annals of clinical & laboratory science, vol. 43, no. 1 ... · sinonasal undifferentiated...
TRANSCRIPT

Available online at www.annclinlabsci.org
Sinonasal Undifferentiated Carcinoma (SNUC): Morphoproteomic-Guided Treatment Paradigm with Clinical Efficacy
Maria Ansari1, Shan Guo1, Samer Fakhri2, Martin J. Citardi 2, Angel Blanco3, Maria Patino4, Jamie Buryanek5, Robert Amato1, Ron Karni2, and Robert E. Brown5
1Division of Oncology, Department of Internal Medicine, University of Texas Medical School at Houston and Memorial Hermann Cancer Center, Houston, TX; 2Department of Otorhinolaryngology, University of Texas Medical School at Houston, and Texas Skull Base Physicians, Houston, TX; 3Memorial Hermann Cancer Center, Memorial Hermann Hospital-Texas Medical Center, Houston TX.; 4Department of Radiology, University of Texas Medical School at Houston, Houston, TX; 5Department of Pathology and Laboratory Medicine, University of Texas Medical School at Houston, Houston, TX, USA
Abstract. Sinonasal undifferentiated carcinoma (SNUC) is a rare and highly malignant tumor that occurs in the nasal cavity and/or paranasal sinuses. Prognosis is poor despite multimodality treatment. Currently, there is no optimal standard of treatment, partially due to a lack of research defining the biology of such tumors. This report discusses two SNUC cases where patients received a novel chemotherapeutic approach using cisplatin, etoposide, Adriamycin (doxorubicin), metformin, and adjuvant melatonin therapies based on morphoproteomic-guidance, followed by consolidation with chemoradiation therapy. This resulted in excellent and objective tomographic and magnetic resonance imaging and clinical responses including com-plete responses in the induction phase utilizing morphoproteomic-guided therapies. Later, endoscopic ex-cision of the tumor bed failed to reveal any residual tumor. Morphoproteomics helped to define the biology of these SNUC tumors and provided targets for the agents employed, creating a new treatment paradigm for such tumors. This treatment regimen poses a new effective regimen to treat SNUC.
Keywords: SNUC, morphoproteomics
Introduction
Sinonasal undifferentiated carcinoma (SNUC) is a poorly differentiated carcinoma that arises from Schneiderian mucosa which lines the nasal cavity and paranasal sinuses. It is a very rare disease with an unknown exact incidence rate. A meta-analysis on treatment outcomes for SNUC included 30 studies with 167 cases described between 1986 to 2009 [1]. In published series, 19 patients were identified in the University of Michigan’s skull base tumor database, which included over 1100 patients with skull base tumors over a 13 year span [2]. The median age at diagnosis is 50 to 60 years with the
5-year overall survival at 22 to 63%. Having been previously diagnosed as esthesioneuroblastoma or neuroendocrine carcinoma, SNUC was first de-scribed as a distinct entity by Frierson, et al [3].
SNUC is a highly aggressive malignancy with a poor prognosis overall. It is often diagnosed at a locally advanced stage due to the rapid growth of the tumor and its propensity to extend into the or-bital and periorbital tissues and the central nervous system. The previously mentioned meta-analysis of 167 patients found that 52.7% of patients had died of the disease with a median follow up of 15 months, despite treatment[1]. The most com-mon causes of death after multimodality treatment include an associated recurrence, either local-re-gional or metastatic or persistent local-regional tu-mor [4].
Annals of Clinical & Laboratory Science, vol. 43, no. 1, 2013
0091-7370/13/0100-045. © 2013 by the Association of Clinical Scientists, Inc.
Address correspondence to Robert E. Brown, M.D.; UT Health-Medical School at Houston, 6431 Fannin Street MSB 2.286, Houston, TX 77030; phone: 1-713-500-5332; fax: 1-713-500-0695; e mail: [email protected]
45

There has been no consensus in terms of optimal management. Multimodality treatments incorpo-rating surgery, radiation, and chemotherapy have been adopted in an effort to improve disease con-trol with the most common regimen being surgical resection followed by adjuvant radiation, with or ithout chemotherapy. Concurrent chemoradiation is commonly used in cases with unresectable tu-mors. Chemotherapy has mostly been used in con-junction with radiation, often in the post-operative and definitive setting. Different combinations of chemotherapeutic agents have been described in published series with a ma-jority incorporating platinum in combination with agents such as etoposide, a taxane or 5-fluorouracil (5-FU). However, the response to chemotherapy has not been extensively studied. The data on in-duction chemotherapy are scarce. Moreover, the response to induction chemotherapy, in published series, has been less than optimal with partial re-sponses or stable disease being the most expected outcome [5]. Morphoproteomics combines morphology using bright field microscopy and immunohistochemical probes to help identify protein analytes in tumor cells and cells of the microenvironment that might define the unique biology of an individual patient’s tumor and expose potential therapeutic targets [6, 7]. By utilizing a combination of the expression level of a given protein (i.e., its level of expression or overexpression vis-à-vis the companionate nonneo-plastic tissues), its state of activation as reflected in
the detection of the molecule’s putative sites of acti-vation using phosphospecific immunohistochemi-cal probes, and/or by noting its subcellular com-partmentalization and correlative expression with other protein molecules, morphoproteomics can help define the biology of an individual tumor. More specifically, morphoproteomics can detect upstream signal transducers, pathways of conver-gence and downstream effectors of signaling path-ways, cell cycle-related analytes, tumorigenic and prosurvival pathways, and stemness characteristics in tumor cells. In the process, morphoproteomics provides therapeutic options that target the basic biology of a tumor in the hope of interrupting his-togenetic and pathogenetic sequences that lead to tumoral growth and chemoradioresistant, recurrent disease. Morphoproteomics was employed in these two cases of SNUC. To date, there have been no reports in the literature (to our knowledge) that have described complete responses in SNUC after treatment only with che-motherapy. Here we describe a series of 2 cases of SNUC in which the patients achieved a complete response after a chemotherapeutic regimen that was based on morphoproteomics. Chemoradiation was given as consolidation treatment, and both patients were without evidence of recurrence at 16 months and 14 months follow-up, respectively.
