adolescent nutrition_koniz-booher
TRANSCRIPT
This presentation was made possible by the American people through the U.S. Agency for International Development (USAID) under Cooperative Agreement No. AID-OAA-A-11-00031, the Strengthening
Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project.
Moving the Adolescent Nutrition Agenda Forward
Peggy Koniz-Booher, Senior Advisor Nutrition SBCC SPRING Nutrition Project
CORE Group… April 14, 2015

Technical Meeting on the Diet and Eating Practices of Adolescent Girls and Women
March 16 – 17 2015 PAHO/WHO, Washington, DC
Some background on rationale for this technical meeting
• The 2013 Lancet Series on Maternal and Child Nutrition provided new evidence on the importance of the nutrition of women at the time of conception and during pregnancy, not only to ensure optimal fetal growth and development but also for the health of the mother.
• The series also identified adolescent girls as a key priority and highlighted the importance of a life course approach, placing them together with women of reproductive age and mothers at the center of nutrition interventions.
• Despite the recognized importance of adolescent girls’, women’s and maternal nutrition for their health and that of their children, this group is virtually neglected in nutrition programming with the exception of provision of iron and folic acid supplements during pregnancy.
Background/rationale (cont.) • In 2012, there were 1.2 billion adolescents in the world – defined as
young people between the ages of 10 and 19 years. • The vast majority of adolescents (90%) live in low- or middle-income
countries (LMIC). In some countries, as many as half of all adolescents are stunted, with impact on physical and cognitive development
• About 16 million girls aged 15 to 19 and some 1 million girls under 15 give birth every year—most in LMIC. Complications during pregnancy and childbirth are the second cause of death for 15-19 year-old girls
• Alarming shift in BMI globally - growing rates of overweight and obesity in many LMIC. (Throughout LAC, the prevalences of overweight and obesity is around 50%. This is also true for Central and Eastern Europe.)
Meeting Objectives
1. Review insights and lessons learned from two discussion papers commissioned by SPRING
2. Identify characteristics of and issues related to key diet and eating practices for strengthening policies and programs for adolescent girls’ and WRA’s nutrition
3. Propose next steps in development of a set of key diet and eating practices
Began by reflecting on the Guiding Principles:
Goal: To develop a set of unified, scientifically based guidelines that could be adapted to local feeding practices and conditions
This earlier review provided the scientific basis for 9/10 principles
(active feeding not evidence based)
Target audience: Policy makers, program planners, health care providers and community leaders
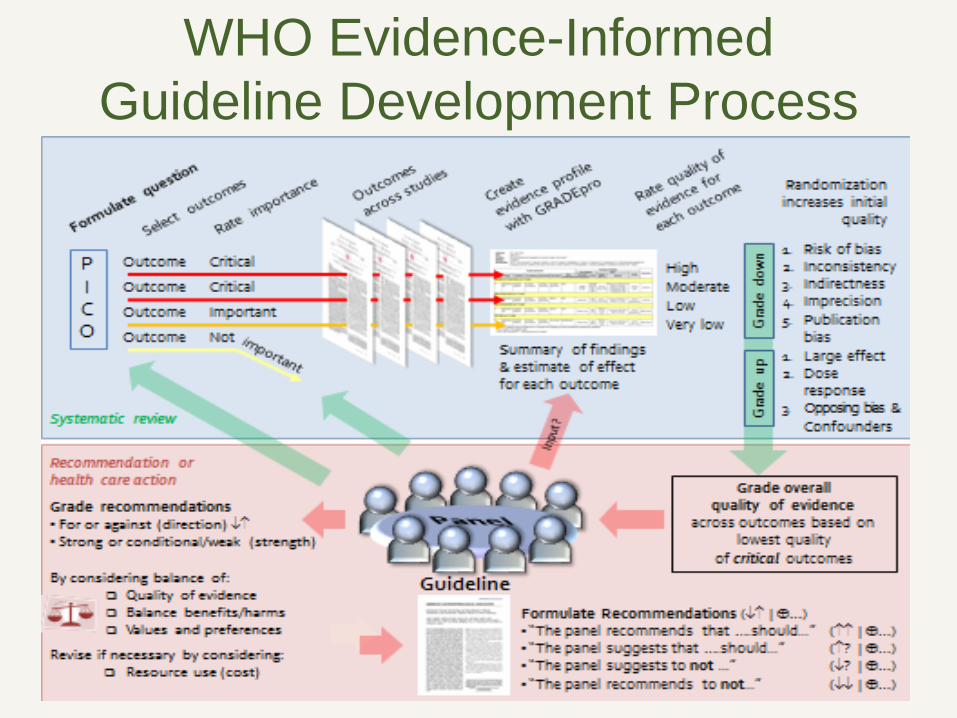
WHO Evidence-Informed Guideline Development Process
Countries have been proliferating Food-Based Dietary Guidelines for about 20 yrs
FAO recently launched an on-line repository of ~100 country FBDGs and associated resources.
A “descriptive summary” project by Mary Arimond, Jennie Coats and Anna Herforth.
