alberta's provincial diversion program - phase one ... · alberta’s provincial diversion...
TRANSCRIPT

Copyright Notice
This document is the property of Alberta Health Services (AHS).
On April 1, 2009, AHS brought together 12 formerly separate health entities in the province: nine geographically based health authorities (Chinook Health, Palliser Health Region, Calgary Health Region, David Thompson Health Region, East Central Health, Capital Health, Aspen Regional Health, Peace Country Health and Northern Lights Health Region) and three provincial entities working specifically in the areas of mental health (Alberta Mental Health Board), addiction (Alberta Alcohol and Drug Abuse Commission) and cancer (Alberta Cancer Board).

PPHHAASSEE OONNEE
IImmpplleemmeennttiinngg TThhee PPrroovviinncciiaall DDiivveerrssiioonn PPrrooggrraamm
IInn AAllbbeerrttaa CCoommmmuunniittiieess:: GGuuiiddeelliinneess AAnndd SSttaannddaarrddss
by Alberta’s Provincial Diversion
Working Committee
January 2003
Alberta’s Provincial Diversion Program

Material appearing in this report may be reproduced or copied without permission. Use of the following acknowledgement to indicate the source is required, however. Provincial Diversion Working Committee. (2003). Phase One--Implementing the Provincial Diversion Program in Alberta Communities: Guidelines and Standards. Alberta: Provincial Forensic Psychiatry Program (AMHB). In reproducing this document, please abide by the Terms of Use of the Alberta Mental Health Board website (http://www.amhb.ab.ca/programs/prog_forensic.html) from which this document has been retrieved.
Acknowledgement of the following ministries and consumer groups as part of the Provincial Diversion Working Committee:
Alberta Health and Wellness
Alberta Solicitor General Alberta Justice and Attorney General
Alberta Children’s Services Alberta Aboriginal Affairs and Northern Development
Alberta Human Resources and Employment Alberta Community Development
Alberta Mental Health Board Calgary Diversion Project
Canadian Mental Health Association Municipal Law Enforcement Representatives Royal Canadian Mounted Police (R.C.M.P.)
Schizophrenia Society of Alberta

Acknowledgements page i
The Diversion Program Implementation: Phase One document for a Provincial Diversion Program is submitted to the Mental Health and Justice Partnering Deputies Committee, consisting of the following members:
Mr. Roger Palmer Deputy Minister, Alberta Health & Wellness
Mr. Murray Finnerty Chief Executive Officer,
Alberta Alcohol & Drug Abuse Commission (AADAC)
Mr. William J. Byrne Deputy Minister,
Alberta Community Development Mr. Ron Hicks Deputy Minister,
Alberta Human Resources & Employment Mr. Terrence Matchett Deputy Minister & Deputy Attorney General
Alberta Justice & Attorney General Ms. Paddy Meade Deputy Minister,
Aboriginal Affairs & Northern Development Mr. Jim Nichols Deputy Solicitor General,
Alberta Solicitor General Mr. Ray Block Acting Chief Executive Officer,
Alberta Mental Health Board (AMHB) Ms. Paula Tyler Deputy Minister,
Alberta Children’s Services

Acknowledgements page ii
ACKNOWLEDGEMENTS The Provincial Diversion Working Committee members are acknowledged for their contribution and guidance in the development of the Provincial Diversion Program:
Dr. Carol Adair Director of Research, Alberta Mental Health Board
Laurie Beverley, Co-Chair
Provincial Administrative Director, Forensic Psychiatry Program, Alberta Mental Health Board
Norman Boucher Chief of Police, Medicine Hat Police Service
Norma Boulton Director, Clinical Practice, Alberta Mental Health Board
Dr. John Brooks
Provincial Medical Director, Forensic Psychiatry Program, Alberta Mental Health Board
Yvonne Collinson Team Leader, Population Health Strategies Branch, Alberta Health and Wellness
Staff Sgt. Bob Couture Court Liaison/APU Administration, Calgary Police Service
Carol Dillman Manager, Program and Service Initiatives, Aboriginal Affairs and Northern Development
Brent Doney, Co-Chair
Director, Division Support Services, Correctional Services Division, Alberta Solicitor General
George Fernhout Regional Services Manager, Joint Position Lakeland Regional Health Authority and Alberta Mental Health Board
Sgt. Steve Gleboff Criminal Operations, “K” Division R.C.M.P.
Stacy Hodgson Adult and Senior Services Manager, Red Deer Mental Health Clinic, AMHB
Sandra Harrison Administrative Director, Children’s Mental Health Services, AMHB
Aggy King-Smith Program Planning & Evaluation Coordinator, Young Offender Services, Provincial Forensic Psychiatry Program, Alberta Mental Health Board
Marty Landrie Adult Services Coordinator, Aboriginal Mental Health, AMHB
Beth Lipsett Manager, Alberta Alcohol and Drug Abuse Commission
Orrin Lyseng Executive Director, Schizophrenia Society of Alberta
Jim Merchant Program Director, Adult Mental Health & Psychiatric Primary Care Alberta Mental Health Board
Ian McKnight Detective Spousal Violence Intervention Unit, Edmonton Police Service
Cassie Palamar Manager, Human Rights & Citizenship Branch, Alberta Community Development
Bob Reddick Program Manager, Forensic Assessment and Community Services (FACS) and Centerpoint, Northern Alberta Forensic Psychiatry Program
Bronwyn Shoush Director, Aboriginal Justice Initiatives, Alberta Solicitor General
Aleck Trawick, Q.C. Board Member, Canadian Mental Health Association
Irving Yaverbaum
Senior Policy Counsel, Appeals, Criminal Law Policy & Planning Branch, Alberta Justice
Sharon Zibin
Provincial Quality Management Coordinator, Forensic Psychiatry Program, Alberta Mental Health Board
Rose Barvir Recording Secretary, Provincial Forensic Psychiatry Program, AMHB

Acknowledgements page iii
The Provincial Diversion Working Committee gratefully acknowledges the contributions of time, energy and thoughtful discussion by numerous subcommittee members and the Calgary Diversion Project Steering Committee and Calgary Diversion Project Staff.
Fran Barnes Calgary Diversion Project Manager Laurie Beverley, Co-Chair
Provincial Administrative Director, Forensic Psychiatry Program, Alberta Mental Health Board
Yvonne Collinson Team Leader, Population Health Strategies Branch, Alberta Health and
Wellness Brent Doney, Co-Chair
Director, Division Support Services, Correctional Services Division, Alberta Solicitor General
Staff Sgt. Bob Couture Court Liaison/APU Administration, Calgary Police Service Cindy Davison Arrest Processing/Court Liaison Unit, Calgary Police Service Ramona Deer Program Manager, Calgary Young Offender Centre, Alberta Solicitor
General Dr. Rick Enns Former Program Manager, Centerpoint, Northern Alberta Forensic
Psychiatry Program Ken Hagel Assistant Chief Probation Officer, Solicitor General Karen Hala Manager, Alberta Alcohol and Drug Abuse Commission, Calgary Peter Halpin Team Service Coordinator, Community Geographic Team Resources,
Provincial Forensic Psychiatry Program, Alberta Mental Health Board Fay Herrick Education/Advocacy, Schizophrenia Society of Alberta, Calgary Chapter Aggy King-Smith Program Planning & Evaluation Coordinator, Young Offender Services,
Provincial Forensic Psychiatry Program, Alberta Mental Health Board Marty Landrie Adult Services Coordinator, Aboriginal Mental Health, Alberta Mental Health
Board Orrin Lyseng Executive Director, Schizophrenia Society of Alberta, Provincial Office Beth Lipsett Manager, Alberta Alcohol and Drug Abuse Commission, Edmonton Jim Merchant Program Director, Adult Mental Health & Psychiatric Primary Care,
Alberta Mental Health Board Lynn McLean Alberta Alcohol and Drug Abuse Commission, Calgary Bob Reddick Program Manager, Forensic Assessment and Community Services (FACS)
and Centerpoint, Northern Alberta Forensic Psychiatry Program
Sharon Sutherland Past Chair, Provincial Advocacy Committee Schizophrenia Society of Alberta, Provincial Office
Aleck Trawick, Q.C. Board Member, Canadian Mental Health Association Sharon Zibin
Provincial Quality Management Coordinator, Forensic Psychiatry Program, Alberta Mental Health Board

Preface to Diversion Program Implementation: Phase One page 1
PPRREEFFAACCEE The most effective diversion begins at the community level through prevention programs, prior
to an individual’s contact with the law. As such, the Provincial Diversion Working Committee
supports the need for prevention and intervention programs within communities, based on the
premise that, whenever possible, communities and individuals should have access to mental
health, social and support services before it is necessary for law enforcement to be involved.
Although the Provincial Diversion Working Committee’s mandate does not include those
individuals with mental illness who are not in conflict with the law but who are at risk of
offending, it is recognized that the optimal situation within communities involves a strong
support for prevention and intervention programs.
The overall goal of this Diversion Program Implementation: Phase One (2003) document is to
provide a set of provincial guidelines and standards for Alberta communities involved in the
diversion of individuals with mental illness who are in conflict with the law. As indicated in the
Proposed Provincial Diversion Implementation Plan (2002), “program” is defined as consisting
of agreed upon values, protocols, processes, and standards of operation that are used within the provincial context and across ministries in the diversion of individuals with mental illness who are in conflict with the law.1 The intent is to capitalize on the existing
resources and expertise within communities, and, if necessary to augment resources as
needed.
For the purposes of the Provincial Diversion Program, mental illness refers to “clinically
significant patterns of behavioural or emotional functioning that are associated with some level
of distress, suffering, or impairment in one or more areas of functioning (for instance, school,
work, social and family interactions). At the basis of this impairment is a behavioural,
psychological, or biological dysfunction, or a combination of these.”2
As noted in previous reports prepared by the Provincial Diversion Working Committee, the
operational definition of diversion—and the one that has received support in principle from the
Mental Health and Justice Partnering Deputies Committee—includes the following
components:
Redirection of individuals with mental illness from the criminal justice system,
whenever appropriate, to mental health, social and support services.

Preface to Diversion Program Implementation: Phase One page 2
Continuum of integrated yet distinct services that include pre-charge diversion and
span the points of entry and exit to and from the criminal justice system and reflect
the unique needs of Alberta's communities.3
Not all individuals, either because of the nature of the offence, previous criminal history, or
their potential risk to society, may be appropriate for redirection from the criminal justice
system. Some individuals may be deemed to require probation and mandated treatment or
even incarceration.
For a truly comprehensive diversion program, those individuals with mental illness who
are incarcerated and those who are released from correctional facilities also require
access to mental health, social and support services.4 In recognition of this need, the
this document outlines guidelines not only for those diversion points at which
individuals are redirected from the criminal justice system to mental health, social and
support services but also for those points that reflect probation, incarceration and
reintegration back into the community.
IIMMPPLLEEMMEENNTTIINNGG TTHHEE DDIIVVEERRSSIIOONN PPRROOGGRRAAMM IINN AALLBBEERRTTAA’’SS CCOOMMMMUUNNIITTIIEESS
In developing the Phase One diversion document, the Provincial Diversion Working
Committee strived to achieve a balance—between ensuring provincial standards for a
diversion program and allowing for a reasonable degree of flexibility for communities. The
strategies, standards and suggested processes will guide a community in its development of a
diversion program. A provincial diversion representative will be available to communities to
further assist with the implementation process.
Following is an overview of the key elements:
Diversion Points refer to those points or occasions during which individuals with mental
illness (or are thought to have mental illness) who come in conflict with the law may be o redirected from the criminal justice system, if appropriate, to mental health,
social and support services

Preface to Diversion Program Implementation: Phase One page 3
o or provided access to and directed to mental health, social and support
services, while within the criminal justice system.
The points address pre-charge diversion and all other “points of entry and exit to and from
the criminal justice system”.5 Having a number of potential diversion points helps ensure
individual and community safety and provides the individual with a number of opportunities
for assistance and greater access to mental health, social and support services. (See
Section I: Diversion Points & Eligibility Criteria for further discussion.)
It is not expected that every community will offer or have the resources or infrastructure to
provide opportunities for diversion at all points presented in this program. Communities
are encouraged to select the specific points that best meet their needs.
Eligibility Criteria are necessary for every community diversion program. These criteria
include at minimum the following three considerations: nature of the incident, individual’s
situation, and available community resources.
Depending on the diversion point, eligibility is decided by a representative of the criminal
justice system, based on the three areas of consideration and any other factors, in
conjunction with any mental health assessment that may be deemed necessary.
The premise is that a lesser offence, a more positive and supportive individual situation,
and availability of appropriate community resources for an individual’s situation increases
the likelihood of that individual being diverted without charges and/or without incarceration.
Existing judicial and corrections processes are in place for diversion points 5 to 7 while the
individual is either on probation, incarcerated or being released from incarceration;
therefore, eligibility per se does not apply to these three points.
Individual safety and community safety are the most important considerations in
whether a certain diversion point is appropriate for an individual. It is recommended that a
risk management framework be developed for each diversion community and that
appropriate assessments of risk are conducted as part of determining an individual’s
eligibility. (See Section V: Appropriate Care, Support and Treatment.)

Preface to Diversion Program Implementation: Phase One page 4
No restrictions exist on the number of times an individual may enter the diversion
program/process. Research, along with evidence from the Calgary Diversion Project,
demonstrates that it may take a number of interactions with mental health, social and
support service professionals before an individual with mental illness may feel comfortable
and benefit from contact with that professional. Community resources vary in terms of types of services, accessibility and ability to be
involved in a diversion program. The Provincial Diversion Working Committee supports
the use of informal supports and ethnoculturally-specific resources as being important to
providing appropriate care, support and treatment. During the development of each
community diversion program, an evaluation of all potential resources is recommended,
including strengths and gaps in service.
Cross-ministerial, cross-agency collaboration: From the research and based on the
Calgary Diversion Project, collaboration and a case management approach are key
elements to a successful diversion program. It is recommended that communities ensure
that collaboration exists between regional health authorities, governmental and non-
governmental agencies/organizations, families or other informal supports (if appropriate) in
providing services to the target population. In addition, a case management approach is
important to ensuring that individuals receive appropriate referral, monitoring and follow up.
(See Section V: Appropriate Care, Support and Treatment.)
Sharing of information among service providers involved in the care, support and
treatment of the target population and between these groups and the criminal justice
system will be necessary. It is recommended that information be shared only with
informed consent and on a need-to-know basis. (See Section III: Information Sharing.)
Education and training are necessary components in the development of a community
diversion program. The belief is that education and training contribute to better knowledge
of the diversion process and the roles and limitations of community partners, as well as to
greater commitment by all stakeholders. It is also important to educate the community
about diversion and its potential impact. (See Section IV: Education and Training.)

Preface to Diversion Program Implementation: Phase One page 5
Appropriate Care, Support and Treatment: For a diversion program to be successful
within a community and on a provincial level, minimum or base standards are required for
care, support and treatment. (See Section V: Appropriate Care, Support and Treatment.) Evaluation of Diversion Programs: Determining whether a program is successful will be
based on appropriate evaluation, with outcome measures addressing a number of
components, including level of functioning, quality of life, degree of re-offending, along with
a cost-benefit analysis. As well, evaluation must consider the perspectives of all involved
stakeholders. (See Section VI: Evaluation and Accountability.)
Each of following sections provides information about what is important to successful
implementation of a diversion program and what strategies to use. A provincial diversion
representative will assist in developing the details for a specific community.

Preface to Diversion Program Implementation: Phase One page 6
EENNDDNNOOTTEESS 1 Provincial Diversion Working Committee. (2002). Alberta’s Provincial Diversion Program:
Proposed Implementation Plan for Reducing Criminalization of Individuals with Mental Illness.
2 Provincial Diversion Framework Working Committee. (2001). Alberta’s Provincial Diversion Framework: Reducing the Criminalization of Individuals with Mental illness
3 Provincial Diversion Framework Working Committee. (2001). Alberta’s Provincial Diversion Framework: Reducing the Criminalization of Individuals with Mental illness.
4 Provincial Diversion Framework Working Committee. (2001). Alberta’s Provincial Diversion Framework: Reducing the Criminalization of Individuals with Mental illness.
5 Provincial Diversion Framework Working Committee. (2001). Alberta’s Provincial Diversion Framework: Reducing the Criminalization of Individuals with Mental illness.

SSEECCTTIIOONN II DIVERSION POINTS & ELIGIBILITY CRITERIA Contents RELATIONSHIP BETWEEN DIVERSION POINTS & ELIGIBILITY CRITERIA DIVERSION POINTS SUMMARIZED DETERMINING FACTORS FOR ELIGIBILITY
The Nature Of The Incident The Individual’s Situation Available Community Resources
THE SEVEN DIVERSION POINTS
Commission Of An Offence/No Apparent Crisis Situation Commission Of An Offence/Crisis Situation During Case Review For Potential Pre-Trial Diversion While An Individual Has Been Remanded To Custody In Sentencing, Mandated Treatment/ Probation During Incarceration Upon Release From Incarceration
…………………………………………….….1 ………………………………………………..2 ………………………………………………..3 ………………………………………………..5

Section I: Diversion Points & Eligibility Criteria page 1
RREELLAATTIIOONNSSHHIIPP BBEETTWWEEEENN DDIIVVEERRSSIIOONN PPOOIINNTTSS && EELLIIGGIIBBIILLIITTYY CCRRIITTEERRIIAA
There may be several points at which an individual with mental illness who is in conflict
with the law may be diverted from the criminal justice system.1 Historically, the belief has
been that diversion is either pre-charge or post-charge. However, the Provincial Diversion
Working Committee has expanded the definition of diversion to include the need for
appropriate care, support and treatment, even if an individual is incarcerated or
transitioning from incarceration to the community.
By taking this comprehensive approach, The Provincial Diversion Working Committee
hopes to achieve the following:
Opportunities for communities to select which points are most appropriate to them,
based on their community’s characteristics and available resources.
The option to defer the decision to divert an individual until later in the process if there
are concerns about individual and/or community safety. For instance, in some cases,
law enforcement or the Crown may feel uncertain as to whether an individual should
be considered for diversion and may require the opinion of a judge.
Most importantly, an opportunity for individuals with mental illness to be provided with
access to appropriate care, support and treatment regardless of whether or not they
enter the criminal justice system. If incarceration is deemed necessary they should
still have opportunities for appropriate care, support and treatment.
Research and preliminary stakeholder consultations have also demonstrated that criteria
are required to assist communities in determining who is eligible for diversion—particularly
in diversion points 1 through 4—as outlined in this section.2 Three factors have been
identified as being important in determining eligibility: nature of the offence, individual’s
situation, and community resources. It is also important to stress that communities may
use their discretion in determining eligibility on “a case-by-case basis”.
The Provincial Diversion Working Committee provides these diversion points as
guidelines for communities that develop a diversion program.
Section I: Diversion Points & Eligibility Criteria page 2
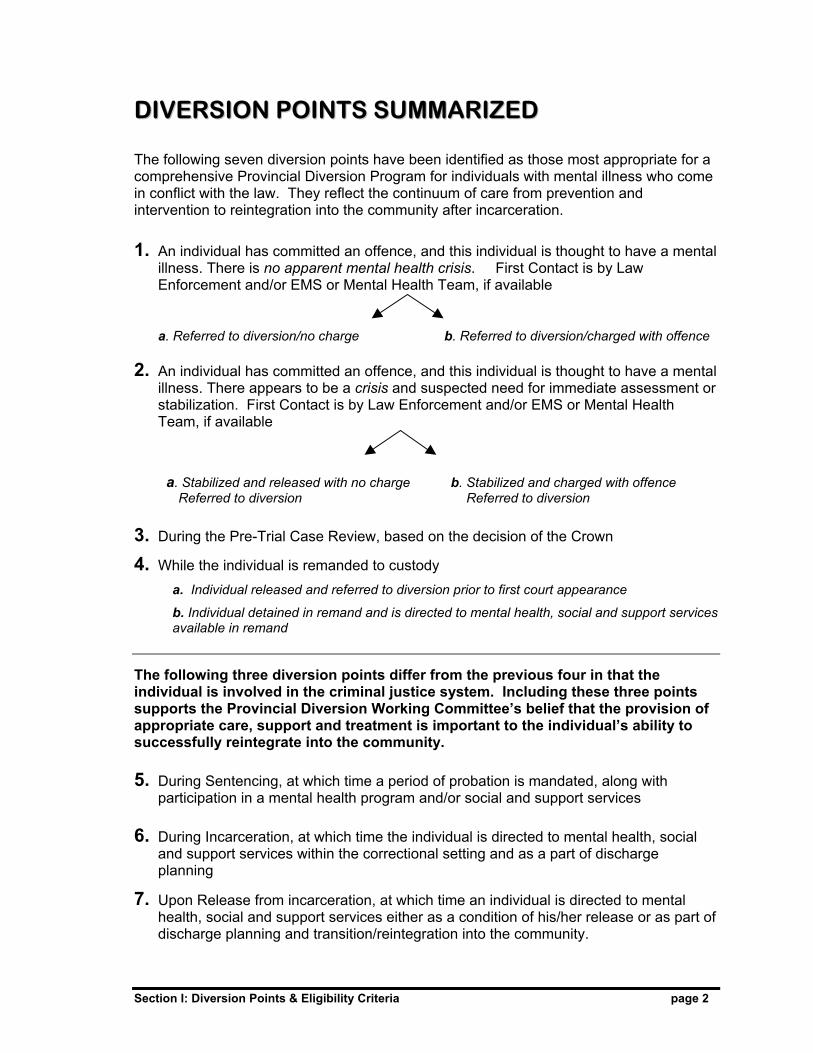
DDIIVVEERRSSIIOONN PPOOIINNTTSS SSUUMMMMAARRIIZZEEDD The following seven diversion points have been identified as those most appropriate for a comprehensive Provincial Diversion Program for individuals with mental illness who come in conflict with the law. They reflect the continuum of care from prevention and intervention to reintegration into the community after incarceration.
1. An individual has committed an offence, and this individual is thought to have a mental illness. There is no apparent mental health crisis. First Contact is by Law Enforcement and/or EMS or Mental Health Team, if available
a. Referred to diversion/no charge b. Referred to diversion/charged with offence 2. An individual has committed an offence, and this individual is thought to have a mental
illness. There appears to be a crisis and suspected need for immediate assessment or stabilization. First Contact is by Law Enforcement and/or EMS or Mental Health Team, if available
a. Stabilized and released with no charge b. Stabilized and charged with offence Referred to diversion Referred to diversion
3. During the Pre-Trial Case Review, based on the decision of the Crown
4. While the individual is remanded to custody a. Individual released and referred to diversion prior to first court appearance
b. Individual detained in remand and is directed to mental health, social and support services available in remand
The following three diversion points differ from the previous four in that the individual is involved in the criminal justice system. Including these three points supports the Provincial Diversion Working Committee’s belief that the provision of appropriate care, support and treatment is important to the individual’s ability to successfully reintegrate into the community.
5. During Sentencing, at which time a period of probation is mandated, along with participation in a mental health program and/or social and support services
6. During Incarceration, at which time the individual is directed to mental health, social and support services within the correctional setting and as a part of discharge planning
7. Upon Release from incarceration, at which time an individual is directed to mental health, social and support services either as a condition of his/her release or as part of discharge planning and transition/reintegration into the community.

Section I: Diversion Points & Eligibility Criteria page 3
DDEETTEERRMMIINNIINNGG FFAACCTTOORRSS FFOORR EELLIIGGIIBBIILLIITTYY Individual and community safety must be reflected in decisions surrounding whether an
individual is eligible for entry to a diversion program. Accordingly, these considerations—
the nature of the incident, the individual’s situation, and the availability of community
resources—should provide the basis for determining eligibility. It is still important to have
the opportunity to determine an individual’s eligibility on a “case-by-case basis”.
1. Evaluating The Nature Of The Incident
The nature of the incident is of particular importance when the decision is made to divert
an individual without charging him/her. Instead of a comprehensive list of offences that
can be included in a diversion program, the following guidelines should be considered
when determining whether the nature of the offence makes it appropriate for an individual
to be diverted:
i. The safety of the individual and community is of primary consideration.
ii. Generally, offences that would be appropriate for diversion without charges would
be those that are considered to be low risk, minor offences.
iii. The determination is made on a case-by-case basis. In some situations, the
offence may be major if based strictly on a legal perspective; however, the
circumstances or knowledge about the individual may indicate that a justice system
response is not appropriate.
The individual’s past history of offending may or may not be known when a law
enforcement officer comes in contact with the person.
2. Evaluating The Individual’s Situation
An individual’s personal situation is an important factor in determining the individual’s
success in a diversion program, especially in the case of diversion without charges. For
instance, Seide (1999) points to the following types of individuals as being least
appropriate for diversion:
◊ “Individuals with poor motivation to change their lifestyle
◊ Those with repeated treatment failures and medication non-compliance
◊ Those with an inability to adjust to limits and structure
◊ Those with little or no community support”3

Section I: Diversion Points & Eligibility Criteria page 4
Research also shows that certain conditions may decrease an individual’s likelihood of
participating voluntarily in mental health, social and support services. A transient lifestyle,
access to appropriate housing, marginal employment skills, few or no support groups, and
substance misuse are often the complicating factors that may determine whether an
individual will attend a voluntary “treatment” program or not.4
Supported by many researchers, Seide’s observations provide a community with a look at
the “realities” regarding this target population.5 It is important to recognize that these
factors are central to determining whether an individual may be successful but not to use
only them in evaluating an individual’s eligibility. It is also necessary to determine what
community resources may be available to assist in changing the individual’s situation.
These are the guidelines for evaluating an individual’s situation:
i. The safety of the individual is of primary consideration, especially if an individual is in
an immediate crisis.
ii. Support increases the individual’s likelihood of following through on the referral, and
perhaps on medication compliance, if appropriate.
3. Evaluating A Community’s Resources
In order for diversion to be effective, there must be a minimum set of both informal and
formal community resources to provide services for the individual.6
The following guidelines are to be considered when communities evaluate their resources
in relation to the needs of the individual and to the nature of the incident. It is
recommended that communities:
i. Identify existing community governmental and non-governmental agencies and
organizations that would participate in a diversion program
ii. Outline the roles and mandates of participating agencies and organizations and
share that information with all professionals involved in diversion
iii. Define all potential informal supports that may exist and outline the role of those
informal supports in diversion.
In summary, these three considerations are provided as guidelines to assist communities
in determining eligibility and necessary supports if an individual is eligible for diversion.

Section I: Diversion Points & Eligibility Criteria page 5
TTHHEE SSEEVVEENN DDIIVVEERRSSIIOONN PPOOIINNTTSS:: Eligibility Criteria & Diversion Processes The following charts each relate to a different diversion point, labelled 1 through 7. The
information can assist a community in determining the following for each diversion point:
◊ whether an individual is appropriate for diversion at select points ◊ who is involved in the diversion process ◊ what general steps can be incorporated for the specific diversion point.
Alberta’s communities are unique and vary in many ways, including available resources,
degree of collaboration, geography, ethnocultural factors, and others. In consideration of
the uniqueness of each community, the following guidelines for each diversion point are
designed to provide flexibility in determining which points may be most appropriate. They
also allow communities to adapt the procedures for a potential diversion point to their
unique circumstances. Further development of the guidelines will occur in conjunction
with each community as it plans its diversion program.

Section I: Diversion Points & Eligibility Criteria page 6
1. COMMISSION OF OFFENCE / NO APPARENT CRISIS SITUATION a. Diversion Without A Charge b. Diversion With A Charge (Involving Law Enforcement / Mental Health Professionals / EMS)
Nature of Incident Individual’s Situation Resource Requirements Low risk, minor offence
Determined on a case by case basis Criminal history may or may not be known
Individual is thought to have a mental illness but does not appear to be in a crisis situation in which he/she would require immediate or emergency psychiatric assessment and/or admission Individual has some support /stability in the community—either housing, family supports, active involvement in program(s).
OR Individual does not have stable environment, but demonstrates willingness to participate in care, support & treatment. A “safe” living environment may be necessary for a designated period. Individual is thought to have a mental illness with a co-existing disorder such as substance abuse, Fetal Alcohol Syndrome (FAS), amongst others YOUTH – SPECIAL SERVICES A youth may not have family stability but may need or currently is under protective services of Alberta’s Children’s Services
Individual should have informal supports available, such as family or community supports, if appropriate, who are willing to assist in enabling individual’s participation in the diversion program. These informal supports may include teachers, church leaders, aboriginal community members, or other individuals deemed appropriate
Access to timely mental health assessment, if deemed necessary, via one of the following:
--Local mental health professionals --Telemental Health Services within reasonable proximity or availability of transportation to Telemental Health Services location Access to mental health, social and support services, including addictions, housing and financial supports
Potential Diversion Procedures 1. Based on the criteria, the attending officer determines whether individual should be diverted without charges or with charges. a) if the individual is not charged, the attending officer provides the individual with a “referral” to person/organization responsible for diversion, who arranges for assessment and a treatment plan. The referral should be written, indicating the name of the diversion person/organization, the address, and phone number. b) if the individual is charged, the attending officer
• provides the individual with a referral to the mental health professionals responsible for assessment for the diversion program
• indicates to the individual that following through on the referral may be a consideration in how the Crown views the charge
• contacts the diversion program personnel—as designated in the community—to conduct the assessment and prepare a report to be forwarded to the Crown Prosecutor’s office regarding recommendation for entry to the diversion program and adjournment for a designated period
2. The option of referring to Extra Judicial Measures and Extra Judicial Sanctions is available, should the individual’s situation be appropriate and agreed to by the Crown and Probation within the community. 3. In the case of a youth, the attending officer notifies the youth’s parents, guardians or deemed responsible party of the following:
• the nature of the incident/offence • the expected action by the youth • any requirements for follow up on the youth’s progress

Section I: Diversion Points & Eligibility Criteria page 7
2. COMMISSION OF AN OFFENCE / CRISIS SITUATION a. Diversion Without A Charge b. Diversion With A Charge (Involving Law Enforcement / Mental Health Professionals / EMS)
Nature of Incident Individual’s Situation Resource Requirements Low risk, minor offence Determined on a case by case basis Criminal history may or may not be known to police
Individual with mental illness is thought to be in a “crisis situation” at the time of commission of the offence and first contact by law enforcement
Individual may have some support and stability in the community
OR Individual does not have stable environment, but demonstrates willingness to participate in treatment. A “safe” living environment is available for a designated period of time
Individual is thought to have a mental illness with a co-existing disorder, such as substance abuse, Fetal Alcohol Syndrome (FAS), amongst others YOUTH – SPECIAL SERVICES A youth may not have family stability but may need or currently is under protective services of Alberta’s Children’s Services
Individual has informal supports available, such as family or community supports, if appropriate, who are willing to assist in enabling the individual’s participation in the program, once individual is past crisis. These informal supports may include teachers, church leaders, aboriginal community members, or other individuals deemed appropriate
Immediate access to local hospital and/or psychiatric facility for assessment and stabilization (facility may vary in community)
Mental Health Outreach
Telemental Health Services within reasonable proximity or availability of transportation to Telemental Health Services
Access to mental health treatment, social and support services, including addictions, housing and financial supports
Potential Diversion Procedures 1. Depending on the nature of the crisis situation and availability of community resources, the attending officer
EITHER: a) Calls for a Crisis Intervention Worker (CIT) to attend the scene and assess the degree of crisis, if such a position is available.
• If the crisis might create possible further risk to self or to community and/or involves weapons, then the CIT worker (or other appropriate mental health professional) assists law enforcement, if necessary, in ensuring the client is taken to a secure facility.
• If crisis is deemed to be of a minor nature, then the CIT worker (or other appropriate mental health professional), in conjunction with law enforcement if deemed necessary, will attempt to diffuse the crisis prior to release of the individual.
OR b) Takes the individual directly to local hospital emergency or to other secure mental health facility for psychiatric assessment and/or patient stabilization. Specific community guidelines—in conjunction with provincial Mental Health Act, if necessary—should dictate the procedures involving the release of these individuals from the local hospital and/or psychiatric facility.
2. Once the crisis situation is controlled, and: a) if the individual is diverted without charges, the attending officer provides the individual with a “referral” to organization/agency responsible for diversion, which arranges for assessment and a treatment plan, if necessary. If required, the officer will give this referral via third party.
b) if the individual is charged, the attending officer • provides the individual with a referral to the mental health professionals involved with the diversion
program, to be used upon the individual’s release from hospital or psychiatric facility should the length of stay be minimal. If required, the officer will give this referral via third party.
• indicates to the individual that following through on the referral may be viewed favourably by the Crown • contacts the diversion program personnel to notify of the referral, if consent for such contact is received.
They in turn will conduct the assessment and prepare a report to be forwarded to the Crown Prosecutor’s office regarding recommendation for entry to the diversion program and adjournment for a designated period of time.
3. The option of referring to Extra Judicial Measures and Extra Judicial Sanctions is available, should the individual’s situation be appropriate and agreed to by the Crown and Probation within the community.
4. In the case of a youth, the attending officer notifies the youth’s parents, guardians or deemed responsible party of the following: the nature of the incident/offence, expected action by the youth, any requirements for follow up.

