acute ischaemic stroke - s2 keperawatans2keperawatan.fk.ub.ac.id/wp-content/uploads/2014/... ·...
TRANSCRIPT
Acute Ischaemic
Stroke
Hospital Kuala Lumpur Acute
Ischaemic Stroke Thrombolysis
Initiatives (HASTE)
Dr Mahathar Abd Wahab,
MBChB, M Med (Emerg. Med), Cert ML
Consultant Emergency Physician
Emergency and Trauma Department,
Hospital Kuala Lumpur

Stroke Epidemiology
3rd most common cause of death in developed countries, exceeded only by coronary heart disease and cancer
In Malaysia, top five leading causes of death with 8.43 per 100,000 population (MOH 2009)
795,000 new or recurrent strokes occur per year in the US, accounting for approximately 1 in 18 deaths
The prevalence of stroke in the US is about 7 million (3.0%) at an estimated cost in 2010 of 73.7 billion US-$
In Europe, the incidence of stroke varies from 101.1 to 239.3 per 100,000 in men and 63.0 to 158.7 per 100,000 in women
The estimated cost of stroke in Europe in 2010 was approx. € 64.1 billion
In China, the prevalence of stroke ranges between 1.8% (rural areas) and 9.4% (urban areas)
Worldwide, China has one of the highest rates of mortality (19.9% of all deaths in China), along with Africa and parts of South America
Gustavsson et al. Eur Neurpsychopharmacol 2011;21:718-779.
AHA and Stroke Statistics Writing Group. Circulation 2010;123:e1-e192.
EROS Investigators. Stroke 2009;40:1557-1563.
Sousa et al. Lancet 2009;374:1821-1830. The Atlas of heart disease and stroke, WHO 2004.

Ischaemic stroke
88%
Stroke Types and Incidence
Albers et al. Chest 2004;126 (3 Suppl):438S-512S.
Thom et al. American Heart Association. Circulation 2006;113:e85-e151.
HaemorrhagicOther
5%
Cryptogenic30%
Cardiacembolism
20%
Small vesseldisease
“lacunes”25%
Atheroscleroticcerebrovascular
disease20%
12%

Stroke : Definition
Clinical syndrome characterized by;
rapidly deteriorating symptoms and/or signs of
focal, at times, global loss of cerebral function,
with symptoms lasting > 24 hours or leading to
death,
with no apparent cause other than that of
vascular origin

Pathophysiology
Stroke is an Emergency

Potential to Reverse Neurologic Impairment With
Thrombolytic Reperfusion
Saver. Stroke 2006;37:263-266.
González. Am J Neuroradiol 2006;27:728-735.
Donnan. Lancet Neurol 2002;1:417-425.
An untreated patient loses
approximately 1.9 million
neurons every minute in
the ischaemic area
Reperfusion offers the
potential to reduce the
extent of ischaemic injury
Ischaemic core
(brain tissue
destined to die)
Penumbra
(salvageable
brain area)

“Time is Brain!”
Saver. Stroke 2006;37:263-266.
Estimated Pace of Neural Circuitry Loss In Typical Large-Vessel
Supratentorial Acute Ischaemic Stroke
Neurons Lost Synapses Lost Myelinated Fibres Lost Accelerated Aging
Per Stroke 1.2 billion 8.3 trillion 7140 km 36 y
Per Hour 120 million 830 billion 714 km 3.6 y
Per Minute 1.9 million 14 billion 12 km 3.1 wk
Per Second 32,000 230 million 200 m 8.7 h
Minutes Hours Days
Inflammation
Peri-infarct
depolarisations
Excitotoxicity
Impact
Apoptosis
Time

Guidelines
AHA
(The American Heart Association)www.americanheart.org
ESO
(The European Stroke Organisation)www.eso-stroke.org

