ahmed group lecture 25 hyperthermia. ahmed group lecture 25 delivery modalities cellular response to...
TRANSCRIPT

Ahmed GroupAhmed GroupLecture 25Lecture 25
Lecture 25
Hyperthermia

Ahmed GroupAhmed GroupLecture 25Lecture 25
• Delivery modalities• Cellular response to heat• Heat shock proteins• Thermo-tolerance• Response of tumors and normal tissues to heat• Combination with radiation therapy

Ahmed GroupAhmed GroupLecture 25Lecture 25
The use of hyperthermia as a medical treatment:
- First case describing a patient with a breast tumor treated withhyperthermia is more than 5,000 years old;
- Heat was used in all cultures for almost any disease includingcancer;
- In 1866 a case was described where sarcoma disappeared afterprolonged infection with a high fever causing bacteria;
- 1898 – marked regression of carcinomas of the uterine cervixafter local hyperthermia;
- Use of hyperthermia alone or in combination with radiation has been attempted over the years
Ahmed GroupAhmed GroupLecture 25Lecture 25
The interest in hyperthermia at the present time is based on documented clinical evidence of tumor regression as well as a biologic rationale and encouraging results from laboratory experiments

Ahmed GroupAhmed GroupLecture 25Lecture 25
• Delivery modalities• Cellular response to heat• Heat shock proteins• Thermo-tolerance• Response of tumors and normal tissues to heat• Combination with radiation therapy
Ahmed GroupAhmed GroupLecture 25Lecture 25
Methods of Heating
1) shortwave diathermy2) radiofrequency-induced currents3) microwaves4) ultrasound

Ahmed GroupAhmed GroupLecture 25Lecture 25
Methods of HeatingLimitations
Heating by hot water baths
- simple in a Petri dish;- more problematic with transplanted tumor-the temperature would nto be the same as the skin
Ahmed GroupAhmed GroupLecture 25Lecture 25
Methods of HeatingLimitations
Heating by microwaves
- good localization at shallow depths;- at greater tumor depths, even with lowered frequency, thelocalization is much poorer and surface heating limitstherapy.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heating by ultrasound
Methods of Heating Limitations
- the presence of bone or air cavities causes distortions of theheating pattern;- good penetration and temperature can be achieved in softtissues, particularly with ultrasound in focused arrays.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Methods of Heating Limitations
One method that suffers from fewer problems is the use of implanted microwave or radiofrequency sources. Good temperature distributions can be achieved and maintained if radiofrequency-induced currents or microwaves are applied to an array of wires actually implanted in the tumor and surrounding tissues. The “wires” used are frequently radioactive sources, so that heat and radiation can be combined.

Ahmed GroupAhmed GroupLecture 25Lecture 25
• Delivery modalities• Cellular response to heat• Heat shock proteins• Thermo-tolerance• Response of tumors and normal tissues to heat• Combination with radiation therapy

Ahmed GroupAhmed GroupLecture 25Lecture 25
Cellular response to heat
Heat kills cellsin a predictableand repeatableway.
Ahmed GroupAhmed GroupLecture 25Lecture 25
Cellular response to heat
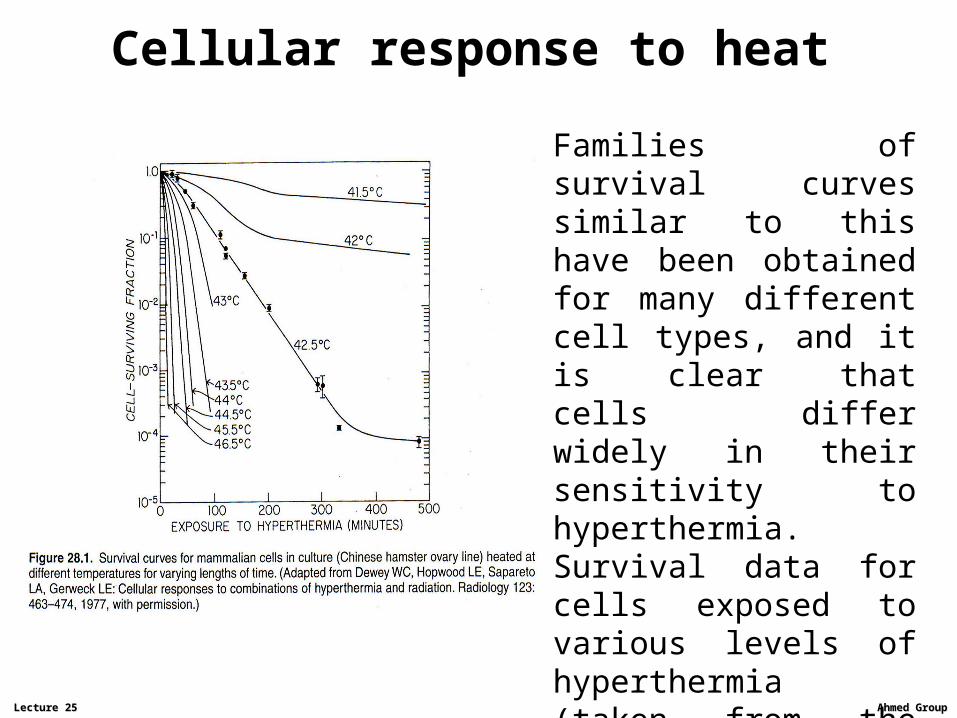
Families of survival curves similar to this have been obtained for many different cell types, and it is clear that cells differ widely in their sensitivity to hyperthermia. Survival data for cells exposed to various levels of hyperthermia (taken from the figure) are re-plotted on the next slide