Section I: Diversion Points & Eligibility Criteria page 8
3. DURING CASE REVIEW FOR POTENTIAL PRE-TRIAL DIVERSION
(At the Discretion Of The Crown / Recommendations From Defence)
Nature of Incident Individual’s Situation Resource Requirements May or May Not Be Low risk, minor offence Determined on a case by case basis
Individual is suspected of having a mental illness, based on information gathered prior to trial or from observations of behaviour Individual is thought to have a mental illness with a co-existing disorder, such as substance abuse, Fetal Alcohol Syndrome (FAS), amongst others Individual may have been previously involved in the diversion process Individual expresses a willingness to participate in mental health assessment, treatment and in social and support services as deemed appropriate, but requires some formal sanctions to encourage participation Individual may or may not have support and stability in the community in terms of housing, family supports, and/or active involvement in treatment program(s) YOUTH – SPECIAL SERVICES A youth may not have family stability but may need or currently is under protective services of Alberta’s Children’s Services
Individual may or may not have informal supports available, such as family or community supports, if appropriate, who are willing to assist in enabling individual’s participation in program. These informal supports may include teachers, church leaders, aboriginal community members, or other individuals deemed appropriate
Access to timely mental health assessment, if deemed necessary, via one of the following:
--Local mental health professionals --Telemental Health Services within reasonable proximity or availability of transportation to Telemental Health Services location
Access to mental health treatment, social and support services, including addictions, housing and financial supports
Potential Diversion Procedures 1. The decision for referral to a diversion program/process is made by the Crown Prosecutor’s Office when the case is being reviewed prior to trial, or from a recommendation from defence counsel to the Crown during this time 2. The accused or counsel will be given contact information regarding the diversion program. A triage assessment is usually completed in an agreed upon, reasonable length of time based on specific community resources and the willingness of the court regarding length of time for adjournment. 3. Assessment report will be forwarded to the Crown Prosecutor’s office.
4. The Crown Prosecutor will return to Court with the Assessment Report and either: • Prosecute the charge(s), if candidate unsuitable for program OR • Request further adjournment for referral to the local diversion process for a designated, reasonable
length of time, based on specific community resources, when the situation can be re-evaluated in Court.
5. At the end of the designated time, a report from the diversion program, which will include information on linkages made, participation of client and progress made, will be forwarded to the Crown Prosecutor’s office to decide whether to withdraw the charge.

Section I: Diversion Points & Eligibility Criteria page 9
4. WHILE INDIVIDUAL HAS BEEN REMANDED TO CUSTODY
(Involving Remand Staff / Mental Health Therapists / At The Discretion Of The Court)
Nature of Incident Individual’s Situation Resource Requirements May or May Not Be Low risk, minor offence Determined on a case by case basis
Individual may or may not have support and stability in the community in terms of housing, family supports, and/or active involvement in treatment program(s) Individual is thought to have a mental illness with a co-existing disorder, such as substance abuse, Fetal Alcohol Syndrome (FAS), amongst others A. FOR REDIRECTION & RELEASE Prior to or during the individual’s time in remand, he/she exhibits signs of mental illness Individual should have access to safe housing
Individual is determined to not present a risk to self or others B. FOR ACCESS TO CARE, SUPPORT & TREATMENT IN CUSTODY Prior to or during the individual’s time in remand, he/she exhibits signs of mental illness
In addition to seriousness of offence, individual may present a risk to self or to others
YOUTH – SPECIAL SERVICES A youth may not have family stability but may need or currently is under protective services of Alberta’s Children’s Services
A. FOR REDIRECTION & RELEASE Individual may or may not have informal supports available, such as family or community supports, if appropriate, who are willing to assist in enabling individual’s participation in program. These informal supports may include teachers, church leaders, aboriginal community members, or other individuals deemed appropriate Access to timely mental health assessment, if deemed necessary, via one of the following: --Local mental health professionals --Telemental Health Services within reasonable proximity or availability of transportation to Telemental Health Services location Access to safe housing, if necessary Access to mental health, social and support services, including addiction, housing, and financial supports, if deemed necessary
B. FOR ACCESS TO MENTAL HEALTH SERVICES IN CUSTODY Those mental health, social and support services deemed appropriate by remand centre
Potential Diversion Procedures 1. The remand staff determines that an individual exhibits signs of mental illness and contacts a mental health
professional affiliated with the diversion program to complete a mental health assessment. 2. Information regarding the court date is also provided to the mental health professional.
3. The Crown and the court will consider this information in determining if fitness for trial needs to be examined
or if an adjournment for a designated, reasonable time will be requested while the individual participates in the diversion program.

Section I: Diversion Points & Eligibility Criteria page 10
5. IN SENTENCING, MANDATED TREATMENT / PROBATION
(At The Discretion Of The Court)
Nature of Incident
Individual’s Situation
Resource Recommendations
The nature of the incident and individual’s situation are those that the Crown Prosecutor will present to the court as part of sentencing.
These resource recommendations are included to demonstrate their importance in improving treatment resources for the individual within the correctional system and his/her ability to function in the community upon his release. Individual may or may not have informal supports available, for instance, family or extended family, if appropriate, or other suitable community members, who are willing to assist in enabling individual’s participation in treatment, once individual is past crisis Access to timely mental health assessment, if deemed necessary, via one of the following:
--Local mental health professionals --Telemental Health Services within reasonable proximity or availability of transportation to Telemental Health Services location Access to mental health, social and support services, including addiction, housing, and financial supports, if deemed necessary
Potential Diversion Procedures 1. Individuals with Supervised Court orders, which include participation in the diversion program, will be followed
up regularly
2. The assigned probation officer will notify the diversion program with contact information.
3. The diversion program will contact the client’s probation officer by telephone at appropriate, agreed upon intervals, for instance, every two weeks for the initial month of the individual’s involvement and progress and then monthly.
4. At the end of the designated period, a report summarizing the individual’s involvement and progress will be
available to the probation officer. 5. If an individual fails to attend a scheduled appointment or refuses to participate in the diversion program, the
Probation Officer will be notified.
The following three diversion points demonstrate the Provincial Diversion Working
Committee’s belief that a comprehensive diversion program should include access to
mental health, social and support services, even if an individual is sentenced and
eventually incarcerated for an offence.

Section I: Diversion Points & Eligibility Criteria page 11
6. DURING INCARCERATION
(Involving The Correctional Centres And Community Resources Available In Centre)
Nature of Incident
Individual’s Situation
Resource Recommendations
The nature of the incident is such that warrants incarceration. The individual’s situation may vary. A mental health assessment has been done to establish that a mental illness is prevalent.
These resource recommendations are included to demonstrate their importance in improving treatment resources for the individual within the correctional system and his/her ability to function in the community upon release. Access to mental health assessment and treatment, social and support services Access to addictions services Access to additional social and support services that are deemed appropriate within a correctional setting
Potential Procedures for Access to Mental Health, Social and Support Services
The specific procedures for an individual’s involvement in mental health, social and support services are based on each correctional facility and its resources.
It is recommended that the correctional centres have in place procedures for
a) assessing individuals who are suspected of having a mental illness
b) referring individuals with mental illness to mental health, social and support services offered in the correctional facility
c) monitoring and documenting the individual’s progress within these programs
d) sharing information regarding that progress with those involved in discharge planning and eventually
transitioning into the community

Section I: Diversion Points & Eligibility Criteria page 12
7. UPON RELEASE FROM INCARCERATION
(Involving Correctional Centres; Transition, Mental Health, Social & Support Services)
Nature of Incident
Individual’s Situation
Resource Recommendations
The nature of the incident is not relevant, unless it places conditions upon the individual’s release.
The individual may or may not have informal supports within the community
These resource recommendations are included to demonstrate the importance of appropriate transitioning and reintegration of the individual into the community upon his/her release. Access to mental health, social and support services, including addiction, housing, and financial supports, if deemed necessary
Potential Procedures For Transition Into Community 1. Discharge planning should be done in conjunction with forensic or community based mental health services.
2. With consent, sharing of information should occur regarding the types of programs/services accessed by the
individual while in incarceration and his/her progress within those programs. This information can be used to plan potential programs/services for that individual upon release.
3. Transitioning into the community should consider the following:
a) individual’s housing situation and needs b) individual’s financial needs c) individual’s education or vocational achievements and needs d) formal community supports

Section I: Diversion Points & Eligibility Criteria page 13
In summary, each community may determine which diversion points it wishes to
incorporate. It is recommended that communities consider their resources and phase in
different diversion points, rather than attempting to provide a comprehensive program
from the outset. Granted, some communities may have the resources and the necessary
foundation of “collaboration” among service providers that enables them to develop a
more comprehensive diversion program from the start.
However, based on the experiences of Calgary Diversion Project, it is important to ensure
that everyone within the community understands the diversion program and supports the
community diversion team in its efforts. This takes time and planning, as well as fine
tuning of the diversion process. Therefore, the recommendation is to start with only a couple of diversion points in order to ensure that communities build a strong program for the target population.

Section I: Diversion Points & Eligibility Criteria page 14
EENNDDNNOOTTEESS
1 Ontario's Human Services and Justice Coordination Project. (1996). A Provincial Strategy to Coordinate Human Services and Criminal Justice Systems in Ontario. Ontario Ministry of Attorney General, Ministry of Community and Social Services, Ministry of Health, Ministry of the Solicitor and Correctional Service. (Although there are a number of sources that refer to the varied diversion points, the Ontario document is most comprehensive.)
2 Teplin, L.A. (2000). Keeping the Peace: Police Discretion and Mentally Ill Persons. National Institute of Justice Journal. Stakeholder Consultations, conducted October – December 2001 with individuals involved with target population in select Alberta communities. *Numerous sources, as well as discussion from Provincial Diversion Working Committee members, refer to the need for criteria.
3 Seide, M. (1999). Letter: A Jail Diversion Program. Psychiatric Services, 50(2): 269-270.
4 National Alliance for the Mentally Ill. Dual Diagnosis: Mental Illness and Substance Abuse. (Substance Abuse complicates almost every aspect of care for the person with mental illness. Individuals are difficult to engage in treatment; difficult to diagnose; often not tolerated in community residences of rehabilitation programs.)
5 Seide, M. (1999). Letter: A Jail Diversion Program. Psychiatric Services, 50(2): 269-270. Alberta Mental Health Board Provincial Forensic Psychiatry Program. (2001-- Document In Progress). Community Geographic Team Resources: Provincial Forensic Psychiatry Needs Assessment
6 Stakeholder Consultations, conducted October – December 2001 with individuals involved with target population in select Alberta communities.

SSEECCTTIIOONN IIII COMMUNITY COLLABORATION Contents COLLABORATION AS A PREREQUISITE PROVINCIAL PROGRAM & COMMUNITY COLLABORATION
Collaboration As Integral To Introducing Diversion To The Community Collaboration In Forming A “Community Diversion Implementation Team”
COLLABORATION AT THE COMMUNITY LEVEL
Determining The Goals Determining Shared Responsibility Setting Up Processes For Diversion Developing The Community Communication Plan Developing The Evaluation Outcomes And Processes
…………………………….1 …………………………….2 …………………………….6

Section II: Community Collaboration page 1
CCOOLLLLAABBOORRAATTIIOONN AASS AA PPRREERREEQQUUIISSIITTEE:: TTOO DDEEVVEELLOOPPIINNGG AA CCOOMMMMUUNNIITTYY DDIIVVEERRSSIIOONN PPRROOGGRRAAMM Research and stakeholder consultations underscore the importance of collaboration in a
successful diversion program both at a provincial and a community level.1
In keeping with Health Canada’s Population Health Approach, the Provincial Diversion
Working Committee supports the statement that collaboration “calls for shared
responsibility and accountability”—in this case for individuals with mental illness who are
in conflict with the law, specifically in regards to their eligibility for diversion and their
involvement in appropriate care, support and treatment.2 Further, the document Best
Practices In Mental Health Reform: Discussion Paper (1997) states that of the unique
characteristics in Canada that have helped shape mental health reform and contribute to
future progress, one of the most important is that “many of the leaders and players within
mental health share a common core of beliefs about the value of collaboration and the
need to overcome vested interests in order to work effectively as a group” 3
In the context of Alberta’s Provincial Diversion Program, COLLABORATION is defined as
including the following:
The province’s and community’s focus on the common goal of ensuring the
provision of appropriate care, support and treatment for individuals with mental
illness who are in conflict with the law, regardless of the diversion point at which
the individual is determined to require services
The shared efforts by organizations, agencies, individuals and consumer
advocacy groups in achieving this goal—including clear communication regarding
processes, problems and successes; the sharing of resources, when necessary
Commitment to building relationships and to providing a coordinated response to
the needs of the target population
A recognition that collaboration and a common will results in community capacity
building (See Glossary in Appendix A for definition)
Clear communication between the community and the recognized provincial body
responsible for coordinating and evaluating the overall Alberta Provincial
Diversion Program.

Section II: Community Collaboration page 2
PPRROOVVIINNCCIIAALL PPRROOGGRRAAMM AANNDD CCOOMMMMUUNNIITTYY CCOOLLLLAABBOORRAATTIIOONN
A report commissioned by the Health and Enforcement in Partnership (HEP) steering
committee highlights five criteria from several Canadian projects in which collaboration
was successful.
1. Policy, whereby there is written direction that clearly supports collaboration, and if
necessary, authorizes individuals to work collaboratively
2. Coordination in the “orientation, training and evaluation of community resources
vis a vis project goals and program delivery”
3. Cooperation, wherein there is “trust and understanding of other partners and of
program objectives, and a willingness to leave professional egos at the door”
4. Ongoing communication among the project partners and with the community
5. Accountability, which includes “requirements for record-keeping and
monitoring…without sacrificing flexibility and street-level decision making” 4
Many new programs within communities would not come to fruition without leadership and
collaboration, or at minimum coordination, from the outset. Potential obstacles to the
success of a new program are often the lack of time and lack of community resources to
do the initial planning and to develop partnerships. Many community programs would not
exist without a collaborative effort in providing solutions for potential obstacles and without
a shared involvement in the program planning.
To support the need for collaboration early in the development of a community diversion
program, we can refer to the Calgary Diversion Project, which capitalized on the
resources and expertise of numerous community partners in its program planning. In an
effort to learn from Calgary’s early success and minimize obstacles, the Provincial
Diversion Working Committee recommends the following approach, which incorporates
collaboration as part of the development of the community diversion program from the
outset.
The approach to developing collaboration is as follows:

Section II: Community Collaboration page 3
1. Collaboration As Integral To Introducing Diversion To The Community
A collaborative approach starts with the initial discussions between the provincial
diversion representative and the community. This approach focuses on the following
steps as being integral to successful development of a community diversion program:
a) Initial Consultations with Community Stakeholders Designated member(s) of the Provincial Diversion Program will initially consult with
identified community stakeholders from the following groups, where appropriate:
Alberta Justice and Attorney General, Alberta Solicitor General, Alberta Health and
Wellness, the regional health authority, the community mental health clinic, and a
local consumer advocacy group that represents (and includes) family and clients.
Families and individuals with mental illness should be considered as partners and
resources that are fundamental to the collaborative process required in program
development and sustained success. In the case of an Aboriginal community,
additional representation from the specific treaty area, Metis Settlements, and/or
Metis Nation of Alberta is important, as well as any Aboriginal Police Services.
These initial consultations with the above stakeholders will assist in:
i) Understanding the Community Dynamics To begin with, a clear understanding of the nature of each specific diversion
community is necessary. As has been found in past projects in which
collaboration across ministries and agencies has been the foundation:
“…Projects must begin with a realistic appraisal, not just of
problems, but also of the capacity to solve those problems.
Solutions that work well for one participating group may spell
disaster for another if the capacity (in terms of manpower, training,
facilities and funding) is not there” 5
Such an evaluation allows for greater understanding of current issues and beliefs,
and, ultimately, fosters commitment to the community diversion program.

Section II: Community Collaboration page 4
ii) Assessing the Involvement of the Target Population with the Criminal Justice System
Determining the number of individuals who may be included in the target
population and the type and number of incidents that occur will help assess the
extent of the problem. This assessment should have some statistical support, for
instance, the number of incidents in which the local law enforcement suspect
mental illness as a contributing factor, or the number of individuals with suspected
mental illness who were incarcerated because of risk issues.
iii) Examining the Community Resources When evaluating the resources within the community, it is important to be as
comprehensive as possible including the following areas:
Services currently provided, including medical, mental health and
psychiatric services, addictions, housing, community supports—further
discussed in the Section V: Appropriate Care, Support and Treatment
Staffing resources and needs, including areas in which there is overlap of
services and/or greater need for communication
Services in kind, for instance, space resources that could be used for
meeting places for the community diversion group or other hardware or
equipment that may be needed by the program.
Part of evaluating the resources is to examine how organizations are providing
service to the target population, and what strengths and gaps may impact the
implementation of a diversion program. This process is most honest and
productive if it includes the following:
A written self-assessment by each organization/agency
An assessment of other stakeholder organizations based on past
experiences and interactions
An objective third party (in this case, the Provincial Diversion Program
representative) to record and summarize the information, as well as keep
the focus on the importance of collaboration.

Section II: Community Collaboration page 5
b) Expanding the Parameters of Collaboration Often community organizations that are not directly involved in providing services
to the target population may be interested in being part of the diversion process.
For instance, local church groups or recreation groups may be able to assist an
individual. They should be included at this point in order to further expand
potential resources for the target population, as well as enable greater community
involvement and eventually commitment.
2. Collaboration In Forming A “Community Diversion Implementation Team”
It is important to have the input from a large number of community stakeholders, not
only at the outset of community diversion program development but also at reasonable
intervals thereafter. However, depending on their size and the availability of
resources, communities may find it difficult to include all stakeholders in an advisory or
operational role at all times. It is recommended that based on the community
information and stakeholder interest, a Community Diversion Implementation Team is
established and formalized. The recommended size, structure and roles of this team
will be outlined next.

Section II: Community Collaboration page 6
CCOOLLLLAABBOORRAATTIIOONN AATT TTHHEE CCOOMMMMUUNNIITTYY LLEEVVEELL
Collaboration between the Provincial Diversion Program and the specific community is
expected to continue, with the provincial representative acting as a resource and being
part of program evaluation. However, once a community diversion program reaches this
stage in its development, the focus of the collaboration shifts more to the community level.
The Community Diversion Implementation Team becomes the focal point for further
planning of the diversion program, including the fostering of a collaborative environment.
It is important that the Community Diversion Implementation Team recognizes that
collaboration is more than simply encouraging organizations to work together and
connecting with or referring to services that are available to this target population.
Collaboration becomes the foundation of a diversion program, and, ultimately, the focus
on greater integration of services will change how business is done.
A good statement on how the Community Diversion Implementation Team should view
collaboration is provided in Health Canada’s Intersectoral Action Toolkit (2000), with the
following:
“Intersectoral Action means our work changes from… Competing → to building consensus Working alone → to including others from a range of cultures, fields and perspectives Thinking mostly about services and programs → to thinking about broader outcomes and strategies Focusing on short-term accomplishments → to seeking long-term outcomes and policy change Using the language of “I” → to using the language of “we” 6
It is these principles that shape the guidelines for the collaboration in a diversion program
within Alberta’s communities.

Section II: Community Collaboration page 7
1. Determining The Goals Although the overall purpose of diversion as it applies to this target population has
been outlined by the Provincial Diversion Working Committee, each community
requires short and long term diversion goals, specific to the client, the systems
involved, and the community as a whole.
Having a clear vision of what a community hopes to accomplish by having a diversion
program will strengthen the commitment by all stakeholders. It is also important to
make the goals relatively specific and time based. This will allow for better evaluation
of progress.
2. Determining Shared Responsibility Ultimately, one of the biggest issues in working together on a new program is who
does what…for how long. Research on other diversion projects clearly demonstrates
that without good leadership and a clear definition of roles, the collaboration required
for diversion tended to break down.7 The tendency to become “territorial” may
overshadow the needs of this target population—needs that transcend the boundaries
often set by funding and specific organization/agency goals.
a) Leadership: Since the specific dynamics within communities may dictate who
assumes a leadership role, the Provincial Diversion Working Committee provides
the following suggestions for leadership: A designated leader(s) of the community diversion program has a good
understanding of the criminal justice processes and of the mental health
needs of the target population.
The leadership is able to access resources required for any additional
planning and lobby for resources in areas that may be lacking.
The leadership may require two individuals, who act as co-leaders.
Time frames for leadership review/evaluation are incorporated within the
community plan.8
b) Definition of Roles: Defining the roles of partners involved in a community
diversion team is required for several reasons:

Section II: Community Collaboration page 8
Outlining what contributions each team member can provide to the
development of the program
Determining who speaks on behalf of the community diversion program
both in terms of communication with the Provincial Diversion Program, the
media, and ultimately the community
Deciding on a conflict resolution process, including who will facilitate such a
process.9
With true collaboration and sharing of information about each other’s services, the
goal would be that all partners have increased knowledge of what each
organization/agency does and what limitations and possibilities may exist in the
provision of services.
3. Setting Up Processes For Diversion As discussed in Section I: Diversion Points & Eligibility Criteria, three criteria are used
to determine whether an individual with mental illness who is in conflict with the law is
eligible for diversion at a given point: the nature of the offence, the individual’s
situation, and the community resources. To reiterate, not all communities may be in
the position of offering diversion as an option at all points. Further, the specific
processes for diverting an individual to appropriate care, support and treatment may
differ in communities.
Determining the processes for diversion will include the following:
a) Clearly deciding which diversion points are most applicable to a community.
Initially, for instance, a community may choose Diversion Point 3: Pre-Trial Case
Review as the focus of its program. There may still be informal diversion based on
a law enforcement officer’s discretion at Diversion Point 1a: First Contact with Law
Enforcement; however, formalized processes are not developed.
b) Once the diversion point(s) are agreed upon, the specific step-by-step processes/
protocols need to be developed (See Appendix B for an example from the Calgary
Diversion Project). These processes should address the following:
i) What processes are involved in securing consent for participation in diversion?
ii) Who contacts whom regarding the diversion candidate?
iii) Where is the diversion candidate referred to for determination of eligibility?

Section II: Community Collaboration page 9
iv) What specific assessments are carried out, particularly for mental health and
potential co-occurring addictions problems?
How does the information get shared? With the criminal justice system if
charges are involved? With other service providers?
What is the specific case management approach within the community?
(See Section V: Appropriate Care, Support and Treatment for further
discussion of Case Management.)
When does the involvement of one organization stop and another start in
the delivery of services?
When is the client “finished” with the diversion program? What happens
then?
What happens if the process breaks down?
Although general guidelines are provided for each main part of a typical diversion
program, the Community Diversion Implementation Team, with input from family and
clients, is responsible for the detailed, formalized processes.
4. Developing The Community Communication Plan Another partner in a diversion program is the community. A multitude of issues—
especially those around perceived community safety—can potentially derail a
diversion program within a community. Recent years of media focus on high profile
crimes involving individuals with mental illness may add to the existing stigma related
to the target population, even if the individual has committed only a minor offence.
Many factors may lead to an individual’s relapse, and such a relapse can possibly
place the diversion program in a negative light.
Collaboration, among diversion program team and stakeholders, and clear
communication can assist in informing and educating the community about the local
program.
The following are some points about the relationship between good collaboration and
good communication and how they should be reflected in a communication plan:
a) Collaboration means that everyone should understand and deliver the same
message about the goals and processes of the program

Section II: Community Collaboration page 10
b) Collaboration means that there is nothing to hide regarding the program and
process; there is transparency and subsequently accountability to the community
c) Collaboration means that the community is part of the diversion program and
receives regular communication about its progress.
5. Developing The Evaluation Outcomes And Processes Outlined in Section VI: Evaluation and Accountability is a strategy for evaluation, as
well as core components to guide the development of outcome measures. In
conjunction with the provincial diversion representative and in consultation with the
community diversion partners, each community will develop more specific outcomes
that relate to the delivery of services to individuals with mental illness who are in
conflict with the law.
In summary, the strength of a diversion program within a community is dependent on the
collaborative efforts of all stakeholders. Solving problems, which may develop regarding
the process or the services provided to the target population, is more effective if it involves
all partners. Ultimately, the success of a diversion program is dependent on developing
relationships and trust among the all stakeholders—the client, the criminal justice system,
the service providers and the community.

Section II: Community Collaboration page 11
EENNDDNNOOTTEESS 1 Steadman, H.J. et al. (2000). Comparing Outcomes of Major Models of Police Responses to Mental
Health Emergencies. Psychiatric Services, 51: 645-649. (This study found that it was essential to have collaboration between the criminal justice system, the mental health system, and the advocacy community plus essential services in order to reduce the inappropriate use of correctional facilities to house persons with acute mental illness.) Ontario's Human Services and Justice Coordination Project. (1996). A Provincial Strategy to Coordinate Human Services and Criminal Justice Systems in Ontario. Ontario Ministry of Attorney General, Ministry of Community and Social Services, Ministry of Health, Ministry of the Solicitor and Correctional Service. Health Canada. (1997). COLLABORATE! Health and Enforcement in Partnership: How to Build Partnerships for Alcohol and Other Drug Projects. Accessed on September 10, 2002 at http://www.hc-sc.gc.ca/hecs-sesc/cds/publications/collaborate/toc.htm. Preliminary Stakeholder Consultations, conducted by Provincial Diversion Working Committee representative. October – December 2001 with individuals involved with target population in select Alberta communities.
2 Health Canada Population Health Approach. What Determines Health? Accessed on November 28, 2002 at: http://www.hc.sc.gc.ca/hppb/phdd/determinants/e_determinants.html.
3 Health Systems Research Unit of Clarke Institute of Psychiatry. (1997). Best Practices in Mental HealthReform: Discussion Paper. Prepared for the Federal/Provincial/Territorial Advisory Network on MentalHealth.
4 Health Canada. (1995). Health and Enforcement in Partnership: How the police, justice, community groups, and health and social agencies are working together to build healthier, safer neighbourhoods. Accessed on August 09, 2001 at http://www.hc-sc.gc.ca/hecs-sesc/cds/publications/index.htm#public_research.
5 Health Canada. (1997). COLLABORATE! Health and Enforcement in Partnership: How to Build Partnerships for Alcohol and Other Drug Projects. Accesses on September 10, 2002 at http://www.hc-sc.gc.ca/hecs-sesc/cds/publications/collaborate/toc.htm
6 Health Canada. (2001). Intersectoral Action Toolkit: The Cloverleaf Model for Success.
7 Roskes, E. & Feldman, R. (December 1999). A Collaborative Community-Based Treatment Program for Offenders With Mental Illness, Psychiatric Services, 50 (12), p. 1614-1619.
8 Health Canada. (1997). COLLABORATE! Health and Enforcement in Partnership: How to Build Partnerships for Alcohol and Other Drug Projects. Accesses on September 10, 2002 at http://www.hc-sc.gc.ca/hecs-sesc/cds/publications/collaborate/toc.htm.
9 Health Canada. (1997). COLLABORATE! Health and Enforcement in Partnership: How to Build Partnerships for Alcohol and Other Drug Projects. Accesses on September 10, 2002 at http://www.hc-sc.gc.ca/hecs-sesc/cds/publications/collaborate/toc.htm.

