antimicrobial activity of garlic, tea tree oil, and chlorhexidine against oral microorganisms
TRANSCRIPT
International Dental Journal (2002) 52. 433-437
Antimicrobial activity of garlic, tea tree oil, and chlorhexidine against oral microorganisms F.C. Groppo, J.C. Ramacciato, R.P. Sim6es, F.M. Florio and A. Sartoratto Sao Paulo, Brazil
Objective: To compare the antimicrobial activity of tea tree oil, garlic, and chlorhexidine solutions against oral microorganisms. Method: The five- week study consisted of thirty subjects. The first week was considered baseline. All subjects used a control solution (second week), and were randomly divided into the three groups (third week): G1- 0.12% chlorhexidine; G2 - 2.5% garlic (Allium sativum, L.); and G3 - 0.2% tea tree oil (Melaleuca alternifolia). Dishes containing blood agar and Mitis Salivarius Bacitracin agar (MSB) were inoculated with the subjects' saliva (collected twice a week). Total microorganisms and mutans streptococci were counted in blood agar and MSB, respectively. Results: Chlorhexidine and garlic groups showed antimicrobial activity against mutans streptococci, but not against other oral microorganisms. The tea tree oil group showed antimicro- bial activity against mutans streptococci and other oral microorganisms. Maintenance of reduced levels of microorganisms was observed only for garlic and tea tree oil during the two consecutive weeks (fourth and fifth). Unpleasant taste (chlorhexidine 40%, tea tree oil 30%, garlic loo%), burning sensation (chlorhexidine 40%, tea tree oil 6O%, garlic 1 OO%), bad breath (chlorhexidine 40%, tea tree oil 20%, garlic 90%), and nausea (chlorhexidine O%, tea tree oil lo%, garlic 30%) were reported. Conclusion: Garlic and tea tree oil might be an alternative to chlorhexidine.
Key words: Antimicrobial activityl garlic, tea tree oill chlorhexidine, oral microorganisms, mutans streptococci
Correspondence to: Dr. Francisco Carlos Groppo, Piracicaba Dental School - UNICAMP, Av. Limeira 901, Bairro Areiao. Piracicaba, Sao Paulo, Brazil CEP 13 414 - 900. E-mail: [email protected]
Dental disease prevention is asso- ciated with a reduction in the number of oral microorganisms'. The number of colonised oral sites is directly related to salivary strep- tococci counts'.
Mouthwash, after or before tooth brushing, is considered an adjunct to oral hygiene and to improve efficacy, antimicrobial agents have been added to mouth- washes and dentifrices3. Chlorhexi- dine is one of the safest and most efficient antimicrobial The minimum effective concentration (MIC) of chlorhexidine is 0.1 2 per cent. Lower concentrations are unable to reduce salivary mutans streptococciG. Dental staining is the most important adverse effect of chlorhexidine', although unpleasant taste, taste alteration, and mucosal erosion are other related adverse effects', all of which motivated the development of other antimicro- bial agents.
Garlic (Allium satiwm L.) is used in folk medicine for the treatment of many diseases'. It consists of various biologically active metabo- lites like alliin, alliinase, allicin, S-allycystein, diallylsulphide, and allymethyltrisulphide. Bacterial growth inhibition and bactericidal activity are attributed to allicin and t iosulph~nates~*'~. There are few reports on garlic antimicrobial activity against oral microorganisms, although 25 Der cent garlic extract
v " 0 2002 FDI/World Dental Press 0020-653gmm43345

434
showed good antimicrobial activ- ity against human oral microbiota' ' .
Tea tree oil is extracted from Mehknca a/tem$h'a leaves (Myrtaceae family). High quality oil must contain 2-5 per cent of cineole and 40-47 per cent of terpinen-4-01. Cineole is a skin-irritating substance and terpinen-4-01 is presumed to be the most important antimicro- bial agent of the tea tree oil". This oil is effective against a high number of gram-positive and gram-nega- tive bacteria, as well as fungi. Minimal inhibitory concentrations P I C ) against common pathogens range from 0.5 to 1 per cent13. MIC against mutans streptococci is lower than 0.0125 per cent, and MIC against ora/h-group s trep to- cocci is lower than 0.05 per cent14.
The aim of this study was to observe the effect and adverse effects of mouthwashes with 2.5 per cent garlic, 0.2 per cent tea tree oil and 0.12 per cent chlorhexidine on oral microorganisms.