Objectives of Background Paper #1: Nutrition of Adolescent Girls and WRA
• Present the current landscape of nutritional status of adolescent girls, women of reproductive age, women during pregnancy and during lactation
• Summarize potential key
nutrition actions and interventions to improve nutritional status of these population groups
Objectives of Background Paper #2: Review of Programmatic Responses
• Conduct a rapid review of the literature & programmatic documentation to: Provide information on global
programmatic experiences to improve the nutrition of adolescent girls and WRA
Summarize inputs, outcomes, and lessons learned from implementers who have/are carrying out nutrition programs

Some highlights #1:
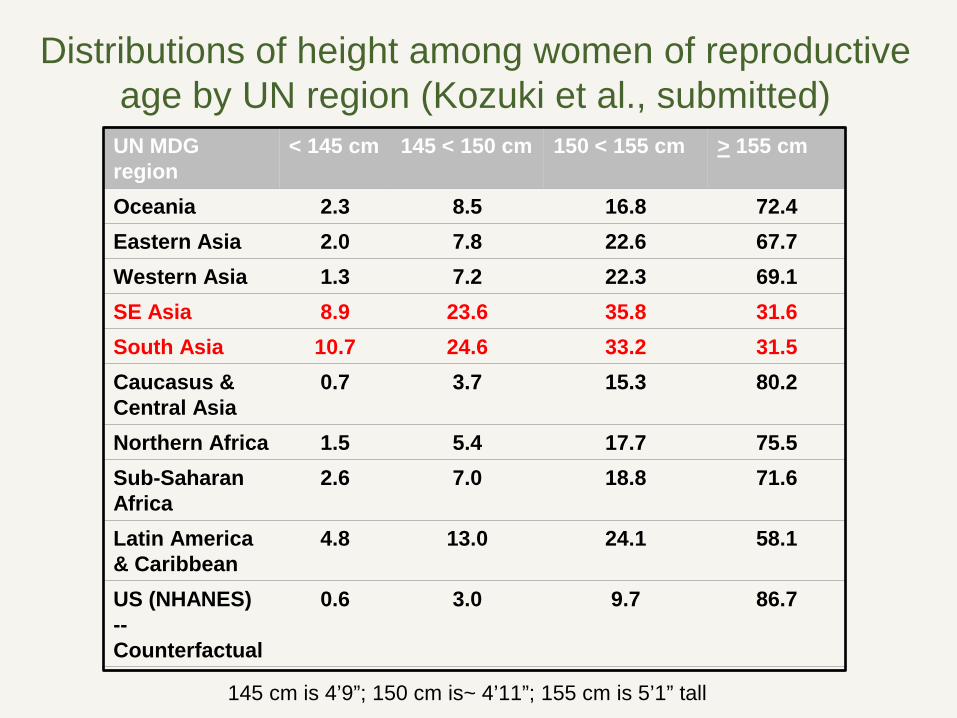
Distributions of height among women of reproductive age by UN region (Kozuki et al., submitted)
UN MDG region
< 145 cm 145 < 150 cm 150 < 155 cm > 155 cm
Oceania 2.3 8.5 16.8 72.4 Eastern Asia 2.0 7.8 22.6 67.7 Western Asia 1.3 7.2 22.3 69.1 SE Asia 8.9 23.6 35.8 31.6 South Asia 10.7 24.6 33.2 31.5 Caucasus & Central Asia
0.7 3.7 15.3 80.2
Northern Africa 1.5 5.4 17.7 75.5 Sub-Saharan Africa
2.6 7.0 18.8 71.6
Latin America & Caribbean
