aerobic exercise systematic review october 2007 - … · progressive resisted muscle strengthening...
TRANSCRIPT
A systematic review of the effectiveness of aerobic exercise interventions for children
with cerebral palsy
An AACPDM evidence report
Written by:
Anna Rogers MSc(PT)*. Barbara-Lynne Furler MSc(PT). Stephen Brinks MSc(PT).
Johanna Darrah PhD.
Approved by AACPDM Treatment Outcomes Committee Review Panel: American Academy for
Cerebral Palsy and Developmental Medicine Lisa Samson-Fang, MD Johanna Darrah, PhD John McLaughlin, MD Lynne Logan, MA, PT William Walker MD
Lesly Wiart, MScPT Meg Barry-Michaels PhD, PT, PCS Michael Msall MD Unni Narayanan MD
Laura Vogtle, PhD, PT Robbin Hickman PT MHS PCS Alexander Hoon, MD
Corresponding Author Anna Rogers 6227 109A St. Edmonton, AB T6H 3C6 Canada Tel: (780) 862-9244 Email:[email protected]
Aerobic Exercise Systematic Review 1
Abstract
The aim of this review was to assess the evidence regarding the effectiveness of aerobic training
interventions for children with cerebral palsy. The target population included children with
cerebral palsy of any severity, aged 2 to 17 years old. The following databases were searched for
English studies from 1960 to the present: MEDLINE, EMBASE, CINAHL, Pascal, Cochrane
Library, CSA Neuroscience Abstracts, PEDro and Sport Discus Search terms included cerebral
palsy, athetoid, ataxic, spastic diplegia, hemiplegia, quadriplegia, aerobic, exercise, training,
physical activity, aquatic/water/pool therapy, and continuous exercise. The American Academy
of Cerebral Palsy and Developmental Medicine (AACPDM) systematic review guidelines were
used to format the review. One thousand four hundred and eighty nine articles were identified
and examined for the stated inclusion and exclusion criteria. Thirteen articles met the criteria for
inclusion. The evidence suggests that aerobic exercise with children with cerebral palsy can
improve physiological outcomes, but the influence of these changes on outcomes representing
activity and participation in unknown. Future research needs improved methodological rigour in
order to determine a specific set of exercise guidelines and safety considerations.
Aerobic Exercise Systematic Review 2
The AACPDM has undertaken the development of systematic reviews to summarize the
literature about specific intervention strategies used to assist children with developmental
disabilities. These reviews are not best practice documents or practice guidelines, but rather they
gather and present the best evidence – for and against – the effectiveness of an intervention.
Their goal is to present the evidence about interventions in an organized fashion to identify gaps
in evidence and help address new research that is needed. The Academy is neither endorsing nor
disapproving of an intervention in these reviews. Every effort has been made to assure that
AACPDM systematic reviews are free from real or perceived bias. Details of the disclosure and
consensus process for AACPDM outcomes reports can be viewed at www.AACPDM.org.
Nevertheless, the data in an AACPDM Systematic Review can be interpreted differently,
depending on people's perspectives. Please consider the conclusions presented carefully.
Background
Therapeutic programs for adults and children with disabilities are increasingly
incorporating a fitness component into intervention strategies. The benefits of aerobic exercise
for persons with disabilities include increased cardiovascular capacity and endurance, weight
management and lower blood lipid levels, preservation of bone mass and overall maintenance of
function.2 In addition, the opportunity for persons with disabilities to participate in community
aerobic fitness programs allows them to take responsibility for their own health and fitness.
People with a physical disability have identified numerous barriers to participation in physical
activities including physical accessibility to exercise facilities, shortage of adapted exercise
equipment, inability to pay for a fitness membership and a lack of knowledge in the fitness and
exercise professions about how to appropriately design an exercise program for specific
Aerobic Exercise Systematic Review 3
disabilities.3 Health counseling about the importance of physical activity and its accessibility for
persons with disabilities is minimal.3
Historically, exercise programs that included aerobic or muscle strengthening
components were often contraindicated for persons with cerebral palsy because of the concern
that increased effort and exertion during exercise would result in increased muscle tone, a
decrease in range of motion, and/or an overall decrease in function.4 Concerns about the safety of
progressive resisted muscle strengthening for children with cerebral palsy have been negated by
recent studies that demonstrate no increase in spasticity and no loss of range of motion following
a resistance training program.4-6 While strength training is now recognized as an effective
intervention for improving muscle strength with children with cerebral palsy4, the efficacy of
aerobic exercise as a safe and beneficial intervention option for children with cerebral palsy has
not been reviewed in the literature. The purpose of this review is to review the evidence for the
effectiveness of aerobic exercise interventions for children with cerebral palsy.
Method
OPERATIONAL DEFINITION AND INCLUSION CRITERIA
Aerobic exercise was defined as any activity that increases heart rate or proposes to
increase heart rate to exact physiological change. The outcomes evaluated represented more than
just physiological measures such as 6 minute walk distance or gait efficiency. All outcomes
included in the studies were documented. Studies with a sample that included children aged 2 to
17 years with any severity of cerebral palsy diagnosis were eligible for inclusion. At least 50%
of subjects in the study sample had to have a diagnosis of cerebral palsy, or the results of the
subjects with cerebral palsy must be distinguishable from children with other diagnoses and
analyzed separately.
Aerobic Exercise Systematic Review 4
LITERATURE SEARCH
A medical librarian assisted with the search strategy. The following databases were
searched in English only from 1960 to 2006: CINAHL (297 studies), Cochrane Library (65),
CSA Neuroscience Abstracts (1), EMBASE (464), MEDLINE (372), Pascal (64), The
Physiotherapy Evidence Database (PEDro) (3), and Sport Discus (223). The search terms used
for the target population were: cerebral palsy, athetoid, ataxic, spastic diplegia, and quadriplegia.
The intervention search terms were: aerobic, exercise, training, physical activity,
aquatic/water/pool therapy, and continuous exercise. A specific pediatric search, ARCHE
(Alberta Research Centre Health Evidence), was also applied to the OVID search engines. The
initial search yielded 1489 articles; 1205 articles were excluded based on the inappropriateness
of their titles. The remaining 284 abstracts were read independently by two reviewers and
conflicts were resolved by a third reader if required. Two-hundred seventy-one articles were
excluded for one or more of the following reasons: 1) lack of aerobic exercise intervention, 2) no
reported aerobic fitness outcomes, 3) use of a one-time exercise protocol, 4) the population did
not match the inclusion criteria, or 5) review articles. Thirteen articles met the inclusion criteria.