Materials and methods
The Ethical Committee of the Dental School of Piracicaba approved this study (protocol # 35/99) in which healthy subjects (14 men and 16 women), 18-35 years of age, having all their teeth except their third molars and presenting no allergies, were selected. The subjects had not used any microbial agent for the two weeks before the study was begun. All subjects formally agreed on all study aspects. Sodium fluoride dentifrice ("andy@ - Kolynos, 1100ppmF) was used for all groups as the standard dentifrice.
Saliva samples were collected using a previously described tech- nique*. Subjects deposited saliva samples directly in sterilised eppendorf tubes by means of steri- lised straws in order to avoid labial contamination. Each sample was immediately sonicated (Vibra Cell 400W, Sonics & Materials Inc - 5 per cent amplitude, 9.9 seconds cycle, 6 pulses) and diluted in saline
solution (100 and 1000 times). The diluted samples (5 pL) were spread on small Petri dishes (5x2 cm) containing blood agar (Difco Co) (agar base + 5 per cent sheep blood) and MSB (Difco Co - Mitis Salivarius agar, bacitracin 200 U/L, 15 per cent sucrose, and 1 per cent potassium tellurite). The dishes were placed in an incubator (Jovan IG 150) with 10 per cent of CO, at 37OC, for 48 hours. Subse- quently, the dishes with blood agar were placed in an aerobic incuba- tor at 37OC, for 24 hours. Counts for the total oral microorganisms were performed in blood agar dishes and for the mutans strepto- cocci in MSB dishes.
The subjects did not receive any treatment or standard dentifrice during the first week. Saliva samples were collected in the morning of the third and sixth days. Counts of both oral microorgan- isms and mutans streptococci were considered as baseline.
In the second week, all subjects were submitted to one-minute mouthwashes - carried out thirty minutes after the last tooth brush- ing of the dayi5 - using lOmL of vehicle solution (distilled water, 5 per cent spearmint essence, and 2 per cent sorbitol) and standard dentifrice. Saliva samples were collected in the morning of the third and sixth days. These samples were used to quantify the oral microorganisms and mutans strep- tococci (control group mean).
In the third week, the subjects were randomised by a draw into three groups, and submitted to one-minute7s mouthwashes for 7 days using 1OmL of one of the following solutions:
2.5 per cent garlic solution: white garlic (Brazil, South America) bulbs were obtained in a local supermarket and the dry peel removed. Only perfect bulbs were used. Aqueous garlic extract was prepared by using 100g of fresh rootless bulbs and 1 OOmL of distilled water, all of which were processed in a
blender for 10 min. The result- ing extract was filtered with a paper filter and sterilised through a 0.2p.m membrane filter by using a vacuum pump. All solid and liquid residues were weighed and the concentration of the final solution was 25 per cent (w/v) or 250 mg/mL""'. It was diluted to 2.5 per cent using a vehicle solution. 0.2 per cent tea tree oil solution: 100 per cent pure oil (Imported from Australia by Galena Phar- macy Ltd) was analysed through gas chromatography (Kovatz 1M gas chromatograph, tempera- ture of 240°C, Helium gas at a flow of lmL/min, DB1 column, and NIST98 compound library). Oil was diluted to 0.2 per cent using a vehicle solution and 0.5 per cent Tween 80. 0.12 per cent chlorhexidine solution: chlorhexidine gluconate (Galena Pharmacy Ltd) 20 per cent were diluted to 0.12 per cent using a vehicle solution. All mouthwashes were carried
out thuty minutes after the last tooth brushing of the day. Saliva samples were collected in the morning of the third and sixth days. These samples were used to quantify the oral microorganisms and mutans streptococci (mouthwash groups mean).
In the two consecutive weeks the treatment was discontinued. Saliva samples were collected once a week to determine oral microor- ganisms and mutans streptococci counts (4" week and 5" week mean counts) to observe the regrowth or antimicrobial residual effects upon microbiota.
Each sample-collecting day, all subjects were questioned about solution taste, breath alteration, burning sensation, tooth colour alteration, and systemic adverse effects during the experimental period. An analytical scale (1 Ocm) was used to determine these parameters. Subjects marked the scale with an 'x' and the length was measured. All reports were inter-
International Dental Journal (2002) Vol. 52INo.6
435
10
- 0 -mutans (XI$) *total (XI&)
preted by using the following clas- sifications: 0 cm - None; 0 cm 2.5 cm < x = 5.5 cm - Moderate; 5.5 cm < x = 8.5 cm - Serious; 8.5 cm < x = 10 cm - Severe.
