anatomy and physiology of cornea
TRANSCRIPT
ANATOMY AND PHYSIOLOGY OF CORNEA
DR.K.V.SUDHEER

The word cornea has come from “Kerato”. The term “Kerato” in greek means horn or shield like. Ancient Greek used to believe that cornea is derived from same material like that of thinly sliced horn of animal.

THE CORNEA
The cornea is a transparent avascular tissue with smooth, convex outer surface and concave inner surface, which resembles a small watch-glass.
To meet the diverse functional demands the cornea must be:- Transparent- Refract light- Contain the intraocular pressure- Provide a protective interface

DIMENSIONS
Microcornea:when HCD is less than 10mm Macrocorneawhen HCD is more than 13 mm
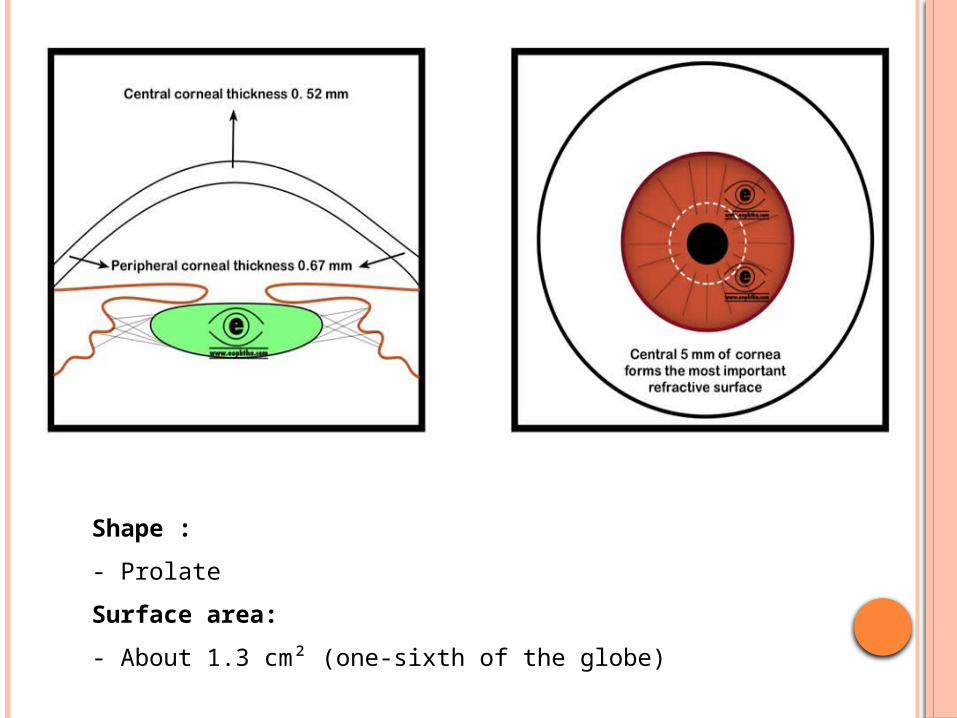
Shape :- ProlateSurface area:- About 1.3 cm² (one-sixth of the globe)
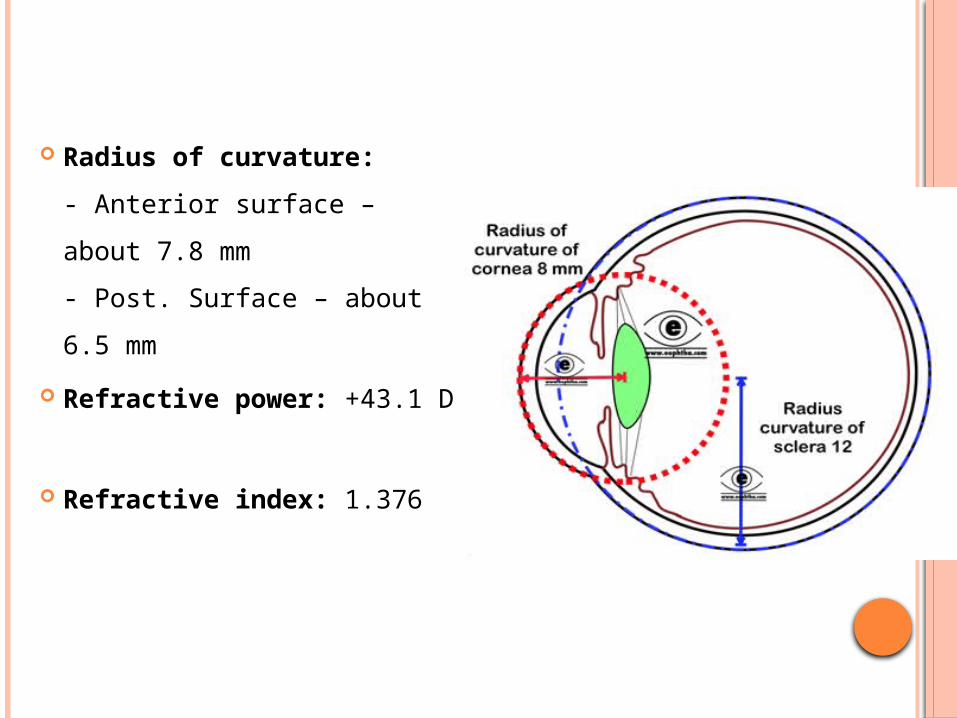
Radius of curvature:- Anterior surface – about 7.8 mm- Post. Surface – about 6.5 mm
Refractive power: +43.1 D
Refractive index: 1.376