ORGANIZATION OF EVIDENCE
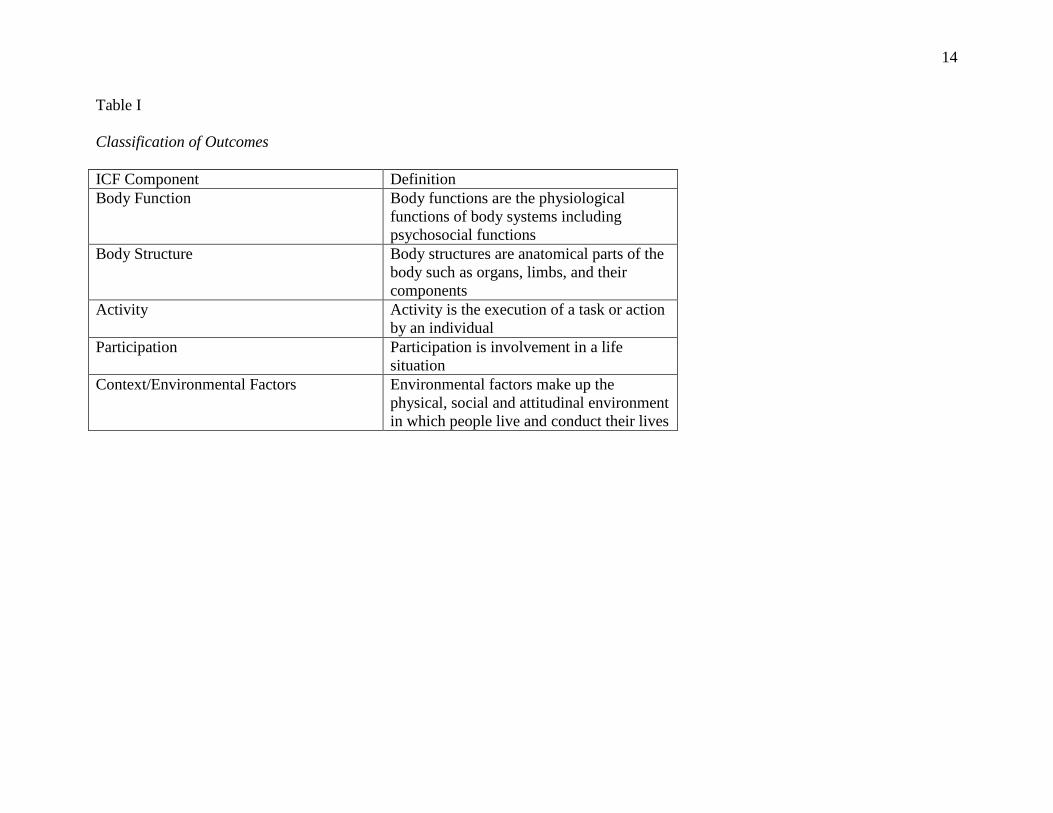
Outcome measures were classified according to the components of the International
Classification of Functioning, Disability and Health (ICF)7 as presented in Table I. Studies were
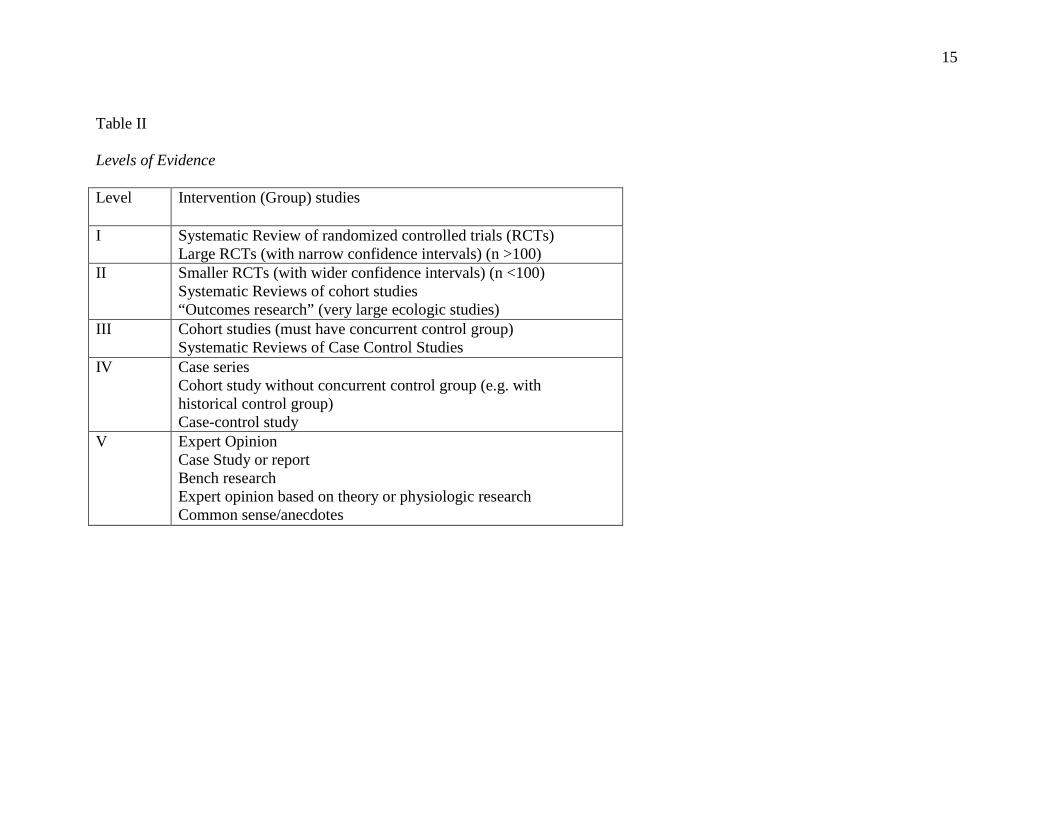
classified using a hierarchy of research design rigour (Table II). Level I studies produce results
from which definitive conclusions can be made. Level II thru level IV studies report
progressively less credible evidence from which only cautious conclusions can be drawn. No
definite conclusions can be made from level V evidence.
Aerobic Exercise Systematic Review 5
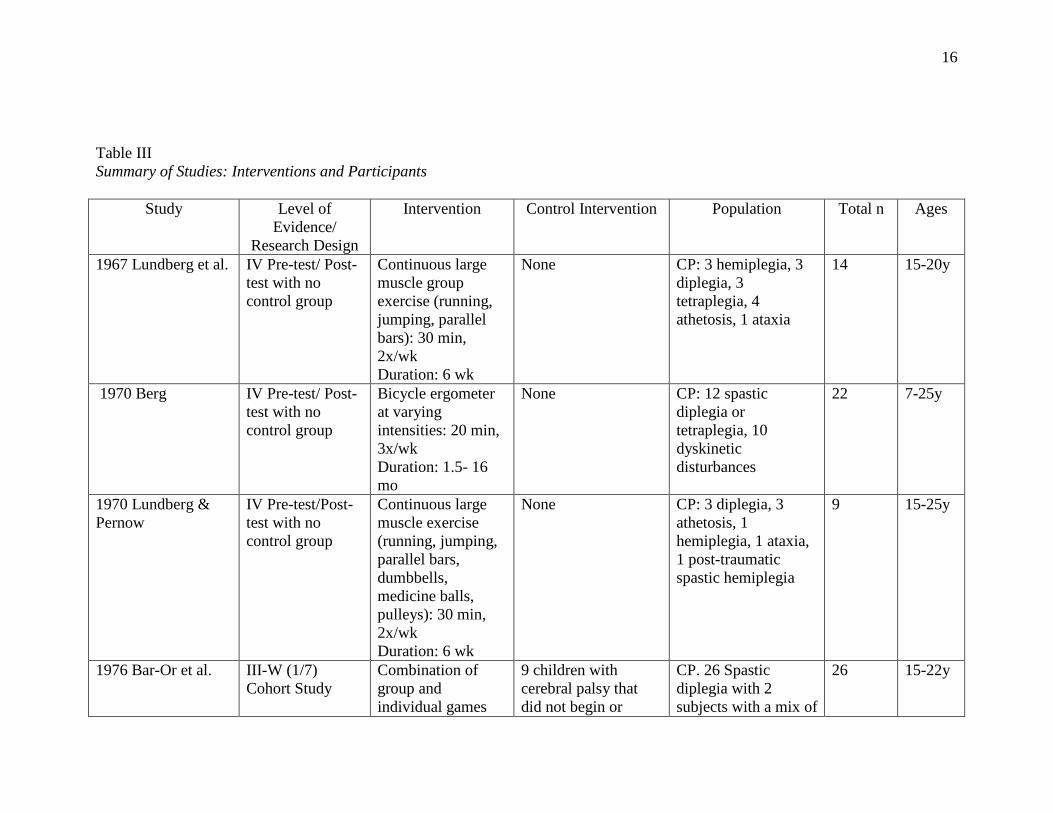
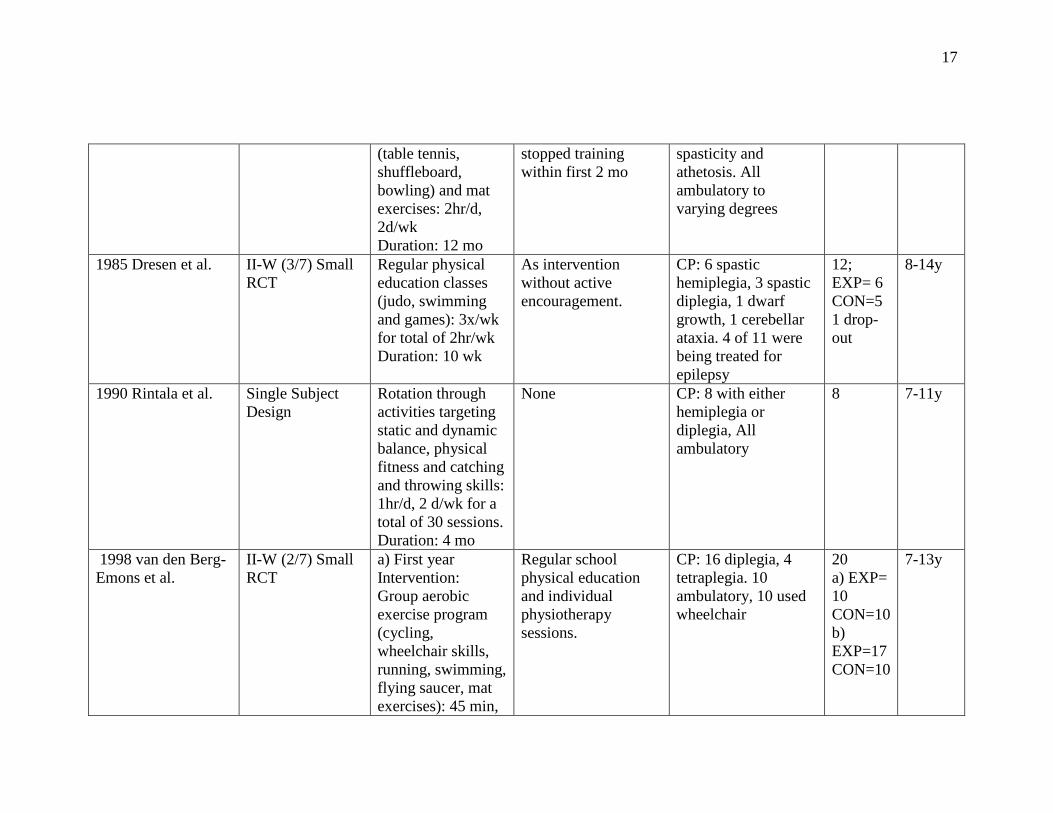
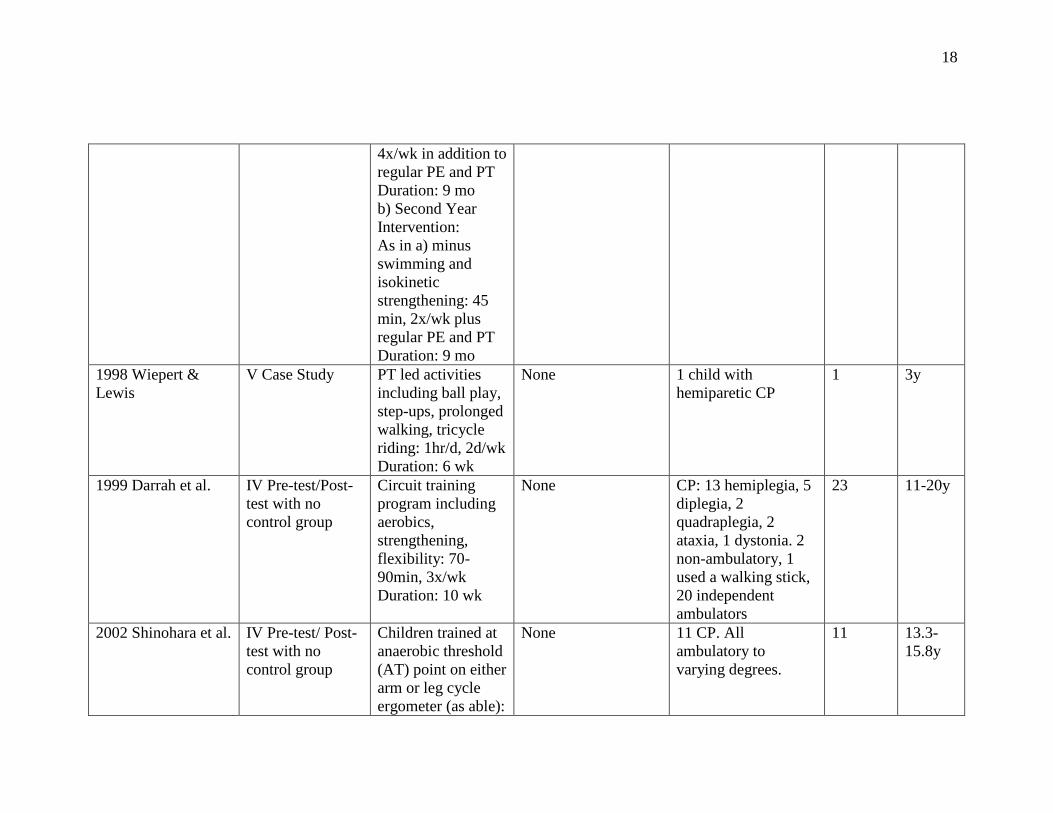
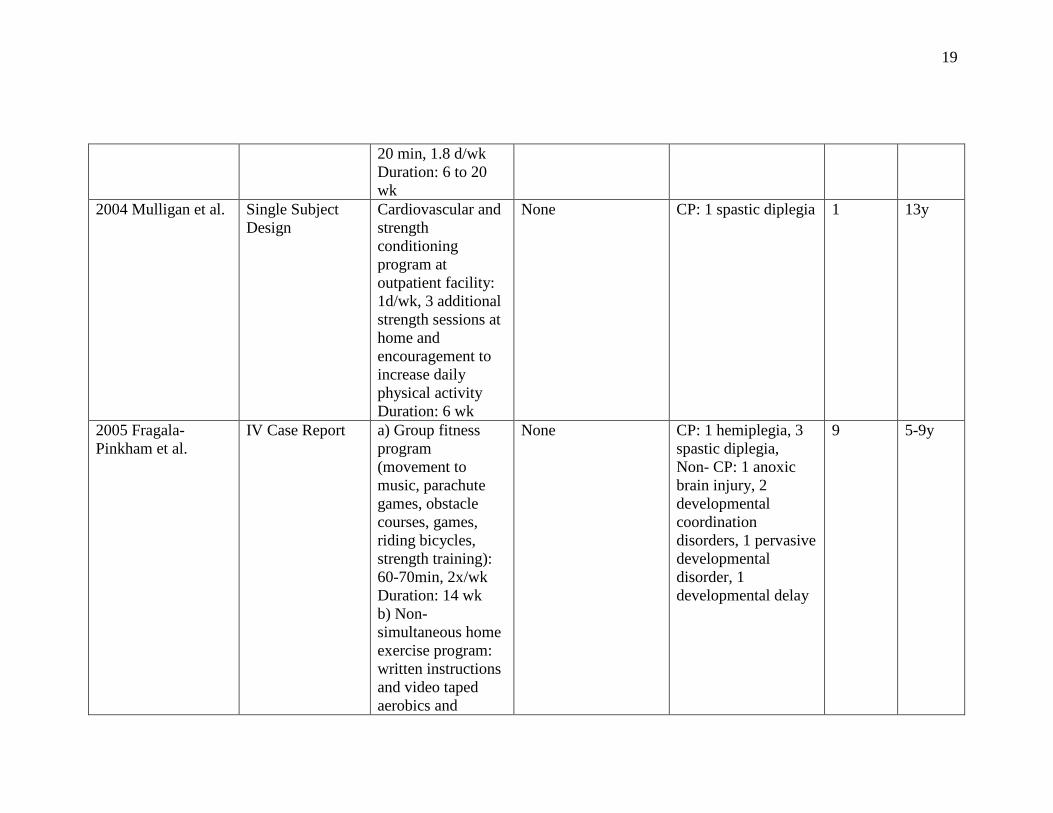
Table III summarizes the 13 studies reviewed. Two small, randomized controlled trials
had control groups that received the same intervention as the experimental group but at a reduced
frequency.8,9 One cohort study used the subjects that dropped out or did not begin training as the
control group.10 Five studies compared the results of a pre-test/post-test in a single group with no
control using a variety of aerobic exercise programs ranging from games to bicycle ergometry.11-
15 The remaining studies consisted of 2 case studies 16,17 and 3 single subject design studies.18-20
Tables IV and V include only evidence from the studies that received a level of evidence
rating of level III or higher. Level IV and V studies are not included in the final evidence tables
because of threats to internal validity due to weak study design. In addition, the level of evidence
of single subject design studies cannot be rated within the levels defined for group studies. Table
IV provides the conduct ratings of the studies rated as level III evidence and higher. The conduct
rating provides an assessment of the quality of the study based on the score from the seven
evaluative questions under Table IV. Each study was rated by two independent reviewers and a
third reader was available to resolve conflict and determine the final rating if necessary.
Table V summarizes the outcomes of interest, the measures used to quantify the
outcomes, the ICF components of health represented by the outcome measures used, and the
statistical results. No study reported power calculations and thus studies reporting a ‘not
reported’ (nr) or ‘not significant’ (ns) result may not have enough power to detect true
differences between groups.
Analysis and discussion of the evidence
1. WHAT EVIDENCE EXISTS ABOUT THE EFFECTS OF AEROBIC EXERCISE ON
