antihypertensive efficacy and safety of perindopril in mild-to-moderate essential hypertension:...
TRANSCRIPT

Antihypertensive Effkacy and Safety of Perindopril in Mild-to-Moderate Essential Hypertension: Results of a Double-Blind Multicenter Study Versus Atenolol TREFOR 0. MORGAN, M.B.B.s., M.D., WILLIAM J. LOUIS, M.B.B.s., M.D., Melbourne, GRAHAM J. MACDONALD, M.B.B.s., M.D., Sydney ELISABETH L. CONWAY, BSC., Pm., Melbourne, LUCILLE C. BARTHOLOMEUSZ, M.B.B.s., Adelaide, ADRIANNE I.E. ANDERSON, M.B.B.s., Melbourne, DONALD P. CAMERON, M.B.B.s., M.D., Brisbane,
THOMAS DONNELLY, M.B.ch.B., Newcastle, DEREK B. FREWIN, M.B.B.s., M.D., Adelaide, MICHAEL J. HOOPER, M.B.B.s., Sydney, BRUCE JACKSON, M.B.B.s., B.Med.Sc., MAURICE L. MASHFORD, M.B.B.s., Melbourne, PAUL S. MOFFITT, M.B.B.s., Newcast/e, ALISON J. NANKERVIS, M.B.B.s., Melbourne, ANTHONY P. ROBERTS, M.B.B.s.,
Adelaide, GORDON S. STOKES, M.B.B.s., M.D., Sydney, GERALD F.M. WHITING, M.B.ch.B.M., B.A.o., B.A., MAXIM
WILSON, M.B.B.s., BSC., M.D., Brisbane, ROGER N. WNDHAM, M.B.B.s., DENNIS YUE, M.B.B.s., Ph.D., Sydney,
RUDOLF ZACEST, M.B.B.s., M.D., Adelaide, Australia
A 3-month double-blind multicenter trial com- pared the efficacy and safety of perindopril, a new angiotensin-converting enzyme (ACE) in- hibitor, with atenolol in mild-to-moderate es- sential hypertension. A total of 190 patients, 49 of whom were diabetic, entered the perin- dopril-atenolol comparison. Of these, 163 had been previously treated and had a $-week run- in period on placebo; 27 had previously been untreated and received,placebo for 2 weeks. At entry, all patients who had a supine diastolic blood pressure (DBP) of 95-115 mm Hg were randomized to receive perindopril 2 mg or atenolol 25 mg, once daily. Patients were as- sessed at 2 weekly intervals for the first month and then monthly for 2 more months. If supine DBP was >90 mm Hg, treatment was in- creased by stepwise doubling of dose up to 8 mg perindopril or 100 mg atenolol once daily, and later by the addition of hydrochlorothia- zide 25 mg, (indapamide 2.5 mg in diabetic pa- tients) once daily. The two groups were homo- geneous prior to treatment except for supine and erect heart rate, which were higher in the perindopril group than in the atenolol group (p CO.05). Mean supine DBP was 101.1 f 0.6 mm Hg in the perindopril group (n = 94) and 99.9 + 0.6 mm Hg in the atenolol group (n = 96). After 3 months’ active treatment, 74% of patients in the perindopril group achieved a supine DBP of 190 mm Hg and 73% of pa- tients in the atenolol group achieved the same goal. Monotherapy controlled supine DBP in
From the Australian Multicentre Study Group, Adelaide, Brisbane, Melbourne, Newcastle, Sydney, Australia.
Requests for reprints should be addressed to T. Morgan, Department of Physiology, The University of Melbourne, ParkwIle. VIC 3052, Australia.
67% of the perindopril group and 63% of the atenolol group. The decrease in supine DBP was not significantly different between the two groups (-12.9 & 0.9 versus -14.7 + 0.9 mm Hg) but the decrease in erect DBP was lower in the perindopril group (-10.3 + 0.9 versus -13.4 rt 1.0 mm Hg, p ~0.02). Heart rate was reduced in the atenolol group (p CO.001). Sixteen pa- tients withdrew from the study; nine were at- tributed to adverse events, two in the perin- dopril group and seven, including one death, in the atenolol group. Cough was spontaneously reported by 13% patients of the perindopril group and 1% patients of the atenolol group. In 5% of the perindopril cases this was mild and associated with upper respiratory tract in- fection. The nature and incidence of other symptoms were similar with both drugs. Changes in laboratory parameters were minor and not significantly different between the two groups. Analysis of the subgroup of diabetic patients showed similar efficacy and safety re- sults.
