advanced illness management sutter health lois cross rn bsn acm sutter health...
TRANSCRIPT
Sutter Health
• 25 acute care hospitals (multiple facilities do transplants)• 3 Patient Transfer Centers• Ambulatory Surgery Centers• Urgent Care Facilities & Care Centers• 5,000 physician members of the Sutter Medical Network (5
Foundations, 4 IPAs)• Approximately 48,000 employees• Home health, hospice & long-term care services• Medical research and training• $2 million a week in charity care • 5 Regions & 6 Boards of Directors• Culturally diverse population• Competitive environment w/ heavy Kaiser presence & multiple
Academic centers
Serving more than 100 cities and towns in
Northern California & Hawaii with:

A Missing Link?
“Curative”Treatment“Curative”Treatment
ComfortCare
ComfortCare
HFHF
COPDCOPD
DMDM
etcetc
ChronicDisease
Management
AdvancedIllness
Management(AIM)
AdvancedIllness
Management(AIM)
??
Goals of Program• Patient Centered• Evidence Based• Patient experience is important across time and all
settings • Support patient that may be actively pursuing curative
treatments• Coordinate care around patient’s goals to improve
patient well being and quality of life• Reduce avoidable hospitalizations, ED visits• Reduce physician practice burden• Provide improved access to quality comprehensive end
of life care for patient and family
Key Elements
– Patient (caregiver) Support– Individualized Care Plans
• Patient-centered: patient’s care goals, that may change as illness progresses
• Curative and comfort• Psychosocial and spiritual• Access to decision support & advice• Advance care planning
– Care Coordination Across Health System• Team approach with providers• PCP relationship is critical to success• Coordinate care over an extended period of time• Integrated with inpatient palliative care• Data driven continuous improvement
5
Team Members
• AIM Care Liaison
• AIM Home Health Team
RN/SW/PT/OT
• Transitions Nurse
• Office Based Case Manager
6
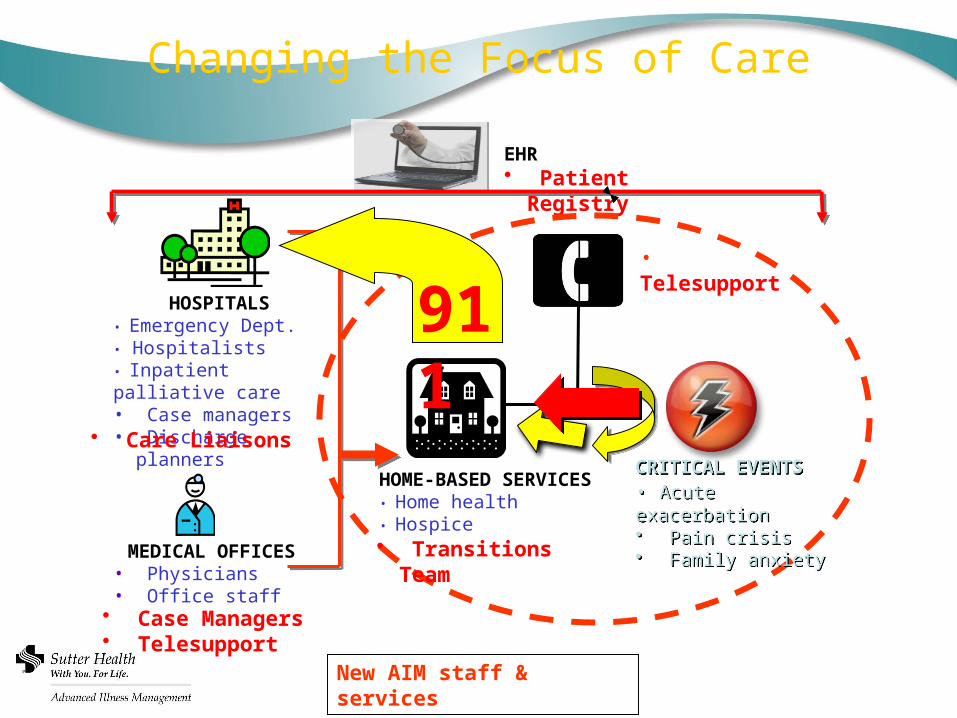
Changing the Focus of Care
