actividad fisica
DESCRIPTION
actividad fisicaTRANSCRIPT
edicine and Rehabilitation
Archives of Physical M journal homepage: www.archives-pmr.orgArchives of Physical Medicine and Rehabilitation 2015;-:-------
ORIGINAL RESEARCH
Promoting Physical Activity Through a ManualWheelchair Propulsion Intervention in Persons WithMultiple Sclerosis
Ian M. Rice, PhD, Laura A. Rice, PhD, Robert W. Motl, PhD
From the Department of Kinesiology and Community Health, University of Illinois at Urbana-Champaign, Urbana, IL.
Abstract
Objective: To examine the efficacy and feasibility of a multifactorial intervention to increase lifestyle physical activity in nonambulatory persons
with multiple sclerosis (MS) based on wheelchair optimization, propulsion skill/technique training, and behavioral strategies based on social
cognitive theory.
Design: Randomized controlled trial, 3-month postintervention follow-up.
Setting: Home and general community, and university research laboratory.
Participants: Nonambulatory individuals with MS (NZ14; mean age � SD, 53.6�8.7y) were randomly assigned to an intervention group (IG) or
a control group (CG).
Interventions: After baseline testing, the IG participants received custom-fit, ultralightweight manual wheelchairs with propulsion/skills
training, followed by 3 months of at-home use with the custom ultralightweight wheelchair and weekly phone calls to deliver support through a
multifactorial intervention. The CG participants received no training and used their own wheelchairs at home during this time.
Main Outcome Measures: All subjects were assessed at baseline and 3 months later for fatigue (Fatigue Severity Scale), upper extremity strength
(digital handheld dynamometer), and propulsion technique (on a treadmill [0.5m/s] with instrumented wheels). Two 1-week bouts of physical
activity were measured in both groups from home with wrist-worn accelerometry at the beginning (IG and CG in own wheelchairs) and end (IG in
study wheelchair, CG in own) of the 3-month period of home use.
Results: The intervention was well tolerated, and no adverse events were reported. The IG demonstrated increased strength (PZ.008) and a trend
toward less fatigue (PZ.068), both with large effect sizes (d>0.8), as well as reduced application of braking torque during propulsion (PZ.003)
with a moderate/large effect size (dZ.73), compared with the CG.
Conclusions: Findings suggest a 3-month physical activity intervention based on manual wheelchair propulsion and training is safe and feasible
for some wheelchair users living with MS and may produce secondary benefits in strength, fatigue, and propulsion technique.
Archives of Physical Medicine and Rehabilitation 2015;-:-------
ª 2015 by the American Congress of Rehabilitation Medicine
There is increasing evidence regarding the importance of physicalactivity (PA) among persons with multiple sclerosis (MS).1 PA isdefined as bodily movement produced by contraction of skeletalmuscles that results in increased energy expenditure,2 and can beaccumulated as part of one’s everyday life.3 This lifestyle PA can bemeasured objectively using body-worn accelerometers,4 and hasbeen associated with subclinical and self-reported cardiovascularhealth,5,6 walking mobility,7 information processing speed,8
Supported by the National Multiple Sclerosis Society, Illinois Department of Public Health,
Office of Health Promotion, Division of Chronic Disease Prevention and Control (grant no. IL
0005).
Disclosures: none.
0003-9993/15/$36 - see front matter ª 2015 by the American Congress of Re
http://dx.doi.org/10.1016/j.apmr.2015.06.011
symptoms of fatigue,9 depression, pain,10,11 and quality of life12
in MS. PA further can be transformed through multifactorial in-terventions that provide participants with the necessary resources,skills, and strategies for successful health behavior change. To date,such interventions have been delivered using the Internet,10 tele-phone,13 and pamphlets,14 and successfully increased PAwith sec-ondary benefits for symptoms. However, these interventions haveonly been delivered among ambulatory personswithMS, and little isknown regarding their feasibility, safety, and efficacy when used forincreased PA among mobility device users with severe MS.3
Despite the documented benefits of PA, many persons livingwith MS are physically inactive and sedentary, and this is
habilitation Medicine

2 I.M. Rice et al
particularly salient among nonambulatory individuals. Forexample, both worsening symptoms and increased levels ofdisability have been associated with reduced PA.15,16 Additionally,those using mobility devices often find unique challenges toaccessing safe and effective methods of exercise.
Consequently we wondered whether delivering a multifactorialintervention based on manual wheelchair propulsion (MWP) fornonambulatory persons with MS could be successful if the propertechnology and training were provided. MWP was selected overformal exercise training to determine the extent to which it affordsindividuals the flexibility to choose the time, duration, and envi-ronment in which activity occurs, along with offering those whoexperience fatigue the convenience of combining exercise andcommunity participation.
This randomized, controlled pilot study examined the efficacyand feasibility of the intervention among nonambulatory personswith MS. We hypothesized that the intervention group (IG) wouldtolerate MWP with few adverse events and increase PA levelsbased on wrist accelerometer vector counts. We further hypothe-sized secondary benefits in propulsion technique, upper limbstrength, and fatigue in the IG compared with a control group (CG).
Methods
Participants
Participants were recruited through the North American ResearchCommittee on MS, phone calls to previous research participants,and local MS Society events. Twenty participants were thenscreened over the telephone for the following inclusion criteria:(1) diagnosis of MS (later confirmed by participants’ physicians);(2) full-time wheelchair user (use of power or manual for >40h/wk and >80% ambulation); (3) aged 18 to 64 years; (4) stablehealth status for the past 3 months; and (5) bilateral gross upperextremity strength of at least 4-/5 (acquired later at University ofIllinois at Urbana-Champaign labs). Exclusion criteria were asfollows: (1) wheelchair athletes; (2) orthopedic upper extremityimpairment; (3) self-reported history of cardiovascular or cardio-pulmonary disease; and (4) pressure ulcers. Of those initial 20interested participants, 6 were excluded (3 did not use a wheel-chair full time, and 3 were unable to travel).