4.8 13.0 24.1 58.1
US (NHANES) -- Counterfactual
0.6 3.0 9.7 86.7
145 cm is 4’9”; 150 cm is~ 4’11”; 155 cm is 5’1” tall
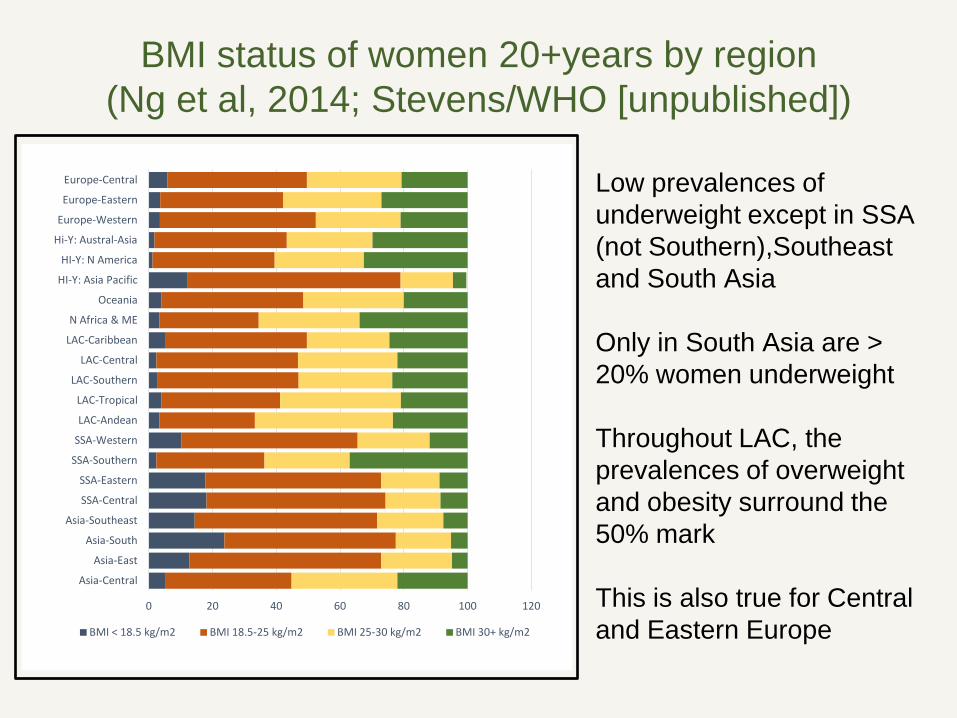
BMI status of women 20+years by region (Ng et al, 2014; Stevens/WHO [unpublished])
Low prevalences of underweight except in SSA (not Southern),Southeast and South Asia Only in South Asia are > 20% women underweight Throughout LAC, the prevalences of overweight and obesity surround the 50% mark This is also true for Central and Eastern Europe
0 20 40 60 80 100 120
Asia-Central
Asia-East
Asia-South
Asia-Southeast
SSA-Central
SSA-Eastern
SSA-Southern
SSA-Western
LAC-Andean
LAC-Tropical
LAC-Southern
LAC-Central
LAC-Caribbean
N Africa & ME
Oceania
HI-Y: Asia Pacific
HI-Y: N America
Hi-Y: Austral-Asia
Europe-Western
Europe-Eastern
Europe-Central
BMI < 18.5 kg/m2 BMI 18.5-25 kg/m2 BMI 25-30 kg/m2 BMI 30+ kg/m2
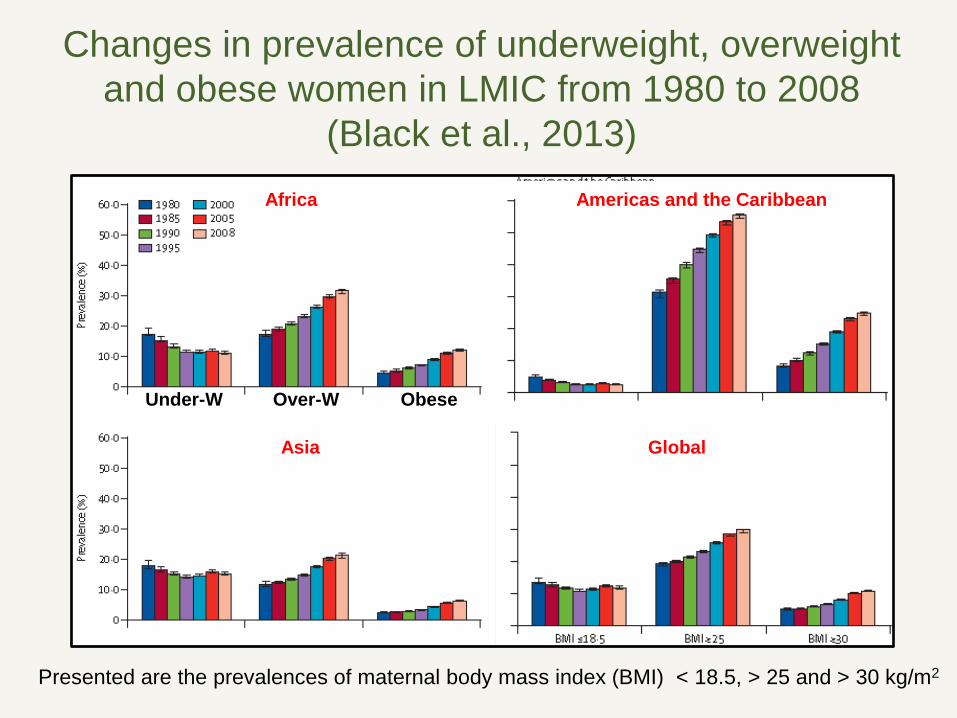
Changes in prevalence of underweight, overweight and obese women in LMIC from 1980 to 2008
(Black et al., 2013)
Presented are the prevalences of maternal body mass index (BMI) < 18.5, > 25 and > 30 kg/m2
Under-W Over-W Obese
Africa Americas and the Caribbean
Asia Global