Results of this interpretation were analysed by using Kruskal- Wallis test (5 per cent of significance level) by using computer software (Bioestat 1 .O for Windows). Also, all oral microorganisms and mutans streptococci counts observed were statistically analysed by the same test (5 per cent of significance level).
< x = 2.5 cm - Low;
basal control mouthwash 4th week 5th week
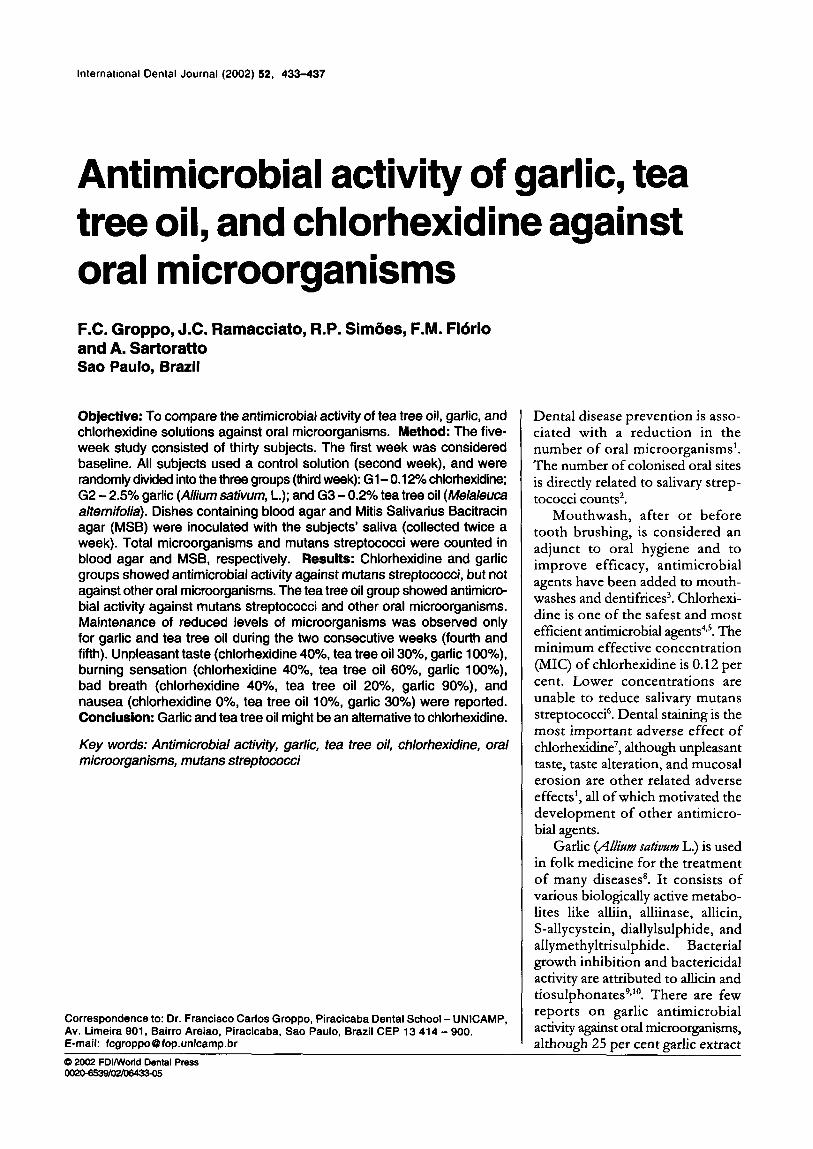
305.5 269.9 81.4 151 248.7
766.5 655.3 456.5 504.2 444.4
Results The chromatographic analyses of tea tree oil indicated high quality oil. Probable concentrations were found to be 3 per cent for cineole and 50 per cent for terpinen-4-01.
Figure 1 shows the oral micro- organism and mutans streptococci means (cfu/mL k sem) for the chlorhexidine group. No statistically significant differences (D0.05) among all groups were observed in relation to oral microorganisms. However, the mouthwash group was statistically different (W0.05) from the other groups (except 4th week) regardtng mutans streptococci.
Figure 2 shows the oral micro- organism and mutans streptococci means for the garlic group. Base- line, control, and mouthwash groups regarding oral microorganisms showed no statistically significant differences (D0.05). Although both 4* week and 5th week groups showed no statistically significant differences (P>0.05), they were significantly different (P<0.05) from the baseline, control, and mouthwash groups. No statistically significant differences (B0.05) were found between the baseline and control groups regarding mutans strepto- cocci. However, these groups (base- line and control) were significantly different (P<0.05) from the mouth- wash, 4* week, and 5"' week groups.