SSEECCTTIIOONN IIIIII INFORMATION SHARING Contents THE SHARING OF INFORMATION: WITHIN A PROGRAM BUILT ON COLLABORATION PRINCIPLES FOR INFORMATION SHARING
Coordinated Services And Supports Consent Based Respect For Privacy Transparency
ALBERTA’S PRIVACY LEGISLATION
Freedom Of Information And Protection Of Privacy Act Health Information Act Alberta Alcohol And Drug Abuse Act
SAMPLE INFORMATION SHARING AGREEMENT SAMPLE CONSENT FORM
…………………………………………….……1 …………………………………………….……2 ………………………………………………….7 ………………………………………….……..17 ………………………………………………...22

Section III: Information Sharing page 1
TTHHEE SSHHAARRIINNGG OOFF IINNFFOORRMMAATTIIOONN:: WITHIN A PROGRAM BUILT ON COLLABORATION
Although the Provincial Diversion Working Committee promotes the need for a high degree of
collaboration within a successful diversion program, this collaboration must be achieved without
sacrificing the personal privacy of the target population. In this respect, there must be
parameters set for the type and amount of client information shared among diversion partners.
Processes and guidelines regarding the sharing of information are required in order to achieve a
balance between:
protecting the privacy of the target population
effectively providing the services required for appropriate care, support and treatment
and, ensuring the individual’s and community’s safety.
The need for information sharing within the Provincial Diversion Program is reflected in the
program’s primary purpose: “the redirection of individuals with mental illness from the criminal
justice system, whenever appropriate, to mental health, social and support services”.1 In order
to achieve this purpose, several systems—for instance, criminal justice, health, mental health,
and addictions—must work together. However, different privacy legislation governs these
systems.
This section discusses the underlying principles for sharing information about the target
population and provides the key elements of Alberta’s privacy legislation.
Section III: Information Sharing page 2
PPRRIINNCCIIPPLLEESS FFOORR IINNFFOORRMMAATTIIOONN SSHHAARRIINNGG In developing the principles for information sharing, the Provincial Diversion Working Committee
acknowledges the considerable work being done within Alberta on protocols for sharing of
information among service providers from different ministries. Within the Alberta Children and
Youth Initiative, a cross-ministerial Information Sharing Committee has been examining the
Freedom of Information and Protection of Privacy Act (FOIP) and the Health Information Act
(HIA), as well as other legislation that impacts the delivery of services through an integrated
system. In acknowledgement of their work, the Provincial Diversion Working Committee
supports the four guiding principles in the Information Sharing Policy (2002).2 Summarized and
applied to the diversion program’s target population, these principles include the following:
1. Coordinated Services And Supports
Despite the information sharing parameters set by FOIP and HIA, a community diversion
program must ensure that every effort is made to adopt a collaborative approach, since the
target population is often in need of supports that are provided by different ministries,
community and private organizations, family, and friends. For the effective provision of services
and supports, there is a need for coordination in the planning and delivery of services for this
target population.
These are some reasons for close communication, collaboration and—when appropriate and in
accordance with the applicable legislation—information sharing with partners in a diversion
program about the target population:
Determining an individual’s eligibility for diversion at a specific diversion point, which
is based on the nature of the offence, the individual’s situation (for instance, living
conditions and use of medication), and the community resources
Determining whether an individual poses a risk to self or to the community
Assessing whether an individual is in a crisis situation
Developing a diversion plan for appropriate care, support and treatment that best
meets the individual’s needs and most effectively utilizes the resources within the
community.
Each of the above reasons supports the need for some “sharing of information” among those
organizations involved in the criminal justice process as well as those involved in the delivery of
services related to appropriate care, support and treatment. However, in order to meet the

Section III: Information Sharing page 3
guidelines of the privacy legislation, clear controls and processes need to exist within each
community to ensure that the individual’s privacy is respected. To be successful, each
community diversion program requires a clear understanding of what constitutes “need to know” information and “with whom”.
2. Consent Based
All three of the key legislations—Freedom of Information and Protection of Privacy Act, Health
Information Act, and the Alcohol and Drug Abuse Act—focus on consent from the individual (and/or guardian) as being as fundamental to disclosure of information.
The Provincial Diversion Working Committee considers an individual’s involvement in mental
health care, support and treatment to be based on his/her voluntary participation, except
perhaps in situations involving hospitalization under the Mental Health Act. Therefore,
informed consent is necessary for an individual’s participation in a community diversion
program and for the sharing of any information among stakeholders. Even in situations in
which the courts mandate that an individual receive treatment, the general practice in Alberta is
to receive informed consent.
A consent form should include the requirements of both FOIP and HIA. A separate consent
form for AADAC is also required.
The specific sections of FOIP and HIA are included to illustrate what is expected of consent.

Section III: Information Sharing page 4
Freedom of Information and Protection of Privacy Act
6. Consent to the disclosure of personal information
The consent of an individual to a public body's using or disclosing any of the individual's personal information under sections 39(1)(b) or 40(1)(d) of the Act
a. must be in writing, and b. must specify to whom the personal information may be disclosed and how the personal
information may be used. AR 200/95 s6;170/98;216/99;251/2001
Health Information Act: Part 5 Disclosure of Health Information Disclosure of individually identifying health information to be with consent
34(1) Subject to sections 35 to 40, a custodian may disclose individually identifying health information to a
person other than the individual who is the subject of the information if the individual has consented to the
disclosure.
(2) A consent referred to in subsection (1) must be provided in writing or electronically and must include
a. an authorization for the custodian to disclose the health information specified in the consent,
b. the purpose for which the health information may be disclosed,
c. the identity of the person to whom the health information may be disclosed,
d. an acknowledgment that the individual providing the consent has been made aware of the reasons
why the health information is needed and the risks and benefits to the individual of consenting or
refusing to consent,
e. the date the consent is effective and the date, if any, on which the consent expires,
f. and a statement that the consent may be revoked at any time by the individual providing it.

Section III: Information Sharing page 5
3. Respect For Privacy
Within the requirements of existing legislation, only the relevant, minimal amount of
information about an individual involved in the diversion program may be shared. Each
community requires a clear indication of what information is considered relevant and minimal.
Each organization and agency providing services to the target population must be aware of
parameters, particularly:
what may be shared with whom
under what circumstances
what process is to be used in the sharing of information.
A Sample Scenario and Process Demonstrating Respect for Privacy: The potential diversion candidate is identified at Diversion Point 1a (Commission of an offence,
no charges by law enforcement). Out of respect for privacy, the law enforcement officer does
not share information about the individual with any other stakeholders involved in the community
diversion program.
However, the law enforcement officer feels that the individual would benefit from the diversion
program and provides a numbered Referral Card, which includes the address and contact name
of whoever is involved in coordinating the community diversion program. On the back of that
referral card, the officer may include the date of the incident, his/her name and contact
information. The law enforcement officer records the name and referral card # in his notes (and
eventually in a separate database)
If the individual follows through on the referral and presents the card, the coordinator then
requests that the individual sign a consent form prior to any further involvement with the
diversion program. If the individual consents, then the coordinator records the officer’s contact
information, date of incident and card referral #. If there is a need to contact the officer (and
with consent from the diversion client), then the referral card number can be used.
Overall, the individual’s privacy must be a consideration throughout his/her involvement with the
diversion program. Even during discussions within the case management team, individual
service providers should present only the “need to know” information that will assist other
members of the team in determining appropriate care, support and treatment.

Section III: Information Sharing page 6
4. Transparency
Individuals with mental illness who are in conflict with the law and who are eligible for diversion
must understand why and how information will be shared and how services will be provided and what legal consequences, if any, exist should they choose not to follow through
with the referral to diversion.
Not only the diversion client but also his/her family and community supports, if applicable and
included in the consent, should be aware of the diversion process, client’s responsibilities, and
service providers’ roles.
Overall, these above mentioned principles are intended to provide a guideline for community
diversion programs. Further development of information sharing protocols within the community
must take place in the diversion planning stages.
Section III: Information Sharing page 7
ALBERTA’S PRIVACY LEGISLATION Both provincial and federal legislation apply to Alberta’s Provincial Diversion Program. The two
specific Alberta Acts that deal with an individual’s privacy and access to information are the
Freedom of Information and Protection of Privacy Act (FOIP) and the Health Information Act
(HIA). Since some of the target population may have co-occurring mental health and addictions
problems, the privacy component of the Alberta Alcohol and Drug Abuse Act is examined.
Included are the key sections of each Act. Specific discussion regarding the impact of this
privacy legislation will be part of the implementation within each diversion community.
11.. Freedom Of Information And Protection Of Privacy Act 3 FOIP focuses on the requirements for providing access to information that is collected by and
held by government organizations (otherwise referred to as public bodies) or their affiliates.
The two specific sections of the FOIP legislation that are most relevant to a diversion program
are Section 17: Disclosure Harmful to Personal Privacy and Section 40: Disclosure of Personal
Information, included next:

Section III: Information Sharing page 8
(Note: The ellipsis (…) is used to show omitted text within the section of the legislation.)
Section 17 - Disclosure harmful to personal privacy
17(1) The head of a public body must refuse to disclose personal information to an applicant if the disclosure would be an unreasonable invasion of a third party's personal privacy.
(2) A disclosure of personal information is not an unreasonable invasion of a third party's personal privacy if (a) the third party has, in writing, consented to or requested the disclosure, (b) there are compelling circumstances affecting anyone's health or safety and notice of the disclosure is mailed to the last known address of the third party, (c) an Act of Alberta or Canada authorizes or requires the disclosure, (d) the disclosure is for research purposes and is in accordance with section 42 or 43,
…(3 omitted because of relevancy)
(4) A disclosure of personal information is presumed to be an unreasonable invasion of a third party's personal privacy if
(a) the personal information relates to a medical, psychiatric or psychological history, diagnosis, condition, treatment or evaluation, (b) the personal information is an identifiable part of a law enforcement record, except to the extent that the disclosure is necessary to dispose of the law enforcement matter or to continue an investigation, (c) the personal information relates to eligibility for income assistance or social service benefits or to the determination of benefit levels, (d) the personal information relates to employment or educational history, (e) the personal information was collected on a tax return or gathered for the purpose of collecting a tax, (f) the personal information consists of personal recommendations or evaluations, character references or personnel evaluations, (g) the personal information consists of the third party's name when
(i) it appears with other personal information about the third party, or (ii) the disclosure of the name itself would reveal personal information about the third party,
(5) In determining under subsections (1) and (4) whether a disclosure of personal information constitutes an unreasonable invasion of a third party's personal privacy, the head of a public body must consider all the relevant circumstances, including whether
(a) the disclosure is desirable for the purpose of subjecting the activities of the Government of Alberta or a public body to public scrutiny,
(b) the disclosure is likely to promote public health and safety or the protection of the environment,
(c) the personal information is relevant to a fair determination of the applicant's rights,
(d) the disclosure will assist in researching or validating the claims, disputes or grievances of aboriginal people,
(e) the third party will be exposed unfairly to financial or other harm,
(f) the personal information has been supplied in confidence,
(g) the personal information is likely to be inaccurate or unreliable,
(h) the disclosure may unfairly damage the reputation of any person referred to in the record requested by the applicant, and (i) the personal information was originally provided by the applicant.
1994 cF-18.5 s16;1999 c23 s9

Section III: Information Sharing page 9
Section 40 - Disclosure of personal information 40(1) A public body may disclose personal information only
(a) in accordance with Part 1, (b) if the disclosure would not be an unreasonable invasion of a third party's personal privacy under section 17. (c) for the purpose for which the information was collected or compiled or for a use consistent with that purpose, (d) if the individual the information is about has identified the information and consented, in the prescribed manner, to the disclosure, (e) for the purpose of complying with an enactment of Alberta or Canada or with a treaty, arrangement or agreement made under an enactment of Alberta or Canada, (f) for any purpose in accordance with an enactment of Alberta or Canada that authorizes or requires the disclosure, (g) for the purpose of complying with a subpoena, warrant or order issued or made by a court, person or body having jurisdiction to compel the production of information or with a rule of court that relates to the production of information, (h) to an officer or employee of the public body or to a member of the Executive Council, if the information is necessary for the performance of the duties of the officer, employee or member, (i) to an officer or employee of a public body or to a member of the Executive Council, if the disclosure is necessary for the delivery of a common or integrated program or service and for the performance of the duties of the officer or employee or member to whom the information is disclosed, (j) for the purpose of enforcing a legal right that the Government of Alberta or a public body has against any person, … (l) for the purpose of determining or verifying an individual's suitability or eligibility for a program or benefit, … (q) to a public body or a law enforcement agency in Canada to assist in an investigation
(i) undertaken with a view to a law enforcement proceeding, or (ii) from which a law enforcement proceeding is likely to result,
…
(s) so that the spouse, relative or friend of an injured, ill or deceased individual may be contacted, (t) in accordance with section 42 or 43. (u) to an expert for the purposes of section 18(2), (v) for use in a proceeding before a court or quasi-judicial body to which the Government of Alberta or a public body is a party,
… (aa) for the purpose of supervising an individual under the control or supervision of a correctional authority, (bb) when the information is available to the public, …
(ee) if the head of the public body believes, on reasonable grounds, that the disclosure will avert or minimize an imminent danger to the health or safety of any person, or
…(2 and 3 not relevant)
(4) A public body may disclose personal information only to the extent necessary to enable the public body to carry out the purposes described in subsections (1), (2) and (3) in a reasonable manner.
1994 cF-18.5 s38;1995 c17 s12;1996 c28 s21;1999 c23 s25

Section III: Information Sharing page 10
Section 17 is described as
“a balancing test to determine when disclosure of personal information would be an unreasonable invasion of a third party’s privacy. The test comes into play whenever someone other than the individual the information is about, or the individual’s authorized representative, makes a request for access to a record containing personal information about a third party.”4
The intent is that the public body that collected the information must weigh whether disclosure
may or may not be harmful to an individual’s personal privacy.
If within Section 40, disclosure is allowed then this section prevails. According to the FOIP
Guidelines and Practices (2002) three examples are: “disclosure with the consent of the
individual, disclosure required or authorized by an Act of Alberta or Canada, and disclosure for
research purposes”.5 To satisfy the disclosure rules of FOIP, a community diversion program
must ensure that as a first step to sharing information, an individual who is being considered
for a diversion program must consent to disclosure of clearly specified information with clearly
identified stakeholders for a clearly stated period of time.
Clearly, stakeholder groups involved in a community diversion program need to be familiar with
all relevant aspects of FOIP as well as those from the Health Information Act (HIA), which
governs the disclosure of information by health care and mental health service providers.

Section III: Information Sharing page 11
2. Health Information Act (HIA)66
The Health Information Act provides the rules for how health information is collected, used,
accessed by the individual, disclosed to third parties and maintained secure. Although like
FOIP there is a focus on an individual’s privacy, there is an additional allowance for sharing of
information, provided that the sharing is controlled. Those professions and organizations that
are identified as “custodians” may access health information that is necessary for their duties
related to providing health services.
Sharing health information with organizations or agencies that are not identified as custodians
may be done with limitations and only with consent, or, in some situations because of
considerable health or safety issues, consent may not be necessary. The appropriate sections
of the HIA are included. It is recommended that community diversion planning teams develop
information sharing processes that recognize the limitations of releasing health information.
Use of individually identifying health information 27(1) A custodian may use individually identifying health information in its custody or under its control for the following purposes:
a) providing health services;
b) determining or verifying the eligibility of an individual to receive a health service;
c) conducting investigations, discipline proceedings, practice reviews or inspections relating to the members of a health profession or health discipline;
d) conducting research
(i) if the custodian has submitted a proposal to an ethics committee in accordance with section 49
(ii) if the ethics committee is satisfied as to the matters referred to in section 50(1)(b), (iii) if the custodian has complied with or undertaken to comply with the conditions, if any, suggested by the ethics committee, and (iv) where the ethics committee recommends that consents should be obtained from the individuals who are the subjects of the health information to be used in the research, if those consents have been obtained;
e) providing for health services provider education;
f) carrying out any purpose authorized by an enactment of Alberta or Canada;
g) for internal management purposes, including planning, resource allocation, policy development, quality
improvement, monitoring, audit, evaluation, reporting, obtaining or processing payment for health services and human resource management.

Section III: Information Sharing page 12
(2) A custodian referred to in section 1(1)(f)(iii), (iv), (vii), (xii) or (xiii) may, in addition, use individually identifying health information in its custody or under its control to carry out the following functions within the geographic area in which the custodian has jurisdiction to promote the objectives for which the custodian is responsible: (a) planning and resource allocation; (b) health system management; (c) public health surveillance; (d) health policy development.
1999 cH-4.8 s27 Use of health information by affiliate 28 An affiliate of a custodian must not use health information in any manner that is not in accordance with the affiliate's duties to the custodian.
1999 cH-4.8 s28
The interpretation of two important phrases—health service and diagnostic, treatment and care
information—is included. It is recommended that each community diversion program examine
its resources and determine the effect of the HIA on the services provided by those resources.
Interpretation (m) "health service" means a service that is provided to an individual
(i) for any of the following purposes and is directly or indirectly and fully or partially paid for by the Department:
(A) protecting, promoting or maintaining physical and mental health; (B) preventing illness; (C) diagnosing and treating illness; (D) rehabilitation; (E) caring for the health needs of the ill, disabled, injured or dying,
…
(i) "diagnostic, treatment and care information" means information about any of the following:
(i) the physical and mental health of an individual; (ii) a health service provided to an individual;
… (iv) a drug as defined in the Pharmaceutical Profession Act provided to an individual;
(v) a health care aid, device, product, equipment or other item provided to an individual pursuant to a prescription or other authorization;
(vi) the amount of any benefit paid or payable under the Alberta Health Care Insurance Act or any other
amount paid or payable in respect of a health service provided to an individual,
It is recommended that each diversion community be fully aware of when consent is necessary
and when information may be shared without the individual’s consent. Policies and processes
are required regarding the following two sections as they apply to a community’s diversion
program.

Section III: Information Sharing page 13
Disclosure of individually identifying health information to be with consent 34(1) Subject to sections 35 to 40, a custodian may disclose individually identifying health information to a person other than the individual who is the subject of the information if the individual has consented to the disclosure. … (specifics of consent discussed separately) (3) A disclosure of health information pursuant to this section must be carried out in accordance with the terms of the consent. (4) A revocation of a consent must be provided in writing or electronically. (5) A consent or revocation of a consent that is provided in writing must be signed by the person providing it. (6) A consent or revocation of a consent that is provided electronically is valid only if it complies with the requirements set out in the regulations.
1999 cH-4.8 s34
Disclosure of diagnostic, treatment and care information 35(1) A custodian may disclose individually identifying diagnostic, treatment and care information without the consent of the individual who is the subject of the information (a) to another custodian for any or all of the purposes listed in section 27(1) or (2), as the case may be, (b) to a person who is responsible for providing continuing treatment and care to the individual, (c) to family members of the individual or to another person with whom the individual is believed to have a close
personal relationship, if the information is given in general terms and concerns the presence, location, condition, diagnosis, progress and prognosis of the individual on the day on which the information is disclosed and the disclosure is not contrary to the express request of the individual,
(d) where an individual is injured, ill or deceased, so that family members of the individual or another person with whom the individual is believed to have a close personal relationship or a friend of the individual can be contacted, if the disclosure is not contrary to the express request of the individual,
(e) to an official of a penal or other custodial institution in which the individual is being lawfully detained if the purpose of the disclosure is to allow the provision of health services to the individual,
… (g) to a committee that has as its primary purpose the carrying out of quality assurance activities within the
meaning of section 9 of the Alberta Evidence Act,
(h) for the purpose of a court proceeding or a proceeding before a quasi-judicial body to which the custodian is a party, (i) for the purpose of complying with a subpoena, warrant or order issued or made by a court, person or body having jurisdiction to compel the production of information or with a rule of court that relates to the production of information, (j) to a municipal or provincial police service for the purpose of investigating an offence involving a life-threatening personal injury to the individual, if the disclosure is not contrary to the express request of the individual,
… (m) to any person if the custodian believes, on reasonable grounds, that the disclosure will avert or minimize an imminent danger to the health or safety of any person,

Section III: Information Sharing page 14
(n) if that individual lacks the mental capacity to provide a consent and, in the opinion of the custodian, disclosure is in the best interests of the individual,
… (p) if the disclosure is authorized or required by an enactment of Alberta or Canada, or (q) to its successor where
(i) the custodian is transferring its records to the successor as a result of the custodian ceasing to be a custodian, and
(ii) the successor is a custodian.
(2) A committee to which health information is disclosed pursuant to subsection (1)(g) must not disclose the information to any other person except in accordance with subsection (3). (3) A committee referred to in subsection (2) may disclose non-identifying health information to another committee that has as its primary purpose the carrying out of quality assurance activities within the meaning of section 9 of the Alberta Evidence Act.
1999 cH-4.8 s35
Disclosure of registration information 36 A custodian may disclose individually identifying registration information without the consent of the individual
who is the subject of the information (a) for any of the purposes for which diagnostic, treatment and care information may be disclosed under section 35(1) or (4), … (c) to a person who is not a custodian if the disclosure is in accordance with the requirements set out in the regulations.
1999 cH-4.8 s36

Section III: Information Sharing page 15
3. Alberta Alcohol And Drug Abuse Act 7
This Act prevails over FOIP and HIA in regard to the sharing of information about clients
involved with AADAC. In this regard, consent from the client will be required by AADAC to
share information with other stakeholders. The process for obtaining consent needs to be
developed within each community. As well, the process should address the issue of what
happens to the case management process if a client does not consent to the release of
information from AADAC but has consented to be involved in the diversion program. The
relevant section of the Act follows:
Secrecy of information CHAPTER A-38 8(1) Except as otherwise provided in this section
(a) a person who is or has been a member or employee of the Commission or is or has been employed or engaged in the administration of this Act shall not disclose or be compelled to disclose any information obtained by him that names or identifies a client who has been provided with treatment, care or services by the Commission, and
(b) any file, record, document or paper in the custody of the Commission that names or identifies a client who has been provided with treatment, care or services by the Commission shall not be disclosed to any person or be admitted in evidence in any proceedings.
(2) In this section "client" means a person who has been provided with treatment, care or other services by the Commission or at a hospital, clinic or centre operated by the Commission. (3) Subsection (1) does not apply
(a) when the disclosure is necessarily made in the course of the administration of the business and affairs of the Commission or in the course of the administration of this Act,
(a.1) if there are compelling circumstances affecting anyone's health or safety and notice of the disclosure is mailed to the last known address of the client,
(b) when the disclosure is made at the request of or with the consent of the client concerned or of a guardian or trustee of the client appointed under the Dependent Adults Act or the Public Trustee Act,
(c) in any special case when permission is given by an order of the Lieutenant Governor in Council, or
(d) when the disclosure is made in respect of a deceased client to a medical examiner appointed under the Fatality Inquiries Act.
(…4 not relevant to Diversion)
(5) Information in the hands of the Commission pertaining to clients and the treatment, care and services provided to clients may be published by the Commission or the Government in statistical form if the individual names of clients are not thereby revealed or made identifiable.
(6) A person who contravenes this section is guilty of an offence and liable to a fine of not more than $500 and in default of payment to imprisonment for a term of not more than 90 days. (7) If the Provincial Court issues a subpoena pursuant to the Child Welfare Act, the Commission or an employee of the Commission shall release, in accordance with that Act, any information, file, record, document or paper in respect of the child to whom the proceedings before the Provincial Court relate or with respect to a guardian of that child.
RSA 1980 cA-38 s8;1984 cC-8.1 s98;1985 c6 s6;1998 c4 s2

Section III: Information Sharing page 16
IINNFFOORRMMAATTIIOONN SSHHAARRIINNGG AAGGRREEEEMMEENNTTSS Since a number of pieces of legislation may be involved in a specific diversion case, each
community should establish information sharing agreements between the organizations and
agencies involved in the diversion program. (see the Sample Information Sharing Agreement
from the Calgary Diversion Project at the end of this section.)
The areas that should be covered within an information sharing agreement include:
1. Limiting The Information Sharing Based On the Diversion Point Even with a standard information sharing agreement, each community must develop procedures
that limit the access to information based on the individual’s point of entry to the diversion
program.
2. Determining When To Obtain Consent And By Whom Based on the diversion program structure within a community, there needs to be a clear process
for obtaining consent. For instance, using the previous example situation, consent for
involvement in the program would be provided at the time the individual follows through on the
referral, possibly at the local mental health clinic or other designated diversion program location.
3. Sharing Of Information Within Case Management Team Because a case management team may be involved with the provision of care, support and
treatment, a representative from each organization/agency should be listed in the Information
Sharing Agreement.
4. Storing Information About The Client Determining how information will be transferred from service provider to service provider (with
consent) and who will store the information in a secure place needs to be addressed in the
information sharing agreement.
Following is a sample of the Calgary Diversion Project Information and Sharing Agreement,
which has been reviewed by various legal professionals. Communities may use this agreement
as a guide.

Section III: Information Sharing page 17
Sample Agreement from Calgary Diversion Project
INFORMATION AND SHARING AGREEMENT
This agreement, made in triplicate and entered into this day of , 2002 BY AND BETWEEN:
The Calgary Police Service (hereinafter referred to as CPS)
and
Alberta Mental Health Board
(hereinafter referred to as AMHB)
WHEREAS the purpose of the Calgary Diversion Project (hereinafter referred to as the “CDP”) is
to redirect persons suffering or believed to be suffering from a mental disorder or a mental disorder with a concurrent substance abuse disorder, who have been arrested for minor, non-violent crime, from the Justice system to community-based health programs and/or to community support services.
AND WHEREAS the Alberta Mental Health Board (AMHB) is the primary operator of the CDP and
the CPS is one of a number of partners working in cooperation with the AMHB on this project. AND WHEREAS the AMHB and CPS are entering into this agreement for the purpose of
disclosing and sharing necessary personal information, primarily with the consent of the participants, in order for CDP Administrators to determine suitability of participants, conduct assessments of participants, and, upon conclusion of the program, evaluate the success of the program.
AND WHEREAS the Province of Alberta has dedicated 1.4 million dollars in funding from a grant
through the Alberta Health and Wellness Innovation Fund for a three-year period.
AND WHEREAS AMHB and CPS recognize the participation and cooperation of other stakeholders in this project, those being the Alberta Solicitor General, Alberta Justice, Calgary Health Region, the Crown Prosecutor’s Office, Alberta Alcohol and Drug Abuse Commission, Calgary Remand Centre, Community Mental Health Services Planning Committee and the Salvation Army.
THEREFORE in consideration of the mutual covenants and agreements contained herein, the parties agree as follows: I. DEFINITIONS
1. “ACT” means the Freedom of Information and Protection of Privacy Act, RSA 2000,
Chapter F-25. 2. “BOOKING SHEET” means a form containing personal information including a
photograph, which is completed when an offender is processed through the Arrest Processing Unit (APU).
3. “CDP Administrators” means: (names listed)

Section III: Information Sharing page 18
“OFFENDER” means a person charged with an offence under an enactment of Alberta or Canada.
4. “PARTICIPANT” means persons that are participating in the CDP or are
being considered for the CDP.
5. “PERSONAL INFORMATION” means recorded information about an identifiable individual, including
i. the individual’s name, home or business address or home or business telephone number,
ii. the individual’s race, national or ethnic origin, colour or religious or political beliefs or associations,
iii. the individual’s age, sex, marital status or family status,
iv. an identifying number, symbol or other particular assigned to the individual,
v. the individual’s fingerprints, blood type or inheritable characteristics,
vi. information about the individual’s health and health care history, including information about a physical or mental disability,
vii. information about the individual’s educational, financial, employment or criminal history, including criminal records where a pardon has been given,
viii. anyone else’s opinions about the individual, and
ix. the individual’s personal views or opinions, except if they are about someone else.
6. “RELEVANT CRIMINAL HISTORY” means Criminal Code charges, charges pursuant to
the Gaming and Liquor Act and offences under local bylaws (e.g.: no ticket on the LRT).
II. EFFECTIVE DATE AND TERM OF THIS AGREEMENT
7. As soon as this agreement has been signed, or earlier as has been agreed between the parties, the CPS will participate and disclose personal information of potential participants to the CDP until the completion of the pilot project in June 2004.
8. Upon the completion of the pilot project CPS will continue to disclose the Relevant
Criminal History, and the Personal Information Management System report (PIMS report) of participants to the CDP in order to facilitate the post 18-month criminal history requirement as described ….
9. AMHB hereby agrees to destroy, by shredding, or in the case of a record in an electronic
form by deleting, writing over or otherwise rendering the record illegible, all records containing personal information received by the AMHB for the purposes of the CDP on or before July 30, 2005.

Section III: Information Sharing page 19
III. ACCESS TO INFORMATION
10. Appendix “A” attached to this agreement describes the research project and scope of the information being requested.
11. The AMHB may use the personal information only for the research purpose set out in the
agreement. If the AMHB wishes to use personal information for any other purpose, the AMHB must obtain written authorization from the CPS.
12. Initial screening will be performed by the Arrest Processing Unit (APU) Staff Sergeant. When an individual has committed a minor offense, is at low risk, and is suspected to suffer from mental illness, the Staff Sergeant at APU will recommend to the presiding Justice of the Peace that the offender be referred to the CDP.
13. When a participant has been identified for possible eligibility for the CDP, the Staff
Sergeant will supply the booking sheet, and accompanying photo, to the CDP Administrators without the necessity of obtaining a signed consent of the participant, in accordance with section 40(1)(b), (i) and (l) of the Act.
14. The purpose of disclosing the booking sheet to CDP Administrators is to enable the CDP
Administrators to contact the potential participant for the purpose of conducting an assessment. The AMHB acknowledges that the CDP Administrators may subsequently contact the participant from the information provided on the booking sheet to determine suitability and willingness to participate in the CDP.
15. In order to determine the suitability of participants for the CDP, participants will be
contacted by the CDP Administrators in order to conduct an initial assessment. In addition participants will be contacted in order to co-ordinate community treatment and support services, depending on the specific needs of each participant.
16. Participants in the CDP must consent in writing to the disclosure of their personal
information, other than the booking sheet and photograph described in paragraph 14, in order for the CDP Administrators to assess and determine a potential participant’s suitability. Attached as Exhibit “B” is the consent form which must be completed by participants.
17. Once the booking sheet is received by the CDP Administrators and in the event the
participant withdraws from the CDP, the AMHB will destroy the booking sheet by shredding it, or in the case of an electronic form, by deleting, writing over or otherwise rendering the record illegible, as soon as is practicable.
18. The CPS, upon receiving a copy of the signed consent form from the participant, will
disclose to the CDP the entire Relevant Criminal History (CR 2) and the Patient Care Report (PCR) of the participant.
19. CPS will make available to the CDP the Relevant Criminal History Reports (CR 2s), and
the PIMS report, for 18-months following the participant’s completion of the Project. The parties acknowledge that disclosure of the Relevant Criminal History Report for this additional period is necessary for the purpose of tracking any subsequent rates of recidivism, such as arrests, court appearances, or mental health relapses, which will assist in measuring the success of the program.
20. In the event that there is a discrepancy between the records requested above and
the records requested in the Proposal to Access Personal Information for Research or Statistical Purposes, the information in this agreement governs the agreement.