HOSPITALS• Emergency Dept.• Hospitalists• Inpatient palliative care• Case managers• Discharge planners
MEDICAL OFFICES• Physicians• Office staff
HOME-BASED SERVICES• Home health • Hospice
• Telesupport
New AIM staff & services
EHR• Patient
Registry
911
• Care Liaisons
• Case Managers• Telesupport
• Transitions Team
CRITICAL EVENTS• Acute exacerbation• Pain crisis• Family anxiety
CRITICAL EVENTS• Acute exacerbation• Pain crisis• Family anxiety
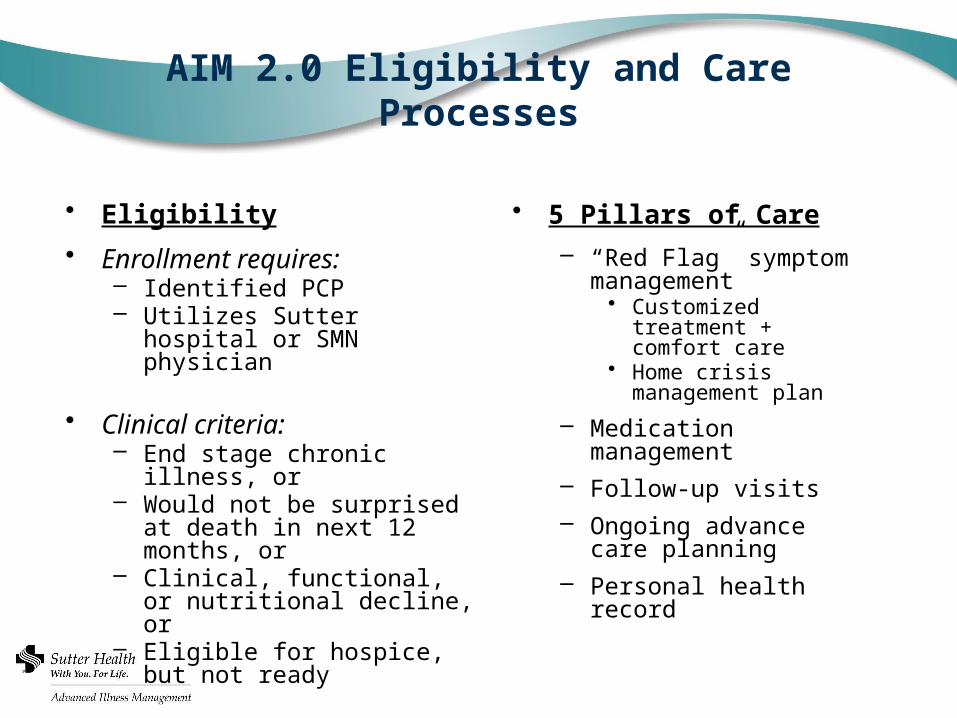
AIM 2.0 Eligibility and Care Processes
• Eligibility
• Enrollment requires:– Identified PCP– Utilizes Sutter hospital or SMN
physician
• Clinical criteria:– End stage chronic illness, or– Would not be surprised at
death in next 12 months, or– Clinical, functional, or
nutritional decline, or– Eligible for hospice, but not
ready
• 5 Pillars of Care
– “Red Flag” symptom management
• Customized treatment + comfort care
• Home crisis management plan
– Medication management– Follow-up visits– Ongoing advance care
planning– Personal health record
Staff Training
• Pillars• Symptom management• Motivational Interviewing• Teach Back• Advanced Care Planning• Cultural Issues
9
Outcome Measures
• Adherence to model supports patient centered goals and evidence based practices– Measured in terms of completion of pillars at key times and
places• Patient Experience – Engagement via crisis planning,
use of personal health record, and satisfaction surveys.• Provider Experience- Satisfaction surveys; (Advisory
Committee)• Utilization and cost of all health services – Hospital,
physician, home health, hospice, snf, etc.• Improvement in number of referrals to and days of
care provided by hospice to an AIM patient
Program Evaluation Methodologies
• Pre / Post utilization and cost data 30 days, 90 days, 180 days - quarterly
• Comparative analysis with Dartmouth Atlas Data Base -quarterly
• Comparative analysis with FFS Medicare non Sutter Health patient population – final results pending
• Concurrent control group- under consideration
Results- What do the trends look like?