Materials and Methods
The histopathologic diagnosis of SNUC in these two patients was based on the microanatomical
Annals of Clinical & Laboratory Science, vol. 43, no. 1, 2013
Table 1. Protein analytes detected by morphoproteomic analysis in sinonasal undifferentiated carcinomas*
Protein Analyte Patient #1 Patient #2CD133 ±-3+ (P-C)** ±-3+ (P)Fatty Acid Synthase (FASN) 2+-3+(C) 1+-3+ (C)Topoisomerase II alpha ~30% (N) ~50% (N)p-mTOR (Ser 2448) 1-2+/±-occ 1+(N/C-P) 1-3+/±-occ 1+(N/C-P)
*Scoring of chromogenic signal intensity of protein analytes based on a scale of 0 to 3+ and included visual estimation of percentage of nuclear immunopositivity for topoisomerase II alpha. **Subcellular compartmentalization of signal (P=plasmalemmal; C= cytoplasmic; N=nuclear). Nuclear (N) phosphorylated (p) mammalian target of rapamycin on serine 2448 favors mTORC2
46
Morphoproteomic-Guided Treatment in SNUC
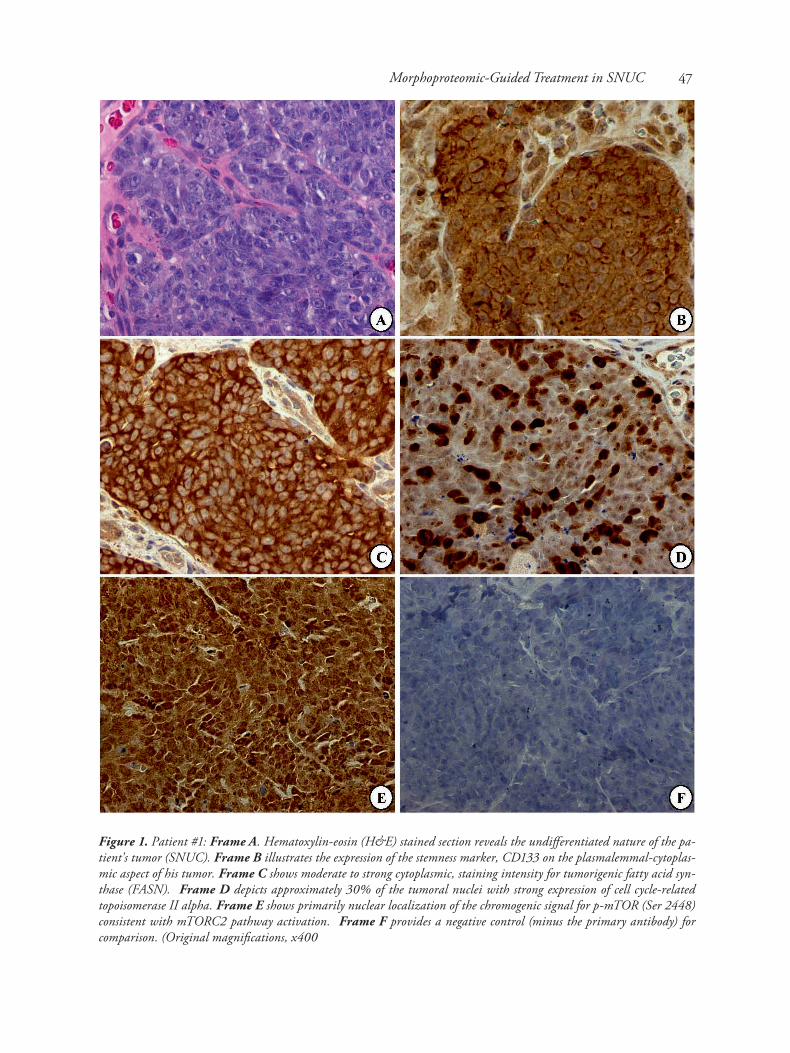
Figure 1. Patient #1: Frame A. Hematoxylin-eosin (H&E) stained section reveals the undifferentiated nature of the pa-tient's tumor (SNUC). Frame B illustrates the expression of the stemness marker, CD133 on the plasmalemmal-cytoplas-mic aspect of his tumor. Frame C shows moderate to strong cytoplasmic, staining intensity for tumorigenic fatty acid syn-thase (FASN). Frame D depicts approximately 30% of the tumoral nuclei with strong expression of cell cycle-related topoisomerase II alpha. Frame E shows primarily nuclear localization of the chromogenic signal for p-mTOR (Ser 2448) consistent with mTORC2 pathway activation. Frame F provides a negative control (minus the primary antibody) for comparison. (Original magnifications, x400
47
features of the tumors, their immunophenotype, and the correlation with their clinical presentation and anatomical location. Morphoproteomic analy-sis of specific protein analytes in representative par-affin-embedded sections from each of these pa-tients’ tumors was carried out according to previously defined procedures [6,7] and with ap-propriate positive and negative controls. Specific probes were utilized to detect the