anafylaksi - fokus på videre utredning - nsf 2008_anaphylaxis.pdf · "anafylaksi - fokus på...
TRANSCRIPT
""AnafylaksiAnafylaksi -- fokus pfokus påå videre videre utredning"utredning"
Anne Berit GuttormsenDepartment of Anaesthesia and Intensive Care,
Haukeland University Hospital and Section for Anaesthesiology and Intensive Care,
Department of Surgical Sciences, Medical Faculty, University of Bergen
• Anaphylaxis in the OR is rare
• What caused the reaction?
• The next procedure?
• Follow-up, documentation and communication
• Information should be put in the journal
IncidenceIncidence• 70 – 80 reactions per year in Norway – reported
to the Norwegian network
• ~ 40% of the patients have a full follow-up– Acute blood samples – Allergological follow-up
• Early diagnosis and correct treatment is mandatory to achieve an optimal result for the patient, i.e survival
AetiologyAetiology
• Allergy is common, but progression of an allergic reaction to a severe life-threatening condition is rare.
• Most common causes of the life-threatening reactions are drugs, stinging insects and food.
European Resuscitation council Guidelines for Resuscitation 2005
Early signsEarly signs• Urticaria
• Rhinitis
• Conjunctivitis
• Abdominal pain
• Vomiting and diarrhoea
• Flushing or pallor
European Resuscitation council Guidelines for Resuscitation 2005
Diagnosis is difficultDiagnosis is difficult• Due to
– Lack of consistent clinical information– A wide range of presentations
• Always exclude anaphylaxis as the cause of the reaction.– Misinterpretation might be fatal!
AnaphylaxisAnaphylaxis• An acute general
hypersensitivity reaction– That takes place seconds/minutes
after exposure with the drug/specimen in question
– The reaction involves one or more organ systems
– The symptoms vary• Often dramatic, potentially
lifethreatening– Several mechanisms
• IgE/Non IgE• Non allergic
Classification
• Grade 1: Symptoms from the skin, only
• Grade 2: Systemic, not lifethreatening
• Grade 3: Systemic, lifethreatening
• Grade 4: Asystoli/or respiratory arrest
• Grade 5: Death
Ring J, Messmer K. Lancet 1977
PatientsPatients
Patient 1 Male born 1972 (2006)
• He developed an itchy head, dizziness, facial oedema and hypotension 10-20 minutes after taking cough-syrup containing ethyl morphine.
• His wife suspected anaphylaxis and took him to hospital.
• On admission; BP was 84/58 mmHg, declining to 68/40 mmHg, and he still had the facial oedema.
• He was treated with adrenaline, i.v. fluids, steroids and antihistamines. He stabilized.
• Observed at the hospital for one night.
Patient 2 Male born 1935 (2005)
• (2005) Spinal anaesthesia, Bupivacaine with fentanyl. After 50 minutes; Urticaria, face, thorax lower part of abdomen and groins, itching sensation on his palms. A small decrease in blood pressure.
• TreatmentEphedrine 10 mg, antihistamine and steroids
• (2001) Had Corsodyl mouth rinse – after surgery in the mouth performed by the dentist. Five minutes after exposure his body felt “itchy and strange”
• He left the dentist office, went to his car, turned the switch, and 30 minutes later he woke up in the Emergency Department, at the local hospital
• He lost his drivers licence for 3 months because doctors thought he had a heart problem.
• Although the patient was convinced that the reaction was due to the mouth rinse.
Patient 3 Pregnant female born 1962 (2006)
19871987• Forceps delivery – performed without general
anaesthesia. She was stable during the procedure
• Cervical laceration – suture in general anaesthesia
• Induction of general anaesthesia– Fentanyl, Thiopenthone, Suxamethonium
• After induction she became cyanotic and hypotensive
• Treatment: Rapid infusion of dextran, iv ephedrine. Still low BP
• Reasons: Embolus to the lungs, amniotic fluid embolus, sepsis or allergy.
1990• Planned caesarean in general anaesthesia. She believes
that she will die during the procedure!
• Induction: Fentanyl, Thiopentone and suxamethonium.
• Reaction: BP dropped to 48 mm/Hg systolic. Vasoconstriction, bronchospasm, cyanosis, oedema in the face and the tongue.
• Treatment: Adrenaline 0,1 mg/ml in increments, Ephedrine in increments and steroids
No followNo follow--up up –– no warning card!no warning card!
