achlorhydria and its clinical significance in diabetes mellitus
TRANSCRIPT

322 T H E A M E R I C A N JOURNAL OF DIGESTIVE DISEASES V o l u m e 16 Nun~ber 9
three times daily thereafter proved to be an effective dosage schedule.
We found this new colloid to be effective in tablet, granular and encapsulated powder form, but our pati- ents expressed a decided preference for the tablets.
In cases of severe, chronic constipation, the harsh laxative used by the patients should be gradually re-
R E F E
1. J~rown, C'. J. a n d H o u g h t o n , A. A.: T h e C h e m i c a l a n d P ~ y s i c a l P r o p e r t i e s of C a r b o x y m e t h y l , e e l l u l o s e a n d i t s Sa l t s , J. Soc. Chem. Ind. 60: 2,54T-258T, October , 19414
2. W e r l e , E . : Chem. Ztg. 65, 320 (C.A. 37: 280,78, 1943). ( T h e H a r m l e s s n e s s of SodiUm Ce l lu lo se G l y c o l a t e k n o w n a s a d i l a t i n g s u b s t a n c e , w h e n fed to r a t a n d
dogs . )
duced until finally omitted. S o d i u m carboxymethylcellulose can be used as an
adjunct in the treatment of hemorrhoids and proctitis.
\Ve found this synthetic gum to possess most of the advantages and none of the disadvantages of other cathartics heretofore available to us.
R E N C E S
3. Rowe, V. K.: SpeTteer, H. C.: AdLams, t3. M., a n d I r i sh , D. D.: R e s p o n s e of L a b o r a t o r y A n i m a l s to Ce l lu lo se Glyeo l i e A c i d a n d i t s S o d i u m a n d A l u m i n u m Sa l t s . Food R e s e a r c h , 9: 175-182, M a y - J u n e , 1944.
4. S h e l a n s k i a n d C l a r k - - I n P r e s s Food R e s e a r c h - - S o d i u m C a r h o x y m e t h y l e e l l u l o s e : I t s P h y s i o l o g i c a l A c t i o n on I ~ t b o r a t o r y A n i m a l s a n d H u m a n s .
Achlorhydria and Its Clinical Significance in Diabetes Mellitu=
By
I. M. R A B I N O W I T C H
MONTREAL
I N A RECENT MORTALITY INVESTIGATION. THE
'writer showed the extent to which it is now possible to control diabetes. Adjusted for age and sex, the ratio of actual to expected deaths in the group of diabetics who had adhered carefully to their treatment was prac- tically normal. Equally gratifying was the finding that, as in the experimental animal, regardless of the sever- ity of the diabetes, there is no evidence of an inherent tendency for the diabetes to become worse; that, in fact, provided treatment is followed carefully, there is an appreciable expectation of improvement of cm, bo- hydrate tolerance (1). This, however, does not warrant the conclusion that all of the problems in diabetes have been solved.
A random sample of a large group of diabetics will show that, though definite anaemia may not be common, a red blood cell count of 5,000,000 will be very uncom- mon. Of 281 consecutive cases, Joslin (2) reported 45 with cell counts below 4,t300,000 - - an incidence of 16 per cent. It is not stated whether they were hospital cases only or whether they reflected the experiences of the clinic for diabetes in general. For statistical pur- poses, it is the writer's practice to take 4,200,000 as the dividing line betwen anaemia, and no anaemia, cor- responding as it does ordinarily to a haemogDbin value of, approximately, 85 per cent. With this standard, as Table 1 shows, the incidence of low red blood cell counts, was appreciably lower, but by no means negligi- ble; of 500 consecutive examinations in his private of- rice practice, 63 showed cell counts below 4,200,000 - - an incidence of 12.6 per cent.
A random sample of a large group of diabetics, care- fully questioned and carefully examined, will show that an appreciable percentage are suffering from diabetic
P e r s o n a l c o n u n u n i e a t i o n
neuritis. Estimates in the literature range between 0.6 and 57.3 per cent (3). Amongst 1,000 patients in Jos- lin's Clinic, Jordan (3) found 25 such cases - - an in- cidence of 2.5 per cent. With the same classification of neuritic manifestations in diabetes, amongst 500 con- secutive cases in the writer's experience, there were 31 - -an incidence of 6.2 per cent (Table 1). Limited
Table 1
I N C I D E N C E OF A N A E M I A A N D A C H L O R H Y D R I A A C C O R D I N G TO AGE IN 500 D I A B E T I C S
S E L E C T E D A T R A N D O M
Age No. A N A E M I A * N E U R I T I S (Yrs. ) No. % No. %
-39 188 6 3.2 3 1.6
40- 312 57 17.7 28 8.9
Al l 500 63 12.6 31 6.2
"4,200,009 r ed b lood ce l l s o r less .
significance is to be attached to smaller samples. Thus, amongst 100 cases only, to be referred to again, the in- cidence was 9 per cent. Joslin* has the impression that the incidence in his clinic now is larger than when Jor- dan published his paper in 1936.
A similarly selected sample will show that tile inci- dence of digestive disturbances - - coated tongue, loss of appetite, nausea, vague epigastric discomfort un- related to meals, belching, bloating, fullness and fluid regurgitation after meals, abdominal distension, etc.-- is high. To a certain extent this may be due to the high incidence of disease of the gall bladder and biliary passages in diabetes. In fact, the earliest reference to the pathology of diabetes was to the pathology of the liver; Mead first drew attention to the fatty infiltra- tion in 1784 (4). Fatt3- infiltration of the liver is a common post-mortem finding in deaths due to diabetic

A. J. D . D . :\CIILORI{YDRIA AND ITS CLINICAL SIGNIFICANCE IN DIABETES MELLITUS 323 Noptember, 1949
coma; it is readily produced in the partially depancrea- tized animal, and, as Best and his associates have shown, the condition is greatly exaggerated in spite of insulin therapy when the choline content of the diet is kept low (5,6). Enlargement of the liver is common in uncontrolled diabetes (7) particularly in children. Priscilla White (8) found palpable livers in 40 per cent of her cases. In one case, the enlargement was such that the lower border was found in the pelvis (9) . Two striking cases of fluctuation of the size of the liver with the degree of control of the diabetes were reported by the writer (10,11). In addkion, there are the func- tional disturbances. In 1926. the writer (12) drew attention to the high incidence of excess quantities of bilirubin in the blood of diabetics and, in 1936. to a high incidence of excess excretions of uorbilinogen in the urine (13). More recently, Gray, Hook and Batty (14) reported a still higher incidence of liver disturb- ances in their group of diM)etics: but that disease of the gall bladder and biliary passages is not alone the explanation of the high incidence of digestive disturb- antes amongst diabetics is suggested from a variety of pathological findings. Many years ago, Munro (15) drew attention to hypertrophy of the dufydenal mucosa in diM)etic conm. Still to be explained is the gastric haemorrhage in diabetic coma and also that with very severe insulin reactions. Nocturnal diarrhoea and nocturnal incontinence of faeces are other examples, and "diabetic indigestion" recently emphasized by Bas- sler and Peters (16) is another.
:knother common occurrence amongst diabetics is achl.orhydria. In 1931. the writer and his associates reported an incidence of 39 per cent (17) which then seemed very high. In the latest editi-n of their book, Joslin and his associates t2) record an average inci- dence of 32.8 per cent, based upon the experiences of eight different authors. More impressive, however, are Joslin's own experiences ; whereas, gastric and duodenal ulcers are nearly alwavs associated with hyperchlor- hydria (18), amongst 58 cases with such ulcers, Joslin found no free hydrochloric acid in the first specimen in 21 - - an incidence of 36.2 per cen t ( ! ) In 5 cases, there was no free hwlrochloric acid even after his- tamine.
When two or more conditions are found in the same individual, it is sound practice to assume a common cause until proven otherwise. That the association of anaemia and achlorhydria, for example, may be causal rather than accidental, is suggested from the part that normal gastric juice plays in erythropoiesis; hydro- chloric acid not only aids in liberation of iron from food materials, but also facilitates its conversion to the fer- rous form which causes a discharge ~f reticulocytes from the bone marrow and an increase of red blood cells. Microcytic hypochrc, nic anaemia, for example, which responds to ferrous iron is not an uncommon re- sult of gastrectomy (18). l~ack of free hwlrochloric acid in the stomach was a frequent finding in the group of cases of anaemia reported by Joslin. In fact, it was the lack of free hydrochloric acid which led to the sus-
picion of a primary anaemia (2) . Suggestive also is
the influence of gastric acidity upon the absorption of iron. As pointed out previously (19) iron is absorbed mainly from the duodenum; and hydrochloric acid aids the absorption; whereas, a high pH in the duodenum facilitates formation of basic iron compounds which are very poorly absorbed. From a practical standpoint, therefore, assuming a causal relationship between the achlorhwtria and anaemia in a case of diabetes, rather than merely prescribing iron, the more logical treat- ment of such a case would be to attempt to correct the pH in the stomach and duodenum by administration of hydrochloric acid.
Equally suggestive of a causal rather than an acci- dental association is the combination of achlorhydria and diM~etic neuritis (19). It is important to note that, though thianline is stable in gastric juice over a wide pH range I 1.5 to 8.0 - - with a pH of over 8.0, i t i s readily destroyed. There is also evidence that achlor- hydria may impair absorption of that part of the thi- amine which has escaped destruction in the alkaline nledimn. Therefore, assuming a causal relationship between the achlorhydria and the neuritis, rather than merely adding thiamine to the diet of a diabetic with achlorhydria, the more logical treatment in such a case would be to attempt to lower the pH of the gastric and duodenal secretions by administration of hydrochloric acid so as to prevent destruction of the thiamine in the food materials. That hydrochloric acid may, alone, correct a vitamine B~ deficiency in cases of achlorhydria is suggested from the observation that, in skin lesions associated with vitamine B~ deficiency and deficiency of hydrochloric acid in the gastric juice, treatment with hydrochloric acid and B complex was found far sup- erior to treatment with B complex alone (20).
In view of the ~bove observations, 100 diabetics were selected at random from a group in whom gastric ana- lysis had been performed, except with regard to age, in order to determine (a) the extent to which anaemia, neuritis, digestive disturbances and achlorhydria were associated with each other and (ib) .by subjecting the data to the proper statistical treatment, whether the associations were causal or accidental.
Because of the relationship noted in the previous study (17) .'between age and the occurrence of aCht6r- hydria, the cases were divided into two groups, namely, (a) those of age '39 years and trader and (b) those of age 40 years and over. In order that the percentage inci- dences of achlorhydria would be strictly comparable, at least with respect to the numbers of subjects from which they were calculated, the numbers of individuals in the two age groups were the same. Otherwise, as stated, the selection was random. The incidence of achlorhydria and the influence of age in this group are briefly summarized in Table 2.
Table 2 I N C I D E N C E OF A C H L O R H Y D R I A ACCORDING TO AGE.