T he renin-angiotensin-aldosterone system has an important role in regulation of blood pres-
sure. Blockade of this system by inhibition of angio- tensin-converting enzyme (ACE) is an effective and well-tolerated approach to the treatment of arterial hypertension [l], and it has been suggested that ACE inhibitors could be used as initial drug ther- apy for mild-to-moderate essential hypertension El.
Perindopril is a new, long-acting, nonsulfhydryl ACE inhibitor. After oral administration, perin- dopril is rapidly de-esterified to its active diacid metabolite, perindoprilat, which is excreted pre- dominantly unchanged by the kidney [31. In normal
April 27, 1992 The American Journal of Medicine Volume 92 (suppl 48) 40-73s
subjects, perindopril causes a dose-dependent inhi- bition of plasma ACE activity with an oral dose range of 1-16 mg/day. There is maximal effect at 4-6 hours and persisting ACE inhibition 24 hours after administration of perindopril 4 or 8 mg [4,5]. A single daily dose of perindopril produced a signifl- cant reduction in both systolic and diastolic blood pressure throughout a 24-hour period in hyperten- sive patients [6,‘7]. In a placebo-controlled study, blood pressure control was achieved in 69% of pa- tients treated with perindopril monotherapy [8].
The aim of the present study was to compare the antihypertensive efficacy and safety of perindopril with atenolol, a widely used p-selective adrenocep- tor blocker [9], in patients with mild-to-moderate hypertension.
PATIENTS AND METHODS A 3-month double-blind parallel group study was
conducted in 16 centers in Australia. In each cen- ter, the protocol was approved by an independent human ethics committee and informed consent was obtained from all patients. Patients of both sexes, between the ages of 18 and 75 years, were included if their supine diastolic blood pressure (DBP) was >95 mm Hg but ~115 mm Hg at the end of a single blind run-in placebo period. The duration of this period was 2 weeks in untreated hypertensive pa- tients and 4 weeks in previously treated patients. Criteria for exclusion were secondary or acceler- ated hypertension, bilateral renal artery stenosis, unstable angina, recent myocardial infarction or stroke, heart failure, clinically significant hepatic dysfunction (alanine transferase >25% of upper limit of normal range), renal dysfunction (serum creatinine >180 pmol/L), serious concomitant dis- ease likely to reduce life expectancy, contraindica- tions to receiving p blockers or ACE inhibitors, clear-cut nonresponse to previous treatment with these agents, or women of childbearing potential.
At the end of the placebo run-in period, patients were randomly allocated to receive perindopril 2 mg or atenolol25 mg once daily under double-blind conditions. Randomization was carried out in blocks of four to ensure an even balance of treatment within each center. Active treatment was contin- ued for 3 months with visits at 2 weekly intervals for the first month, then at 4 weekly intervals for the second and third months. At each visit, dosage was adjusted to achieve a supine DBP 190 mm Hg. If supine DBP was >90 mm Hg, there was a step- wise increase in dose to 4 and then 8 mg perindopril or 50 and then 100 mg atenolol, once daily. If supine DBP still remained uncontrolled, hydrochlorothia- zide 25 mg (or indapamide 2.5 mg in diabetic pa- tients) once daily was added. The end point of the study was defined as the number of patients in each
treatment group who achieved a supine DBP 190 mm Hg after 3 months of active treatment. Pa- tients could be withdrawn from the study for one of the following reasons: serious adverse effect, su- pine DBP >115 mm Hg, poor compliance with treatment, or at the patient’s request.
At each visit, blood pressure and heart rate were recorded in triplicate after 10 minutes of supine rest and after 2 minutes in the erect position. A standard mercury sphygmomanometer was used to measure systolic blood pressure (SBP) and DBP (Korotkoff phase V). Heart rate was measured by counting the radial pulse over 1 minute. The time of measurements and time of last drug intake were recorded at each visit. Clinical tolerance was as- sessed at each visit by recording spontaneous com- plaints and by symptoms elicited by a direct ques- tionnaire (14 items). Routine hematology, urea, creatinine, electrolytes, glucose, lipid profile, uric acid, and liver function tests were carried out be- fore and after 1 and 3 months of treatment. In addi- tion, glycosylated hemoglobin was measured before and at 1 and 3 months in diabetic patients.