Patient 4 Female born 1942 Breast cancer surgery (2005)
• Daycare surgery• Premedication; paracetamol and a NSAID• Induction; remifentanil and propofol, circulation stable.• Subcutaneous injection of Patent Blue (sentinal node)
• 20 minutes after induction; – BP cannot be measured, – Sinus rhythm on ECG– Read skin, but no urticaria, – No bronchospasm– Saturation 68-78% on FiO2 1.0. – 10 minutes with BP < 65 mmHg systolic
• The Emergency team was alarmed
•• TreatmentTreatment– Chest compressions– Intubation – Extra iv lines– Arterial line– Ephedrine and phenylephrine– Increments i.v with adrenaline, total 4 mg4 mg, , –– AdrenalineAdrenaline infusioninfusion 0,1 0,1 µµg/kg/min g/kg/min -- 0,02 0,02 µµg/kg/ming/kg/min
–– FluidsFluids
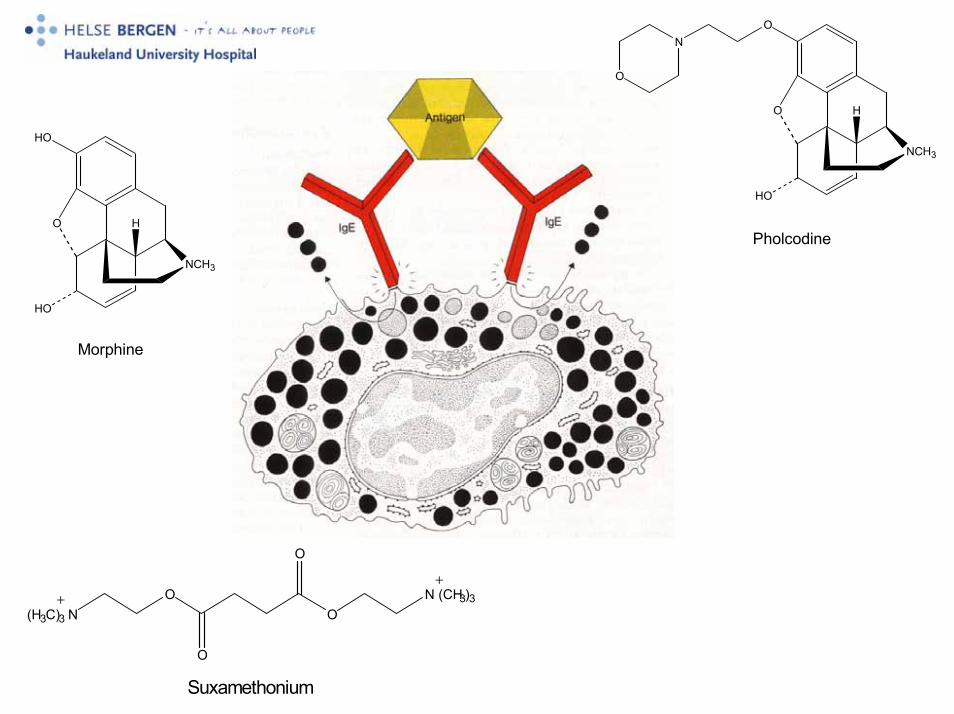
Follow-up• Patient 1 Patient drinking cough syrup
– He refused re-challenge - but the most probable cause to the reaction was ethyl-morphine –no other exposure
– He had antibodies towards morphine and pholcodine in serum
– Incremental challenge up to 5 mg showed tolerance to morphine.
• Patient 2 Patient with mouth rinse and spinal anaesthesia– IgE mediated reaction towards Chlorhexidine – specific IgE and
positive skin test.
– Chlorhexidine in the mouth rinse and in the disinfectant used towash the operation field
• Patient 3 Pregnant female
– Suxamethonuim – identified 19 years after the first reaction – her GP referred her
• Patient 4 Patient with breast cancer
– Patent blue

Urticaria in a patient with a suspected reaction on patent blue
Challenges
• Early diagnosis
• Early and adequate treatment– Adrenaline and fluids are the cornerstones in treatment
Key to success
• Identify risk patients
– Patients who have suffered severe
anaphylaxis
• A standardized follow-up to identify the
cause of anaphylaxis in risk patients
There was a complete match between the suspected cause and the result of follow-up in only 7% of the cases
FollowFollow--upup• Blood sampling
– sTryptase– Total IgE– Specific IgEs
• Three samples from each patient
• Secondary follow-up
”Anaphylaxis kit”
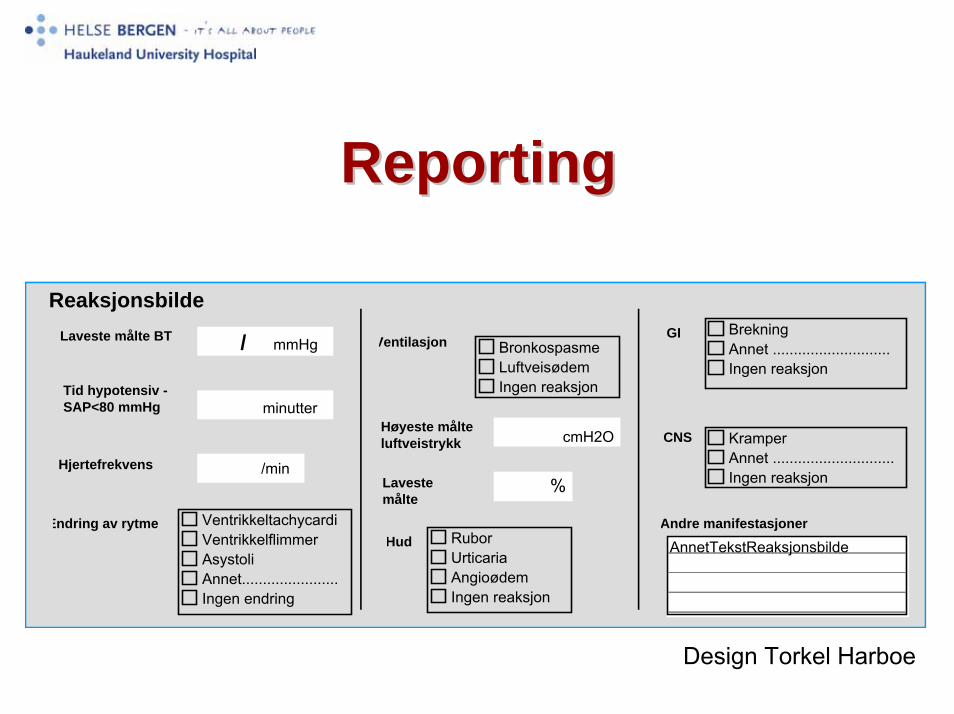
ReportingReporting