following: CD133, a putative stemness marker [8] in the con-text of the tumor’s undifferentiated state; fatty acid synthase (FASN),a tumorigenic molecule[9 ]; topoisomerase II alpha, a cell cycle-related analyte [10]; and mammalian target of rapamycin (mTOR) phosphorylated on serine 2448[6,7,11]. The score of the immunohistochemical reactions for each of these analytes was graded on a scale of 0 to 3+, according to the chromogenic (brown) signal intensity of the 3, 3’- diaminobenzidine (DAB) chromogenic reaction. Subcellular compartmental-ization as plasmalemmal (P), cytoplasmic (C) and/or nuclear (N) was also noted.
In addition, the percentage of nu-clei with immu-nopositivity for topoisomerase II alpha expression was visually esti-mated. These were utilized to help de-velop a combinato-rial therapy.
Case Reports
Patient #1. Clinical Presentation. A 40 year-old male with no significant past medical history presented with a sudden onset of si-nus pressure, con-gestion and right-sided headache that
was associated with increased lacrimation in the right eye, right periorbital pressure, epiphora, anos-mia and mild proptosis. His endoscopic results re-vealed a pedunculated mass in the middle meatus extending anteriorly into the nasal cavity. Office nasal endoscopy, computerized tomography (CT), and magnetic resonance (MR) imaging defined a 7.8 cm x4.6 cm x6.9 cm sinonasal mass with intra-cranial extension and right orbital involvement. The initial MRI also confirmed a large 7.7cm x 3.6cm x 7cm in anteroposterior diameter, right na-sal ethmoidal mass with intracranial extension and extension into the medial extraconal space of the right orbit. It displaced, but did not invade into the right medial rectus muscle. Initial staging with positron emission tomography (PET)/CT imaging showed right nasal cavity mass with an 18 F-fluorodeoxyglucose (FDG) standardized uptake value (SUV) of 21.7 and FDG-avid bilateral cervi-cal lymphadenopathy at level II measuring up to 1 cm. There were no distant metastases. Biopsy of the nasal mass had the histopathologic features and im-munophenotype of SNUC.
Annals of Clinical & Laboratory Science, vol. 43, no. 1, 2013
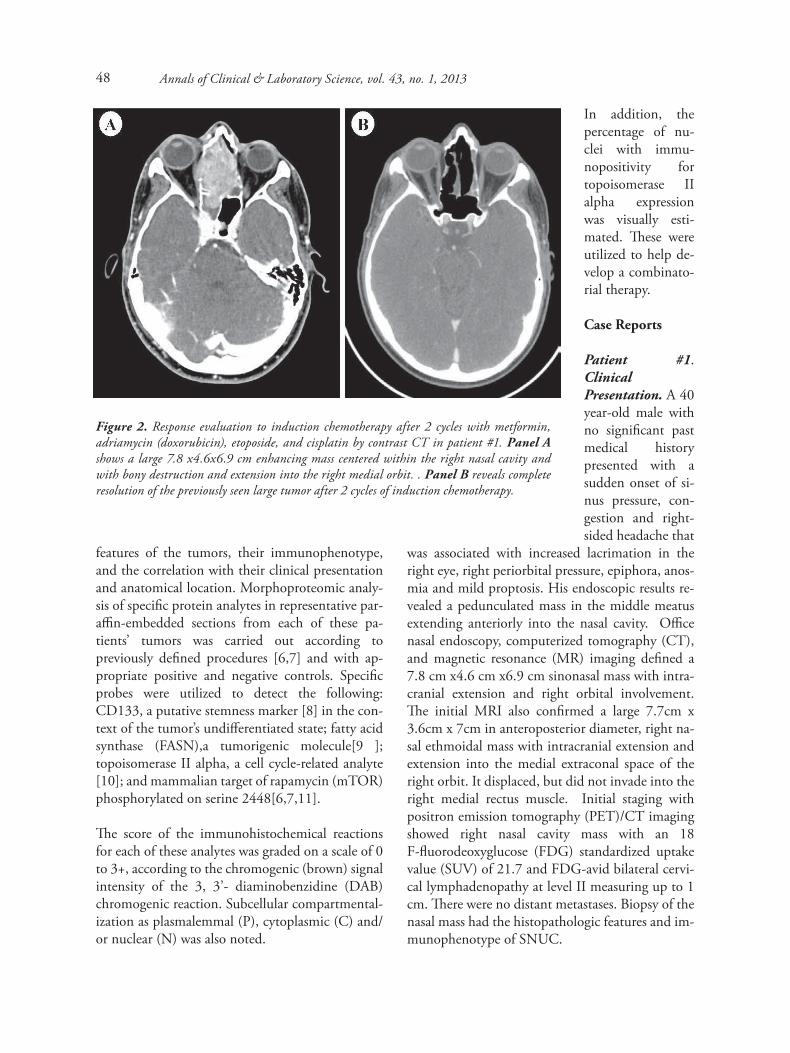
Figure 2. Response evaluation to induction chemotherapy after 2 cycles with metformin, adriamycin (doxorubicin), etoposide, and cisplatin by contrast CT in patient #1. Panel A shows a large 7.8 x4.6x6.9 cm enhancing mass centered within the right nasal cavity and with bony destruction and extension into the right medial orbit. . Panel B reveals complete resolution of the previously seen large tumor after 2 cycles of induction chemotherapy.
48
Morphoproteomic Findings. Morphoproteomic studies on the patient’s tumor, as described above revealed: (1) plasmalemmal and cytoplasmic ex-pression of the stemness marker CD133 at ± to 3+; (2) moderate to marked expression of FASN in the cytoplasmic compartment; (3) immunopositivity for topoisomerase II alpha, comprising approxi-mately 30% of the tumoral nuclei; and (4) moder-ate expression of p-mTOR (Ser 2448) at 1+ to 2+ in tumoral nuclei with minimal to mild expression in the cytoplasmic-plasmalemmal compartments, favoring mTOR complex2 (mTORC2) over mTORC1 [ 11,12 ]. These are summarized in Table 1 and depicted in Figure 1. Morphoproteomic-Guided Targeted Therapy with Rationale. A collaborative effort was under-taken by the health care team in devising a thera-peutic strategy in the context of the morphopro-teomic findings. Metformin, etoposide, adriamycin (doxorubicin) ,and cisplatin, as well as melatonin as an adjunctive agent, were chosen with the follow-ing rationale: metformin and etoposide have anti-tumoral stem cell actions [13,14], and should have antitumoral activity against the CD133 positive cell population and the undifferentiated state of the tumor; metformin downregulates FASN expression [15] and should reduce its tumorigenic influence [9]; doxorubicin and etoposide both target the topoisomerase II [16] and metformin works
collaboratively with doxorubicin while reducing the latter’s potential cardiotoxicity [13,17]; and metformin inhibits both mTORC1 and compo-nents of the mTORC2 pathway, when driven by the insulin-like growth factor pathway [18]. Cisplatin has shown efficacy with epidoxorubicin in locally advanced undifferentiated nasopharyn-geal carcinoma [19] and was included in the regi-men. Melatonin at 20 mg per day at bedtime was chosen as an adjunctive therapy given its ability to reduce the toxicity while improving the clinical ef-ficacy of chemotherapeutic agents such as etopo-side, cisplatin, and doxorubicin, including the po-tential to reduce myelosuppression and doxorubicin-associated cardiotoxicity [20-22]. Clinical Outcome in Patient#1 Treated with Morphoproteomic-Guided Therapies. Combinatorial chemotherapy consisting of doxorubicin(25mg/m2 ) on day 1, etoposide (80mg/m2 ) and cisplatin (25 mg/m2 ) on days 2 -4, and metformin (500 mg) b.i.d. every 21 days, along with melatonin 20 mg at bedtime was ad-ministed to the patient. He tolerated the therapeu-tic regimen well with the only side effect being grade II nausea which was easily controlled by anti-emetics. His re-staging CT scans after cycle 2 showed complete resolution of both the sinonasal mass and the bilateral cervical lymphadenopathy (Figure 2). His re-staging FDG-PET/CT
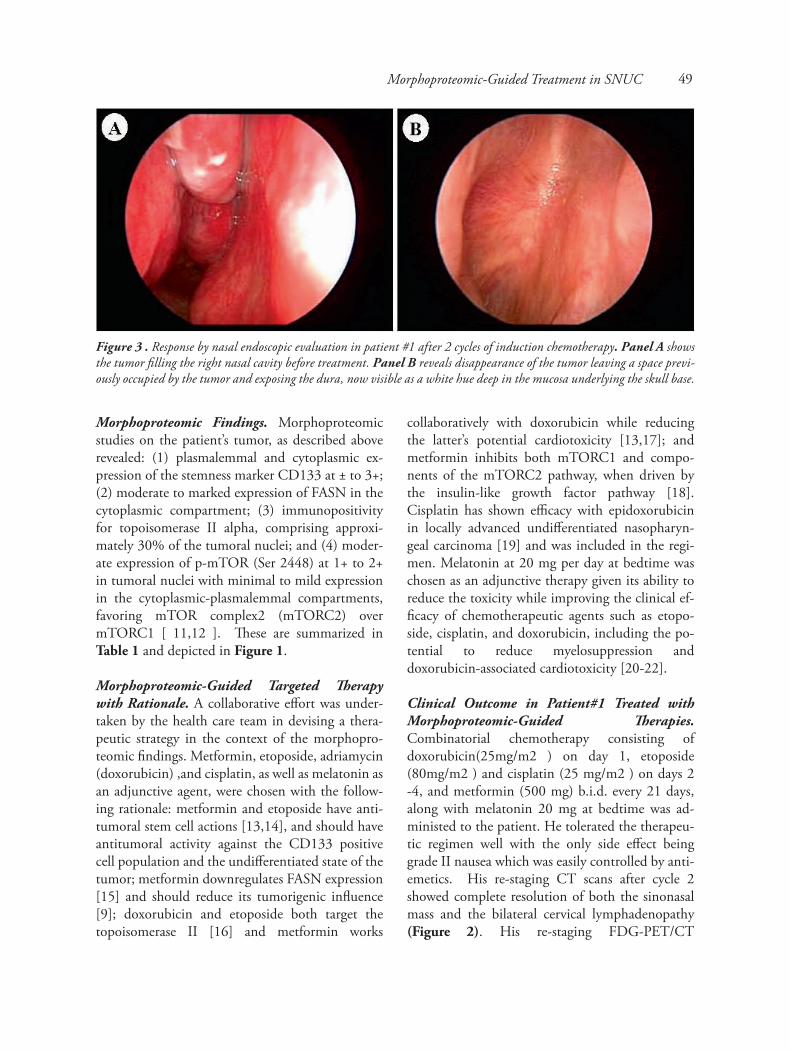
Figure 3 . Response by nasal endoscopic evaluation in patient #1 after 2 cycles of induction chemotherapy. Panel A shows the tumor filling the right nasal cavity before treatment. Panel B reveals disappearance of the tumor leaving a space previ-ously occupied by the tumor and exposing the dura, now visible as a white hue deep in the mucosa underlying the skull base.
Morphoproteomic-Guided Treatment in SNUC 49
Annals of Clinical & Laboratory Science, vol. 42, no. 3, 2012after cycle 2 also showed complete response to treatment. Endoscopic exam revealed an open cav-ity in the right nasal region, where the space result-ed from the resolution of the tumor. In short, there was no residual tumor seen (Figure 3).
The left side nasal cavity was clear. He completed 1 more cycle of the above induction chemotheray fol-lowed by concurrent chemoradiation (60Gy in 30 fractions to the involved sinuses with weekly carbo-platin AUC 1.5). He has been followed by serial imaging studies and underwent endoscopic biop-sies of the original tumor bed 6 months after the completion of treatment. He has remained free of disease 16 months after completion of treatment. He did not require oncologic resection or any ad-ditional treatment.
Patient #2. Clinical Presentation. A 20-year old otherwise healthy female presented with 6 months of progressive left nasal obstruction, left sided sinus pressure, headache, intermittent left epistaxis, and 1 month of left proptosis, diplopia and peri-orbital mass. She had been treated in the past for rhinosi-nusitis without improvement. Her physical exami-nation revealed the presence of a left periorbital mass with left proptosis and lateral gaze to the left, on the left side. Endoscopic exam confirmed a fun-gating left sinonasal mass.
The initial imaging with CT and MRI detected a mass of 3.6 cm x 2.5 cm x 2.4 cm with extension into the left orbit and also an intracranial extension into the right frontal region measuring 7.2 cm x 5.7cm x5.1 cm. The latter was associated with bony erosion and destruction of parts of the skull base as well as vasogenic edema, and mass effect upon the frontal horns of the lateral ventricle. Initial staging with FDG-PET/CT imaging showed increased FDG uptake of the large mass in the up-per sinonasal cavity and the intracranial extension. There was no regional nor distant metastasis noted. An office biopsy of the mass revealed histopatho-logic and immunophenotypic features of SNUC. Morphoproteomic Findings. The morphopro-teomic findings with regard to the expression of CD133, FASN, topoisomerase II alpha, and p-mTOR (Ser 2448) in this patient’s tumor largely
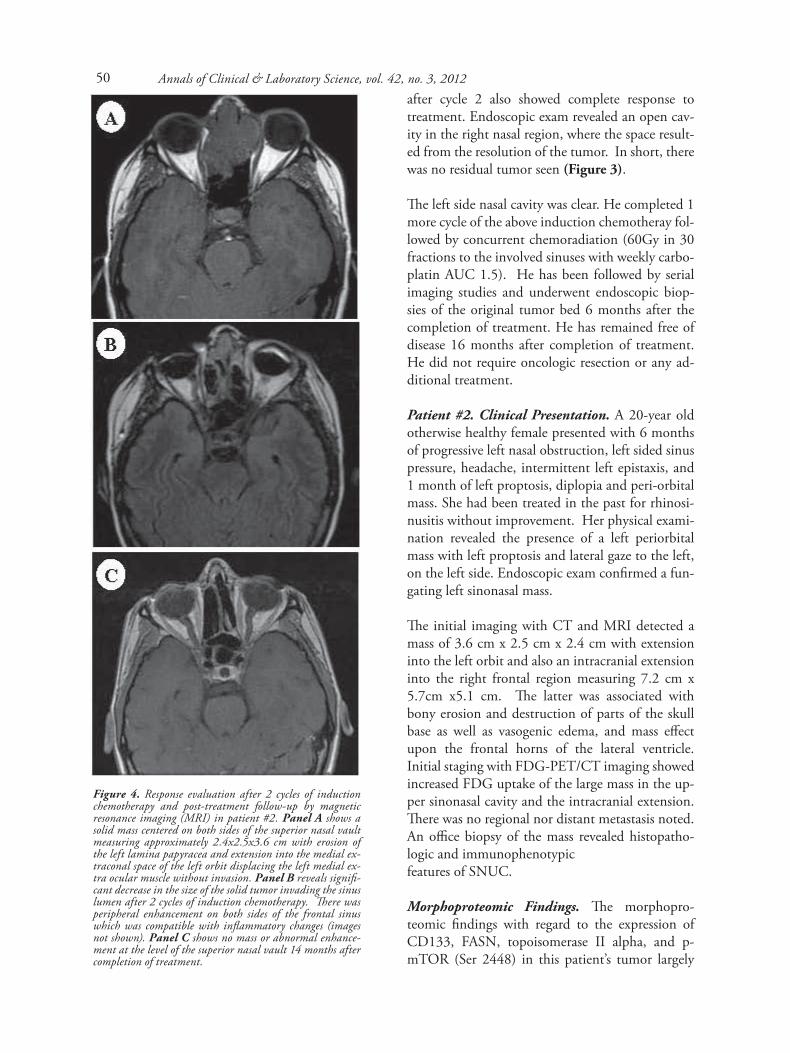
Figure 4. Response evaluation after 2 cycles of induction chemotherapy and post-treatment follow-up by magnetic resonance imaging (MRI) in patient #2. Panel A shows a solid mass centered on both sides of the superior nasal vault measuring approximately 2.4x2.5x3.6 cm with erosion of the left lamina papyracea and extension into the medial ex-traconal space of the left orbit displacing the left medial ex-tra ocular muscle without invasion. Panel B reveals signifi-cant decrease in the size of the solid tumor invading the sinus lumen after 2 cycles of induction chemotherapy. There was peripheral enhancement on both sides of the frontal sinus which was compatible with inflammatory changes (images not shown). Panel C shows no mass or abnormal enhance-ment at the level of the superior nasal vault 14 months after completion of treatment.
50

replicated those in patient #1, except for a princi-pally plasmalemmal expression of CD133, a stron-ger nuclear expression of p-mTOR (Ser 2448), and higher percentage of tumoral nuclei expressing topoisomerase II alpha in patient #2 (see Table 1 and morphoproteomic parallels in Figure 1).
Morphoproteomic-Guided Target Therapy with Rationale. The morphoproteomic findings in the tumor of patient #2 supported a therapeutic regi-men identical to that used for induction therapy in patient #1 (vide supra).
Clincal Outcome in Patient #2 Treated with Morphoproteomic-Guided Therapies. A combina-tion regimen, based on the morphoproteomic find-ings and comprised of doxorubicin (25 mg/m2 ) on day 1, etoposide (80 mg/m2 ) and cisplatin (25mg/m2 ) on days 2-4, along with metformin at 500 mg b.i.d.every 21 days and adjunctive melato-nin (20 mg/day at bedtime), was given. The main side effect that this patient experienced was also nausea, which was readily managed by anti-emet-ics. Otherwise, the therapeutic regimen was well tolerated. The patient had improvement in her na-sal obstruction and diplopia after 1 cycle of treat-ment. Restaging FDG-PET/CT after 2 cycles showed a complete response to treatment with no abnormal FDG avidity to suggest residual active disease or recurrence. MRI of her face after 2 cycles of treatment revealed significant resolution of the solid component of the previously seen large sino-nasal mass and intracranial extension (Figures 4 and 5). Subsequently, the patient was given another cycle of combination chemotherapy for a total of 3 cycles. This was followed by chemoradiation (60 Gy in 30 fractions to the involved sinuses with weekly carboplatin AUC 1.5). She then underwent endoscopic surgical resection of the left ethmoid. The skull base looked attenuated, but it seemed in-tact. Subsequent, biopsies confirmed the absence of any residual tumor. After that surgery, she had symptoms suggesting a CSF leak; operative explo-ration did not confirm the presence of a CSF leak, but a free mucosal graft was placed over the eth-moid roof. The patient has remained free of disease for 14 months after completion of treatment (see Figures 4 and 5, Panel C).
Figure 5. Response evaluation after 2 cycles of induction chemotherapy and post-treatment follow-up by magnetic resonance imaging (MRI) in patient#2. Panel A shows the intracranial component measuring approximately 5.1x5.7x7.2 cm and associated with a large rim enhancing cyst. The mass is surrounded by a small amount of vasogenic edema which has resulted in a significant mass effect upon the frontal horns of the lateral ventricle. The anterior cere-bral arteries are also displaced by the mass but remain pat-ent. Panel B depicts partial resolution of the solid intracra-nial tumor in the right frontal region with residual incompletely enhancing cystic lesion measuring approxi-mately 2.5x4.1cm with minimal mass effect upon the right frontal horn after 2 cycles of induction therapy. The tumor extending into the medial aspect of both orbits, left greater than right resolved completely. Panel C shows decreased size of the residual cystic component of the mass and mass effect in the anterior inferior right frontal lobe 14 months after completion of treatment.
Morphoproteomic-Guided Treatment in SNUC 51

Discussion
Sinonasal undifferentiated carcinoma (SNUC) presents a particular challenge for clinicians due to its rarity, aggressive behavior, overall prognosis, and lack of consensus on optimal management. Although there have been scattered reports on long term survival with aggressive multimodality treat-ment, the role of induction chemotherapy and the optimal agents for the management of SNUC have not been well defined.
Our two patients received a combination of met-formin, doxorubicin, and etoposide as primary in-duction therapy based on morphoproteomic analy-sis of their SNUC tumors. Specifically, morphoproteomics helped to define the biology of these tumors revealing stemness (CD133), tumori-genic (FASN), cell cycle (Topoisomerase II alpha) and mTOR (p-mTOR [Ser 2448]) pathway ana-lytes targetable by this combination of agents, as previously outlined (vide supra [8-18]). Cisplatin was included given its reported efficacy with epi-doxorubicin against locally advanced, undifferenti-ated nasopharyngeal carcinoma [19]. Melatonin was also used as an adjunctive agent to reduce the risk of chemotherapy-associated toxicity, particu-larly that associated with doxorubicin [20-22]. Both patients achieved a complete response with induction chemotherapy alone, negating the need for surgical resection. They also both received chemoradiation as consolidation treatment. Moreover, the induction regimen was well tolerated with minimal side effects in both patients. To our knowledge, there have been no reports in SNUC of a complete response to combination che-motherapy in the induction phase. Furthermore, the combined use of doxorubicin, etoposide, cispla-tin, and metformin with melatonin as adjunctive therapy to treat SNUC has not been previously re-ported in the literature from our review of the National Library of Medicine’s MEDLINE Database. In light of the excellent response and good tolerance of this regimen in our patients with morphoproteomic correlates, further investigation
in the form of a prospective trial should be consid-ered. In summary, our case studies illustrate the application of morphoproteomic analysis in help-ing to define the biology of sinonasal undifferenti-ated carcinoma and in providing guidance in the design of a treatment paradigm, leading to a com-plete clinical response to induction therapy with doxorubicin, etoposide, cisplatin, and metformin, and with melatonin as adjunctive therapy.
Acknowledgements The authors thank Ms Pamela K. Johnston, HT (ASCP) for technical support, Ms Bheravi Patel for secretarial support and help with the graphics, and Ms. Mika Stepankiw for assistance in editing and preparing the manuscript.
References
1. Riersen DA, Pahilan ME, Devalah AK. Meta-analysis of treat-ment outcomes for sinonasal undifferentiated carcinoma. Otolaryngol Head Neck Surg. 2012;147:7-14.
2. Lin EM, Sparano A, Spalding A, Eisbruch A, Worden FP, Heth J, Sullivan SE, Thompson BG, Marentette LJ. Sinonasal undif-ferentiated carcinoma : a 13-year experience at a single institu-tion. Skull Base. 2010;20:61-7.
3. Frierson HF, JF, Mills SE, Fechner RE, Taxy JB and Levine PA. Sinonasal undifferentiated carcinoma. An aggressive neo-plasm derived from schneiderian epithelium and distinct from olfactory neuroblastoma. Am J Surg Pathol. 1986; 10:771-779.
4. Miyamoto RC, Gleich LL, Biddinger PW and Gluckman JL. Esthesioneuroblastoma and sinonasal undifferentiated carci-noma: impact of histological grading and clinical staging on survival and prognosis. Laryngoscope. 2000;110:1262-1265.
5. Rischin D, Porceddu S, Peters L, Martin J, Corry J, Weih L. Promising results with chemoradiation in patients with sinona-sal undifferentiated carcinoma. Head and Neck. 2004;26:435-41.
6. Brown RE. Morphoproteomics: exposing protein circuitries in tumors to identify potential therapeutic targets in cancer pa-tient. Expert Rev Proteomics.2005; 2:337-348.
7. Brown RE. Morphogenomics and morphoproteomics: a role for anatomic pathology in personalized medicine. Arch Pathol Lab Med. 2009; 133:568-579.
8. Wei XD, Zhou L, Cheng L, Tian J, Jiang JJ, and Maccallum J. In vivo investigation of CD133 as a putative marker of cancer stem cells in Hep-2 cell line. Head Neck. 2009; 31:94-101.
9. Xiao R, Su Y, Simmen RC, and Simmen FA. Dietary soy pro-tein inhibits DNA damage and cell survival of colon epithelial cells through attenuated expression of fatty acid synthase. Am J Physiol Gastrointest Liver Physiol. 2008;294:G868-876.
10. Li H, Wang Y, Liu X. Plk1-dependent phosphorylation regu-lates functions of DNA topoisomerase II alpha in cell cycle progression. J Biol Chem. 2008; 283:6209-6221.
11. Rosner M, Siegel N, Valli A, Fuchs C, Hengstschlager M. mTOR phosphorylated at S2448 binds to raptor and rictor. Amino Acids.2010; 38:223-228.
Annals of Clinical & Laboratory Science, vol. 42, no. 3, 201252

12. Rosner M, Hengstschlager M. Cytoplasmic and nuclear distri-bution of the protein complexes mTORC1 and mTORC2: ra-pamycin triggers dephosphorylation and delocalization of the mTORC2 components rictor and sin1. Hum Mol Genet. 2008; 17:2934-2948.
13. Hirsch HA, Iliopoulos D, Tsichlis PN, Struhl K. Metformin selectively targets cancer stem cells, and acts together with che-motherapy to block tumor growth and prolong remission. Cancer Res. 2009; 69:7507-7511.
14. Gupta PB, Onder TT, Jiang G, Tao K, Kuperwasser C, Weinberg RA, Lander ES. Identification of selective inhibitors of cancer stem cells by high-throughput screening. Cell. 2009; 138:645-659.
15. Algire C, Amrein L, Zakikhani M, Panasci L, Pollak M. Metformin blocks the stimulative effect of a high-energy diet on colon carcinoma growth in vivo and is associated with re-duced expression of fatty acid synthase. Endocr Relat Cancer. 2010;17:351-360.
16. Washiro M, Ohtsuka M, Kimura F, Shimizu H, Yoshidome H, Sugimoto T, Seki N, Miyazaki M. Upregulation of topoisom-erase II alpha expression in advanced gallbladder carcinoma: a potential chemotherapeutic target. J Cancer Res Clin Oncol. 2008;134:793-801.
17. Asensio-Lopez MC, Lax A, Pascual-Figal DA, Valdes M, Sanchez-Mas J. Metformin protects against doxorubicin-in-duced cardiotoxicity: involvement of the adiponectin cardiac system. Free Radic Biol Med. 2011;51:1861-1871.
18. Zakikhani M, Blouin MJ, Piura E, Pollak MN. Metformin and rapamycin have distinct effects on the AKT pathway and pro-liferation in breast cancer cells. Breast Cancer Res Treat. 2010;123:271-279.
19. Onat H, Basaran M, Esassolak M, Bavbek SE, Anacak Y, Kaytan E, Altun M, Haydaroglu A. High-dose epirubicin and cisplatin in locally advanced undifferentiated nasopharyngeal carcinoma. Clin Oncol (R Coll Radiol). 2002;14:449-454.
20. Lissoni P, Barni S, Mandala M, Ardizzoia A, Paolorossi F, Vaghi M, Longarini R, Malugani F, Tancini G. Deccreased toxicity and increased efficacy of chemotherapy using the pi-neal hormone melatonin in metastatic solid tumour patients with poor clinical status. Eur J Cancer. 1999;35:1688-1692.
21. Lissoni P. Biochemotherapy with standard chemotherapies plus the pineal hormone melatonin in the treatment of advanced solid neoplasms. Pathol Biol (Paris). 2007;55:201-204.
22. Oz E, Erbas D, Surucu HS, Duzgun E. Prevention of doxoru-bicin-induced cardiotoxicity by melatonin. Mol Cell Biochem.2006;282:31-37.
Morphoproteomic-Guided Treatment in SNUC 53