Statistical Analysis Results are expressed as mean ? standard error
of the mean @EM). Homogeneity of the groups be- fore treatment was assessed by one-way analysis of variance for all parameters apart from gender and previous antihypertensive treatment, which were tested by the chi-square test. All 190 patients who entered the study were included in the analysis of tolerance, but only patients who completed the trial were used in the analysis of efficacy. Since dosage was adjusted in both groups in accordance with the blood pressure response, an overall analysis of effi- cacy was carried out without taking into account the dose factor. Efficacy was assessed in terms of numbers of patients who achieved a supine DBP of 190 mm Hg as well as in terms of changes in blood pressure after 3 months of active treatment. The numbers of patients controlled were compared by the chi-square test. The changes in blood pressure and heart rate (difference after 3 months to before treatment) were compared using one-way analysis of variance. Changes in laboratory parameters were assessed by two-way analysis of variance for comparison within each group completed and, if necessary, by a Newman-Keuls test. Differences of ~5% (p ~0.05) were regarded as significant.
RESULTS A total of 190 patients (66 women and 124 men)
were included in the study. The mean age was 57.2 + 0.7 years (mean + SEM), mean weight was 78.7 + 1.0 kg and the mean duration of known hy- pertension was 10.4 2 0.6 years (range, cl-40
SYMPOSIUM ON ACE lNHlBiTlON! MORGAN ET AL
40-74s April 27, 1992 The American Journal of Medicine Volume 92 (suppl 4B)
SYMPOSIUM ON ACE INHlBlTlON I MORGAN ET AL
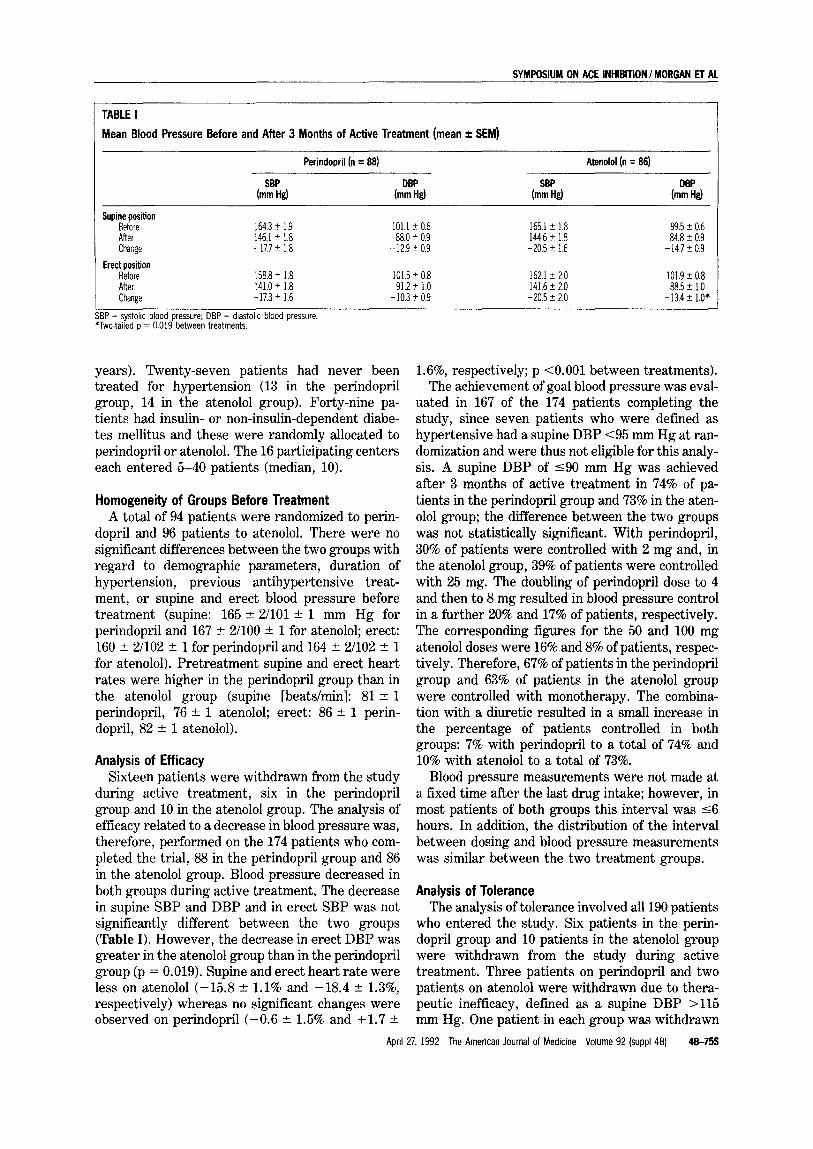
TABLE I Mean Blood Pressure Before and After 3 Months of Active Treatment (mean f SEM)
Perindopril (n = 88) Atenolol (n = 86)
SBP DBP SBP DBP (mm bl (mm k! (mm Hd (mm Hd
Supine position Before After Chatige
164.3 of: 1.9 101.1 ?r 0.6 165.1 k 1.8 99.5 + 0.6 146.1 ? 1.8 88.0 r 0.9 144.6 + 1.8 84.8 k 0.9 -17.7 i 1.8 - 12.9 k 0.9 -20.5 k 1.6 - 14.7 k 0.9
Erec;;? 158.8 + 1.8 After 141.0 i 1.8 Change -17.3? 1.6
SBP = systolic blood pressure; DBP = dlastollc blood pressure. *Two-takd D = 0.019 between treatments.