Age No. A-CHLORHYDR!A (Yrs) No. go
-39 50 9
4 0 : 50 ~2 All Ages 100 - - 41
18 i
64
41
3 2 4 T H E A M F R I C A N JOURNAL OF DIGESTIVE DISEASES V o l u m e 16 N u m b e r 9
INCIDENCE OF ACIILORHYDRIA
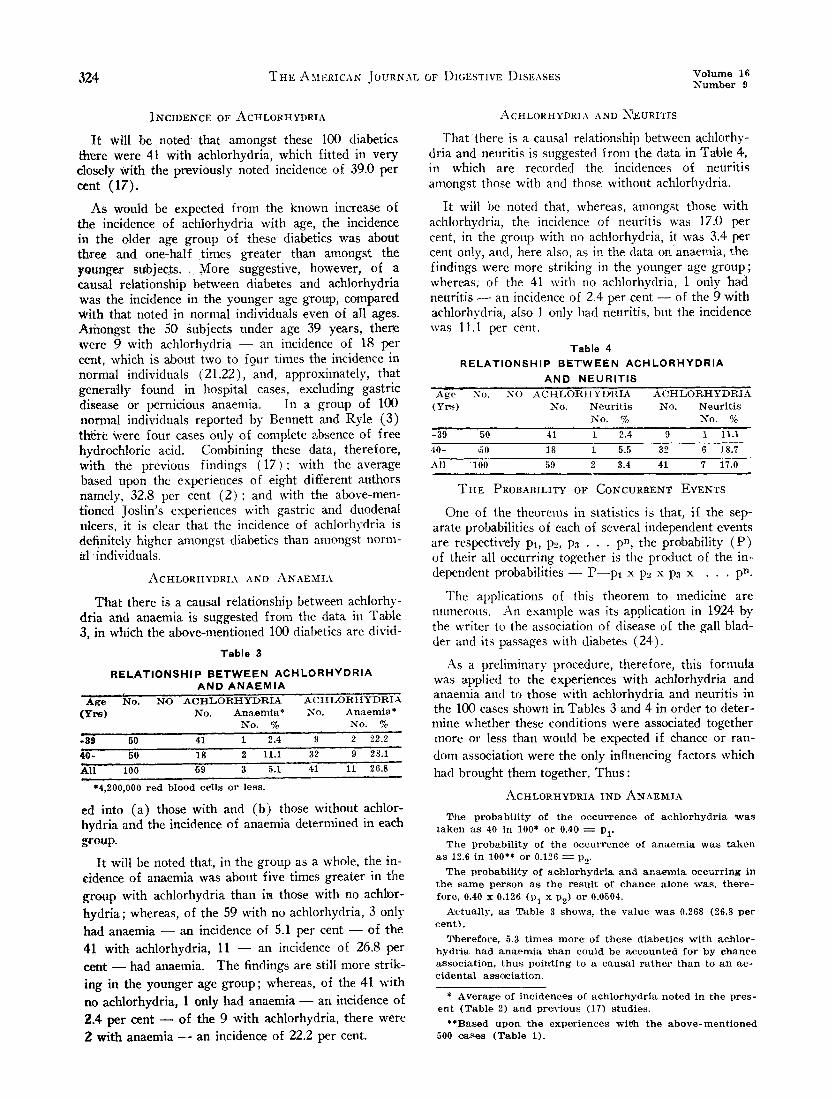
I t will be noted that amongst these 100 diabetics there were 41 with achlorhydria, which fitted in very closely with the previously noted incidence of 39.0 per cent (17).
As would be expected from the known increase of the incidence of achlorhydria with age, the incidence in the older age group of these diabetics was about three and one-half times greater than amongst the younger sub j ec t s . . More suggestive, however, of a causal relationship between diabetes and achlorhydria was the incidence in the younger age group, compared with that noted in normal individuals even of all ages. Arilongst the 50 Subjects under age 39 years, there were 9 with achlorhydria - - an incidence of 18 per cent, which is about two to four times the incidence in normal individuals (21.22), and, approximately, that generally found in hospital cases, excluding gastric disease or pernicious anaemia. In a group of 100 normal individuals reported by Bennett and Ryle (3) there Were four cases only of complete absence of free hydrochloric acid. Combining these data, therefore, with the previous findings (17) : with the average based upon the experiences of eight different authors namely, 32.8 per cent ( 2 ) : and with the above-men- tioned Joslin's experiences with gastric and duodenal ulcers, it is clear that the incidence of achlorhydria is definitely higher amongst diabetics than amongst norm- a l individuals.
ACHLORHYDRIA AND ~A.NAEMIA
That there is a causal relationship between achlorhy- dtda and anaemia is suggested from the data in T~ble 3, in which the above-mentioned 100 diabetics are divid-
Table 3
R E L A T I O N S H I P B E T W E E N A C H L O R H Y D R I A A N D A N A E M I A
A g e No. ( Y r s )
-39 50
40- 5o ku loo
NO AC HI_JORHYDRI.A XCTILORHYDRIX No. Anaemia* No. Anaemia*
No. % No. %
41 1 2.4 9 2 22.2
18 2 I i . i 32 9 28.1
69 3 5.1 41 ' 11 26.8
*4,200,000 r ed b lood ce i l s o r less .
ed into (a) those with and (b) those without achlor- hydria and the incidence of anaemia determined in each group.
I t will be noted that, in the group as a whole, the in- cidence of anaemia was about five times greater in the group with acblorhydria than in those with no achlor-
hydria; whereas, of the 59 with no achlorhydria, 3 only
had anaemia - - an incidence of 5.1 per cent - - of the 41 with achlorhydria, 11 - - an incidence of 26.8 per cent - - had anaemia. The findings are still more strik-
ing in the younger age group; whereas, of the 41 with
no achlorhydria, 1 only had anaemia - - an incidence of 2.4 per cent ~ of the 9 with achlorhydria, there were 2 with anaemia ~ an incidence of 22.2 per cent.
ACBLORHYDRIA AND ~EURITIS
Thatthere is a causal relationship between achlorhy- dria and neuritis is suggested from the data in Table 4, in which are recorded the incidences of neuritis amongst those with and those without achlorhydria.
It will be noted that, whereas, amongst those with achlorhydria, the incidence of neuritis was 17.0 per cent, {n the group with no achlorhydria, it was 3.4 per cent only, and, here also, as in the data on anaemia, thc findings were more striking in the younger age group; whereas; of the 41 with no achlorhydria, 1 only had neuritis ~ an incidence of 2.4 per cent - - of the 9 with achlorhydria, also l only lind neuritis, but the incidence was II.I per cent.
Table 4
R E L A T I O N S H I P B E T W E E N A C H L O R H Y D R I A A N D N E U R I T I S
"Ag'-e "'N(;. NO A C H L O R H Y I > R I A AC'~tLORHYDRI:% (Yrs ) No. N e u r i t i s No. N e u r i t i s
No. % No. %
-39 50 41 i 2.4 9 1 Ii .I
40- 60 18 I 5.5 32 6 18.7
All "I00 59 2 3.4 41 7 17.0
T H E PROBABILITY OF CONCURRENT EVENTS
One of the theorenIS in statistics is that, if the sep- arate probabilities of each of several independent events are respectively pl, p2, p~ • • • pn, the probability ( P ) of their all occurring together is the product of the in- dependent probabilities - - P - - p t x p2 x p3 x . . . pn.
The applications of this theorem to medicine are numerous. An example was its application in 1924 by the writer to the association of disease of the gall blad- der and its passages with diabetes (24).
As a preliminary procedure, therefore, this fommla was applied to the experiences with achlorhydria and anaemia and to those with achlorhydria and neuritis in the 100 cases shown in Tables 3 and 4 in order to deter- mine whether these conditions were associated together more or less than would be expected if chance or ran- dom association were the only influencing factors which had brought them together. Thus :
.A,_CHLORHYDRIA IND A N A E M I A
The p r o b a b i l i t y of t he o c c u r r e n c e of a c h l o r h y d r i a Was t a k e n a s 40 in 100" or 0.40, ~ Pl"
The p r o b a b i l i t y of t he o ~ c u r r c n c e of a n a e m i a w a s t a k e n a s 12.6 in 100"* or 0.126 -~- P2'
T h e probabt l i , t y of ach lo rhyc~r ia a n d anaeTnia o c c u r r i n g in t he s a m e p e r s o n a s t he r e s u l t ~f c h a n c e a l o n e was , t h e r e - fore, 0.40 x 0.126 (PI x p2 ) or 0.0504.
~ c t u a l l y , a s Tab le 3 shows , t h e v a l u e w a s 0.268 (26.8 p e r c e n t ) .
The re fo re , 5.3 t i m e s m o r e of t h e s e d i a b e t i c s w i t h a c h l o r - h y d r i a h a d a n a e m i a t 'han cou ld be a c c o u n t e d fo r by c h a n c e a s s o c i a t i o n , t h u s po in ' t ing to a c a u s a l r a t h e r t h a n to a n ~c- c i d e n t a l as .socia t ion.
• A v e r a g e of i n c i d e n c e s of a e h l o r h y d r i a n o t e d in t he p r e s - en t ( T a b l e 2) a n d p r e v i o u s (17) s t u d i e s .
• * B a s e d u p o n the e x p e r i e n c e s w i t h t he a b o v e - m e n t i o n e d 500 causes (T~b le 1).
A . J . D . I) . ~ p t e n ~ b ~ r , 1949
A C H L O R H Y D R I A A N D N E U R I T I S
T h e p r o b a b i l i t y o f o c c u r r e n c e o f a e h l o r h y d r i a w a s a g a i n
t a k e n a s 40 i n 100" o r 0.40 ~ Pl"
T h e p r o b a b i l i t y o f o ~ c u r r e n c e o f n e u r i ' t i s w a s t a k e n a s
6.2 i n 100"* o r 0.062 ~ P2"
T h e p r o b a b i l i t y o f a e h l o r h y d r i a a n d n e a t ' i r i s o c c u r r i n g i n t h e s a m e p e r s o n a s a r e s u l t o f c h a n c e a l o n e w a s , t h e r e f o r e ,
0.4 x 0.062 ( P l x p, , ) o r 0.0248.
A c t u a l l y , a s T a b l e 4 s h o w s , t h e v a l u e w a s 0.17 (17 p e r c e n t ) . T h e r e f o r e , 6.8 t i m e ' s m o r e o f t h e s e d i a b e t i c s h a d n e u r i t i s t h a n c o u l d b e a c c o u n t e d f o r b y c h a n c e a s soc ia~t ion , t h u s , a s in t h e c a s e o f a n a e m i a , p o i n t i n g t o a c a u s a l r a t h e r
t h a n t o a n a c c i d e n t a l a s s o c i a t i o n .
T H E R A P E U T I C T E S T
. 5 t C H L O R H Y I ) R I A A N D , 2 k N A E M I A
If, in fact, there is a causal relationship between achlorhydria and anaemia, hydrochloric acid should cor- rect the anaemia to a certain extent at least, independent of any iron medication by liberating iron from the food materials; by aiding conversion of the liberated iron to the ferrous state, and also by aiding its absorption.
To test this possibility, 25 individuals were selected at random, except that (a) none had a red blood cell connt higher than 4.2(30,000 and I b ~ in all cases, the diabetes was under good control, since imt)rovement of the dia- betes in a poorly controlled case would alone probably tend to improve the anaemia to a certain extent by the general improvement of nutrition. In each case,
therefore, the only change of treatment was the addi- tion of hydrochloric acid, in the forln of glutamic acid
hydrochloride (5 grains, three times a day, before
meals) to avoid the possible solvent action of hydro-
chloric acid on dental enamel. Such amounts of hydro- chloric acid, it should be noted, may not be sufficient to allow the appearance of appreciable free acid in the
stomach, but, nevertheless, as Goodman and Gilman have pointed out (25), for some unexplained reason,
they are often effective in relieving the symptoms of
achlorhydria.
In order to compare the effects, if any, of hydro- chloric acid with those of administration of iron, in each case, at the end of one month, the glutamic acid hydrochloride was replaced by a preparation of iron, which contained 6 3/4 grains of ferrous carbonate, which was also to .be taken three times a day. To deter- mine the extent to which, if any, hydrochloric acid would aid the absorption of the added iron, at the end
of one month of treatment with iron alone, the glutamic
acid hydrochloride was again prescribed in the ~bove- mentioned dosage with no change in the treatment with
the iron for a period of one month. The combined data
are briefly summarized in Table 5.
* A v e r a g e o f i n c i d e n c e s o f a e h l o r h y d r i a n o t e d in t h e p r e s - e n t a n d p r e v i o u s (17) s t u d i e s .