HudVentrikkeltachycardiVentrikkelflimmerAsystoliAnnet.......................Ingen endring
Endring av rytme
BronkospasmeLuftveisødemIngen reaksjon
Ventilasjon
KramperAnnet .............................Ingen reaksjon
CNS
BrekningAnnet ............................Ingen reaksjon
GI
Andre manifestasjoner
AnnetTekstReaksjonsbilde
Reaksjonsbilde
Høyeste målteluftveistrykk
Laveste målte BT
Tid hypotensiv -SAP<80 mmHg
HjertefrekvensLavestemålte
RuborUrticariaAngioødemIngen reaksjon
/ mmHg
minutter
/min
cmH2O
%
Design Torkel Harboe
That most drugs given during induction and maintenance of anaesthesia have cardiodepressive effects.
Hypotension and tachycardia are rather common
Overtriage!
That most drugs given during induction and maintenance of anaesthesia have cardiodepressive effects.
Hypotension and tachycardia are rather common
Overtriage!
The problem isThe problem is
OO
O
O
N (CH3)3(H3C)3 N
++
Suxamethonium
O
NCH3
H
O
HO
N
O
PholcodineO
NCH3
H
HO
HO
Morphine
sTryptasesTryptase --ImmunoCapImmunoCap• Measures continously released inactive
proformes (monomers) and active forms of α-and β-tryptase.
• Cannot differentiate between tryptase released from the mastcell or the basophil – Mastcell 10-35 pg tryptase/cell– Basophil ~ 0,04 pg tryptase/cell
• The proforms mirrors the number of mastcells • Represents the basal level • Elevated in mastocytosis
sTryptasesTryptase -- ImmunoCapImmunoCap• Mature β-tryptase, a serin-protease (tetramer)
– Stored in granulas of the resting mastcell– Released to the circulation during activation of the
mast cell
– Increased levels after iv stimuli and IgE mediated reactions
– A peak after 15- 120 min, half-life 2 h– After 24-28 h basal level is reached
60
0
10
20
30
40
50
Time (h)
Tryp
tase
(U/L
)
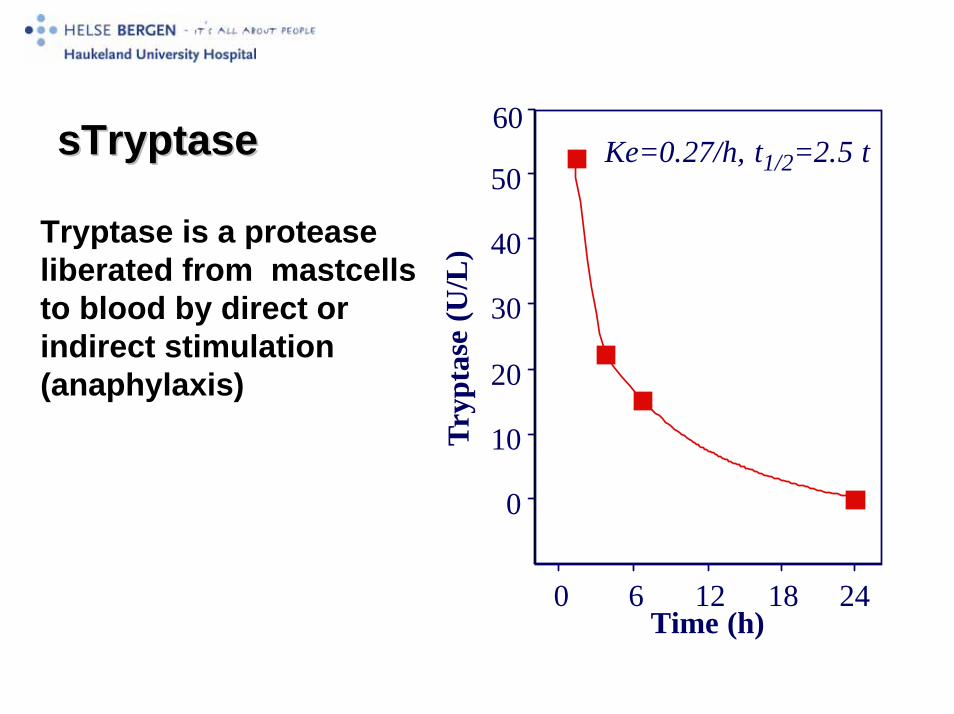
Ke=0.27/h, t1/2=2.5 t
2460 12 18
sTryptasesTryptase
Tryptase is a protease liberated from mastcellsto blood by direct or indirect stimulation (anaphylaxis)
SS--tryptase (MCT) tryptase (MCT) Sensitivity ~95%. Specificity ~70% (Fisher, Baldo,
BJA 1998)
33 of 158 patients with elevated MCT did not have specific IgE
7 of 143 patients with specific IgE did not have elevated s-tryptase
“Elevation of MCT favours aIgE-mediated cause.”