MEASURES REPRESENTING THE COMPONENTS OF BODY FUNCTION AND
STRUCTURE?
Aerobic Exercise Systematic Review 6
All outcomes measured in the studies reported in Tables IV and V represent the
components of body structure and function. All three studies evaluated physiological variables
related to aerobic fitness, two reported body composition9,10 and one study measured grip
strength and mechanical efficiency10 but these two outcomes were not analyzed statistically.
Aerobic fitness.
Significant improvement in aerobic fitness following training was reported in all three
studies. Different outcome measures were used to determine change in aerobic fitness, including
heart rate (HR) during sub-maximal and maximal tests,10 VO2peak and VO2max9,10 and the
relationship between VO2 and workload and VO2 and heart rate.8
The level II study by van den Berg-Emons et al. demonstrated an improvement in aerobic
fitness following two, 9-month, “high intensity” training sessions 45 minutes in duration, four
times a week which involved cycling, wheelchair skills, running, swimming and mat exercises.9
In contrast, Dresen et al. (level II) showed a significant decrease in VO2/workload after a 10-
week training program that consisted of regular physical education activities (judo, swimming
and games) for a total of two hours per week.8 The only difference between the control and
experimental groups in this study was that the latter simply received undefined “active
encouragement” from the instructor. Van den Berg-Emons et al. found a significant increase in
peak aerobic power after training.9 This same increase was not observed following a two month
rest period, suggesting that although children with cerebral palsy are able to improve their level
of aerobic fitness, it may not be maintained over time if the exercise level is not maintained.
Body composition.
Both van den Berg-Emons et al.9 (level II) and Bar-Or et al.10 (level III) used the
measures of height, weight and skinfolds to report anthropometric variables. Bar-Or et al.10
Aerobic Exercise Systematic Review 7
reported significant change in the height variable, in both the control and exercise groups, while
van den Berg-Emons et al.9 measured fat mass (skinfolds) and showed a significant increase in
the control group.
2. WHAT EVIDENCE EXISTS ABOUT THE EFFECTS OF AEROBIC EXERCISE ON
MEASURES REPRESENTING THE COMPONENTS OF ACTIVITY AND
PARTICIPATION?
None of the studies in the evidence tables reported outcomes representing the ICF
components of activity and participation.
3. WHAT KINDS AND MAGNITUDE OF COMPLICATIONS HAVE BEEN
DOCUMENTED?
