an intervention to improve antibiotic prescribing habits of doctors in a teaching hospital
DESCRIPTION
An Intervention To Improve Antibiotic Prescribing Habits of Doctors in a Teaching Hospital. Ofei F, Forson A, Tetteh R, Ofori-Adjei D University of Ghana Medical School, Korle-Bu Teaching Hospital and Noguchi Memorial Institute for Medical Research, Accra, Ghana. ABSTRACT. - PowerPoint PPT PresentationTRANSCRIPT
An Intervention To Improve Antibiotic Prescribing Habits of Doctors in a Teaching Hospital
Ofei F, Forson A, Tetteh R, Ofori-Adjei D University of Ghana Medical School, Korle-Bu Teaching Hospital and Noguchi Memorial Institute for Medical Research, Accra, Ghana.
ABSTRACT Problem Statement: Inappropriate prescribing of antibiotics by doctors is common.
Hospital consultants are role models in the clinical arena. It is expected that solutions they generate to this problem will be better adhered to by the junior doctors they mentor.
Objectives: To assess the effect of a managerial and educational intervention selected by hospital consultants for the treatment of Lower Respiratory Tract Infection (LRTI) on the antibiotic prescribing habits of house officers.
Design: A baseline 6-month prospective review of antibiotic prescribing by house officers for community-acquired LRTI for in-patients, followed by a controlled intervention involving three consecutive batches of house officers at the beginning of their house job.
Setting: Two 1500-bed teaching hospitals (study and control groups) Study Population: Review of clinical notes and prescriptions of all in-patient cases
admitted to medical wards at study and control sites with community- acquired LRTI. Intervention: Use results of a baseline data collected to prepare guidelines for house
officers, in collaboration with their consultants, on the treatment of common medical emergencies including LRTI. Introduction of the guidelines accompanied by talks and discussions on the rational use of antibiotics at the start of each housemanship rotation.
Outcome measures: Appropriateness of antibiotic prescribing - number of drugs per prescription, % antibiotics, % generics, % on the National Essential Drugs List (EDL), % non-guideline drugs and final patient outcomes.
Results: The intervention did not result in change in prescribing behaviour of junior doctors. Prescribing drugs on the EDL and by generics, already low at the study site at baseline compared with control, deteriorated for all drugs as well as antibiotics in the study but not the control group. Paradoxically, patient outcomes improved compared with baseline data.
Conclusions: Other factors influencing the prescribing behaviour of junior doctors, especially the role of Drugs and Therapeutics Committees (DTCs) and Pharmaceutical Company representatives, need to be carefully studied.
Study funding by WHO/EDM and ARCH project Ethical Approval: Protocol and Ethics Committee, University of Ghana Medical School
Introduction/Background
The selection of clinically inappropriate and expensive antibiotics by doctors in the treatment of infections result in a higher cost of medication for the patient, the hospital and the Health Ministry and may cause increased patient morbidity and mortality.
Medical consultants in university teaching hospitals greatly influence the prescribing habits of junior doctors, especially newly qualified house officers.
Getting consultants to generate the solutions to the problem of inappropriate antibiotic prescribing themselves, may make them more likely to adhere to the prescribed intervention and ensure that the junior doctors they mentor do the same.
Study and Control sites are 1500-bed teaching hospitals in two different cities in Ghana

Objectives
Promote appropriate antibiotic prescribing behaviour in house officers through a managerial and educational intervention generated by the contribution and participation of consultants.
Specific Objectives
1. Establish the magnitude of inappropriate prescribing practice with respect to the treatment of community-acquired lower respiratory tract infections (LRTI).
2. Implement an intervention proposed by consultants to correct house officers’ prescribing of inappropriate antibiotics in the treatment of community-acquired LRTI.
3. To evaluate the effect of the intervention (guidelines, education and feedback) on the appropriateness of antibiotic prescribing by house officers.
