act training 15 aug 2011 m sills edits
TRANSCRIPT

+
ACT TrainingSAFTINet Partner Engagement Community

+
ACT Training
SAFTINet Partner Engagement Community
Outline
1. Clinical Use of the Asthma Control Test (ACT)
2. Workflow for Using the ACT

+1. Clinical Use of the Asthma Control Test (ACT)A. BackgroundB. Guideline-based context for the ACTC. The ACT

+Asthma Epidemiology
Up to 18% diagnosed by high school graduation
More common in males before age 12 and in females after age 12
Over 3,900 deaths (14/day)
Disproportionately affectschildren and African Americans

+
2 million ED visits
500,000 hospitalizations
Costs of asthma $16 billion American Lung Association Fact Sheet: Asthma in Adults, June 2004. Available at: http://www.lungusa.org/site/.
National Institute of Allergy and Infectious Disease. Focus on Asthma. Available at: http://www3.niaid.nih.gov/news.American Medical Association. Clinical Performance Measures – Asthma, 2005.
Asthma-Related Annual Utilization

+NIH Guidelines
National Institutes of Health, National Heart, Lung and Blood Institute. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (EPR-3 2007).
Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm.
EPR-3

+Guidelines: Ambulatory Asthma Care
Diagnose asthma
Identify precipitating factors and co-morbidities
Classify asthma severity
Assess patient’s knowledge/skills for self-management
Provide an asthma action plan
Monitor asthma control
Administer influenza vaccine to all with asthma

+Guidelines: Ambulatory Asthma Care
Diagnose asthma
Identify precipitating factors and co-morbidities
Classify asthma severity
Assess patient’s knowledge/skills for self-management
Provide an asthma action plan
Monitor asthma control
Administer influenza vaccine to all with asthma
ACT helps here

+ Assessment/Monitoring: Control vs. Severity
Used for evaluating disease activity and initiating therapy
Categories: Intermittent Persistent (mild,
moderate, severe)
Is not what the ACT measures
Used for monitoring and adjusting therapy
ACT score can be used to measure part of control (impairment)
Severity Control

+Control
Includes two domains Impairment is the present: effects on quality of
life and functional capacity Risk refers to the future: exacerbations and
progressive loss of pulmonary function
Well controlled vs. not well controlled/very poorly controlled
Should be measured at least every 6 months
Use control rating to step up or step down therapy after assessing compliance, device technique and environment

+Assessing Control

+Assessing Control

+ Assessment of Control Using Standardized Tools: ACT (Asthma Control Test)
Simple assessment and easy-to-use scoring method
Assesses asthma control over the past 4 weeks: activity limitations daytime symptoms nighttime symptoms short-acting beta-agonist (SABA) use self-assessment of level of control
Available in >12 languages

+Childhood ACT
Child questions
Parent questions
Instructions
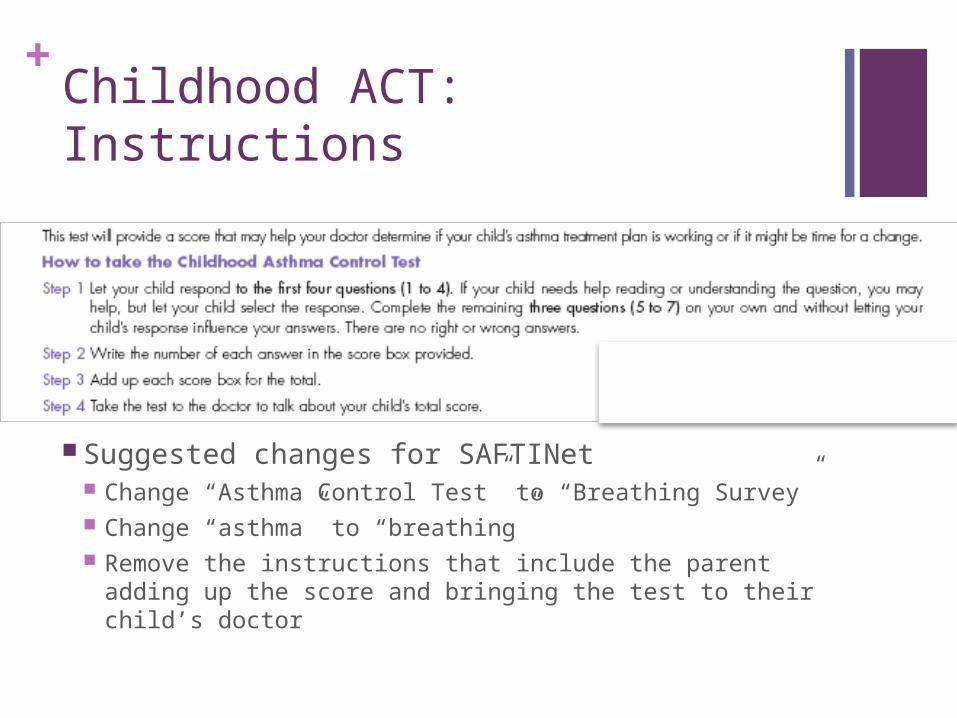
+Childhood ACT: Instructions
Suggested changes for SAFTINet Change “Asthma Control Test” to “Breathing Survey” Change “asthma” to “breathing” Remove the instructions that include the parent adding
up the score and bringing the test to their child’s doctor