Study design/procedures
OverviewThe local institutional review board approved all experimentation.Participants were randomly assigned to either an IG or a CG on a2:1 ratio to best characterize the IG, but still have data on teststability and administration from the CG (fig 1). Participants (IGand CG) visited the university labs 2 times, for baseline (visit 1)and posttesting (visit 2) (fig 2).
List of abbreviations:
CG control group
FSS Fatigue Severity Scale
IG intervention group
MS multiple sclerosis
MWP manual wheelchair propulsion
PA physical activity
RESNA Rehabilitation Engineering Society of North America
Intervention groupDuring visit 1, IG participants were examined for upper limbstrength and fatigue. Next they received seating evaluations toconfigure the study wheelchair (ICON A1 wheelchaira) to meettheir needs. Next, baseline propulsion biomechanics were recor-ded followed by technique/safety training. The IG participantswere then given the ICON for 3 months of home use andencouraged to incorporate it into their daily lives. Example ac-tivities were provided to help them achieve this endeavor. Duringhome use, wrist-worn accelerometers were sent through the mailto record two 1-week bouts of PA at the beginning and end of the3-month period (see fig 2). Bout 1 consisted of activity using theirprimary mobility device(s) (not the ICON), while bout 2 recordedactivity with the ICON. Finally, IG participants returned to the lab3 months after visit 1 for follow-up testing identical to baseline.
Study wheelchairThe ICON A1 wheelchair is a rigid, ultralightweight, aluminum-framed manual wheelchair meeting Rehabilitation EngineeringSociety of North America (RESNA)/American National StandardsInstitute voluntary standards. This chair was selected because itoffered the flexibility to meet the standards set forth by RESNA ina position paper17 on the application of ultralight manual wheel-chairs. These standards include durability, adjustability, custom-ization, and the ability to meet the specific mobility and posturalneeds of the intended user. The ICON is fully adjustable (eg,width, length, footrest height, seat/back angle, center of gravity,back height) and weighs <25lb with rear suspension (fig 3A andB). All ICON wheelchairs had 25-in quick release rear wheelswith pneumatic tires and 4-in-diameter front caster wheels. Anexternal contoured aluminum back supportb was attached foradded postural support, and Varilite seat cushionsc were provided.
TrainingSafety and technique training were provided to IG participants byan occupational therapist and a licensed physical therapist with anAssistive Technology Professional certification. An instructionalmultimedia presentation used previously was presented as well.18
The multimedia presentation guidelines are consistent with therecommendations published by the Consortium for Spinal CordMedicine to prevent upper limb pain and injury.19 Manualwheelchair users are encouraged to use low-frequency, long andsmooth strokes (large contact angle) during the propulsive phaseto decrease the force exerted at a given velocity.19 Additionally,subjects are encouraged to match the speed of the handrim oncontact to minimize braking torques that slow the wheel.
Behavioral interventionBased on social cognitive theory,20 the behavioral interventionwas delivered through weekly phone calls by a physical therapistto IG participants, during which strategies for initiation andmaintaining PA with the ICON were taught. Such strategiesincluded self-monitoring, goal setting, planning, optimizingoutcome expectations, enhancing self-efficacy, overcoming bar-riers, and identifying facilitators.
Wheelchair data logger manipulation checkOnly the IG members’ ICON wheelchairs were equipped withdata loggers to ascertain the 3 months of home use. Additionally,the data logger allowed researchers to determine whether wristaccelerometer vector counts accumulated during the second1-week period of home use resulted from ICON use or their own
www.archives-pmr.org
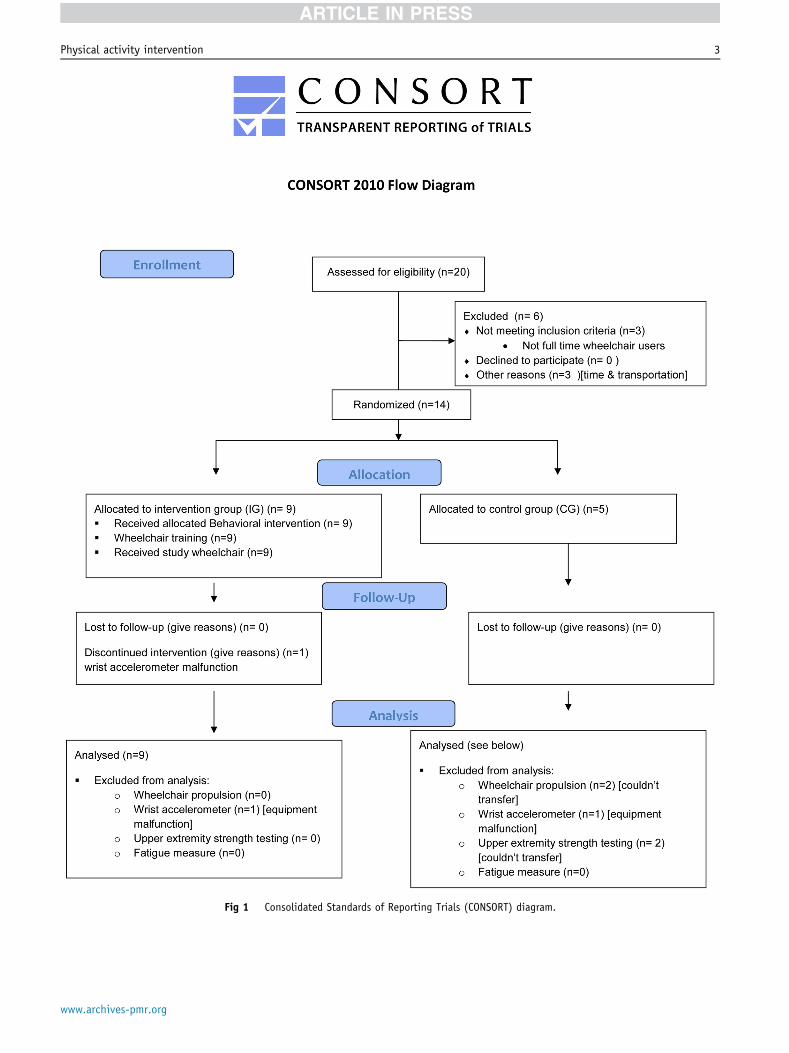
Fig 1 Consolidated Standards of Reporting Trials (CONSORT) diagram.
