altered states of consciousness - aeng-nsag · 2019-09-24 · altered states of consciousness...
TRANSCRIPT

Altered states of consciousness
Laszlo Vutskits MD, PhDDepartment of Anesthesiology, Pharmacology and Intensive Care, University Hospital of GenevaDepartment of Neuroscience, University of Geneva Medical School

objective: give some functional and mechanistic insights into biological processes and substrates underlying consciousness
plandefinition(s) of consciousnessstudying consciousness through altered states of consciousness
sleepgeneral anesthesiacoma, vegetative and minimal mental statesepilepsy
☞☞
☞☞☞☞

Definitions of Consciousness
“the perception of what passes in a man’s own mind”(Locke 1690)
“anything that we are aware of at a given moment forms part of our consciousness, making conscious experience at once the most familiar and most mysterious aspect of our lives” (Welmans & Schneider 2008)
“quality or state of being aware of an external subject or something within oneself”
(Merriam-Webster 2012)
“consciousness is synonymous with experience - any experience - of shapes, sounds, thoughts or emotions about the world or about the self”
(Tononi 2012)

How to study consciousness in neuroscience?
explore changes in the level of consciousnessconsider conditions in which consciousness is globally diminished, and ask what has changed in the brain
☞
investigate changes in the content of consciousness☞examine how and where brain activity changes when, everything else is being as equal as possible, a stimulus is experienced or not
develop theoretical framework☞clarify what consciousness is; how it can be generated in a physical system; how it can be measured; test the obtained theoretical predictions against biological data