COMPOSITION OF HUMAN CORNEA Water: 78 % Collagen: 15 %
of which: Type-I : 50-55 % Type-III : 1 % Type-IV : 8-10 % Type-VI : 25-30 %
Other protein: 5 % Keratan sulphate: 0.7 % Condroitin/dermatan sulphate: 0.3 % Hyaluronic acid: + Salts: 1 %

EMBRYONIC ORIGIN OF CORNEA:
Structure Derived from
Corneal epithelium Surface ectoderm
Stroma, Descmet’s membrane, endothelium
Paraxial mesoderm

STRUCTURE
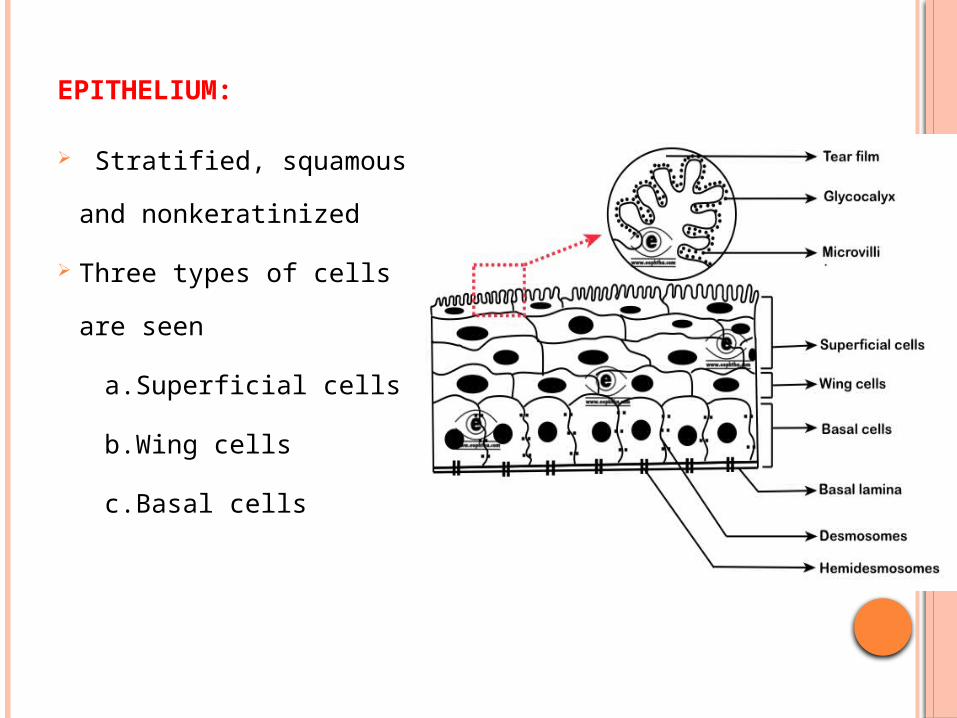
EPITHELIUM:
Stratified, squamous and nonkeratinized
Three types of cells are seen
a.Superficial cells b.Wing cells c.Basal cells
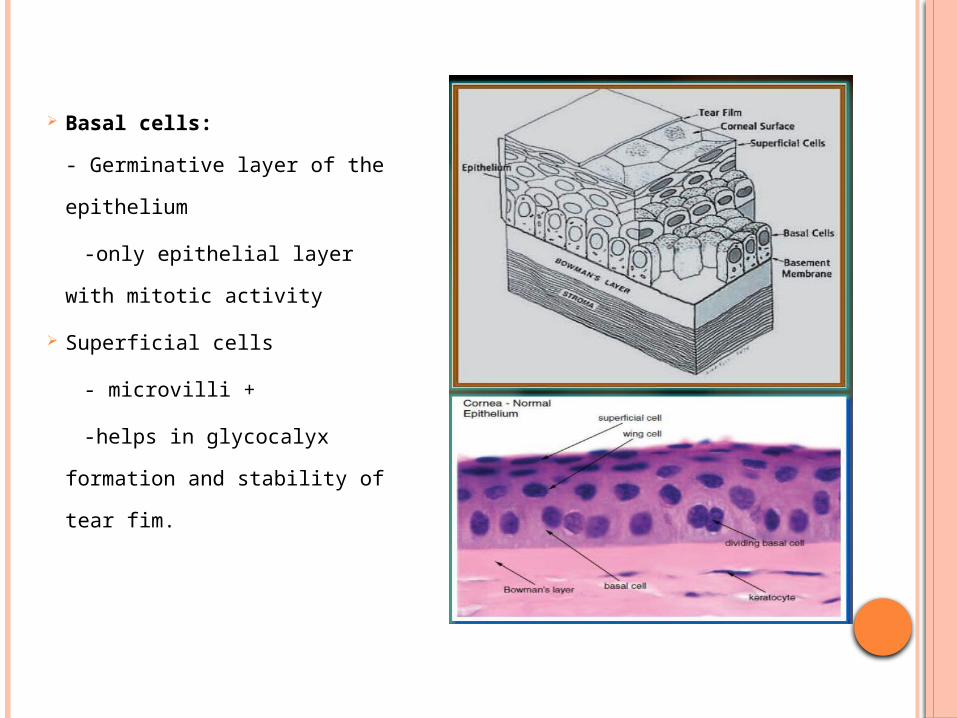
Basal cells:- Germinative layer of the epithelium
-only epithelial layer with mitotic activity
Superficial cells - microvilli + -helps in glycocalyx
formation and stability of tear fim.
- Adhesion is achieved by –desmosomes And hemidesmosomes
- Desmosomes are tight junctions between cells- Hemidesmosomes are tight junctions between cell
and basal lamina
- - Langerhans cells (cells of immune recognition system) present near periphery. They are almost absent at central cornea but aggregate in response to infection