* * B a s e d u p o n t h e e x p e r i e n e e ~ w i t h t ' he ~ b o v e - m e n t l o n e d 500 c a s e s ( T a b l e 1) .
A C H L O R I I Y D R I A A N D I T S C L I N I C A L S I G N I F I C A N C E I N DIABETES M E L L I T U S 325
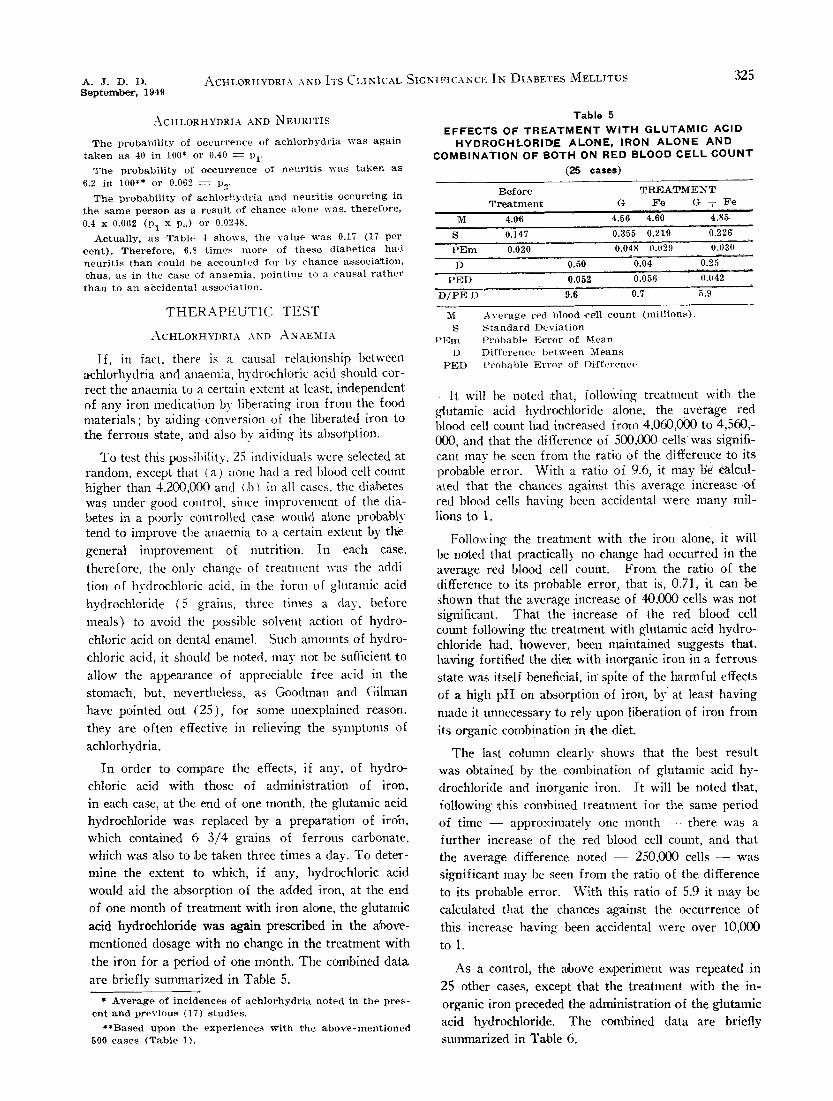
Table 5 EFFECTS OF T R E A T M E N T W I T H G L U T A M I C ACID
HYDROCHLORID~E ALONE, IRON A L O N E A N D C O M B I N A T I O N OF BOTH ON RED BLOOD CELL C O U N T
(25 cases)
B e f o r e T R I ~ I A T M E~N T T r e a t m e n t G F e G + F e
M 4.0.6 4.56 4.60 4.851
S 0.147 0.355 0 .219 0 .226
P E r u 0.020 0.048 0.02.9 0.030
D 0.50 0.04 0.25
P ~ D 0.052 0.056 0.042
D / P E D : - 9.6 0.7 5.9
M S
l ' E m
D P E D
A v e r a g e r e d b l o o d c e l l c o u n t ( m i l l i o n s ) . S t a n d a r d D e v i a t i o n P r o b a b l e B r r o r o f M e a n D i f f e r e n c e b e t w e e n M e a n s P r o b a b l e E r r o r o f D i f f e r e n c e
It will be noted ~that; following treatment with the gtntamic acid hydrochloride a lone , the average red blood cell count had increased from 4,060,000 to 4,560,- 000, and that the difference of 500,000 cellswas signifi- cant may be seen from the ratio of the difference to its probable error. With a ratio of 9.6, it may be calcul- ated that the chances against this average increase .of red blood cells having been accidental were many mil- lions to 1.
Following the treatment with the iron alone, it will be noted that practically no change had occurred in the average red blood cell count. Front the ratio of the difference to its probable error, that is, 0.71, it can be shown that the average increase of 40,000 cells was not significant. That the increase of the red :blood cell count following the treatment with glntamic acid hydro- chloride had, however, been maintained suggests that, having fortified the di~t with inorganic iron in a ferrous state was itself beneficial, in spite of the harmful effects of a high pH on absorption of iron, by at least having
made it unnecessary to rely upon liberation of iron from
its organic combination in the diet.
The last column clearly shows that the best restflt was obtained by the combination of glutamic acid hy- drochloride and inorganic iron. It will be noted that, following ¢~his com'bined treatment for the same period of time - - approximately one month - - there was a further increase of the red blood cell count, and that the average difference noted - - 250,000 cells - - was significant may be seen from the ratio of the difference to its probable error. With this ratio of 5.9 it nmy be calculated that the chances against the occurrence of
this increase having been accidental were over 10,000
to 1.
As a control, the above e~periment was repeated in 25 other cases, except that the treatment with the in-
organic iron preceded the administration of the glutamic acid hydrochloride. The combined data are briefly summarized in Table 6.
326 THE AMERICAN JOURNAL OF DIGESTIVE DISEASES VolUme 16 N u m b e r 9
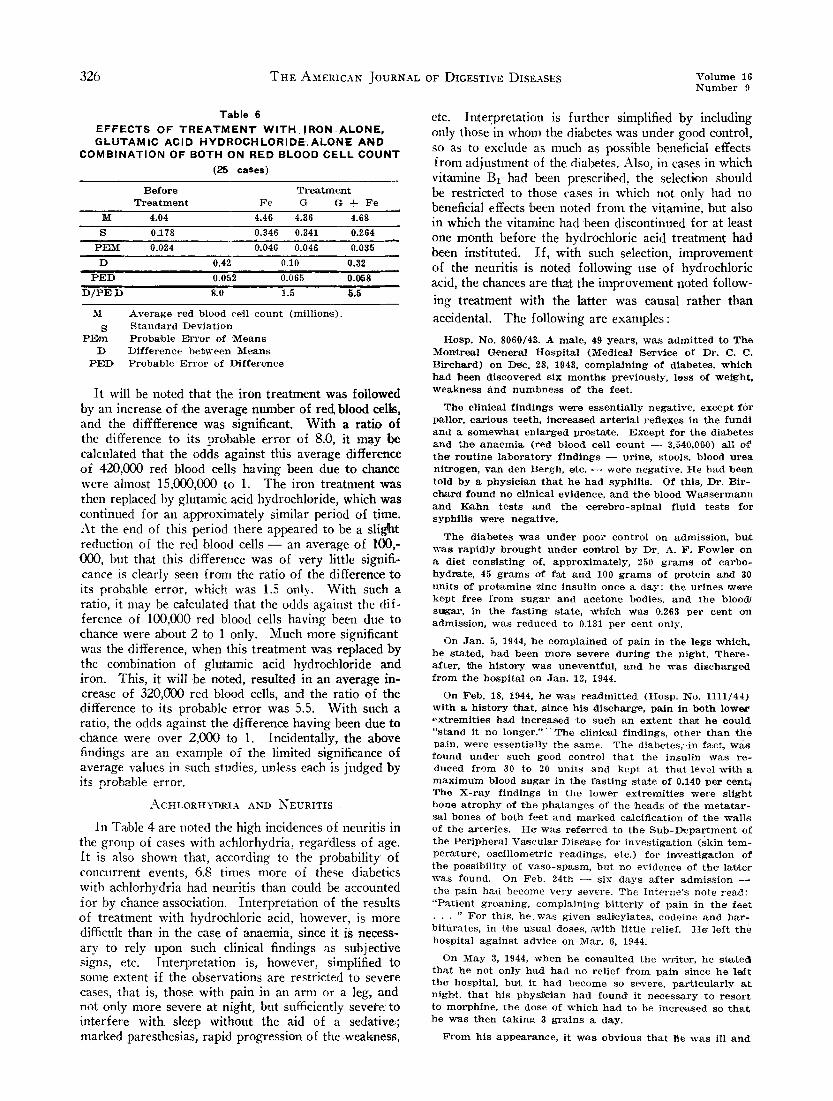
Table 6 E F F E C T S OF T R E A T M E N T W I T H , I R O N , A L O N E , G L U T A M I C ACID H Y D R O C H L O R I D E , A L O N E A N D
C O M B I N A T I O N OF BOTH ON RED BLOOD CELL C O U N T (25 cases)
B e f o r e T r e a t m e n t T r e a t m e n t F e G G + F e
:hi' 4 .04 4.46 4.36 4.68
S 0,178 0.346 0.341 0.264
PELM 0.024 0.046 0.046 0.035
D 0.42 0.10 0,32
P E D 0.052 0.065 0.058
D / P E D 8.0 1.5 S.5
M
S PEm
D pL-~D
A v e r a g e r e d b l o o d c e l l c o u n t ( m i l l i o n s ) . S t a n d a r d D e v i a t i o n P r o b a b l e E r r o r o f M e a n s D i f f e r e n c e b e t w e e n M e a n s P r o b a b l e E r r o r o f D i f f e r e n c e
It will be noted that the iron treatment was followed by an increase of ¢he average number of red blood cells, and the difffference was significant. With a ra t io of the difference to its probable error of 8.0, it may be calculated that the odds against this average difference of 420,000 red blood cells having been due to chance were almost 15,000,000 to 1. The iron treatment was then replaced by glutamic acid hydrochloride, which was continued for an approximately similar period of time. At the end of this period there appeared to be a slignat reduction of the red blood cells - - an average of 100,- 000, but that this difference was of very little signifi- cance is clearly seen from the ratio of the difference to its probable error, which was 1.5 only. With such a ratio, it may be calculated that the odds against the dif- ference of 100,000 red blood cells having been due to chance were about 2 to 1 only. Much more significant was the difference, when this treatment was replaced by the combination of glntamic acid hydrochloride and iron. This, it will be noted, resulted in an average in- crease of 320,(~)0 red blood cells, and the ratio of the difference to its probable error was 5.5. With such a ratio, the odds against the difference having been due to chance were over 2,000 to 1. Incidentally, the above findings are an example of the limited significance of average values in such studies, unless each is judged by its probable error.