Sleep: a physiologically altered state of consciousness
453 hours in humans

Sleep: a physiologically altered state of consciousness
physiological rhythm of waking /sleeping in
humans
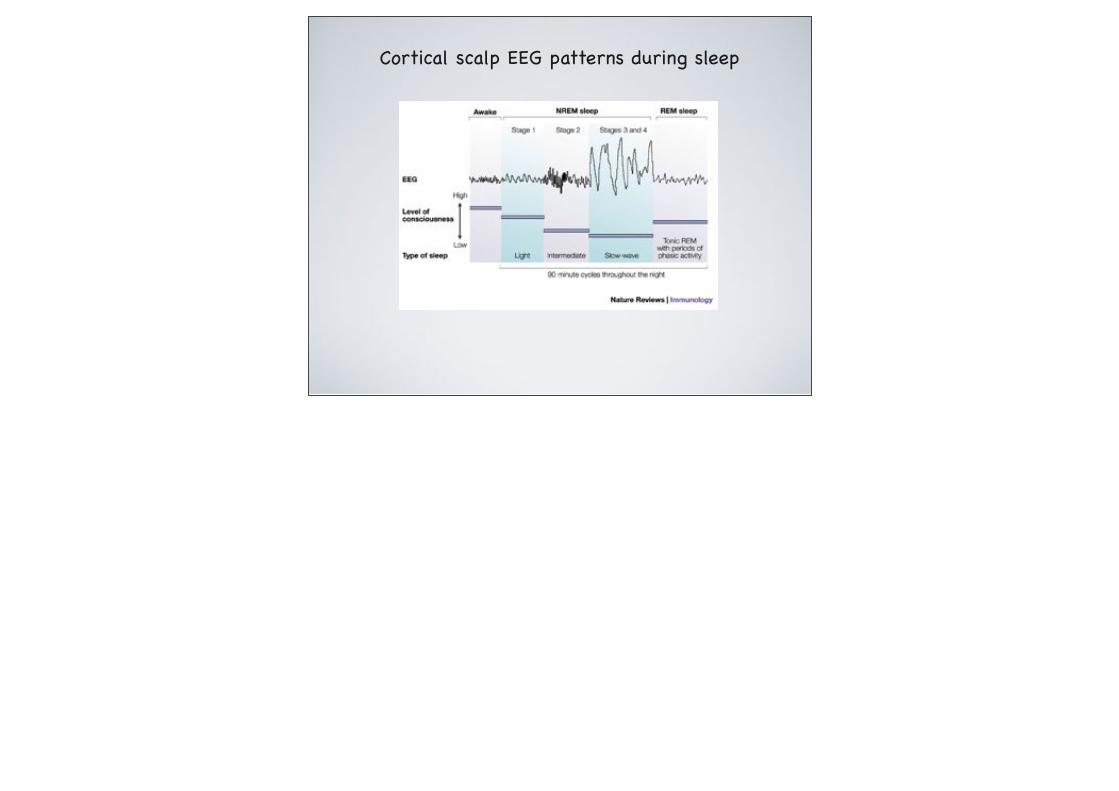
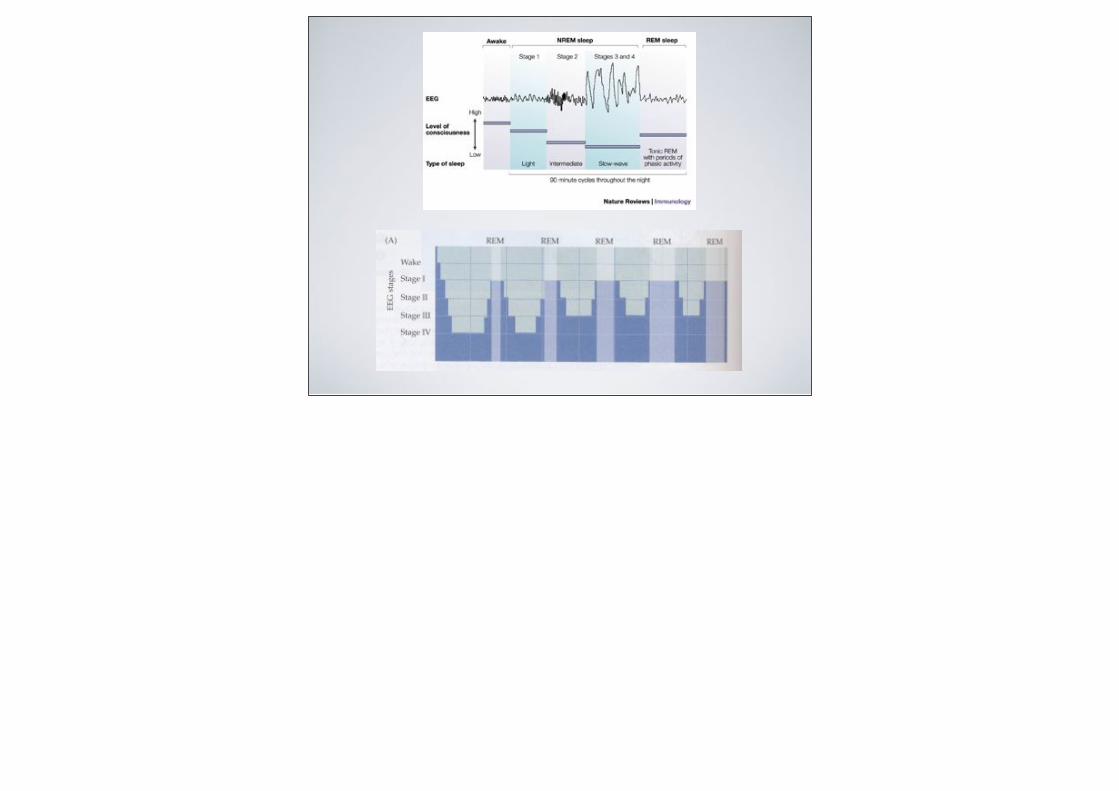
Cortical scalp EEG patterns during sleep

Neural circuits governing sleep
first steps ....

Functional neuroimaging of human sleep usingpositron emission tomography
brain areas with significant reduction of rCBF during slow wave NREM sleep
(compared to awake)

Functional neuroimaging of human sleep usingpositron emission tomography - REM phase
brain areas with significant increase in rCBF (compared to awake)

Neural circuits governing sleep
cholinergic nuclei
raphe nuclei(serotonin)
locus coeruleus(noradrenalin)
tuberomamillary n.(histamine)

cholinergic nuclei locus coeruleus raphe nuclei
brainstem nuclei
tuberomamillarynucleus
hypothalamus
orexin neurons
+ +
Cerebral cortex
Subcortex
Thalamus
+
+
+
ventrolateral preopticnucleus
-
-
circadian oscillator(suprachiasmatic n.)
integration of homeostatic and circadian inputs
retina
environmental light
homeostasis

Summary of the cellular mechanisms that govern sleep and wakefulness
Brainstem/hypoth nuclei responsible
Neurotransmitter involved
Activity state of neurons
Wakefulnesscholinergic nuclei
locus coeruleus
raphe nuclei
tuberomamillary nucleus
Acetylcholine
activeNorepinephrine
Serotonin
Histamine / Orexin
active
active
active
Non-REM sleep
cholinergic nuclei
locus coeruleus
raphe nuclei
tuberomamillary nucleus
Acetylcholine
decreasedNorepinephrine
Serotonin
Histamine / Orexin
decreased
decreased
decreased
REM sleepAcetylcholine
decreased
activecholinergic nuclei
others

General anesthesia
Is this pharmacologically-induced physiological sleep?