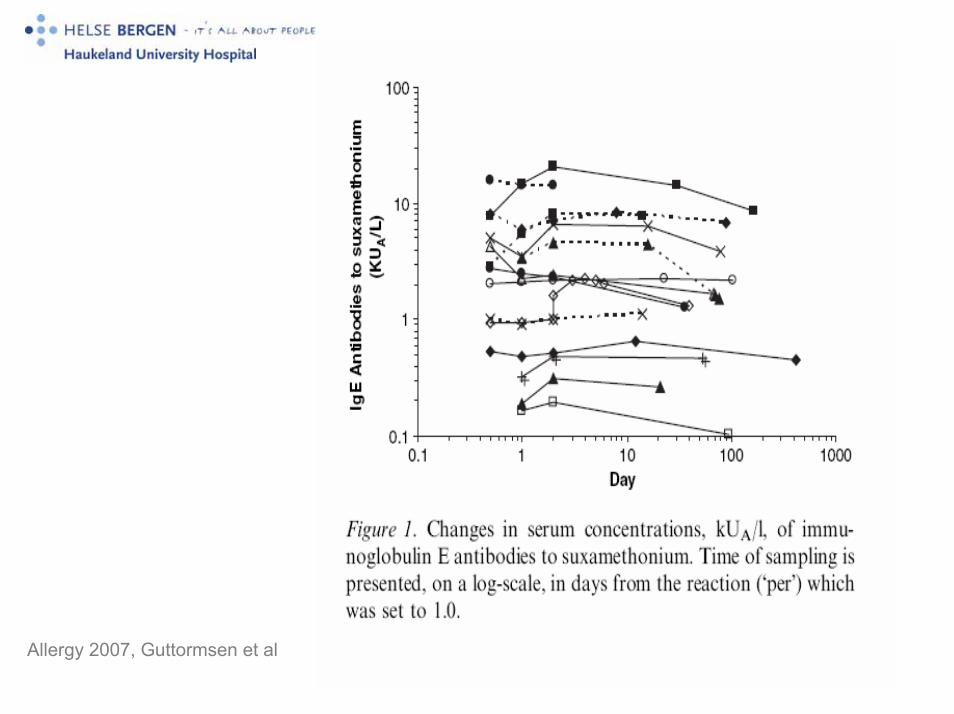
Allergy 2007, Guttormsen et al
ConclusionsConclusions• In anaphylaxis induced by NMBA in NMBA-IgE-
sensitized individuals there is a small decrease of serum IgE antibodies to suxamethonium.
• None of the patients became sero negative.
• There is no reason to doubt that these findings do not apply to other drugs.
• Serum IgE antibody levels in many patients seem to decrease over time
• New blood sampling at allergy work-up.