+Childhood ACT: Child Questions

+Childhood ACT: Parent Questions

+ACT: Teen/Adult Version
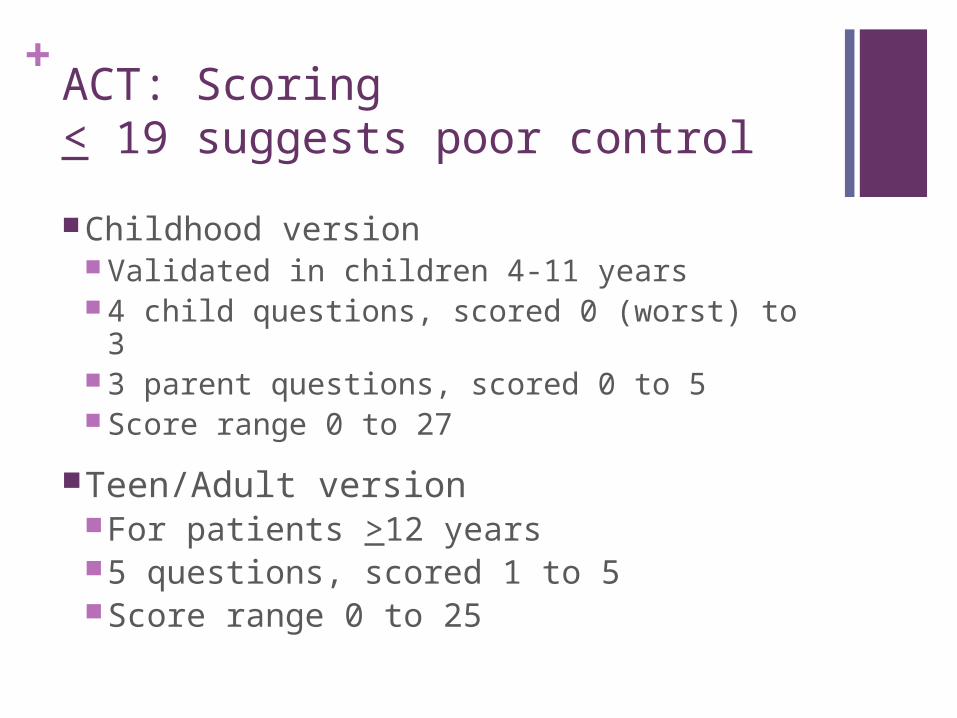
+ACT: Scoring< 19 suggests poor control
Childhood version Validated in children 4-11 years 4 child questions, scored 0 (worst) to 3 3 parent questions, scored 0 to 5 Score range 0 to 27
Teen/Adult versionFor patients >12 years5 questions, scored 1 to 5Score range 0 to 25

