anal fissure: the facts (are there any?) tamzin cuming colorectal consultant homerton university...
TRANSCRIPT
Anal Fissure: the Facts
(Are there any?)Tamzin Cuming
Colorectal ConsultantHomerton University Hospital

Classic fissure in ano
90% posterior
< 6 weeks: acute
> 6 weeks + sentinel pile + visible sphincter
= chronic

When is a fissure not a fissure?
• Be suspicious • multiple or lateral– Crohn’s

?fissure
• Post-childbirth woman– ‘low-pressure fissure’– Anterior– Weak pelvic floor– rectocele
?fissure
• In an old person– Cancer: – anal cancer even– (esp if HIV+)
?fissure
• In someone with bad skin• Eczema, psoriasis, dermatitis
OK some facts
• 90% are the fissures you are thinking of– Young man– High pressure anus– Split is posterior • Because the blood supply is worst at the back• The pain is from anal spasm
Management
Acute Lignocaine, Fybogel and sympathy (90% cure)
Chronic
ALL THE TREATMENTS (except one) TREAT THE SPASM
and let the body heal the fissure

Anal spasm treatment I
• Give it nitrous oxide– GTN 0.4% >0.2% • 25% headache (cling film)
• Cure 60%1 Recurrence 50%2
– Diltiazem 2% • 15% pruritis• Cure: 75%3 RRecurrence 0.664
• Why not block the Ca2+ channels?– nifedipene top/oral
1 2006 Cochrane Review Nelson 2 DCR 2004;47:422-431 3Steele SR 2006 Aliment Pharm 4Sajid MS Colorectal Dis 2013

Anal Spasm treatment II
Paralyse it!
• At least Botox wears off
• Clinical conviction
• Less expensive than 5 years ago
Cochrane review• Healing rate variable: 75%• Recurrence rate 50% at 4 yrs• 10% temporary incontinence• No better than GTN 0.2%• More expensive than NO
(£77/pt)• Works for NO-resistant
Nelson 2012; NICE ESUOM14; Lindsey DCR 2004

Anal spasm treatmentCUT IT!
– Lateral anal (internal) sphincterotomy
– FINALLY! A CURE!
• 95%
– 5% up to 47% ‘mild’ incontinence• forever
No longer
• Posterior sphincterotomy: key-hole deformity
• Lord’s anal stretch

If all else fails
• Histology to exclude odd things plus DOSH• Advancement flap anoplasty– 48% cure with 0% incontinence– Also a treatment for low pressure fissures– recur if pelvic floor dysfunction not addressed
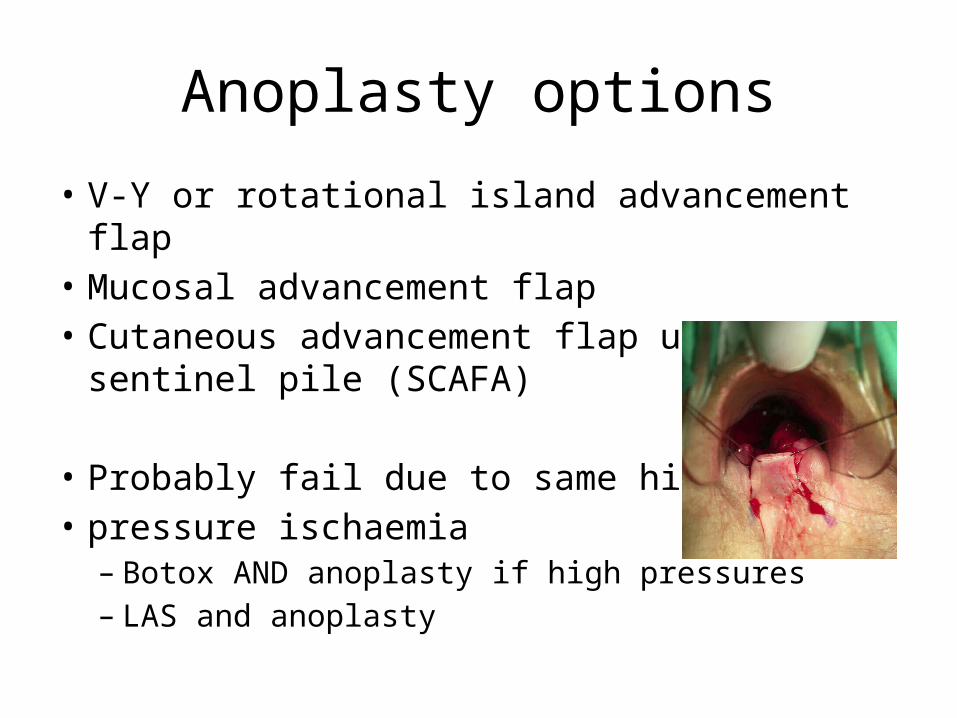
Anoplasty options
• V-Y or rotational island advancement flap• Mucosal advancement flap• Cutaneous advancement flap using sentinel pile
(SCAFA)
• Probably fail due to same high • pressure ischaemia– Botox AND anoplasty if high pressures– LAS and anoplasty

Conclusion
• If it’s not at the back in a young man: worry– (but you don’t need to do a PR)
• If it is:• Diltiazem is good• Botox is good• LAS short term good long term bad• and• Anoplasty can be good if desperate