101.5 ?r 0.8 162.1 k 2.0 101.9 2 0.8 91.2 k 1.0 141.6 + 2.0 88.5 t 1.0
- 10.3 5 0.9 -20.5 t 2.0 -13.4 * 1.0*
years). Twenty-seven patients had never been treated for hypertension (13 in the perindopril group, 14 in the atenolol group). Forty-nine pa- tients had insulin- or non-insulin-dependent diabe- tes mellitus and these were randomly allocated to perindopril or atenolol. The 16 participating centers each entered 5-40 patients (median, 10).
Homogeneity of Groups Before Treatment A total of 94 patients were randomized to perin-
dopril and 96 patients to atenolol. There were no significant differences between the two groups with regard to demographic parameters, duration of hypertension, previous antihypertensive treat- ment, or supine and erect blood pressure before treatment (supine: 165 & Z/101 +- 1 mm Hg for perindopril and 167 + Z/100 + 1 for atenolol; erect: 160 + 2/102 ? 1 for perindopril and 164 of 2/102 + 1 for atenolol). Pretreatment supine and erect heart rates were higher in the perindopril group than in the atenolol group (supine [beats/min]: 81 ? 1 perindopril, 76 + 1 atenolol; erect: 86 or: 1 perin- dopril, 82 + 1 atenolol).
Analysis of Efficacy Sixteen patients were withdrawn from the study
during active treatment, six in the perindopril group and 10 in the atenolol group. The analysis of efficacy related to a decrease in blood pressure was, therefore, performed on the 174 patients who com- pleted the trial, 88 in the perindopril group and 86 in the atenolol group. Blood pressure decreased in both groups during active treatment, The decrease in supine SBP and DBP and in erect SBP was not significantly different between the two groups (Table I). However, the decrease in erect DBP was greater in the atenolol group than in the perindopril group (p = 0.019). Supine and erect heart rate were less on atenolol (-15.8 +- 1.1% and -18.4 + 1.3%, respectively) whereas no significant changes were observed on perindopril (-0.6 + 1.5% and +1.7 +
1.6%, respectively; p <O.OOl between treatments). The achievement of goal blood pressure was eval-
uated in 167 of the 174 patients completing the study, since seven patients who were defined as hypertensive had a supine DBP <95 mm Hg at ran- domization and were thus not eligible for this analy- sis. A supine DBP of 590 mm Hg was achieved after 3 months of active treatment in 74% of pa- tients in the perindopril group and 73% in the aten- 0101 group; the difference between the two groups was not statistically significant. With perindopril, 30% of patients were controlled with 2 mg and, in the atenolol group, 39% of patients were controlled with 25 mg. The doubling of perindopril dose to 4 and then to 8 mg resulted in blood pressure control in a further 20% and 17% of patients, respectively. The corresponding figures for the 50 and 100 mg atenolol doses were 16% and 8% of patients, respec- tively. Therefore, 67% of patients in the perindopril group and 63% of patients in the atenolol group were controlled with monotherapy. The combina- tion with a diuretic resulted in a small increase in the percentage of patients controlled in both groups: 7% with perindopril to a total of 74% and 10% with atenolol to a total of 73%.
Blood pressure measurements were not made at a fixed time after the last drug intake; however, in most patients of both groups this interval was 56 hours. In addition, the distribution of the interval between dosing and blood pressure measurements was similar between the two treatment groups.