Section III: Information Sharing page 20
IV. CONFIDENTIALITY AND STORAGE OF INFORMATION
21. All copies of records and notes, which contain personal information, will be stored at the following address: The Calgary Diversion Project Centre of Hope 420 – 9th Ave S.E. Calgary Alberta
22. In accordance with section 42(d) of the Act, the AMHB agrees and covenants to keep
confidential and not disclose to persons, other than those listed or defined as CDP Administrators, personal information supplied by the CPS for the purpose of assessing and evaluating potential and actual participants in the CDP and for research and analysis.
23. Security at the CDP Centre of Hope, 420 – 9th Avenue SE, will be maintained by ensuring
that the door leading into the storage area be securely locked. The CDP Administrators agree to store all documents within a locked cabinet in a locked office. Individually identifiable information from the records will be maintained on a computer system to which only CDP Administrators will have access and will be restricted through the use of passwords and by other security measures that prevent unauthorized access.
24. Upon the participant’s completion of his or her participation in the CDP, the AMHB will
ensure that all personal identifiers are stripped from all information received from the CPS when the AMHB conducts research, evaluation and analysis. An internal study ID number, replacing the personal identifiers, will be assigned to each participant in order to generate profiles, identifying characteristics of those most suited for diversion and track any future criminal activity and relapse into the mental health system of participants.
25. A separate database, used for evaluation purposes, will be created by the AMHB, which
will not contain any personal identifiers collected. External study IDs will be used to manage data collection.
V. DIVERSION PROJECT MEMBERS/ASSISTANTS
26. CDP Administrators must in writing notify the CPS immediately if he or she become
aware that any of the conditions set out in this agreement has been breached. 27. The following named persons will have access to personal information for the purpose of
reviewing, analyzing and evaluating the information: 28. No other persons other than those named in paragraph 28 shall have access to personal
information without the prior written consent of the CPS. Any changes to the list of persons having access to personal information at CDP will be submitted in writing to CPS and CPS reserves the right to require that the new individual submit to a security clearance which is to the satisfaction of the CPS.
29. Database administrators, or other persons engaged in a technical support role, may have
temporary access to personal information without the prior approval of CPS, as determined by Fran Barnes, the Manager of the CDP. The persons referred to in this paragraph may have access to personal information without prior approval, for the purpose of engaging in repair work, or other technical support work in association with the operations of the CDP.

Section III: Information Sharing page 21
30. The CPS may conduct security checks for the persons listed in paragraph 28 and any other persons who are deemed to be necessary for the operations of the CDP. All persons will be informed of these security checks, if they are conducted.
31. Fran Barnes, Manager of the CDP will be responsible for ensuring that there is no
disclosure of the information related to the CDP by other members of the CDP. VI. PUBLICATION RIGHTS
32. The AMHB agrees and covenants not to identify, either directly or indirectly, any person
participating in the project in any paper, article or presentation. AMHB further acknowledges and promises that it shall ensure that no other members of the CDP will identify, either directly or indirectly, any participant or any individual whose personal information was supplied by the CPS to the AMHB, or persons interviewed in the course of the evaluations.
33. The AMHB shall provide copies of any proposed publication relating to this Agreement to
the CPS, at least thirty days (30) in advance of presentation or publication. If the CPS does not object, in writing, to such disclosure within fifteen (15) days of receipt, the AMHB shall be free to proceed with the presentation or publication.
34. In the event of a written objection being supplied by the CPS, the parties shall negotiate
an acceptable version of the proposed disclosure, including the release date, within the thirty-day (30) notice period as defined in paragraph 34.
VII. COPYRIGHTS
35. Copyright in any reports will be jointly held by the CPS, the AMHB, and the CDP.
VIII. INDEMNIFICATION
36. To the fullest extent permitted by law, the AMHB, agrees to indemnify and save harmless
the CPS of and from all manner of actions, causes of action, proceedings, claims, demands, losses, costs, damages and expenses of whatsoever nature and kind which may be brought or made against the CPS or which the CPS may suffer, sustain, pay or incur as a result or in connection with the negligence, willful misconduct or breach by the AMHB of its obligations as per this Agreement.
To the fullest extent permitted by law, the CPS agrees to indemnify and save harmless the AMHB of and from all manner of actions, causes of actions, proceedings, claims, demands, losses, costs, damages and expenses whatsoever nature and kind which may be brought or made against the AMHB or which the AMHB may suffer, sustain, pay or incur as a result or in connection with the negligence, willful misconduct or breach by the CPS of its obligations as per this Agreement.
37. The provision of paragraph 37 shall survive the duration of this information sharing
agreement for any reason whatsoever.
IX. NOTICES 38. Any notices or other communications required or permitted to be given hereunder, must
be in writing given by either next-day courier, facsimile or other means of electronic communication and addressed as follows:
If to CPS: Names of Committee Chairpersons included
IN WITNESS WHEREOF the parties hereto have executed this Agreement the day and year first above set forth Signatures included

Section III: Information Sharing page 22
Sample Consent Form
Calgary Diversion Project Client Consent to Participate and Disclosure of Information
I ,__________________________ consent to disclosure of information about me so that:
my health registration assessment, diagnostic and treatment information can be shared with partner agencies to get me the services I need. (These partners may include: the Salvation Army, the Calgary Health Region, the Alberta Mental Health Board, and the Alberta Alcohol and Drug Abuse Commission.)
• information about my relevant criminal history can be obtained on me to date and over the next 18 months.
• the Diversion Project will keep my treatment information separate from my justice information, and will not share my arrest history.
• my name will not be used in any reports • the information will be kept strictly confidential and secure in locked cabinets and
secure databases. I understand the risks and benefits to me of participating in the Diversion Project, or refusing to participate. I know I have the right to revoke this consent to participate in the Diversion Project at any time in writing and return to the Justice system. I agree to participate in the Calgary Diversion Project. YES____ NO___ ______________________________ ____________ Participant’s Signature Date ______________________________ Participant’s Name (PRINT) ______________________________________________ ____________ Diversion Project Manager or delegate’s signature Date ________________________________ Diversion Staff Name (PRINT) If you have any questions or issues concerning this Project, you may contact Fran Barnes, Manager of the Diversion Project at (403) 410-1132
A copy of this consent form must be given to the participant
Revised November 26, 2002
Section III: Information Sharing page 23
In summary, there is fine balance between operating an effective diversion program based on
collaboration among community stakeholders and ensuring the protection of an individual’s
privacy. Certain issues may arise in which diversion is not possible because of the limitations
within the privacy legislation. The Provincial Diversion Working Committee recognizes these
potential limitations and the need for further discussion of the legislation, in particular the Health
Information Act.
In the meantime, communities are encouraged to work closely with the Provincial Diversion
Working Committee representatives who are assisting in the planning of a program to ensure
that there is adherence to the legislation within each community’s diversion guidelines and
processes.

Section III: Information Sharing page 24
EENNDDNNOOTTEESS 1 Provincial Diversion Framework Working Committee. (2001). Alberta’s Provincial Diversion Framework:
Reducing the Criminalization of Individuals with Mental illness.
2 Alberta Children and Youth Initiative. (October 23, 2002). Information Sharing: Policy Framework. (Draft).
3 Freedom of Information and Protection of Privacy Act (FOIP) (cF-25 RSA 2000)
4 Government of Alberta. (2002). Freedom of Information and Protection of Privacy: Human Resources Guide for Local Public Bodies.
5 Government of Alberta. (2002). Freedom of Information and Protection of Privacy: Human Resources Guide for Local Public Bodies.
6 Health Information Act (HIA) (cH-5 RSA 2000)
7 Alberta Alcohol and Drug Abuse Act RSA 2000,Chapter A-38 http://www.qp.gov.ab.ca/Documents/acts/A38.CFM

SSEECCTTIIOONN IIVV EDUCATION & TRAINING Contents THE RELATIONSHIP OF EDUCATION/TRAINING TO COLLABORATION
The Goals EDUCATION/TRAINING DEFINED IN THE CONTEXT OF DIVERSION APPROACH TO EDUCATION/TRAINING
Determining The Community’s Education / Training Needs Anticipating Potential Questions And Concerns Incorporating Education/Training In Community Diversion Program Development Developing A Plan And Schedule
The Roles and Responsibilities of Service Providers Mental Illness and the Client Needs The Criminal Justice Process Service Provider Roles and Limitations Legislation That May Impact the Diversion Process Diversion Protocols and Processes Ongoing Training for Service Providers
SAMPLE EDUCATION AND TRAINING MODULES
Mental Disturbance (Calgary Diversion Project) Substance Abuse and Mental Illness (Calgary Diversion Project) Medication and Mental Illness (Calgary Diversion Project) Risk Assessment (Calgary Diversion Project)
PROFESSIONAL DEVELOPMENT EDUCATING THE COMMUNITY ABOUT DIVERSION: THE COMMUNICATION PLAN
………………………..1 ………………………..2 ………………………..4 ………………………13 ………………………17 ………………………17

Section IV: Education and Training page 1
TTHHEE RREELLAATTIIOONNSSHHIIPP OOFF EEDDUUCCAATTIIOONN//TTRRAAIINNIINNGG TTOO CCOOLLLLAABBOORRAATTIIOONN Education/training and collaboration go hand in hand in the development of a community
diversion program. Effective collaboration among stakeholders, clients and family is
dependent on the knowledge and understanding that each has about the other’s roles,
expectations, limitations and goals regarding the target population. This can be
accomplished only through a systematic and ongoing process of educating and training of
all service providers, criminal justice personnel, and the community on the diversion
program and on the needs and characteristics of the target population. Doing so will
assist in the community’s efforts to collaborate in order to provide the most seamless
provision of services possible.
Better understanding of the partners in a diversion program leads to better understanding
of the client’s needs and available community resources, which in turn contributes to the
success of a community diversion program. As an example, it has been cited that training
of law enforcement officers by mental health providers, family advocates and mental
health consumer groups resulted in much more than knowledge: “it promote[d] a
philosophy of responsibility and accountability to consumers of mental health services,
their relatives and the community”.1 Similarly, training of mental health professionals and
other service providers about the criminal justice processes leads to a greater
understanding of the process and related needs.
The Calgary Diversion Project recognized the importance of providing education about
diversion early in its diversion program development. In order to receive quality referrals
from members of the criminal justice system, the project educated law enforcement,
justices of the peace, Crown, defense counsel, judges and remand center staff (just to
name a few) about the target population, the referral process, the diversion program and
the anticipated outcome. 2

Section IV: Education and Training page 2
The Goals Of Education/Training
Incorporating education/training in the development of a community diversion program is
based on the following goals:
To provide for a forum in which all community diversion partners can better
understand the distinct roles of all service providers, the limitations of each role,
and the areas of overlap. Although each partner in a community diversion
program is familiar with his/her own ministry’s or organization’s structures and
roles, there is also a need to understand how those roles and goals can work
together for a common integrated service.
To learn specifics about the target population such as the definition of mental
illness, the relationship between mental illness and substance abuse, techniques
for intervening in a crisis, the need for and effects of psychotropic medications,
treatment modalities, clients’ rights and responsibilities, the parameters set by
legislation, among others.3
To ensure that all diversion partners are familiar with the diversion processes at
the community’s chosen diversion points or know where to get information.
To understand the relevant aspects of the criminal justice process as it relates to
the client at each diversion point.
To relate the community diversion goals and anticipated outcomes to the diversion
program.
EEDDUUCCAATTIIOONN//TTRRAAIINNIINNGG DDEEFFIINNEEDD IINN TTHHEE CCOONNTTEEXXTT OOFF DDIIVVEERRSSIIOONN Two types of education/training are important to the success of a community diversion
program. The first is the education and training as they specifically relate to the
implementation and continued success of diversion within a community. The second is
the further education and training that may be necessary in some communities to enhance
the professional skill levels of individuals involved in the provision of appropriate care,
support and treatment for this target population.
The primary focus of this section is on education and training necessary to the
development of a community diversion program. A brief discussion of opportunities for

Section IV: Education and Training page 3
further professional education/development is also provided; however, a more
comprehensive discussion will be included in Phase Two of the Provincial Diversion
Program implementation.
To discuss education and training as it relates to a community diversion program, we first
provide some distinction between the two terms:
In the context of a diversion program, EDUCATION refers to acquiring knowledge that
increases an individual or community’s understanding of the objectives of a diversion
program and its significance within the community, with the intent that a shared
philosophy be developed. It refers to the providing of information, general concepts, and
theories that relate to the overall diversion program; a development of an understanding of
the need for integration of services across the continuum of care; and, increased
knowledge of the characteristics and needs of the target population, and the relationship
between the client, family and community.4
The ultimate goal of education is to assist communities with the development of their
diversion programs and to foster a greater understanding of the goals of diversion and the
needs of the target population.
Professional education (professional development) refers specifically to the education
provided via courses and affiliated with educational institutions or professional bodies.
In the context of diversion, TRAINING focuses on the practical level of learning a skill by
instruction or practice. One goal of this training may be to bring an individual or group to a
desired standard of performance.5
Training also refers to the sharing of specific information related to the roles, processes,
and limitations of each diversion partner. The training is designed for all diversion
partners and may be in the form of workshops, ride-alongs, or job shadowing, or be based
on written material describing each participating organization’s goals and processes or
key workers’ roles.

Section IV: Education and Training page 4
AAPPPPRROOAACCHH TTOO EEDDUUCCAATTIIOONN//TTRRAAIINNIINNGG Incorporating education/training in a community diversion program is not difficult, although
it may require a time commitment at the outset. Because of this commitment of time and
other profession-related biases, some diversion partners may resist being involved in the
education/training process. The following approach may help:
1) Identify all potential audiences within the community and their
information/education needs
2) Anticipate potential questions and concerns that may be raised by each
audience
3) Incorporate the education/training in the initial program development, at the
stage at which all potential partners are identified
4) Set up a plan for providing education/ training at different stages of the
community diversion program development. Within this plan, include diversion
partners as “trainers” on the roles and processes of their organization and take
the “classroom” to the location of specific diversion partners, should it be
appropriate, in order to foster greater understanding.6
This approach works best if it involves the key stakeholders in its development. In
conjunction with the Provincial Diversion Program representative (especially in the initial
planning), identify potential groups or individuals to assist in the education process. For
instance, the local chapter of the Schizophrenia Society of Alberta, where appropriate,
may have family or clients who are willing to be involved in increasing the understanding
of stakeholders about mental illness and related needs.
1. Determining The Community’s Education/Training Needs
A complete assessment of the potential stakeholders involved, their roles, and their
potential education, professional development and training needs is suggested. As well, it
may be useful to examine existing sources for workshops on specialized topics related to
mental illness and/or addictions.
The following is a list of potential stakeholders who may either require further training
about some aspect of the community diversion program or have expertise that can be
utilized in providing training to others.

Section IV: Education and Training page 5
♦ Mental health professionals, including community clinics and specialized programs:
the specific processes of law enforcement and criminal justice systems; the
limitations of law enforcement authority in certain situations
♦ Law enforcement, including supervisory staff, arrest processing units: ways to
recognize mental illness, methods of dealing with psychotic behavior, strategies to
address a person who is threatening suicide, and the process for accessing either
mobile crisis teams or local hospital emergency services; general classification of
mental disorders used by mental health professionals
♦ Addictions personnel: how to deal with co-occurring mental health and substance
abuse disorders within the community diversion program
♦ Social and support services, such as those involved with accommodations,
Assured Income for the Severely Handicapped (AISH), aids to daily living,
transition, advocacy: the diversion process, ways to recognize mental health crisis
and the action to take both in terms of dealing with the crisis and the process for
accessing other services
♦ Families, guardians, and/or peer groups: the diversion process, their role in the
provision of support, and appropriate response to a mental health crisis and the
process for accessing other services
♦ General Practitioners and local hospital emergency staff: the diversion process, law
enforcement’s role, and steps to follow if they encounter an individual in crisis who
has been brought in by law enforcement
♦ Pharmacists, in terms of how they can assist with providing information on
medication and medication compliance, which can be especially helpful to families,
law enforcement personnel, and other service providers
♦ Courts, including relevant court workers, Crown prosecutors, defense, judges,
justices of the peace: the diversion process, their roles in the process, and the type
of care, support and treatment available via the community diversion program
♦ Probation: the relationship between probation orders and the provision of
appropriate care, support and treatment
♦ Corrections, if applicable: the relationship between programs within corrections
facilities and potential reintegration
♦ Ethnocultural support networks, in general, and with specific focus on Aboriginal
communities: the diversion process, signs and symptoms of mental illness, and
dealing with crisis situations. For those directly involved in diversion: how to

Section IV: Education and Training page 6
discuss mental illness and associated stigma with a specific community or group;
how to bridge the gap or collaborate within the community and with organizations
and agencies providing services outside of the specific ethnocultural community
♦ General Public, as part of the Communication Plan: the diversion process, the
goals of diversion, the impact on the community, and issues of safety.
Within each diversion community, the needs and expertise of all stakeholders should be
detailed in consultation with representatives from each of these groups.
2. Anticipating Potential Questions And Concerns
As with anything new, especially system related, there might be questions, concerns,
objections and possibly opposition. As part of the education and training process—which
also informs the development of a communication plan—it is important to understand as
much as possible about the audience/stakeholders, including the following:
♦ Approximate level of education and professional training
♦ Specific mandates of organizations, agencies, and other support groups
♦ Existing barriers to previously attempted collaboration and coordination efforts
♦ Identified community leaders related to each specific group, including their personal
frames of reference based on past experience, and the level of their potential
support (or resistance)
♦ The specific concerns of each group, including the stigma associated with working
with forensic clients
♦ Accountability to the Crown, if applicable to the specific diversion point, in terms of
whether a charge will be withdrawn; this requires commitment to the program and
faith in the services provided.
Although an analysis of this type may seem to focus on potential negatives, it is better to
understand the community issues at the outset than to face major obstacles because
these issues were not recognized and addressed. Including individuals from the specific
groups in this type of analysis is very important. Capitalizing on any existing informal
linkages between professionals within the community can assist in this process.

Section IV: Education and Training page 7
3. Incorporating Education/Training In Community Diversion Program Development Although some community members may be aware of what is involved in a diversion
program, everyone has a different frame of reference regarding diversion. This is
supported by the research and the stakeholder consultations. Even within the
development of the Provincial Diversion Program, committee members representing
varied ministries and agencies each had his/her own views and beliefs of “how diversion
should look” and “who should be eligible for diversion”.
This initial education involves the representative(s) from the Provincial Diversion Program
with a focus on the following:
a) Discussing the background information regarding the provincial commitment to
diversion in order to provide context and to increase community commitment
i) overview of the rationale for a diversion program
ii) a historical context for the development of diversion within Alberta and
Canada
b) Outlining and providing rationale for key elements of the Provincial Diversion
Program
i) target population and eligibility criteria
ii) the diversion points and potential community resources for each point
iii) risk and safety issues as they may relate to any given community
iv) the need for base standards for appropriate care, support and treatment
c) Providing information from organizations/agencies who act as advocates for the
target population in order to increase understanding of
i) needs of the client and family
ii) the impact of “criminalization”
iii) types of supports that could increase the client’s sustained community
tenure (See definition of community tenure in Appendix A: Glossary.)
iv) any specific ethnoculturally-based information that may be important, for
instance, specific cultural approaches to care, support and treatment for
Aboriginal clients
d) Discussing the implications of a diversion program in terms of client and
community safety and risk and overall community well being.

Section IV: Education and Training page 8
Such education should create an appropriate environment or social context for developing
the foundation for a community diversion program. This initial education will enable those
involved to more effectively encourage participation from other service providers and from
the community itself.
4. Developing A Plan And Schedule
It is recommended that the community diversion team outline an education/training plan
and schedule based on each stage of development. This can be done with the assistance
of the Provincial Diversion Program representative.
This plan should incorporate the following areas, along with clearly defined objectives, as
shown in the following sample:
General Education Training Objectives Initial program development provide a historical look at diversion
relate relevant research about diversion programs
learn about client characteristics and needs Initial forum related to
service provider roles and how they could work within program development
provide a general overview of key service provider roles, responsibilities, and limitations
outline criminal justice process provide overview of mental illness,
medication, co-occurring mental health and substance abuse—defined as per target population
assist in evaluating community resources and determining appropriate diversion points
Presentation to media for dissemination to general public
invite community participation and involve those local family and consumer groups in advocating
Forum related to general legislation considerations, i.e., FOIP, HIA, Alberta Alcohol and Drug Abuse Act, Mental Health Act, YCJA
familiarize service providers with the key elements from each piece of legislation
provide the basis for learning about the importance of “consent”
Training of service providers about the diversion process
provide information about the process as it relates to each selected diversion point
Community workshop to provide media and general public with specifics of diversion program
outline the specifics of the diversion process and anticipated outcomes
address “safeguards” for ensuring community safety
discuss the overall objectives, specifically as they relate to the community
Ongoing training , as needed, regarding the role of each service provider in the diversion process
provide specific “re-training” in response to observed “rapid cycle” or short term outcomes (defined in Section VI: Evaluation and Accountability)

Section IV: Education and Training page 9
The education/training plan should be outlined early in the development of the community
diversion program. It should be re-evaluated periodically to address specific needs and
ensure continued support.
The plan should include information about the following:
a) The roles and responsibilities of diversion partners
b) Legislation that may impact the diversion process
c) Diversion program protocols and processes
d) Ongoing training for service providers
a) The Roles and Responsibilities of Diversion Partners “I didn’t know that [your organization] provided that service. We do __________. We
should try to see if we can work together on some clients.”
Front line staff members have probably heard the above phrase many times in their
careers. Administrators, too, may have wondered exactly what care, support and
treatment other service providers deliver and how they could share resources.
However, service providers involved in a community diversion program cannot just
“wonder” about what another organization does; they require the information and
knowledge to be able to appropriately refer or connect their clients with these services.
An understanding of the specific services provided within a community is required in
order to determine which diversion points will be targeted and what processes will best
ensure individual and community safety and the provision of appropriate care, support
and treatment.
This understanding may be gained by having some initial general training of the
Community Diversion Implementation Team, specifically to discuss the following
areas:
i) Presentations by representative from each community service provider about
specific mandates, goals, objectives of the organization
the types of roles that staff have in relation to the target population
specific processes that may enhance or create obstacles to a community
diversion program based on collaboration

Section IV: Education and Training page 10
other limitations, for instance, governing legislation, that may impact the
diversion process
ways in which service provider could become involved with the target
population.
ii) Information session on the criminal justice process within the community, for
instance:
what often occurs if an individual with mental illness comes in conflict with
the law
what roles, responsibilities, and limitations pertain to each of the following:
law enforcement, the crown, judiciary, probation, corrections, if applicable
beliefs, attitudes of front line staff in relation to the target population
introduction to specific justice terminology.
iii) Presentation/information session on mental illness, with specific focus on
signs and symptoms
crisis intervention strategies
medication compliance and the effects of non-compliance
mental illness and substance abuse.
(See sample Definitions from Calgary Diversion on pages 13 to 15.)
The above training is most appropriately provided at a couple of stages:
early in the program development (perhaps with the assistance of the
Provincial Diversion Program representative) in order to establish a
common base of understanding;
once protocols and processes are completed; then a more “practical”
training may be appropriate for staff providing the delivery of services to the
target population. In addition, each service provider should provide a brief
written submission about his/her role and organization as it applies to the
diversion program, which can then be incorporated into an Education/
Training Packet.

Section IV: Education and Training page 11
b) Legislation That May Impact Diversion As indicated in Section III: Information Sharing, a number of pieces of legislation may
impact a community diversion program, specifically as they relate to the privacy rights
of the client. Specific education sessions should be set up in terms of
i) the Criminal Code, as it relates to minor, low risk offences
ii) the Youth Criminal Justice Act, specifically with a focus on
Extra Judicial Measures and Extra Judicial Sanctions
Reintegration
iii) Applicable Legislation, including the following
Freedom of Information and Protection of Privacy (FOIPP)
Health Information Act (HIA)
Alberta Alcohol and Drug Abuse Act
Child Welfare Act
Mental Health Act
iv) Informed Consent as a prerequisite
c) The Diversion Protocols and Processes If education/training has been integrated into the program development and if it has
been a collaborative effort, then educating the service providers on the diversion
process should be uncomplicated. By this stage, a number of key stakeholders
should have contributed to the development and understand the importance of
knowing about the target population, eligibility, legal aspects, mental illness, and so
forth.
However, it is still important to place the above topics into context by relating them to
the diversion process. All professionals, organizations, and agencies that may be
involved require education about the diversion process, with a focus on the following:
i) What the eligibility criteria are for each specific diversion point. The Calgary
Diversion Project developed and used a video that depicts potential diversion
scenarios. This education tool proved to be very useful for clarifying eligibility
and process, as well as for communication with the media.7
ii) How the diversion program process works in terms of the criminal justice
process, specifically in terms of:

Section IV: Education and Training page 12
the referral process
the time frame for diversion and what happens after that time
service provider collaboration and the case management approach
and the process for transitioning of the individual to ongoing community
resources.
iii) What role “diversion staff” plays in terms of assessment, triage, determining
risk and eligibility, and providing or referring to appropriate care, support and
treatment.
iv) What the goals are once the client has gone through the process.
It is important to ensure that criminal justice, mental health, health, addictions,
housing and other service providers are comfortable with the process of referral and
the expectations of the diversion program. It is equally important that clients and
family, if appropriate, become aware of the process through information sessions,
which are supported by written material and more detail on a case by case basis.
The general public also requires information on the diversion process and the “risks
and benefits” of this process to the client and to the community. This information can
become part of the communication plan designed for each community.
d) Ongoing Training for Service Providers
The process of training is not a one time effort. It must be part of collaboration and
ongoing communication. Collaboration requires reinforcement, as is often illustrated in
other community projects that depend on multiple stakeholders. In some rural
communities and depending on population and resources, the diversion process may not
be used frequently. There may be only a few eligible cases in a given month or year. To
ensure that the momentum of collaboration continues, it is beneficial to use training and
sharing of organization information to reinforce communication and collaboration.
The above process provides an overall approach that will ensure, as best as possible,
understanding of and specific training in relation to the community diversion program. A
natural result is greater acceptance and commitment to the program.

Section IV: Education and Training page 13
SSAAMMPPLLEE EEDDUUCCAATTIIOONN AANNDD TTRRAAIINNIINNGG MMOODDUULLEESS The attached sample education modules have been provided by the Calgary Diversion
Project and were used as part of their education/training process for service providers.
They are intended as examples for communities developing a diversion program.
Note: Because of its mandate, Calgary Diversion uses the definition of “mental disorder” in determining their eligibility criteria instead of “mental illness”, which is used in the Provincial Diversion Program. Source: The Calgary Diversion Project. (February 2002). Reprinted with permission.
M ENTAL DISO RDERM ENTAL DISO RDER General Overview and Definitions “M ental d isorder” as defined in the M ental H ea lth Act, re fers to any ind ividual who has a substan tial d isorder of thought, mood, perception , o rientation or m em ory that grossly im pairs
(i) judgm ent,
(ii) behavior,
(iii) capacity to recognize rea lity , or
(iv) ability to m eet the ordinary dem ands of life. Individuals who are m entally ill experience problem s w ith their m ood, th inking, and/or perception and these disturbances becom e evident in their behavior. Signs and Sym ptom s A client’s presentation is often the first indicat ion of the severity of the m ental illness. M enta l illness is often first noticed by an ind iv idual's fam ily or friends and m ay rem ain unnoticed or undiagnosed for a period of t im e. They m ay notice changes in the way the individual behaves, reacts or fee ls toward the world around them . The individual m ay be struggling to cope w ith everyday life. The c lient can present with various signs and symptom s which can be identified in the fo llowing areas:
1) Appearance - poor hygiene and personal groom ing.
- decreased ability to care for se lf.
2) M ood – irritab ility , depression , elevated m ood, mood swings.
3) Behavior – anxious, agitated, angry outbursts, unusual m ovem ents, inability to sit st ill, uncooperative. 4) Speech Pattern – rap id , incoherent, illog ica l, m ute, over-ta lkat ive, hesitant, m um bling. 5) Thought Processes and Content – delusions, hallucinat ions, paranoia, preoccupations– often with death , racing thoughts, excessive fears. 6) Sensorium – im paired judgm ent, lim ited insight, decreased concentration and attention, d isorientat ion . * See gloss ary for further explanation of term s .*

Section IV: Education and Training page 14
Source: The Calgary Diversion Project. (February 2002). Reprinted with permission.
SUBSTANCE USE AND MENTAL ILLNESSSUBSTANCE USE AND MENTAL ILLNESS
Substance use is the use of a chemical substance, licit or illicit, resulting in a person’s physical, men-tal, emotional or social impairment. Mentally disordered means a substantial disorder of thought, mood, perception, orientation or mem-ory that grossly impairs:
Judgement, Behavior, Capacity to recognize reality, or Ability to meet the ordinary demands of life.
The impact of substance use on mentally ill persons is significant. A percentage of persons who are mentally ill are also using drugs and/or alcohol. It is often difficult to determine if a person is men-tally ill, under the influence of substances or both. The key factor to remember when encountering someone who is thought to be using drugs and/or alcohol, is that you do not know what the person’s pre-intoxication personality was like. Before assuming a mental illness, time must be given for the person to “clear” of substances. A complete and accurate mental status assessment cannot be done when the person is toxic or under the influence. Some individuals may actually be much more trou-bled, sick or violent than at the time of encounter. Persons who are both using substances and suf-fering from a mental illness are said to be “dual-diagnosis” i.e.: They have two co-existing mental health diagnoses. Although the main cause of psychiatric relapse is medication non-compliance, another common cause is the use of drugs and/or alcohol. Likewise, a common cause of alcohol and drug relapse to-day is untreated psychiatric conditions. Because of this, an integrated model of service delivery is needed for effective treatment. This means a variety of community agencies providing a number of different resources are required to provide the person with quality care. i.e.: detox, shelter, support groups, medical care, mental health treatment, etc. Symptoms of withdrawal from these substances can range from being very uncomfortable to life-threatening, depending on the substances used. Cognitive and thinking processes are often altered significantly and a person who is withdrawing from a substance is not thinking clearly or rationally. Their behavior and actions are irritable and unpredictable and the person can be very aggressive if feeling threatened. The main focus for the person in this state is to find a way to obtain more of the substance to alleviate their symptoms. If substance use is coupled with a mental illness, behavior may present as being quite bizarre, and may be due to the drug itself and the existing mental disorder. It is also quite possible that the person may not be taking prescribed psychiatric medications and is beginning to deteriorate men-tally. It is important to take into consideration that the person’s bizarre or irrational presentation may be due to substance use, mental deterioration or both. Safety should be a consideration for both the affected person and others who may come into contact with him/her. When the person clears from substances, a thorough assessment may shed further light on the precipitating factors that have caused the person’s behavior.