Safety concerns were not discussed in any articles, including studies categorized as Level
IV and V. There were no reports of increased spasticity, medical problems or the occurrence of
musculoskeletal trauma in any of the studies reviewed. Evaluation of adverse effects such as
fatigue was not reported.
4. WHAT IS THE STRENGTH OF THE EVIDENCE?
The results of the three level II-III studies all suggest that aerobic exercise intervention
can improve physiological outcomes in children with cerebral palsy. However, the total number
of subjects in the review is only 58, and the largest single sample was 26 participants.10 As
described in Table III, most samples were extremely variable both in the ages of the children and
their physical abilities. Given the small sample size, the heterogeneity of both the samples and
inventions and the poor conduct ratings received by the Level II and III studies (Table IV), it is
difficult to identify specific components of aerobic intervention that are most effective.
Aerobic Exercise Systematic Review 8
The age range of participants among the studies ranged from 7 to 22 years. The physical
abilities of the children within the same study ranged from mild to severe diplegia and
hemiplegia, and ability levels included ambulatory and non-ambulatory. This heterogeneity of
age and motor abilities makes it difficult to discern the extent to which each subject was able to
participate in an exercise program. Children with differing motor abilities and different ages may
respond differently to aerobic exercise intervention. The samples in the studies were all too
small to allow for subgroup analyses.
Most of the interventions are non-replicable because of lack of detail provided.
Intervention activities ranged from game activities in a physical education setting with “active
encouragement”8 to more specific aerobic exercise such as cycling, wheelchair skills and
running. There was no description as to whether the activity was continuous or non-continuous
or what equipment/intervention adaptations had to be made for the non-ambulatory participants.
Exercise parameters varied among the studies; intensity of exercise varied from inconsistent
monitoring of 160 beats per minute8 to subjective opinions based on investigators’ observations
during game play.10 Frequency varied from a total of 2-6 hours a week spread over a range of 2-
4 exercise sessions a week. Duration of the intervention programs varied from 10 weeks to 18
months.8,9 Standardized guidelines for frequency, duration, intensity and type of exercise
necessary to impose physiological change cannot be extracted from this body of literature.