• Descriptive Statistics• Utilization Trends• Cost Trends
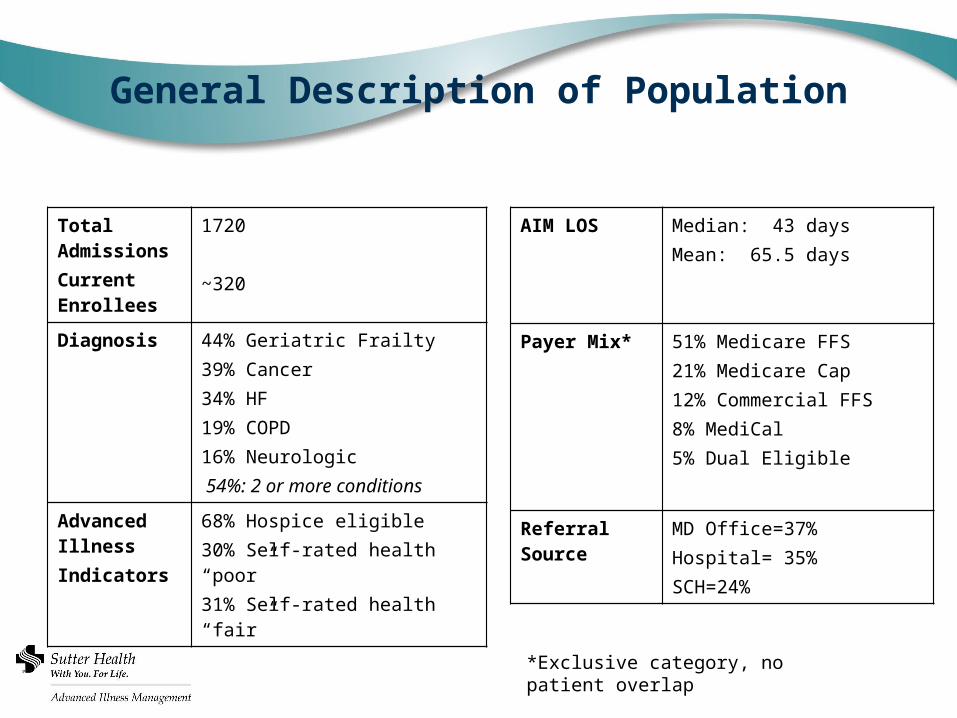
General Description of Population
Total AdmissionsCurrent Enrollees
1720
~320
Diagnosis 44% Geriatric Frailty39% Cancer 34% HF 19% COPD 16% Neurologic 54%: 2 or more conditions
Advanced IllnessIndicators
68% Hospice eligible30% Self-rated health “poor”31% Self-rated health “fair”
AIM LOS Median: 43 daysMean: 65.5 days
Payer Mix* 51% Medicare FFS21% Medicare Cap12% Commercial FFS8% MediCal5% Dual Eligible
Referral Source
MD Office=37%Hospital= 35%SCH=24%
*Exclusive category, no patient overlap
14
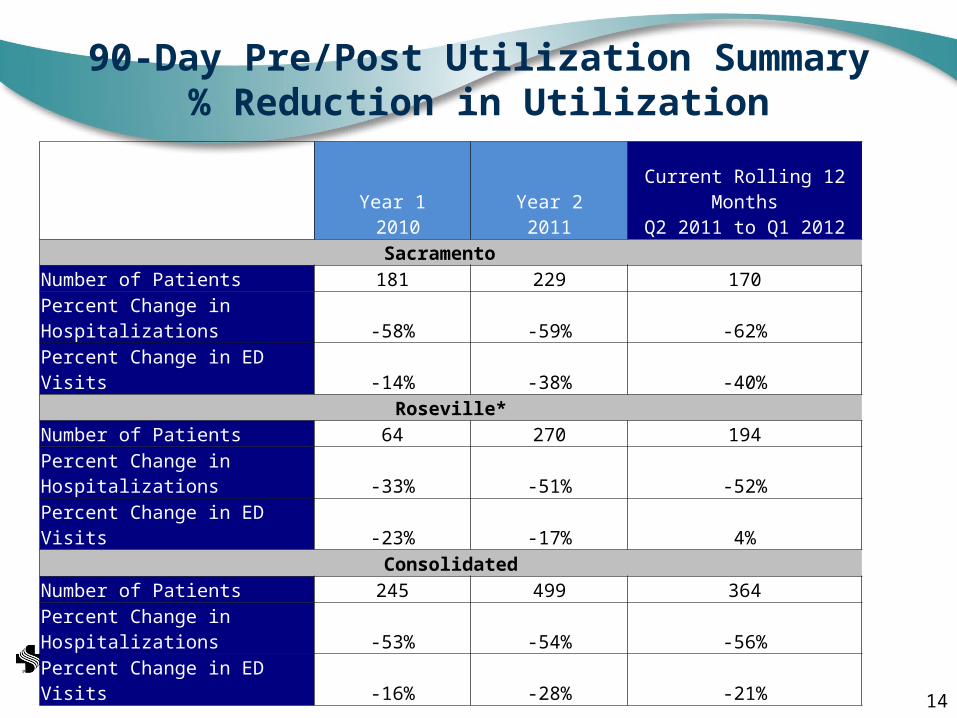
90-Day Pre/Post Utilization Summary% Reduction in Utilization
Year 1 2010
Year 22011
Current Rolling 12 MonthsQ2 2011 to Q1 2012
Sacramento Number of Patients 181 229 170