Section IV: Education and Training page 15
Source: The Calgary Diversion Project. (February 2002). Reprinted with permission.
Medications and Mental Illness
Psychiatric medications are prescribed to help control symptoms of mental illness, but they are not a cure and symptoms may persist. Medications need to be monitored by a physician regularly as adjustments may be required. Individuals who are mentally ill may attempt to self medicate by using street drugs, alcohol, over the counter medications or even prescribed medications, contributing to deterioration of their men-tal health. The main cause of psychiatric relapse is non-compliance. Reasons for non-compliance include unfavorable side effects of the medication, substance use, the belief they are well and paranoia due to their mental illness. It is helpful for the Mental Health Professional to be provided with background information on the client such as the individual’s behavior and appearance upon arrest and whether they had medica-tion bottles or possible drug paraphernalia on their person. It is also important to note any general observations, including any rapid and unprovoked changes in the individual’s behavior. Questions recommended at the scene, if possible, include:
• Are you currently seeing anyone for mental health concerns? • Are you currently taking medication? If no, has your physician suggested that you
take medication?
• Are you taking the medication as your physician instructed? • How long have you been taking this medication? Do you have any with you? (if de-
tained for an extensive period of time may need to ensure meds are available for the client)
• Have you ever been hospitalized due to mental illness?
Details regarding medication will be asked by the Paramedic at the APU as part of the screening process.

Section IV: Education and Training page 16
Source: The Calgary Diversion Project. (February 2002). Reprinted with permission.
RISK ASSESSMENTRISK ASSESSMENT A risk assessment will assist in determining an individual's risk for aggressive behavior, including substance abuse issues. Not only does a risk assessment determine an individual’s level of risk, it also assists in identifying the level of intervention required. The reason it is important for the CDP to utilize a risk assessment is to ensure safety issues are ad-dressed. The CDP believes that regular and frequent risk assessments are necessary as an individ-ual’s presentation may change. Once rapport is established, certain questions can be asked. SUBSTANCE USE • Do you use alcohol or drugs? • What do you use and how often? • When did you last use? • Any history of withdrawal? RISK TO SELF • Have you had thoughts of wanting to die? • Have you made any plans on how you would die? • What are those plans? When did you plan to do this? • Have you had these thoughts before? • Have you ever tried to hurt yourself before? • If yes, how did you attempt and when? • Did you receive any mental health treatment then? • Are you feeling suicidal now?
RISK TO OTHERS Consideration must be given to the fact the person may be psychotic or paranoid and questions must be carefully posed. • Have you had thoughts of hurting someone else? How? • Who is this person? • Have you hurt someone in the past? • When and what happened? • If a weapon was used, what? • Do you have access to this weapon now? The answers the person may give one person may also differ from what he/she tells another, depend-ing on the level of trust or rapport present. It is helpful to have the information about the person’s behavior and presentation on first contact in order for a more thorough and accurate mental status as-sessment to be done later. A helpful tool in assessing a person’s risk level is the Crisis Triage Rating Scale which was discussed earlier. Keep in mind this is merely a tool for guidance in the decision making process and can be used as an option to assist, however cannot replace clinical judgment and education.

Section IV: Education and Training page 17
PPRROOFFEESSSSIIOONNAALL DDEEVVEELLOOPPMMEENNTT The second type of education and training relates to professional development of staff.
Offering opportunities to be involved in workshops and courses that may enhance the
clinical expertise of service providers is another area in which the community diversion
team can increase the acceptance of and commitment to the program. Such opportunities
also help ensure that all service providers are meeting the base standards for providing
appropriate care, support and treatment, as well as increasing the capacity of the
community in the future.
Professional development opportunities, for instance, via internet based education
modules, will be explored in Phase Two development and in conjunction with specific
diversion communities.
EEDDUUCCAATTIINNGG TTHHEE CCOOMMMMUUNNIITTYY AABBOOUUTT DDIIVVEERRSSIIOONN:: THE COMMUNICATION PLAN
Throughout the process of developing a community diversion program, communication
with the general public is important for several reasons, specifically to
determine the public’s potential reaction to diversion of this target population
assist in determining which diversion points may be most appropriate
demonstrate the “transparency” of the goals, processes and anticipated outcomes
determine what risk management strategies may be required in addition to those
used in assessing the client’s eligibility to ensure the safety of the community
involve the community in decisions regarding the provision of services
provide the opportunity for community involvement in critical areas such as
provision of housing.
In consultation with the Provincial Diversion Program, each community diversion team
requires a communication plan, which should be developed early in the process.
Consultation with the Provincial Diversion Program will assist in providing communication
strategies, as well as ensure consistency in the messages.

Section IV: Education and Training page 18
In general, a communication plan should include the following type of information:
the goals of the community diversion program
an overview of the background of diversion development in Alberta
specific communication objectives
clearly identified audiences
a strategy that incorporates the type of media used and at what stage of
development
an outline of key messages that need to be conveyed to the community
the key outcome measures that will help determine success.8
Additionally, for communication to be effective and the message to be consistent, there
should be an identified source for media contact. There should also be measures put in
place regarding how to address potential obstacles, objections or conflict.
Establishing a relationship with a local media source early in the process will assist in the
development.
Further assistance in developing a communication plan will be provided by the Provincial
Diversion Program representative as part of the implementation of the program into each
community.
In summary, the relationship between education/training, collaboration and community
acceptance and commitment must be recognized as fundamental to the success of the
program.

Section IV: Education and Training page 19
EENNDDNNOOTTEESS 1 Borum, R. (1999). Jail Diversion Strategies for Misdemeanor Offenders with Mental Illness:
Preliminary Report. Department of Mental Health Law & Policy, Louis de la Parte Florida Mental health Institute, University of South Florida, Tampa, Florida.
2 Discussions with Fran Barnes, Manager of the Calgary Diversion Project. (September 2002).
3 A series of articles, as well as the Calgary Diversion Project, highlight these areas as importantcomponents of education. Borum, R. (1999). Jail Diversion Strategies for Misdemeanor Offenders with Mental Illness: Preliminary Report. Department of Mental Health Law & Policy, Louis de la Parte Florida Mentalhealth Institute, University of South Florida, Tampa, Florida.
4 A combination of sources including several dictionaries in an effort to most accurately depict the interpretation by the Provincial Diversion Working Committee.
5 A combination of sources including several dictionaries in an effort to most accurately depict the
interpretation by the Provincial Diversion Working Committee.
6 Calgary Diversion Project. They found it to be very insightful to hold some training sessions onsite—at the precincts, the court house, the community mental health clinic—if the topic related to the roles and processes of that particular diversion partner.
7 Discussions with Fran Barnes, Manager of the Calgary Diversion Project.
8 Adapted from the Calgary Diversion Project Communication Plan, 2001

SSEECCTTIIOONN VV
AAPPPPRROOPPRRIIAATTEE CCAARREE,, SSUUPPPPOORRTT && TTRREEAATTMMEENNTT Contents APPROPRIATE CARE, SUPPORT AND TREATMENT: The Foundation Of Diversion SERVICE DELIVERY REQUIREMENTS
Case Management Protocols Risk Management Framework
TYPES OF SUPPORT SERVICES
Description Of Support Services Core Support Services
BASE AND PREFERRED STANDARDS
Family & Community Supports Mental Health & Psychiatric Services Ethnocultural Accommodations Addictions Medical Vocational/Recreational Support, Self Help & Transition
…………………………………………….…………1 ……………………………………………………….3 ……………………………………………………..12 ……………………………………………………..17

Section V: Appropriate Care, Support & Treatment page 1
AAPPPPRROOPPRRIIAATTEE CCAARREE,, SSUUPPPPOORRTT && TTRREEAATTMMEENNTT:: THE FOUNDATION OF DIVERSION Providing appropriate care, support and treatment for individuals with mental illness who
are in conflict with the law is the foundation of an effective diversion program. As
previously identified within the Provincial Diversion Framework: Reducing the
Criminalization of Individuals with Mental Illness (2001), the primary purpose of Alberta’s
Provincial Diversion Program is
to ensure that, whenever appropriate, adults and adolescents with mental illness who are in conflict with the law receive appropriate care, support and treatment from mental health, social and support services thereby reducing reliance on the criminal justice system.1
Mental health and psychiatric services form the basis of appropriate care, support and
treatment in terms of providing crisis intervention, assessment and ongoing therapeutic
and medication related services. However, these services cannot function in isolation
within a community; instead, for a holistic approach, “social and support services” are
required.
Social and support services are defined as:
… the broad spectrum of services that have a direct bearing or interest on the quality of life of the mentally ill. It speaks to income and housing support, but also the other services such as transportation, education, supportive and spiritual counselling and general support.2
In addition, for appropriate care, support and treatment to take place, there needs to be a
close relationship with those ministries involved in the criminal justice process. Only with
cooperation from these professionals—for instance, law enforcement, legal counsel,
judiciary, probation and corrections—can the individual with mental illness who is in
conflict with the law be identified and referred to appropriate care, support and treatment
from any of the seven diversion points outlined in Section I: Diversion Points & Eligibility
Criteria.
In order for a diversion program to be effective within a community, it is recommended
that individuals with mental illness who receive probation, are incarcerated, or are given a
combination of sentences should be provided with the opportunity for appropriate care
and treatment. As well, those individuals who are released from incarceration should be

Section V: Appropriate Care, Support & Treatment page 2
referred to appropriate supports that may enable them to achieve increased community
tenure. For the purposes of the Diversion Program and this target population, community
tenure is defined as the following:
Community tenure is based on the individual’s ability to spend his/her time in a meaningful, and hopefully gainful way, inclusive of the following specifics—
♦ Improved functioning as demonstrated by greater independence in several life areas such as housing, financial stability, etc.
♦ Reduction of number of incidents resulting in criminal justice system involvement and number of days in incarceration
♦ Reduction of symptoms resulting in criminal behaviour ♦ Reduction in number of days in hospitalization ♦ Increased quality of life, including connection with familial, social and
community supports and activities.3
An individual may “enter” the diversion program several times before the frequency of
his/her involvement with the law is decreased and sustained community tenure is
achieved. Moreover, even though a time period for an individual’s involvement in a
diversion program may be stipulated by the criminal justice system, this period may not
signify an end to care, support and treatment. In many communities the organizations or
agencies that provide the care, support and treatment as part of the diversion program will
often be the same ones that provide services to the community in general or to individuals
with mental illness who are not in conflict with the law. Care, support and treatment
should be ongoing within the parameters of the diversion program and from there, based
on referral to appropriate community services.
This section of Phase One outlines service delivery requirements including case
management protocols, risk management framework, types of services, and minimum and
preferred standards for mental health, social and support services.

Section V: Appropriate Care, Support & Treatment page 3
SSEERRVVIICCEE DDEELLIIVVEERRYY RREEQQUUIIRREEMMEENNTTSS The document—Alberta’s Provincial Diversion Framework: Reducing the Criminalization
of Individuals with Mental Illness (2001)—outlines the principles of effective service
delivery, several of which apply to the appropriate care, support and treatment of
individuals who are eligible for the diversion program. Summarized, these principles
include the following:
i) “Safety and Security of both the individual and community must be considered during the initial contact and throughout service delivery.
ii) Timeliness of Assessments is required to ensure the safety of the
community and is essential to the well being of the individual.
iii) The use of an interdisciplinary approach and varied treatment options is preferred for an effective and holistic approach. A variety of service options and, when appropriate, a multi-disciplinary approach should be available for individuals across the continuum of care. An integrated, individualized treatment plan should be developed. Services may include individual, group and family counselling where appropriate, rehabilitation, follow-up and other treatment options.
iv) Collaboration and Cooperation between ministries is necessary to provide
the best possible service delivery within the province, and ultimately, will enhance the well being of individuals with mental illness.
v) Linkages and Access to Services—for instance, health care, housing,
education, finances, and activities of daily living—are integral to service delivery.” 4
Adhering to these principles by communities involved in the diversion program is
important to ensuring a continuum of care and enabling sustained community tenure for
the target population.
In order to put these principles into practice, each diversion community is encouraged to
take the following preliminary steps when developing its community service delivery model
for a diversion program,
Determine case management protocols
Set up a risk management framework

Section V: Appropriate Care, Support & Treatment page 4
Case Management Protocols
In order to implement a service delivery model, it is recommended that a case
management approach be used. Communities have varied available resources for the
provision of appropriate care, support and treatment, with each resource having different
organizational structures and mandates. In order for there to be clear communication
among service providers and a holistic approach, clear case management protocols need
to exist within a community.
As the research demonstrates, many models of case management are currently utilized,
ranging from Intensive Case Management to Assertive Community Treatment to simply
providing referrals.5 Each community needs to determine which model best fits its
resources and existing structures, within the realm of the following purpose:
To ensure a coordination of needs including assessment and planning of care,
connections with appropriate resources, transitions from the criminal justice
system, and when necessary, compliance with legal aspects of release
To ensure a commitment to long term treatment, if required, and social and
support services to maximize stabilization of individual and reduce incidents of
relapse.
The use of a case management team appears to be most appropriate for a cross-
ministerial, cross-agency program such as diversion. The team concept does not suggest
that all organizations/agencies involved with a specific individual need to take turns as
case manager. However, in situations where specific needs, for instance, addictions, are
prevalent, there may be a need for a shared responsibility in the role of case manager.
Further specifics will apply to each community, based on its situation.
Plus, the case management team has an understanding of the “overall picture” concerning
the client, including the availability of appropriate community resources, the nature of the
offence as well as previous history, the client’s family situation, his/her involvement with
others, and his/her predilections. Periodic conferencing by the case management team
regarding the delivery of services and the individual’s response to those services helps to
provide a more seamless approach.

Section V: Appropriate Care, Support & Treatment page 5
Guidelines
Although the specifics of the case management approach are the responsibility of each
community, the following guidelines may assist in implementing a diversion program:
1 Case Management Team a) Including a team approach for the purposes of case management will allow
i) for representation from a number of involved organizations/agencies
ii) greater continuity over a longer period of time as necessary to reduce reliance
on the criminal justice system
iii) and a sharing of responsibility for the individual’s community tenure
b) A case management team ideally consists of the following:
the client
an individual representing the criminal justice process
mental health professional
self help or cultural support, if appropriate
family or designated community member, if appropriate
addictions, if appropriate
general medical practitioner, if appropriate
translator, if necessary.
c) The roles of team members involved in managing each case are clearly defined; a
process exists for replacing members if required because of attrition.
d) Determining who leads the case management team is based on:
i) The diversion point at which the individual becomes involved
ii) The professional with whom the client feels comfortable
iii) Most prevalent problem whether it be mental health or addictions, if applicable
iv) Greatest need(s) in terms of achieving community tenure.
The lead of an individual’s team may change depending on his/her needs. However,
all members of the case management team need to be available to help
“troubleshoot” when issues may arise with the individual and/or with any of the
agencies/groups providing support.
e) All members of the case management team should understand the requirements
of the criminal justice system as they relate to each individual.
f) Regular team meetings are held to discuss the progress of the individual, based
on his/her needs and the requirements of the criminal justice system.

Section V: Appropriate Care, Support & Treatment page 7
Risk Management Framework The safety of both the individual and community are important considerations in
determining what specific types of care, support and treatment are required and when
and how the services are delivered. Each community is responsible for developing a
risk management framework to assist in reducing the risk of harm to self or others at the
point of the individual’s initial contact with the criminal justice system and during the
individual’s involvement with the diversion program. This framework should include the
following components:
1 Processes for Reducing Risk Associated with Crises When an individual with mental illness comes in conflict with the law, he/she may be in
the midst of a crisis related to his/her mental illness or substance abuse. The
following need to be considered as part of a risk management framework geared
toward individuals in conflict with the law and in crisis:
a) A process for ensuring timely access to services for individuals with mental illness
who are thought to be in a crisis situation at the time of their commission of an
offence, inclusive of
i) A clearly defined set of procedures for law enforcement, EMS or other service
providers who typically encounter individuals with mental illness who may be in
a crisis situation at the time when the offence is committed. These procedures
should include the following:
Guidelines for determining where the individual should be taken if he/she
appears to be at risk to self or to others and is thought to have a mental
illness Guidelines for the use of fitness assessments as a method of stabilization.
(This is currently done in many Provincial Courts in that Provincial Court
Judges, Crown, and defence counsel, all see it, use it and recommend it as
a way of stabilizing the accused at least to the point of being able to deal
with the charges) Guidelines for determining who is responsible for transporting the individual A list of contact persons who are involved in providing care, support and
treatment for individuals who are involved in the diversion program A listing of the documentation required in addition to that specified by each
profession’s organization.

Section V: Appropriate Care, Support & Treatment page 8
b) A process to ensure timely assessment of individuals who are thought to have a
mental illness or co-occurring mental illness and substance abuse issues
i) In the case of communities that do not have ready access to mental health
professionals qualified to perform these assessments, the process should
include how to access Telemental Health Services
ii) Determining a time period in which these assessments should take place in
order to ensure treatment, if necessary, in a timely fashion
iii) In regards to the assessment itself, the community should determine some
guidelines for what should be included in an assessment and how the
assessment should be done.
c) A listing of types of available mental health and substance abuse services that
provide assessment
i) An outline of the types of standard assessments used and their purposes
d) A process for enabling smooth transition from a facility that provides services to an
individual who was in crisis to community-based services, or whatever is deemed
appropriate
i) Once the individual is stabilized, if he/she is being diverted without charges,
then transition should include
connection with the case management team, who will assist in directing the
individual to other services, for instance, outpatient mental health
assessment and treatment, addictions, housing, cultural supports—
whichever are deemed necessary
provision of any interim housing or financial aid, if required
ii) Once the individual is stabilized, if he/she is diverted with charges, then
transition should include
Connection with appropriate professionals involved in the criminal justice
process, if necessary, in order to discuss the nature of the charges and
obtain consent for the diversion program.
e) Availability of some type of mobile crisis intervention process, should the individual
suffer relapse during his/her time within a diversion program.

Section V: Appropriate Care, Support & Treatment page 9
2 Processes for Minimizing Risk During Involvement with Diversion Program A number of situations may exist with a community diversion program:
The individual may have no charges, with only a recommendation to participate in
services
They may be charged, with the provision that they participate in a diversion
program for charges to be dropped
They may be on probation, with mandated participation as part of the probation
order
They may be incarcerated, with participation in available services being part of
their daily structure
They may be discharged from incarceration with the recommendation that they
participate in community services or with conditions placed upon their release.
Regardless of the situation and whenever appropriate, it is important that each
community’s diversion program assesses the risk and monitors or supervises the
individual and his/her progress within the program to minimize potential risks to self and
community. The following considerations apply:
a) Processes for ensuring a comprehensive assessment of risk during triage
b) Processes for developing a plan of care for the individual that includes information
from the assessment and incorporates information regarding the individual’s
“treatment responsivity” as outlined in the following definition and illustrated by the
following diagram: “Treatment responsivity… incorporates treatability (treatment
motivation and readiness; treatment compliance and participation) and treatment
effectiveness (treatment gains and treatment generalization)”6

Section V: Appropriate Care, Support & Treatment page 10
Figure 1: Assessment of Treatment Responsivity
Source: Serin. R. (2001) Treatability, Treatment Responsivity and Risk Management. In Douglas. K.S. et al. (Ed) HCR-20 Violence Risk Management Companion Guide (p. 113). British Columbia: Mental Health, Law, and Policy Institute, Simon Fraser University.
c. Processes for monitoring the progress of the target population’s participation in
plan of care and progress, including reassessment of risk, if necessary
d. Processes that outline methods of intervention designed to minimize risk
should an individual with mental illness not comply with recommended care
and treatment, inclusive of taking of medications, if applicable, or relapse.
3 Coordination with Appropriate Criminal Justice Professionals A process outlining communication procedures and coordination of services between
professionals directly involved in the care, support and treatment and those involved in
the criminal justice process via the case management team:
Treatability
Treatment Responsivity
Treatment Effectiveness
Treatment Motivation & Readiness
Treatment Compliance & Participation
Treatment Gains
Treatment Generalization

Section V: Appropriate Care, Support & Treatment page 11
a) In situations in which the case management team deems that the individual is
placing him/herself at risk by not complying with medication or engaging in harmful
behaviors, there needs to be a clear process for notifying criminal justice
professionals, if necessary
b) In situations in which the individual is being discharged from a correctional facility,
there needs to be a process for involving the case management team in the
discharge planning.
4 Coordination with Family or Community Supports
When the family or community individuals are actively involved in the care, support
and treatment of the individual, a process needs to exist for communicating concerns
or incidents that may signify increased risk.
5 Communication with the Community Part of risk management becomes education of the community about mental illness
and about the diversion program.

Section V: Appropriate Care, Support & Treatment page 12
TTYYPPEESS OOFF SSUUPPPPOORRTT SSEERRVVIICCEESS In implementing the diversion program, each community needs to assess the types of
available support services, the needs of each eligible individual, and the role of each
service provider in delivering appropriate care, support and treatment.
Research describes “support” as encompassing one or all of the following, based on
Henggeler, et al., 1998):
instrumental, “to provide the necessities of life”, which can include activities such
as assisting in financial support, finding accommodations, and activities to daily
living
emotional, “to give strength to”, which can include showing empathy for the
individual and being committed to providing assistance
appraisal, “to give aid or courage to”, which can include positive reinforcement to
the individual in regards to decisions made or actions followed
information, “to tend to establish by providing new facts”, which can include guiding
individuals and family to appropriate resources and to support groups that have
been through similar situations.7
Support systems may be regarded as formal (social workers, nurses, general medical
practitioners, psychiatrists, etc.) and informal (family members, friends, peer support,
clubs, etc.). Of the above, those supports that are most appropriate for providing care and
treatment depend upon the individual’s situation and accessibility to community resources.
An individual’s situation may include specific ethnocultural considerations, defined as
“common, distinctive ethnicity, heritage, culture, language, social patterns, and sense of
belonging”.8
Also important are the roles played by law enforcement, legal counsels, judiciary,
probation—who are instrumental in the referral and follow up—and corrections personnel
who facilitate the provision of care, support and treatment services to incarcerated
individuals with mental illness and are responsible for their discharge planning. Sharing of
information, when it is appropriate based on the legislation, regarding the type of care,
support and treatment the individual has received within the correctional facility and

Section V: Appropriate Care, Support & Treatment page 14
Description Of Support Services
1 Family And Community Supports Research and stakeholder consultations refer to the important role of families, friends,
peer support, clubs, teachers, community group leaders, church leaders, elders, etc.
who have an impact on the individual’s ability to sustain tenure within the community.
a) Family: In determining who the family is, the Provincial Diversion Working
Committee follows Wright and Leahey’s definition of the family, which states: the
family is who they say they are.9
Should family supports be available and be willing to assist in the care and
treatment, it is recommended that they be included in the diversion process at the
outset, provided there is consent from the individual.
b) Community Supports: These individuals may be from any of the above-
mentioned groups, particularly if they may be instrumental in assisting in the care
and treatment because of their relationship to the individual with mental illness
and/or their position in the community.
2 Mental Health And Psychiatric Services Assessment and treatment services across the continuum of health, inclusive of both
crisis/emergency response, short term inpatient treatment and outpatient/out reach
are considered necessary for an effective diversion program.
3 Ethnocultural Support that incorporates ethnocultural needs, inclusive of language, traditional
treatments, or other facets that increase the individual’s willingness to participate in
ongoing treatment and care. Ethnocultural refers to “common, distinctive ethnicity,
heritage, culture, language, social patterns, and sense of belonging.”10

Section V: Appropriate Care, Support & Treatment page 13
collaborating with community-based service providers enhances the opportunity for better
reintegration into the community and increased community tenure.
The Provincial Diversion Working Committee has identified the types of formal and
informal services that may be required for care, support and treatment of an individual
deemed eligible for diversion.
These supports are outlined in the following diagram.
DIVERSION CLIENT
Family &
Community Supports
Recreational/ Vocational
Transition
& Support Self Help
Addictions
Accommodations
Ethnocultural
Mental Health &
Psychiatric Services
Medical

Section V: Appropriate Care, Support & Treatment page 15
4 Accommodations Secure, safe housing, inclusive of that required for crisis/emergency response to
diminish the risk of harm to self and others, short-term housing to allow for greater
stability while in the initial stages of treatment, and when appropriate, supported or
independent living accommodations that contribute to long term stability of the
individual with mental illness.
5 Addictions Assessment, treatment and reassessment, inclusive of both crisis/emergency
response, short term inpatient treatment and outpatient/out reach for individuals who
are suspected of having both substance abuse and mental health problems and are in
conflict with the law. The services focus specifically on how the substance has
affected the major life areas of the individual in a negative way. Gambling as an
addiction is included in the primary services, if the individual with mental illness has
come into conflict with the law as a result of gambling addiction.
6 Medical
Assessment, diagnosis, treatment and care in relation to physical health issues are
often integral to the individual’s initial and continued well-being.
7 Transition /Support Self Help Inclusive of those which provide information, financial assistance, potential referral,
advocacy, a sense of community, a safe haven, or any aspects of activities of daily
living.
8 Recreational/Vocational
Facilitating linkages with appropriate recreational services and programs and/or
vocational programs that may increase community tenure.

Section V: Appropriate Care, Support & Treatment page 16
Core Support Services Many differences exist throughout Alberta in terms of the types of services available in a
given area, the organizations and agencies that provide services, the distance traveled to
access, and so forth. Because of these differences, it is not feasible to identify specific
services as being core. Rather, for the purposes of a community diversion program, core
support services are those that are
♦ required for response to crises and for stabilization of the individual prior to
ongoing treatment
♦ and play a principal role in the ongoing treatment.
These supports include family and community members, as well as services that provide
assessment and treatment for mental health, addictions, and medical issues.
Accommodations may be included as a core support because of the importance of
ensuring safe and secure environment for the target population. In addition, translation
services should be provided if there are potential language barriers. These supports are
considered as being central to the effective service delivery of the diversion program.
In addition to the above-mentioned, other supports are often required to enhance the
individual’s treatment and care and/or to encourage the individual’s continued
participation. The need for these supports will vary according to the individual’s situation.
As an example, ethnocultural supports should also be thought of as core or primary if
language or culture is considered to be important to an individual’s success in a diversion
program.
Section V: Appropriate Care, Support & Treatment page 17
BBAASSEE AANNDD PPRREEFFEERRRREEDD SSTTAANNDDAARRDDSS DDEEFFIINNEEDD There are many reasons for including “base and preferred standards” for communities
planning to implement a diversion program:
Alberta’s communities have different types of organizations and agencies
potentially offering similar services
In order to work together in a case management model, each service provider
needs to feel confident that others are following the same set standards
From a risk management perspective, documented and adhered to standards help
to minimize the risk to the individual and the community
For eventual evaluation of program effectiveness on a provincial level.
Base and Preferred Standards are defined below and discussed for each support service.
Base standards are those that outline a base level of care and delivery of services
for a diversion program. These base (or minimum) standards are considered to be a point
from which to build.
Preferred standards are those that reflect a strived for, yet realistic level of practice
with realistic resources and integrated services, and ultimately leading to an opportunity to
provide for appropriate immediate and long-term support for both—individuals with mental
illness and the families who care for them. These standards meet the requirements and
standards as set out by the Canadian Council on Health Services Accreditation (CCHSA)
and best practices as identified through current evaluation and research literature.11 An
accountability and evaluation component is included in Section VI: Evaluation and
Accountability to allow for a monitoring of services as they relate to specific standards.
About the Canadian Council on Health Services Accreditation…
The Canadian Council on Health Services Accreditation (CCHSA), which was started in 1958, is an independent, non-government, non-profit organization that functions as the major accrediting body for organizations across all health sectors in Canada. The standards set by CCHSA are considered “goals to be reached” by the specific organization. In developing the standards, CCHSA gets input from the organizations using them, as well as consulting with health professionals, consumers and other experts.

Section V: Appropriate Care, Support & Treatment page 18
Standards Applied To Each Service The base and preferred standards are outlined for each of the support services. Under
each service, key components, for instance, staffing competency and accessibility, are
discussed. While the standards provide a baseline, they are not to be considered
restrictive or all-inclusive and may be modified in consideration of specific community
resources. These standards will continue to be developed—on the provincial level, in
Phase 2 of the Implementation; on the community level, based on the community’s
available resources.
1a. Family
Best practices literature indicates that including families or extended family, if appropriate,
in care, support and treatment is important for an individual with mental illness. In such
cases, the family is the primary caregiver and is often involved with the individual with
mental illness for the long term. Because of this involvement, the family needs to be
considered as important to a community’s plans for appropriate care, support and
treatment in a diversion program.
Families may take many forms and meanings—from the single parent family to the
stepfamily, the extended family to the nuclear family. The definition will vary according to
culture, religion or life experience. However, families are not simply people connected by
blood or kinship and accordingly labeled “family”. They need to have strong emotional
bonds, a feeling of belonging and commitment to each other.
The reasons for including family, if appropriate, are many:
It is without doubt that social isolation including the absence of family support is a
significant factor leading to the relapse of persons with mental illness. Overall,
family support can be fundamental to providing the client with the emotional
support and environment needed to create continued stabilization.
The impact of mental illness upon family members can be far reaching, from fear
and denial to emotional and financial exhaustion. A challenge that often faces
these families is weak or non-existent support and on many occasions, exclusion
from the care planning process, yet family members often are expected to bear
much of the responsibility for primary care.