Epithelial Turnover:
- Early studies suggested that the epithelium replaced
approximately weekly by division of basal cells and the
oldest shed from the surface
- It is now recognized that the germinative region lies at the
limbus, the stem cells, and cells migrate at a very slower
rate (123 µm/week) to the center of the cornea which may
be as long as a year
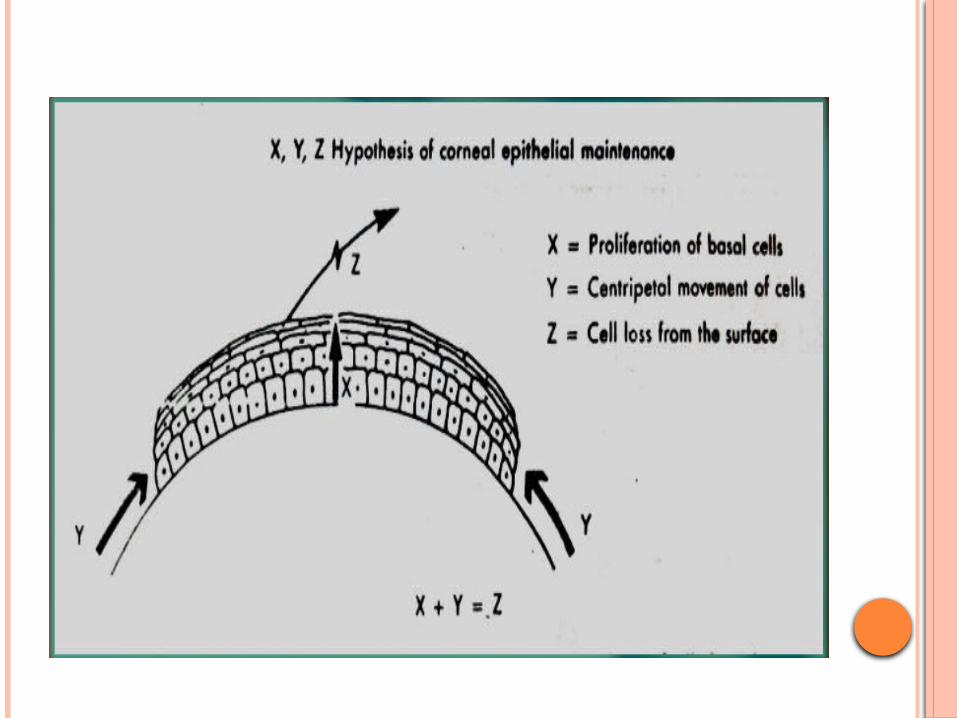
- The XYZ hypothesis:
1. Thoft R. and Friend J. (1983) proposed that both limbal basal and corneal basal cells are the source for corneal epithelial cells, and there is a balance among division, migration & shedding.

Epithelial Repair:
Repair of corneal epithelial injury like abration follows a distinctive sequence of events.
Injury (abration)
Cells at wound edge retract, thicken and lose attachment.
Travel in an amoeboid movement to cover the defect
Cells at wound edge ruffle and send out filopodia and
lamellipodia towards the center of wound