• Still to be elucidated– If the prick test is reliable in the immediate time frame
after an adverse drug reaction as antibody detection is only available for a limited number of drugs
• Thus, a serum sample for analyses of IgEantibodies to QAI can be drawn right after the anaphylactic reaction
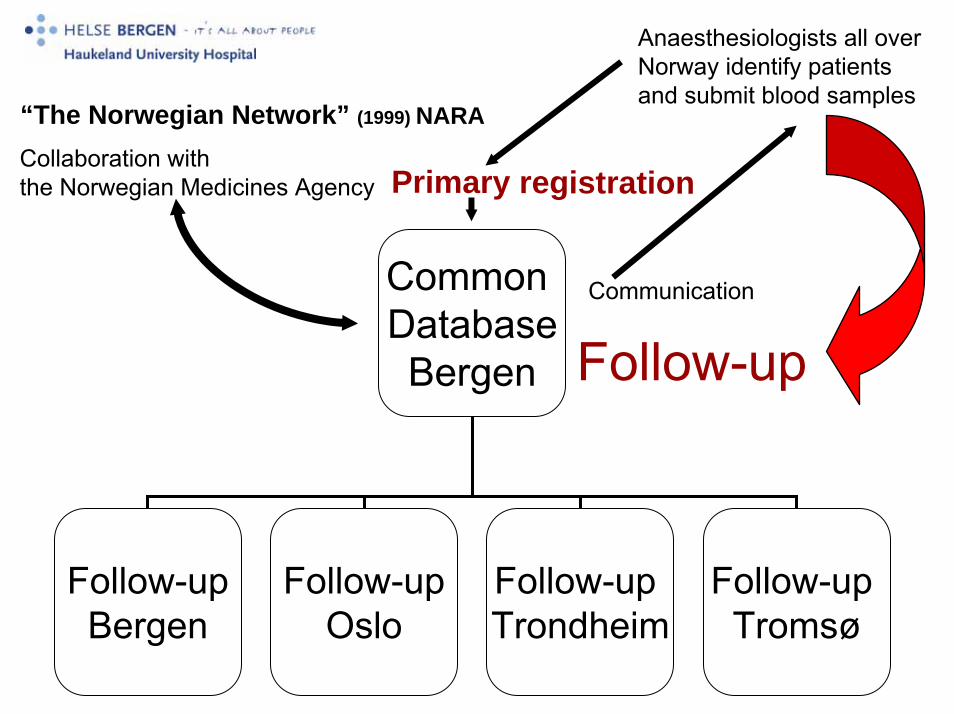
Common DatabaseBergen
Follow-upBergen
Follow-upOslo
Follow-up Trondheim
Follow-up Tromsø
Communication
Follow-up
“The Norwegian Network” (1999) NARA
Collaboration withthe Norwegian Medicines Agency Primary registration
Anaesthesiologists all over Norway identify patientsand submit blood samples

1.1.
Skin-prick testSkin-prick test
2.2.
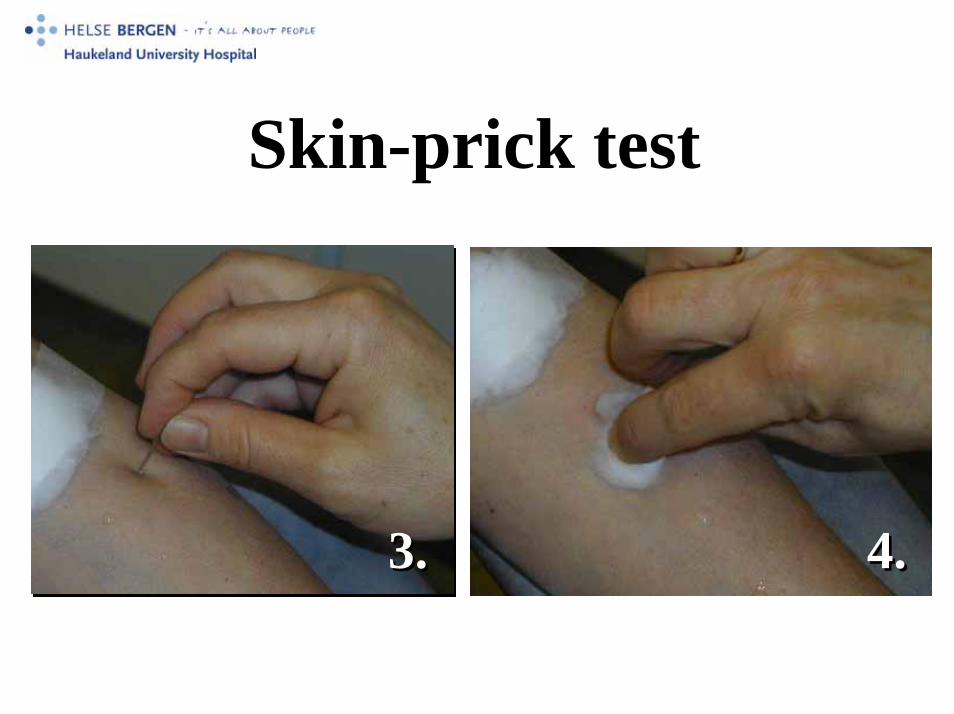
Skin-prick testSkin-prick test
3.3. 4.4.