Methods
Prospective controlled time –series intervention study in two teaching hospitals, one acting as the study site and the other as control
6-month baseline prospective study of antibiotic prescribing by doctors for community-acquired lower respiratory tract infection (LRTI)
Discussion of results with consultants and junior doctors and development of intervention (treatment guidelines for community-acquired LRTI) with the help of consultants
Pilot testing of intervention Subsequently
6-month prospective data collection of antibiotic prescribing among 3 consecutive batches of house officers
Final dissemination of results
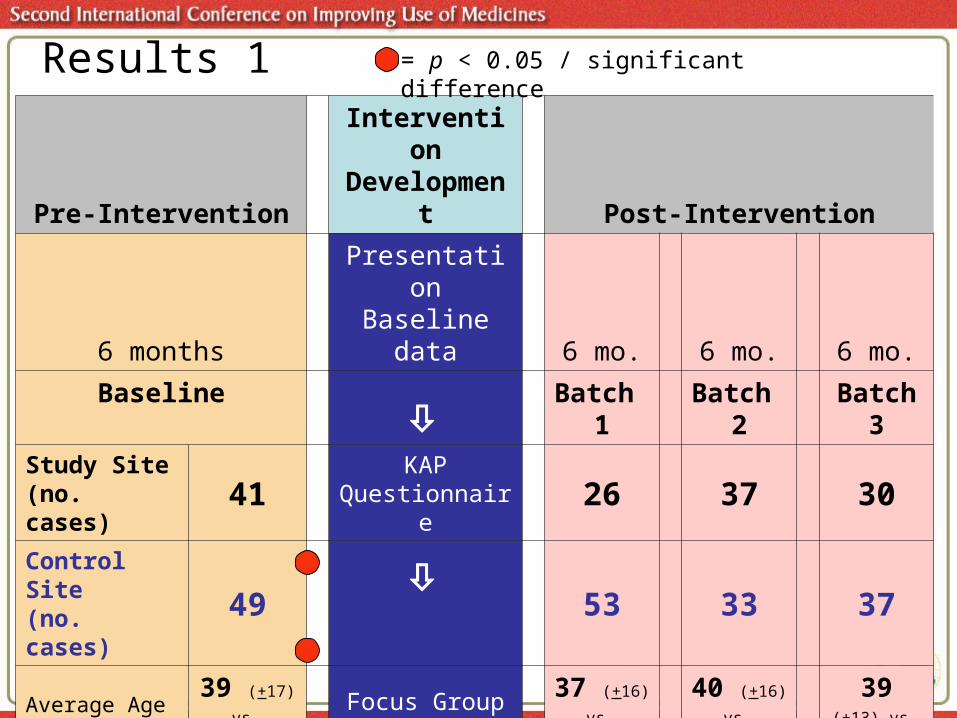
Pre-InterventionIntervention
Development Post-Intervention
6 monthsPresentation Baseline data 6 mo. 6 mo. 6 mo.