Migration process is halted by contact inhibition
They then anchor and
Mitosis resumes to re-establish epithelial thickness
Surface tight junctions re-establised
Adhesion with Bowman’s layer within 7 days (if basal lamina intact)
The healing process occurs rapidly, rate of cellmigration is 60 – 80 µm/hr
Bowman’s layer: (Ant. Limiting lamina)- Modified region of anterior stroma- Acellular homogeneous zone- 8 – 14 µm thick- It delineates the anterior junction between cornea and limbus
Compact arrangement of collagen gives it greatstrength and relatively resistant to trauma bothmechanical and infective.
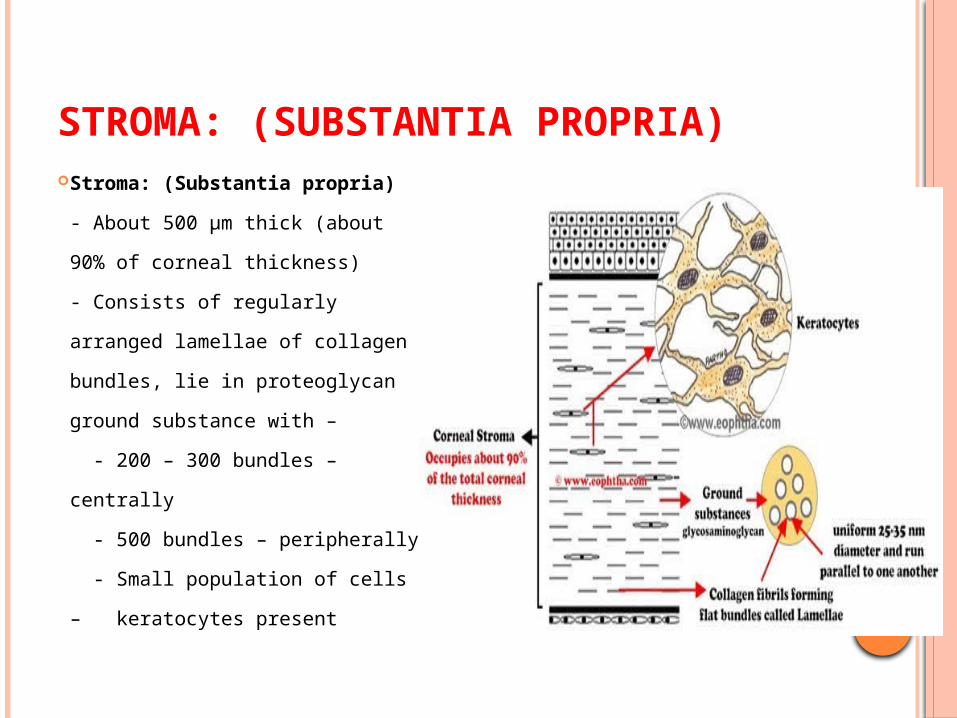
STROMA: (SUBSTANTIA PROPRIA) Stroma: (Substantia propria)
- About 500 µm thick (about 90% of corneal thickness)- Consists of regularly arranged lamellae of collagen bundles, lie in proteoglycan ground substance with – - 200 – 300 bundles – centrally - 500 bundles – peripherally - Small population of cells – keratocytes present
- Arrangement of lamellae –- Lamellae are arranged in layers, parallel with each other & with corneal surface- In deeper stroma the lamellae form strap-like ribbons which run approximately at right angles to those in consecutive layers- At the periphery this right-angular arrangement is slightly changed where it gets scleral fibres- At the limbus the bundles appeared to take a circular course
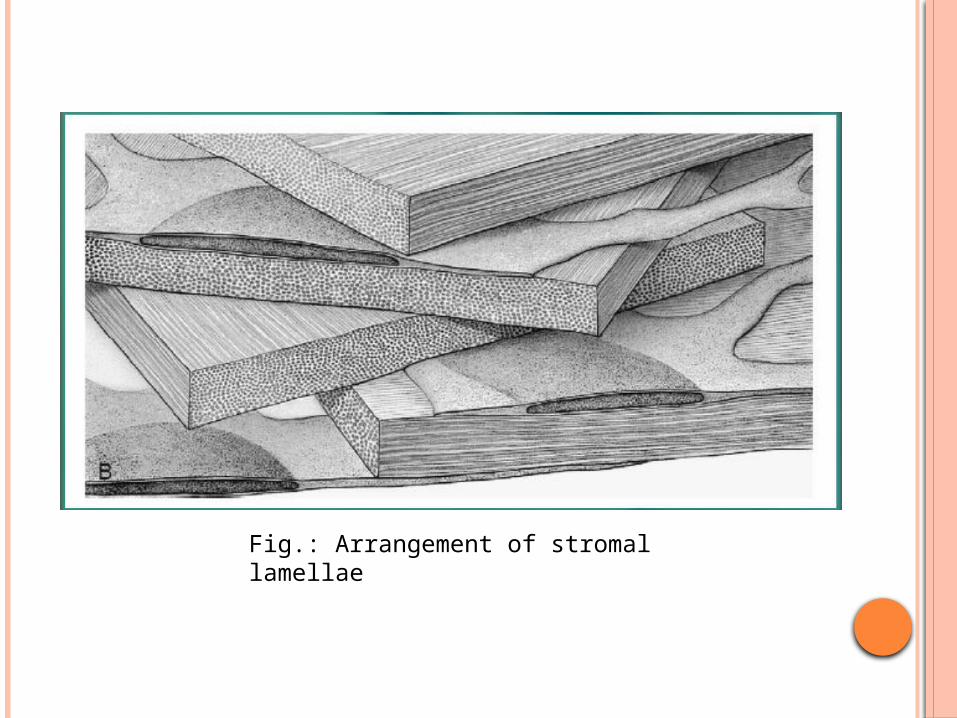
Fig.: Arrangement of stromal lamellae
Ultrastructural features:- Each lamellae comprises of a band of collgenfibrils arranged in parallel with each other- There is a unique uniformity of fibril diameter,it is 22 (±1) nm from ant. to post.- There is remarkable regularity of seperationboth within and between lamella
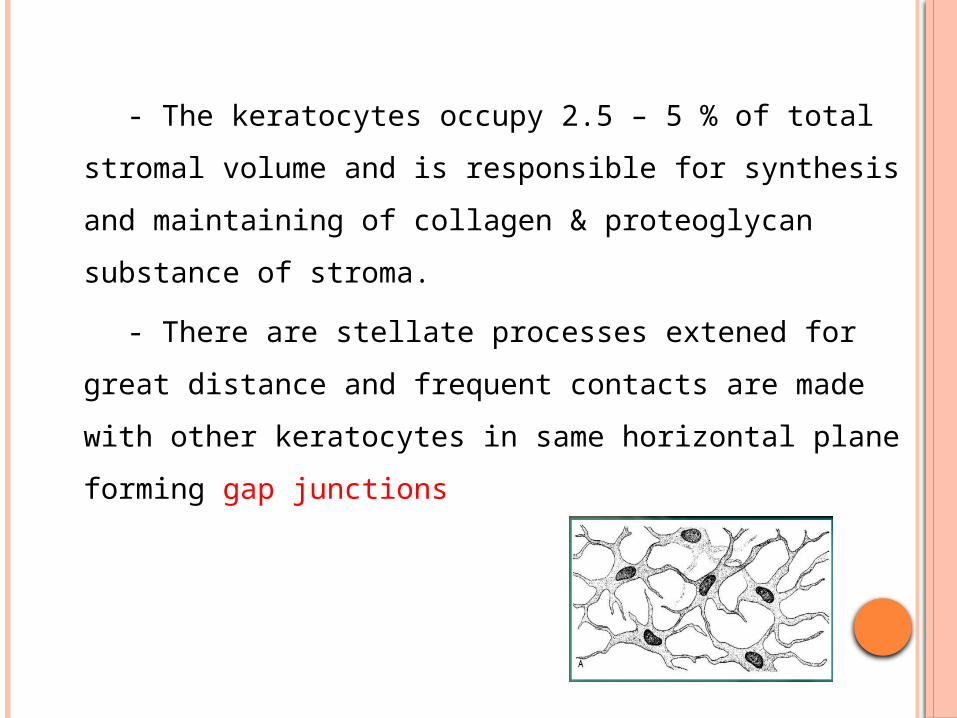
- The keratocytes occupy 2.5 – 5 % of totalstromal volume and is responsible for synthesisand maintaining of collagen & proteoglycansubstance of stroma.
- There are stellate processes extened for great distance and frequent contacts are made with other keratocytes in same horizontal plane forming gap junctions