Analysis of Tolerance The analysis of tolerance involved all 190 patients
who entered the study. Six patients in the perin- dopril group and 10 patients in the atenolol group were withdrawn from the study during active treatment. Three patients on perindopril and two patients on atenolol were withdrawn due to thera- peutic inefficacy, defined as a supine DBP >115 mm Hg. One patient in each group was withdrawn
April 27, 1992 The American Journal of Medicine Volume 92 (suppl 413) 4575s
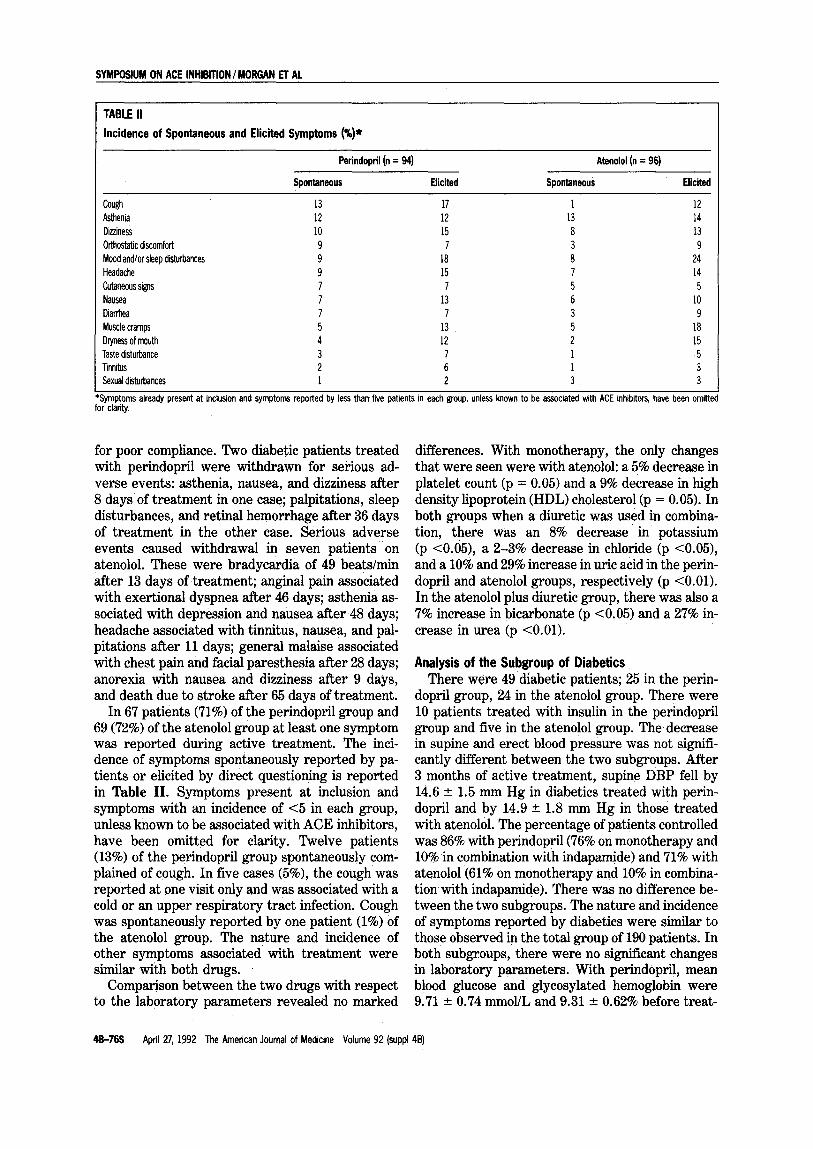
TABLE II
Incidence of Spontaneous and Elicited Symptoms (%)*
Perindopril (n = 94)
Spontaneous Elicited
Atenolol (n = 96)
Spontaneous Elicited
Cough 13 17 1 12 Asthenia 12 12 13 14 Dizziness 10 15 8 13 O&static discomfort 9 7 3 9 Mood and/or sleep disturbances 9 18 8 24 Headache 9 15 1 14 Cutaneous signs 7 7 5 5 Nausea 7 13 6 10 Diarrhea 7 7 3 9 Muscle cramps 5 13 5 18 Dryness of mouth 4 12 2 15 Taste disturbance 3 7 1 5 Tinnitus 2 6 1 3 Sexual disturbances 1 2 3 3
*Symptoms already present at inclusion and symptoms reported by less than five patients in each group, unless known to be associated with ACE inhibitors, have been omittel for clarity.