AHA/ASA Guidelines
Recommendations on Emergency Systems
Suspected acute stroke – be identified rapidly by dispatch centres, which should dispatch the highest level of care available in the shortest possible time
EMS should briefly assess the patient on site (Class I, LOE B)
EMS should begin initial stroke management in the field (Class I, LOE B)
Patients should be transported rapidly for evaluation and treatment to the closest stroke facility (Class I, LOE B) and the EMS should inform the ED prior to arrival
Telemedicine can be an effective method to provide expert stroke care to patients located in rural areas (Class IIA, LOE B)
Pre-hospital providers, emergency physicians, and stroke experts should collaborate to develop training, assessment and transportation protocols
Acker et al. Stroke 2007;38:3097-3115.
Adams et al. Stroke 2007;38:1655-1711.EMS, emergency medical services
ED, emergency department

AHA/ASA Guidelines
Recommendations on Stroke Centres
Creation of primary stroke centres is strongly
recommended (Class I, LOE B)
Development of comprehensive stroke centres is
recommended (Class I, LOE C)
Certification of stroke centres by an external body
(e.g. JCAHO) is encouraged (Class I, LOE B)
Patients with suspected stroke should bypass
hospitals without stroke resources and go to the
closest facility capable of treating acute stroke (Class I, LOE B)
Adams et al. Stroke 2007;38:1655-1711.JCAHO, Joint Commission on the
Accreditation of Healthcare Organisations

AHA Guidelines for Cardiopulmonary Resuscitation and
Emergency CV Care
Several studies a higher likelihood of good to excellent functional outcome when rt-PA is administered to adult patients with acute ischaemic stroke within 3 hours of symptom onset
Treatment of carefully selected patients with acute ischaemic stroke with IV rt-PA between 3 and 4.5 hours after onset of symptoms has also been shown to improve clinical outcome, although the degree of clinical benefit is smaller than that achieved with treatment within 3 hours
Administration of IV rt-PA to patients with acute ischaemicstroke who meet the NINDS or ECASS 3 eligibility criteria is recommended if rt-PA is administered by physicians in the setting of a clearly defined protocol, a knowledgeable team, and institutional commitment(Class I, LOE B)
Jauch et al. Circulation 2010;122(suppl.3):S818-S828.

ESO Guidelines for the Management of Ischaemic
Stroke and Transient Ischaemic Attack
In patients admitted within 3 hours of stroke onset brain CT should be obtained to guide routine thrombolysis treatment with rt-PA (Class I, Level A)
I.V. rt-PA (0.9 mg/kg body weight, max. 90 mg), with 10% of the dose given as a bolus followed by a 60-minute infusion, is recommended within 4.5 hours of onset of ischaemic stroke (Class I, Level A)
The use of multimodal imaging may be useful for patient selection for thrombolysis but is not recommended for routine clinical practice (Class III, Level C)
ESO Guidelines 2009 Update. www.eso-stroke.org

ESO Guidelines: Recommendations for
Stroke Services and Stroke Units
All stroke patients should be treated in a stroke unit (Class I,
Level A)
Acute stroke patients should have access to high technology
medical and surgical stroke care when required (Class III,
Level B)
The development of clinical networks, including
telemedicine, is recommended to expand access to high
technology specialist stroke care (Class II, Level B)
ESO Guidelines 2009 Update. www.eso-stroke.org

Acute Ischemic Stroke - Issues
Public awareness
Delay in seeking treatment
Institutional commitment
Collaboration and multidisciplinary agreement
Financial implications
Longer hospital stays

The Initiatives
Hospital Kuala Lumpur, Kuala Lumpur, Malaysia

Raising Public Awareness
Campaigns
Target the general public as stroke witnesses
Symptom awareness
Awareness to take action
Keep the message easy
The ultimate aim is to keep the time to treatment as short as possible
Public awareness campaigns can increase ambulance dispatches for stroke
Example of a German stroke
awareness campaign