A C H L O R H Y D R I A A N D N E U R I T I S ~
In Table 4 are noted the high incidences of neuritis in the group of cases with achlorhydria, regardless of age. i t is also shown that, according to the probability of concurrent events, 6.8 times more of these diabetics with achlorhydria had neuritis than could be accounted for by chance association. Interpretation of the results of treatment with hydrochloric acid, however, is more difficult than in the case of anaemia, since it is necess- ary to rely upon such clinical findings as subjective signs, etc. Interpretation is, however, simplified to some extent if the observations are restricted to severe cases, that is, those with pain in an arm or a leg, and not only more severe at night, but sufficiently severe to interfere with. sleep without the aid of a sedative;; marked paresthesias, rapid progression of the .weakness,
etc. Imerpretation is further simplified by including only those in when1 the diabetes was under good control, so as to exclude as much as possible beneficial effects from adjustment of the diabetes. Also, in cases in which vitamine B1 had been prescribed, the selection should be restricted to those cases in which not only had no beneficial effects been noted from the vitamine, but also in which the vitamine had 'been discontinued for at least one month before the hydrochloric acid treatment had been instituted. If, with such selection, improvement of the neuritis is noted following use of hydrochloric acid, the chances are that the iinproventent r~oted follow- ing treatment with the latter was causal rather than
accidental. The following are exanlples:
H o s p , N o . 8 0 6 0 / 4 3 . A m a l e , 49 y e a r s , w a s a d m i t t e d t o T h e M o n ~ r e ~ l G e n e r a l H o s p i t a l ( M e d i c a l Ser~xice o f D r . C. C . B i r c h ~ r d ) o n D e e . 28, 1943, c o m p l a i n i n g o f d i a b e t e s , w h i c h h a d b e e n d i s c o v e r e d s i x m o n t h s p r e v i o u s l y , l o s s o f w e i g h t , w e a k n e s s A n d n u m b n e s s o f t h e f e e t .
T h e c l i n i c a l f i n d i n g s w e r e e s s e n t i a l l y n e g a t i v e , e x c e p t f o r p a l l o r , c a r i o u s t e e t h , i n c r e a s e d a r t e r i a l r e f l e x e s i n t h e f u n d i a n d a s o m e w h a t e n l a r g e d p r o s t a t e . E x c e p t f o r t h e d i a b e t e s a n d t h e a n a e m i a ( r e d b l o o d c e l l c o u n t - - 3 ,540 ,000) a l l o~ t h e r o u t i n e l a b o r a t o r y f i n d i n g s - - m - i n e , s t o o l s , b l o o d u r e a n i t r o g e n , v a n d e n B e r g b , e~c. - - w e r e n e g a t i v e . H e h a d b e e n t o l d b y a p h y s i c i a n t h a t h e h a d s y p h i l i s . O f t h i s , D r . B i r - C h ~ r d f o u n d n o c l i n i c a l e v i d e n c e , a n d t h e b l o o d W a s s e r m a n n a n d K a h n t e s t s a n d t h e ¢ e r e b r o - s p i n a l f l u i d t e s t s f o r s y p h i l i s w e r e n e g a t i v e .
T h e d i a b e t e s ' w a s u n d e r p o o r c o n t r o l o n a d m i s s i o n , b t~t ~ s r a p i d l y b r o u g h t u n d e r con~trol b y D r . A . F . F o w l e r o n a d i e t c o n . s i s t i n g of , a p p r o x i m a t e l y , 250 g r a m s o f c a r b o - h y d r ~ t e , 45 g r a m s o f fa~ a n d 100 g r a m s o f p r o t e i n a n d 30 u n i t s o f p r o t ~ m i n e z i n c i n s u l i n o n c e a d a y ; t h e u r i n e s w a r e k e p t f r e e f r o m s u g a r a n d a c e t o n e b o d i e s , a n d t h e b l o o d / s u g a r , i n t h e f a s t i n g s t a t e , ~ h l c h w a s 0.263 p e r c e n t o n a d m i s s i o n , w a s r e d u c e d t o 0.131 p e r c e n t o n l y .
O n J a n . 5, 1944, h e c o m p l a i n e d o f p a i n i n t h e l e g s w h i c : h , h e s t a t e d , h a d b e e n m o r e s e v e r e d u r i n g t h e n i g h t . T h e r e - a f t e r , ~he h i s t o r y w a s u n e v e n t f u l , a n d h e w ~ s d i s c h a r g e d f r o m t h e h o s p i t a l o n J a n . 12, 1944.
O n F e b . 18, 1944, h e wets r e a d m i t t e d ( H o s p . N o . 1 1 1 1 / 4 4 ) w i t h a h i s t o r y ~b_at, s i n c e h i s d i s c h a r g e , p a i n i n b o t h l o w e r ~ x t r e m i t i e s Ihad i n c r e a s e d ~o s u c h a n e x t e n t thaYc h e c o u l d " s t a n d i.t n o l o n g e r . " : ' T h e , e l i n i ~ l f i n d i n g s , o t h e r t h a n t h e p a i n , w e r e e s s e n t i a l l y t h e s a m e . T h e d i a b e ~ e s , - i n facet, W~.s f o u n d u n d e r s u c h g o o d c o n , t r o l t h a t t h e i n s u l i n w a s r e - d u c e d f r o m 30 t o 20 u n i t s a n d k e p t a t t h a t l e v e l w i t h a m a x i m u m b l o o d s u g a r i n t h e f a s t i n g s¢tate o f 0 .140 p e r c e n t ~ T h e X - r a y f i n d i n g s i n t h e l o w e r e x t r e m i t i e s w e r e s l i g h t b o n e a t r o p h y o f t h e p h a l a n g e s o f t h e h e a d s o f t h e m e t a t a r - s a l b o n e s o f b o t h f e e t a n d m a r k e d c a l c i f i c a t i o n o f t h e w a l l s o f t h e a z ' t e r i e s . H e w a s r e f e r r e d t o t h e S u b - D e p a r t m e n t o f t h e P e r i p h e r a l V a s c u l a r D i s e a s e f o r i n v e s t i g a t i o n ( s k i n t e m - p e r a t u r e , o s c i l l o m e " c r i c r e a d i n g s , e t c . ) f o r i n , v e s t i g a t i o n o f t h e p o s s i b i l i t y o f v a s e - s p a s m , b u t n o e v i d e n c e o f t h e la fc ter ~vas f o u n d . O n F e b . 2 4 t h - - s i x d a y s a f t e r a d m i s s i o n t h e p a i n h a d b e c o m e v e r y s e v e r e . T h e I n t e r n e ' s n o t e r e a d : " P a t i e n t g r o a n i n g , c o m p l a i n i n g b i t t e r l y o f p a i n i n t h e f e e t • . . " F o r t h i s , h e w a s g i v e n s a l t c y l a t e s , c o d e i n e a n d b a r - b i t u r a t e s , i n ~he u s u a l d o s e s , ~vcith l i t t l e r e l i e f . H e ' l e f t t h e h o s p i t a l a g a i n s t a d v i c e o n M a r . 6, 1944.
O n M a y 3, 1944, w h e n h e c o n s u l t e d t h e w r i t e r , h e s t a t e d t h a t h e n o t o n l y h a d h a d n o r e l i e f f r o m p a i n s i n c e h e l o f t t h ~ h o s p i t a l , bu, t i t h a d b e c o m e s o s e v e r e , p a r t i c u l a r l y a t n igh , t , t h a t h i s p , h y s 2 c i a n h a d f o u r ~ d i t n e c e s s a r y t o r e s o r t t o m o r p h i n e , t h e d o s e o f w h i c h h a d t o b e i n c r e a s e d so t h a t h e w a s t h e n t a k i n g 3 g r a i n s a d a y .
F r o m h i s a p p e a r a n c e , i t w a s o b v i o u s t h a t t ie w a s il l a n d

A . J . D . D . ~ e p t e m b o r , 1949
A C H L O R H Y D R I A A N D I T S C L I N I C A L S I G N I F I C A N C E I N D I A B E T E S M E L L I T U S 327
in m u c h p a i n , t h o u g h t h e p u p i l s w e r e s t i l l e o n t r a c t e d f r o m t h e l a s t d o s e o f m o r p h i n e ; t, h e s k i n w a s p a l e a n d m o i s t ank l h i s c o n v e r s a t i o n w a s r e p e a t e d l y i n t e r r u p t e d b y m o a n s . H e w e i g h e d 112 1-2 p o u n d s o n l y in c l o t h e s ( H e i g h t - - 6 3 in, c h e s ) . Sin~ce h i s n a k e d w e i g h t xx~hen h e l e f t t he ' h o s p i t a l o n ~Ylar. 6, 1944 , w a s 116 p o u n d s , a . l h*wing a b o u t 8 p o u n d s f o r c l o t h e s , h e h a A l o s t , a p p r o x i m a t e l y , 12 p o u n d s s i n c e t h e n .
T h e d ~ a b e t e s w a s u n d e r g o o d c o n t r o l ; t h e u r i n e ~ s f r e e f r o m s u g a ~ a n d a c e t o n e b o d i e s , a n d t, h e b l o o d s u g a r w a l s p r a c t i c a l l y " n o r m a l , n a m e l y , 0.129 p e r c e n t . T h e r e d b l o o d ce l l , c o u n t w a s 3,100,000 a n d t h e h a e m o g l o b i n 60 p e r c e n t .
B o t h f e e t w e r e w a r m ; p u l s a t i o n s w e r e e l i c i t e d i n t h e d o r s a l i s p e d i s , p o s t e r i o r t i b i M a n d p o p l i t e a l a . r t e r i e s o f b o t h s i d e s , a n d ~he p ~ t e l l a r r e f l e x w a s p r e s e n t o n b o t h s i d e s , t h o u g h t h e l e f t w a s l e s s a c t i v e t h a n t h e r i g h t . T 'he a b n o r m - a l i t i e s w e r e m a r k e d p a r e s t h e s i a s , a b n o r m a l s e n s a t i o n s t o p i n p r i c k , m ~ r k e d , w e a k n e s s a n d , in f a c t , s l i g h t f o o t - d r o p o n o n e s i d e ( r i g h t ) . T h e r e w a s n o s u g g e s t i o n i n t h e h i s - t o r y o f a n y a t t a c k s o f i n t e r m i t t e n t c l a u d i e a t i o n .
T h e f i r s t c o n s i d e r a t i o n s w e r e r e l i e f o f t h e p a i n a n d m e a n s o f d i s p e n s i n g w i t h t h e m o r l ) h i n e . T h e i m l ) r e s s i o n wins t h a t h e w o u l d ~ o o p e r a t e , s i n c e h e s t a t e d t h a t Vhe m o r p h i n ' . c a u s e d m u c h n a u s e a a n d a l s o , p e r i o d i c a l l y , v o m i t i n g . I n f a c t , h e v o m i t e d d u r i n g t h e e x a m i n a t i o n . * H e w a s , t h e r e - f o r e , a d v i s e d t o d i s c o n t i n u e t h e n m r p h i n e ~ n d , i n s t e a d o f it~ w a s g i v e n a s a l i e y l a t e m i x t u r e , t h e e q u i v a l e n t of , a p p r o x i - m a t e l y , 50 g r a i n ~ o f a c e t y l - s a l i c y l i c a c i d p e r d a y . F o l n i g h t s , h e w ~ s g i v e n a b r o m i d e m i x t u r e c o r r e s p o n d i n g t o t;,, g r a i n s o f e q u a l p a r t s o f s o d i u m , p o t a s s i u m a n d a m m o n i u m b r o m i d e a n d a l s o o n e a n d o n e - h a l f g r a i n s o f p h e n o b a r b i t a l . B o t h r w e r e t o b e r e p e ~ t e d i f n e c e s s a r y . I~or t h e a n a e m i a , h e w a s g i v e n ~he a b o v e - m e n t i o n e d p r e p a r a t i o n o f f e r r o u s c a r - b o n a t e . I n & d d t t i o n t o a l l o f t h e a b o v e , h e w a s g i v e n d i l u t e h y d r o c h l o r i c a c i d , t e n m i n i m s , t h r e e t i m ~ s a d a y b e f o r e m e a l s . T h e n o t e s s h o w t h a t i t w a s t ~ e i n t e n t i o n t o p r e s c r i b e v i t ~ m i n e B l a l s o a t t 'he n e x t v i s i t , i f t h e r e w a s n o a p p r e c i - a b l e r e l i e f f r o m t h e p a i n .