Figure 3 shows the oral micro- organism and mutans streptococci means for the tea tree oil group.
basal control mouthwash
w I r I
4th week 5th week
- 0 -mutans(xI$) *total (XI&)
Figurn 7. Means of microorganism counts (total number of microorganisms and mutans streptococci) for the chlorhexidine group.
305.2 259.8 78.8 65.9 105.2
5 14 464.8 359.5 93.3 185.6 ,
- 0 -mutans(xI$) 146.8 141.8 43.2 40 32.7 L*total (xlO6) 504.6 477.5 221.9 72.5 94
Figurn 2. Means of m'icroorganism counts (total number of microorganisms and mutans streptococci) for the garlic group.
10 basal 1 control I mouthwash I 4th week I 5th week
I I I I I I I
No statistically significant differences (P>0.05) were found between basal and control groups regarding oral microorganisms and mutans streptococci. Mouthwash, 4"' week, and 5'h week groups showed no statistically significant differences (D0 .05) . However, these groups were statistically different (P<0.05)
from the baseline and control groups. Solution taste, breath, burning
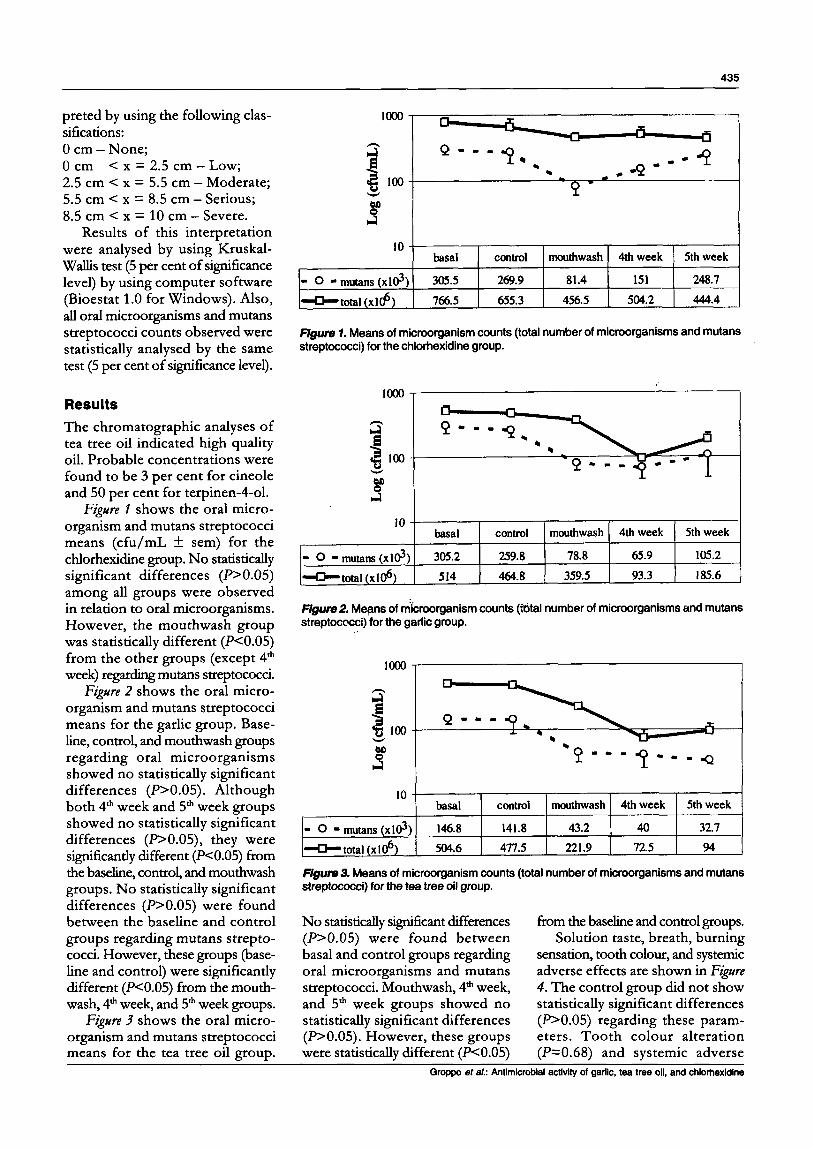
sensation, tooth colour, and systemic adverse effects are shown in Figure 4. The control group did not show statistically significant differences (B0.05) regarding these param- eters. Tooth colour alteration (P=0.68) and systemic adverse - -
Groppo eta/.: Antimicrobial activity of garlic, tea tree oil, and chlorhexidine

436
100
[ 50 E
- 0 z
100
so 8 - 0 9 D-50 E
-1 00 whltout 111110 modonto rrlous rwnn h n g a h n g o dungs dungs -ng.