(D+d)/2 >3mm
Positive skin prick test = immunological reaction
D
d
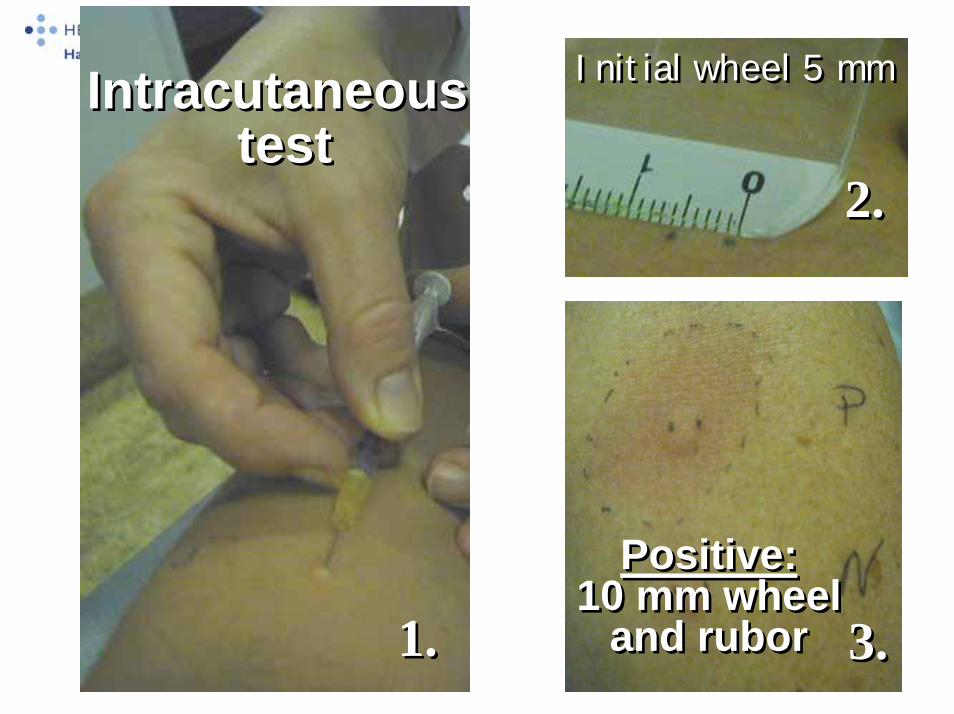
1.1.
Intracutaneoustest
Intracutaneoustest
2.2.
Initial wheel 5 mmInitial wheel 5 mm
3.3.
Positive:10 mm wheel
and rubor
Positive:10 mm wheel
and rubor
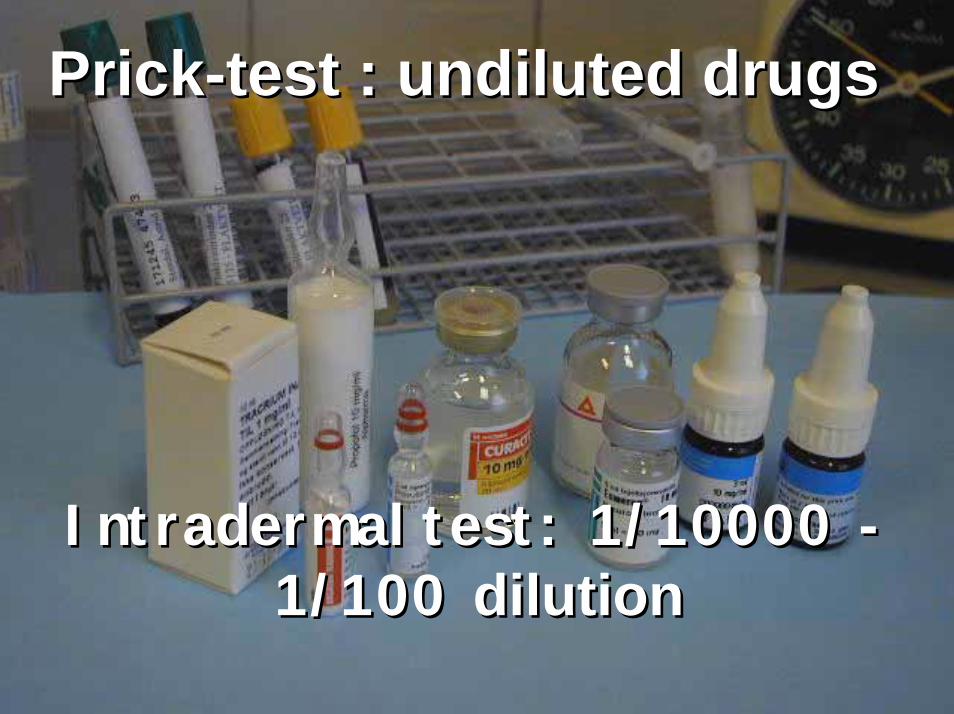
Prick-test : undiluted drugsPrick-test : undiluted drugs
Intradermal test: 1/10000 -1/100 dilution
Intradermal test: 1/10000 -1/100 dilution
AnafylaksiAnafylaksi under anestesiunder anestesiKommunikasjon av kritisk informasjon internt i Kommunikasjon av kritisk informasjon internt i
sykehus og mellom sykehussykehus og mellom sykehus
Anne Berit Anne Berit GuttormsenGuttormsen, KSK, Haukeland Universitetssykehus, KSK, Haukeland UniversitetssykehusNils Oddvar Skaga, UllevNils Oddvar Skaga, Ullevåål Universitetssykehusl Universitetssykehus
PasienteksempelPasienteksempel• Kvinne 38 år. Innlegges med en penetrerende skade i buken.