Ahmed GroupAhmed GroupLecture 25Lecture 25
Cellular response to heatArrhenius plot

Ahmed GroupAhmed GroupLecture 25Lecture 25
Cellular response to heatArrhenius plot
The Arrhenius plot for a given cell line can be modified by a number of things. For example, altering the pH of the cells raises the curves, and the break point occurs at a higher temperature.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Cellular response to heat. Sensitivity to heat as a function of cell age in the mitotic cycle

Ahmed GroupAhmed GroupLecture 25Lecture 25
Cellular response to heatEffect of pH and nutrient deficiency on sensitivity to heat
- Cells at acid pH appear to be more sensitive to killing by heat;- Cells deficient in nutrients are certainly heat sensitive;
Conclusion: cells in tumors that are nutritionally deprived and at acid pH because of their location remote from a blood capillary may be particularly sensitive to heat. In addition, these cells are out of cycle and possibly hypoxic too. This correlates with the observation that large necrotic tumors shrink darmatically after a heat treatment.
Heat and X-rays appear to be complementary in their action.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Hypoxia and hyperthermia
The response of hypoxic cells constitutes a vital difference between X-rays and hyperthermia. Hypoxia protects cells from killing by X-rays.
By contrast, hypoxic cells are not more resistant than aerobic cells to hyperthermia;
Cells made acutely hypoxic and then treated with heat have a sensitivity similar to aerated cells;
Cells subject to chronic hypoxia show a slightly enhanced sensitivity to heat. This may be a consequence of the lowered pH and the nutritional deficiency as a result of prolonged hypoxia.

Ahmed GroupAhmed GroupLecture 25Lecture 25
• Delivery modalities• Cellular response to heat• Heat shock proteins• Thermo-tolerance• Response of tumors and normal tissues to heat• Combination with radiation therapy

Ahmed GroupAhmed GroupLecture 25Lecture 25
Mechanisms of action of hyperthermia
-Hyperthermia induces effects in both the nucleus and cytoplasm.Heat killing appears to be associated with degradation or denaturationof proteins. It is different from that for radiation killing, whichclearly involves primarily damage to DNA;-Although the intermediate steps may be different, the ultimatecytotoxic effect of both heat and radiation is at the DNA level;-In organized tissues heat damage occurs more rapidly than radiationdamage, because differentiated cells are killed as well as dividing cells;-The events associated with heat radiosensitization involve DNA damage and the inhibition of its repair. The role of heat is to blockthe repair of radiation-induced lesions.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat-shock proteins
If cells are exposed to heat, proteins of a defined molecularweight (mainly 70 or 90 kDa) are produced. The appearanceof these heat-shock proteins tends to coincide with thedevelopment of thermotolerance and their disappearancewith the decay of thermotolerance.Even though they have been given the name heat-shock proteins, they are produced after treatment with other agents, includingarsenic and ethanol.Heat-shock proteins are well conserved, they are found in cellsof many species.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat-shock proteinsHeat-shock proteins areidentified by gel electrophoresis,in which they show up as clearlydefined bands of specific MW.

Ahmed GroupAhmed GroupLecture 25Lecture 25

Ahmed GroupAhmed GroupLecture 25Lecture 25

Ahmed GroupAhmed GroupLecture 25Lecture 25
• Delivery modalities• Cellular response to heat• Heat shock proteins• Thermo-tolerance• Response of tumors and normal tissues to heat• Combination with radiation therapy

Ahmed GroupAhmed GroupLecture 25Lecture 25
Thermo-tolerance
The development of a transient and non-heritable resistance to subsequent heating by an initial heat treatment has been described variously as induced thermal resistance, thermal tolerance, or most commonly, thermo-tolerance

Ahmed GroupAhmed GroupLecture 25Lecture 25
Thermotolerance
Thermotolerance is a serious problem in the clinical use of hyperthermia. Figure on the left illustrates why by contrasting heat and radiation:-top graph-X-ray,-bottom graph- hyperthermia

Ahmed GroupAhmed GroupLecture 25Lecture 25
Thermal dose
Non-uniform temperature distribution in a tumor. It stems from two sources:
-power deposition, and-tumor blood perfusion, which carries the heat away.
The formal definition of thermal dose:
“the time in minutes for which the tissue would have to be held at 43°C to suffer the same biologic damage as produced by the actual temperature, which may vary with time during a long exposure”

Ahmed GroupAhmed GroupLecture 25Lecture 25
Thermal dose
Although the concept of thermal dose is attractive, there areproblems in its implementation:
- Nonuniformity of temperature occures throughout the tumor.
- The concept relates only to cell killing by heat and does not include radiosensitization
- It relates to one heat treatment, so it is not possible to add one treatment to the next given a few days later, because of the problem of thermotolerance.