Baseline
Batch 1
Batch 2
Batch 3
Study Site(no. cases) 41 KAP
Questionnaire 26 37 30
Control Site (no. cases) 49
53 33 37
Average Age + SD (yrs)
39 (+17) vs
39 (+18)
Focus Group Discussions
37 (+16) vs
41 (+17)
40 (+16) vs
40 (+15)
39 (+13) vs
40 (+17)
Duration of Admission + SD (days)
9 (+ 6) vs
6 (+ 4) 6 (+ 6) vs
6 (+ 3)
6 (+ 4) vs
5 (+ 3)
6 (+ 3) vs
5 (+ 2)
Outcome(% recovered)
37 % vs
77%In-depth
interviews81 % vs
77%81 % vs
79%83 % vs
78%
Results 1 = p < 0.05 / significant difference

p< 0.05 p< 0.05 p< 0.05 NS
p< 0.05 p< 0.05 p< 0.05 p< 0.05
All Drugs
Antibiotics
0
1
2
3
4
5
6
7
8
9
Base Batch1 Batch 2 Batch 3
Nu
mb
er
of
Dru
gs
Study - All drugs
Control - All drugs
Study - Antibiotics
Control - Antibiotics
Average Number of All Drugs and Antibiotics Prescribed for LRTI
Results 2
(n=41 vs 49) (n=26 vs 53) (n=37 vs 33) (n=30 vs 37)

Percent of All Drugs and Antibiotics Prescribed as Generics
0
20
40
60
80
100
Base Batch 1 Batch 2 Batch 3
Per
cent
Study -All Drugs
Control -All Drugs
Study-Antibiotics
Control -Antibiotics
Antibiotics
Results 3
p< 0.05 p< 0.05 p< 0.05 p< 0.05
p< 0.05 p< 0.05 p< 0.05 p< 0.05
All Drugs
(n=200/184) (n=45/88) (n=181/45) (n=139/63)
(n=205/184) (n=68/247) (n=285/122) (n=216/205)
0
20
40
60
80
100
Baseline Batch 1 Batch 2 Batch 3
Pe
rce
nt
Study
Control
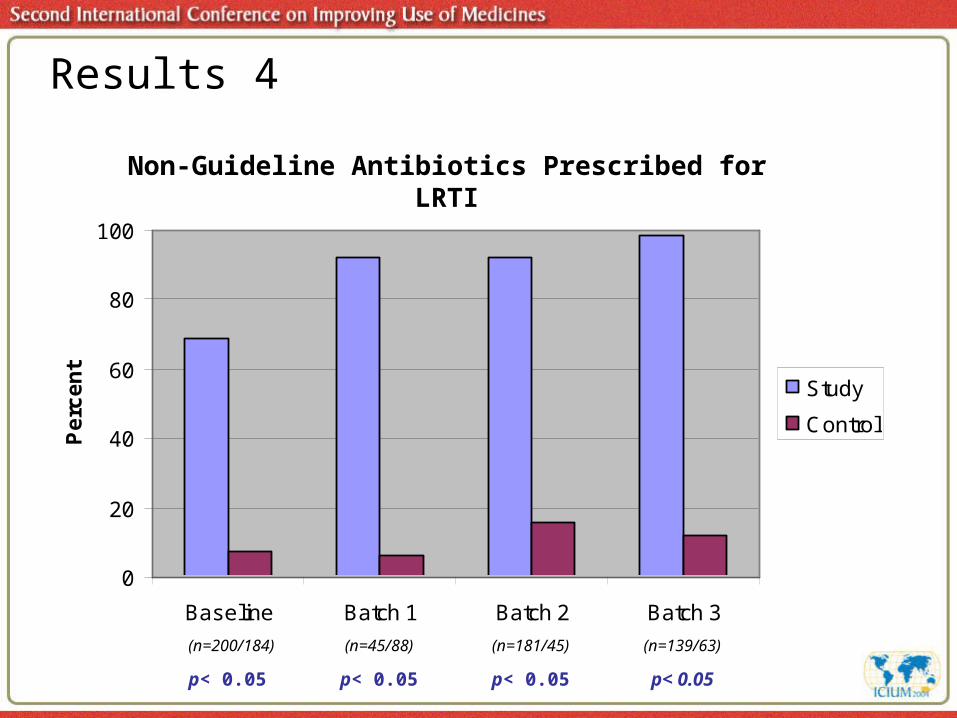
Non-Guideline Antibiotics Prescribed for LRTI
p< 0.05 p< 0.05 p< 0.05 p< 0.05
Results 4
(n=200/184) (n=45/88) (n=181/45) (n=139/63)

0
20
40
60
80
100
Baseline Batch 1 Batch 2 Batch 3
■ House Officer
■ Resident
■ Consultant