A t h i s n e x t v i s i t o n M a y 22, 1944 - - 19 d a y s l a t e r - - h e l o o k e d a n d s t a t e d h e f e l t b e t t e r . T h e r e w a s l e s s p a i n d u r i n g t h e d a y , a n d h e s t a t e d t h a t h e , h a d b e e n M e e p i n g b e t t e r atl n igh , t . T h e f o o t - d r o p h a d di, s a p p e a r e d , b u t t h e p a r e s t h e M a s w e r e s t i l l r n ~ r k e d . ~ h e d i a b e t e s w a s u n d e r s a t i s f a c t o r y - c o n t r o l . T h e r e d b l o o d c e l l c o u n t hax l i r~c : reased t o g,800,0@0 a n d t h e h a e m o g l o b i n t o 73 p e r c e n t . A f u r t h e r l o s s o f w e i g h t , h O w e v e r , h a d o c c u r r e d : he" n o w we ig~hed 10.8 p o u n d s , b u t h e s t a t e d t h a t t h e weigh~: h a d b e e n s t a t i o n a r y d u r i n g t h e p r e v i o u s w e e k . H e c o m p l a i n e d o f n o i s e s in t h e e a r s . " T h e o n l y c h a n g e o f t r e a t m e n t , ~ h e r e f o r e , w a s a 75 p e r c e n t r e d u , e t i o n o f t h e s a l i c y l ~ ' t e s .
O n e m o n t h l a t e r ( J u n e 22, 1944) a s t i l l f u r t h e r i m , p r o ~ ' e - m e n t w a s n o t e d i n h i s g e n e r a l c o n d i t i o n . H e s t a t e d t h a t h e ~had b e e n s l e e p i n g w e l l a n d h a d h a d p a i n o c c a s i o n a l l y o n l y . T h e p a r e s t h e s i a s w e r e s t i l l p r e s e n t , b u t t h e y ~ - e r e d e - t i n i t e l y l e s s m a r k e d , a l l of .~whi.eh f i t t e d i n w i t h t h e i n c r e a s e o f Iweig°a t t o 115 p o u n d s , a n d t~he i n c r e a s e o f r e d b l o o d ce l l c o u n t t o 4 ,100,000 a n d t h e h a e m o g l o b i n t o 83 p e r c e n t . t i e w a s n o w a d v i s e d t o d i s c o n t i n u e t h e s a l i c y l a t e s a n d t o r e - d u c e t h e b r o m i d e d o s a g e 50 p e r c e n t , b u t t o m a k e n o c h a n g e o f t h e b a r b i t u r a t e , i r o n a n d h y d r o c h l o r i c a c i d d o s a g e s .
O n J u l y 27, 1944, t h e r e w a s a s t i l l f u r t h e r i m p r o ~ ' e m e n t ~ T h e p a i n h a d d i s a p p e a r e d ; h e h a d b e e n s l e e p i n g w e l l ~ t n i g h t ; t h e p a r e s t h e s i a s WeTC n o t e d p e r i , , d i c a l l y o n l y ; t h e w e i g h , t / had i n c r e a s e d t o 124 p o u n d s ; t h e r e d b l o o d c e l l c o u n t t o 4 ,4400,000 a n d t h e h a e m o g l o b i n t o 87, p e r c u t . t-Ie~ w a s n o w a d v i s e d t o d i s c o n t i n u e t h e b r o m i d e s a n d t h e b a r - b i t u r a t e , b u t to c o n t i n u e w i t h t h e i r o n a n d h y d r o c h l o r i c a c i d .
O n N o v . 3, 1944, a f u r t h e r i m p r o v e m e n t o f h i s g e n e r a l c o n d i t i o n , w a s n o t e d a n d , a t t h e n e x t v i s i t ()n M a r c h 1, 19.t5, b.e l o o k e d a n d s t a t e d h e f e l t , " v e r y w e l l " : a n d h e s t a t e d t h a t
*TFhe t e s t s f o r f r e e h y d r o c h l o r i c a c i d in t h e v o m i t u s w e r e
n e g a t i , ve .
h- had been working 12 to 13 hours a day and sleeping 7 to 8 hours a night for oveT a month: the weight ha d in- creased to 151 pound.s. The red blood cell count was 4,600,-, 000 and ti~e haemoglobin 93 per cent. T~he iron t reatment was therefore, di~con,t~nued, but he was advised ~o eon,tinue with the hydrochloric acid. Since then, the history has-been u n e v e n t f u l , e ~ c e l ) t t h a t h e h a s b e c o m e c a r e l e s s w i t h t h e d i e t .
The experiences with two somewhat similarly severe cases (M. J. M. and H. St. M.) may be noted her.e, though the diagnosis of the type of neuritis was not as simple, i11 both cases, however, the experiences pointed similarly to henefical effects o[ the hydrochloric acid treatnlent.
B o t h w e r e o f a d v a n c e d a g e s ~ 72 a n d 79 y e a r s r e s p e c - t i v e l y : b o t h h a d s c i a t i c n e r v e i n v o l v e m e n t a n d , a l s o , f a i r l y a d v a n c e d a r t e r i o s c l e ' r o s i s , w i t h a b s e n t p u l s a t i o n s i n t h e d o r s a l i s 1)edis a n d p o s t e r i o r t i b i a l a r t e r i e s ; b o t h h a d h y p e r - t e n s i o n a n d , in b o t h , t h e p i c t u r e w a s c o m p l i c a t e d b y o s t e o - a r t h r i r t i e c h a n g e s . In t h e c a s e o f M. J . M. , a l c o h o l w a s a n a d d i t i o n a l c o m p l i c a t i n g f a c t o r . I n b o t h , t h e h y p e r g l y c a e - m i c t y p e o f n e u r i t i s a p p e a r e d to b e e x c l u d e d , i n v ie ,w o f t h e s a t i s f a c t o r y c o n t r o l o f d i a b e t e s ; b u t , b e c a u s e o f ~the ad, v a n c e d a g e s a n d t h e a r t e r i o s c e l e r o t i c a n d o s t e o a r t h r i e c h a n g e s . I t ~ s d i f f i , c u l t t o r u l e o u t bhe p o s s i b i l i t y o f t h e c i r c u l a t o r y 1 a n d the ' d e g e n e r a t i v e t y p e s o f n e u r i t i s . I n n e i t h e r c a s e w ~ s t h e r e a n y h i s t o r y s u g g e s t i v e o f a t t a c k s o f i n t e r m i t X e n t c l a u d i c a t i o n . T h a t e a c h w a s a c a s e o f t y p i c a l d i a b e t l c ~ n e u r i t i s , h o w e v e r , s e e m e d c l e a r f r o m t h e facr~ thaJ t ~he n e u r - i t i s w a s t h e m a j o r c o m p l a i n t ; t ' he o n s e t o f t h e p a i n h a d b e e n s u d d e n a n d m u c h m o r e s e v e r e a t n i g h t ; t h e r ~ h a ~ b e e n r a p i d p r o g r e s s i o n o f w e a k n e s s o f t h e m u s c l e s a n d t h e p a r e s t h e s i a s w e r e m a r k e d .
T h a t t h e d i a b e t e s w a s n o t a n i m p o r t a n t c o n t r i b u t i n g f a c - t o r m a y b e s e e n f r o m t h e f o l l o w i n g t e n c o n s e c u t i v e b l o o d s u g a r d e t e r m i n a t i o n s in e a c h c ~ s e :
M . J . M . : 0 .153 0.111 0.125 0 .166 0.100 0.100 0.143 0.143 0.111 0 .120
H . S t . M . : 0 .133 0.09,9 0.085 0.114 " 0 .090 0.IIi 0.III 0.I00 0.12'0 0.133
Following institution of ?she treatment with the hydro- chloric &cid, in the case of M.J.M., the neuritis had com- pletely cleared up within less than a month: treatmen£ was instituted on June 6, 1943, and, at his vi.sit on July 5, he stated that he had been completely free from all symptOm~ fo,r a b o u t a w e e k p r e c i o u s l y .
I n t h e , c a s e o f H . ~ t . M . , t h e p a i n w h e n h e ~ a s f i r s t s e e n w a s so s e x ' e r e t h a t h e w a s u n a b l e t o s i t i n a c h a i r . H e w a s , t h e r e f o r e , a d m i V t e d t o t h e h o s p i t a l a n d , a s r e c o r d s s h o w (I-Iosp. N o . 2 7 2 3 / 4 4 ) t h e p ~ i n h a d s o d e c r e a s e d f o l l o w i n g t h e t r e a t m e n t lwit~h h y d r o c h l o r i . c a c i d t h a t h e w ~ s a b l e t o l e a v e t 'he h o s p i t a l e l e v e n d a y s l a t e r . A t h i s visi~t o n O c t . 11, 1944,~ s e v e n week , s l a t e r , h e w a s c o m p l e t e l y f r e e f r o m a l l s y m p - t o m s .
It would thus appear that. in both ot these cases, the neuritis had been due to deficiency of vitamine BI which required no other treatment than lowering of the pH in the gastric and duodenal secretions, so as to prevent destrttction of the vitamine BI content of the diet.
The idea that vitanfine Bt deficiency nfight explain typical diabetic neuritis is not new.* Needles (27) found no deficiency of this vitamine in the diets of his cases of neuritis, but the possibility of its destruction by high pH in the stomach and duodenum were not cott- sidered. The possibility of defective absorption is men- tioned, bttt apparently no experiments had been made to test this possibility. A relative deficiency as a result

328 T H E AMERICAN JOURNAL OF DIGESTIVE DISEASES Volume 16 Number
of a high carbohydrate intake and also possibly loss due to polyuria (28,29) may at times, be a consideration. In the above-described cases, however, there had been no change of the carbohydrate intake during the period of observation, and, as the diabetes was under good control, there was no polyuria.
That destruction of the vitamine B~ in the diets of both of these cases was the dominant factor in the pro- duction of the neuritis is also suggested from the de- calification of the bones of the feet in both of these cases and from the known relationship between the pH in the duodenum and absorption of calcium. As pointed out previously (19) in addition to vitamine D and other substances in the diet f o r normal bone metabolism, efficiem absorption of calcium from the diet is also es- sential The evidenc~ of the many ~ttempts to corre- late impaired absorption with the decrease in the solu- bility of phosphates of calcium in high pH media is confusing, but that soluble calcinm salts are essential and that an acid reaction in the upper part of the in- testinal tract aids in solution of calcium compounds seems clear from a number of observations. For ex- ample, rarefaction of bones of puppies following gas- trectomy may be prevented to a large extent, and parti- ally corrected, by addition of soluble calcium salts to the diet (18). Relevant here, therefore, is the fact that the acid phosphate of calcium is more soluble and, therefore, more readily absorbed, than the basic phos- phate, and whether calcium is primarily in the acid or basic form depends upon the pH of the medium. A priori, therefore, any condition which tends to decrease the acidity in the duodenum (increase the ph) tends to impair absorption of calcimn and achlorhydria is one of these conditions.