Physical activity intervention 3
www.archives-pmr.org
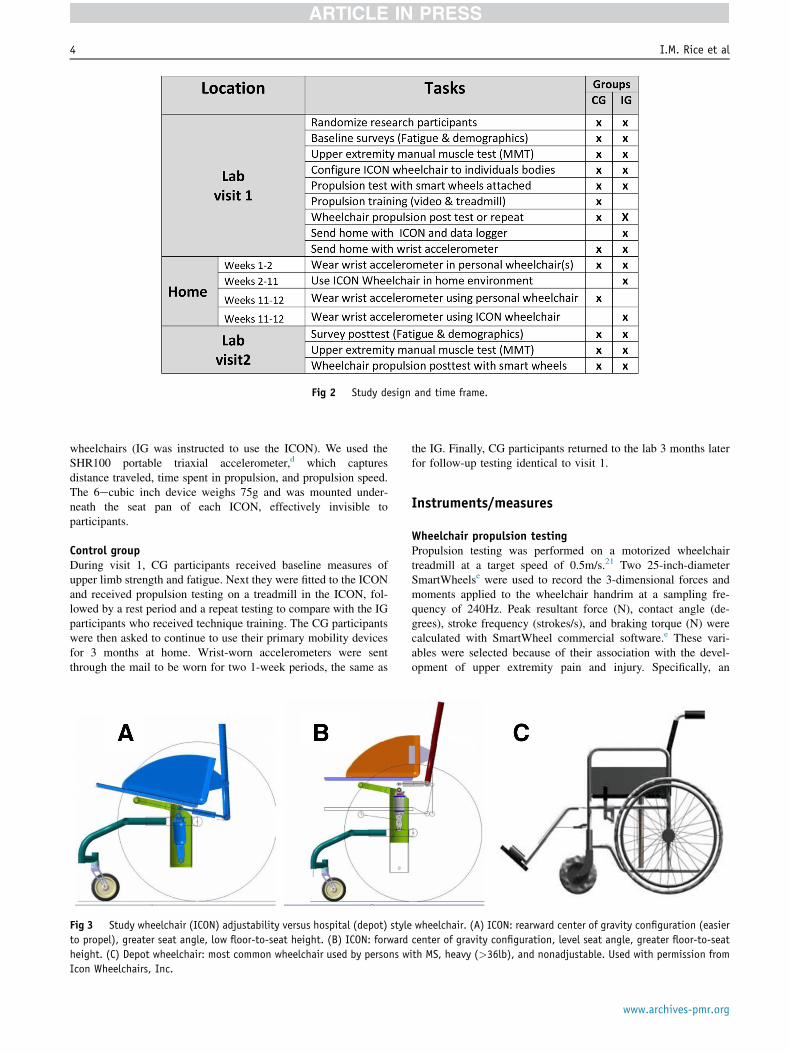
Fig 2 Study design and time frame.
4 I.M. Rice et al
wheelchairs (IG was instructed to use the ICON). We used theSHR100 portable triaxial accelerometer,d which capturesdistance traveled, time spent in propulsion, and propulsion speed.The 6ecubic inch device weighs 75g and was mounted under-neath the seat pan of each ICON, effectively invisible toparticipants.
Control groupDuring visit 1, CG participants received baseline measures ofupper limb strength and fatigue. Next they were fitted to the ICONand received propulsion testing on a treadmill in the ICON, fol-lowed by a rest period and a repeat testing to compare with the IGparticipants who received technique training. The CG participantswere then asked to continue to use their primary mobility devicesfor 3 months at home. Wrist-worn accelerometers were sentthrough the mail to be worn for two 1-week periods, the same as
Fig 3 Study wheelchair (ICON) adjustability versus hospital (depot) style
to propel), greater seat angle, low floor-to-seat height. (B) ICON: forward
height. (C) Depot wheelchair: most common wheelchair used by persons w
Icon Wheelchairs, Inc.
the IG. Finally, CG participants returned to the lab 3 months laterfor follow-up testing identical to visit 1.
