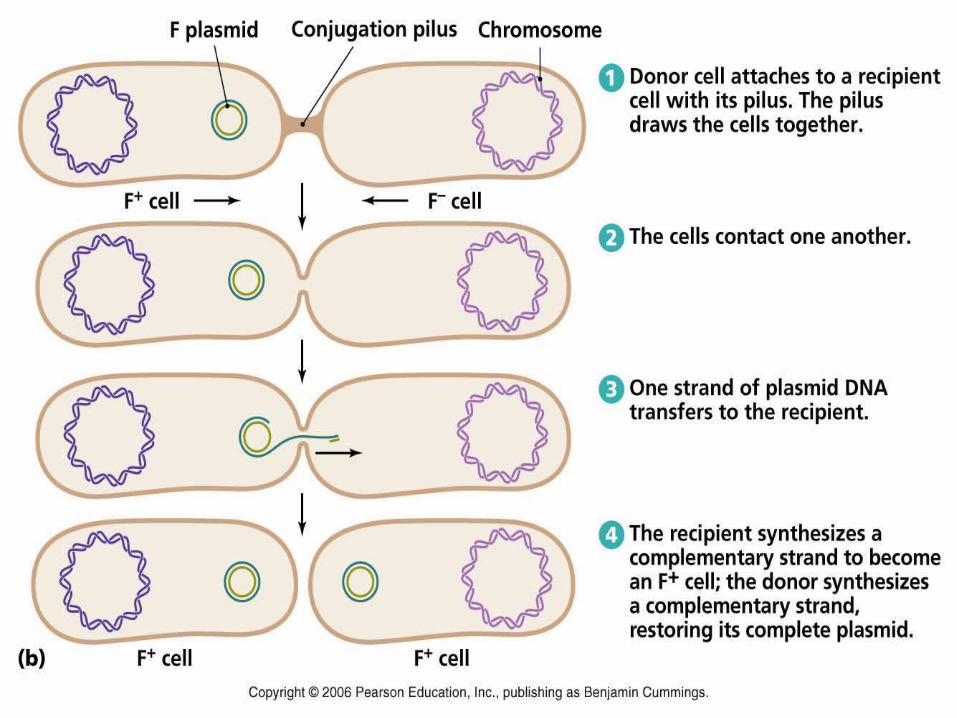
Conjugation
This is the commonest method by which, multi-drug
resistance spreads among different genera of
gram-negative bacteria.
But also occurs among some gram-positive cocci.
The usual plasmid found in resistant gram-negative
bacteria consists of two distinct but frequently linked
elements:
a. One or more linked genes each conferring resistance to
a specific antibacterial drug
(resistance determinants).
b. A resistance transfer factor (RTF) that enable the cell to
conjugate with a sensitive bacterium and to transfer to
It a copy of the entire plasmid.