Use of hydrochloric acid for the neuritic manifesta- tions of diabetes is not new, but evaluation of the results reported - - failures and successes - - is difficult be- cause of failure to differentiate between the different types of neuritis met with in diabetes : failure to differ- entiate between cases with achlorhydria and those with normal gastric acidities, and also lack of control by use of two or more therapeutic measures at the same time. As the literature shows, differentiation of the types of neuritic manifestations as by Jordan (3) and Treusch (30) have been exceptions, and, as is well known, ad- justment of the diabetes alone suffices in most cases to improve neuritis of the hyperglycaemic type. Here the dominant factor is probably a toxic one, rather than vitamine deficiency. With poor control of the diabetes fatty infiltration of the liver is common, and with fatty infiltration, the probability, as the writer has shown (11), is that there is also some impairment of the de- toxifying function. Proper conclusions from simnl- taneous adjustment of the diabetes and administration of hydrochloric acid in such cases is thus obviously difficult. That achlorhydria is not the only factor, even in typical diabetic neuritis, is suggested from the resis- tance to treatment noted at times even in such cases, though, here, a factor in practically all of the writer's
*For l i terature, see Ref. Nos. 2, 3 and 26.
cases had been the long duration of the neuritis before the hydrochloric acid treatment had been instituted and thus possibly development of irreparable changes in the nervous tissues. Three cases only, however, regardless of how striking the findings may have been, do not af- ford proof of the effectiveness of any treatment upon any disease. The aJbove three cases were cited merely because (a) they were amongst the earliest experiences with hydrochloric acid (b) the neuritis in each case was very severe and the findings, therefore, more significant and (e) in each case it was possible to differentiate fairly clearly between typical diabetic neuritis and the hyperglycaemic, circulatory and degenerative types. Since then, however, the writer has carefully controlled data of use of hydrochloric acid, with and without vit- amine B1 therapy, in a large group of cases, which will the subject-matter of a separate comnmnication. In this study, the subjects are being grouped according to (a) the type of neuritis (b) the degree of control of the diabetes and (c) the treatment otherwise - - vit- amine B1 alone for a long time; hydrochloric acid alone; hydrochloric acid preceded by vitamine B1, and hydrochloric acid and vitamine B1 combined.
ACHLORttYDRIA AND DIGESTIVE DISTURBANCES
On much more speculative grounds than the associa- tions of anaemia and neuritis with achlorhydria is the association noted between the latter and digestive dis- turbances. The data, however, are sufficiently suggestive and, as will be noted, of sufficient practical importance to warrant their publication so that others with simil- arly large groups of cases and laboratory facilities may add their experiences.
As stated, a random sample of a large group of dia- betics will show that the incidence of digestive distur- bances - - coated tongue, loss of appetite, nausea, vague epigastric discomfort unrelated to meals, belching, bloating, a sense of fulness and fluid regurgitation after meals, abdominal distension, etc. - - is high. Also, though the symptoms of achlorhydria are poorly defined the sbove, it should be noted, correspond almost ex- actly with the syndrome of achlorhydria described by Goodman and Gilman (25) and, for which, according to these authors, hydrochloric acid has been found ef- fective in a significant percentage of cases.
A causal rather than an accidental association be- tween achlorhydria and digestive disturbances is sug- gested from a number of experiences. For example, all ten cases of diarrhoea of diabetes reported by Bowen and Aaron (31) had achlorhydria, and, in Joslin's group, 14 of 29 cases showed achlorhydria even after histamine (2). Achlorhydria is frequently associated with the alternating constipation and diarrhoea of dia- betes and also with the nocturnal incontinence of faeces. Thus, as Shay, Gershen-Cohen and Fels (32) have pointed out, it would appear that anacidity is of real clinical significance; that it not only indicates a loss of gastric function, but also conditions disturbed physio- logical states in parts of the body often quite remote from the stomach. Gradwohl (33) noted improvement

A. a. D . D . ACHLORItYDRIA AND ITS CLINICAL SIGNIFICANCE IN DIABETES MELLITUS 3 ~ September, 1949
of symptoms following use of hydrochloric acid in cases of dia:betes with achlorhydria.
How achlorhydria might account for digestive symp- toms is suggested from the known facts about the pH in the gastro-intestinal tract and how the latter may in- fluence bacterial activity. Normally, even the secre- tions of the resting stomach contain appreciable amounts of free acid. In general, the free hydrochloric acid and total acidity of gastric juice are such that its pH ranges between 0.9 and 1.5, which accounts for its powerful antiseptic properties: streptococci, staphylo- cocci and B.Coli are readily destroyed. As a rule, there- fore, the duodenal contents are virtually sterile. In the duodenum, the acidity varies in proportion to the acid- ity of the chyme from the stomach, and the volume of alkaline fluids especially from the pancreatic juice. The type of food and stage of its digestion are also factors - - meat tends to increase the acidity. As a rule, the pH ranges between 6 and 7 and is thus still on the acid side. In the small intestines, below the duodenum, the reaction is also still as a rule acid, thongh only sligh~y, due chiefly to the organic acids produced by the fer- mentative bacteria - - acetic, butyric, lactic from carbo- hydrates, etc. The pH then increases so that faeces are usually either neutral or alkaline (ph 7.0 - 7.5), all of which influence the bacterial flora. In general, begin- ning with the duodenmn, bacteria are found in increas- ing numbers, until they nmy account for 20 to 30 per cent of the dry weight of faeces and 50 per cent of its nitrogen. In the small intestines, their action is, as stated, dominantly fermentative: whereas, in the large intestines, the dominaut action is putrefactive, and some of the products of this putrefaction are toxic - - try- amine, ethylamine, indole, skatole, phenol cresol, hist- amine, etc. Normally. however, the large intestine is well equipped to resist passage of toxic products into the blood stream, and, as a further protection, there is the powerful detoxifying capacity of the liver to deal with toxic products that have passed the intestinal bar- rier and entered the portal circulation, b'or example, though normally there are about 50 mgms. of indole in 100 gms. of dry faeces and, though, as nmch as one gram of indole administered orally may not produce an 3, symptoms and, even, 2 grams cause some dizziness and slight headache only (183, with failure of the de- toxifying function of the liver, administration of as little as 25 mgms. may produce loss of appetite, belch- ing, nausea and headache (11).
\Vith achlorhydria, the picture changes. It is only so long as the nficro-organisms of the acid producing type flourish that any bacteria from the large intestines which may have invaded the small intestines are unable to gain a foothold. Even with temporary achlorhydria, the duodenum may be rapidly invaded by micro-organ- isms from the colon (18) and the combination of alka- linity and lack of available oxygen favour the growth of obligate anaerobes in the metabolism of which re- ducing reactions predominate: biliru'bin is reduced to colourless urobilinogen, sulphur and even sulphates to hydrogen sulphide. Many dyes and pigments (for ex- ample, methylene blue and litmus) are decolourized,
bisnmth salts are converted into the suboxide, but more relevant here is the increased production of the above- mentioned putrefactive substances (34). Furthermore, the small intestines are not as well equipped as the large intestines to resist passage of toxic products into the blood stream (18). In view of the above observa- tions, an attempt was made to determine the extent to which, if any, the a~bove-mentioned digestive disturb- ances are due to intestinal putrefaction as the result of achlorhydria.
TESTS OF PUTREFACTION
Of the nmnerous tests of putrefaction in the intest- inal tract, those for indican in the urine were selected for this study for a number of reasons. Indican is de- rived from indole, which is one of the products of put- refaction which is toxic. Also, differing from the other ethereal sulphates is the fact that the latter are derived from protein metabolism, whereas indican arises, in great part, if not wholly, from putrefaction. That it may alone be taken as a rough index of the extent of the putrefaction changes is generally accepted (18,34, 35). Indican itself is not toxic. It is well-known that large amounts of indican may be found in the urine of apparently healthy individuals. It, therefore, would not account for the above-mentioned digestive disturb- ances. As in the case of the increase of the blood ure~ nitrogen in uraemia, however, an excess might point to excess production of other products which are toxic, and which are not being detoxified as readily as indole. Suggestive, for example, are the high incidences of in- dicanuria noted in gastro-intestinal conditions associ- ated with headache, nausea, vomiting, etc. Suggestive also were Soper's (36) findings in his study of "toxic~ headache", in the diagnosi,s of which nasal sinus condi- tions, eye disorders, syphilis, allergy, hypertension, etc., were excluded; amongst a group of 696 such cases, ex- cess quarrtities of indican were found in 85 per cent. .ks a preliminary step in this investigation, therefore, an attempt was made to determine the incidence of excess indicanuria amongst diabetics, compared with the gen- eral incidence.
SELECTION OF TESTS FOR IlqDICAN
Normally, the excretion of indican ranges between 4 and 20 mgms. per day. Quantitative tests such a s Ellinger's (37), Askenstedt's (38), or Parker's modifi- cation of the latter (34) are, however, time-consuming and, therefore, not practical on a large scale. Provided, however, that the intensity of the colour produced by urine with indican concentration which correspond to the upper limit of the normal excretion is taken as th~ standard of normality, and that careful attention is paid to details - - use of freshly voided urine only; removal of interfering substances; uniform proportions of urine and reagents*; allowance for maximum colour develop- ment, etc.,--and provided the conclusions are statistical --based upon a large number of observations and not upon simple tests--such simple qualitative procedures as the Obermeyer, Jolle and Jaffe yield useful informa- tion. They are not, however, equally sensitive. Thet Jaffe test is the least satisfactory due to the ease Wifli
~ ' ~ 0 T H E A M E R I C A N J O U R N A I . OF D I G E S T I V E D I S E A S E S V o l u m e 16 N u m b e r 9
which overoxidation may occur by use of calcium hypo- chlorite as the oxidizing agent. Jolle's test is by far the most sensitive. However, in this study, all three were used in every c a s e .
I N C I D E N C E OF E X C E S S I V E I N D I C A N U R I A I N D I A B E T E S
To determine the incidence of indicanuria amongst di- abetics in general, tests were performed in 500 consecu- tive cases and, amongst them, excess excretions, accord- ing to the above-mentioned standard, were found in 198 - - a n incidence of 39.6 per cent. This, it will be noted, was over twice the incidence reported by Soper (36) in a large group of individuals in general.
R E L A T I O N S H I P ] ~ E T W E E N . S t C H L O R H Y D R I A A N D
E X C E S S I N D I C A N U R I A
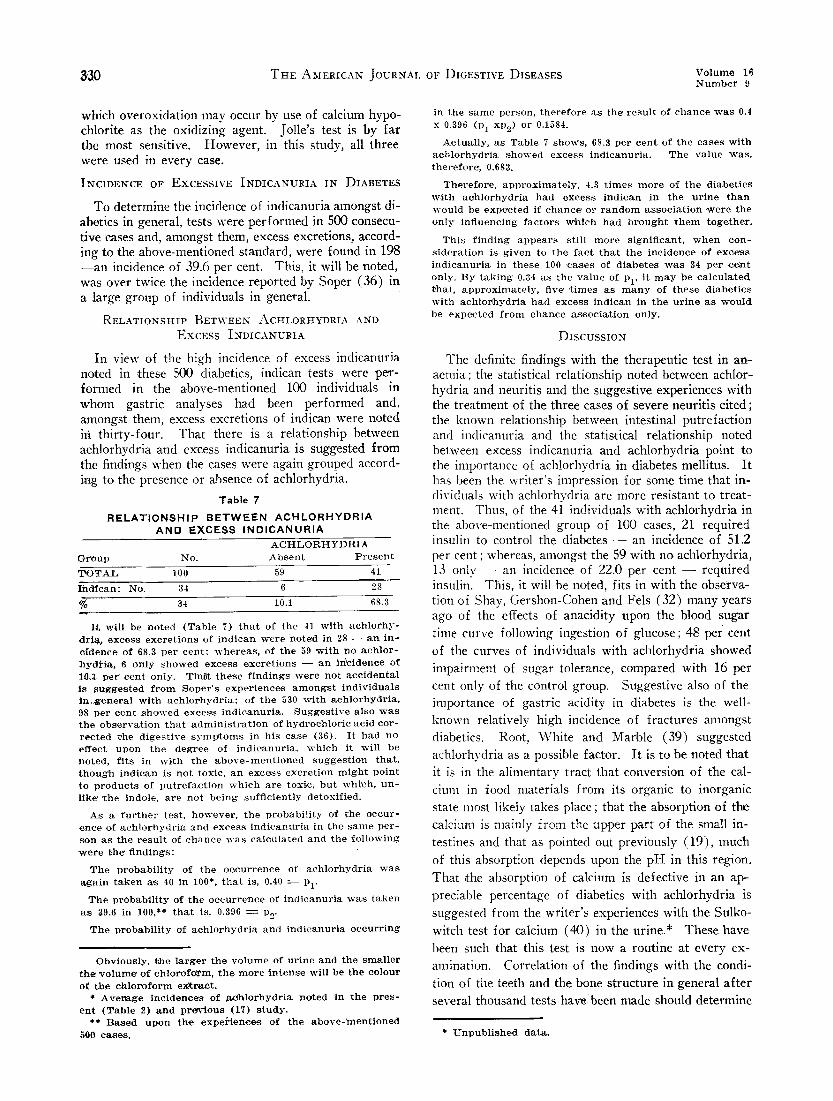
In view of the high incidence of excess indicanuria noted in .these 500 diabetics, indican tests were per- formed in the above-mentioned 100 individuals in whom gastric analyses had been performed and, amongst them, excess excretions of indican were noted ili thirty-four. That there is a relationship between achlorhydria and excess indicanuria is suggested from the findings when the cases were again grouped accord- ing to the presence or absence of achlorhydria.