■ All doctors
Per
cen
t
Proportion of Non-Guideline Antibiotics Prescribed at Study Site for LRTI by category of Prescriber
Results 5
(n=52,69,46,19) (n=8,11,3,4) (n=29,39,10,26) (n=26,31,3,15)
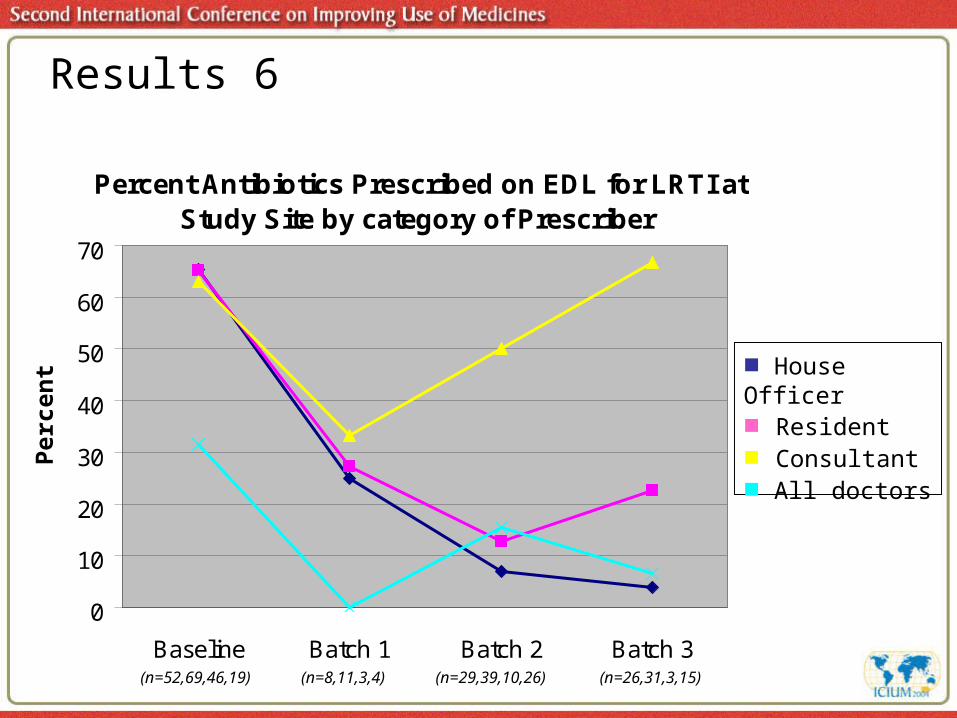
Percent Antibiotics Prescribed on EDL for LRTI at Study Site by category of Prescriber
0
10
20
30
40
50
60
70
Baseline Batch 1 Batch 2 Batch 3
Per
cen
t
Results 6
■ House Officer■ Resident■ Consultant■ All doctors
(n=52,69,46,19) (n=8,11,3,4) (n=29,39,10,26) (n=26,31,3,15)

Percent Antibiotics Prescribed as Generics for LRTI at Study Site by category of Prescriber
0
10
20
30
40
50
60
70
Baseline Batch 1 Batch 2 Batch 3
■ House Officer■ Resident■ Consultant■ All doctors
Per
cen
tResults 7
(n=52,69,46,19) (n=8,11,3,4) (n=29,39,10,26) (n=26,31,3,15)
Implications/Conclusions
Study results limited by small sample size Different antibiotic prescribing practices exist at the study and
control sites Control site has well established and effective Drug and
Therapeutics Committee (DTC) Consultant prescribing differs from junior doctors at study site Possibility of factors other than consultant influence
motivating junior doctors to prescribe specific antibiotics Intervention did not result in improved prescribing practice However, length of hospital stay and patient outcomes
significantly improved at study site Future research should address
Quality of Consultant supervision Need for regulatory measures Influence of the DTC on antibiotic prescribing at study site Role of drug promotion by pharmaceutical companies