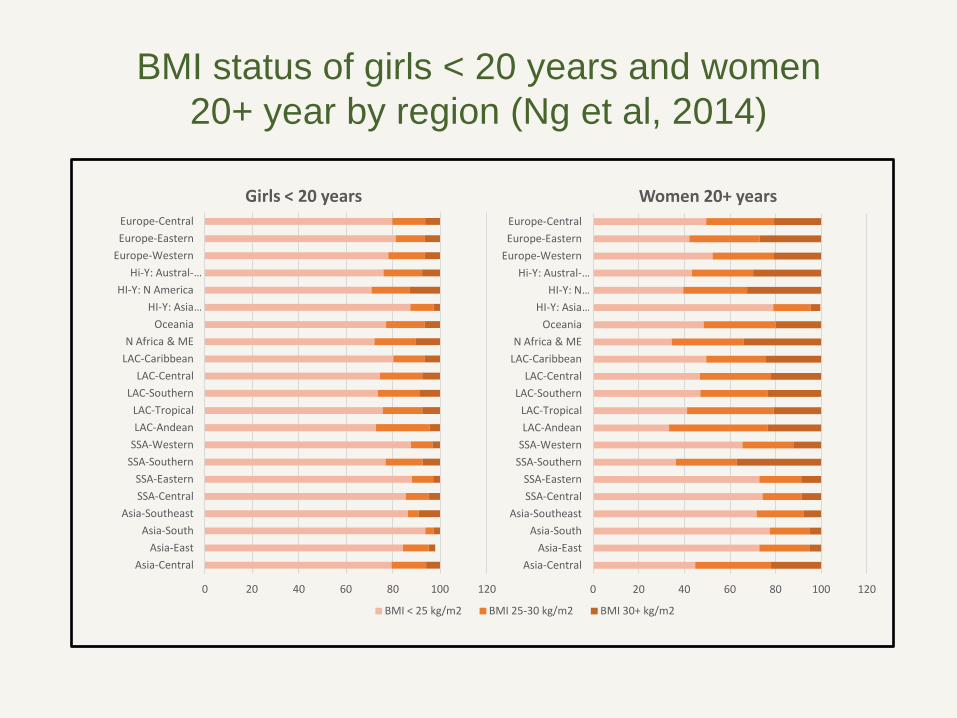
BMI status of girls < 20 years and women 20+ year by region (Ng et al, 2014)
0 20 40 60 80 100 120
Asia-Central Asia-East
Asia-South Asia-Southeast
SSA-Central SSA-Eastern
SSA-Southern SSA-Western LAC-Andean LAC-Tropical
LAC-Southern LAC-Central
LAC-Caribbean N Africa & ME
Oceania HI-Y: Asia …
HI-Y: N America Hi-Y: Austral-…
Europe-Western Europe-Eastern Europe-Central
Girls < 20 years
BMI < 25 kg/m2 BMI 25-30 kg/m2 BMI 30+ kg/m2
0 20 40 60 80 100 120
Asia-Central Asia-East
Asia-South Asia-Southeast
SSA-Central SSA-Eastern
SSA-Southern SSA-Western LAC-Andean LAC-Tropical
LAC-Southern LAC-Central
LAC-Caribbean N Africa & ME
Oceania HI-Y: Asia …
HI-Y: N … Hi-Y: Austral-…
Europe-Western Europe-Eastern Europe-Central
Women 20+ years
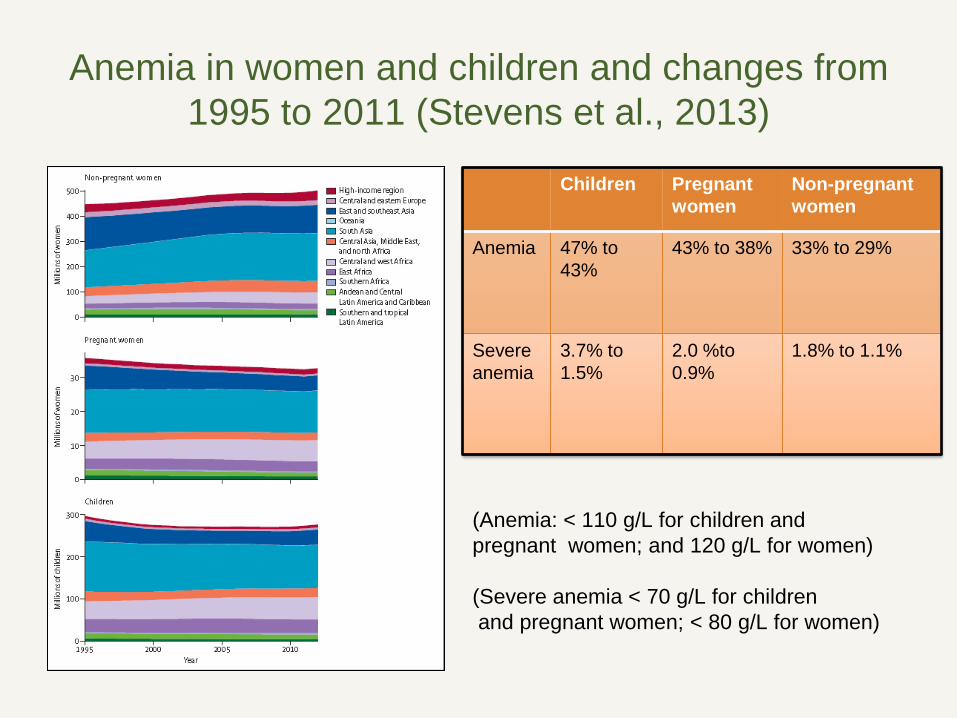
Anemia in women and children and changes from 1995 to 2011 (Stevens et al., 2013)
Prevalence of anemia is declining in most regions
Children Pregnant women
Non-pregnant women
Anemia 47% to 43%
43% to 38% 33% to 29%
Severe anemia
3.7% to 1.5%
2.0 %to 0.9%
1.8% to 1.1%
(Anemia: < 110 g/L for children and pregnant women; and 120 g/L for women) (Severe anemia < 70 g/L for children and pregnant women; < 80 g/L for women)