Table 7
R E L A T I O N S H I P B E T W E E N A C H L O R H Y D R I A A N D EXCESS I N D I C A N U R I A
A C H L O R H Y D R I A G r o u p N o . A b s e n t P r e s e n t
T O T A L 100 59 41
I h d f c a n : N o . 34 6 28
% 34 10.1 68.3
I t w i l l b e n o t e d ( T a b l e 7) t h a t o f t h e 41 w i t h a c h l o r h y - ,d r ia , e x c e s s e x c r e t i o n s o f i n d i c a n w e r e n o t e ' d in 28 - - a n i n - e f d e n c e o f 68.3 p e r c e n t ; w h e r e a s , o f t h e 59 w i t h n o a c h l o r - h y d H . a , 6 o n l y s h o w e d e x c e s s e x c r e t i o n s - - a n i f f c i d e n c e o f 1 0 3 p e r C e n t o n l y . T h a t t h e s e f i n d i n g s w e r e n o t a c c i d e n t a l i s s u g g e s t e d f r o m S o p e r ' s e x p e r i e n c e s a m o n g s t i n d i v i d u a l s i r~ .~genera l w i t h a c h l o r h y d r i a " o f t h e 530 w i t h a c h l o r h y d r i a , 98 p e r c e n t s h o w e d e x c e s s i n d i c a n u r i a . S u g g e s t i v e a l s o w a s t h e o b s e r v a t i o n t h a t a d m i n i s t r a t i o n o f h y d r o c h l o r i c a c i d c o r - r e c t e d t ,he d i g e s t i v e s y m p t o m s i n h i s c a s e (36) . I t h a d n o e f f e c t u p o n t h e d e g r e e o f i n d i c a n u r i a , w h i c h i t w i l l b e n o t e d , f i t s i n w i t h t h e a b o v e - m e n t i o n e d s u g g e s t i o n t h a t , t h o u g h i n d i e a n i s n o t t o x i c , a n e x c e s s e x c r e t i o n m i g h t p o i n t t o p r o d u c t s o f p u t r e f a c t i o n w h i c h a r e t o x i c , b u t w h i ' e h , u n - l ike ' ' t h e i n d o l e , a r e n o t b e i n g s u f f i c i e n t l y d e t o x i , f i e d .
A s a f u r t h e r t e s t , h o w e v e r , t h e p r o b a b i l i t y o f t h e o c c u r - e n e e o f a c h l o r h y d r i a a n d e x c e s s i n d l c a n u r i a i n t h e s a m e p e r - s o n a s t h e r e s u l t o f c h a n c e w a s c a l c u l a t e d a n d t h e f o l l o w i n g w e r e t h e f i n d i n g s :
T h e p r o b a b i l i t y o f t h e o c , c u r r e n c e o f a c h l o r h y d r i a w a s
a g a i n t a k e n a s 40 i n 100" , t h a t i s , 0.40 ~ - Pl"
T h e p r o b a b i l i t y o f t h e o c c u r r e n c e o f i n d i c a n u r i a w a s t a k e n
a s 39.6 in 100,** t h a t i s , 0.396 = P2"
T h e p r o b a b i l i t y o f a c h l o r h y d r i a a n d i n d i e a n u r i a o c c u r r i n g
O b v i o u s l y , t h e l a r g e r t h e v o l u m e o f u r i n e a n d t h e s m a l l e r t h e " ¢ o l u m ~ o f c h l o r o f o r m , t h e m o r e i n t e n s e w i l l b e t h e e o l o u r
o f t h e c l a l o r o f o r m e x t r a c t . * A v e r ~ g e i n c i d e n c e s o f ~ 0 h l o r h y d r i a n o t e d i n t h e p r e s -
e n t ( T a b l e 2) a n d p r e v i o u s (17) s t u d y . ** B a s e d u p o n t h e e x p e r i e n c e s o f t h e a b o v e - m e n t i o n e d
5 0 0 c a s e s .
in t h e s a m e p e r s o n , t h e r e f o r e a s t he ' r e s u l t o f c h a n c e w a s 0A
x 0.396 ( P l x P 2 ) o r 0.1584.
A c t u a l l y , a s T a b l e 7 s h o w s , 68.3 p e r c e n t o f t h e c a s e s w i t h a c h l o r h y d r i a s h o w e d e x c e s s i n d i c a n u r i a . T h e v a l u e w a s . t h e r e f o r e ' , 0.683.
T h e r e f o r e , a p p r o x i m a t e l y , 4.3 t i m e s m o r e o f t h e d i a b e t i c s w i t h a ( ~ h l o r h y d r i a h a d e x c e s s i n d i c a n i n t h e u r i n e t h a n w o u l d b e expe~c ted i f c h a n c e " o r r a n d o m a s s o c i a t i o n w e r e t h e o n l y i n f l u e n c i n g f a c t o r s v c h i c h h a d b r o u g h t t h e m t o g e t h e r .
T h i s f i n d i n g a p p e a r s s t i l l m o r e s i g n i R c a n t , w h e n c o n - s i d e r a t i o n is g i v e n t o t h e f a c t t h a t t h e i n c i d e n c e o f e x c e s s i n d i c a n u r i a i n t h e s e 100 ' c a s e s o f d i a b e t e s w a s 34 p e r c e l a t o n l y . B y t a k i n g 0.34 a s t h e v a l u e o f P l ' i t m a y b e c a l c u l a t e d . t h a t , a p p r o x i m a t e l y , five" t i m e s a s m a n y o f t h e s e d i a b e t i c s w i t h a e h l o ~ h y d r i a h a d e x c e s s i n d i c a n i n t h e u r i n e a s w o u l d b e e x p e c t e d f r o m c h a r m e a s s o c i a t i o n o n l y .
D I S C U S S I O N
The definite findings with the therapeutic test in an- aemia; the statistical relationship noted between achlor- hydria and neuritis and the suggestive experiences with the treatment of the three cases of severe neuritis cited; the known relationship between intestinal putrefaction and indicanuria and the statistical relationship noted between excess indicanuria and achlorhydria point to the importance of ach!orhydria in diabetes mellitus. It has been the writer's impression for some time that in- dividuals with achlorhydria are more resistant to treat- ment. Thus, of the 41 individuals with achlorhydria in the above-nlentioned group of 100 cases, 21 required insulin to control the diabetes - - an incidence of 51.2 per cent ; whereas, amongst the 59 with no achlorhydria, 13 only - - an incidence of 22.0 per cent - - required insulin. This, it will ,be noted, fi`ts in with the observa- tion of Shay, Gershon-Cohen and Fels (32) many years ago of the effects of anacidity upon the blood sugar time curve following ingestion of glucose; 48 per cent
of the curves of individuals with achlorhydria showed impairment of sugar tolerance, compared with 16 per cent only of the control group. Suggestive also of the importance of gastric acidity in diabetes is the well- known relatively high incidence of fractures amongst diabetics. Root, White and Marble (39) suggested achlorhydria as a possible factor. It is to be noted that it is in the alimentary tract that conversion of the cal- cium in food nmterials from its organic to inorganic state most likely takes place; that the absorption of the calcium is mainly from the upper part of the small in- testines and that as pointed out previously (19), much
of this absorption depends upon the pH in this region.
That ,the absorption of calcium is defective in an ap- preciable percentage of diabetics with achlorhydria is suggested from the writer's experiences with the Sulko- witch test for calcium (40) in the urine.* These have been such that this test is now a routine at every ex- amination. Correlation of the findings with the condi- tion of the teeth and the bone structure in general af ter several thousand tests have been made should determine
* Unpublished dat~.

A. a. D . D . ACttLORHYDRIA AND I T S C L I N I C A L S I G N I F I C A N C E I N D I A B E T E S M E L L I T U S 331 S e p t e m b e r , 1949
the extent t() which this test is of value in the routine managment of the diabetic.**
SUMMARY
A studv was made of the occurrence of anaemia, neuritis and digestive disturhances in diahetes melli- tUS and their association with achlorhvdria.
The association of each of these conditions with ach.-
lorhvdria was more than would be expected if chance
or random association were the only influencing factors
which had brought them together.
()11 the assumption that the anaenaia in many cases of
diabetes with achlorhvdria is due to a high pH of the
duodenal secretions which interferes with liberation of
** E v e n i f d e t e r m i n e d q u a n t i t a t i v e l y , t he ' u r i n a r y e x c r e - t i o n o f c a l c i u m is a l o n e o f l i m i t e d v a l u e in d ~ < e r m i n i n g thel de~al'ee o f i t s absc ) r l ) t i (m , sill('(, it ln;.ty a c e H u u t f()r a n y w h e l ' e fl'illT1 10 tO 41} l ~ e r e e n t u f the" t o t a l OUtl)ut . ' P h e r e f o r e , s t i l l l e s s i n d i c a t i w , o f t h e d e g r u e (~f u b s o r p t i o n o f c a l c i u m is t h e
," . . lulkuwiteh t e s t , s i n c e , e v e n a s m o d i f i e d b y t h e w r i t e r , i t i s q u a l i t a t i v e ~mly. L i k e t h e p e ' r e e n , t a g e o f s u g a r in t h e u r i n e , h o w e v e r , a v e r a g e s b a s e d u p o n v e r y l a r g e n u l n b e r s of t e s t s m i g h t y i e l d u s e f u l i n f o r m a t i o n , p r o v i d e d t h e y a r e s u b j e c t e d to t h e lU'l)per s t a t i s t i c a l t r e a t n l e n t 1o d e t e r m i n e t h e i r s i g n i f i , ( . a n c e .
T h i s w o r k w a s d o n e w i t h t h e a i d o f at g r a n t f r o m t h e S u g a r R e s e a r ( . h F o u n d a t i o n , Inc . , N e w Y, ) rk .
R I { F I ' ; R E
1. l g a b i n [ ~ w i t c h , I . M . , l ) i a b e t e s m e l l i t u s , A m . J . D i g . D i s . , 16: 95, ]949.
2. J o s l i n , E. P . , e t a l , T h e T r e a t m e n t o f D i a b e t e s M e l l i t u ~ , ,';th Ed. , ( L e ' a & F e b i g e r ) 1946.
3. J ( ) r d a n , W. R., N e u r i t i c m a n i f e s t a t i o n s in d i a b e t e s m e l l i - t u s , A r c h . I n t . M e d . , 57: 307, 1,q36.
4. M e a d . R, c i t e d b y \ V a t ' r e n , S h i e l d s , T h e P a t h o l o g y off D i a b e t e s M e l l i t u s ( L e a & V e b i g e r ) 19:/0.
5. B e s t , C. H . , F e r g u s o n , G. C.. & H e r s h e y , J . M., C h o l i n e . a n d l i v e r £at in d i a b e t i c d o g s , J . P h y s i o l , 79: 94, t 9 3 3 .
6. B e s t C. i-I., & S, h a n n o n , H . a . , T h e a c t i o n o f c h o l i n e a n d o t h e r s u b s t a n c e s in t h e p r e v e n t i o n a n d c u r e o f f a t t y l i v e r s , B i o c h . J., 29: 2651, 1935.