Instruments/measures
Wheelchair propulsion testingPropulsion testing was performed on a motorized wheelchairtreadmill at a target speed of 0.5m/s.21 Two 25-inch-diameterSmartWheelse were used to record the 3-dimensional forces andmoments applied to the wheelchair handrim at a sampling fre-quency of 240Hz. Peak resultant force (N), contact angle (de-grees), stroke frequency (strokes/s), and braking torque (N) werecalculated with SmartWheel commercial software.e These vari-ables were selected because of their association with the devel-opment of upper extremity pain and injury. Specifically, an
wheelchair. (A) ICON: rearward center of gravity configuration (easier
center of gravity configuration, level seat angle, greater floor-to-seat
ith MS, heavy (>36lb), and nonadjustable. Used with permission from
www.archives-pmr.org
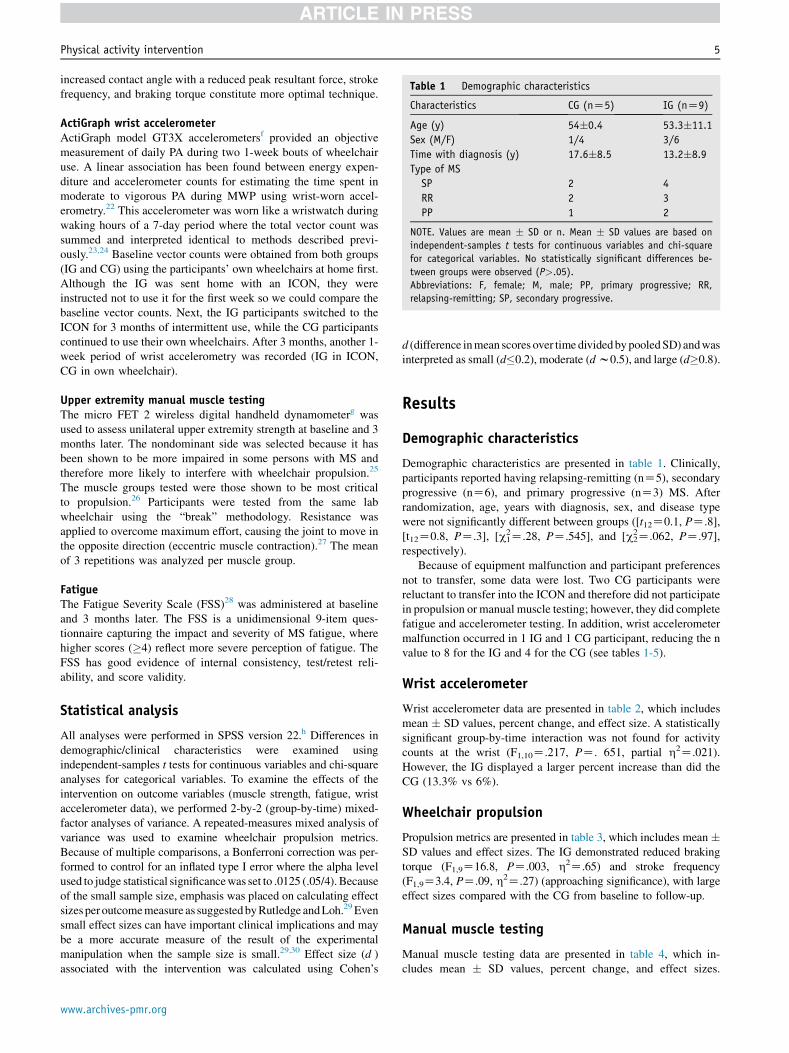
Table 1 Demographic characteristics
Characteristics CG (nZ5) IG (nZ9)
Age (y) 54�0.4 53.3�11.1
Sex (M/F) 1/4 3/6
Time with diagnosis (y) 17.6�8.5 13.2�8.9
Type of MS
SP 2 4
RR 2 3
PP 1 2
NOTE. Values are mean � SD or n. Mean � SD values are based on
independent-samples t tests for continuous variables and chi-square
for categorical variables. No statistically significant differences be-
tween groups were observed (P>.05).
Abbreviations: F, female; M, male; PP, primary progressive; RR,
relapsing-remitting; SP, secondary progressive.
Physical activity intervention 5
increased contact angle with a reduced peak resultant force, strokefrequency, and braking torque constitute more optimal technique.
ActiGraph wrist accelerometerActiGraph model GT3X accelerometersf provided an objectivemeasurement of daily PA during two 1-week bouts of wheelchairuse. A linear association has been found between energy expen-diture and accelerometer counts for estimating the time spent inmoderate to vigorous PA during MWP using wrist-worn accel-erometry.22 This accelerometer was worn like a wristwatch duringwaking hours of a 7-day period where the total vector count wassummed and interpreted identical to methods described previ-ously.23,24 Baseline vector counts were obtained from both groups(IG and CG) using the participants’ own wheelchairs at home first.Although the IG was sent home with an ICON, they wereinstructed not to use it for the first week so we could compare thebaseline vector counts. Next, the IG participants switched to theICON for 3 months of intermittent use, while the CG participantscontinued to use their own wheelchairs. After 3 months, another 1-week period of wrist accelerometry was recorded (IG in ICON,CG in own wheelchair).
Upper extremity manual muscle testingThe micro FET 2 wireless digital handheld dynamometerg wasused to assess unilateral upper extremity strength at baseline and 3months later. The nondominant side was selected because it hasbeen shown to be more impaired in some persons with MS andtherefore more likely to interfere with wheelchair propulsion.25
The muscle groups tested were those shown to be most criticalto propulsion.26 Participants were tested from the same labwheelchair using the “break” methodology. Resistance wasapplied to overcome maximum effort, causing the joint to move inthe opposite direction (eccentric muscle contraction).27 The meanof 3 repetitions was analyzed per muscle group.
FatigueThe Fatigue Severity Scale (FSS)28 was administered at baselineand 3 months later. The FSS is a unidimensional 9-item ques-tionnaire capturing the impact and severity of MS fatigue, wherehigher scores (�4) reflect more severe perception of fatigue. TheFSS has good evidence of internal consistency, test/retest reli-ability, and score validity.
Statistical analysis
All analyses were performed in SPSS version 22.h Differences indemographic/clinical characteristics were examined usingindependent-samples t tests for continuous variables and chi-squareanalyses for categorical variables. To examine the effects of theintervention on outcome variables (muscle strength, fatigue, wristaccelerometer data), we performed 2-by-2 (group-by-time) mixed-factor analyses of variance. A repeated-measures mixed analysis ofvariance was used to examine wheelchair propulsion metrics.Because of multiple comparisons, a Bonferroni correction was per-formed to control for an inflated type I error where the alpha levelused to judge statistical significancewas set to .0125 (.05/4). Becauseof the small sample size, emphasis was placed on calculating effectsizesperoutcomemeasure as suggestedbyRutledge andLoh.29Evensmall effect sizes can have important clinical implications and maybe a more accurate measure of the result of the experimentalmanipulation when the sample size is small.29,30 Effect size (d )associated with the intervention was calculated using Cohen’s
www.archives-pmr.org
d (difference inmean scores over timedividedbypooledSD) andwasinterpreted as small (d�0.2), moderate (dw0.5), and large (d�0.8).
Results
Demographic characteristics
Demographic characteristics are presented in table 1. Clinically,participants reported having relapsing-remitting (nZ5), secondaryprogressive (nZ6), and primary progressive (nZ3) MS. Afterrandomization, age, years with diagnosis, sex, and disease typewere not significantly different between groups ([t12Z0.1, PZ.8],[t12Z0.8, PZ.3], [c2
1Z.28, PZ.545], and [c22Z.062, PZ.97],
respectively).Because of equipment malfunction and participant preferences
not to transfer, some data were lost. Two CG participants werereluctant to transfer into the ICON and therefore did not participatein propulsion or manual muscle testing; however, they did completefatigue and accelerometer testing. In addition, wrist accelerometermalfunction occurred in 1 IG and 1 CG participant, reducing the nvalue to 8 for the IG and 4 for the CG (see tables 1-5).