100
e K so
:-so
E * - 0
- c >
:: -1 00 whlout lltb modrrrto t r b u n rrwrr
m r r l b n nrnnrtbn nrnsrtbn rmrr lbn srnrrtbn
100
f
1” 0 chlorhexidlne
anyono llght modonto bad tonlM0
F/gum4. Adverse effects related: control group, tooth colour alteration, systemic adverse effects, burning sensation, breath, and taste of solution.
effects (PzO.49) did not show statistically significant differences among the treatments (P>0.05). Burning sensation was more intense in the garlic group than in the chlorhexidine (P=0.003) and tea tree oil (P=0.049) groups. In comparison with chlorhexidine (P0.049) and tea tree oil (P=0.007), garlic caused the worst breath. The taste of garlic solution was the worst, compared to chlorhexidine (P=0.007) and tea tree oil (P=0.002). No statistically significant differences were verified between chlorhexidine and tea tree oil (-0.05).
Discussion
Salivary mutans streptococci count- ing was used in this study due to its direct correlation with the number of colonised oral sites2. A decline in the number of these microor- ganisms has been considered to be equivalent to a decrease in dental diseases1J6. Garlic, chlorhexidine, and tea tree oil each caused a reduction of salivary mutans strep- tococci counts.
Chromatographic analyses of tea tree oil showed adequate concentration of cineole (less than 15 per cent) and terpinen-4-01
(more than 30 per cent) according to the Australian Standard AS 2782-851ef13. In fact, it could be considered as high quality oilt2. The emulsifymg agent (Tween 80) was used because it does not inter- fere with the oil antimicrobial properties”. The MIC of the tea tree oil against common pathogens ranges from 0.5 to 1.0 per cent”. MIC against mutans streptococci is lower than 0.0125 per cent and MBC is 0.2 per cent14. Therefore, in the present study, tea tree oil was used as a 0.2 per cent solution.
A significant reduction of oral microorganisms was previously
International Dental Journal (2002) Vol. 5WNo.6

437
observed after the use of 10 per cent garlic solution". However, a terrible taste and odour was veri- fied at this concentration. A lower concentration used in the present study showed satisfactory anti- microbial activity as well as better taste and odour.
A single daily 0.12 per cent chlorhexidine mouthwash reduced by ten times the initial number of oral mutans streptococci'. The results observed in the present study showed similar efficacy of the substances against these micro- organisms. Despite its large anti- microbial spectrum, chlorhexidine has better activity against mutans streptococci than other oral microorganismsI8. This fact could explain the lack of efficacy of chlorhexidine against oral micro- organisms in this study.
NetuschP observed that 0.1 per cent chlorhexidine mouthwashes decreased living plaque micro- organisms up to 76 per cent 1 hour after mouth rinsing. However, 6-8 hours later, microorganisms rose to the original number. In the present study, chlorhexidine did not maintain low mutans streptococci levels after 1 or 2 weeks of mouth- washes. Persistent reduction (residual effect) of oral microorganisms levels was verified in both garlic and tea tree oil groups. A three- month maintained reduction of mutans streptococci was previously described when xylitol chewing gum was used after 14 days of chlorhexidine therapy.
Adverse effects of chlorhexidine such as dental staining', unpleasant taste, gustative alteration, and gingival inflammation' were not observed in this study. Maybe a short-term course of mouthwash was the main reason for the absence of chlorhexi- dine adverse effects.
In spite of its related toxicity2', tea tree oil did not show significant adverse effects, probably due to a low oil concentration. Even at low concentration, the 2.5 per cent garlic showed the highest signifi- cant adverse effects in the present
study. Further studies are necessary to reduce these adverse effects.