Raising Public Awareness

Acute Ischemic Stroke Thrombolysis Initiative
Multidiscipline approach
Emergency Medicine
Neurology
Neurosurgery
Radiology and Neuroradiology
Pharmacy
To achieve common goals

Development of
Critical Pathways
HASTE

CRITICAL PATHWAY(HKL – HASTE)

MECC acute stroke patients - identified rapidly by dispatch centres, which should dispatch the highest level of care available in the shortest possible time

Critical Pathway
TIME SITE ACTIVITY PERSONNEL OUTCOME
0 MECC 1. Receive Emergency Call
From Public.
2. History :
a. Facial asymmetry ,
b. Arm drift,
c. Slurred speech,
d. Time of Onset
Call Taker Time <3hrs

MECC Call Card

MECC Call Card

DISPATCH

Critical Pathway
TIME SITE ACTIVITY PERSONNEL OUTCOME
5-30
mins
Dispatc
h/
Incident
Site
1. Scene Safety & Primary
Survey
2. Perform Cincinnati Pre
Hospital Stroke Scale: Facial
asymmetry , Arm drift,
Slurred speech, Time of
Onset
3. Prompt Transport To HKL.
4. Enroute:
a. PERFORM PRIMARY
SURVEY
b. Protect airway,
c. Assist Ventilation,
d. Oxygen Supplement if
needed
e. Monitoring & Head
elevated 15o.
PPP /SN Response
Time <
20mins
P2

Cincinnati Stroke Scale: A Checklist for Emergency
Medical Dispatchers
Govindarajan et al. BMC Neurology 2011;11:14.
Total score:
3 Clear evidence of stroke
2 Strong evidence of stroke
1 Partial evidence of stroke
0 No evidence of stroke
3-Question Checklist Score
1. Ask patient to smile
Normal 0
Slight difference 1
Obvious difference 3
Cannot complete at all
2. Ask patient to raise both arms above head
Both arms raise equally 0
One arm higher than the other 1
Cannot complete request at all
3. Ask patient to say “the early bird catches the worm”
Said correctly 0
Slurred speech 3
Garbled or not understood 3
Cannot complete request at all

Critical Pathway
TIME SITE ACTIVITY PERSONNEL OUTCOME
15 -30
mins
Dispatch 5. Specific Assessment:
a. Age,
b. Time of onset,
c. GCS,
d. History of bedridden or
wheelchair bound,
e. history of seizure,
f. blood glucose,
g. name/ phone no of
person who can give
consent.
6. Radio in
7. Communication
• MECC to Resus
• Patient Arrival
Preparation
• Facilitate Early CT
PPP / SN Response
Time <
20mins
P2

TRIAGE COUNTER

Critical Pathway
TIME SITE ACTIVITY PERSONNEL OUTCOME
30-35
mins
Triage
Counter
1. History :
a. Facial asymmetry ,
b. Arm drift,
c. Slurred speech,
d. Time of Onset
2. FIRST LOOK Assessment
1. Ambulating
2. Wheel Chair Bound
3. Trolley Bound
3. Three Bells
4. Transfer patient to RESUS
if time of onset <3hrs.
PPP / SN
Triage
Time onset
<3hrs

RESUS


Critical Pathway – ED MO
TIME SITE ACTIVITY PERSONNEL OUTCOME
35
min –
4.5
hours
RESUS 1. Primary Survey & stabilize
the patient.
2. Activate Stroke Team.
3. Acute Stroke Code Flow
Chart / Checklist
4. History : Ascertain time of
onset & symptoms.
5. Indications &
contraindications for
thrombolysis
6. Focal neurological signs
evidence.
7. Modified Rankin Score
8. Arrange & perform CT Brain.
MO ED
incharge of
Resus
Door to CT <
45mins