Stromal repair:- Repair of stroma after small injuries involves: -
Keratocytes activation
Migration & transformation into fibroblasts
Production of scar tissue
Initial fibrils are large & irregular
Remodelling of scar tissue occurs, it ensues –1. Thinning of fibrils2. Reformation of lamellae over months3. Increase in transparency- Larger wounds provoke rapid vascular responseand leaving vascularised scar .
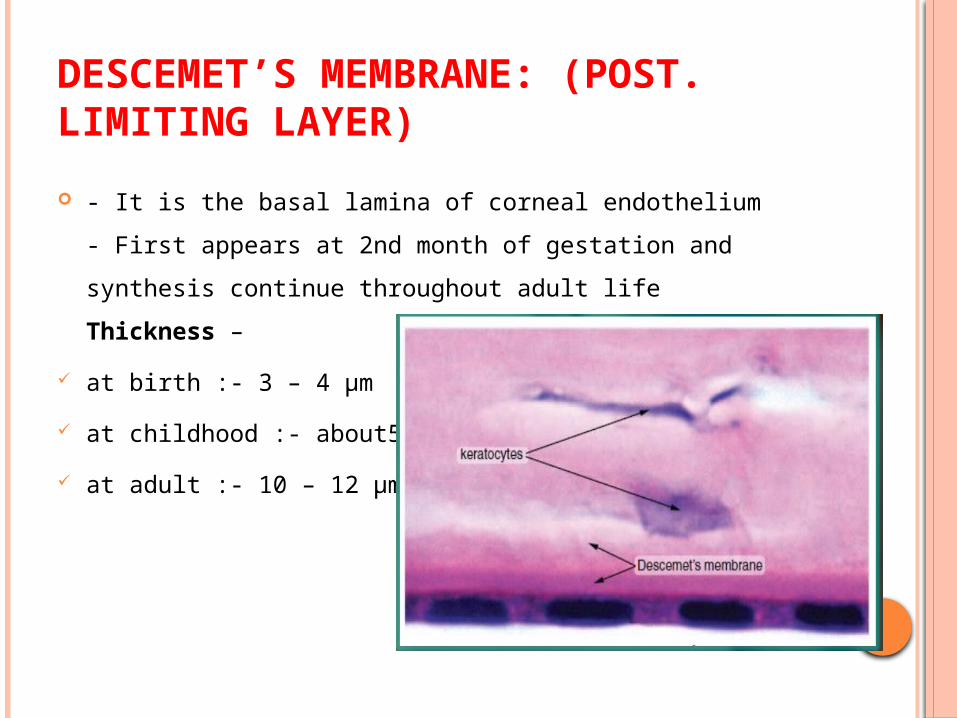
DESCEMET’S MEMBRANE: (POST. LIMITING LAYER) - It is the basal lamina of corneal endothelium
- First appears at 2nd month of gestation and synthesis continue throughout adult lifeThickness –
at birth :- 3 – 4 µm at childhood :- about5µm at adult :- 10 – 12 µm
- It is a strong resistant sheet- It thickens with age and in some cornealdegenerative conditions- Major protein of DM is Type IV collagen
Hassal-Henle bodies:- It is the peripheral posterior excrescence produced by focal overproduction of basal lamina like material in aging cornea- No clinical abnormality in corneal function