Section V: Appropriate Care, Support & Treatment page 19
Despite the potential positives of having family involvement, in some cases it may not be
in the best interest of the individual with mental illness or the family to have family to be
involved, for a number of reasons:
The offence committed by the individual may have involved a family member.
The family is estranged from the individual and is unwilling to be involved.
The individual is unwilling to be involved with the family.
Other issues within the family make it not in the best interest of the individual.
If none of the above situations with the family exists and the family and the individual are
willing, then this informal support may prove to be useful in the treatment and care plan.
Consent from the individual must also be obtained. (Note: Efforts to receive consent should be not done while the individual is a state of crisis. Should initial attempts at receiving consent not be successful, the case management team is encouraged to continue to attempt to obtain consent at designated intervals, particularly in situations in which the family is willing to provide the needed emotional support and environment to create the individual’s continued stabilization.)
Base Standards A genuine desire by the family to be involved in
the care, support and treatment
Preferred Standards A genuine desire by the family to be actively
involved in the care, support and treatment
The family is given appropriate information regarding the nature and impact of the illness, if appropriate, and the process for accessing community resources
The family is given the opportunity for education and training regarding the nature of the illness and understands the process for accessing community resources
The family is aware of who functions in the role of case manager and how to contact that individual/team
The family works closely with the case management team on a consultative basis, when appropriate and required, in the treatment planning
If appropriate, for youth with mental illness in conflict with the law, the family or guardian is aware of any discharge planning from psychiatric emergency, inpatient treatment, or incarceration
If appropriate and consented to, for adults with
mental illness who are in conflict with the law, the family is aware of any discharge planning from psychiatric emergency, inpatient treatment or incarceration
If appropriate, for youth with mental illness in conflict with the law, the family or guardian is consulted on any discharge planning from psychiatric emergency, inpatient treatment, or incarceration
If appropriate and consented to, for adults with
mental illness who are in conflict with the law, the family is consulted on any discharge planning from psychiatric emergency, inpatient treatment or incarceration
Opportunities are created for respite care for
families (as defined) who are actively involved with individuals with mental illness who are in a community diversion program
A clear established system for providing respite exists for families who are actively involved with individuals with mental illness who are in a community diversion program

Section V: Appropriate Care, Support & Treatment page 20
1b. Other Community Groups/Individuals
Other community groups/individuals may assume an important role in the individual’s care
and treatment, including situations in which family may require assistance or there is no
family involvement. Examples may include teachers, church leaders, and Aboriginal
community elders. These individuals or groups must understand the nature and extent of
their involvement and be willing to accept the role. As indicated by the appropriate
legislation, consent from the individual must also be obtained.
Base Standards The Community person is given appropriate
information regarding the nature and impact of the illness, if appropriate, and the process for accessing community resources
Preferred Standards The Community person is given the opportunity
for education and training regarding the nature and impact of the illness and understands the process for accessing community resources
The Community person is aware of who
functions in the role of case manager and how to contact that individual/team
The Community person works closely with the case management team on a consultative basis, when appropriate and required, in the treatment planning
If appropriate, for youth with mental illness in conflict with the law, the Community person is aware of any discharge planning from psychiatric emergency, inpatient treatment, or incarceration
If appropriate and consented to, for adults with
mental illness who are in conflict with the law, the Community person is aware of any discharge planning from psychiatric emergency, inpatient treatment or incarceration
If appropriate, for youth with mental illness in conflict with the law, the Community person is consulted on any discharge planning from psychiatric emergency, inpatient treatment, or incarceration
If appropriate and consented to, for adults with
mental illness who are in conflict with the law, the Community person is consulted on any discharge planning from psychiatric emergency, inpatient treatment or incarceration
Knowledge of a range of local community resources and willingness to access those resources, including justice, corrections, addictions, probation, police and advocacy and support.
Understanding of a range of local community resources and skill in accessing those resources, including justice, corrections, addictions, probation, police and advocacy and support.

Section V: Appropriate Care, Support & Treatment page 21
2. Mental Health & Psychiatric Services
Mental health and psychiatric services refer to assessment and treatment and
consultation services across the continuum of health, inclusive of crisis/emergency
responses, short-term inpatient treatment and outpatient/outreach.
Following are the Base and Preferred Standards for several areas associated with the
provision of mental health and psychiatric services:
Base Standards 1. Staffing Core Competency Education and comparable experience in a
health-related field or social sciences
Preferred Standards 1. Staffing Core Competency Education and minimum 2 years experience in
health-related field or social sciences, preferably with the target population
Practical knowledge of psychiatric illness
related to youth, adult and geriatric Education/training and experience in
assessment and clinical interventions related to crises and mental health emergencies
Extensive practical knowledge of psychiatric illness related to youth, adult and geriatric
Experience with mental illness and understanding
of its relationship to offending behavior Education/training and experience in assessment
and clinical interventions related to mental health emergencies, for managing risk for Fetal Alcohol Syndrome, if it is a
contributing factor to offending behavior Experience working within an interdisciplinary
approach to care Training and experience working with individuals
with co-occurring mental illness and addictions Experience working with professionals representing
criminal justice system, inclusive of law enforcement, probation and corrections
Adequate knowledge of appropriate Acts,
inclusive of the Mental Health Act, FOIP, HIA, Criminal Code, YCJA, Alcohol and Drug Abuse Act, Child Welfare Act or resources by which to gain that knowledge
Good knowledge of appropriate Acts, inclusive of Mental Health Act, FOIP, and HIA and adequate knowledge of Criminal Code, YCJA, Alcohol and Drug Abuse Act, Child Welfare Act and good community resources related to these Acts
Understanding of range of local community roles and resources, including justice, addictions, advocacy, etc., and willingness to access those resources
Understanding of range of local community roles and resources, including justice, addictions, advocacy, etc., and skill in accessing those resources

Section V: Appropriate Care, Support & Treatment page 22
2. Access to Services Mental health services are provided to
individuals who are in conflict with the law and are referred
Whenever possible, individuals with mental
illness who are at risk of offending have access to mental health and psychiatric services before it is necessary for law enforcement to be involved, as part of the continued support for prevention and intervention programs.
2. Access to Services Mental health services are provided to individuals
who are in conflict with the law and are referred Whenever possible, individuals with mental illness
who are at risk of offending have access to mental health and psychiatric services before it is necessary for law enforcement to be involved as part of the continued support for prevention and intervention programs.
Access includes both that which involves direct in-person contact with a service OR that which is indirect such as services provided by Telemental Health or Community Geographic Resource Teams (as defined in Glossary) and supported by a mental health professional within the community
Access includes both that which involves direct in-person contact with a service OR that which is indirect such as services provided by Telemental Health or Community Geographic Resource Teams (as defined in Glossary) and supported by a mental health professional within the community
Access to mental health and psychiatric services is timely, as set out by the community definition of “timely”
Access to mental health and psychiatric services is timely as set out by the community definition of “timely” and in conjunction with provincial standards
Mental health service professionals respond
promptly to those who are referred to services from
agencies participating in the Diversion program to information about the services provided to
the target group
To ensure access to assessment, treatment and ongoing support, informal linkages are developed between family physicians and psychiatrists and psychiatric services;
Access to mental health and psychiatric services is integrated and coordinated with other providers, services and organizations
To ensure access to assessment, treatment and ongoing support, a formalized system outlining linkages is developed between family physicians and psychiatrists and psychiatric services;
The individual and family have access to a range of services and alternatives to address the individual’s health problems, as applicable
Transportation is available in cases in which
reasonable access is prohibited by distance as defined by the transportation protocol for each community
Services are provided as close to the individual’s community as possible

Section V: Appropriate Care, Support & Treatment page 23
3. Assessment Consent is received from the individual with
mental illness to perform the assessment, unless a Mental Health Warrant has been executed under Alberta’s Mental Health Act
3. Assessment Consent is received from the individual with mental
illness to perform the assessment, unless a Mental Health Warrant has been executed under Alberta’s Mental Health Act
The assessment is carried out by qualified individuals who
use accepted methods and tools and a biopsychosocial approach (see Glossary)
carried out in a safe manner and environment
The assessment is carried out by qualified interdisciplinary
healthcare providers who use accepted methods and tools and a bio-psychosocial approach
carried out in a safe manner and environment
Assessment is a available in a timely manner in accordance with legal mandates and the diversion program risk management framework of the community
In a crisis/emergency situation, assessment
is available in a timely manner, based on standards set by the community diversion program risk management framework
Assessment is a available in a timely manner in accordance with legal mandates and the diversion program risk management framework of the community
The mental health professional collaborates with other services, for instance, the addictions counselor, to ensure that assessments are completed within the time frames set by the community in conjunction with the defined provincial standards
All relevant collateral information is obtained as
part of assessment, inclusive of family history if available
In a crisis/emergency situation, assessment is available in a timely manner, based on standards set by the community diversion program risk management framework and according to provincial standards
When assessing clients, the assessment is
coordinated among service providers and organizations
When assessing clients, the assessment is coordinated among service providers and organizations
Availability of mobile crisis outreach for immediate assessment / stabilization during crisis situations in which risk of self-harm or harm to others may exist
Availability of crisis line for family or others involved with individual with mental illness for situations in which a potential for risk of self-harm or harm to others may exist
Translation services available, if necessary, during assessments
Specific cultural diversity issues, inclusive of language, are incorporated
4. Treatment The team’s process for deciding whether to
offer services to potential clients and families, if appropriate, includes Obtaining, with consent, the potential
client’s history Using set criteria for accepting clients Determining if its services fit the potential
client’s needs and wishes Identifying and addressing the client’s
immediate and urgent needs
4. Treatment The team’s process for deciding whether to offer
services to potential clients and families, if appropriate, includes Obtaining, with consent, the potential client’s
history Using set criteria for accepting clients Determining it its services fit the potential
client’s needs and wishes Identifying and addressing the client’s
immediate and urgent needs

Section V: Appropriate Care, Support & Treatment page 24
Using set guidelines to decide on priorities for service
Taking into account the views of all providers involved with the client
Recording the decision The team delivers and records service in
accordance with current legislation, accepted standards or practice and guidelines, and codes of ethical practices
There is an established “plan of care” in
which the team considers the individual’s biopsychosocial needs, informed choices and preferences, if appropriate
The plan of care is based on the individual’s
assessment and any changes to the individual’s needs, and provides effective options
The treatment plan is in keeping with the
safety needs of the individual and community
In keeping with an integrated plan, the roles
and responsibilities of the team, other providers, other organizations, families and the individual are outlined
Using set guidelines to decide on priorities for service
Taking into account the views of all providers involved with the client
Recording the decision
The team delivers and records service in accordance with current legislation, accepted standards or practice and guidelines, and codes of ethical practices
There is an established “plan of care” in which the interdisciplinary team considers the individual’s biopsychosocial needs, informed choices and preferences, if appropriate
The plan of care is based on the individual client’s assessment, any changes to the individual’s needs, research and best practices evidence and provides effective options
The treatment plan is in keeping with the safety needs of the individual and the community and attempts to minimize risk while focusing on the individual’s long term wellness
The team’s services are integrated and coordinated to ensure continuity An interdisciplinary approach is used From first contact, clients and their families, if
appropriate, can identify and contact the team member responsible for coordinating their service
In keeping with an integrated plan, the roles and responsibilities of the team, other providers, other organizations, clients and families are outlined
In developing an integrated plan of care, the team describes where and how services will be provided, goals, expected results, and transition or follow-up once clients leave the diversion service
The use of medications and other treatment modalities is safe, efficient and effective
The use of medications and other treatment modalities is safe, efficient and effective and promotes the best possible quality of life
The team has access to current information and advice, and receives ongoing education on using medications and other treatment modalities
The team helps and encourages the individuals to participate in developing and carrying out the service plan
With the individual and their family, if appropriate, the team monitors the individual’s progress in achieving goals and expected results
There is transition and follow up by the case manager of the treatment and care of the individual client, inclusive of evidence that interventions offered are effective
There is transition and follow-up by the case manager, inclusive of evidence that interventions offered are effective, evaluation of the individual’s satisfaction with services and functioning within the community Services are coordinated by facilitating clients, their
families, and service providers to work together, by matching clients with the most appropriate service provider(s), level of service, and resources across the continuum

Section V: Appropriate Care, Support & Treatment page 25
3. Ethnocultural
In many communities, an individual’s care, support and treatment needs are better met if
his/her ethnocultural background is considered in the planning. The appropriateness of
using culturally specific care and treatment should be determined through discussions
with the individual. It should not be assumed that because the individual is of a specific
ethnocultural background that he/she wishes to be actively involved in support services
that have been designed by and for individuals from the same background. For instance,
an individual who is from a First Nations community may not be interested in being
involved with an elder from that community as part of the support. As indicated by the
appropriate legislation, consent from the individual must be obtained prior to sharing
information.
Base Standards 1. Staffing Core Competencies An understanding of and sensitivity to cultural
diversity is required of all organizations and agencies involved in an individual’s care and treatment
Preferred Standards 1. Staffing Core Competencies An understanding of and sensitivity to cultural
diversity is required of all organizations and agencies involved in an individual’s care and treatment
For staff involved in delivering culturally specific care and treatment support:
Some experience in providing support to individuals with mental illness
Willingness to work with case management team in the delivery of services
For staff involved in delivering culturally specific care and treatment support:
Experience with mental illness and understanding of its relationship to offending behavior
Willingness to work with case management team in the delivery of services
Successful completion of a Suicide Awareness Workshop
Training and experience in assessment of crises and addictions emergencies
Resources by which to access information
about appropriate Acts, inclusive of the Mental Health Act, FOIP, HIA, Criminal Code, YCJA, Child Welfare Act, Alcohol and Drug Abuse Act
Resources by which to access information about appropriate Acts, inclusive of the Mental Health Act, FOIP, HIA, Criminal Code ,YCJA, Child Welfare Act, Alcohol and Drug Abuse Act
2. Access /community resources Irrespective of cultural background, access to
services must be provided with no exclusions An understanding of the roles of community
resources dedicated to culturally specific needs
2. Access / community resources Irrespective of cultural background, access to
services must be provided with no exclusions A listing of community resources related to
culture, inclusive of their mandates
Availability of interpreters either locally or via Telemental Health services in the case of psychiatric assessment
Availability of interpreters either locally or via Telemental Health services in the case of psychiatric assessment A database of available interpreters

Section V: Appropriate Care, Support & Treatment page 26
4. Accommodations Research and stakeholder consultations support the belief that diversion of individuals
with mental illness who are in conflict with the law becomes more difficult without key
supports such as housing. The availability of suitable and affordable housing for this
target population is typically limited, especially in communities in which privately run or
government funded housing is minimal. These communities should examine creative
options to access accommodations, for instance, those offered by private citizens,
provided that they are “approved” by the case management team and that the individual
with mental illness is considered to be stable enough.
Base Standards 1. Staffing Core Competency Individuals involved in providing housing require
a basic understanding of the needs of individuals with mental illness or be provided with training in regards to those needs and be approved by the case management team
Short stay housing staff and group home managers have a basic understanding of the needs of individuals with mental illness, with the housing being approved by the appropriate government bodies
Preferred Standards 2. Staffing Core Competency Individual citizens involved in providing housing
require a basic understanding of the needs of individuals with mental illness or be provided with training in regards to those needs and be approved by the case management team
For formalized group home settings or approved short stay housing, at least one staff should have a combined education and 2 years experience with individuals who are in conflict with the law
Basic understanding of the relationship between mental illness and addictions
Understanding of Suicide Awareness Knowledge of Standard First Aid Approved Group Home Operators Course, if
applicable
Experience with mental illness and addictions and an understanding of their relationship to offending behavior Successful completion of a Suicide Awareness Successful completion of Standard First Aid Approved Group Home Operators Course, if
applicable Training and experience in assessment of crises
and addictions emergencies
Adequate knowledge of appropriate Acts, inclusive of the Mental Health Act, FOIP, HIA, Criminal Code, YCJA, Child Welfare Act, Alcohol and Drug Abuse Act or resources by which to gain that knowledge
Good knowledge of appropriate Acts, inclusive of Mental Health Act, FOIP, and HIA and adequate knowledge of Criminal Code, YCJA, Child Welfare Act, Alcohol and Drug Abuse Act and good knowledge of community resources related to these Acts
Understanding of range of local community
resources and supports and willingness to access those resources
Understanding of range of local community resources and supports and skill in accessing those resources
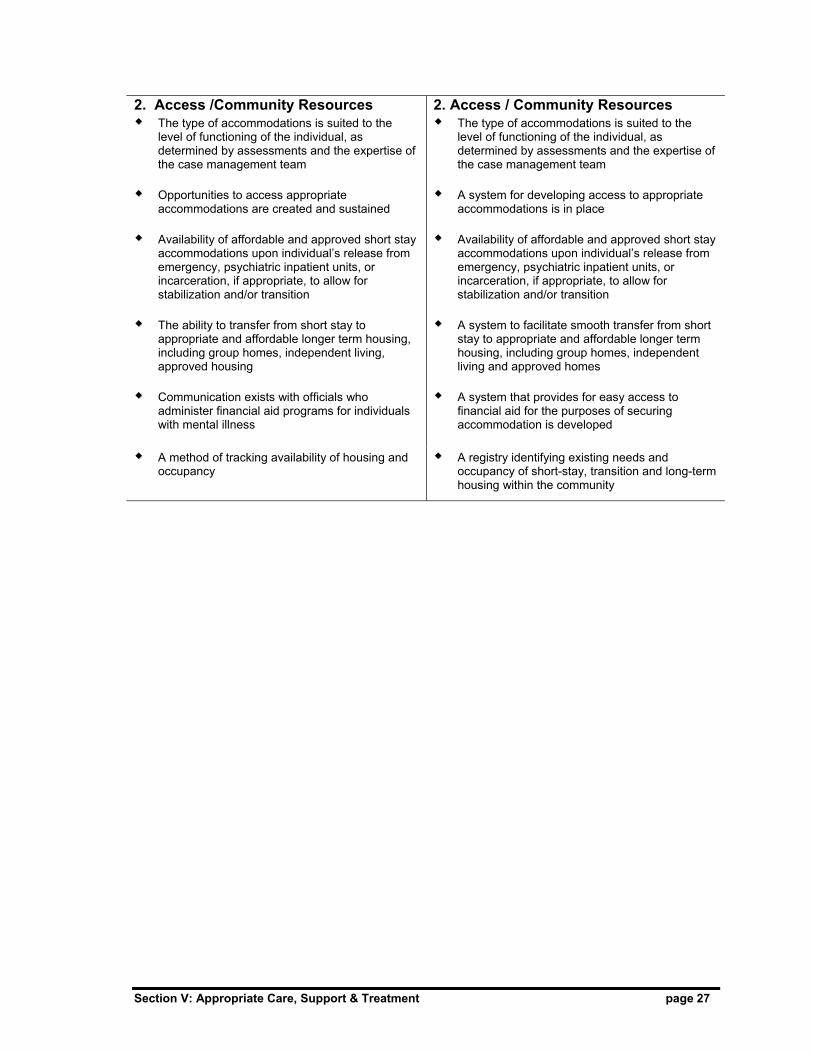
Section V: Appropriate Care, Support & Treatment page 27
2. Access /Community Resources The type of accommodations is suited to the
level of functioning of the individual, as determined by assessments and the expertise of the case management team
Opportunities to access appropriate
accommodations are created and sustained Availability of affordable and approved short stay
accommodations upon individual’s release from emergency, psychiatric inpatient units, or incarceration, if appropriate, to allow for stabilization and/or transition
The ability to transfer from short stay to
appropriate and affordable longer term housing, including group homes, independent living, approved housing
Communication exists with officials who
administer financial aid programs for individuals with mental illness
2. Access / Community Resources The type of accommodations is suited to the
level of functioning of the individual, as determined by assessments and the expertise of the case management team
A system for developing access to appropriate
accommodations is in place Availability of affordable and approved short stay
accommodations upon individual’s release from emergency, psychiatric inpatient units, or incarceration, if appropriate, to allow for stabilization and/or transition
A system to facilitate smooth transfer from short
stay to appropriate and affordable longer term housing, including group homes, independent living and approved homes
A system that provides for easy access to
financial aid for the purposes of securing accommodation is developed
A method of tracking availability of housing and
occupancy A registry identifying existing needs and
occupancy of short-stay, transition and long-term housing within the community

Section V: Appropriate Care, Support & Treatment page 28
5. Addictions Addictions services refer to assessment, treatment and reassessment, including
crisis/emergency response, short-term inpatient treatment and outpatient/outreach for
individuals who are suspected of having both substance abuse and mental health
problems and are in conflict with the law. The services focus specifically on how the
substance has affected the major life areas of the individual in a negative way.
Following are the Base and Preferred Standards for several areas associated with the
provision of addictions services for individuals who are identified as having both
substance abuse and mental illness and who are in conflict with the law:
Base Standards 1. Staffing Core Competency Combined education and experience with
addictions counseling, as deemed appropriate by AADAC
Preferred Standards 1. Staffing Core Competency Combined education and 2 years experience
in addictions counseling with individuals who are in conflict with the law
Basic understanding of the relationship between mental illness and substance abuse/misuse
Experience with mental illness and substance abuse/misuse and understanding of the relationship of each to offending behavior
Training and experience in assessment of
crises and addictions emergencies
Adequate knowledge of appropriate Acts, inclusive of the Alcohol and Drug Abuse Act, Mental Health Act, FOIP, HIA, Criminal Code and YCJA, Child Welfare Act or resources by which to gain that knowledge
Good knowledge of appropriate Acts, inclusive of Alcohol and Drug Abuse Act, Mental Health Act, FOIP, and HIA and adequate knowledge of Criminal Code and YCJA, Child Welfare Act and good knowledge of community resources related to these Acts
Understanding of range of local community resources and supports, and willingness to access those resources
Understanding of range of local community resources and supports, and skill in accessing those resources
2. Access / Community Resources As part of an integrated approach, access to
addictions services is based on which is the most prevalent—the mental health or addictions’ needs
2. Access / Community Resources As part of an integrated approach, access to
addictions services is based on which is more prevalent—the mental health or addictions’ needs
Addictions services must be provided to individuals with mental illness who are in conflict with the law and are referred and consent to treatment
Addictions services must be provided to individuals with mental illness who are in conflict with the law and are referred and consent to treatment

Section V: Appropriate Care, Support & Treatment page 29
Access may include that provided by the 1-800 number or by Internet connection and is supported by an addictions counsellor within the community
Access may include that provided by the 1-800 number or by Internet connection and is supported by an addictions counsellor within the community
Access to addictions services is timely, as set out by the community and in accordance with the Provincial Access Standard. Summarized, this standard allows for the following:
7 calendar days for the main Screening Assessment Interview to be completed from the date of the service request
up to 21 days for additional Assessment for youth.
Access to addictions services is timely, as set out by the community and in accordance with the Provincial Access Standard. Summarized, this standard allows for the following:
7 calendar days for the main Screening Assessment Interview to be completed from the date of the service request
up to 21 days for additional Assessment for youth.
Transportation is available in cases in which
reasonable access is prohibited by distance as defined by transportation protocol for each community
Services are provided as close to the individual’s community as possible
3. Assessment Assessments are voluntary carried out by qualified individuals who use
accepted methods and tools, inclusive of the standard addictions assessment tool required provincially.
carried out in a safe manner and environment
available in a timely manner in accordance with legal mandates
In a crisis/emergency situation, assessment is
available in a timely manner, based on standards set by the community and in accordance with AADAC’s Provincial Access Standards.
3. Assessment Assessments are voluntary carried out by qualified individuals who use
accepted methods and tools and a bio-psychosocial approach, inclusive of the standard addictions assessment tools
carried out in a safe manner and environment
available in a timely manner in accordance with legal mandates and the community’s risk management framework
The addictions counselor collaborates with the
mental health professionals to ensure that a complete assessment is completed within the time frames set by the diversion program
All relevant collateral information is obtained
with assessment, inclusive of family history if available
In a crisis/emergency situation, assessment is
available in a timely manner, based on standards set by the community in its risk management framework and in accordance with AADAC’s Provincial Access Standards
Availability of outreach and residential services
to provide immediate assessment and possible stabilization through detox in which there is a risk of self-harm or harm to others Availability of assistance for family or others
involved with individual with mental illness for situations in there is a potential of risk of self-harm or harm to others
Specific ethnocultural issues, including language, are incorporated

Section V: Appropriate Care, Support & Treatment page 30
4. Treatment There is an established treatment plan in which
the addictions counsellor considers the individual’s physical and biopsychosocial needs, informed choices and preferences, if appropriate
The plan of care is based on the individual’s
assessment The plan of care provides effective options and
is in keeping with the safety needs of the individual and the community
In keeping with an integrated plan and case
management protocols, the roles and responsibilities of the treatment team, other providers, other organizations, families and the individual are outlined
The addictions service supports the use of
medications and other treatment modalities which are considered to be safe, efficient and effective
The counsellor helps and encourages the
individual to participate in developing and carrying out his/her treatment plan
There is transition, follow up and after care
4. Treatment There is an established plan of care in which
the addictions counselor collaborates with the case management team to consider the individual’s physical and psychosocial needs, informed choices and preferences, if appropriate
The plan of care is based on the individual's
assessment and any changes to the individual’s needs
The plan of care provides effective options and
is in keeping with the safety needs of the individual and the community and attempts to minimize risk while focusing on the individual’s long term wellness
In keeping with an integrated plan, the roles
and responsibilities of the team, other providers, other organizations, families and the individual are outlined
The addictions service supports the use of
medications and other treatment modalities, which are safe, efficient and effective and promote the best possible quality of life
The counsellor has access to current
information and advice, and receives ongoing education in varied treatment modalities
With the individual and families, if appropriate,
the counsellor monitors the individual’s progress in achieving goals and expected results
There is transition and follow-up by the case
manager, inclusive of evaluation of the individual’s satisfaction with services and functioning within the community

Section V: Appropriate Care, Support & Treatment page 31
6. Medical
Medical services include any assessment, treatment and care provided in relation to
physical health issues of individuals with mental illness or co-occurring mental health and
addictions disorders who are in conflict with the law. They may also include any ongoing
provision of medication required for the treatment of the mental illness.
In many communities, especially those in which mental health and psychiatric services are
limited, the family physician, or possibly nursing staff, may be involved in crisis
intervention either through the local hospital emergency services or the family practice.
Base Standards 1. Staffing Core Competency Professional designation with appropriate
provincial body—Alberta College of Physicians and Surgeons, Alberta Associated of Registered Nurses, etc.
Preferred Standards 1. Staffing Core Competency Professional designation with appropriate
provincial body—Alberta College of Physicians and Surgeons, Alberta Associated of Registered Nurses, etc.
Basic understanding of the relationship between
mental illness and substance abuse/misuse
Experience with mental illness and substance abuse/misuse and understanding of the relationship of each to offending behavior
Training and experience in assessment of mental health & addictions emergencies
Adequate knowledge of appropriate Acts,
including the Mental Health Act, FOIP, HIA, Alcohol and Drug Abuse Act, and some information about the Criminal Code and YCJA, Child Welfare Act or resources by which to gain that knowledge
Good knowledge of appropriate Acts, including Mental Health Act, FOIP, HIA, Alcohol and Drug Abuse Act, and adequate knowledge of Criminal Code and YCJA, Child Welfare Act and good knowledge of community resources related to these Acts
Understanding of range of local community
resources and supports and willingness to access those resources
Understanding of range of local community resources and supports and skill in accessing those resources
2. Access / Community Resources Timely access to local hospital emergency for
physical or mental health crises
Consultation and collaboration with local mental health professionals for mental health assessment, treatment and referral, with addictions and other social and support services as required, and criminal justice officials
2. Access / Community Resources Timely access to local hospital emergency for
physical or mental health crises
A defined system for collaboration with local mental health professionals, addictions, social and support services, and criminal justice officials involved with the individual with mental illness who is in conflict with the law
Clear admission and discharge/transfer criteria within local hospitals in regards to mental health crises, which is communicated to other service providers, including law enforcement and other legal professionals, as appropriate
Clear admission and discharge/transfer criteria within local hospitals for mental health crises, which is communicated to other service providers, including law enforcement and other legal professionals, as appropriate

Section V: Appropriate Care, Support & Treatment page 32
7. Support, Self Help And Transition
Support and Self Help Services could be provided at any diversion point and would
include organizations that provide information and advocacy, aids to independent living,
connection to financial support, and even spiritual support.
Transition services would typically be provided for those individuals for whom a sentence
was imposed, especially those individuals released from incarceration. In some
communities, organizations that focus specifically on transition and referral/connection of
the target population exist, especially for the youth, while in other communities, the
transition role is carried out by varied agencies and groups. These agencies and groups
have different mandates, most of which focus on providing support and fostering the
individual’s ability to function independently.
The importance of the involvement of agencies, organizations and volunteers in the target
population’s continued well being cannot be understated. In fact, in many situations, the
individual with mental illness may have a “life time” of contact with some of these groups,
especially if a sense of safety and community is created.
This same sense of “community” may never exist with those service providers involved in
active treatment or with family members.