Critical Pathway – ETD MO
TIME SITE ACTIVITY PERSONNE
L
OUTCOME
<4.5
hrs
RESUS
1. Weigh The Patient
2. Venous access (at least
16G) at cubital fossa
1. Investigations (Mark
the Ix form:
Emergent Acute
Stroke
Thrombolysis) :
2. DXT stat,
3. ECG,
4. Blood Test: FBC ,
RP, COAG, LFT,
BSH,
5. CT Brain
3. Interpret CT Scan
MO ED
incharge of
Resus
SN/PPP
Emergency
Physician/
Neurologist/Ra
diologist
Door to CT <
45mins

Patient Weight

Patient Weight
Before calibration

Patient Weight
After calibration

Critical Pathway – Radiology
TIME SITE ACTIVITY PERSONNEL OUTCOME
RESUS
(cont.)
1. Prepare machine &
perform the CT Brain
2. Radiologist to interpret CT
3. ASPECT score
4. Inform result to MO
Neurology/ED MO.
Radiology Door to CT
<45 mins

Critical Pathway – Neuro Medical
TIME SITE ACTIVITY PERSONNEL OUTCOME
RESUS
(cont.)
1. Determine the severity of
deficit using the NIHSS
2. Thrombolysis if indicated
and no absolute
contraindication.
3. 0.9mg/kg not to exceed a
max of 90mg. 10% to be
given IV bolus over 1 – 2
mins & remaining 90% to
be given over 60 mins.
4. Keep patient NBM for 24
hours.
MO
Neuromedical
/Neurologist
Door to
Needle (DTN)
<60 mins

Critical Pathway – Resus SN
TIME SITE ACTIVITY PERSONNEL OUTCOME
RESUS
(cont.)
1. Drug Preparation and
Dilution
2. Patient Monitoring:
a. Monitor
BP/PR/RR/SpO2
a. Every 15mins
during infusion &
b. then 30mins for
the next 2hrs.
c. Thereafter every
hour for the next
24hrs.
b. GCS monitoring every
15mins during infusion.
SN Resus /
Neuro SN
Complete
Monitoring as
per indicated

Critical Pathway
TIME SITE ACTIVITY PERSONNEL OUTCOME
<5hrs Acute
Stroke
Ward/IC
U
1. Admit patient to ward
1. Transfer Checklist
2. Patient Monitoring
PPP/SN/PPK Checklist
before
Transfer
complete

Critical Pathway
Acute Stroke
Summary


Thank You

Other Reference
1. Special Thanks to Prof Ismail Saiboon and Assoc. Prof Dr Mohd
Idzwan Zakaria for sharing the stroke protocols from their institutions
2. UMMC – Guidelines for Thrombolysis od Acute Ischemic Stroke Patient
3. tPA Patient Information's Sheet – Boston Medical Centre
4. Acute Stroke Pathway for ED – PPUKM
5. ED PPUKM Pre hospital Stroke Guidelines
6. Use of ASPECT in Acute Ischemic Stroke
7. Acute Iscahemic Stroke Thrrombolysis Protocol – Hospital Kuala
Lumpur

Actilyse®
Product Details

Actilyse®
Actilyse®, rt-PA, is a serine protease, similar to naturally occurring tissue plasminogen activator (t-PA)
Mode of action
With high affinity, Actilyse® binds to and activates plasminogen attached to the fibrin netting of a blood clot
Plasminogen is converted to plasmin, which catalyses the breakdown of fibrin to its degradation products, resulting in break up of the clot
The affinity for freely circulating plasminogen is low, so Actilyse® has highly effective local fibrinolytic effects and relatively few systemic effects
Hoylaerts et al. J Biol Chem1982;257:2912-2919.