Schwalbe’s line:• The peripheral rim of DM is the internal landmark of corneal limbus and also it is the anterior limit of drainage angle, is called Schwalbe’ line
Posterior embryotoxon:Schwalbe’s line may hypertrophied in congenital anomalies and appears as visible shelf on gonioscopy, is called posterior embryotoxon
Repair of Descemet’s layer:
After traumatic interuption of DM (Path./Mech.)
Endothelium spread its cells to resurface the defect
Synthesis of fresh basal lamina
which is structurally identical to normal descemet’s layer
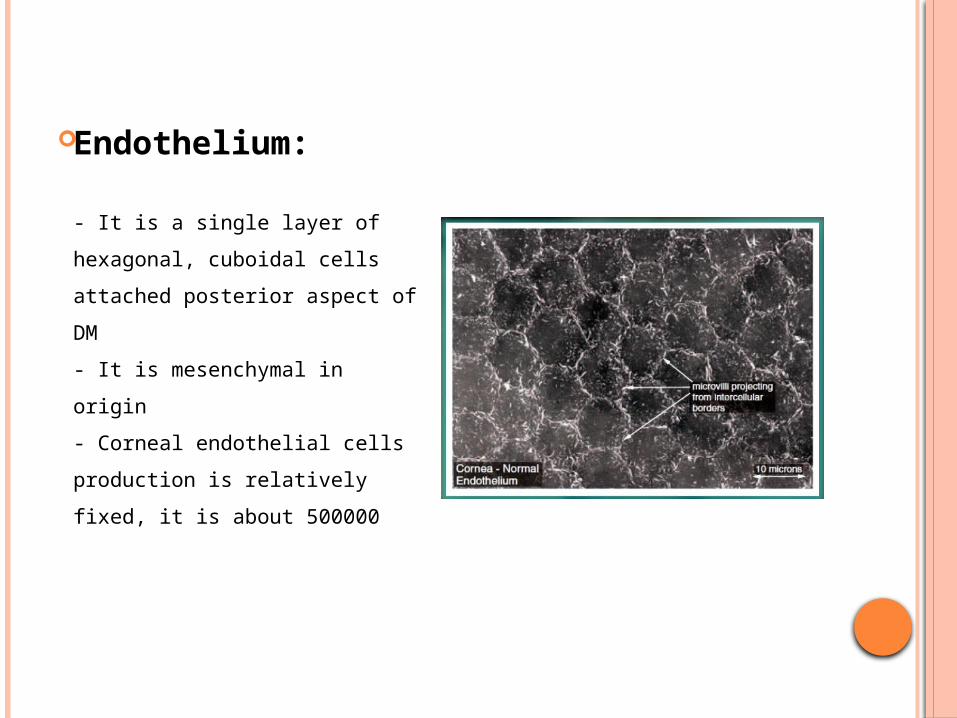
Endothelium:
- It is a single layer ofhexagonal, cuboidal cellsattached posterior aspect of DM- It is mesenchymal in origin- Corneal endothelial cellsproduction is relativelyfixed, it is about 500000
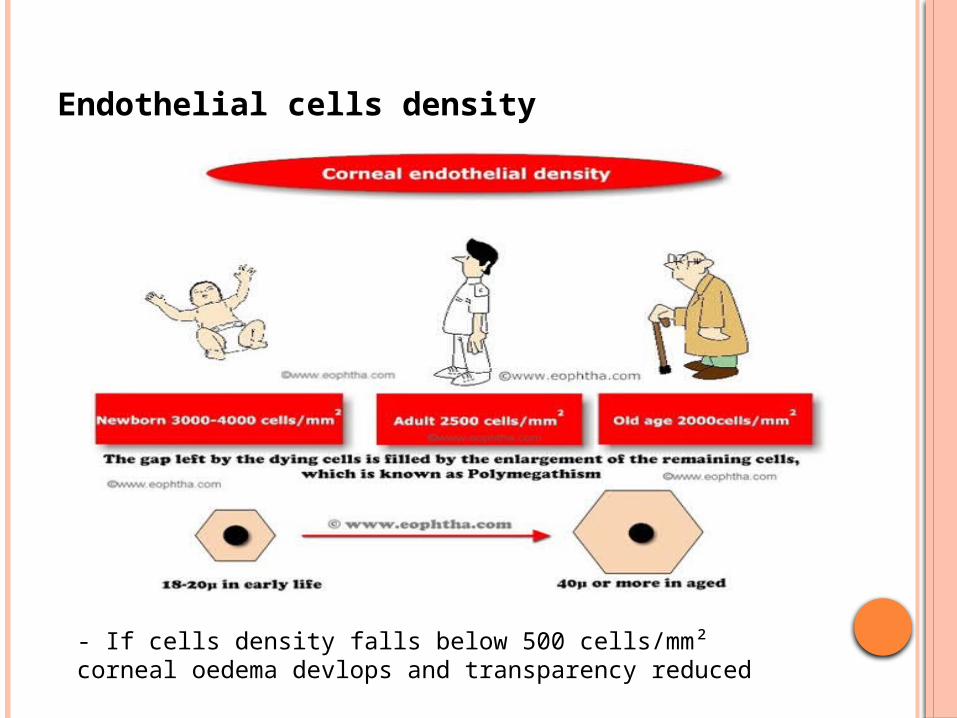
Endothelial cells density
- If cells density falls below 500 cells/mm² corneal oedema devlops and transparency reduced
Endothelium is rich in subcellular organeles –- large number of mitochondria, both rough and smooth endoplasmic reticulum, free ribozomes, these reflects that endothelium is extremely active metabolically
Nutrition to endothelium:- Endothelium gets its nutrition & O₂ from aqueous- Essential nutrients (such as glucose & amino acids) pass across its surface to supply the cellular needs of all the corneal layers
Endothelial Repair:- Physical & chemical damage to endothelium results in loss of cells- Neighboring cells move over to fill the gap by sliding process and enlargement of cells occur
(polymegathism)- Thus, after injury, the endothelial cell density falls, the cell area increases and the cell height decreases