Wrist accelerometer
Wrist accelerometer data are presented in table 2, which includesmean � SD values, percent change, and effect size. A statisticallysignificant group-by-time interaction was not found for activitycounts at the wrist (F1,10Z.217, PZ. 651, partial h2Z.021).However, the IG displayed a larger percent increase than did theCG (13.3% vs 6%).
Wheelchair propulsion
Propulsion metrics are presented in table 3, which includes mean �SD values and effect sizes. The IG demonstrated reduced brakingtorque (F1,9Z16.8, PZ.003, h2Z.65) and stroke frequency(F1,9Z3.4, PZ.09, h2Z.27) (approaching significance), with largeeffect sizes compared with the CG from baseline to follow-up.
Manual muscle testing
Manual muscle testing data are presented in table 4, which in-cludes mean � SD values, percent change, and effect sizes.

Table 2 Activity counts with wrist accelerometer
Group Baseline 3mo % Change Cohen’s d* Effect Size
CG (nZ4) 923,499.3�475,384.4 979,454.1�639,999.5 6.0[ .14 Approaching small
IG (nZ8) 980,428.9�547,676.5 1,111,080.1�510,500.4 13.3[
NOTE. Values are mean � SD or as otherwise indicated. The wrist accelerometer used was an ActiGraph model GT3X accelerometer.
Abbreviation: [, increase.* Cohen’s d calculated mean change/pooled SD at baseline (range: 0.2 small, 0.5 moderate, 0.8 large).
6 I.M. Rice et al
Statistically significant group-by-time interactions were observedfor the pectoralis major (F1,10Z11.0, PZ.008, partial h2Z.526),while strength gains approaching significance occurred at themiddle deltoid (F1,10Z3.68, PZ.084, partial h2Z.26).
Fatigue
FSS results are presented in table 5. There was a group-by-timeinteraction for fatigue that approached statistical significancewith a large effect size (F1,12Z4.0, PZ.068, partial h2Z.25).
Wheelchair data logger manipulation check
Wheelchair data logger results are presented in figure 4. Data arebased on 7 IG members because 2 devices malfunctioned.Figure 4 represents the group averages (bars) and individualweekly distance traveled (lines) at 1-, 2-, and 3-month time points.Month 1 corresponds to the first month of ICON use in the IG. Thedata suggest that the wheelchairs were generally used, but withconsiderable variability. Based on group averages, participantswere most active the first month, which declined in month 2 andincreased slightly in month 3.
Safety/feasibility
IG participants were asked to describe their experience with theICON wheelchairs, and no adverse events were reported. IGmembers reported that the ICON wheelchairs were lightweightand comfortable, made mobility easier, and enabled them toachieve and maintain speed. However, those performing standingpivot transfers reported that the fixed footplate interfered withstanding. Swing-away footrests were their preference. Those whoperformed sitting pivot transfers were unaffected. In addition,some found the nonfolding frame and antitippers interfered withcar transport, making them less willing to travel. Also, some re-ported difficulties managing the hideaway locking brakes.
Table 3 Wheelchair propulsion biomechanics
Performance Variables
CG (nZ3)
Baseline 3mo Ba
Peak resultant force (N) 37.7�10.4 54.6�11.2 46
Contact angle (deg) 32.4�1.3 38.9�6.8 43
Frequency (strokes/s) 1.0�0.1 1.0�0.1 0
Braking force (N) �7.3�3.3 �8.1�3.4 �5
NOTE. Values are mean � SD or as otherwise indicated. Mean � SD values a
speed condition 0.5m/s.
* P<.09.y P<.0125.
Discussion
The purpose of this study was to evaluate the feasibility, safety, andefficacy of a multifactorial lifestyle PA intervention for personswith severe MS.We believe this to be the first experimental attemptto examine an intervention for increased PA in this population.Despite the preliminary nature of the study, intervention outcomeswere encouraging and may offer insights into the design of methodsto improve PA in a population where research is scarce.
The current study design did not allow for the determination ofwhich interventional component (optimization, training, behavioralintervention) led to improvements, only the system’s influence as awhole, which is a limitation. However, as a preliminary study,safety was a primary concern, where providing an extremelyresponsive wheelchair to novice users without training/support inorder to separate the influence of the behavioral intervention or theICON was deemed unnecessarily risky. Instead, our goal was todeliver a balanced approach offering IG subjects more supportiveconditions compared with a CG receiving the standard of care. Itwas our intention to learn from participants’ reactions to improvethe study design for future, sufficiently powered investigations.