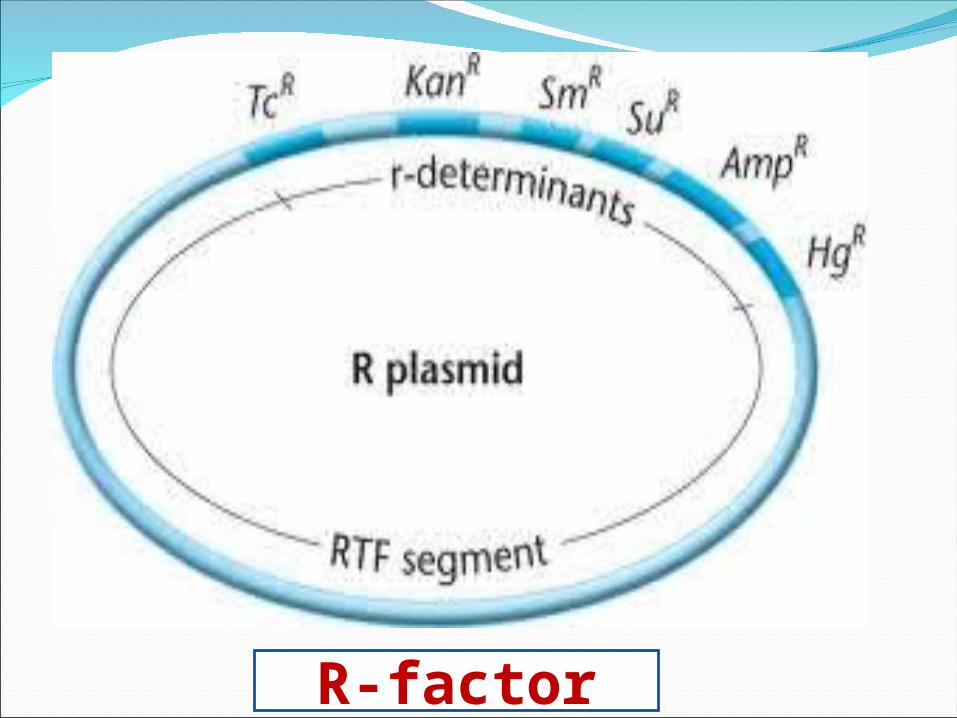
R-factor
The entire linked complex of RTF and resistance
determinants is known as R-factor and takes the form of
a double stranded circular molecule of DNA.
A proportion of R-factor-bearing cells (R* cells) possess
hair-like structures that extend out from the bacterial
surface known as pili.
The pili, whose synthesis is under the control of the
RTF component of the R-factor are essential to the
conjugation phenomenon with R' bacteria and the
transfer of an R- factor.
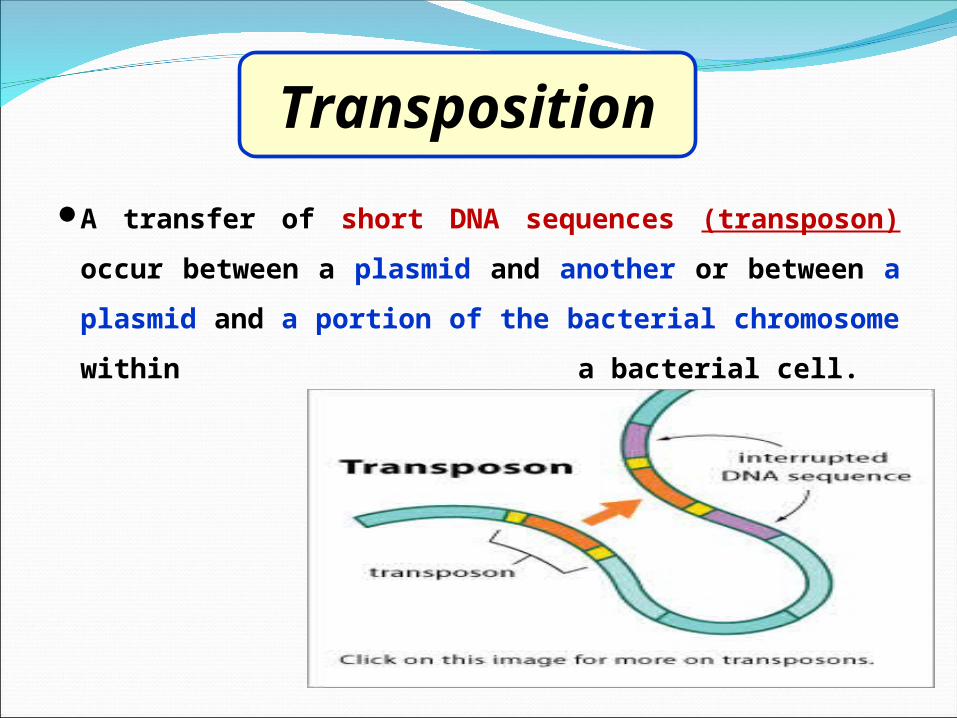
A transfer of short DNA sequences (transposon) occur
between a plasmid and another or between a plasmid
and a portion of the bacterial chromosome within
a bacterial cell.