Impressum
Published by
Boehringer Ingelheim GmbH
www.actilyse.com
Realisation
infill healthcare communication
www.infill.com
Supported by
Professors Peter Schellinger & Patrick Goldstein

Indications for IV rt-PA
Diagnosis of ischaemic stroke comfirmed clinically.
Time of ischaemic stroke less than 4.5hrs from onset
of stroke.
Consent obtained from patient/guardian.
Measurable and clinically significant deficit on NIHSS
scale examination (6-22)
CT brain scan does not show hemorrhage or non
vascular cause of stroke.
Patient‟s age >18 years, <80 years.Back

Absolute contra indications for IV rt-PA
Time of onset unknown or „ wake up‟ stroke.
Coma or severe obtundation with fixed eye deviation
and complete dense hemiplegia.
Only minor stroke deficit which appears to be rapidly
improving.
Seizure observed or known to have occurred at onset
of stroke.
Hypertension with systolic ≥ 180mmHg or diastolic
>110mmHg on repeated measurements.

Absolute contra indications for IV rt-PA -
cont
Clinical presentation suggestive of SAH even if CT
Brain scan is normal.
Presumed septic embolus.
Patient has received heparin within the last 48 hours
and has elevated PTT or has a known hereditary or
acquired haemorrhagic diathesis (PT or APTT greater
than normal)
INR > 1.7
Platlet count < 100 000/ul
Serum glucose < 2.8 mmol or >22 mmol/l

Relative contraindications for IV rt-PA -
Severe neurological impairment with NIHSS>22?
Age > 80 years.
CT Brain evidence of extensive MCA territory
infarction greater than 1/3 of MCA territory.
Stroke or serious head injury within the past 3 month
where the risk of bleeding outweight the benefit of
therapy.
Major surgery within the last 14 days.
Suspected recent (within 30 days) myocardial
infarction

Relative contraindications for IV rt-PA -
Patient has known history of ICB , SAH, known
intracranial AVM or previously known intracranial
neoplasm such that, in the opinion of the clinician, the
increased risk of intracranial bleeding would outweigh
the potential benefits of treatment.
Recent (within 30 days) biopsy of a parenchymal
organ or surgery that, in the opinion of the
responsible clinician, would increase the risk of
unmanageable bleeding.
Recent (within 30 days) trauma with internal injuries
or ulcerative wounds.

Relative contraindications for IV rt-PA -
GI or GU haemorrhage within the last 30 days or any
active or recent haemorrhage that, in the opinion of
the responsible clinician, would increase the risk of
unmanageable bleeding.
Arterial puncture at non compressible site within the
last 7 days.
Concomitant serious, advanced or terminal illness or
any other condition that in the opinion of the
responsible clinician would pose a risk to treatment
Back

Back
ACUTE ISCHEMIC STROKE
FLOW CHART / CHECK LIST

Back

Back

Total dose : 0.9mg/kg(<100mg)First dose:
10%of total dose given bolus over 10 minute.
Second dose :The remaining dose infused over 1
hour.Do not mix the drug with other drugs(dedicated IV line)
Dose & Administration

Step 1 : Bawa preskripsi wad ke Farmasi
Kecemasan.Sila pastikan dos ubat ditulisdan pastikan Doktor Pakar neurologiyang endorse ubat.
Example:IV Actilyse 7mg bolus over 1 minute followed by 63mg infusion over 1 hour
(Sila pastikan pegawai farmasi di kecemasan menulis dos ubat sekiranya dos tidak ditulis doktor) Berat pesakit diperlukan.Ingat!!
How to prepare the drug?
Step 2 : Confirm bolus dose and infusion
dose with Neurologist
How to prepare the drug?

Step 3 : Reconstitute using the solvent provided.
Use the transfer cannula provided. Only reconstitute after a written
prescription is done. After reconstitution, concentration is 1mg/ml.
Do not shake the vial. Just swirl it. Let solution to stand for a few minutes to clear large
bubbles Please take note that patient might need 2 vial..
How to prepare the drug?

Step 4 :Use 10ml syringe for withdrawing bolus dose.Eg : 7mg bolus stat. Jadi syringe out 7 ml.
Step 5 : Label Nama Ubat dan DosEg : IV Actilyse 7 mg(7ml)
Remember : bolus dose will be administered by the Dr for 1 minute.
How to prepare the drug?