for poor compliance. Two diabetic patients treated with perindopril were withdrawn for serious ad- verse events: asthenia, nausea, and dizziness after 8 days of treatment in one case; palpitations, sleep disturbances, and retinal hemorrhage after 36 days of treatment in the other case. Serious adverse events caused withdrawal in seven patients on atenolol. These were bradycardia of 49 beatslmin after 13 days of treatment; angina1 pain associated with exertional dyspnea after 46 days; asthenia as- sociated with depression and nausea after 48 days; headache associated with tinnitus, nausea, and pal- pitations after 11 days; general malaise associated with chest pain and facial paresthesia after 28 days; anorexia with nausea and dizziness after 9 days, and death due to stroke after 65 days of treatment.
In 67 patients (‘71%) of the perindopril group and 69 (72%) of the atenolol group at least one symptom was reported during active treatment. The inci- dence of symptoms spontaneously reported by pa- tients or elicited by direct questioning is reported in Table II. Symptoms present at inclusion and symptoms with an incidence of <5 in each group, unless known to be associated with ACE inhibitors, have been omitted for clarity. Twelve patients (13%) of the perindopril group spontaneously com- plained of cough. In five cases (5%), the cough was reported at one visit only and was associated with a cold or an upper respiratory tract infection. Cough was spontaneously reported by one patient (1%) of the atenolol group. The nature and incidence of other symptoms associated with treatment were similar with both drugs.
Comparison between the two drugs with respect to the laboratory parameters revealed no marked
differences. With monotherapy, the only changes that were seen were with atenolol: a 5% decrease in platelet count (p = 0.05) and a 9% decrease in high density lipoprotein (HDL) cholesterol (p = 0.05). In both groups when a diuretic was used in combina- tion, there was an 8% decrease in potassium (p <0.05), a 2-3% decrease in chloride (p <0.05), and a 10% and 29% increase in uric acid in the perin- dopril and atenolol groups, respectively (p cO.01). In the atenolol plus diuretic group, there was also a 7% increase in bicarbonate (p ~0.05) and a 27% in- crease in urea (p <O.Ol).
Analysis of the Subgroup of Diabetics There were 49 diabetic patients; 25 in the perin-
dopril group, 24 in the atenolol group. There were 10 patients treated with insulin in the perindopril group and five in the atenolol group. The decrease in supine and erect blood pressure was not signifi- cantly different between the two subgroups. After 3 months of active treatment, supine DBP fell by 14.6 + 1.5 mm Hg in diabetics treated with perin- dopril and by 14.9 ~fr 1.8 mm Hg in those treated with atenolol. The percentage of patients controlled was 86% with perindopril(76% on monotherapy and 10% in combination with indapamide) and 71% with atenolol(61% on monotherapy and 10% in combina- tion with indapamide). There was no difference be- tween the two subgroups. The nature and incidence of symptoms reported by diabetics were similar to those observed in the total group of 190 patients. In both subgroups, there were no significant changes in laboratory parameters. With perindopril, mean blood glucose and glycosylated hemoglobin were 9.71 + 0.74 mmol/L and 9.31 r 0.62% before treat-
4B-76s April 27, 1992 The American Journal of Medicine Volume 92 (suppl 46)

SYMF’OSIUM ON ACE lNHlBiTlON /MORGAN IT AL
ment and 8.98 +- 0.76 mmol/L and 9.86 + 0.91% after treatment. With atenolol, the corresponding figures were 10.41 + 0.87 mmol/L and 10.17 + 0.77% before treatment and 10.71 + 1.12 mmol/L and 10.47 -+ 0.67% after treatment.
COMMENT This study compared the antihypertensive effi-
cacy and safety of perindopril with atenolol as treatment of mild-to-moderate essential hyperten- sion. In this double-blind parallel group study, drugs were allocated by block randomization to minimize the risk of any imbalance of relevant clini- cal factors between treatment groups in each par- ticipating center. Thus, apart from heart rate, the two groups were well matched for demographic data, history of hypertension, and initial level of blood pressure. No explanation other than chance allocation is apparent for the difference between the heart rates; however, the analysis is on a within-patient basis, which should eliminate any bias between the two groups.