LIMBAL STEM CELLS: Only 5% to 15% of the cells in the limbus are stem
cells The basal cells of limbal epithelium comprises the
limbal stem cells. They are the precursor for all other cells of the tissue They have a self maintaining population They accounts for only a small portion of total cells
of the tissue In vivo,they show slow cycling,but when placed in
cell culture,they demonstrate high potential to proliferate.
They can not be differentiated with rest of the cells of tissue.
BLOOD SUPPLY TO CORNEA:
In normal condition, cornea does not contain any blood vessels
Anterior ciliary artery, a branch ophthalmic artery forms a vascular arcade in the limbal region and helps in corneal metabolism and wound repair by providing nourishment.
Absence of blood vessel in cornea is one of the contributing factors for its transparency.
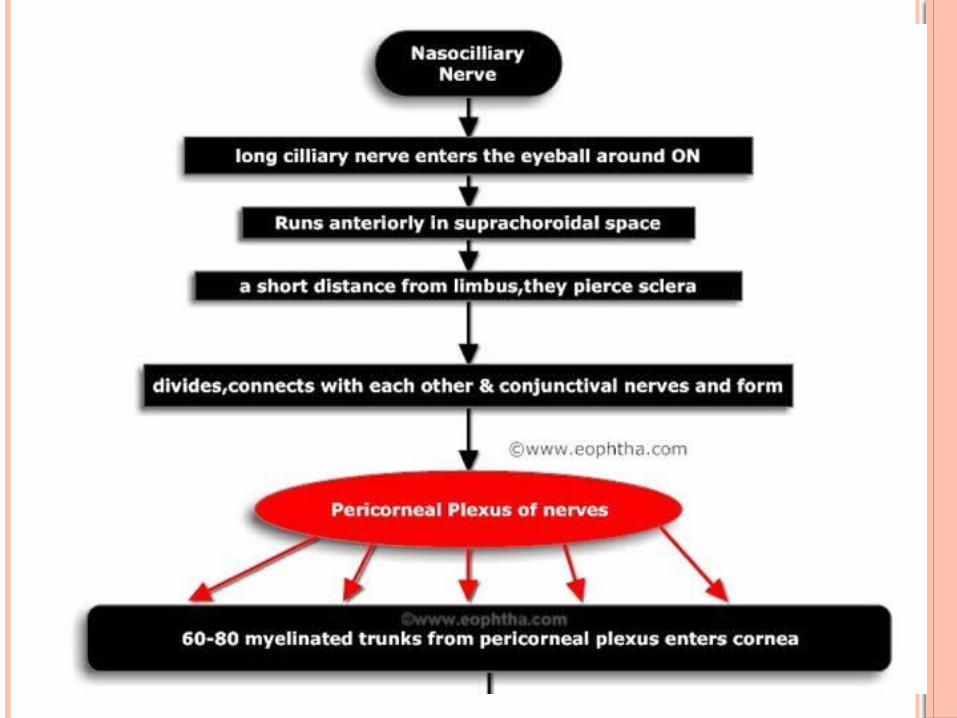
NERVE SUPPLY OF CORNEA:
Density of the nerve ending in cornea is about 300 times of that of skin.
The ophthalmic division of the trigeminal nerve has three parts: the frontal nerve, the lacrimal nerve, and the nasociliary nerve.
The nasociliary nerve provides sensory innervation to cornea.

CORNEAL NUTRITION & METABOLISM
Cornea requires energy for normal metabolicactivities as well as for maintainingtransparency and dehydration
Energy is generated by the breakdown ofglucose in the form of ATP
Most actively metabolizing layers areepithelium & endothelium
Sources of Nutrients:- Oxygen – mainly from atmosphere through tear film, with minor amounts supplied by the aqueous and limbal vasculature- Normal Po₂ in tears is 155 mm Hg- In aqueous is about 40 mm Hg- Minimum 25 mm Hg Po₂ is needed for maintaining deturgescent state and transparency