EEG patterns in sleep vs general anesthesia

Characteristic differences between anesthesia and sleep
Anesthesia Sleep
Ons
etM
aint
enan
ceOff
set
Drug-inducedNo homeostatic controlFailure to initiate is non-existentNot altered by environmental factors
Endogenously generatedHomeostatic and circadian regulationFailure to initiate is a recognized pathologySignificantly modulated by environmental factors
Duration dependent on doseDepth at a given anesthetic dose is constantFailure to maintain is non-existentAltered minimally by environmental factors
Duration function of homeostatic and circadian factorsDepth fluctuates rhythmically and spontaneouslyFailure to maintain is a recognized pathologySignificantly altered by environmental factors
Returns to normal wakefulness in hours to daysDuration of anesthesia and elimination of agent governs timing of wakefulness
Return to normal wakefulness within minutesTiming of wakefulness governed by environment, sleep duration, and circadian rhythm

some definitions related to general anesthesia ...
Amnesiapartial or complete loss of memory
Sedationdecreased level of arousal
Hypnosisimpairment of neural functions that are required to respond to verbal commands
Immobilitylack of movements in response to noxious stimuli
diff
eren
t mec
hani
sms
of a
ctions
/
diff
eren
t an
atom
ical t
arge
ts

Neuroanatomical substrates for anesthetics
5 right-handed volunteers
propofol infusion titrated to (i) mild sedation, (ii) deep sedation; (iii) no response to verbal commands (defined as unconsciousness...)evaluate global and regional cerebral blood flow using PET
☞☞
☞

Neuroanatomical substrates for anesthetics
Alkire & Miller 2005

20 right-handed volunteers☞dexmedetomidine infusion titrated to loss of response to verbal commands (LOC)and then tactile stimuli for return of consciousness (ROC) at the same drug concentration
☞
imaging ROC with propofol☞
dexmedetomidine propofol

Unconsciousness is associated with a loss of information (integration) capacity
breakdown of efficient cortical connectivity
control isoflurane (1.1%)
flash light at 0.2 Hz flash light at 0.2 Hz
Alkire et al. 2008

Loss of consciousness is associated with the breakdown of efficient cortical connectivity
Alkire et al. 2008

Neuroanatomical substrates for anesthesia
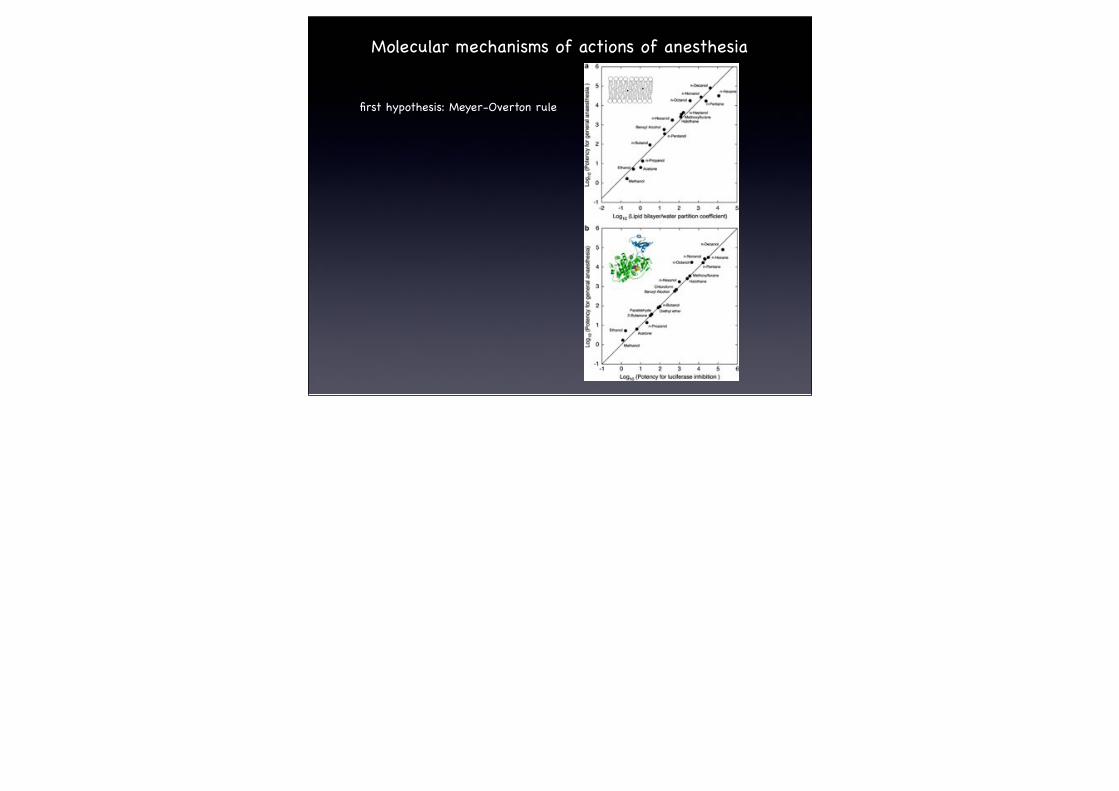
Molecular mechanisms of actions of anesthesia
first hypothesis: Meyer-Overton rule

Nicotinic receptor superfamilyNicotinic receptor superfamilyNicotinic receptor superfamilyNicotinic receptor superfamily Ionotropic glutamate receptors
Ionotropic glutamate receptors
Ionotropic glutamate receptors
GABAA Glycine nACh 5-HT3 AMPA kainate NMDA
Etomidate ++ + - 0 ND ND ND
Propofol ++ + - - - 0 -Barbiturates ++ + -- -- -- -- -Ketamine + 0 -- -- 0 0 --Isoflurane ++ ++ -- -- -- ++ -Sevoflurane ++ ++ -- -- ND ND ND
Nitrous oxide + + -- -- - -- --
Effects of currently used anesthetics on ligand-gated ion channels
++: significant potentiation; +: weak potentiation; --: significant inhibition; -: weak inhibition; 0: no effect; ND: remains to be determined.


Functional switch in GABAergic neurotransmission during development
Na+, K+
Cl-
NKCC1
Cl-GABAAR
GLU-R
Cl-
Na+
excitation
Na+, K+
Cl-
NKCC1
K+
Cl-
KCC2
GABAAR Cl-
Cl-
hyperpolarization
GLU-R


How to study efficacy of anesthesia in laboratory animals?
tail clamp test (classic for MAC determination)
locomotor activity (i.e. sedation)
righting reflex / sedation score (hypnotic activity)
hindlimb withdrawal reflex (immobilizing action)

How to study receptors and receptor subtypes mediating anesthesia effects?
receptor knock-out mice
knock-in transgenic approach (point mutations)



Adenosine receptors

How to ascertain that our patient sleeps during anesthesia?
EEG
BIS (and related qEEG)
physiological signs (BP, HR, RR)
isolated arm test (“Gold Standard”)

Arthur Guedel M.D.

EEG monitoring and anesthesia (I)
scalp EEG: voltage detected on the scalp
measure mean dendritic currents (post-synaptic potential) of hundreds to millions of cortical neurons that underlie the active electrode

EEG monitoring and anesthesia (II)

Bispectral index (BIS) monitoring


Memory formation during anesthesia
Explicit: awareness
Implicit: unconscious (but detectable/testable)Memory for mock crisis - Levinson 1965


Explicit memory formation during anesthesia (II)
Incidence (prospective studies are the only valid methodology
Overall: 1960-70: > 1.2% 1990-2000: 0.1-0.2%
Cardiac surgery: 0.5-23% (type of anesthesia, commorbidities)
Obstetrical surgery: 1960-70: > 1.2% 1990-2000: 0.4%

Explicit memory formation during anesthesia (I)
Explicit recall of events during general anesthesia is detected by direct (non-suggestive) questioning:
What was the last thing you remember before you went to sleep?What was the first thing you remember when you woke up?Can you remember anything in between these periods?Did you dream during your operation?
More than one interview is needed
Credibility of reports should always be verified

Explicit memory formation during anesthesia (III)

Implicit memory formation during anesthesia (II)
Occurence: strong association with BIS>50(studies were conducted under anesthesia in the absence of surgery! )
Does implicit memory matter?
Research in psychology suggests that even this very rudimentary activity may have profound effects on behaviour and emotion
Priming does not induce novel behaviours; it enhances existing tendencies

Bispectral index (BIS) monitoring


Memory formation during anesthesia
Explicit: awareness
Implicit: unconscious (but detectable/testable)Memory for mock crisis - Levinson 1965


Explicit memory formation during anesthesia (II)
Incidence (prospective studies are the only valid methodology
Overall: 1960-70: > 1.2% 1990-2000: 0.1-0.2%
Cardiac surgery: 0.5-23% (type of anesthesia, commorbidities)
Obstetrical surgery: 1960-70: > 1.2% 1990-2000: 0.4%

Explicit memory formation during anesthesia (I)
Explicit recall of events during general anesthesia is detected by direct (non-suggestive) questioning:
What was the last thing you remember before you went to sleep?What was the first thing you remember when you woke up?Can you remember anything in between these periods?Did you dream during your operation?
More than one interview is needed
Credibility of reports should always be verified

Explicit memory formation during anesthesia (III)

Implicit memory formation during anesthesia (II)
Occurence: strong association with BIS>50(studies were conducted under anesthesia in the absence of surgery! )
Does implicit memory matter?
Research in psychology suggests that even this very rudimentary activity may have profound effects on behaviour and emotion
Priming does not induce novel behaviours; it enhances existing tendencies

Implicit memory formation during anesthesia (I)
(Memory for mock crisis - Levinson 1965 )
Methods to test:
Hypnosis
Perceptual primingdef.: perceptual priming represent temporarily increased activation of a word or idea in memorymethod: word stem completion (eg. “tractor” per-op then asscociation tra- (traffic, tractor, travail etc.......) post-op
Conceptual primingdef.: conceptual priming refers to activation of related knowledge
method: e.g. Robinson Crusoe test (“Friday”)

Dreaming during anesthesia
Incidence : 1-81%
Predictors :patient factors : women > men young > old
anesthetics : ketamine-based*
opioid-based**
propofol-based**volatiles**>
* bizarre, hallucinating** pleasant (family, work, recreation, sexual)
depth of anesthesia : light > heavy
Consequences?

Pathologically-altered states of consciousness

Pathologically-altered states of consciousness

Pathologically-altered states of consciousness
Monti et al. 2010

Anatomo-pathological correlates
diffuse damage to subcortical white matter (diffuse axonal injury) - traumatic injury
☞
extensive cortical necrosis - non-traumatic injury☞thalamic damage - non-traumatic & traumatic injury☞
brainstem damage - mainly in locked-in syndrome☞

One of the major challenge in pathologically-altered states of consciousness
AVOID MISDIAGNOSIS
vegetative state vs minimally conscious state vs locked-in syndrome
Difficulties in diagnosis- based nearly entirely on clinical assessment- needs lots of experience (awareness vs wakefulness)- confusion between definitions/terminology- place for functional tools?

an intriguing example ........
- 23-year-old woman - severe traumatic brain injury in road accident - remained unresponsive 5 month later with preserved sleep-wake cycles - fulfilled the criteria of vegetative state according to international guidelinesunderwent fMRI imaging when asked to imagine to play tennis

- 54 patients with diagnosis of vegetative state
- fMRI to assess each patient’s ability to generate willful, neuroanatomically specific, blood-oxygenation-level-dependent responses during two established mental-imagery tasks- 5 patients were able to willfully modulate their brain activity
in 3 pts, additional bedside tests revealed some signs of awareness in 2 pts, further clinical assessment did not reveal signs of awareness

- 16 patients with diagnosis of vegetative state vs 12 healthy controls
- EEG task involving motor imagery
3 of 16 patients (19%) could repeatedly and reliably generate appropriate EEG responses to two distinct commands

6-month double-blind alternating crossover study
bilateral deep brain stimulation (DBS) of the central thalamus
one patient with the diagnosis of minimally conscious state for 6 years following traumatic brain injury


Schiff 2009

Conclusions
multiple underlying anatomical substrates☞
loss of efficient cerebral connectivity☞
general anesthesia as a model to study consciousness and neuronal plasticity
☞
pathologically-altered states of consciousness: challenges for appropriate diagnosis and potential therapy
☞

Readings
1. Purves, Neuroscience 4th edition, Chapter 28: Sleep and Wakefulness
2. Monti et al.,: The vegetative state. BMJ 2010, 341:c3765
3. Rudolph & Antkowiak: Molecular and neuronal substrates for general anesthetics. Nature Reviews Neuroscience 2004, 5:709