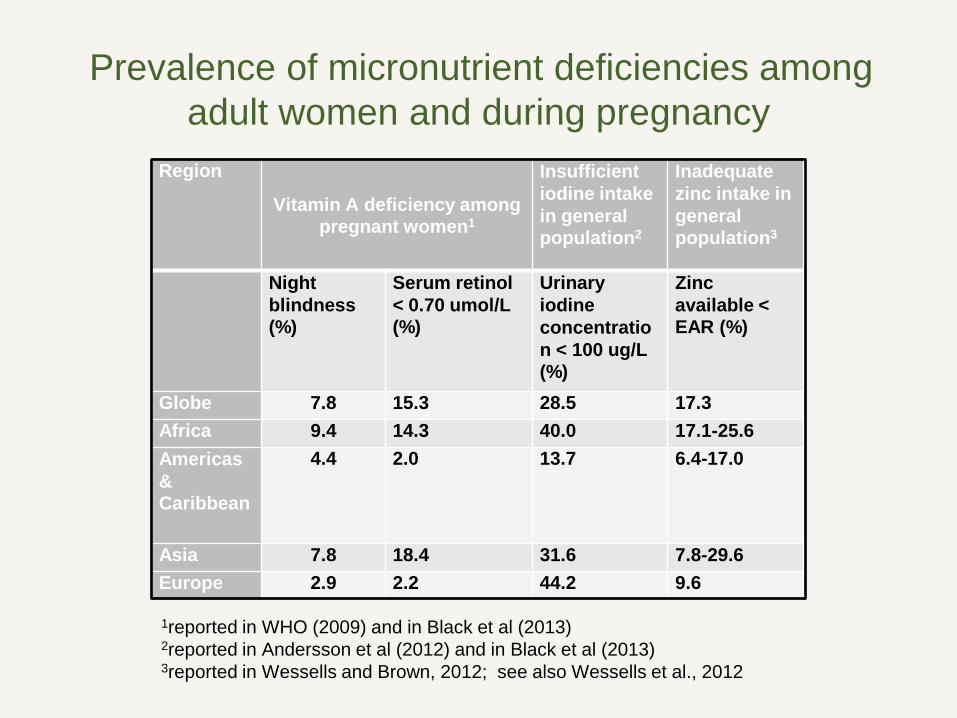
Prevalence of micronutrient deficiencies among adult women and during pregnancy
Region
Vitamin A deficiency among pregnant women1
Insufficient iodine intake in general population2
Inadequate zinc intake in general population3
Night blindness (%)
Serum retinol < 0.70 umol/L (%)
Urinary iodine concentration < 100 ug/L (%)
Zinc available < EAR (%)
Globe 7.8 15.3 28.5 17.3 Africa 9.4 14.3 40.0 17.1-25.6 Americas & Caribbean
4.4 2.0 13.7 6.4-17.0
Asia 7.8 18.4 31.6 7.8-29.6 Europe 2.9 2.2 44.2 9.6
1reported in WHO (2009) and in Black et al (2013) 2reported in Andersson et al (2012) and in Black et al (2013) 3reported in Wessells and Brown, 2012; see also Wessells et al., 2012
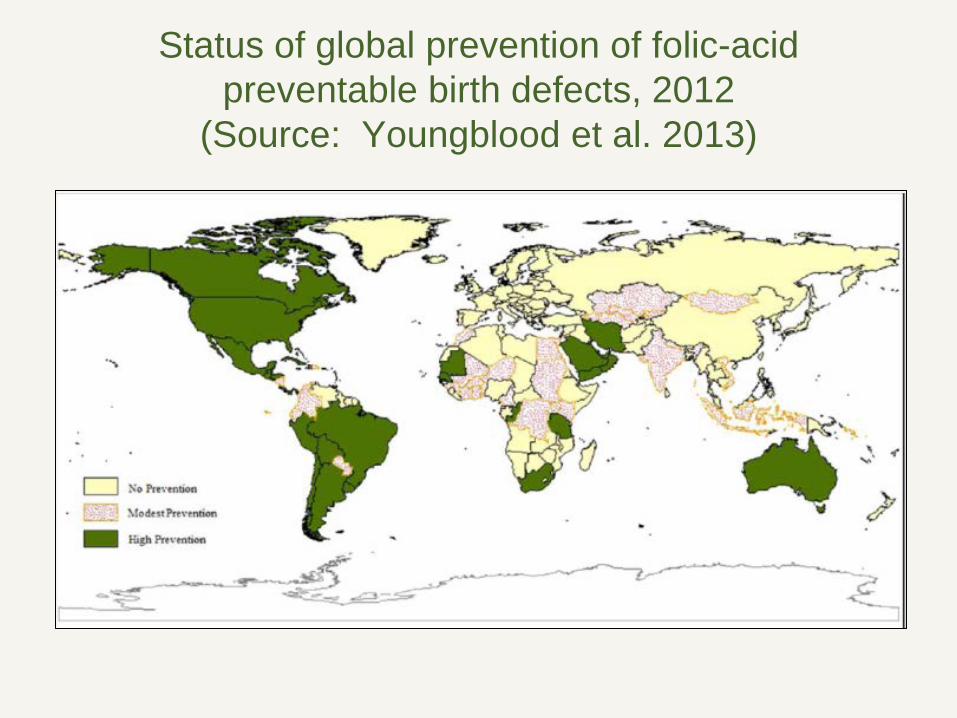
Status of global prevention of folic-acid preventable birth defects, 2012
(Source: Youngblood et al. 2013)
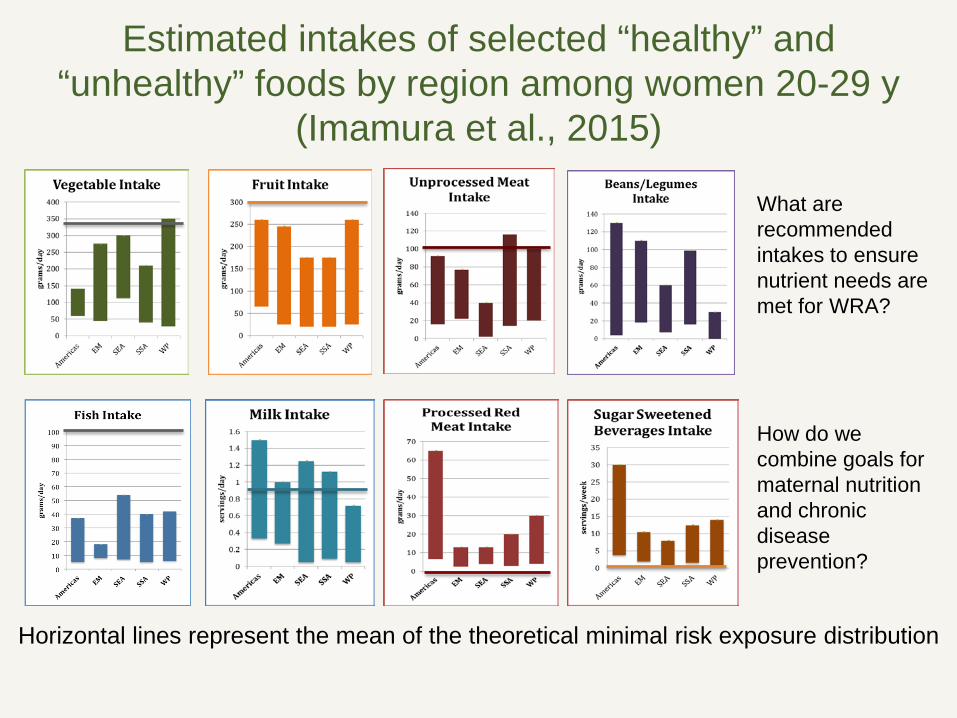
Estimated intakes of selected “healthy” and “unhealthy” foods by region among women 20-29 y
(Imamura et al., 2015) What are recommended intakes to ensure nutrient needs are met for WRA? How do we combine goals for maternal nutrition and chronic disease prevention?