7. H a n s s e n , P., E n l a r g e m e n t (ff t h e live'Y i n d i a b e t e s m e l l i - t u s , J . A . M . A . , 106: 914, 1936.
S. \V,hi te , t ' r i s e i l l a , q u o t e d b y . l o s l i n , E . P , N e w E n g a . Med . , 209: 519, 1933.
~. \V,hi, te , P r i s c i l l a , D i a b e t e s in C h i l d h o o d ( L e a & F e b i g e r ) 1932.
10. R a b i n o w i t c h , I. M., F ] f f e c t s o f b e t a i n e u p o n t h e c h o l e s - t e r o l a n d b i l i r u b i n c o n t e n t s o f t h e b l o o d p l a s m a i n d i a - b e t e s m e l l i t u s , C a n . Meal. A s s o c . J . , 34: 137, 1936.
11. R a b i n o w i t e h , I . M . , R e ' l a t i o n s h i p b e t w e e n i m p a i r m e n t o f l i v e r f u n c t i o n a n d p r e m a t u r e d e v e l o p m e n t o f a r t e r i o s - c l e r o s i s in d i a b e t e s m e l l i t u s , C a n M e d . A s s o c . a . , 58: 547' 1948.
12. R a b i n o w i t e h , I. M., T h e v a n d e n B e r g h r e a c t i o n in d i - a b e t e s m e l l i t u s , B r i t . a . E x p . P a t h . , 7: 155, 19')6.
13. R a b i n o w i t c h , I. M., A n o t e o n t h e b i l i r u b i n c o n t e n t o f b l o o d a n d u r b i l i n t , g e n c o n t e n t o f u r i n e in d i a b e t e s m e l l i - t u s . B r i t . . 1 . E x p . P a t h . , 12: 249. 1936.
14. ( t r a y . ~. J. , Ho()k. \V. . & B a t t y , .I. I~. . l a v e r f u n e t b , n
s t u d i e s in d i a b e t e s m e l l i t u s . A n n . I n t . M e d . , 24: 72, 1946. 15. M o n t e , T. K., M a n u a l o f M e d i c i n e , 2n(l 15(1. ( B a i l l i e r e ,
T i n d a l l & ( ' o x ) 1906. p. 241.
16. B a s s l e r , A.. & P e t e r s , A. ¢1., D i a b e t i c i n d i g e s t i o n , a k n n . I n t . iVied., 30: 74(I, 1M9.
17. R a b i n o w i t ( . h , I. M., V,~wler , A.t, ' . , & W a t s o n , B. A., G a s -
iron from the food materials; with its conversion to the ferrous form and also with its absorption, an at- tempt was made to treat the anaemia with hydrochlorie acid onh'. Statistically, this resulted in an increase of the red blood cell count. That the difference - - average increase of red blood cell count - - noted was signifi- cant was found l)v the ratio of the difference to its i)robable error.
()n the assumption that typical diaSetic neuritis is due to a combination of destruction and defective ab- sorption of Vitamine B~ due to a high pH of the gastric and duodenal secretions, an attempt was made to treat such cases of neuritis with hvdrochloric acid only. The results in the three cases of severe neuritis cited suggest that this is probably the correct explanation.
A sttulv was made of the occurrence of excess ex- cretions of iudican in the urine in diabetes mellitus and, c .mpared with that noted in non-diabetics, the incidence was high and defingely higher amongst a group with ach!f)rhvdria than amongst the control group. The association of the excess excretions with aehlorhydria was m~,re than would be expected if random or chance association were the (mlv influencing factors which, had bronght then1 together.
The prohable relationships between achlorhydria and other disturl)ances met with in diabetes mellitus are brief h discussed.
N C E S
tH( . a c i d i t y i n d i a b e t e s m e l l i t u s , A r c h . I n t . M e G 41: a84 , 1936.
1,~. Bes, t , C. H . , & T a y l o r . N . B. , T h e P h y s i o l o g i c a l B a s i s o f M e d i c a l P r a e t i e e , 3 r d Ed . , ( V ¢ i l l l a m s & V ¢ i l k i n s ) 1943 ) .
I:L R a b i n o w i t c i l , I. 5I. , I n a d e q u a t e n u t r i t i o n wil~h a d e q u a t e d i e t s ; C a n . H o s p . J . , 25: 44, N o v . , 1948; 25: 46, D e c . , 1948.
2(L A l l i s o n , J . T. , T h e r e l a t i o n o f h y d r o , c h l o r i c a c i d ~pxl v i t a m i n e B c o m p l e x d e l i c i e n e y in c e r t a i n s k i n d i s e a s e s , S o u t h . M e d . J . , 38: 235, 1945.
2 l . H u r s t , A . F . , A c h l o r h y d r i a , L a n c e t , 1: 111, 1923. 22. g g g l e s t o n , E. L. . ( l a s t r i e s e c r e t o r y d i s t u r b a n e e s , B u l l .
t ; a t t l e " ( ' r e e k S a n . & H o s p . C l i n i c , 20: 89, 1925. 23. B e n n e t t , T. I. & ~ y l e , J . A., S t u d i e s in g a s t r i e s e c r e t i o n ,
G u y ' s H o s l ) . R e p . , 71: 286, 1921. 24. R a b i n o ~ i t c h , I. M.. T h e i n c i d e n e e o f d i a b e t e s m e l l i t u s i n
d i s e a . s e o f t h e g a l l b l a d d e r a n d i t s p a s s a g e s , C a n . M e d . A s s o c . J . , 14: 296. 1924.
25. G o o d m a n , L . & ( l i l m a n , A.. T h e P h a r m a c o l o g i c a l B a s i s o f T h e r a p e u t i c s ( M a c m i l l a n ) 1941.
26. R o o t , H . F . , & R o g e r s , M. H. , D i a b e t i c n e u r i t i s w i t h p a r a l y s i s , N e w E n g . J . M e d , 202: 1049, 1930.
27. N e e d l e s , V¢., V i t a m i n s t u d i e s i n e a s e s o f d i a b e t i . c h e p a t - i t i s , A r c h . N e u r o l . & P s y c h . , 41: 1222, 1939.
28. Q u e r i e s a n d M i n o r N o t e s , V i t a m i n B c o m p l e x i n d i a b e t e s m e l l i t u s , J . A . M. A., 129: 839, 1945.
29. H o o t , H. F . , & M a s e a r e n h a s , C. C., D i e t i n u n e o n t r o l l e 4 d i a b e t e s p r e c e d i n g a e u t e n e u r o p a t h y , A m & D i g . D i s . , l a : 173, 1!)46.
:;tL T r e u s e h , J . V., D i a b e t i c n e ' u r i t i s , P ro ,c . M a y o C l i n i c , 20: 3:J3, 1945.
31. B o w e n , B. D., & A a r o n , A. H . , G a s t r i c s e c r e t i o n in d i a - b e t e s m e l l i t u s , A r c h . I n t . M e d . , 37: 674, 1926.
32. S h a y , H. , G e r s h o n - ( ' o b e n . J . , & P e l s , S S. , G l u c o s e t o l - e r a n c e in a n a e i d i t y . A m . a . D i g . D i s , 5: 4, 1 9 3 8 - 3 9
aS. ( ; r a d w o h l R . B. H . , C l i n i c a l ' a n d L a b o r a t o r y M e t h o d s a n d D i a g n o s i s , 3 r d E d , vo l . 1, 1). 381 ( M o s b y ) 1943.
34. H a w k , P. B. , & B e r g e i m , O., Prae . t i ' c . a l P h y s i o l o g i c a l ~ ' h e m i s t r y , 1 1 t h I';d., ( B l a k i s t o n ) 1944.

332 T H E AMERICAN IOURNAL OF DIGESTIVE DISEASES Volume 16 - N u m b e r 9
35. Todd, J. C.. & Sanford , A. H., Clinical D iagnos i s and I ~ b o r a t o r y Methods , 9th Ed,, ( S a u n d e r s ) 1940.
36 Soper, H. V~L, The Clinical sign}fieance of indican, Am.
a. Dig. ])is., 3: ,564, 1937.
37 Hawk , P. B., P rac t ica l Phys io logica l Chemis t ry , 8th Ed.,
(Blak is ton) p. 568, 1923.
3.% Askens ted t , F. C., A s imple and improved q u a n t i t a t i v e tes t for indiea~n, N.Y. Med. J., 95: la6a, 1912
3.q. Root, H. V., \Vhite, P, & ,Marble, A, Abnor ma l i t i e s of cal- oium delmsi t ion in .diabetes mel l i tus Arch. Int . Med., 5a: 46, 1934.
40. Barney , J. 1)., & Sulkowi teh , H. %V., P r o g r e s s in the m,~nal_,~ament of u r i n a r y calculi, J. l r ro logy, .37: 7t6, 1937.
The Palpatory Examination of the Paucreas." Description of a New Method
By JOZEF W. GROTT, M.D.
LODZ, POLAND
T he pancreas has long been of clinical interest be- cause of its varied and important functions. Detec-
tion of pancreatic pathology even today is dfficult because of the lack of simple diagnostic procedures, something which the practitioner has long awaited. The work of Obraztzow and Hausmann and that of Chauffard and Rivet on the zona paucreatico-choledochica and of De- jardins on the point douloureaux for the head of the pancreas, represent clinical progress, and we refer also, in the Polish literature, to the Witold Orowski method (1910) which permits examination of the tender point of the head of the pancreas, independently of the vari- able position of the umbilicus.
I have previously described a palpatory method for pancreatic examination in 1935 and a "point doulo- ureux" for the body of the pancreas determined by my palpatory method in the dorsal position. I have noted the trophic changes of the skin in the epigastrium as a new sign of chronic pancreatitis in 1937. In 1946 and 1947, i described my second palpatory me~hod in the standing and sitting positions.
In 1943, Professor P. MaUet-Guy described an inter- esting method of manual examination of the pancreas in which he determines the tender point by deep palpa- tion in the left hypochondrium. By comparing ~he re- sults of my own methods, in the supine and standing positions, with the method of Mallet-Guy in April, 1946, I noticed that these results, with the patient lying on his right side, are much better if performed by the method which I elaborated in detail.
~7"
Fig 1 Grott's first paLp,atory method of pancreas in dorsal position .1935)
THE MODIFICATION OF GROTT
With the patient lying on his right side, the physician stands in front of him, using his right hand for the e x -
Fig. 2. Grott's second palpat~ry method of pancreas in standing position (1946-1947).
amination and employing his left hand on the lower part of the lateral aspect of the patient's thorax. In order to determine if a tender point can be found in the body or tail of the pancreas, whether the organ be enlarged or not, we palpate deeply with the right and in the upper part of the niesogastrium and in the left epigastrium, trying to push the movable viscera from left to right to facilitate palpation. The examining hand is pressed deeply till it reaches the left edge of the vertebral cohunn and until the point is reached where the pan- creas crosses it, and any tenderness or enlargement of the organ noted. In the second stage of this examina; tion we attempt to palpate the tail of the pancreas by starting in the left hypochondrium, going deeply, and diverting the left rectus muscle to the right, and event- uallv noting if either tenderness or enlargement is present in the tail of the-organ. The essential point here is getting outside the lateral edge of the left rectt~ muscle. An X-ray check-up by Prof. Misiewicz, after a bariunt meal, indicated that the stomach and duodenum during such an examination are pushed forward, thus permitting the examining hand to reach the space be- tween the stomach and the vertebral column.
EXAMINATION ~vVITIt P ATI ENT LYING ON LEFT SIDE
The palpatory method above-described lends itself equally well to an examination of the head of the pan- creas, mereh, by placing the patient on his left side. The right mesogastrium is then explored in a similar manner and any enlargement or tenderness in the head of the pancreas ascertained.