+Assessing Control and Adjusting Therapy in Teens and Adults
+Assessing Control and Adjusting Therapy in Children 5–11
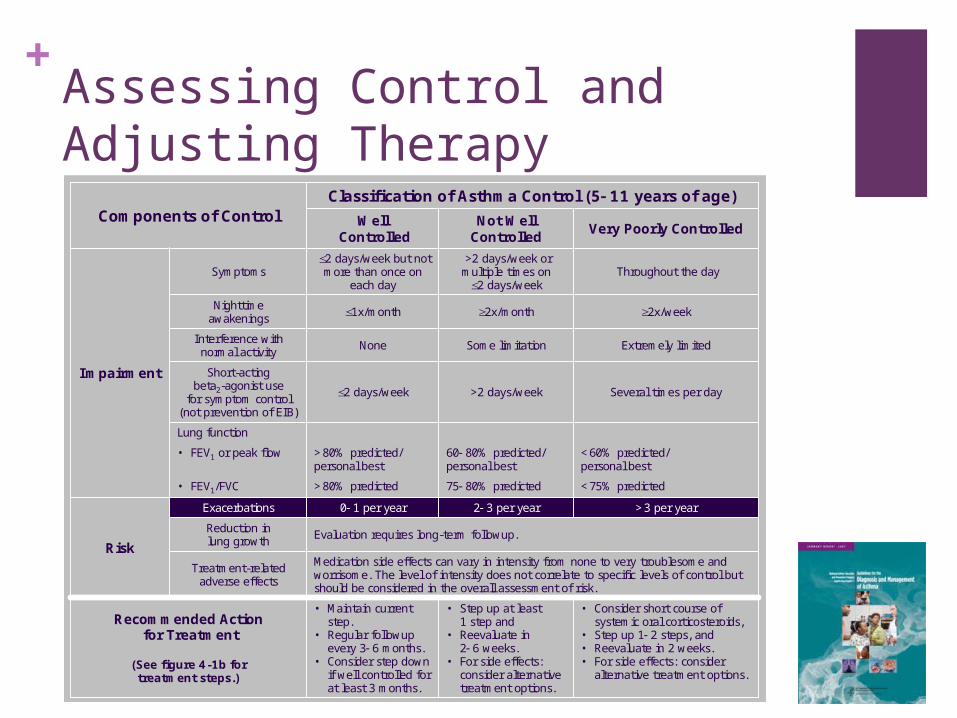
• Consider short course of systemic oral corticosteroids,
• Step up 1 2 steps, and• Reevaluate in 2 weeks.• For side effects: consider
alternative treatment options.
• Step up at least 1 step and
• Reevaluate in 2 6 weeks.
• For side effects: consider alternative treatment options.
• Maintain current step.
• Regular followupevery 3 6 months.
• Consider step down if well controlled for at least 3 months.
Recommended Actionfor Treatment
(See figure 4-1b fortreatment steps.)
Lung function
<60% predicted/personal best
60 80% predicted/personal best
>80% predicted/personal best
• FEV1 or peak flow
Evaluation requires long-term followup.
Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
Treatment-related adverse effects
>3 per year2 3 per year0 1 per yearExacerbations
Risk
Several times per day>2 days/week2 days/week
Short-actingbeta2-agonist use
for symptom control(not prevention of EIB)
Extremely limitedSome limitationNoneInterference with normal activity
Classification of Asthma Control (5 11 years of age)
Impairment
Components of Control
Reduction inlung growth
<75% predicted75 80% predicted>80% predicted• FEV1/FVC
2x/week2x/month1x/monthNighttimeawakenings
Throughout the day>2 days/week or multiple times on
2 days/week
2 days/week but not more than once on
each daySymptoms
Very Poorly ControlledNot Well
ControlledWell
Controlled