Horizontal lines represent the mean of the theoretical minimal risk exposure distribution
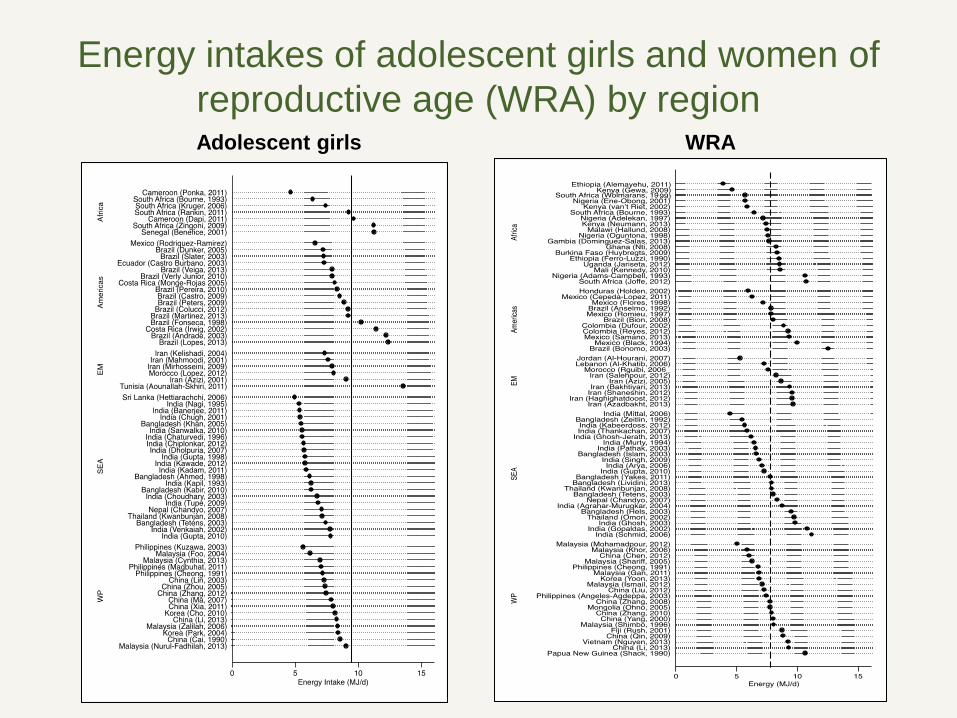
Energy intakes of adolescent girls and women of reproductive age (WRA) by region Adolescent girls WRA
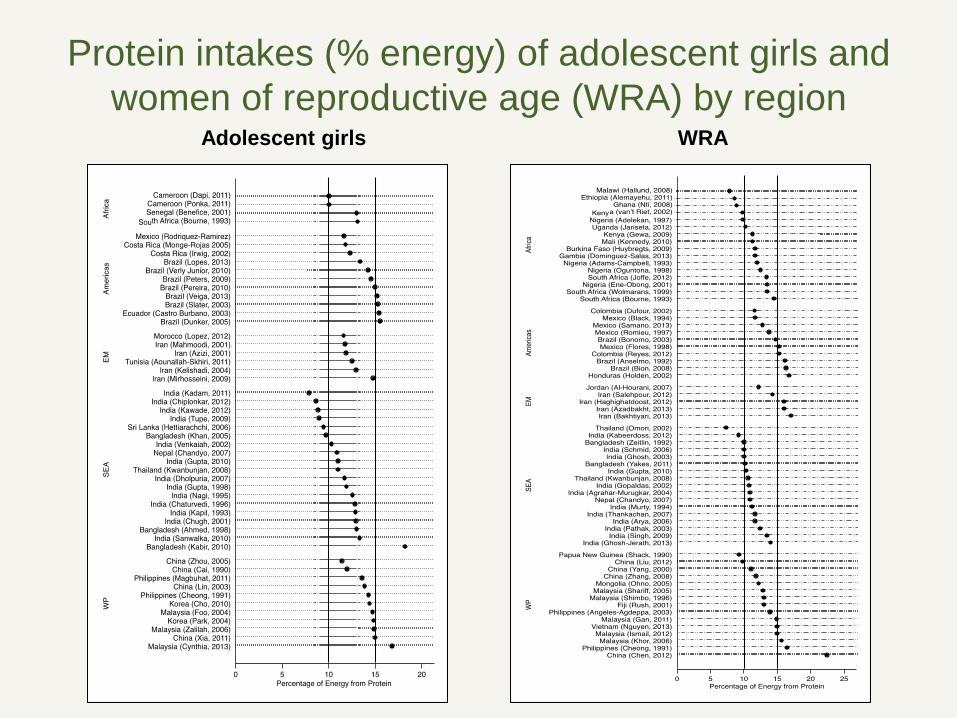
Protein intakes (% energy) of adolescent girls and women of reproductive age (WRA) by region
Adolescent girls WRA
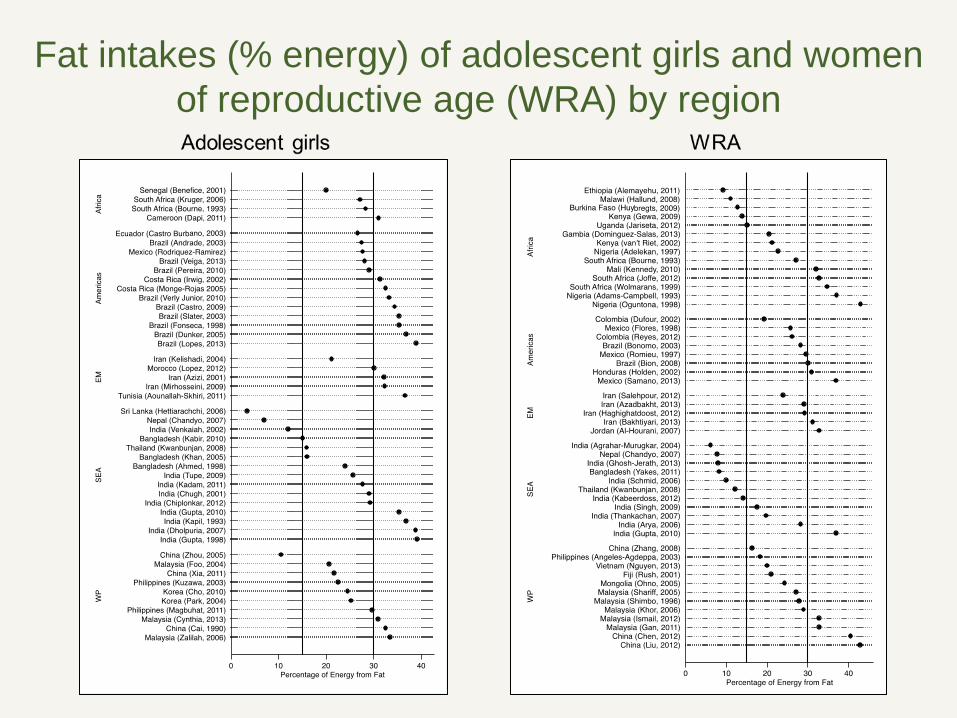
Fat intakes (% energy) of adolescent girls and women of reproductive age (WRA) by region
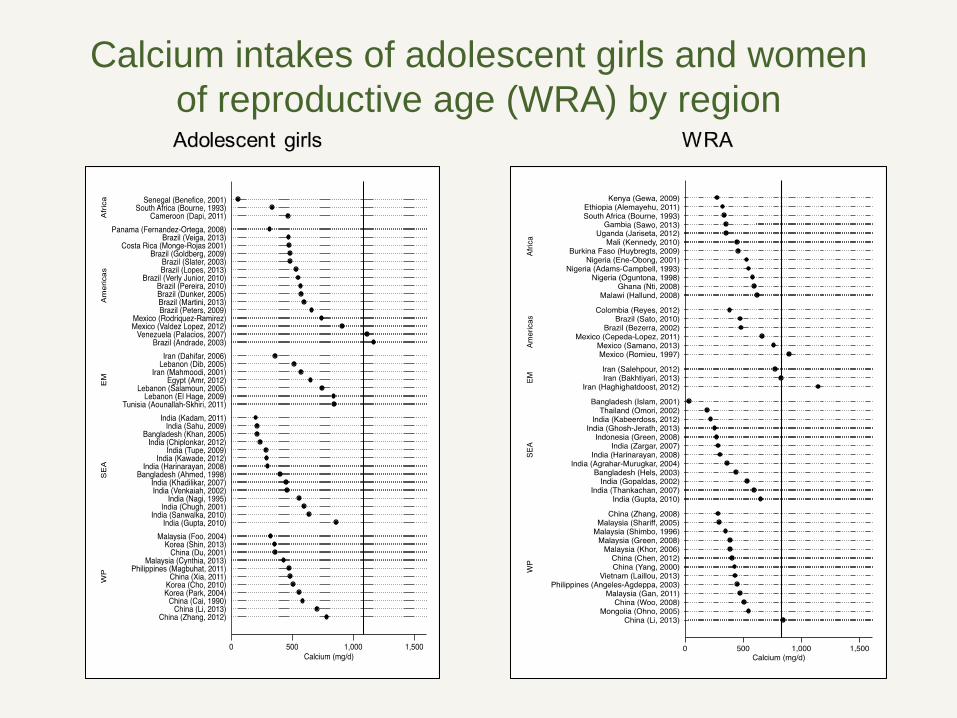
Calcium intakes of adolescent girls and women of reproductive age (WRA) by region
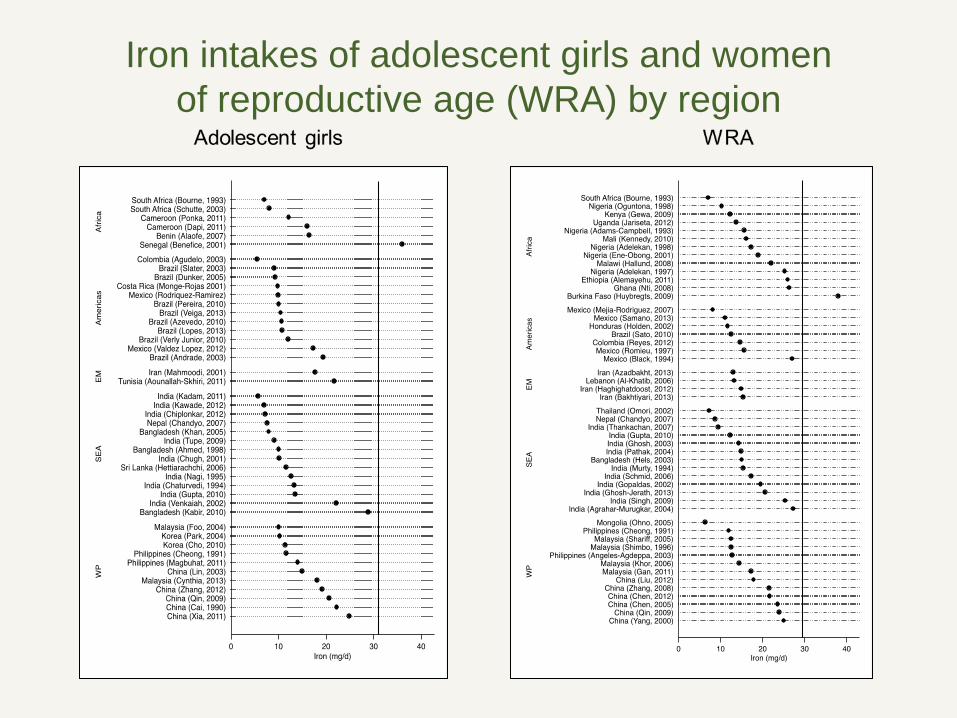
Iron intakes of adolescent girls and women of reproductive age (WRA) by region
Some Key Findings • Reducing short maternal stature requires continued
improvements in nutrition lifecycle of girls. • Key nutrition interventions include support for
maternal nutrition during pregnancy and lactation, IYCF and development of healthy eating patterns.
• Nutritional interventions during later childhood
and/or adolescence need study (efficacious?). • Family planning to delay age at first pregnancy
likely contributes to improving maternal stature.
Key Findings (cont.)
• The nutritional status of WRA has shifted over time, with some reductions in the prevalence of underweight, and shifts from normal weight to overweight/obesity.
• The problem of underweight
at the national level is less 10% in all areas except for some parts of Sub-Saharan Africa, and South Asia.
Key Findings (cont.)
• The problem of under-weight among adolescent girls, particularly those 15-19 is less well characterized, but appears to be consistent with those of women 20+, except in South Asia where it may be as high as 40%.
• In South Asia, there is urgent need to address the problem of underweight among girls and women.
Key Findings (cont.)
• When examined by age, overweight and obesity increased among women 20-30, suggesting postpartum weight retention as an explanatory factor
• There is a need to characterize
BMI status for local programming; in most areas the goal of having normal BMI means weight loss rather than weight gain.
Key Findings (cont.)
• Postpartum weight management is needed.
• Progress has been achieved in reducing maternal deficiencies of vitamin A and iodine, as well as anemia, but the problems remain.
• Inadequate zinc intake in LMIC appears significant.
• Folic acid fortification coverage is not optimal
Key Findings (cont.)
• Average nutrient intakes are inadequate in LMIC across regions and target groups. Importantly, adolescent girls, WRA and pregnant and lactating women do not face dietary concerns distinct from one another in terms of imbalanced macronutrient intakes, and inadequate micronutrient intakes
• More studies are needed and a comprehensive
strategy for nutrition during lactation is needed • Improvements in nutrient intake need to be placed
within the context of overall weight management.