Perindopril2-8 mg daily, plus diuretic when nec- essary, lowered blood pressure in mild-to-moderate hypertension as effectively as atenolol 25-100 mg once daily plus diuretic when needed. The decrease in supine blood pressure, as well as the percentage of patients controlled, was not significantly differ- ent between the two treatment groups. However, the decrease in erect DBP was significantly greater with atenolol than with perindopril. The overall response to atenolol was similar to that found in previous comparative multicenter trials in mild-to- moderate hypertension [lO,ll], suggesting that the present study produced a true estimate of the anti- hypertensive efficacy of atenolol for a valid compar- ison with that of perindopril. In both groups, the first dose level administered appeared to demon- strate particularly good efficacy, resulting in 30% of patients controlled with perindopril 2 mg and 39% with atenolol 25 mg. However, caution must be made in interpreting the response rate because there was no placebo control and some of the effect may have been due to regression to the mean 1121 or an effect of time that may persist for a large number of visits [13]. In a previous double-blind dose-response study, Luccioni et al 1141, using a DINAMAP for continuous blood pressure monitor- ing over 8 hours, found a significant and linear rela- tionship between the logarithm of dose and the an- tihypertensive efficacy of perindopril. The dose of 2 mg was not significantly different from placebo and was significantly less effective than the doses of 4 and 8 mg. However, in the Luccioni study only 10 patients received 2 mglday compared with 88 pa- tients on perindopril in this study. Thus, the power
of the present study to determine an effect was greater. However, 4 and 8 mg of perindopril once daily had an additional antihypertensive effect. Al- though most patients were controlled by monother- apy, an additional 7% of patients achieved control on addition of the diuretic, leaving 26% uncon- trolled. In a similar comparative study between perindopril and atenolol, Zanchetti and Desche [ 151 reported a similar efficacy rate with perindopril, although the efficacy of atenolol was less than in this study.
There was a significant decrease in mean heart rate with atenolol. Despite the decrease in blood pressure, heart rate was not changed by perin- dopril. The hypothesis of a reinforcement of cardiac vagal tone has been given to explain this absence of reflex tachycardia, which seems to be a property shared by all ACE inhibitors [16].
From the present study of 190 patients, it is pos- sible to gain an estimate of the safety profile of perindopril. There were seven withdrawals for ad- verse events in the atenolol group, whereas only two patients were withdrawn from treatment with perindopril because of symptoms. The incidence of side effects reported in the present study was high, 71% of patients in the perindopril group and 72% in the atenolol group complaining of at least one symp- tom either spontaneously or by direct questioning. Cough, an adverse effect frequently reported with ACE inhibitors [17], was spontaneously reported by 13% of patients of the perindopril group and by only 1% of those of the atenolol group. However, in 5 of the 12 cases of cough with perindopril, the symptom was transitory, reported at one visit, and associated with an upper respiratory tract infec- tion, suggesting that the true incidence of perin- dopril-induced cough was 7% rather than 13%. This incidence is similar to that described with other ACE inhibitors [17]. In addition, no case of cough necessitated withdrawal of treatment. The nature and incidence of other symptoms reported with perindopril were similar to those observed with atenolol. These symptoms were minor, nonspecific, and corresponded to those usually described with other antihypertensive drugs [18]. The changes in laboratory parameters were minor and of no clinical relevance. There was no case of leukopenia or ab- normal renal function with perindopril.
ACE inhibitors have been shown to be effective and well-tolerated antihypertensive drugs in dia- betics who are either insulin [19] or noninsulin de- pendent [20]. In the present study, analysis of the subgroup of diabetic patients showed that the anti- hypertensive efficacy of perindopril was similar to that of atenolol. Likewise, apart from cough, the nature and incidence of symptoms were similar in
April 27, 1992 The American Journal of Medicine Volume 92 (suppl 48) a-77s

SYMPOSIUM ON ACE INHIBITION /MORGAN ET AL
both groups of diabetics. In a study of nondiabetic hypertensive patients, enalapril treatment was as- sociated with a slight but significant decrease in mean fasting blood glucose [lo]. In diabetics, anec- dotal reports of blood glucose-lowering effects of ACE inhibitors have been published [21,22] but have not been confirmed by others [19,20,23]. In the present study, no significant change in glycemic control was observed during treatment with perin- dopril or with atenolol.
The results show that perindopril lowered blood pressure to a similar extent as atenolol with a lower incidence of patient withdrawals. Except for cough, there was also a similar incidence of side effects. Perindopril may therefore be considered as first- line treatment for mild to moderate essential hy- pertension.
ACKNOWLEDGMENT The study was supported by Servier Laboratories, Australia.