The measures used in the level I to III studies focused on the outcomes of body structure
and function. All three studies used oxygen consumption (VO2), heart rate (HR) or the
relationship between VO2 and HR to detect change in aerobic fitness, but these measures were
not standard across or even within these studies. For example, Bar-Or et al.10 used both a sub-
maximal and a maximal VO2 test, whereas Dresen et al.8 used only sub-maximal VO2 testing.
Aerobic Exercise Systematic Review 9
Although both groups of authors reported an improvement in oxygen consumption, they are
reporting different outcomes (VO2max vs. sub-maximal VO2 to workload ratios) and therefore do
not allow for the discussion of a trend across studies. No studies evaluated the relationship
between improvement of aerobic fitness at a physiological level and improvement of outcomes
representing the ICF components of activity and participation. Therapists are interested in
optimizing the functional abilities of children with cerebral palsy and future studies need to
systematically evaluate the relationship of outcomes representing components of body function
and structure and activity and participation. For example, does an increase in VO2max result in
improved walking endurance or mobility in school?
Summary and directions for future research.
The limited evidence available suggests that children with cerebral palsy who participate
in an aerobic exercise training program demonstrate improvements in physiological measures of
aerobic fitness. However the body of research has methodological limitations and is based on a
small sample size.
The current emphasis on functional goals and community exercise opportunities for
children with cerebral palsy may have moved research about the effects of aerobic exercise too
rapidly from controlled laboratory settings to community exercise programs. The paucity of
controlled laboratory research suggests that more information is needed from laboratory settings
to establish the efficacy of aerobic exercise models using exercise regimes with different
intensity, frequency and duration parameters. When these parameters are better established and
understood, then the effectiveness of the programs in community setting could be systematically
evaluated. However, because of the interest in community fitness programs for children with
cerebral palsy, it is doubtful that the community programs will wait until the efficacy
Aerobic Exercise Systematic Review 10
information from laboratory settings is available. If the research in the two different settings
continues to develop simultaneously, it would be valuable to collect similar information from
both settings for comparison. By using the same cadre of measures representing all components
of the ICF in both controlled laboratory condition and community settings, future research
endeavors can begin to systematically evaluate the relationships across the ICF components.
Although the study designs of levels IV and V evidence inherently limit the confidence
that can be placed in these results, it is interesting to note that measures that target outcomes
within the ICF components of activity and participation were used in some of these studies.
Several studies reported an improvement in gait efficiency 16,17 and in the distance walked during
a 6-minute walk test 19. A few authors reported improvement in psychological variables such as
self-perception of physical appearance 11, athletic competence and self-worth using either the
Self Perception Profile for Adolescents (SPPA) or College students (SPPC).12,20 These types of
outcomes need to be incorporated in studies of more rigorous research design. No complications
or safety concerns were reported in any of the Level IV and V studies.
The finding that children with cerebral palsy are able to train to elicit physiological
change is a positive outcome that should serve as a catalyst for future well-designed studies to
establish safe, effective, and specific exercise guidelines for children of different ages and ability
levels.
Acknowledgements: Dr. Darrah was funded as a CIHR New Investigator during the preparation
of this review. Michelle Kelly MScPT reviewed the manuscript and provided valuable
suggestions.
11
References
1. O’Donnell M, Darrah J, Adams R, Butler C, Roxborough L, & Damiano D. (2004)
AACPDM methodology to develop systematic reviews of treatment interventions.
http://www.aacpdm.org/resources/systematicReviewsMethodology.pdf (accessed
November 2005).
2. Rimmer JH. (2005) Exercise and physical activity in persons aging with a disability. Phys
Med Rehabil in North America 16: 41-56.
3. Rimmer, JH, Riley B, Wang E, Rauworth A, & Jurkowski J. (2004) Physical activity
participation among persons with disabilities: barriers and facilitators. Am J Prev Med
26(5): 419-425.
4. Dodd KJ, Taylor NF, & Damiano DL. (2002) A systematic review of the effectiveness of
strength-training programs for people with cerebral palsy. Arch Phys Med Rehabil 83(8):
1157-1164.
5. MacPhail HE, & Kramer JF. (1995) Effect of isokinetic strength-training on functional
ability and walking efficiency in adolescents with cerebral palsy. Dev Med Child Neurol
37: 763-775.
6. Tweedy, S. (1995) Strength training for athletes with cerebral palsy. Ultra-Fit Australia,
26: 66-70.
7. World Health Organization. (2001) International Classification of Functioning,
Disability and Health. Geneva: World Health Organization.
8. Dresen MH, de Groot G, Mesa Menor JR, & Bouman, LN (1985) Aerobic energy
expenditure of handicapped children after training. Arch Phys Med Rehabil 66(5): 302-
306.
12
9. Van den Berg-Emons RJ, Van Baak MA, Speth L, & Saris WH. (1998) Physical training
of school children with spastic cerebral palsy: effects on daily activity, fat mass and
fitness. Int J Rehabil Res 21(2): 179-194.
10. Bar-Or O, Inbar O, & Spira R. (1976) Physiological effects of a sports rehabilitation
program on cerebral palsied and post-poliomyelitic adolescents. Medicine & Science in
Sports 8(3): 157-161.
11. Berg K. (1970) Effect of physical training of school children with cerebral palsy. Acta
Paediatr Scand 204 (Suppl): 27-33.
12. Darrah J, Wessel J, Nearingburg P, & O'Connor M. (1999) Evaluation of a community
fitness program for adolescents with cerebral palsy. Pediatr Phys Ther 11(1): 18-23.
13. Lundberg A, Ovenfors CO, & Saltin B. (1967) Effect of physical training on school-
children with cerebral palsy. Acta Paediatr Scand 56(2): 182-188.
14. Lundberg A, & Pernow B. (1970) The effect of physical training on oxygen utilization
and lactate formation in the exercising muscle of adolescents with motor handicaps.
Scandinavian Journal of Clinical & Laboratory Investigation 26(1): 89-96.
15. Shinohara TA, Suzuki N, Oba M, Kawasumi M, Kimizuka M, & Mita K. (2002) Effect
of exercise at the AT point for children with cerebral palsy. Bulletin of the Hospital for
Joint Diseases, 61(1-2), 63-67.
16. Wiepert SL, & Lewis CL. (1998) Effects of a 6-week progressive exercise program on a
child with right hemiparesis. Physical Therapy Case Reports, 1(1), 21-26.
17. Fragala-Pinkman MA, Haley SM, Rabin J, & Kharasch VS. (2005) A fitness program for
children with disabilities. Physical Therapy, 85(11), 1182-1200.
13
18. Rintala P, Lyytinen H, & Dunn JM. (1990) Influence of a physical activity program on
children with cerebral palsy: A single subject design. Pediatr Exerc Sci 2(1): 46-56.
19. Mulligan H, Abbott S, Clayton S, McKegg P, & Rae R. (2004) The outcome of a
functional exercise programme in an adolescent with cerebral palsy: A single case study.
New Zealand Journal of Physiotherapy, 32(1), 30-38.
20. Schlough K, Nawoczenski D, Case LE, Nolan K, & Wigglesworth JK. (2005) The effects
of aerobic exercise on endurance, strength, function and self-perception in adolescents
with spastic cerebral palsy: A report of three case studies. Pediatr Phys Ther 17(4): 234-
250.