Percent Change in Hospitalizations -58% -59% -62%
Percent Change in ED Visits -14% -38% -40%Roseville*
Number of Patients 64 270 194
Percent Change in Hospitalizations -33% -51% -52%
Percent Change in ED Visits -23% -17% 4%Consolidated
Number of Patients 245 499 364
Percent Change in Hospitalizations -53% -54% -56%
Percent Change in ED Visits -16% -28% -21%
15
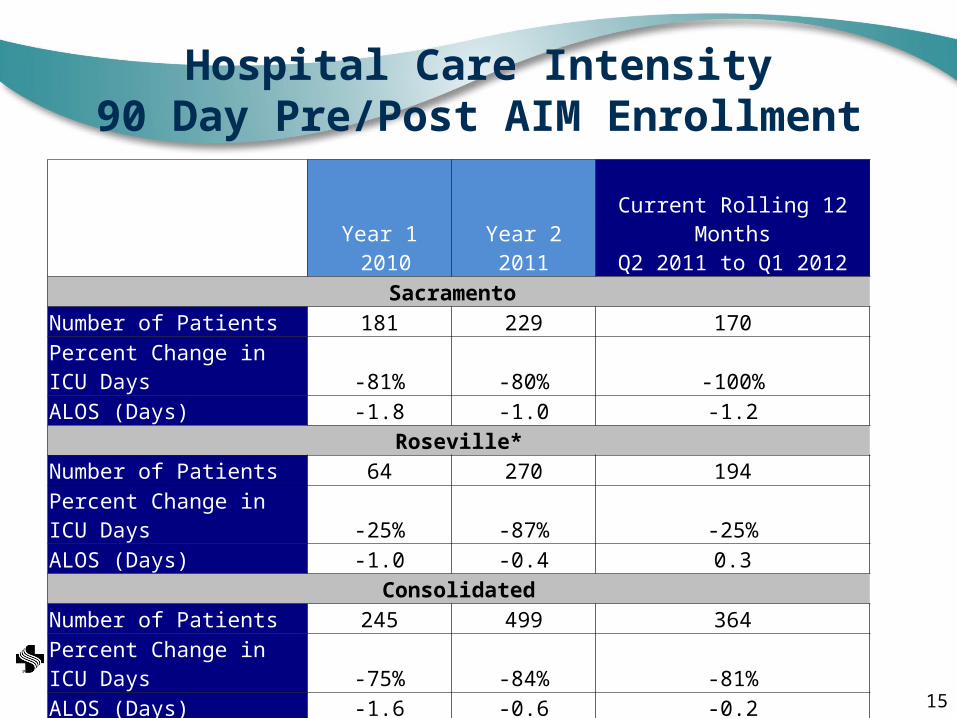
Hospital Care Intensity90 Day Pre/Post AIM Enrollment
Year 1 2010
Year 22011
Current Rolling 12 MonthsQ2 2011 to Q1 2012
Sacramento Number of Patients 181 229 170Percent Change in ICU Days -81% -80% -100%ALOS (Days) -1.8 -1.0 -1.2
Roseville*Number of Patients 64 270 194Percent Change in ICU Days -25% -87% -25%ALOS (Days) -1.0 -0.4 0.3
ConsolidatedNumber of Patients 245 499 364Percent Change in ICU Days -75% -84% -81%ALOS (Days) -1.6 -0.6 -0.2