Agitasjon og motorisk uro - umulig å undersøke
• ”Tåler du narkose – nei jeg tåler ikke narkose – jeg blir kvalm”
• ”Rapid Sequence Induction” gjennomføres med KetalarKetalar 200 mg, 200 mg, StesolidStesolid 5 mg , 5 mg , FentanylFentanyl 0,1 mg og 0,1 mg og CuracitCuracit 100mg100mg, intuberes
• Alvorlig anafylaktisk sjokk med bronkospasmebronkospasme, hypotensjonhypotensjon og cyanosecyanose. Rask diagnose, korrekt behandling.
• Dokumentert i kritisk informasjon – To alvorlige anafylaktiske sjokk – Utredning har vist allergi mot CuracitCuracit, ,
NorcuronNorcuron, , EsmeronEsmeron– Toleranse for Nimbex (ikke original dokumentasjon)
• Opplysningene ble ikke kommunisert til anestesilege
• Tiltak: – Traumeteamet blir varslet dersom koordinator
ser at "kritisk info" foreligger i journalen når den åpnes.
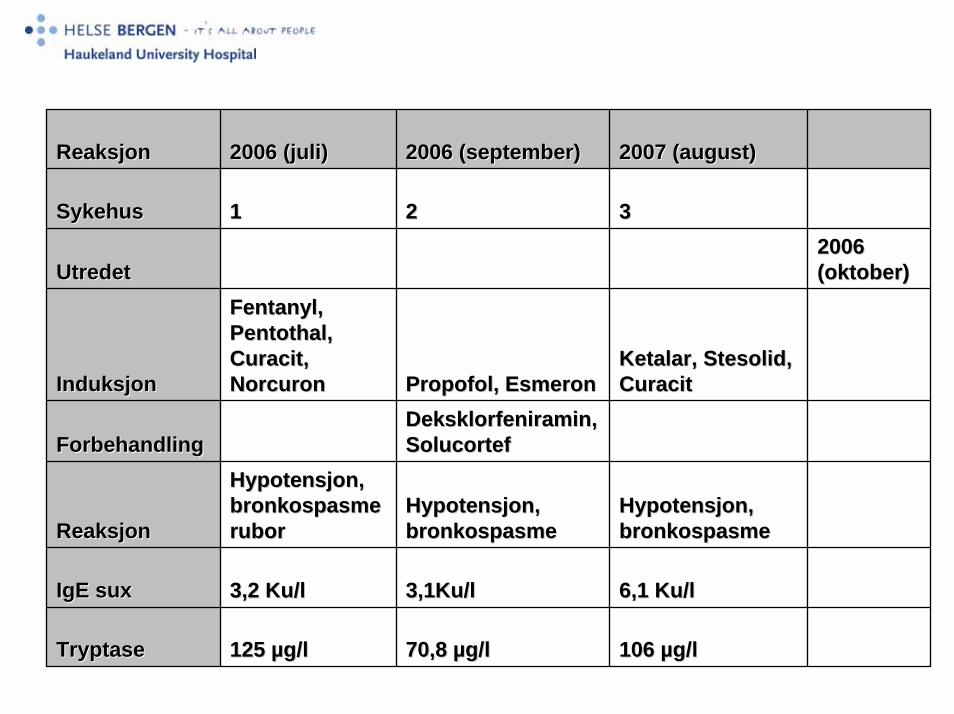
ReaksjonReaksjon 2006 (juli)2006 (juli) 2006 (september)2006 (september) 2007 (august)2007 (august)
SykehusSykehus 11 22 33
UtredetUtredet2006 2006 (oktober)(oktober)
InduksjonInduksjon
Fentanyl, Fentanyl, Pentothal, Pentothal, Curacit, Curacit, NorcuronNorcuron Propofol, EsmeronPropofol, Esmeron
Ketalar, Stesolid, Ketalar, Stesolid, CuracitCuracit
ForbehandlingForbehandlingDeksklorfeniramin, Deksklorfeniramin, SolucortefSolucortef
ReaksjonReaksjon