Ahmed GroupAhmed GroupLecture 25Lecture 25
• Delivery modalities• Cellular response to heat• Heat shock proteins• Thermo-tolerance• Response of tumors and normal tissues to heat• Combination with radiation therapy

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and tumor vasculatureThe capacity of tumor blood flow to increase during heating appears to be limited in comparison with normal tissues. A postulated mechanism for the selective solid tumor heating is shown in Figure.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and tumor vasculatureHeat appears to preferentially damage the fragile vasculature of tumors; as a consequence, the heat-induced change in blood flow is different from that in normal tissues.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and tumor vasculature
The microcurculation of tumors after hypothermia. At the higher temperaturescompression, occlusion, hemorrhage, and stasis thrombosis were observed.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and tumor vasculature
There is a complex interplay in tumors between hyperthermia,blood flow, and cell killing; this is illustrated in Figure.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Hyperthermia and tumor oxygenation
In transplanted tumors in rodents heat causes vascular damage; however, in spontaneous human tumors the vasculature is considerably more resistant to thermal damage.
It now is recognized that mild hyperthermia actually can promote tumor re-oxygenation, with the degree of re-oxygenation correlating with the level of cytotoxicity.

Ahmed GroupAhmed GroupLecture 25Lecture 25
• Delivery modalities• Cellular response to heat• Heat shock proteins• Thermo-tolerance• Response of tumors and normal tissues to heat• Combination with radiation therapy

Ahmed GroupAhmed GroupLecture 25Lecture 25
The interaction between heat and radiation
Biologic effect of the combination of heat and radiation:
1. Additive cytotoxic effect. 2. Sensitization of the radiation cytotoxicity by heat.
Additive cytotoxic effect takes place in a practical situation in clinic-synergistic interaction of the two modalities.There are differences between different heat treatments-acute hyperthermia (45°C)-more modest level of hyperthermia (40-43°C).

Ahmed GroupAhmed GroupLecture 25Lecture 25
The interaction between heat and radiationIf heat and radiation are combined, an important considerationis sequencing. Picture on this slide shows sequencing in vitro.

Ahmed GroupAhmed GroupLecture 25Lecture 25
The interaction between heat and radiationComparable data for mouse skin are shown here.
There was a markedvariation in the normaltissue response after agiven dose of X-rays,depending on the timeinterval, and the order inwhich the two treatments were given

Ahmed GroupAhmed GroupLecture 25Lecture 25
Thermal enhancement ratio
In the case of either normal tissues or transplantable tumors in experimental animals, the extent of the interaction of heat and radiation is expressed in terms of the:
Thermal enhancement ratio (TER), defined as the ratio of doses of X-rays required to produce a given level of biological damage with and without the application of heat.
The TER has been measured for a variety of normal tissues, including skin, cartilage, and intestinal epithelium. The data form a consistent pattern of increasing TER with increasing temperature, up to a value of about 2 for 1-hour heat treatment at 43°.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and the therapeutic gain factor
The therapeutic gain factor can be defined as the ratio of theTER in the tumor to the TER in the normal tissues.There is no advantage to using heat plus lower doses of X-rays if there is no therapeutic gain compared with the useof higher doses of X-ray alone.The question of a therapeutic gain factor is complicated in the caseof heat because the tumor and normal tissues are not necessarilyat the same temperature.Generally speaking, there are good reasons to believe thatthe effects of heat, alone or in combination with X-rays,may be greater on tumors than on normal tissues.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and chemotherapeutic agents
The cell-killing potential of some but not allchemotherapeutic agents isenhanced substantially by a temperature elevation ofeven a few degrees.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and chemotherapeutic agents
Table below is a listing of drugs that are potentiated by heat and those that are not.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat and chemotherapeuticagents
There are severaldifferent mechanisms that may be involved,some of which are listed in the tablebelow.

Ahmed GroupAhmed GroupLecture 25Lecture 25
Hyperthermia and implantsGood results have been claimed for the combination of hyperthermia and high dose rate implants. The success is a result of the favorable physical distribution of both heat and radiation that are possible with implants rather than of any particular biologic advantage

Ahmed GroupAhmed GroupLecture 25Lecture 25
Heat plus radiation: current status ofclinicalstudiesHyperthermia hasbeen used extensivelyas an adjuvant to radiation in thetreatment of localand regional cancer

Ahmed GroupAhmed GroupLecture 25Lecture 25
Current position on hyperthermia
1. The biologic properties of hyperthermia make it an attractivemodality for the treatment of cancer
2. It is still difficult to achieve uniform heating of a volume deepwithin the body. The basic laws of physics make the desiredend difficult to achieve.
3. The clinical value of hyperthermia in the routine treatment ofcancer is still not clear, despite its proven efficiency in a fewspecific instances. Hyperthermia is most effective in situations that involve either combination with external-beam radiotherapy orwith brachytherapy.