14
Table I
Classification of Outcomes ICF Component Definition Body Function Body functions are the physiological
functions of body systems including psychosocial functions
Body Structure Body structures are anatomical parts of the body such as organs, limbs, and their components
Activity Activity is the execution of a task or action by an individual
Participation Participation is involvement in a life situation
Context/Environmental Factors Environmental factors make up the physical, social and attitudinal environment in which people live and conduct their lives
15
Table II
Levels of Evidence
Level Intervention (Group) studies
I
Systematic Review of randomized controlled trials (RCTs) Large RCTs (with narrow confidence intervals) (n >100)
II
Smaller RCTs (with wider confidence intervals) (n <100) Systematic Reviews of cohort studies “Outcomes research” (very large ecologic studies)
III Cohort studies (must have concurrent control group) Systematic Reviews of Case Control Studies
IV
Case series Cohort study without concurrent control group (e.g. with historical control group) Case-control study
V
Expert Opinion Case Study or report Bench research Expert opinion based on theory or physiologic research Common sense/anecdotes
16
Table III Summary of Studies: Interventions and Participants
Study Level of
Evidence/ Research Design
Intervention Control Intervention Population Total n Ages
1967 Lundberg et al. IV Pre-test/ Post-test with no control group
Continuous large muscle group exercise (running, jumping, parallel bars): 30 min, 2x/wk Duration: 6 wk
None CP: 3 hemiplegia, 3 diplegia, 3 tetraplegia, 4 athetosis, 1 ataxia
14 15-20y
1970 Berg IV Pre-test/ Post-test with no control group
Bicycle ergometer at varying intensities: 20 min, 3x/wk Duration: 1.5- 16 mo
None CP: 12 spastic diplegia or tetraplegia, 10 dyskinetic disturbances
22 7-25y
1970 Lundberg & Pernow
IV Pre-test/Post-test with no control group
Continuous large muscle exercise (running, jumping, parallel bars, dumbbells, medicine balls, pulleys): 30 min, 2x/wk Duration: 6 wk
None CP: 3 diplegia, 3 athetosis, 1 hemiplegia, 1 ataxia, 1 post-traumatic spastic hemiplegia
9 15-25y
1976 Bar-Or et al. III-W (1/7) Cohort Study
Combination of group and individual games
9 children with cerebral palsy that did not begin or
CP. 26 Spastic diplegia with 2 subjects with a mix of
26 15-22y
17
(table tennis, shuffleboard, bowling) and mat exercises: 2hr/d, 2d/wk Duration: 12 mo
stopped training within first 2 mo
spasticity and athetosis. All ambulatory to varying degrees
1985 Dresen et al. II-W (3/7) Small RCT
Regular physical education classes (judo, swimming and games): 3x/wk for total of 2hr/wk Duration: 10 wk
As intervention without active encouragement.
CP: 6 spastic hemiplegia, 3 spastic diplegia, 1 dwarf growth, 1 cerebellar ataxia. 4 of 11 were being treated for epilepsy
12; EXP= 6 CON=5 1 drop-out
8-14y
1990 Rintala et al. Single Subject Design
Rotation through activities targeting static and dynamic balance, physical fitness and catching and throwing skills: 1hr/d, 2 d/wk for a total of 30 sessions. Duration: 4 mo
None CP: 8 with either hemiplegia or diplegia, All ambulatory
8 7-11y
1998 van den Berg- Emons et al.
II-W (2/7) Small RCT
a) First year Intervention: Group aerobic exercise program (cycling, wheelchair skills, running, swimming, flying saucer, mat exercises): 45 min,
Regular school physical education and individual physiotherapy sessions.
CP: 16 diplegia, 4 tetraplegia. 10 ambulatory, 10 used wheelchair
20 a) EXP= 10 CON=10 b) EXP=17 CON=10
7-13y
18
4x/wk in addition to regular PE and PT Duration: 9 mo b) Second Year Intervention: As in a) minus swimming and isokinetic strengthening: 45 min, 2x/wk plus regular PE and PT Duration: 9 mo
1998 Wiepert & Lewis
V Case Study PT led activities including ball play, step-ups, prolonged walking, tricycle riding: 1hr/d, 2d/wk Duration: 6 wk
None 1 child with hemiparetic CP
1 3y
1999 Darrah et al. IV Pre-test/Post-test with no control group
Circuit training program including aerobics, strengthening, flexibility: 70-90min, 3x/wk Duration: 10 wk
None CP: 13 hemiplegia, 5 diplegia, 2 quadraplegia, 2 ataxia, 1 dystonia. 2 non-ambulatory, 1 used a walking stick, 20 independent ambulators
23 11-20y
2002 Shinohara et al. IV Pre-test/ Post-test with no control group
Children trained at anaerobic threshold (AT) point on either arm or leg cycle ergometer (as able):
None 11 CP. All ambulatory to varying degrees.
11 13.3- 15.8y
19
20 min, 1.8 d/wk Duration: 6 to 20 wk
2004 Mulligan et al. Single Subject Design
Cardiovascular and strength conditioning program at outpatient facility: 1d/wk, 3 additional strength sessions at home and encouragement to increase daily physical activity Duration: 6 wk