Hypotensjon, Hypotensjon, bronkospasmebronkospasmeruborrubor
Hypotensjon, Hypotensjon, bronkospasmebronkospasme
Hypotensjon, Hypotensjon, bronkospasmebronkospasme
IgE suxIgE sux 3,2 Ku/l3,2 Ku/l 3,1Ku/l3,1Ku/l 6,1 Ku/l6,1 Ku/l
TryptaseTryptase 125 125 µµg/lg/l 70,8 70,8 µµg/lg/l 106 106 µµg/lg/l

How do we become better?• To train
– Patients– Relatives– Paramedics– Nurses– Doctors
• Anaphylaxis drill among hospital employees
• Focus on– How to recognize anaphylaxis?– How to treat – appropriate doses and correct
administration of adrenaline – How to prevent new anaphylactic episodes – to
perform follow-up
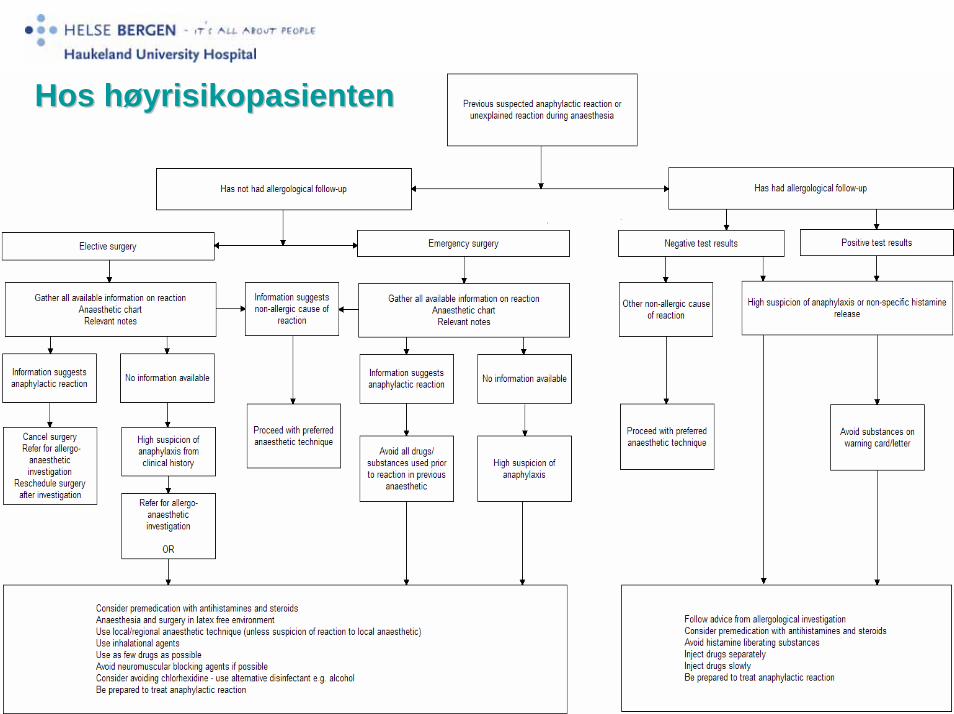
Hos hHos høøyrisikopasientenyrisikopasienten
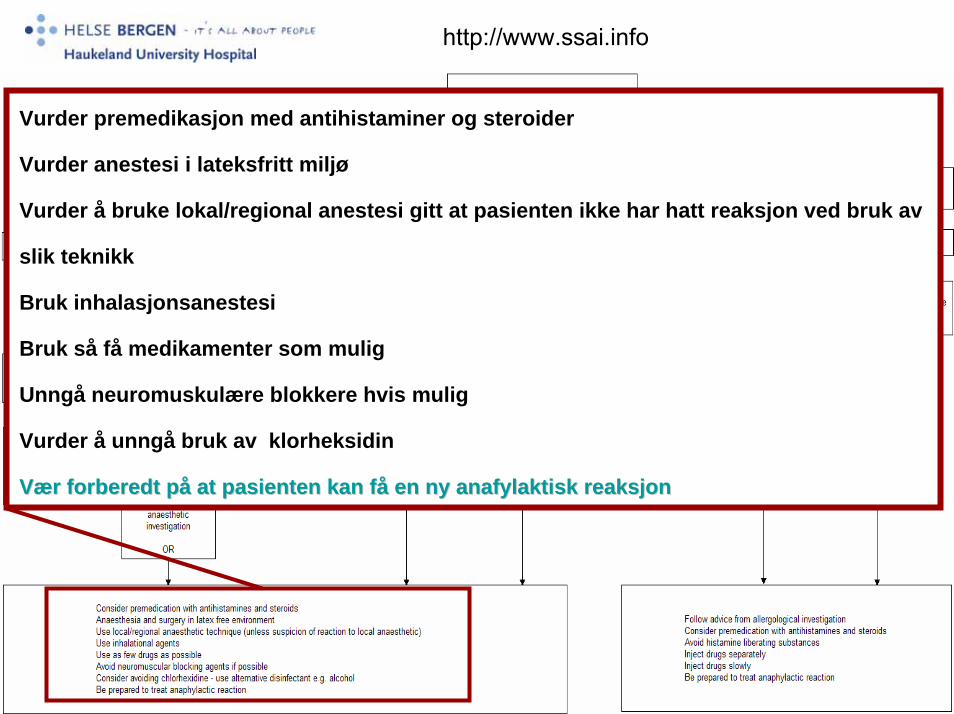
http://www.ssai.info
Vurder premedikasjon med antihistaminer og steroider
Vurder anestesi i lateksfritt miljø
Vurder å bruke lokal/regional anestesi gitt at pasienten ikke har hatt reaksjon ved bruk av
slik teknikk
Bruk inhalasjonsanestesi
Bruk så få medikamenter som mulig
Unngå neuromuskulære blokkere hvis mulig
Vurder å unngå bruk av klorheksidin
VVæærr forberedtforberedt ppåå at at pasientenpasienten kankan ffåå en en nyny anafylaktiskanafylaktisk reaksjonreaksjon
• Be AAlert• Be AAggressive in your approach• To give AAdrenaline and Fluids• Perform Follow-up