REFERENCES 1. Williams GH. Convertingenzyme inhibitors In the treatment of hypertension. N Engl J Med 1988; 319: 1517-25. 2. The 1988 report of the Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure. Arch Intern Med 1988; 148: 1023-38. 3. Lees KR, Green ST, Reid JL. Influence of age on the pharmacokinetics and phar- macodynamics of perindopril. Clin Pharmacol Ther 1988; 44: 418-25. 4. Bussien JP, Fasanella d’Amore T, Perret L, eta/. Single and repeated dosing of the converting enzyme inhibitor perindopril to normal subjects. Clin Pharmacol Ther 1986; 39: 554-8. 5. Lees KR, Reid JL. Haemodynamic and humoral effects of oral perindopril, angio- tensin converting enzyme inhibitor, in man. Br J Clin Pharmacol 1987; 23: 159-64. 6. Asmar RG, Pannier BM, Santoni JP, Safar ME. Angiotensin converting enzyme inhibition decreases systolic blood pressure more than diastolic pressure as shown by ambulatory blood pressure monitoring. J Hypertens 1988; 6(Suppl 3): S79-81.
7. West JNW, Smith SA, Stallard TJ, Littler WA. Effects of perindopril on ambulatory intra-arterial blood pressure, cardiovascular reflexes and forearm blood flow in es- sential hypertension. J Hypertens 1989; 7: 97-104. 8. Morgan TO, Anderson A, Wilson 0, Murphy J, Nowson C. The effect of perindopril on blood pressure in humans on different sodium intakes. J Cardiovasc Pharmacol 1987; lO(Suppl 7): S116-8. 9. Heel RC. Brogden RN, Speight TM, Avery GS. Atenolol: a review of its pharmaco- loglcal properties and therapeutic efficacy in angina pectons and hypertension. Drugs 1979; 17: 425-60. 10. Helgeland A, Stroemmen, R, Hagelund CH, Tretli S. Enalapril, atenolol and hy- drochlorothiazide in mild to moderate hypertension. A comparative multicentre study In general practice in Norway. Lancet 1986; 1: 872-5. 11. Bolzano H, Arriaga J, Bernal R, et a/. The antihypertensive effect of lisinopril compared to atenolol in patients with mild to moderate hypertension. J Cardiovasc Pharmacol 1987; 9(Suppl 3): S43-7. 12. Gill JS, Zezulka AV, Beevers DG, Davies P. Relation between initial blood pres- sure and its fall with treatment. Lancet 1985; 1: 567-9. 13. Chalmers J, Morgan TO, Doyle AE, eta/. Australian National Health and Medical Research Council dietary salt study in mild hypertension. J Hypertens 1987; 4(Suppl 6): S629-37.
14. Luccioni R, Frances Y, Gass R, Schwab C, Santoni JP, Perret L. Evaluation of the dose-effect relationship of a new ace inhibitor (perindopril) by an automatic blood pressure recorder. Eur Heart J 1988; 9: 1131-6. 15. Zanchetti A, Desche P. Perindopril: first-line treatment for hypertension. Clin Exp (Theory and Pracbce) Hypertens [A] 1989; All(Suppl 2): 555-73. 16. Ajayi AA, Lees KR, Reid JL. Effects of angiotensin converting enzyme inhibitor, perindopril, on autonomic reflexes. Eur J Clin Pharmacol 1986; 30: 177-82. 17. Tugwell S, Stokes GS. Angiotensin converting-enzyme inhibitor agents and respi- ratory symptoms. Med J Aust 1987; 147: 263-4. 18. Husserl FE, Messerli FH. Adverse effects of antihypertensive drugs. Drugs 1981; 22: 188-210. 19. Passa P, Leblanc H, Marre M. Effects of enalapril in insulin-dependent diabetic
subjects with mild to moderate uncomplicated hypertension. Diabetes Care 1987; lo: 200-4. 20. Moore MP, Elliott TW, Nicholls GM. Hormonal and metabolic effects of enalapril treatment in hypertensive subjects with NIDDM. Diabetes Care 1988; 11: 397-401. 21. McMurray J, Fraser DM. Captopril, enalapril and blood glucose. Lancet 1986; 1: 1035. 22. Rett K, Wicklmayr M, Dietze G. Hypoglycemia in hypertensive diabetic patients treated with sulphonylureas, biguanides and captopril. N Engl J Med 1988; 319: 1609. 23. Winocour P, Waldek S, Anderson DC. Captopril and blood glucose. Lancet 1986; 2: 461.
40-78s April 27, 1992 The American Journal of Medicine Volume 92 (suppl 46)