None CP: 1 spastic diplegia 1 13y
2005 Fragala-Pinkham et al.
IV Case Report a) Group fitness program (movement to music, parachute games, obstacle courses, games, riding bicycles, strength training): 60-70min, 2x/wk Duration: 14 wk b) Non-simultaneous home exercise program: written instructions and video taped aerobics and
None CP: 1 hemiplegia, 3 spastic diplegia, Non- CP: 1 anoxic brain injury, 2 developmental coordination disorders, 1 pervasive developmental disorder, 1 developmental delay
9 5-9y
20
strengthening activities: 2x/wk Duration: 3 mo
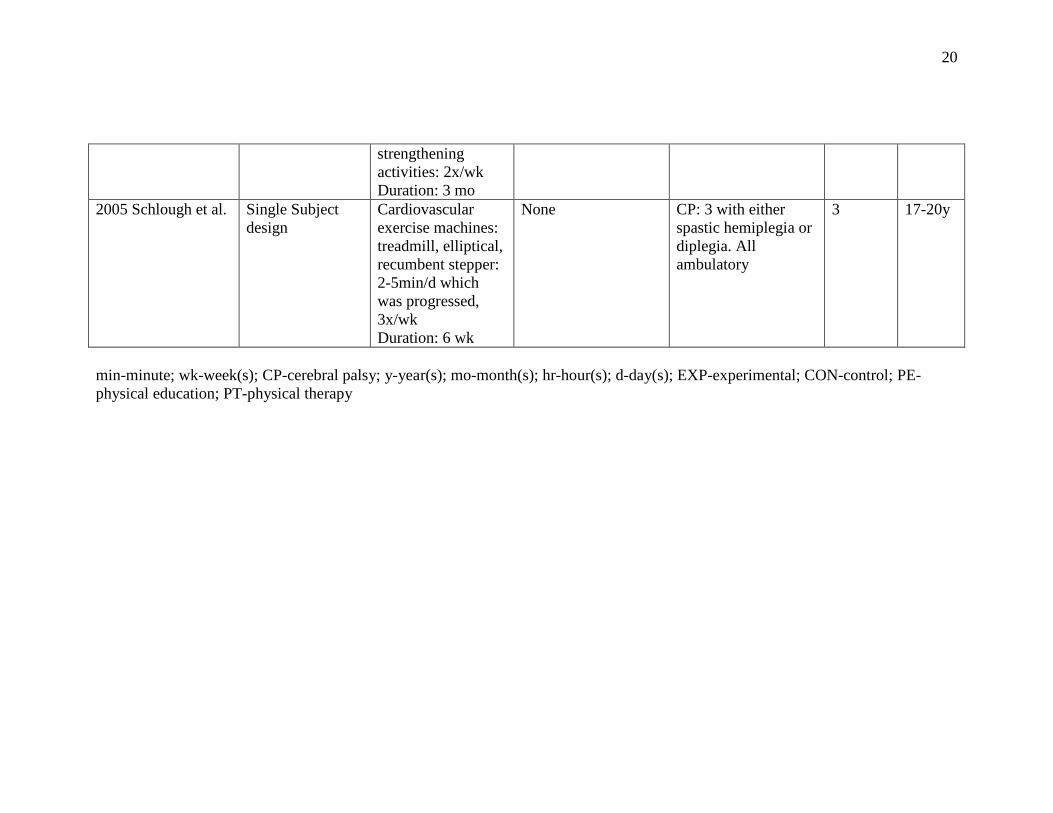
2005 Schlough et al. Single Subject design
Cardiovascular exercise machines: treadmill, elliptical, recumbent stepper: 2-5min/d which was progressed, 3x/wk Duration: 6 wk
None CP: 3 with either spastic hemiplegia or diplegia. All ambulatory
3 17-20y
min-minute; wk-week(s); CP-cerebral palsy; y-year(s); mo-month(s); hr-hour(s); d-day(s); EXP-experimental; CON-control; PE-physical education; PT-physical therapy
21
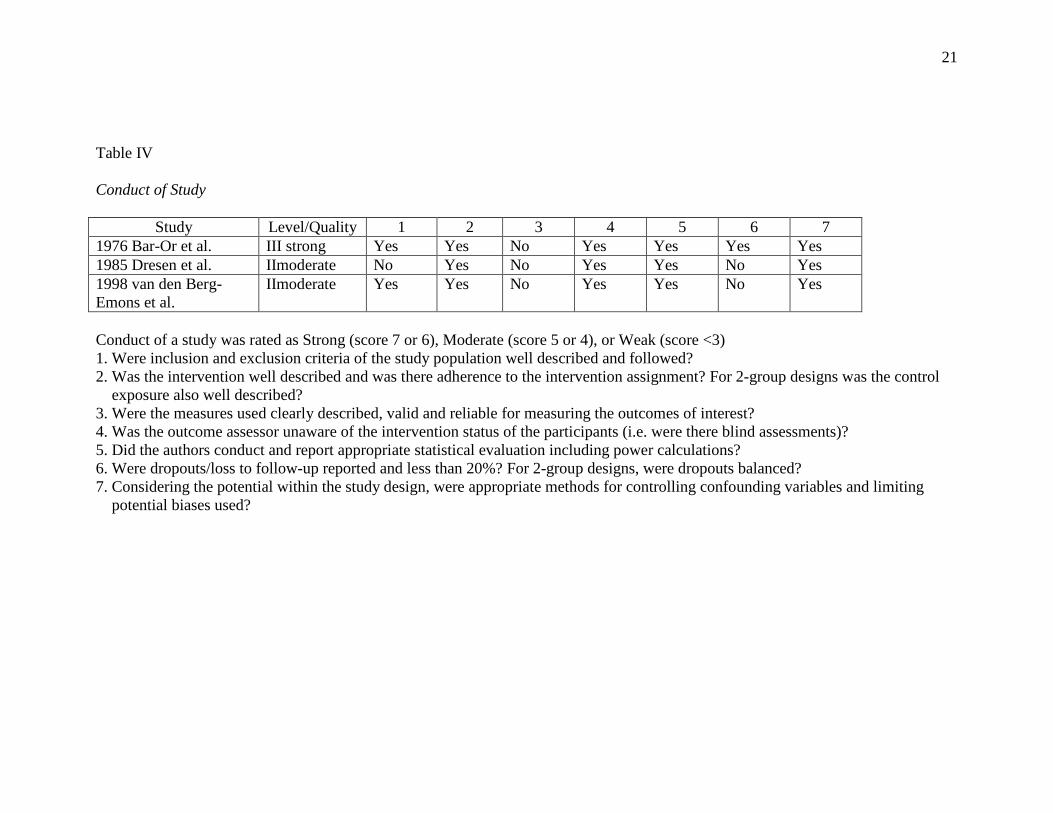
Table IV
Conduct of Study
Study Level/Quality 1 2 3 4 5 6 7 1976 Bar-Or et al. III strong Yes Yes No Yes Yes Yes Yes 1985 Dresen et al. IImoderate No Yes No Yes Yes No Yes 1998 van den Berg- Emons et al.
IImoderate Yes Yes No Yes Yes No Yes
Conduct of a study was rated as Strong (score 7 or 6), Moderate (score 5 or 4), or Weak (score <3) 1. Were inclusion and exclusion criteria of the study population well described and followed? 2. Was the intervention well described and was there adherence to the intervention assignment? For 2-group designs was the control exposure also well described? 3. Were the measures used clearly described, valid and reliable for measuring the outcomes of interest? 4. Was the outcome assessor unaware of the intervention status of the participants (i.e. were there blind assessments)? 5. Did the authors conduct and report appropriate statistical evaluation including power calculations? 6. Were dropouts/loss to follow-up reported and less than 20%? For 2-group designs, were dropouts balanced? 7. Considering the potential within the study design, were appropriate methods for controlling confounding variables and limiting potential biases used?