Consistent with our hypothesis, the intervention was well toler-ated and no adverse events occurred. Additionally, moderate to largeeffects sizes were observed, signifying favorable changes in aspectsof propulsion technique, upper extremity strength, and trends towardreduced fatigue. Because fatigue has been cited as a primary factorprecluding individuals with MS from propulsion,31 this trend wasencouraging. Although strength measures should be interpretedcautiously, the strength increase observed in the pectoralis majormay be of interest because it has been identified as both a primarycontributor to propulsion and as a muscle specifically shown to fa-tigue in some wheelchair users with MS during propulsion.32
Fundamental to our intervention was use of a custom-fit,ultralightweight high-performance wheelchair, intended tomaximize ease of propulsion. Consistent with RESNA’s recom-mendations, each ICON was customized to participants’ needswhile preserving its lightweight.17 Our IG participants learned to
IG (nZ9)
Cohen’s d Effect Sizeseline 3mo
.1�20.0 45.8�12.9 1.04 Large
.9�16.3 46.2�15.1 0.36 Small/moderate
.8�0.1* 0.79�0.2* 0.1 Small
.6�1.9y �2.9�1.1y 0.73 Moderate/large
re based on repeated-measures multivariate analysis of variance. Target
www.archives-pmr.org
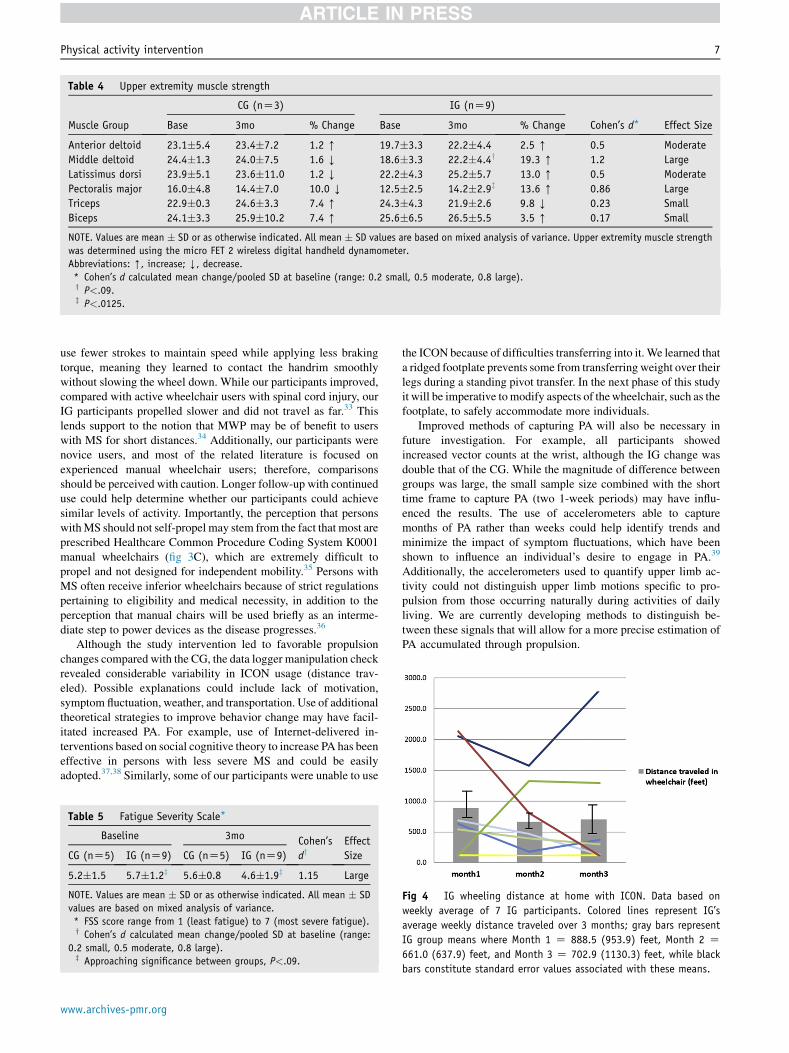
Table 4 Upper extremity muscle strength
Muscle Group
CG (nZ3) IG (nZ9)
Cohen’s d* Effect SizeBase 3mo % Change Base 3mo % Change
Anterior deltoid 23.1�5.4 23.4�7.2 1.2 [ 19.7�3.3 22.2�4.4 2.5 [ 0.5 Moderate
Middle deltoid 24.4�1.3 24.0�7.5 1.6 Y 18.6�3.3 22.2�4.4y 19.3 [ 1.2 Large
Latissimus dorsi 23.9�5.1 23.6�11.0 1.2 Y 22.2�4.3 25.2�5.7 13.0 [ 0.5 Moderate
Pectoralis major 16.0�4.8 14.4�7.0 10.0 Y 12.5�2.5 14.2�2.9z 13.6 [ 0.86 Large
Triceps 22.9�0.3 24.6�3.3 7.4 [ 24.3�4.3 21.9�2.6 9.8 Y 0.23 Small
Biceps 24.1�3.3 25.9�10.2 7.4 [ 25.6�6.5 26.5�5.5 3.5 [ 0.17 Small
NOTE. Values are mean � SD or as otherwise indicated. All mean � SD values are based on mixed analysis of variance. Upper extremity muscle strength
was determined using the micro FET 2 wireless digital handheld dynamometer.
Abbreviations: [, increase; Y, decrease.* Cohen’s d calculated mean change/pooled SD at baseline (range: 0.2 small, 0.5 moderate, 0.8 large).y P<.09.z P<.0125.
Physical activity intervention 7
use fewer strokes to maintain speed while applying less brakingtorque, meaning they learned to contact the handrim smoothlywithout slowing the wheel down. While our participants improved,compared with active wheelchair users with spinal cord injury, ourIG participants propelled slower and did not travel as far.33 Thislends support to the notion that MWP may be of benefit to userswith MS for short distances.34 Additionally, our participants werenovice users, and most of the related literature is focused onexperienced manual wheelchair users; therefore, comparisonsshould be perceived with caution. Longer follow-up with continueduse could help determine whether our participants could achievesimilar levels of activity. Importantly, the perception that personswithMS should not self-propel may stem from the fact that most areprescribed Healthcare Common Procedure Coding System K0001manual wheelchairs (fig 3C), which are extremely difficult topropel and not designed for independent mobility.35 Persons withMS often receive inferior wheelchairs because of strict regulationspertaining to eligibility and medical necessity, in addition to theperception that manual chairs will be used briefly as an interme-diate step to power devices as the disease progresses.36
Although the study intervention led to favorable propulsionchanges compared with the CG, the data logger manipulation checkrevealed considerable variability in ICON usage (distance trav-eled). Possible explanations could include lack of motivation,symptom fluctuation, weather, and transportation. Use of additionaltheoretical strategies to improve behavior change may have facil-itated increased PA. For example, use of Internet-delivered in-terventions based on social cognitive theory to increase PA has beeneffective in persons with less severe MS and could be easilyadopted.37,38 Similarly, some of our participants were unable to use
Table 5 Fatigue Severity Scale*
Baseline 3mo Cohen’s
dyEffect
SizeCG (nZ5) IG (nZ9) CG (nZ5) IG (nZ9)
5.2�1.5 5.7�1.2z 5.6�0.8 4.6�1.9z 1.15 Large
NOTE. Values are mean � SD or as otherwise indicated. All mean � SD
values are based on mixed analysis of variance.
* FSS score range from 1 (least fatigue) to 7 (most severe fatigue).y Cohen’s d calculated mean change/pooled SD at baseline (range:
0.2 small, 0.5 moderate, 0.8 large).z Approaching significance between groups, P<.09.
www.archives-pmr.org
the ICON because of difficulties transferring into it. We learned thata ridged footplate prevents some from transferring weight over theirlegs during a standing pivot transfer. In the next phase of this studyit will be imperative tomodify aspects of thewheelchair, such as thefootplate, to safely accommodate more individuals.
Improved methods of capturing PA will also be necessary infuture investigation. For example, all participants showedincreased vector counts at the wrist, although the IG change wasdouble that of the CG. While the magnitude of difference betweengroups was large, the small sample size combined with the shorttime frame to capture PA (two 1-week periods) may have influ-enced the results. The use of accelerometers able to capturemonths of PA rather than weeks could help identify trends andminimize the impact of symptom fluctuations, which have beenshown to influence an individual’s desire to engage in PA.39
Additionally, the accelerometers used to quantify upper limb ac-tivity could not distinguish upper limb motions specific to pro-pulsion from those occurring naturally during activities of dailyliving. We are currently developing methods to distinguish be-tween these signals that will allow for a more precise estimation ofPA accumulated through propulsion.
Fig 4 IG wheeling distance at home with ICON. Data based on
weekly average of 7 IG participants. Colored lines represent IG’s
average weekly distance traveled over 3 months; gray bars represent
IG group means where Month 1 Z 888.5 (953.9) feet, Month 2 Z661.0 (637.9) feet, and Month 3 Z 702.9 (1130.3) feet, while black
bars constitute standard error values associated with these means.

8 I.M. Rice et al
Study limitations
As the current pilot study was a first step, inherent limitationsexist. The primary limitation of the current study is evident in theuse of a small sample size to examine numerous outcome mea-sures. Because this was an early-phase study, the importance ofeffect sizes cannot be overstated. A multisite design or the abilityto test remotely may increase enrollment in future studies.Another limitation is evident in our lack of knowledge regardingparticipants’ usage of their own wheelchairs because only theICON wheelchairs were instrumented. We plan to monitor mul-tiple mobility devices in the future. Additionally, these results maynot generalize to all nonambulatory persons with MS because ourparticipants possessed a minimum level of upper limb strength.The extent to which others with less strength could benefit from asimilar intervention is unclear and warrants investigation. Inaddition, wheelchair propulsion measures were recorded at atarget speed during level treadmill propulsion that may notrepresent users’ technique in the community. Finally, datacollection occurred over 10 months in central Illinois where theweather may have influenced participants’ activity levelsdifferently.
Conclusions
Preliminary findings suggest that a PA intervention based onwheelchair optimization, training, and a behavioral intervention isfeasible for some individuals with MS and may produce sec-ondary benefits in strength, fatigue, and propulsion technique.Both groups increased PA levels, with the IG showing a largerpercent change; however, differences were not statisti-cally significant.
Suppliers
a. ICON A1 wheelchair; Icon Wheelchairs, Inc.b. External contoured aluminum back support; Accessible De-
signs, Inc.c. Varilite seat cushions; Varilite.d. SHR100 portable triaxial accelerometer; Autonomous
Innovations.e. SmartWheels; Out-Front.f. ActiGraph model GT3X accelerometer; Actigraph Corp.g. Micro FET 2 wireless digital handheld dynamometer; HOG-
GAN Scientific, LLC.h. SPSS version 22; SPSS Inc.
Keywords
Fatigue; Motor activity; Multiple sclerosis; Rehabilitation; Qualityof life; Wheelchairs
Corresponding author
Ian M. Rice, PhD, Department of Kinesiology and CommunityHealth, University of Illinois at Urbana-Champaign, 332 FreerHall, Urbana, IL 61801. E-mail address: [email protected].
References
1. Motl RW. Lifestyle physical activity in persons with multiple scle-
rosis: the new kid on the MS block. Mult Scler 2014;20:1025-9.
2. Bouchard C, Shephard RJ. Physical activity, fitness and health: the
model and key concepts. Champaign: Human Kinetics; 1994.
3. Dunn AL, Andersen RE, Jakicic JM. Lifestyle physical activity in-
terventions. History, short- and long-term effects, and recommenda-
tions. Am J Prev Med 1998;15:398-412.
4. Motl RW, Sandroff BM. Objective monitoring of physical activity
behavior in multiple sclerosis. Phys Ther Rev 2010;15:204-11.
5. Motl RW, Fernhall B, McAuley E, Cutter G. Physical activity and self-
reported cardiovascular comorbidities in persons with multiple scle-
rosis: evidence from a cross-sectional analysis. Neuroepidemiology
2011;36:83-191.
6. Ranadive SM, Yan H, Weikert M, et al. Vascular dysfunction and
physical activity in multiple sclerosis. Med Sci Sports Exerc 2012;44:
238-43.
7. Snook EM, Motl RW. Effect of exercise training on walking mobility
in multiple sclerosis: a meta-analysis. Neurorehabil Neural Repair
2009;23:108-16.
8. Sandroff BM, Pilutti LA, Dlugonski D, Motl RW. Physical activity and
information processing speed in persons with multiple sclerosis: a
prospective study. Ment Health Phys Act 2013;6:205-11.
9. Pilutti LA, Greenlee TA, Motl RW, Nickrent MS, Petruzzello SJ.
Effects of exercise training on fatigue in multiple sclerosis: a meta-
analysis. Psychosom Med 2013;75:575-80.
10. Pilutti LA, Dlugonski D, Sandroff BM, Klaren R, Motl RW. Ran-
domized controlled trial of a behavioral intervention targeting symp-
toms and physical activity in multiple sclerosis. Mult Scler 2014;20:
594-601.
11. Sandroff BM, Klaren RE, Pilutti LA, Dlugonski D, Benedict RH,
Motl RW. Randomized controlled trial of physical activity, cognition,
and walking in multiple sclerosis. J Neurol 2014;261:363-72.
12. Motl RW, Gosney JL. Effect of exercise training on quality of life in
multiple sclerosis: a meta-analysis. Mult Scler 2008;14:129-35.
13. Bombardier CH, Ehde DM, Gibbons LE, et al. Telephone-based
physical activity counseling for major depression in people with
multiple sclerosis. J Consult Clin Psychol 2013;81:89-99.
14. Plow M, Bethoux F, McDaniel C, McGlynn M, Marcus B. Random-
ized controlled pilot study of customized pamphlets to promote
physical activity and symptom self-management in women with
multiple sclerosis. Clin Rehabil 2014;28:139-48.
15. Motl RW, Arnett PA, Smith MM, Barwick FH, Ahlstrom B, Stover EJ.
Worsening of symptoms is associated with lower physical activity levels
in individuals with multiple sclerosis. Mult Scler 2008;14:140-2.
16. Marrie R, Horwitz R, Cutter G, Tyry T, Campagnolo D, Vollmer T.
High frequency of adverse health behaviors in multiple sclerosis. Mult
Scler 2009;15:105-13.
17. Rehabilitation Engineering and Assistive Technology Society of North
America. RESNA position on the application of ultralight manual
wheelchairs. Arlington; 2012.
18. Rice IM, Pohlig RT, Gallagher JD, Boninger ML. Handrim wheelchair
propulsion training effect on overground propulsion using biomechan-
ical real-time visual feedback. Arch PhysMedRehabil 2013;94:256-63.
19. Consortium for Spinal Cord Medicine. Preservation of upper limb
function following spinal cord injury: a clinical practice guideline for
health-care professionals. Washington (DC): Paralyzed Veterans of
America; 2005.
20. Bandura A. Health promotion by social cognitive means. Health Educ
Behav 2004;31:143-64.
21. Sonenblum SE, Sprigle S, Lopez RA. Manual wheelchair use: bouts of
mobility in everyday life. Rehabil Res Pract 2012;2012:753165.
22. Learmonth YC, Kinnett-Hopkins D, Rice IM, Dysterheft JL, Motl RW.
Accelerometer output and its association with energy expenditure
during manual wheelchair propulsion. Spinal Cord. 2015 Mar 17.
[Epub ahead of print]
www.archives-pmr.org
Physical activity intervention 9
23. Motl RW, McAuley E. Pathways between physical activity and quality
of life in adults with multiple sclerosis. Health Psychol 2009;28:682-9.
24. Motl RW, McAuley E, Snook EM, Gliottoni RC. Physical activity and
quality of life in multiple sclerosis: intermediary roles of disability,
fatigue, mood, pain, self-efficacy and social support. Psychol Health
Med 2009;14:111-24.
25. Lamers I, Kerkhofs L, Raats J, Kos D, Van Wijmeersch B, Feys P.
Perceived and actual arm performance in multiple sclerosis: rela-
tionship with clinical tests according to hand dominance. Mult Scler
2013;19:1341-8.
26. Schantz P, Bjorkman P, Sandberg M, Andersson E. Movement and
muscle activity pattern in wheelchair ambulation by persons with
para-and tetraplegia. Scand J Rehabil Med 1999;31:67-76.
27. Stratford PW, Balsor BE. A comparison of make and break tests using
a hand-held dynamometer and the Kin-Com. J Orthop Sports Phys
Ther 1994;19:28-32.
28. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The Fatigue
Severity Scale. Application to patients with multiple sclerosis and
systemic lupus erythematosus. Arch Neurol 1989;46:1121-3.
29. Rutledge T, Loh C. Effect sizes and statistical testing in the deter-
mination of clinical significance in behavioral medicine research. Ann
Behav Med 2004;27:138-45.
30. Cohen J. Statistical power analysis. CurrDir Psychol Sci 1992;1:98-101.
31. Fay BT, Boninger ML, Fitzgerald SG, Souza AL, Cooper RA,
Koontz AM. Manual wheelchair pushrim dynamics in people with
multiple sclerosis. Arch Phys Med Rehabil 2004;85:935-42.
www.archives-pmr.org
32. Fay B, Boninger ML, Ambrosio F, Cooper RA. Aspects of fatigue in
multiple sclerosis during manual wheelchair propulsion. In: Pro-
ceedings of the 25th Annual lnternational Conference of the IEEE
EMBS; September 17-21, 2003; Edmonton, Alberta, Canada.
33. Tolerico ML, Ding D, Cooper RA, et al. Assessing mobility charac-
teristics and activity levels of manual wheelchair users. J Rehabil Res
Dev 2007;44:561-71.
34. Verza R, Battaglia MA, Uccelli MM. Manual wheelchair propulsion
pattern use by people with multiple sclerosis. Disabil Rehabil Assist
Technol 2010;5:314-7.
35. Beekman CE, Miller-Porter L, Schoneberger M. Energy cost of pro-
pulsion in standard and ultralight wheelchairs in people with spinal
cord injuries. Phys Ther 1999;79:146-58.
36. Ambrosio F, Boninger ML, Fitzgerald SG, Hubbard SL, Schwid SR,
Cooper RA. Comparison of mobility device delivery within Depart-
ment of Veterans Affairs for individuals with multiple sclerosis versus
spinal cord injury. J Rehabil Res Dev 2007;44:693-701.
37. Dlugonski D, Motl RW, McAuley E. Increasing physical activity in
multiple sclerosis: replicating Internet intervention effects using
objective and self-report outcomes. J Rehabil Res Dev 2011;48:
1129-36.
38. Motl RW, Dlugonski D, Wojcicki TR, McAuley E, Mohr DC. Internet
intervention for increasing physical activity in persons with multiple
sclerosis. Mult Scler 2011;17:116-28.
39. Evers KJ, Karnilowicz W. Patient attitude as a function of disease state
in multiple sclerosis. Soc Sci Med 1996;43:1245-51.