Transposition
Transferable or infective drug resistance is important for the following reasons
i. The transferable plasmids commonly determine resistance to several unrelated drugs.
ii. Such plasmids are transferable not merely to related strains of the same species but to strains of other species and genera; for example, antibiotic-resistant but harmless organism in human or animal intestine (E. coli) can confer antibiotic resistance, by plasmid transfer, on pathogenic but previously antibiotic-sensitive bacteria of other genera which the host happens to ingest (such as typhoid or dysentery bacilli).
iii. It is possible for multiple-resistant enterobacteria to
develop in farm animals and be transmitted to man.
Development of this resistance is due to the
widespread use of antibiotics especially cheap
types, as food supplements for young animal to
accelerate their growth by partial suppression of
their intestinal flora.
a.Specific resistance: When the organism acquire
resistance to a certain drug but Its susceptibility to other
drugs is unaffected.
b. Cross resistance: Microorganisms resistant to a certain
drug may also be resistant to other drugs that share
a mechanism of action.
Specific and Cross Resistance
Such relationship exist mainly between agents that are
closely related
Polymyxin B and Polymyxin E.
Erythromycin and Oleandomycin.
Neomycin and kanamycin.
However, it may also exist between unrelated
chemicals Erythromycin-Lincomycin.
When the active nucleus of the chemicals is so similar,
extensive cross-resistance is to be expected e.g.
resistance to one of the tetracyclines imparts resistance
to the other members of the group e.g. resistance to
one sulfonamide cause resistance to hundreds of other
sulfonamides.
Abuse of antibiotics, is avoided for many reasons
including the following:
a.To prevent the emergence of antibiotic resistance.
b.To reduce the cost of antibiotic use.
c. To prevent antibiotic toxicity.
Antibiotic Policies
Unless there is a valid reason for giving an antibiotic, the patient would probably be better off without it.
General Principles of Optimal Antibacterial
Therapy 1
Treatment of Known or Suspected Infection
Prevention of Bacterial Infection
Peri-operative Prophylaxis
Patients at Special Risk
In cases when immediate drug treatment is necessary.2It is bad treatment to use broad-spectrum antibiotics when an infective condition can be treated with a more specific agent.
3
It is essential to use bactericidal and not bacteriostatic therapy.4
It is essential to use combination of antimicrobial drugs in certain situations.5
For treatment of superficial infections it is important to use either antiseptic or antibiotics which are rarely or never used systemically.
6Give enough, for long enough, and then stop treatment with the antibiotic.7To reduce the spread of microbial resistance, avoid the use of antibiotics as food supplement for animals or for preservation of human food stuffs, avoid liberation of antibiotic powders and solutions into the environment.
8
To reduce the emergence of antibiotic-resistant strains, an antibiotic policy has to be introduced for a hospital or area e.g., using antibiotics in rotation, keeping a particular antibiotics and permitting their use only on rare and special occasions, or insisting on combined therapy.
9
1. To provide broad coverage.
2. For initial (blind) therapy when the patient is seriously ill
and results of cultures are pending.
3. To provide synergism when organisms are not effectively
eradicated with a single agent alone e.g., in enterococcal
endocarditis both penicillin and an
aminoglycoside are given because their combined effect
is greater than the sum of their independent activities.
Drug combination
4. To prevent emergence of resistance, as in the treatment of
tuberculosis. Inappropriate use of combinations could result in: Antagonism it occurs when a bactericidal agent is used with a
bacteriostatic one as in penicillins plus tetracycline or
Chloramphenicol.
Sulphonamides do not antagonize penicillins, possibly because their
bacteriostatic action is too low. An increase in the number or severity of adverse reactions. Increased coast.