+Assessing Control and Adjusting Therapy
Components of Control
Classification of Asthma Control
Well Controlled Not Well Controlled
Very Poorly Controlled
Age 5-11
ACT >20 13-19 <12
Age >12
ACT >20 16-19 <15
Recommended Action for Treatment
• Regular followups every 1-6 months to maintain control
• Consider step down if well controlled for at least 3 months
• Step up 1 step and
• Reevaluate in 2-6 weeks
• Consider short course of oral systemic corticosteroids
• Step up 1-2 steps, and
• Reevaluate in 2 weeks
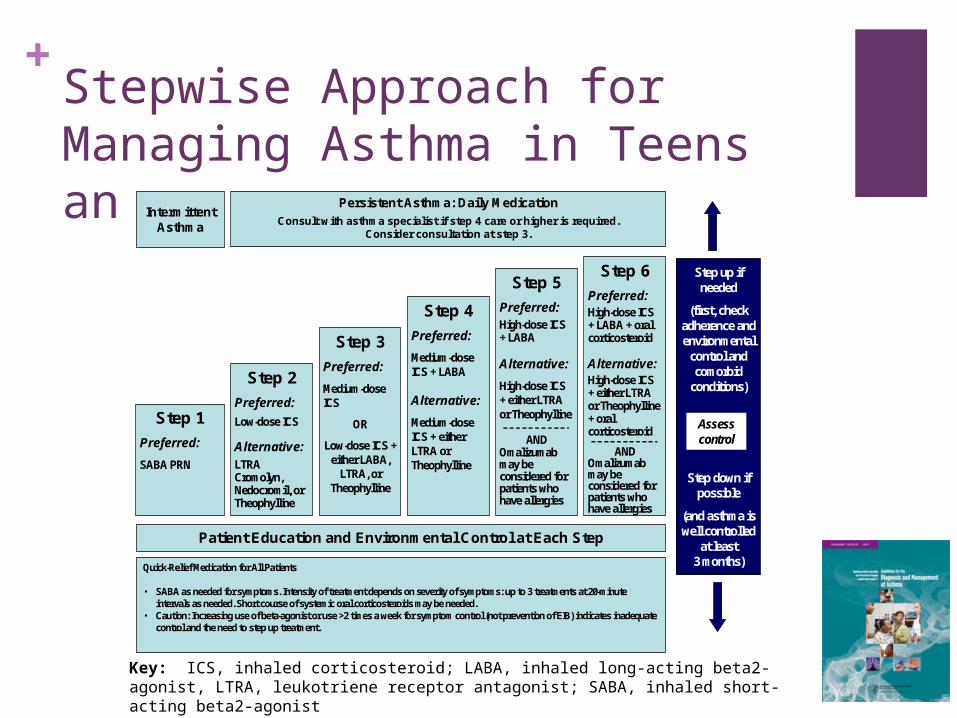
+Stepwise Approach for Managing Asthma in Teens and Adults Intermittent
Asthma
Persistent Asthma: Daily MedicationConsult with asthma specialist if step 4 care or higher is required.
Consider consultation at step 3.
Step 1
Preferred:
SABA PRN
Step 2
Preferred:
Low-dose ICS
Alternative:LTRA Cromolyn, Nedocromil, orTheophylline
Step 3
Preferred:
Medium-dose ICS
OR
Low-dose ICS + either LABA,
LTRA, or Theophylline
Step 5
Preferred:High-dose ICS + LABA
Alternative:
High-dose ICS + either LTRA or Theophylline
ANDOmalizumabmay be considered for patients who have allergies
Step 6
Preferred:High-dose ICS+ LABA + oral corticosteroid
Alternative:High-dose ICS + either LTRA or Theophylline+ oral corticosteroid
ANDOmalizumabmay be considered for patients who have allergies
Step up if needed
(first, check adherence and environmental
control and comorbid
conditions)
Step down if possible
(and asthma is well controlled
at least3 months)
Patient Education and Environmental Control at Each Step
Step 4
Preferred:
Medium-dose ICS + LABA
Alternative:
Medium-dose ICS + either LTRA or Theophylline
Assess control
Quick-Relief Medication for All Patients
• SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids may be needed.
• Caution: Increasing use of beta-agonist or use >2 times a week for symptom control (not prevention of EIB) indicates inadequate control and the need to step up treatment.
Key: ICS, inhaled corticosteroid; LABA, inhaled long-acting beta2-agonist, LTRA, leukotriene receptor antagonist; SABA, inhaled short-acting beta2-agonist

+Stepwise Approach for Managing Asthma in Children 5–11
Key: ICS, inhaled corticosteroid; LABA, inhaled long-acting beta2-agonist, LTRA, leukotriene receptor antagonist; SABA, inhaled short-acting beta2-agonist

+Stepwise Approach for Managing Asthma in Teens and Adults
IntermittentAsthma
Persistent Asthma: Daily MedicationConsult with asthma specialist if step 4 care or higher is required.
Consider consultation at step 3.
Step 1
Preferred:
SABA PRN
Step 2
Preferred:
Low-dose ICS
Alternative:LTRA Cromolyn, Nedocromil, orTheophylline
Step 3
Preferred:
Medium-dose ICS
OR
Low-dose ICS + either LABA,
LTRA, or Theophylline
Step 5
Preferred:High-dose ICS + LABA
Alternative:
High-dose ICS + either LTRA or Theophylline
ANDOmalizumabmay be considered for patients who have allergies
Step 6
Preferred:High-dose ICS+ LABA + oral corticosteroid
Alternative:High-dose ICS + either LTRA or Theophylline+ oral corticosteroid
ANDOmalizumabmay be considered for patients who have allergies
Step up if needed
(first, check adherence and environmental
control and comorbid
conditions)
Step down if possible
(and asthma is well controlled
at least3 months)
Patient Education and Environmental Control at Each Step
Step 4
Preferred:
Medium-dose ICS + LABA
Alternative:
Medium-dose ICS + either LTRA or Theophylline
Assess control
Quick-Relief Medication for All Patients
• SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids may be needed.
• Caution: Increasing use of beta-agonist or use >2 times a week for symptom control (not prevention of EIB) indicates inadequate control and the need to step up treatment.
ACT fits in here
Note the other components in the blue box

+Guidelines: Ambulatory Asthma Care
Identify precipitating factors
Identify comorbidities that may aggravate asthma
Assess patient’s knowledge/skills for self-management
Classify asthma severity
Monitor asthma control
Provide an Asthma Action Plan
Administer influenza vaccine to all patients with asthma
ACT helps here

+ 2. Possible Workflow for Using the ACT

+Identify patients with Asthma
Run reports to yield patient registries based upon ICD9 code 493 (asthma) in the electronic health record
(EHR) Reason for visit: any
Reports run by a clinical analyst the prior day
Medical assistant reviews report and flags patient charts for receiving ACT before the clinic opens in the morning For adolescents and young
men this may be the only way to measure their control
Think like you do for immunizations, missed opportunities
EHR marker flags patient for ACT

+Who can give ACT
Physician or other clinician seeing patient Been shown to miss most patients
Nursing staff putting patient in room Can be combined as a vital sign
Receptionist May allow patient time to complete before in office

+Administering the ACT: An example of patient flow
Several laminated copies of ACT in English and Spanish are available at the front rooms of the office
Receptionist asks about patient’s preferred language and then hands the patient the ACT and erasable marker to flagged patients at check-in

+Administering the ACT: An example of patient flow
Medical assistant or rooming nurse addresses questions about ACT while checking heart rate and blood pressure
Medical assistant or rooming nurse scores and enters ACT result in the asthma worksheet in the EHR
Laminated ACT remains with the patient in the exam room

+Possible script
“Hello, we are starting a new program that will help us take care of patients with asthma/wheeze/breathing problems better. We are asking any patient with asthma etc to fill out this form so that we can figure out the best way to help you get better.”
If the patient is adult, ask them to read the questions and give the answer that describes how they have felt over the last 4 weeks
If you are treating a child under 12, the parent and child should read the first 5 questions and the CHILD should pick the face. The parents then answers the last 3 questions.
Tell them that there is no need to add the numbers up, the provider will review it with them and add up the total in the room

+Clinician Interaction with ACT
Clinician reviews ACT score
Clinician also has available the laminated ACT copy to review specific items
The clinician enters the score in the EHR if not already entered
After encounter, medical assistant or rooming nurse wipes clean the laminated ACT and returns it to the receptionist

+Documenting ACT results in EHR
ACT template has been developed in our EHR
Result entered directly into template (describe where)

+Discussion
No one way is right for everyone
May have several strategies for different types of situations Urgent visits Asthma check ups others

+Potential Barriers Brainstorm on Solutions
Lack of familiarity with the ACT
Time and resource constraints
Patient literacy levels
Fit within the clinical workflow