Section V: Appropriate Care, Support & Treatment page 33
Base Standards 1. Staffing Core Competency Experience in delivering services that meet the
needs of individuals with mental illness Willingness to provide services to individuals
with mental illness and addictions, if applicable, who are in conflict with the law
Preferred Standards 2. Staffing Core Competency Extensive experience in delivering services that
meet the needs of individuals with mental illness who are in conflict with the law
Willingness to provide services to individuals
with mental illness and addictions, if applicable, who are in conflict with the law—no discrimination
Basic understanding of the relationship between
mental illness and addictions Understanding of Suicide Awareness Knowledge of Standard First Aid
Experience with mental illness and understanding of its relationship to offending behavior Successful completion of a Suicide Awareness
Workshop Successful completion of Standard First Aid Training and experience in assessment of crises
and addictions emergencies
Resources by which to access information about appropriate Acts, inclusive of the Mental Health Act, FOIP, HIA, Criminal Code and YCJA, Alcohol and Drug Abuse Act, Child Welfare Act
Resources by which to access information about appropriate Acts, inclusive of the Mental Health Act, FOIP, HIA, Criminal Code and YCJA, Alcohol and Drug Abuse Act, Child Welfare Act
Understanding of range of local community resources and supports and willingness to access those resources
Understanding of range of local community resources and supports and skill in accessing those resources
2. Access /Community Resources Availability of Information and knowledge about
the community resources dedicated to support and self help
2. Access / Community Resources A listing of community resources, including their
mandates, roles and limitations
Timely access to services, based on requirements set out by community
Continued access to those services beyond
time periods mandated by criminal justice system, if applicable
Timely access to services, based on requirements set out by community
Continued access to those services beyond
time periods mandated by criminal justice system, if applicable

Section V: Appropriate Care, Support & Treatment page 34
8. Recreational/ Vocational
Sustained community tenure for an individual with mental illness who has been in conflict
with the law is often difficult to achieve without supports that can enhance that individual’s
feeling of self and community worth. Recreational and vocational supports play an
important role in providing a sense of achievement and community involvement. The
recreational supports may include involvement with a community program or team. This
approach has been used with youth, especially with the intent of increasing their range of
Base Standards 1. Staffing Core Competencies Recreational: Experience working with
individuals with mental illness Educational/Vocational: Education and
experience in providing vocational services to individuals with mental illness
Preferred Standards 1. Staffing Core Competencies Recreational: Appropriate Recreational
Therapist courses and experience working with the target population Educational/Vocational: Education and
experience in providing vocational services to individuals with mental illness
For staff involved in delivering programs,
Willingness to work with individuals with mental illness
Willingness to collaborate with case management team
For staff involved in delivering programs Experience with mental illness and
understanding of its relationship to offending behavior, or working in consultation with mental health professional
Collaboration with case management team in the delivery of services
For Recreation: Successful completion of Standard
First Aid Successful completion of Suicide
Awareness Workshop
Resources by which to access information about appropriate Acts, inclusive of the Mental Health Act, FOIP, HIA, Criminal Code and YCJA, Child Welfare Act
Resources by which to access information about appropriate Acts, inclusive of the Mental Health Act, FOIP, HIA, Criminal Code and YCJA, Child Welfare Act
2. Access / Community Resources Connections with community programs and
resources who are willing to provide services Direct support and guidance to facilitators, if
necessary, in the delivery of services, particularly with a focus on keeping the target population involved in the services and providing assistance with mental health issues
2. Access / Community Resources Connections with community programs and
resources who are willing to provide services Trained recreational therapists who are directly
involved in the delivery of services in conjunction with program facilitators Educators and vocational program facilitators
who have experience and courses regarding delivering programs to special needs clients

Section V: Appropriate Care, Support & Treatment page 35
In summary, the above Base and Preferred Standards are intended to be guidelines to
assist communities in implementing a diversion program that provides a level of care,
support and treatment that better enable the target population to achieve the goal of
sustained community tenure. Communities may wish to set additional standards that
reflect their unique resources, specific geographic issues and community needs.

Section V: Appropriate Care, Support & Treatment page 36
EENNDDNNOOTTEESS 1 Provincial Diversion Framework Working Committee. (2001). Alberta’s Provincial Diversion
Framework: Reducing the Criminalization of Individuals with Mental illness.
2 Provincial Diversion Working Committee. (2002). Alberta’s Provincial Diversion Program: Proposed Implementation Plan for Reducing Criminalization of Individuals with Mental Illness.
3 A series of articles, as well as the Calgary Diversion Project, discuss community tenure as a desiredfinal goal. Continued refinement of the definition of community tenure will occur in Phase Two.
4 Provincial Diversion Framework Working Committee. (2001). Alberta’s Provincial Diversion Framework: Reducing the Criminalization of Individuals with Mental illness.
5 Gorey, K.M., et al. (1998). Effectiveness of Case Management with Severely and Persistently Mentally Ill People. Community Mental Health Journal, 34(3): 241-250. Marty, D., Rapp, C.A. & Carlson, L. (2001). The Experts Speak: The Critical Ingredients of Strengths Model Case Management. Psychiatric Rehabilitation Journal. 24(3): 214-221. Ziguras, S.J. & Stuart, G.W. (2000). A Meta-Analysis of the Effectiveness of Mental Health Case Management Over 20 Years. Psychiatric Services, 51(11): 1410-1421.
6 Serin. R. (2001). Treatability, Treatment Responsivity and Risk Management. In Douglas. K.S. et al. (Ed) HCR-20 Violence Risk Management Companion Guide (p. 113). British Columbia: Mental Health, Law, and Policy Institute, Simon Fraser University.
7 Henggeler, S.W. et al. (1998). Multisystemic treatment of antisocial behavior in children and adolescents. New York: The Guildford Press.
8 Provincial Diversion Working Committee. (2002). Alberta’s Provincial Diversion Program: Proposed Implementation Plan for Reducing Criminalization of Individuals with Mental Illness.
9 Wright, & Leahey. (2000). Nurses and Families, 3rd Edition.
10 Provincial Diversion Working Committee. (2002). Alberta’s Provincial Diversion Program: Proposed Implementation Plan for Reducing Criminalization of Individuals with Mental Illness.
11 Canadian Council on Health Services Accreditation. (2002). AIM: Achieving Improved Measurement: Accreditation Program (2nd ed). Standards for Mental Health. (This set of standards have been used as the foundation from which to inform both the base and preferred standards throughout this section.) Other Sources that have contributed greatly to the committee’s development of base and preferred standards include, but are not limited to the following: British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S Mental Health Reform Best Practices. (Concepts and standards from all seven reports—Housing, Assertive Community Treatment, Crisis Response/Emergency Services, Inpatient/Outpatient Services, Consumer involvement and Initiatives, Family Support and Involvement, Psychosocial Rehabilitation and Recovery—were considered.) Minkoff, K. (2001). Developing Standards of Care for Individuals with Co-occurring Psychiatric and Substance Use Disorders. Psychiatric Services, 52(95): 597-599.
Minkoff, K. & Ajilore, C. (1998). Co-Occurring Psychiatric and Substance Disorders in Managed Care Systems: Standards of Care, Practice Guidelines, Workforce Competencies, and Training Curricula. Report of The Center for Mental Health Services Managed Care Initiative. Green, G., et al. (2002). The role and impact of social relationships upon well-being reported by mental health service users: A qualitative study. Journal of Mental Health, 11 (5): 565-579.

SSEECCTTIIOONN VVII EVALUATION & ACCOUNTABILITY Contents DIFFERING VIEWS AND DIFFERING EXPECTATIONS EVALUATION CONSIDERATIONS AND GOALS AN EVALUATION AND ACCOUNTABILITY STRUCTURE APPROACH TO EVALUATION
The Three Levels THE EVALUATION PROCESS APPLIED TO COMMUNITY DIVERSION PROGRAMS
Mapping The Multiple Perspectives Describing The Evaluation Process Focusing The Evaluation Design
CORE COMPONENTS
EVALUATION METHODOLOGY
…………………….……………………….1 ……………………………………………..2 ……………………………………………..4 ……………………………………………..5 ……………………………………………..7 ……………………………………….…...10 ………………………………...……….…14

Section VI: Evaluation and Accountability page 1
DDIIFFFFEERRIINNGG VVIIEEWWSS AANNDD DDIIFFFFEERRIINNGG EEXXPPEECCTTAATTIIOONNSS Each ministry and organization that has been involved in the development of the
Provincial Diversion Program has supported the goal of reducing the criminalization of the
target population and providing appropriate care, support and treatment to these
individuals. Each group is also interested in how the program will impact his/her
organization in its contact with the target population.
The goals are varied depending on the interest group; thus, the “measures of success”
through evaluation also vary to some degree. For instance, the RCMP and municipal law
enforcement would like a diversion program to result in a reduced number of “mental
health crisis calls”; an increase in their knowledge of “what to do” when they encounter an
individual with mental illness who is in a crisis; and even a reduced number of officer
hours devoted to monitoring an individual with mental illness who has committed a minor
offence because there is no where else to keep him/her besides the local jail cell.
Consumer groups would also like to see the above in addition to less stigma associated
with the target population and, of course, better access to care, support and treatment
services instead of incarceration, and so forth.1 Each ministry and organization has its
own “expectations” of a Provincial Diversion Program. A comprehensive evaluation
program will assess not only how well the target population is able to sustain community
tenure but also how well the expectations are met and the cost effectiveness of doing so.
This section on Evaluation and Accountability provides general guidelines for:
overall evaluation structure and general goals
process for implementing an evaluation plan in each community diversion program
suggested areas of evaluation, along with potential process and core components
from which outcome measures can be created
suggested methodology.
Further development of specifics related to the process and outcomes measures and
performance indicators will be done in Phases Two, Three and Four, in consultation with
stakeholders and in response to service delivery configurations and governance structure.

Section VI: Evaluation and Accountability page 2
EEVVAALLUUAATTIIOONN CCOONNSSIIDDEERRAATTIIOONNSS AANNDD GGOOAALLSS Since the Provincial Diversion Program is “multi stakeholder, multi level, and cross
ministerial”, the potential for creating an overly cumbersome system of evaluation that
tries to meet all perceived needs is a primary concern. Efforts to provide meaningful
information that will inform key stakeholders, whether they are funders or consumers,
must take into consideration the following:
recognizing the importance of having a coordinated approach to evaluation
across the province, while still acknowledging and respecting the diversity of
communities and their resources
maintaining the credibility of the evaluation procedure and tools through
employing scientific rigor while ensuring that the procedure and tools are useable
on several levels (clinical, case management, evaluation, and potentially
research), user friendly, easy to administer and document, and cost effective
relating the outcomes to Canadian Council of Health Services Accreditation
(CCHSA) standards, for instance, the four quality dimensions, which include
system competency, client and community focus, responsiveness, and work life.2
CCHSA standards are being used as a benchmark for base and preferred
standards of appropriate care, support and treatment
incorporating where possible measures of success and standardized instruments
already used by key organizational partners, for instance, criminal justice, mental
health, and addictions
assessing the impact of data collection upon the clinical resources within a
community diversion program
providing an Information Technology structure to support data management.
These considerations are based on the basic principle that evaluation should be central to
diversion program service delivery and not considered to be an imposed, artificial task that
is cumbersome to administer.
The above considerations are reflected in the following goals for an evaluation system:

Section VI: Evaluation and Accountability page 3
GOAL 1: The system of evaluation achieves a balance of comprehensiveness and
minimal additional stress on the community resources dedicated to diversion
GOAL 2: The process and outcome measures reflect the needs of the key partners in
the program— client/community, criminal justice system, mental health, addictions—and
where appropriate, incorporate current measures being used by these partners in
measuring success.
GOAL 3: The system of evaluation is developed in conjunction with stakeholders in each
diversion community and is incorporated at the outset of community program development
as part of the collaborative process.
GOAL 4: The evaluation process incorporates each diversion point and is used across
the continuum of care.
GOAL 5: Evaluation encompasses several levels of performance measurement
including process, utilization and outcome-related measures and has qualitative and
quantitative items.
GOAL 6: Evaluation is inherent in the development process of the community diversion
programs, consists of short term (rapid cycle) and longer term process and outcome
measures, performs a quality assurance function, and allows for modifications to the
diversion process should there be issues of quality improvement.
These goals are reflected in the following evaluation and accountability structure, as well
as the process recommended for implementing the structure.
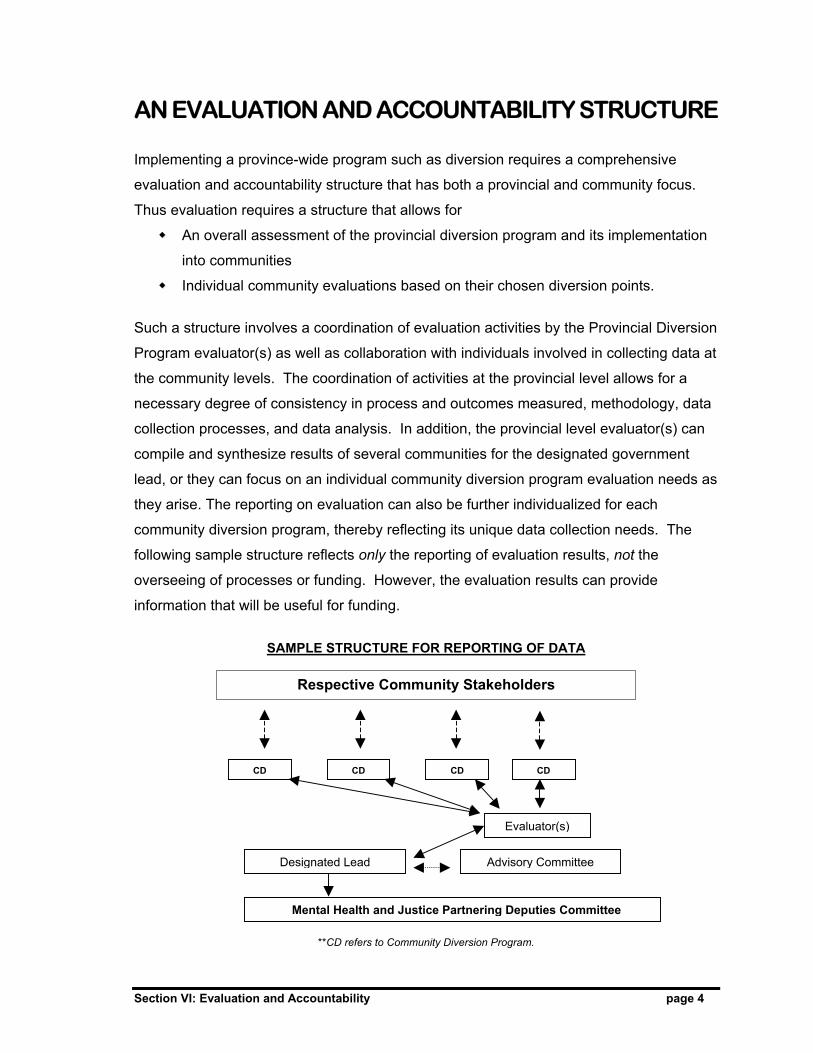
Section VI: Evaluation and Accountability page 4
AN EVALUATION AND ACCOUNTABILITY STRUCTURE Implementing a province-wide program such as diversion requires a comprehensive
evaluation and accountability structure that has both a provincial and community focus.
Thus evaluation requires a structure that allows for
An overall assessment of the provincial diversion program and its implementation
into communities
Individual community evaluations based on their chosen diversion points.
Such a structure involves a coordination of evaluation activities by the Provincial Diversion
Program evaluator(s) as well as collaboration with individuals involved in collecting data at
the community levels. The coordination of activities at the provincial level allows for a
necessary degree of consistency in process and outcomes measured, methodology, data
collection processes, and data analysis. In addition, the provincial level evaluator(s) can
compile and synthesize results of several communities for the designated government
lead, or they can focus on an individual community diversion program evaluation needs as
they arise. The reporting on evaluation can also be further individualized for each
community diversion program, thereby reflecting its unique data collection needs. The
following sample structure reflects only the reporting of evaluation results, not the
overseeing of processes or funding. However, the evaluation results can provide
information that will be useful for funding.
SAMPLE STRUCTURE FOR REPORTING OF DATA
**CD refers to Community Diversion Program.
Respective Community Stakeholders
CD
Evaluator(s)
CD CD CD
Mental Health and Justice Partnering Deputies Committee
Designated Lead Advisory Committee
Section VI: Evaluation and Accountability page 5
AAPPPPRROOAACCHH TTOO EEVVAALLUUAATTIIOONN According to the research and based on practical application, there are generally three
main levels of stakeholders to be considered in the evaluation approach. These three
levels of client /community, program, and system meet the multiple evaluation needs of
Alberta’s Provincial Diversion Program3. Each level reflects what each set of
stakeholders needs to know about the effectiveness of diversion.
The following approach to developing an evaluation and accountability structure is also
based on the Provincial Diversion Program goals and objectives, categories of best
practices, the use of program logic models (discussed further in this Section), and the
information from the Calgary Diversion Project.4
The Three Levels
In terms of the Provincial Diversion Program, the Client /Community Level is focused on
the individual involved in the diversion program, on his/her family and peers, and on the
community as a whole. In terms of the client, information about his/her functioning, quality
of life and satisfaction with services would be the basis of this level of evaluation.
Moreover, how the client functions within the community and how the community views
the client and his/her involvement in the program contribute to the type of information
assessed at this level.
The Program Level relates to each specific community diversion program, the local
funders, care providers (staff), and collaborative stakeholder organizations, for example,
existing mental health clinics and regional health authorities. A major part of its focus is
on the “critical pathways and processes that clients follow from the time the case is
opened to the time it is closed”.5 For the community diversion program, the collaborative
processes involved in developing the program and the use of case management team
approaches are included within the Program Level.
The System Level is considered to be the overarching level focusing on the following:
the provincial bodies, such as ministries and public and private bodies involved in
the allocation of resources and support for the diversion process

Section VI: Evaluation and Accountability page 6
provincial coordination of the actual programs, ensuring best practices and
coordination
the processes of coordination, communication, clinical assistance that is provided
provincially to the diversion communities.
According to Health Canada’s Review of Best Practices in Mental Health Reform (1997),
the system level measures inform about “whether the service system as a whole is
balanced, integrated, community-based, consumer-driven, accessible, efficient, and cost
effective”.6 This type of information can assist in the decision making regarding funding,
overall quality improvement and maintenance of best practices.
Many of the outcomes required at the Systems Level will overlap and will be relevant to
many of those required at the Program Level, thereby reducing duplication and the need
for additional evaluation resources.
There is a clear relationship between the process and outcome measures applied to each
level. For example, if at the Client Level it is determined the client is not functioning well
and at the Program Level the community arrest or incarceration rates are not reduced,
then the problem could be a result of some action or lack thereof at the System Level.

Section VI: Evaluation and Accountability page 7
TTHHEE EEVVAALLUUAATTIIOONN PPRROOCCEESSSS AAPPPPLLIIEEDD TTOO CCOOMMMMUUNNIITTYY DDIIVVEERRSSIIOONN PPRROOGGRRAAMMSS As outlined in the six goals of an evaluation system for the Provincial Diversion Program,
there needs to be a clear relationship between the data collected within the community
diversion programs, the needs of the provincial governing and funding sources, and the
clients and community. To achieve this balance, the following process has been chosen:
1. Mapping the multiple perspectives together with stakeholders
2. Describing the evaluation process
3. Focusing the evaluation design7
1. Mapping The Multiple Perspectives Together With Stakeholders
In conjunction with the designated evaluator(s) from the Provincial Diversion Program,
each community needs to first answer the question of “who is involved” in order to
ascertain the multiple perspectives. With this in mind,
a) All potential stakeholders need to be defined for each selected diversion point: for
instance, law enforcement, the crown, probation, corrections, mental health,
physicians, client, family, community, etc.
b) For each potential stakeholder, a clear indication of “what constitutes success”
should be examined.
The above steps allow for involvement of stakeholders at the outset of the process. This
approach is supported by the following statement from the Framework for Program
Evaluation in Public Health (1999):
“The evaluation cycle begins by engaging stakeholders (i.e., the person or
organization having an investment in what will be learned from an
evaluation and what will be done with the knowledge)….Stakeholders must
be engaged in the [evaluation] to ensure that their perspectives are
understood. When stakeholders are not engaged, an evaluation might not
address important elements of the program’s objectives, operations, and
outcomes. Therefore, evaluation findings might be ignored, criticized or
resisted…”8

Section VI: Evaluation and Accountability page 8
This step becomes critical to overall acceptance by stakeholders and communities
of the need for evaluation and the process involved. Recognizing that their points
of view are incorporated supports the focus on collaboration as being integral to
successful development and continuation of a community diversion program.
2. Describing The Evaluation Process
In order to arrive at a clear picture (of where, who and why) of the most logical and
relevant points at which to target evaluation, it is important to map in detail the service
delivery process. This sequence of service delivery should be mapped against the
community’s chosen diversion points.
One of the tools recommended by the program development and evaluation literature, and
incorporated by the Calgary Diversion Project in its evaluation, is a program logic model.
Defined, a program logic model
“describes the sequence of events for bringing about change by synthesizing the main
program elements into a picture of how the program is supposed to work….One of the
virtues of a logic model is its ability to summarize the program’s overall mechanism of
change by linking processes… to eventual effects.”9
It is a diagram that is usually developed by program planning groups consisting of
community stakeholders, evaluators, and staff—primarily those groups or individuals that
are knowledgeable about the program’s objectives and/or the client.
A program logic model is described as including the following:
Target group
Resources, i.e., service providers, those responsible for financial / physical
resources
Activities that are necessary to achieve program outcomes
Components that reflect the “conceptually related activities”
Outcomes, including process, short term and long term
Indicators that show when the objectives have been achieved. 10
Basically, it is a mapping that matches the program development and processes to the
outcomes.

Section VI: Evaluation and Accountability page 9
Assessment Main Components
Implementation Objectives
Output
Short Term Outcome
Long Term Outcome
Goal Setting Education Medication Compliance
Complete standard assessment on all clients
Assist client in identifying goals they will work toward in Day Program
Initiate opportunities of learning in response to identified goals Identify community resources…
To improve compliancy to medication regime
Educate re meds and illness
# of goals reached # and type of goals identified
# & type of education needed # & type critical incidents # of clients refused service
# of clients with hx of non-compliancy # of clients in regular contact with physician # & type of resources needed
# of assessments completed # of psychiatric consultations # of clients available
To avoid assessment duplication To identify client needs To expedite most appropriate interventions
Clear purpose of participation in Day P.
Client will participate in identifying goals
To improve match of services to client needs To ensure safety of clients and staff To offer support during transition …
To increase treatment compliance To enhance community tenure To improve communication among caregivers
To provide a seamless system of mental health services
To improve quality of life To decrease involvement in Criminal justice …
Enclosed is an excerpt from a portion of the logic model used by the Calgary Diversion
Project for the development and evaluation of its Day Program.11
**Source: Calgary Diversion Project Annual Independent Evaluation Report, October 2002
3. Focusing The Evaluation Design
The evaluation must be focused to assess the issues of greatest concern to stakeholders,
while targeting the most appropriate and meaningful points of service delivery as
described in the program logic model.
When using the program logic model, the methodology of evaluation should allow for both
short term (or rapid cycle) and longer term outcomes.
Short term (rapid cycle) outcomes are used in order to assess small events of change
under a variety of conditions and to provide feedback in a timely fashion.12 For example,
evaluating the eligibility outcome will give both referral sources and program providers
immediate information about the appropriateness of referral. This information can then be
used to educate referral sources and reduce the time spent in triaging ineligible clients.

Section VI: Evaluation and Accountability page 10
Basically, using short term (rapid cycle) outcomes provides a method of “accelerating
improvement” in specific areas.13
Longer term outcomes incorporate activities such as using post tests to determine
treatment effectiveness, measures of change upon discharges from the program, follow
up in the community, and so forth.
Both types of outcomes are necessary for evaluation of the Provincial Diversion Program.
CCOORREE CCOOMMPPOONNEENNTTSS FFOORR EEVVAALLUUAATTIIOONN OOFF TTHHEE DDIIVVEERRSSIIOONN PPRROOGGRRAAMM The initial step in focusing the evaluation is addressed in this section, with further
development being part of Phases Two and Three of the Provincial Diversion Program.
The primary step was to examine the themes that appeared to be consistent across the
three levels of client, program and system. These themes were then compared to
domains most prevalent in the literature; CCHSA standards as reflected in Section V:
Appropriate Care, Support and Treatment; the objectives of the Provincial Diversion
Program; and information from the initial stakeholder consultations. The result is a list of
seven Core Components to be used in Provincial Diversion Program evaluation.
These core components are the categories under which specific process, utilization, and
outcome measures will be identified. Having core components helps reduce the potential
complexity associated with a program evaluation because they can be applied to the
needs of varied stakeholders and a number of points of diversion. These core
components are as follows:
1. Communication And Linkages
In its development and delivery of services, the diversion program is based on
collaboration among a number of stakeholders on both the provincial and community
levels. Communication and linkages are the foundation on which each community
diversion program is built and must be sustained. The success of the communication and

Section VI: Evaluation and Accountability page 11
linkages will determine the most comprehensive service for the client while avoiding
duplication or gaps.
2. Safety
One of the clear objectives of the diversion program is to balance safety of the individual,
the rights of the individual, and the safety of the community. The core component of
safety incorporates reduced criminalization, recidivism, community perception of risk, and
ultimately reduced stigma.
3. Standards Of Practice
Standards of practice encompass setting benchmarks, striving for best practices,
adhering to legislation, and assuring overall quality of the program. These standards of
practice should ensure that regardless of where the client resides in Alberta that he/she is
receiving the best possible care, support and treatment to enable sustained community
tenure. Should resources or professional training not be conducive to a community’s
meeting the standards of practice, then recognizing these issues early in the development
of the program allows for closer examination and determination of “what may be needed
in order to ensure the quality of care necessary”. For instance, in communities where
psychiatric care is not available or over extended, then additional resources via
Telemental Health Services or Community Geographic Resource Teams can be provided.
4. Access
Historically, access to services has been a primary concern at all levels, and this concern
was echoed in the initial stakeholder consultations. Plus, at some diversion points, the
access to the program, to assessment and treatment will become even more important to
measure, particularly if delays in access increase the length of time that a person remains
charged with an offence within the criminal justice system.
5. Clinical Outcomes
Although clinical outcomes relate to the components of Net Benefit and Safety on the
system level, the focus of this core component is largely on the Program and Client /
Community level. Clinical outcomes are both tools that providers use for assessment and
treatment and are valuable in measuring day-to-day service delivery. Examples include

Section VI: Evaluation and Accountability page 12
quality of life, risk, symptom reduction, and integration of treatment for co-occurring
disorders.
6. Net Benefit
The effectiveness and overall savings to the province and the community should outweigh
the costs and resources associated with the implementation of a diversion program.
Effectiveness relates to outcome measures such as increased quality of life, symptom
reduction and satisfaction by the client, as well as decreased risk to the communities. The
dollar savings are related to the balancing of the cost of provision of services versus the
cost of law enforcement, incarceration, hospitalization or inpatient admissions related to
mental health crises.
7. Population Health Determinants
As a final component, processes and outcome measures will also be related to the
Population Health Determinants developed by Health Canada.
Within the following table, each core component is presented, along with some examples
of potential areas that may relate to each component at each level of system, program
and client/community. The examples are not set up as definitive measures, simply
because as indicated previously, specific process and outcome measures should be
created in conjunction with and after consultation with stakeholders at all levels.
Creating measures and performance indicators related to each of the examples will be the
responsibility of the Provincial Diversion Program designated evaluator(s), with the goal of
streamlining the evaluation and data collection procedures. The intent is to provide a
comprehensive and systematic approach in which stakeholders’ perspectives are
considered, while reducing the burden on front line staff for the data collection.

Section VI: Evaluation and Accountability page 13
As previously mentioned, stakeholder input is crucial, program logic models need to be
developed, and the evaluation needs to be focused further prior to creating specific
process and outcome measures. This process will occur in the remaining Phases of
Diversion Program Implementation, should there be approval for continuation.
CORE COMPONENT
EXAMPLES
SYSTEM PROGRAM CLIENT Communication & Linkages
Collaboration Information sharing Stakeholder satisfaction Education- cross training Promotion / stigma
Reintegration Inter-agency committee Stakeholder satisfaction Education Stigma
Reintegration from incarceration. Knowing which services are available and how to access
Net Benefit
Costs & Resources Presence and Absence of services Community capacity building
Local operating dollars Presence and Absence of services
Community capacity building
No cost or minimal cost for services
Standards of Practice
Appropriate interventions Best practices Risk management Adherence to legislation Quality assurance Client rights
Case management Base standards Risk management Adherence to legislation Quality assurance Client rights
Know who is case management team Best Quality of Care Access to information on medication
Access
Eligibility criteria Use of diversion points Timeliness
Utilization # of diversion points Timeliness of assessment, treatment, and social support
Minimum time in incarceration Satisfaction with access to services
Safety
Risk Reduced criminalization Recidivism Community perception Stigma
Risk # of clients returning to criminal justice system Structured environments & supports in place Community perception
Knowing who to call in times of crisis Structured environment
Clinical Outcomes
Quality of Life Risk Symptom Reduction Substance Abuse Integration.
Quality of Life Sustained community tenure
Population Health Determinants
Social support network Social environment Health services Culture
Social support network Physical health
Coping mechanisms
Section VI: Evaluation and Accountability page 14
EEVVAALLUUAATTIIOONN MMEETTHHOODDOOLLOOGGYY Discussions of methodology have been integrated throughout this section. The following
summary outlines some of the key principles:
The data gathering methods depend on a number of factors, such as organizational
culture, environment, policy and legislation, resources and the service delivery model
itself.14 There are also several well researched and documented principles of
program evaluation methodology.
As mentioned previously, evaluation should incorporate all levels of service delivery
including client and community, program, and system.
Both short term or episodic, “rapid cycle” measurement and longer-term or longitudinal
measurement should be implemented.
The measurement design should consider the “data gatherer,” assuming that those
involved in data collection would range from professional evaluation staff and research
assistants to service delivery providers and staff involved in the criminal justice
process.
Data collection should be focused and purposeful since the process can be long and
tedious. Data should clearly reflect the program’s objectives using only the quantity
necessary to make decisions and understand the quality of service.
Important characteristics of outcome measures include the following:
Clinically relevant
Easy to understand and teachable methodology
Gathered from multiple respondents
Psychometrically sound
Cost effective
Understandable by a non-professional audience and uncomplicated
interpretation.

Section VI: Evaluation and Accountability page 15
Analytic techniques should anticipate difficulties typically encountered in collection
such as missing data and client refusal.
If possible, a method for follow up should consider comparison between treatment
completers and “drop-outs”
An information technology infrastructure is crucial for ease of data gathering, accuracy
of data, portability of data, and timely information sharing. Many evaluation projects
are hindered by the inability to obtain timely information from a large paper trail.
“Health Canada defines knowledge management as a departmental strategy for
ensuring that health knowledge and information are identified, captured, created,
shared, analyzed, used and disseminated to improve and maintain the health of
Canadians”15
Evaluation processes and standards should also be communicated to the general
public.
In summary, often there is no one instrument that completely captures a single target for
the outcome. Therefore, it is recommended that elements within instruments be
considered. In addition, the varying stakeholders are interested in knowing different
outcomes, yet these outcomes may be conceptually related and cross the
client/community, program, and system levels. The focus should be placed on domains or
core components that are to be monitored, within which several measures/indicators may
be identified. This allows for consistency of outcome measures while affording relevancy
to the multiple perspectives and flexibility for the programs who are tasked with gathering
the data.