Key Findings (cont.)
• Promotion of nutrient dense foods or foods providing key nutrients within the context of weight maintenance or loss (shift in consumption) is different from promotion of greater food intake (of the same or greater nutrient density) within the context of increasing BMI to normal.
• The relative effectiveness of interventions to reduce
“unhealthy foods” (e.g., sugar-sweetened beverage) consumption and/or increase consumption of “healthy foods” requires research in LMIC.
Goals for Diet and Eating Practices
Achieve normal weight • Low maternal BMI is a widely accepted risk factor for poor
pregnancy outcomes • For underweight women, it sets up a recommendation for
higher gestational weight gains that may not be achievable • Entering pregnancy overweight/obese increases the
likelihood of complications, including fetal demise • For overweight women, gestational gain and postpartum
weight retention contribute to obesity Maintain or improve diet quality as a lifestyle goal • Adequate intakes of calcium, iron, vitamin C, vitamin A, folic
acid, whole grains, vegetables and fruits, reduce alcohol intake
Goals for Diet and Eating Practices (cont.)
Maintain or improve physical activity level/active lifestyle • Important since physical activity tends to decline during
pregnancy, and starting new physical activity is not recommended)
Other • Prevent/treat anemia and achieve adequate iron stores • Maintain sufficient iodine intake to avoid thyroid disorders • Maintain sufficient vitamin A intake to maintain retinol
concentrations; • Ensure folic acid intake of 400 ug/d
Some Gaps in Evidence
• In places where you have women of low BMI (South Asia, West/Central/East Africa), what is the evidence around the efficacy of interventions to increase BMI on women entering pregnancy with low BMI?
• “Eating down” during pregnancy to avoid a large baby – is the practice less common than the concept?
• Catch-up growth in adolescence – what is the contribution of animal source foods?
• What is the efficacy of dietary guidelines - do they actually change behaviors?
• Can the balance within meals and the timing of meals avoid spikes in blood sugar levels, macronutrient and caloric intake
• What are the determinants of dietary behavior? • What is the impact of marketing of products to adolescents?
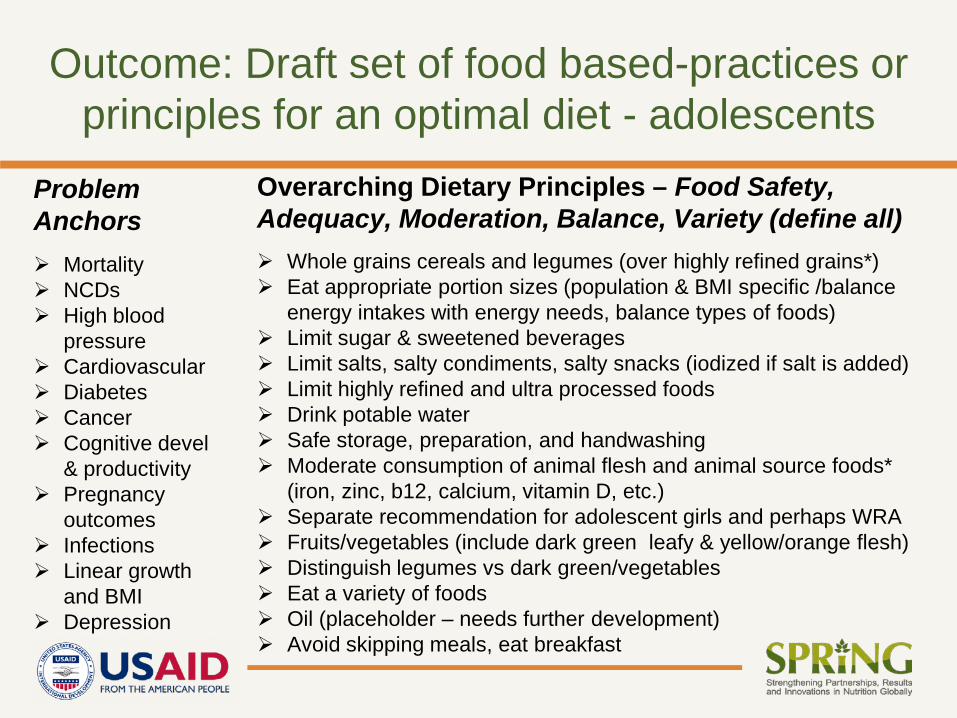
Outcome: Draft set of food based-practices or principles for an optimal diet - adolescents
Whole grains cereals and legumes (over highly refined grains*) Eat appropriate portion sizes (population & BMI specific /balance
energy intakes with energy needs, balance types of foods) Limit sugar & sweetened beverages Limit salts, salty condiments, salty snacks (iodized if salt is added) Limit highly refined and ultra processed foods Drink potable water Safe storage, preparation, and handwashing Moderate consumption of animal flesh and animal source foods*
(iron, zinc, b12, calcium, vitamin D, etc.) Separate recommendation for adolescent girls and perhaps WRA Fruits/vegetables (include dark green leafy & yellow/orange flesh) Distinguish legumes vs dark green/vegetables Eat a variety of foods Oil (placeholder – needs further development) Avoid skipping meals, eat breakfast
Overarching Dietary Principles – Food Safety, Adequacy, Moderation, Balance, Variety (define all)
Problem Anchors Mortality NCDs High blood
pressure Cardiovascular Diabetes Cancer Cognitive devel
& productivity Pregnancy
outcomes Infections Linear growth
and BMI Depression
Next steps
• Finalize meeting report, with proposed way forward (next steps) in establishing food based-principles/practices for an optimal diet. Circulate.
• Finalize 2 background papers (copyright issues and incorporate feedback). Circulate. Publish /present.
• Finalize the set(s) of draft principles/practices for an optimal diet for adolescent girls and WRA.
• Circulate food-based principles/practices for review by participants and other stakeholders.
• Conduct additional systematic reviews (if/as needed).
• Move through agreed upon mechanism……
www.spring-nutrition.org/events
For more information on the technical meeting (background materials and presentations), please visit: