anesthesia after renal transplant
TRANSCRIPT
ANESTHESIA AFTER RENAL TRANSPLANT
DR. DAVIS KURIAN
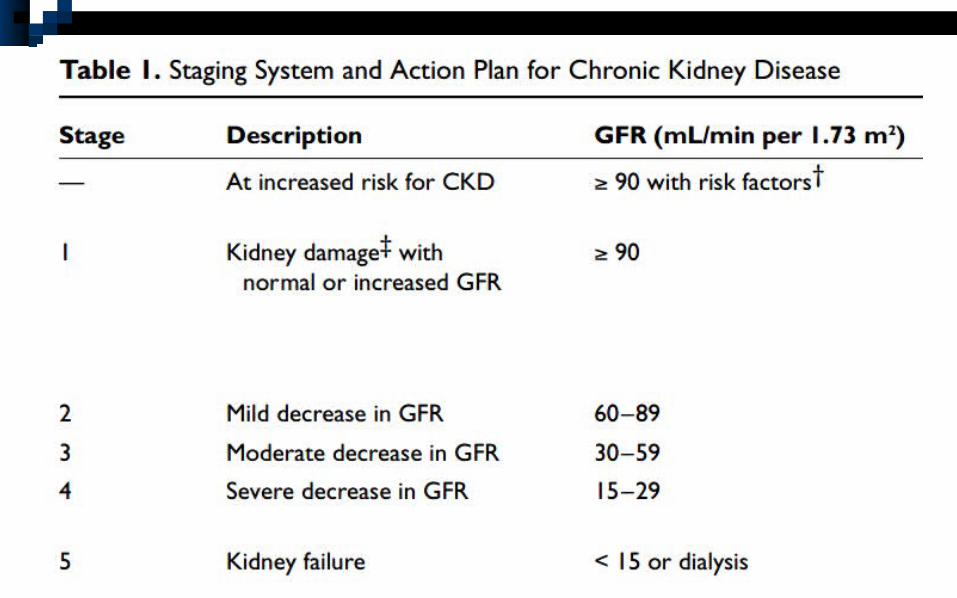
Most patients classified as National Kidney foundation – stage 2 or 3 CKD.
GFR deteriorates by 1.4-2.4ml/min/yr in recipients.
Pre operative workup very important.
CONCERNS Renal physiology and renal function.
Rejection – acute or chronic.
Pharmacotherapy.
Immunosupression.
PRE OP EVALUATIONThe level of renal function - RFTs – despite
normal creatinine, GFR is decreased.
Records of transplant – sought and examined for pre transplant functional status and post transplant.
Rejection – must be ruled out.
PRE OP EVALUATION Anemia, dysfunctional platelets –
coagulation parameters assessed.
Acid-base status – baseline ABG.
PRE OP EVALUATION Patients at increased risk of post
transplant malignancies, anemia, osteodystrophy.
Increased susceptibility to opportunistic and community acquired infections – CMV being the most common – if transfusion needed – CMV negative blood must be used in CMV negative pts
PRE OP EVALUATION Renal function impairment – can
predispose to electrolyte abnormalities, altered drug metabolism.
Dosage of all immunosuppressant medications – noted – patient instructed to continue in the peri-operative period.
PRE OP EVALUATION Assessment of complications of
immunosuppressant therapy - hyperglycemia and adrenal suppression
(steroids)hypertension, infection and renal insufficiency
(steroids, cyclosporine & tacrolimus), myelosuppression – anemia,
thrombocytopenia, leukopenia (azathioprine, sirolimus)
Cytokine release and fever (mistaken preop).
PRE OP EVALUATION
No need for increased antibiotics.Doppler study to assess blood flow to the graft.
PRE OP EVALUATION Careful cardiac evaluation –
CVS also affected in CKD Impact of underlying d/s – DM/HTN in the
pathogenesis of CKDPotential for drug regimens, transplantation
and rejection episodes to worsen CVS status.Metabolic syndrome – common in 1-6 yrs. IHD, CVA, PVD – significantly affect survival.
REJECTION
Hyperacute – rejection in minute to hrs – destruction of vascularity (preformed antibodies).
Acute – after 1 wk – antibodies – if no immunosuppressant therapy.
Chronic – in months to years.
SIGNS & SYMPTOMS OF REJECTION
Increased temp. Dec in urine output. Pain, tenderness, swollen graft. Increased BP. Sudden increase in weight or ankle
swelling. Elevated creatinine.
PRE OP EVALUATION Other co-morbidities Airway and spine examination. Blood workup – Hb, TC, PLC,
S.electrolytes, RFT, Blood sugars, ABG CXR, ECG. Doppler study.
PRE OP EVALUATION Patient instructed to
Continue all medications in the peri-operative period in the same dose.
Appropriate thromboprophylaxis in all transplant pateints.
All nephrotoxic drugs to be avoided.
INTRA OPERATIVERegional, local, GA.Sterile precautions to be followed.All nephrotoxic drugs to be avoided – as
patients have a low GFR.Serial monitoring of renal functions and
electrolytes with urine output whenever possible.
Very high risk for cardiovascular complications than general population.
INTRA OPERATIVE Renal transplant- adequate hydration -
BSS Difficult and edematous airway. Full stomach. Prolonged elimination half life of drugs
eliminated by kidneys
REGIONAL ANESTHESIA Epidural/spinal/CSE. Stable hemodynamics with epidural, post
op analgesia, risk for epidural hematoma. Chance of fluid overload – CVP and urine
output monitoring. Increased sensitivity to LA.
GENERAL ANESTHESIA Aspiration prophylaxis (esp emergencies).
Induction with low dose TPS/propofol (hypotension), not ketamine (worsen HTN)
Cis atracurium/atracurium – ms relaxant
GENERAL ANESTHESIA O2+N2O/air + iso/sevo/des maintenance
Opioid – fentanyl (preferred)
Ms relaxant action – monitored with PNS and reversal confirmed.
GENERAL ANESTHESIA CVP and urine output monitoring Avoid excess fluid. Serial monitoring of renal function,
electrolytes, blood glucose, acid-base status and urine output.
POST OPERATIVE Monitor renal functions and serum
electrolytes. Avoid nephrotoxic drugs – like NSAIDs,
COX – 2 inhibitors. Adequate antibiotic coverage to prevent
infections. Analgesia – epidural / fentanyl infusions.

THANK YOU