Conclusions
Mouthwashes with 2.5 per cent garlic and 0.2 per cent tea tree oil were as able to reduce oral microorganisms as 0.12 per cent chlorhexidine Mouthwashes with 2.5 per cent garlic and 0.2 per cent tea tree oil showed a greater residual effect against microorganisms than 0.12 per cent chlorhexidine A garlic mouthwash showed more adverse effects than mouthwashes with 0.2 per cent tea tree oil and 0.12 per cent chlorhexidine.
Acknowledgments
The authors thank to CNPq for financial support and Mr. Jorge Valerio for his assistance in manu- script preparation.
References 1 .
2.
3.
4.
5.
6.
7.
Bowden G H. Mutans streptococci caries and chlorhexidine. J Can Dent AJJOC 1996 6 2 700. Dasanayake A P, Caufield P W, Cutter G R, et a/. Differences in the detec- tion and enumeration of mutans strep- tococci due to differences in methods. A r c h Oral Biol 1995 40: 345-351. Owens J , Addy M, Faulkner J , et al. A short-term clinical study design to investigate the chemical plaque inhibi- tory properties of mouthrinses when used as adjuncts to toothpastes: applied to chlorhexidine. J Clin Periodontol 1997 24: 732-737. Renton-Harper P, Addy M, Moran J , e f al. A comparison of chlorhexidine, cetylpyridinium chloride, triclosan, and C31G mouthrinse products for plaque inhibition. J Periodontol 1996 67: 486-489. Hildebrandt G H. Effects o f repeated treatment with sustained-release chlorhexidine mouth guards on sali- vary levels of mutuns streptococci, Caries Res 1996 30: 445-453. Clark D C, Guest J L. The effective- ness of three different strengths of chlorhexidine mouthrinse. J Can Dent
Leard A, Addy M. The propensity of AJ.WC 1994 60: 711-714.
different brands of tea and coffee to cause staining associated with chlor- hexidine. J Clin Periodontol 1997 2 4
8. Biedermann B. Garlic - a 'secret mira- cle of God'? Schtveiq Rundscb Med Prax 1995 8 4 7-10.
9. Gonzalez-Fandos E, Garcia-Lopez M L, Sierra M L, et a/. Staphylococcal growth and enterotoxins (A-D) and thermonuclease synthesis in the pres- ence o f dehydrated garlic. J A p p l Bacteriol 1994 77: 549-552.
10. Shelef I, A. Antimicrobial effects of spices. J Food Saf 1984 6 29-44.
1 1 . Elnima E I, Ahmed S A, Mekkawi A G, e f a/. The antimicrobial activity of garlic and onion extracts. Pbarmurie
12. Williams L R. Antimicrobial activity of oil of melaleuca (tea tree oil). Its potential use in cosmetics and toilet- ries. Cosmet Aerosols Toil Aust 1990 4: 12-22.
13. Altman P M. Australian tea tree oil - a natural antisseptic. Aust J Biotech 1989 3: 247-248.
14. Ramacciato J C, Simaes R P, Fl6rio F M, et a/. Antimicrobial activity o f Melaleuca alternifolia against streptococci and S. aunus. J Dent Res 2000 7 9 1071.
15. Barkvoll P, Rella G, Bellagamba S. Interaction between chlorexidine digluconate na sodium monofluoro- phosphate in vitro. Scan J Dent Res 1988 96: 30-33.
16. Axelsson P, Lindhe J, Nystron B. O n
115-1 18.
1983 38: 747-748.
17
18
19
the prevention of caries and periodon- tal disease. Results of a 15-year longi- tudinal study in adults. J Clin Periodontol 1991 18: 182-1 89. Carson C F, Hammer K A, Riley T V. Broth micro-dilution method for determining the susceptibility o f Eschericbia coli and Staphylococcus aureus to the essential oil o f Melaleuca alternifolia (tea tree oil). Micmbios 1995 82: 181-185. Schaeken M J, de Jong M H, Franken H C, etal. Effect of chlorhexidine and iodine o n the composition of the human dental plaque flora. Curies Res 1984 18: 401-407. Netuschil L, Reich E, Brecx M. Direct measurement of the bactericidal effect o f chlorhexidine o n human dental plaque. J Clin Periodontoll989 16: 484- 488.
20. Hildebrandt G H, Sparks B S. Main- taining mutans streptococci with xylitol chewing gum. J A m Dent Assoc 2000 131: 909-916.
21. Jacobs M R, Hornfeldt C S. Melaleuca oil poisoning. J Toxicol Clin Toxicol 1994 32: 461-464.
Groppo et a/.: Antimicrobial activity of garlic, tea tree oil, and chlorhexidine