Step 6 : Use 10ml syringe for withdrawing
10% of total dose ( bolus dose.)
Eg : 7mg bolus stat. Jadi syringe out 7 ml.
How to prepare the drug?

Step 7 : Use 1 or 2 50ml syringe for withdrawing
the dose for infusion.(Do NOT syringe out All the balance!)Cth: Jika Total dose :63mg(63ml)=2 vialDose bolus :6.3mg(6.3ml)Dose Infusion:63ml-6.3ml=56.7ml
The balance:
Disposed in sharp bin!!
How to prepare the drug?

Please label the infusion correctly
Eg. Label :• Concentration/dose on each syringe Nama ubat Masa start infusion Cth: 56.7ml continuos infusion 1 hour Syringe 1 :IV Actilyse 50mg Start:7am at 56.7ml/hr Syringe 2 :IV Actilyse 6.7 mg Start:? at 56.7ml/hr
How to prepare the drug?
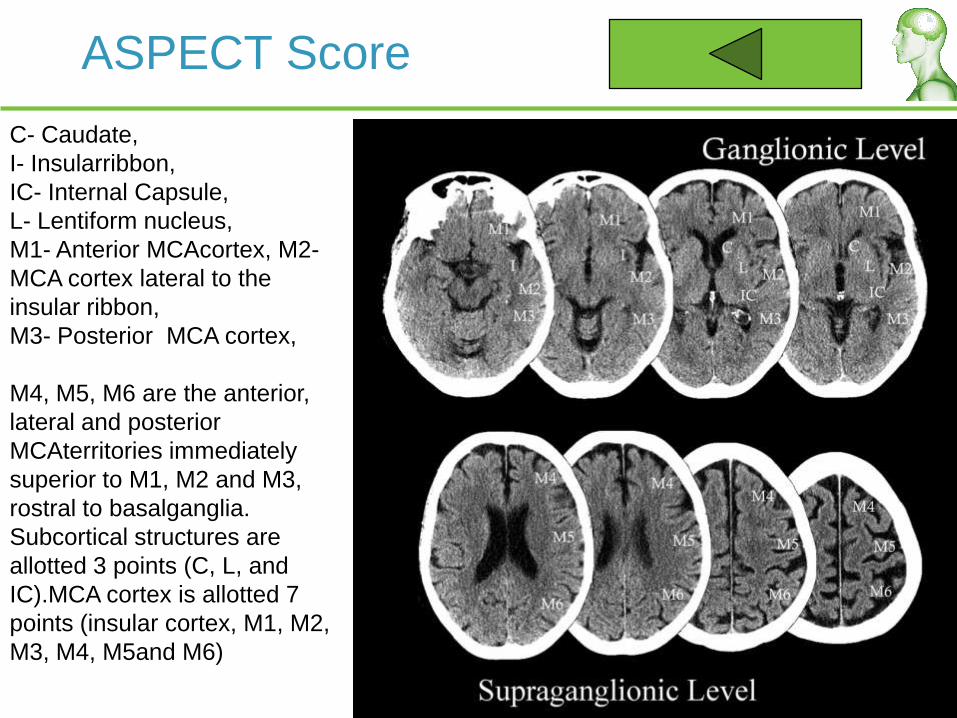
ASPECT Score
C- Caudate,
I- Insularribbon,
IC- Internal Capsule,
L- Lentiform nucleus,
M1- Anterior MCAcortex, M2-
MCA cortex lateral to the
insular ribbon,
M3- Posterior MCA cortex,
M4, M5, M6 are the anterior,
lateral and posterior
MCAterritories immediately
superior to M1, M2 and M3,
rostral to basalganglia.
Subcortical structures are
allotted 3 points (C, L, and
IC).MCA cortex is allotted 7
points (insular cortex, M1, M2,
M3, M4, M5and M6)