Section VI: Evaluation and Accountability page 16
EENNDDNNOOTTEESS 1 Stakeholder Consultations, conducted October – December 2001 with individuals involved with
target population in select Alberta communities.
2 Canadian Council on Health Services Accreditation. (2002). AIM: Achieving Improved Measurement: Accreditation Program (2nd ed). Standards for Mental Health.
3 Goering, P. (1997). Review of Best Practices in Mental Health Reform. Prepared for Advisory Network on Mental Health by Health Systems Research Unit, Clarke Institute of Psychiatry. Publications: Health Canada. McEwan, K & Goldner, E.M. (2001). Accountability and Performance Indicators for Mental HealthServices and Supports – A Resource Kit (Prepared for the Federal/Provincial/Territorial AdvisoryNetwork on Mental Health). Health Canada.
4 A three-year evaluation is being conducted on the Calgary Diversion Project. Results from theevaluation—processes, outcomes, assessment tools—will help inform the Provincial Diversion Program.
5 Goering, P. (1997). Review of Best Practices in Mental Health Reform. Prepared for Advisory Network on Mental Health by Health Systems Research Unit, Clarke Institute of Psychiatry. Publications: Health Canada.
6 Goering, P. (1997). Review of Best Practices in Mental Health Reform. Prepared for Advisory Network on Mental Health by Health Systems Research Unit, Clarke Institute of Psychiatry. Publications: Health Canada, p. 136.
7 CDC (1999) Framework for Program Evaluation in Public Health. Accessed on November 27, 2002 at www.cdc.gov/epo/mmwr/preview/mmwrhtml/rr4811a1,htm
8 CDC (1999) Framework for Program Evaluation in Public Health. Accessed on November 27, 2002 at www.cdc.gov/epo/mmwr/preview/mmwrhtml/rr4811a1,htm, p 9.
9 CDC (1999) Framework for Program Evaluation in Public Health. Accessed on November 27, 2002 at www.cdc.gov/epo/mmwr/preview/mmwrhtml/rr4811a1,htm, p 11.
10 Kirkpatrick, S. (2001) The Program Logic Model: what, why and how? Accessed on November 04, 2002 at: http://www.charityvillage.com/charityvillage/research/rstrat3.html. Dwyer, J.J.M. & Makin, S. (1997). Using a Program Logic Model that Focuses on Performance Measurement to Develop a Program. Canadian Journal of Public Health, 88(6): 421-425. Millar, A., Simeone, R.S. & Carnevale, J.T. (2001). Logic models: a systems tool for performance management. Evaluation and Program Planning, 24: 73-81.
11 Simpson, L. & Gardner, L.. (2002). Health Innovation Fund Project #231: Calgary Diversion Project Annual Independent Evaluation Report. Submitted to Alberta Health and Wellness on October 17, 2002.
12 Taylor, J.A. & Hamilton Crowe, V.L. (1999) Rapid Cycle Change Sells Itself . JHQ Continuing Education Article. Accessed on December 03, 2002 at http://www.allenpress.com/jhq/082/082.htm
13 Taylor, J.A. & Hamilton Crowe, V.L. (1999) Rapid Cycle Change Sells Itself . JHQ Continuing Education Article. Accessed on December 03, 2002 at http://www.allenpress.com/jhq/082/082.htm
14 Martin, L.A. (2000). Effective Data Collection. Total Quality Management,11(3):341-344.
15 Health Canada. (2002). Vision and Strategy for Knowledge Management and IM/IT for Health Canada.

AAPPPPEENNDDIICCEESS APPENDIX A: GLOSSARY OF TERMS APPENDIX B: SAMPLE PROTOCOLS APPENDIX C: KEY REFERENCES

Appendices for Phase One page i
APPENDIX A: Glossary of Terms
TERMS
DEFINITIONS
BIOPSYCHOSOCIAL APPROACH
A bio psychosocial approach is best viewed as the most holistic approach to provide care, support and treatment. It not only focuses on an individual’s medical or “biological” state, but also on the psychological and social factors or conditions that exist for the person.
COMMUNITY CAPACITY BUILDING
About building partnerships, helping communities to help themselves, and integrating social, economic and human development.. It is about developing the capacity of communities to respond to their own challenges and opportunities. (Community Capacity Building Workshop: Facilitator’s Guide)
COMMUNITY GEOGRAPHIC TEAMS
Dedicated resources that have been developed in partnership with the core forensic psychiatry services situated in Edmonton and Calgary, regional health authorities, existing community mental health clinics, and provincial programs. These resources will include direct and indirect services in other regional centres and rural areas for those individuals who have difficulty accessing assessment and treatment due to distance, transportation, and lack of forensic psychiatry expertise. Telemental Health Services form an important component of this service.
COMMUNITY TENURE
Based on the individual’s ability to spend his/her time in a meaningful, and hopefully gainful way, inclusive of, but not restricted to, the following specifics:
Improved functioning as demonstrated by greater independence in several life areas such as medication compliance, daily living activities, housing, financial stability, etc. Reduction of number of incidents resulting in criminal
justice involvement and number of days in incarceration Reduction of number of days in hospitalization due to
mental illness Increased quality of life
DIVERSION COMMUNITY
A diversion community is based on boundaries determined by criminal justice processes and resources allocated for the provision of care, support and treatment of individuals with mental illness. In rural areas, the diversion community may encompass several small towns that use one hospital even though they may have several RCMP detachments.
ETHNOCULTURAL
“a group of people who share a common, distinctive ethnicity, heritage, culture, language, social patterns, and sense of belonging” (Source: Niels Aggr-Gupta, Alberta Community Development. Terminologies of Diversity 1997: A Dictionary of Terms for Individuals, Organizations and Professionals)

Appendices for Phase One page ii
FRAME OF REFERENCE An individual’s or organization’s perceptions, views, beliefs, attitudes,
understanding, expectations as they relate to a situation, another group of individuals. Each organization has a different history, mandate, role and organizational culture; therefore, individuals representing each organization will project the organization’s attitude in response to a situation. Additionally, individuals within an organization have differing frames of reference based on their collections of past experiences, values, beliefs and expectations.
OUTCOME MEASURES "Results of service/processes and/or end points of care that are linked to goals associated with: clients, programs/services, organizational performance, mental health system" (Alberta Mental Health Board’s Performance Indicator Committee, Sept. 2001)
PERFORMANCE INDICATORS
"What you want to measure. It is a flag, piece of information you want to know about. It is usually expressed in a quantitative manner. It is used to monitor and/or compare performance/service over a period of time" (Alberta Mental Health Board’s Performance Indicator Committee, Sept 2001).
PROGRAM (DIVERSION PROGRAM)
In the context of this implementation plan, “Program” is defined as consisting of agreed upon values, protocols, processes, and standards of operation that are used within the provincial context and across ministries in the diversion of individuals with mental illness who are in conflict with the law.
SOCIAL AND SUPPORT SERVICES
Social and other support services refer to the broad spectrum of services that have a direct bearing or interest on the quality of life of the mentally ill. It speaks to income and housing support, but also the other services such as transportation, education, supportive and spiritual counselling and general support.
TELEMENTAL HEALTH SERVICES
The use of audio-video conferencing technology for the delivery of mental health services such as assessment, treatment, consultation, conferencing, education and training. It is an established and efficient option in situation where geographical distances preclude the delivery of necessary and timely services. Depending on location, these services may usually be found within the local hospital or local community mental health clinic.
Appendices for Phase One page iii
APPENDIX B: Sample Protocols **Reprinted with permission of the Calgary Diversion Project. (2002). The above process has been presented as a sample; it is subject to modification by the Calgary Diversion Project.
CALGARY POLICE SERVICE ARREST PROCESSING UNIT/COURT UNIT PROCEDURES
ROLE OF THE CALGARY POLICE SERVICE
When it is determined that an individual located in the Arrest Processing Unit is suffering from a form of mental disorder, the following procedures will take place:
1. The Arrest Processing staff will inform the Calgary Diversion team that a person is in custody and of their need for assessment.
2. The Arrest Processing staff will process the individual as per normal procedures. 3. An assessment report will be forwarded to the Crown Prosecutor’s office where a decision will be made
regarding adjournment for 3 months for participation in the Calgary Diversion Project.
PROCESS
Arrest Processing Unit
1. The Staff Sergeant is responsible for making the decision to recommend a diversion assessment to the Calgary Diversion Project.
2. The recommendation for triage assessment decision is based on the information received from the arresting officer regarding the persons behavior before and upon arrest, the persons presentation while in the APU, and /or the concerns of the paramedic after screening.
3. When a person is brought into the APU he or she is assessed by a paramedic who is responsible for screening for physical and mental health problems as well as determining their level of risk.
4. When mental health concerns exist, the paramedic will alert the Staff Sergeant of these concerns. 5. If the person meets the criteria for the Calgary Diversion Project, the Staff Sergeant will ensure that a copy of
the booking sheet is stamped “RECOMMENDED FOR DIVERSION ASSESSMENT” and placed in the Diversion drawer.
6. The Staff Sergeant will ensure that the arrest report, and (Report to Prosecutor cover sheet) or (PTA) Promise To Appear (and Report to Prosecutor cover sheet) are stamped “RECOMMENDED FOR DIVERSION ASSESSMENT”, which will be the key indicator for the Crown Prosecutor to follow up on.
7. The Staff Sergeant will ensure that the Report to Prosecutor, synopsis section, also reflects that the individual has been recommended for the Diversion Assessment.
8. The Diversion staff will pick up the booking sheets from APU, every morning Monday-Friday. 9. The Staff Sergeant also has the option of contacting the Diversion staff directly to attend the APU for an
assessment during regular working hours (410-1132). 10. If the person is no longer within the APU, the contact location for the individual will be attached to the booking
sheet if known as well as their next court appearance date (disposition). 11. The Staff Sergeant will ensure that the individual is given a Calgary Diversion Project information card prior to
being released from Arrest Processing. Court Unit
1. Once the mental health triage assessment is completed by the Diversion staff, they will return this information along with a consent to disclose to the Court Unit supervisor. The Court Unit will retrieve from JOIN the information number, attach this to the file and forward the completed file to the Crown Prosecutor Screening team. In addition, the Court Unit will obtain from CPIC a CR2 for the past 18 months. This CR2 and the PCR (Patient Care Report) will be forwarded to the Diversion staff.
2. When an individual in the Diversion Program refuses to participate in the program, the Diversion staff will forward this information to the Court Unit who will add the JOIN information to the file, and then forward to the Crown Prosecutor’s Screening team.
Date Approved:_________24/02/03________________ Review Date:__________08/03_________________ P-1

Appendices for Phase One page iv
**Source: Calgary Diversion Project. Reprinted with permission of the Calgary Diversion Project. (February 2003). The above process has been presented as a sample; it is subject to modification by the Calgary Diversion Project.
CROWN COUNSEL
Protocol The Crown Prosecutor’s Office may refer individuals to the Calgary Diversion Project if the person appears to meet the criteria of the Project.
Procedure
1. The top portion of the (blue) Calgary Diversion Project Form will be completed. (see attached) 2. The Crown Prosecutor will sign this document and forward it to the Pre-Trial Unit Supervisor, who
will forward it to the Police Court Unit Supervisor.
3. The Crown Prosecutor will request an adjournment for 2 weeks.
4. The accused or counsel will be given contact information for the Calgary Diversion Project, where a triage assessment is usually completed in 72 hours following receipt of the referral.
5. Assessment Report will be forwarded to the Police Court Unit Supervisor who will forward it on to
the Pre-Trial Unit Supervisor at the Crown Prosecutor’s office.
6. The Crown Prosecutor will return to Court with the Assessment Report and either: - Prosecute the charge(s), if candidate unsuitable for program OR - Request further adjournment for referral to the Calgary Diversion Project for three months
when the situation will be reevaluated in Court.
7. At the end of 3 months the Calgary Diversion Project Summary Report, which will include linkages made, participation of client and progress made, will be forwarded to the Crown Prosecutor’s office to decide whether to withdraw the charge.
Date Approved:_____24/02/03____________________ Review Date:______08/03_____________________ P-2

Appendices for Phase One page v
APPENDIX C: Key References* Notation: The references provided in this list reflect only those documents that represent the key materials to support development of Phase One. A comprehensive review of diversion literature has been conducted and will help inform future phases of the Provincial Diversion Program development. A Community’s Commitment to Empowering Families and Children Through a Network of
Support: The Wraparound Process of the Oaklawn Psychiatric Centre, Elkhart, Indiana. (2002). Psychiatric Services, 53 (10): 1308-1310.
Alberta Children and Youth Initiative. (October 23, 2002). Information Sharing: Policy
Framework. (Draft). Alberta Community Development. (2000). Moving Forward… Homelessness Policy
Framework: Implementation Strategy. Alberta Community Development. (2000). A Housing Policy Framework for Alberta: Family
and Special Purpose Housing. Alberta Government. (2000). Strengthening Relationships: The Government of Alberta’s
Aboriginal Policy Framework. Altschuler, D.M. & Armstrong, T.L. (1994). Intensive Aftercare for High-Risk Juveniles: A
Community Care Model. Office of Juvenile Justice and Delinquency Prevention: Anderson, C.E. (2000). An Insider’s Perspective of Managed Mental Health Care. Care
Management Journals, 2(2): 93-100. Appelbaum, K. L., Hickey, J.M.& Packer, I. (2001). The Role of Correctional Officers in
Multidisciplinary Mental Health Care in Prisons. Psychiatric Services, 52(10): 1343-1347.
Baker, J.G. (1998). A Performance Indicator Spreadsheet for Physicians in Community
Mental Health Centres. Psychiatric Services, 49 (10): 1293-1298. Birmingham, L. (2001). Diversion From Custody. Advances in Psychiatric Treatment, 7:
198-207. Blankertz, L. & Cook, J.A. (1998). Choosing and Using Outcome Measures. Psychiatric
Rehabilitation Journal, 22 (2): 167-174. Borum, R. (1999). Jail Diversion Strategies for Misdemeanor Offenders with Mental
Illness: Preliminary Report. Department of Mental Health Law & Policy, Louis de la Parte Florida Mental health Institute, University of South Florida, Tampa, Florida.
Brekke, J.S., Prindle, C., Woo Bae, S. & Long, J.D. (2001). Risks for Individuals With
Schizophrenia Who Are Living in the Community. Psychiatric Services, 52 (10): 1358-1366.

Appendices for Phase One page vi
British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S Mental Health Reform Best Practices: Psychosocial Rehabilitation and Recovery.
British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S
Mental Health Reform Best Practices: Crisis Response/Emergency Services. British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S
Mental Health Reform Best Practices: Family Support and Involvement. British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S
Mental Health Reform Best Practices: Housing. British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S
Mental Health Reform Best Practices: Assertive Community Treatment. British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S
Mental Health Reform Best Practices: Inpatient/Outpatient Services. British Columbia Ministry of Health and Ministry Responsible for Seniors. (2001). B.C.’S
Mental Health Reform Best Practices: Consumer Involvement and Initiatives. Canadian Council on Health Services Accreditation. (2002). AIM: Achieving Improved
Measurement: Accreditation Program (2nd ed). Standards for Mental Health. Carter, M.F., Crosby, C., Geerthuis, S. & Startup, M. (1995). A Client-Centred
Assessment Of Needs Assessment. Journal of Mental Health, 4: 383-394. Cayce, J.D. & Burrell, K. (1999) King County’s Mental Health Court: An Innovative
Approach for Coordinating Justice Services. Accessed on May 3, 2001 at: http://www.wsba.org/barnews/1999/06/mentalhealth.html.
Challis, D., Von Abendorff, R., Brown, P., Chesterman, J. & Hughes, J. (2002). Care
Management, Dementia Care and Specialist Mental Health Services: An Evaluation. International Journal of Geriatric Psychiatry, 17: 315-325.
Clarkson, P. & Challis, D. (2002). Developing Performance Indicators for Mental Health
Care. Journal of Mental Health, 11(3): 281-293. Clearing House Health Outcomes. Exploring the Outcomes of Severe Mental Illness.
Accessed on July 23, 2001 at http://www.leeds.ac.uk/nuffield/infoservice/UKCH/smi.html.
Cohen, A. & Eastman, N. (2000). Needs Assessment For Mentally Disordered Offenders:
Measurement Of ‘Ability To Benefit’ And Outcome. British Journal of Psychiatry, 177: 493-498.
Community Building Resources. (1997). Listen and Learn…The Answers are with
Communities. Accessed on November 14, 2002 at: http://www.cbr-aimhigh.com/research_evaluation/Listen_Learn_1.htm

Appendices for Phase One page vii
Community Information Toronto. (2002). Information and Referral for the Homeless: The Street Helpline (powerpoint presentation).
Cornwall, P.L., Gorman, B., Carlisle, J & Pope, M. (2001). Ten Years in The Life Of a
Community Mental Health Team: The Impact of the Care Programme Approach in the UK. Journal of Mental Health, 10 (4): 441-447.
Council of State Governments (2002). Criminal Justice / Mental Health Consensus
Report. (grants awarded by Office of Justice Programs, U.S. Department of Justice; Center for Mental Health Services, Substance Abuses and Mental Health Services Administration, U.S. Department of Health and Human Services).
Cuffel, B.J., Held, M. & Goldman, W. (2002). Predictive Models and the Effectiveness of
Strategies for Improving Outpatient Follow-Up Under Managed Care. Psychiatric Services, 53 (11): 1438-1443.
Dausey, D.J., Rosenheck, R.A. & Lohman, A.F. (2002). Preadmission Care as a New
Mental Health Performance Indicator. Psychiatric Services, 53 (11): 1451-1455 Dolan, M. & Doyle, M. (2000). Violence Risk Prediction: Clinical and Actuarial Measures
and the Role of the Psychopathy Cheklist. British Journal of Psychiatry, 177: 303-311.
Draine, J., Salzer, M.S., Culhanes, D.P. & Hadley, T.R. (2002). Role of Social Disadvantages in Crime, Joblessness, and Homelessness Among Persons With Serious Mental Illness. Psychiatric Services, 3(5): 565-573.
Duffee, D., McDowall, D., Mazerolle, L.G. & Mastrofski, S.D. (2000). Measurement and
Analysis of Crime and Justice: An Introductory Essay. Criminal Justice. 4: 2-31 Dwyer, J.J.M. & Makin, S. (1997). Using a Program Logic Model that Focuses on
Performance Measurement to Develop a Program. Canadian Journal of Public Health, 88(6): 421-425.
Farabee, D. (2002). Reexamining Martinson’s Critique: A Cautionary Note for Evaluators.
Crime & Delinquency, 48 (1): 189-192. Feldman, R. & Roskes, E. (1999). A Collaborative Community-Based Treatment Program
for Offenders with Mental Illness. Psychiatric Services, 50(12): 1614-1619. Forchuk, C. et al. (2002). Mental Health Case Management in Canada: Job Description
Analyses. Issues in Mental Health Nursing, 23: 477-496. Ford, R. et al. (1997). Intensive Case Management for People With Serious Mental
Illness—Site 2: Clinical and Social Outcome. Journal of Mental Health, 6(2): 181-190.
Frank, F. & Smith, A. (1999). The Community Development Handbook: A Tool to Build
Community Capacity. Ottawa: Human Resources Development Canada (HRDC).

Appendices for Phase One page viii
GAINS Center. (2000). Creating Integrated Service Systems for People with Co-Occurring Disorders Diverted from the Criminal Justice System: The King County (Seattle) Experience. A Product of the SAMHSA Jail Diversion Knowledge Development and Application Initiative. Delmare, NY: Policy Research Associates, Inc.
Goering, P. (1997). Review of Best Practices in Mental Health Reform. Prepared for
Advisory Network on Mental Health by Health Systems Research Unit, Clarke Institute of Psychiatry. Publications: Health Canada.
Goering, P. (1997). Best Practices in Mental Health Reform: A Discussion Paper.
Prepared for Advisory Network on Mental Health by Health Systems Research Unit, Clarke Institute of Psychiatry. Publications: Health Canada.
Goldston, S.E. (1998). Cost Analysis and Primary Prevention: A Sound Idea Whose Time
Has Come. Journal of Mental Health, 7 (5): 505-518 Gorey, K.M., et al. (1998) Effectiveness of Case Management with Severely and
Persistently Mentally Ill People. Community Mental Health Journal, 34(3): 241-250. Green, G., et al. (2002). The Role and Impact of Social Relationships Upon Well-Being
Reported by Mental Health Service Users: A Qualitative Study. Journal of Mental Health, 11 (5): 565-579.
Griffin, P. A., Steadman, H.J. & Petrila, J. (2002). The Use of Criminal Charges and
Sanctions in Mental Health Courts. Psychiatric Services, 53 (10): 1285-1289.
Haimowitz, S. (2002) Can Mental Health Courts End the Criminalization of Persons With Mental Illness? Psychiatric Services, 53 (10): 1226-1228.
Harrell, A. et al. Evaluation Strategies for Human Services Programs – A Guide for
Policymakers and Providers. Washington, D.C.: The Urban Institute. Accessed on August 28, 2002 at: http://www.bja.evaluationwebsite.org/html/documents/evaluation_strategies.html
Hartwell, S.W. & Orr, K. (1999) The Massachusetts Forensic Transition Program for
Mentally Ill Offenders Re-Entering the Community. Psychiatric Services, 50 (9) Health Canada (1995). The Mentally Ill and the Criminal Justice System: Innovative
Community-Based Programs. Health Canada. (1995). Health and Enforcement in Partnership: How The Police, Justice,
Community Groups, and Health and Social Agencies are Working Together to Build Healthier, Safer Neighbourhoods. Accessed on August 09, 2001 at http://www.hc-sc.gc.ca/hecs-sesc/cds/publications/index.htm#public_research.
Health Canada. (1997) COLLABORATE! Health and Enforcement in Partnership: How to
Build Partnerships for Alcohol and Other Drug Projects. Accesses on September 10, 2002 at http://www.hc-sc.gc.ca/hecs-sesc/cds/publications/collaborate/toc.htm.

Appendices for Phase One page ix
Health Canada. Population Health Approach. What Determines Health? Accessed on November 28, 2002 at: http://www.hc.sc.gc.ca/hppb/phdd/determinants/e_determinants.html.
Health Canada. (1996). Guide to Project Evaluation: A Participatory Approach.
Population Health Directorate. Accessed on November 20, 2002 at: http://www.hc-sc.gc.ca/hppb/familyviolence/html/1project.htm.
Health Canada (2002). Summary Report of the Workshop on Best Practices for Concurrent Mental Health and Substance Abuse Disorders: February 21 and 22, 2002, Ottawa, Ontario.
Henggeler, S.W. et al. (1998). Multisystemic Treatment of Antisocial Behavior in Children
and Adolescents. New York: The Guildford Press. Huxley, P. (1998). Outcomes Management in Mental Health: A Brief Review. Journal of
Mental Health, 7 (3): 273-283 Juvenile Justice (2000). Youth With Mental Health Disorders: Issues and Emerging
Responses. Accessed on June 19, 2002 at: http://www.ncjrs.org/html/ojjdp/jjnl_2000_4/wrap_3.html
Kennedy, H. (2001). Risk Assessment Is Inseparable From Risk Management (Comment)
Psychiatric Bulletin, 25: 208-211.
Kirkpatrick, S. (2001). The Program Logic Model: what, why and how? Accessed on November 27, 2002 at: http://www.charityvillage.com/charityvillage/research/rstrat3.html.
Kuno, E., Rothbard, A.B., & Sands, R.G. (1999). Service Components of Case
Management Which Reduce Inpatient Care Use for Persons with Serious Mental Illness. Community Mental Health Journal, 35(2): 153-167.
Lamb, H.R., Weinberger, L.E. & Gross, B.H. (1999). Community Treatment of Severely
Mentally Ill Offenders Under the Jurisdiction of the Criminal Justice System: A Review. Psychiatric Services, 50 (7): 907-913.
Lamb, H.R., Weinberger, L.E. & DeCuir, W.J. (2002). The Police and Mental Health.
Psychiatric Services, 53: 1266-1271. Latimer, E.A. Economics of Assertive Community Treatment: A Review of the Literature
Accessed on January 3, 2002 at: http://www.cpa-apc.org/subscriptions/Archives/1999/June/latimer.htm
Lovell, D., Gagliardi, G.J. & Peterson, P.D. (2002). Recidivism and Use of Services
Among Persons with Mental Illness After Release From Prison. Psychiatric Services, 53 (10): 1290-1296.
Mandler, A., Gomes, A., & Castle, D. (2002). The Management of Change in Community
Mental Health Team. Australian Health Review, 25(2): 115-121.

Appendices for Phase One page x
Marty, D., Rapp, C.A. & Carlson, L. (2001). The Experts Speak: The Critical Ingredients of
Strengths Model Case Management. Psychiatric Rehabilitation Journal. 24(3): 214-221.
Martin, L.A. (2000). Effective Data Collection. Total Quality Management,11(3):341-344. Maxfield, M.G. (2001). Guide to Frugal Evaluation for Criminal Justice. US Department of
Justice. McGlynn, E.A. (1996). Setting the Context for Measuring Patient Outcomes. New
Directions for Mental Health Services, 71:19-32 McEwan, K & Goldner, E.M. (2001). Accountability and Performance Indicators for Mental
Health Services and Supports – A Resource Kit (Prepared for the Federal/Provincial/Territorial Advisory Network on Mental Health). Health Canada.
Millar, A., Simeone, R.S. & Carnevale, J.T. (2001) Logic Models: A Systems Tool for
Performance Management. Evaluation and Program Planning, 24: 73-81. Minkoff, K. & Ajilore, C. (1998). Co-Occurring Psychiatric and Substance Disorders in
Managed Care Systems: Standards of Care, Practice Guidelines, Workforce Competencies, and Training Curricula. Report of The Center for Mental Health Services Managed Care Initiative.
Monahan, J. et al. (2001) Mandated Community Treatment: Beyond Outpatient
Commitment. Psychiatric Services, 52 (9): 1198-1205. Mullen, P. E. (2000) Forensic Mental Health, British Journal of Psychiatry, 174: 307-311. NTAC’S Newsletter “networks” (1998) Building Bridges Between Mental Health and
Criminal Justice: Strategies for Community Partnerships. Accessed on October 10, 2002 at: http://www.nasmhpd.org/ntac/networks/spg98merg.html.
Ontario's Human Services and Justice Coordination Project (1996). A Provincial Strategy
to Coordinate Human Services and Criminal Justice Systems in Ontario. Ontario Ministry of Attorney General, Ministry of Community and Social Services, Ministry of Health, Ministry of the Solicitor and Correctional Service.
Peck, E. & Norman, I.J. (1999). Working Together in Adult Community Mental Health
Services: Exploring Inter-Professional Role Relations. Journal of Mental Health, 8 (3): 231-242.
Presser, L. & Van Voorhis, P. (2002) Values and Evaluation: Assessing Processes and
Outcomes of Restorative Justice Programs. Crime and Delinquency, 48 (1): 162-188.
Regional Policy for Personal Directives - Approving Authority: Executive Management and
Medical Advisory Board – Classification: Patient Rights, Privacy and Protection – accessed on: October 24, 2002 at: http://www.calgaryhealthregion.ca/polpublic/ShowPolicy?policy_id=1407.

Appendices for Phase One page xi
Robertson, A., Grimes, P. & Rogers, K.E. (2001). A Short-Run Cost-Benefit Analysis of Community-Based Interventions for Juvenile Offenders. Crime and Delinquency,47 (2): 265-285.
Roskes, E. & Feldman, R. (1999). A Collaborative Community-Based Treatment Program
for Offenders With Mental Illness. Psychiatric Services, 50 (12): 1614-1619. Seide, M. (1999). Letter: A Jail Diversion Program. Psychiatric Services, 50(2): 269-270.
Serin. R. (2001) Treatability, Treatment Responsivity and Risk Management. In Douglas. K.S. et al. (Ed) HCR-20 Violence Risk Management Companion Guide
(p. 113). British Columbia: Mental Health, Law, and Policy Institute, Simon Fraser University.
Shepherd, G. (1998) Models of Community Care. Journal of Mental Health 7(2): 165-177 Sorensen, J.E. (nd) Client Outcomes and Costs in Frontier Mental Health Organizations.
Accessed on October 4, 2001 at http://www.wiche.edu/MentalHealth/Frontier/Letter13/letter13.html
Steadman, H.J. Cocozza, J.J. & Veysey, B. (1999). Comparing Outcomes for Diverted
and Nondiverted Jail Detainees with Mental Illnesses. Law and Human Behaviour, 23(6): 615-627.
Stuart, H.L. & Arboleda-Flórez, J. (2000) Homeless Shelter Users in the
Postdeinstitutionalization Era. Canadian Journal of Psychiatry, 45: 55-62. Substance Abuse and Mental Health Services Administration (2001). Integrated Services
Reduce Recidivism Among Homeless Adult with Serious Mental Illness in California.
Tait, L., Birchwood, M. & Trower, P. (2002). A New Scale (SES) to Measure Engagement
with Community Mental Health Services. Journal of Mental Health, 11 (2): 191-198.
Taylor, J.A., Crowe, V.L.H. (1999). Rapid Cycle Change Sells Itself. Journal of Health
Care Quality. Accessed on December 03, 2002 at http://www.allenpress.com/jhq/082/082.htm .
Trauer, T. & Sacks, T. (1998) Medication Compliance: A Comparison of the Views of
Severely Mentally Ill Clients in The Community. Their Doctors and Their Case Managers. Journal of Mental Health, 7 (6): 621-629.
Taylor, J.A. & Hamilton Crowe, V.L. (1999) Rapid Cycle Change Sells Itself (JHQ
Continuing Education Article) Accessed on December 03, 2002 at http://www.allenpress.com/jhq/082/082.htm.
Teplin, L.A. (2000). Keeping the Peace: Police Discretion and Mentally Ill Persons.

Appendices for Phase One page xii
Weissberg, R.P. & Greenberg, M.T. (1998). Prevention Science and Collaborative Community Action Research: Combining the Best From Both Perspectives. Journal of Mental Health, 7(5), p. 479-492.
Wraparound’s Future – Wraparound Milwaukee: Aiding Youth With Mental Health Needs.
(2000). Juvenile Justice – Youth With Mental Health Disorders: Issues and Emerging Responses, VII (1) Accessed on June 19, 2002 at: http://www.ncjrs.org/html/ojjdp/jjnl_2000_4/wrap_5.html.
Ziguras, S.J. & Stuart, G.W. (2000). A Meta-Analysis of the Effectiveness of Mental Health
Case Management Over 20 Years. Psychiatric Services, 51(11): 1410-1421.