22
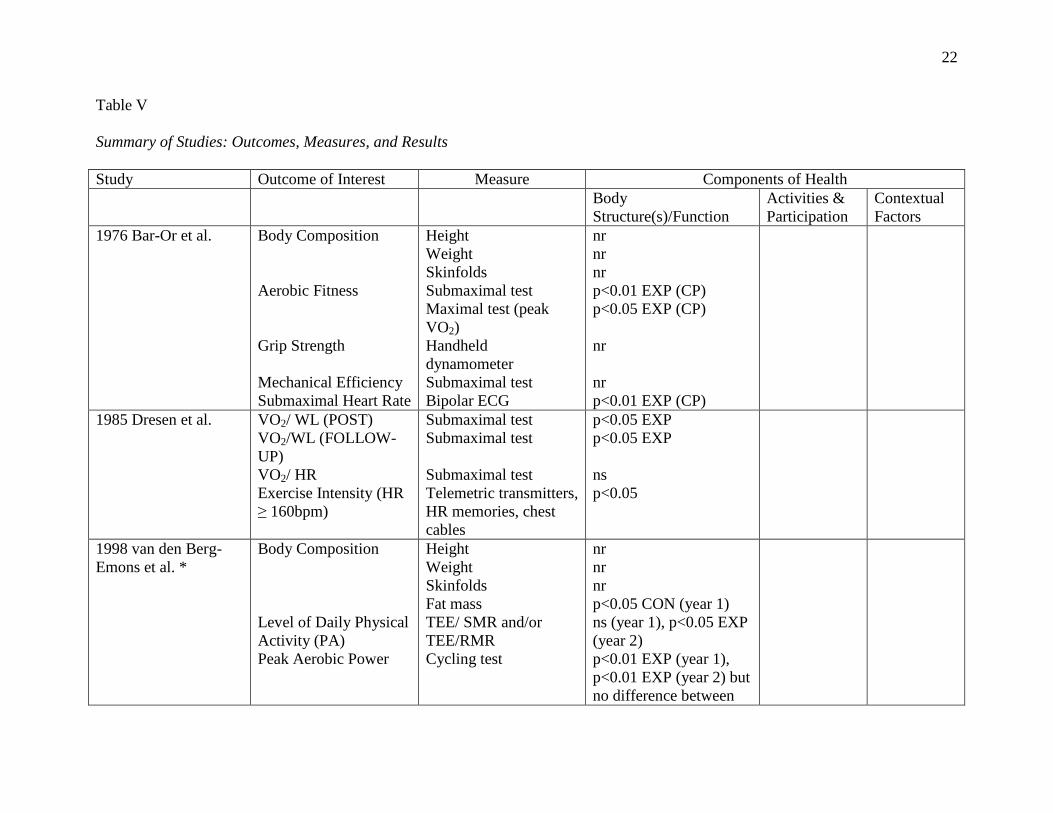
Table V
Summary of Studies: Outcomes, Measures, and Results
Study Outcome of Interest Measure Components of Health Body
Structure(s)/Function Activities & Participation
Contextual Factors
1976 Bar-Or et al. Body Composition Aerobic Fitness Grip Strength Mechanical Efficiency Submaximal Heart Rate
Height Weight Skinfolds Submaximal test Maximal test (peak VO2) Handheld dynamometer Submaximal test Bipolar ECG
nr nr nr p<0.01 EXP (CP) p<0.05 EXP (CP) nr nr p<0.01 EXP (CP)
1985 Dresen et al. VO2/ WL (POST) VO2/WL (FOLLOW-UP) VO2/ HR Exercise Intensity (HR ≥ 160bpm)
Submaximal test Submaximal test Submaximal test Telemetric transmitters, HR memories, chest cables
p<0.05 EXP p<0.05 EXP ns p<0.05
1998 van den Berg- Emons et al. *
Body Composition Level of Daily Physical Activity (PA) Peak Aerobic Power
Height Weight Skinfolds Fat mass TEE/ SMR and/or TEE/RMR Cycling test
nr nr nr p<0.05 CON (year 1) ns (year 1), p<0.05 EXP (year 2) p<0.01 EXP (year 1), p<0.01 EXP (year 2) but no difference between
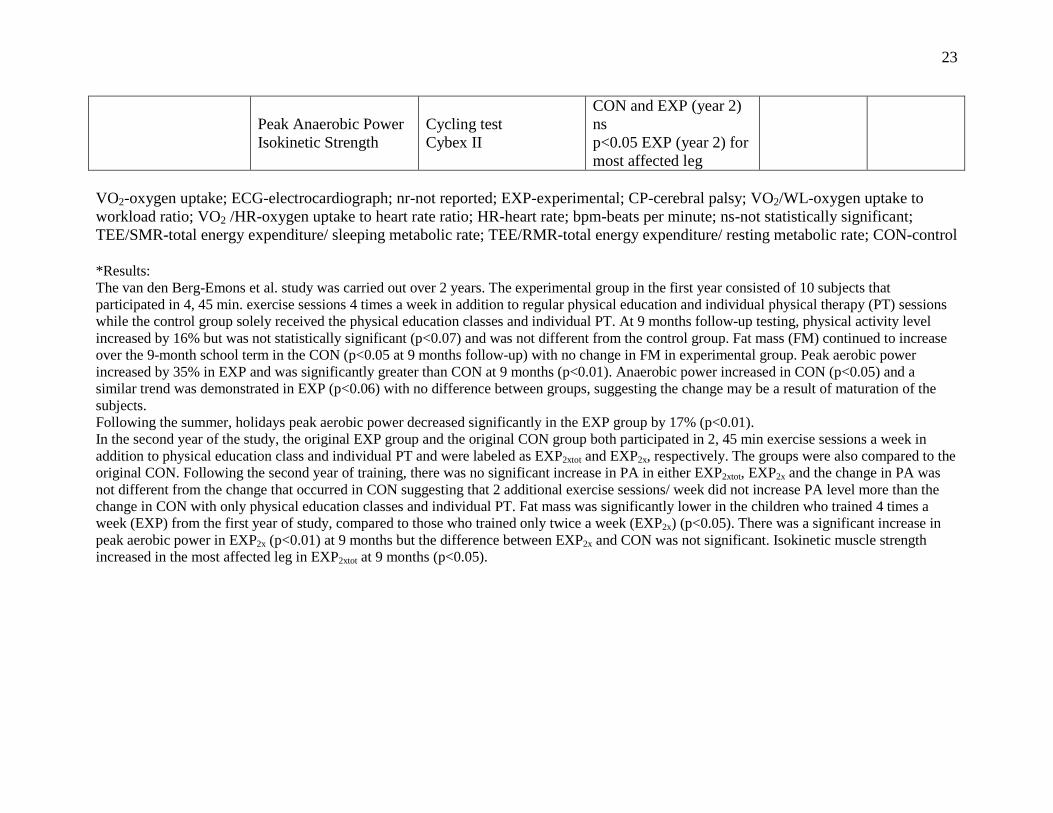
23
Peak Anaerobic Power Isokinetic Strength
Cycling test Cybex II
CON and EXP (year 2) ns p<0.05 EXP (year 2) for most affected leg
VO2-oxygen uptake; ECG-electrocardiograph; nr-not reported; EXP-experimental; CP-cerebral palsy; VO2/WL-oxygen uptake to workload ratio; VO2 /HR-oxygen uptake to heart rate ratio; HR-heart rate; bpm-beats per minute; ns-not statistically significant; TEE/SMR-total energy expenditure/ sleeping metabolic rate; TEE/RMR-total energy expenditure/ resting metabolic rate; CON-control *Results: The van den Berg-Emons et al. study was carried out over 2 years. The experimental group in the first year consisted of 10 subjects that participated in 4, 45 min. exercise sessions 4 times a week in addition to regular physical education and individual physical therapy (PT) sessions while the control group solely received the physical education classes and individual PT. At 9 months follow-up testing, physical activity level increased by 16% but was not statistically significant (p<0.07) and was not different from the control group. Fat mass (FM) continued to increase over the 9-month school term in the CON (p<0.05 at 9 months follow-up) with no change in FM in experimental group. Peak aerobic power increased by 35% in EXP and was significantly greater than CON at 9 months (p<0.01). Anaerobic power increased in CON (p<0.05) and a similar trend was demonstrated in EXP (p<0.06) with no difference between groups, suggesting the change may be a result of maturation of the subjects. Following the summer, holidays peak aerobic power decreased significantly in the EXP group by 17% (p<0.01). In the second year of the study, the original EXP group and the original CON group both participated in 2, 45 min exercise sessions a week in addition to physical education class and individual PT and were labeled as EXP2xtot and EXP2x, respectively. The groups were also compared to the original CON. Following the second year of training, there was no significant increase in PA in either EXP2xtot, EXP2x and the change in PA was not different from the change that occurred in CON suggesting that 2 additional exercise sessions/ week did not increase PA level more than the change in CON with only physical education classes and individual PT. Fat mass was significantly lower in the children who trained 4 times a week (EXP) from the first year of study, compared to those who trained only twice a week (EXP2x) (p<0.05). There was a significant increase in peak aerobic power in EXP2x (p<0.01) at 9 months but the difference between EXP2x and CON was not significant. Isokinetic muscle strength increased in the most affected leg in EXP2xtot at 9 months (p<0.05).