16
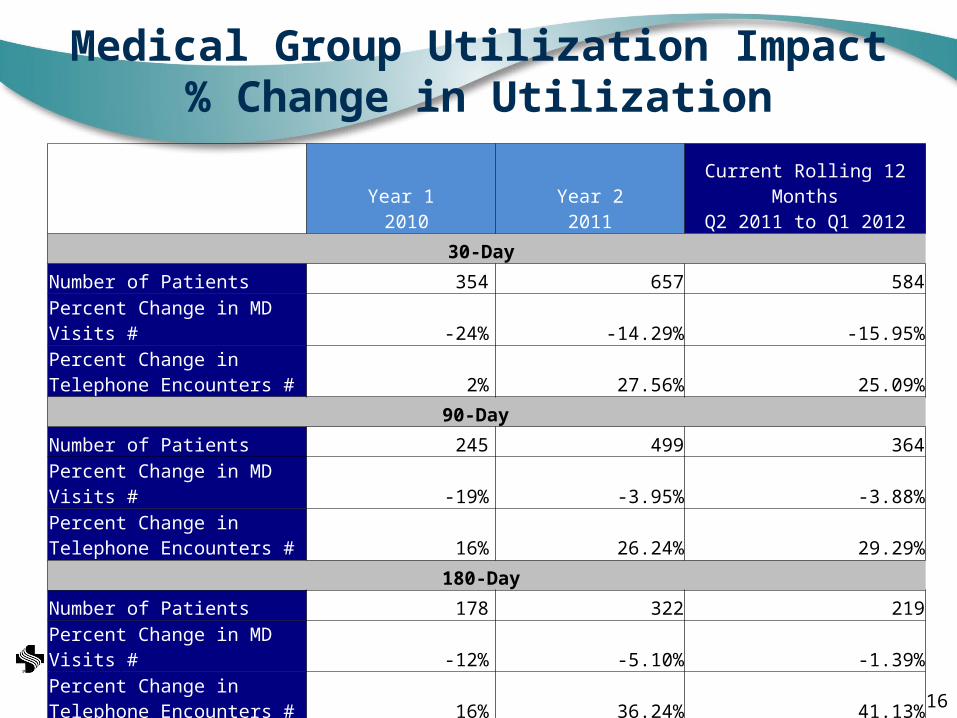
Medical Group Utilization Impact% Change in Utilization
Year 1 2010
Year 22011
Current Rolling 12 MonthsQ2 2011 to Q1 2012
30-Day
Number of Patients 354 657 584
Percent Change in MD Visits # -24% -14.29% -15.95%
Percent Change in Telephone Encounters # 2% 27.56% 25.09%
90-Day
Number of Patients 245 499 364
Percent Change in MD Visits # -19% -3.95% -3.88%
Percent Change in Telephone Encounters # 16% 26.24% 29.29%
180-Day
Number of Patients 178 322 219
Percent Change in MD Visits # -12% -5.10% -1.39%
Percent Change in Telephone Encounters # 16% 36.24% 41.13%
17
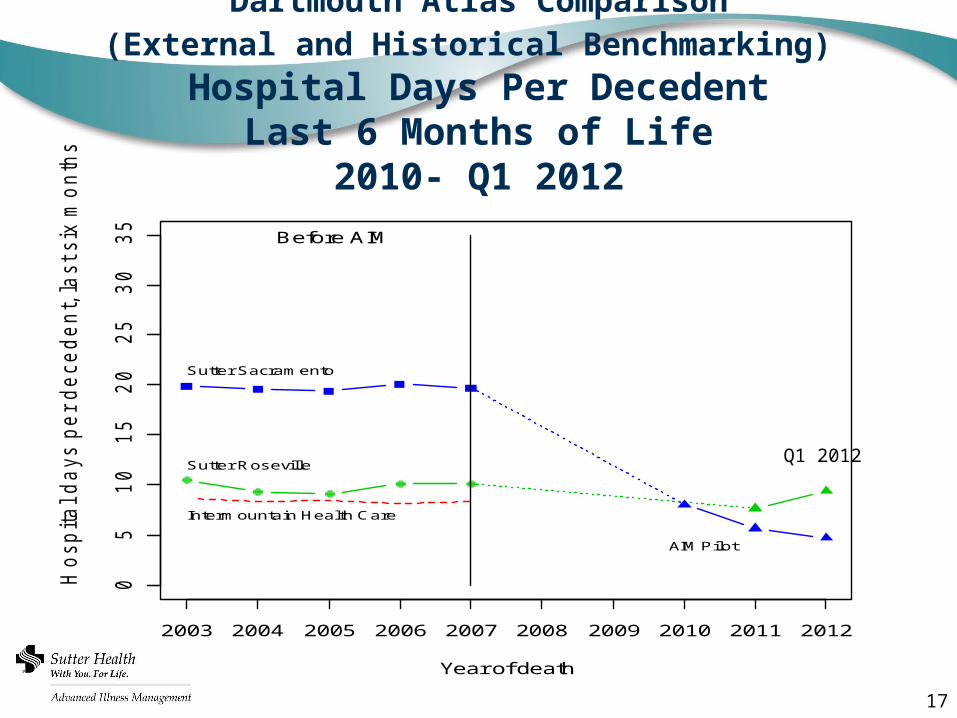
Dartmouth Atlas Comparison(External and Historical Benchmarking)
Hospital Days Per DecedentLast 6 Months of Life