- Glucose, amino acid, vitamins, and other nutrients supplied to cornea by aqueous humor, a lesser amounts from tears or limbal vessels.- Glucose also derived from glycogen stores in corneal epithelium.- Epithelium consumes O₂ 10 times faster than stroma.
METABOLIC PATHWAYS: Three processes or pathways –
1. Pentose shunt (Hexose monophosphate shunt) – occurs both In hypoxic and normoxic condition forms NADPH and Pentose (Ribose 5-P) from glucose
which are used in nucleic acid synthesis2. Glycolysis (Embden meyerhof pathway) – Glucose/glycogen converted to pyruvate yelding 2 ATPs3. TCA or Krebs or citric acid cycle – in aerobic conditions pyruvate is oxidized to yield 36 ATP, water, CO₂.
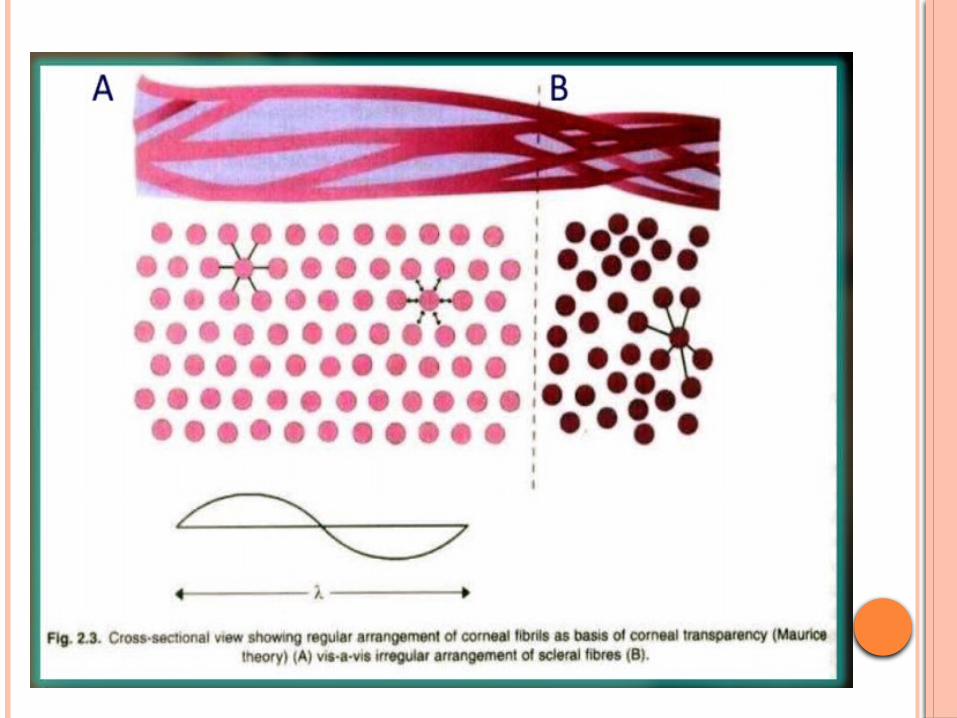
CORNEAL TRANSPARENCYThe cornea transmits nearly 100% of the lightthat enters it. Transparency achieved by –1. Arrangement of stromal lamellae
Two theories –i) Maurice (1957): The transparency of the stromais due to the lattice arrangement of collagen fibrils.He explained, because of their small diameter andregularity of separation, back scattered light wouldbe almost completely suppressed by destructiveinterference

ii) Goldman et al. (1968): Proposed that lattice arrangement is not a necessary factor for for stromal transparency . Cornea is transparent because fibrils are small in relation to light and do not interfere with light transmission unless they are larger than one half of a wavelenght of light(2000 A).
Both theories failed to explain why there is corneal clouding occurs with raised IOP and why there is corneal clearing occurs on reduction of IOP.
Other factors of corneal transparency –
2. Corneal epithelium & tear film• Epithelial non-keratinization• Regular & uniform arrangement of corneal epithelium• Junctions between cells & its compactness and alsotear film maintain a homogenicity of its refractive index
3. Relative deturgescence state of normal cornea.4. Corneal avascularity5. Non myelenated nerve fibres

FACTORS AFFECTING CORNEAL HYDRATION:i. Stromal swelling pressure exerted by GAGs IP = IOP – SP or IP = 17 -60 = -43ii. Barrier function of epithelium and endotheliumiii. Hydration controled by active pump mechanisms of
the corneal endothelium
The enzyme pump systems are –• Na⁺/K⁺ ATPase pump system• Bicarbnate dependent ATPase• Carbonic anhydrase enzyme• Na⁺/H⁺ pump
iv. Evaporation of water from corneal surfacev. Intraocular pressure
DRUG PERMEABILITY ACROSS THE CORNEA Factors affecting drug penetration through the
cornea are –1. Lipid and water solubility of the drug2. Molecular size, weight and concentration ofdrug3. Ionic form of the drug4. pH of the solution5. Tonicity of the solution6. Surface active agents7. Pro-drug form

1. LIPID AND WATER SOLUBILITY OF THE DRUG Drug should be amphipathic,should have
both lipid and wter soluble properties. Epithelium – lipophilic Stroma - hydrophilic

2. MOLECULAR SIZE, WEIGHT AND CONCENTRATION OF THE DRUG lipid soluble molecules can cross the corneal
epithelium irrespective of their molecular size,while water molecules with size less than 4A only canfilter through pores in cell membrane.
Substances with molecular weight less than 100 can pass &more than 500 can not.
3. IONIC FORM OF THE DRUG Capacity to exist in both ionic and non-ionic
forms,becaus only non-ionised drugs can penetrate epithelium and ionised drugs can pass through stroma.
Florescein dye test
4. PH OF THE SOLUTION Normal range – 4 to 10 Any solution outside this range increases
permeability.
5. TONICITY OF THE SOLUTION Hypotonic solutions increase permeability. Those below 0.9%NaCl.
6. SURFACE ACTIVE AGENTS Agents which reduce surface
tension,increase corneal wetting and ,therefore ,present more drug for absorption.
Eg.Benzalkonium chloride
7. PRO-DRUG FORM Pro-drug forms are lipophilic which after
absorption through epithelium converted into proper drug which can easily pass through stroma.
Eg. dipivefrine - epinephrine

THANK YOU