2010- Q1 2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
05
10
15
20
25
30
35
Year of death
Ho
sp
ita
l d
ays p
er
de
ce
de
nt, la
st six
mo
nth
s o
f life
Before AIM
Intermountain Health Care
Sutter Roseville
Sutter Sacramento
AIM Pilot
Q1 2012
18
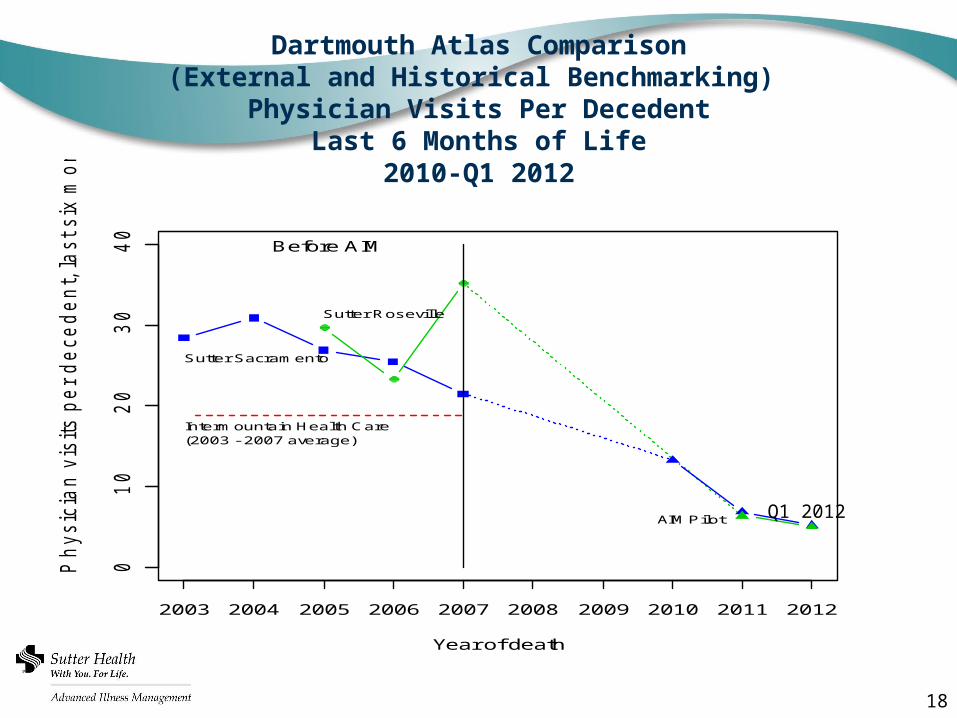
Dartmouth Atlas Comparison(External and Historical Benchmarking)
Physician Visits Per DecedentLast 6 Months of Life
2010-Q1 2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
01
02
03
04
0
Year of death
Ph
ysic
ian
vis
its p
er
de
ce
de
nt, la
st six
mo
nth
s o
f life
Before AIM
Intermountain Health Care (2003 - 2007 average)
Sutter Roseville
Sutter Sacramento
AIM Pilot Q1 2012
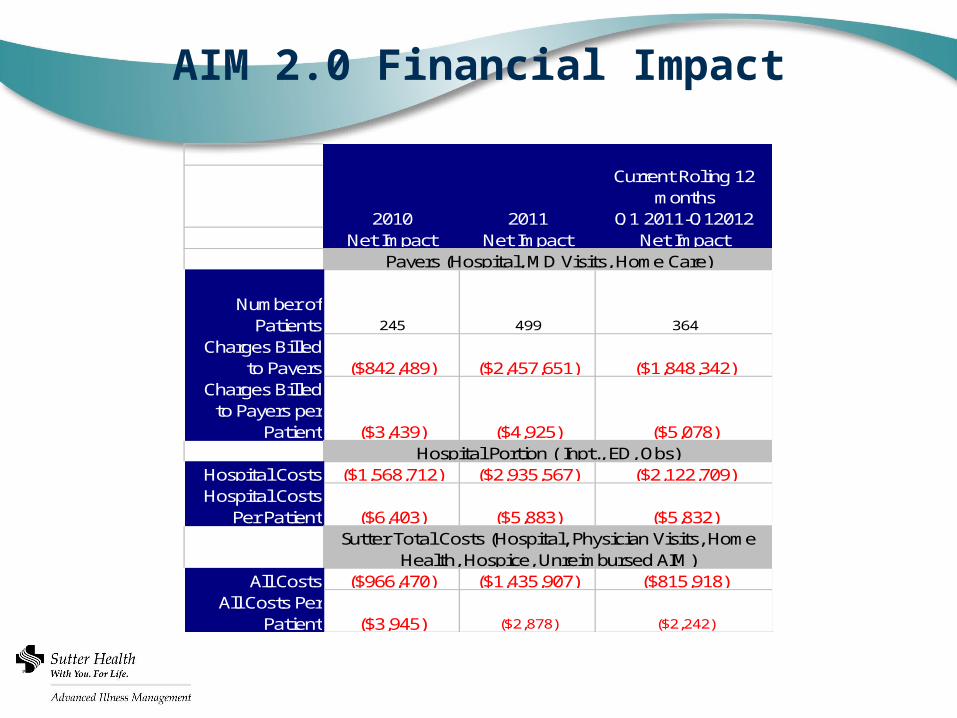
AIM 2.0 Financial Impact
2010 2011
Current Roling 12 months
Q1 2011-Q12012Net Impact Net Impact Net Impact
Number of Patients 245 499 364
Charges Billed to Payers ($842,489) ($2,457,651) ($1,848,342)
Charges Billed to Payers per
Patient ($3,439) ($4,925) ($5,078)
Hospital Costs ($1,568,712) ($2,935,567) ($2,122,709)Hospital Costs
Per Patient ($6,403) ($5,883) ($5,832)
All Costs ($966,470) ($1,435,907) ($815,918)All Costs Per
Patient ($3,945) ($2,878) ($2,242)
Payers (Hospital, MD Visits, Home Care)
Hospital Portion ( Inpt., ED, Obs)
Sutter Total Costs (Hospital, Physician Visits, Home Health, Hospice, Unreimbursed AIM)
OpportunitiesInfrastructure• Every geographic area looks different• Incorporating other agencies/hospitals
Hiring the right team members
Physician Engagement
Reports
Education
IT-Just In Time communication• EPIC• Home Care Home Base
Team Integration
20