acceptability of web-delivered psychosocial...
TRANSCRIPT
ACCEPTABILITY OF WEB-DELIVERED PSYCHOSOCIAL TREATMENT WITH URBAN AMERICAN INDIAN/ALASKA NATIVE CLIENTS ENROLLED IN OUTPATIENT SUBSTANCE ABUSE TREATMENT
Grant Support: NIDA CTN U10 DA13035 (Nunes/Rotrosen), U10
DA013732 (Winhusen), U10 DA015815 (McCarty/Sorensen)
Aimee Campbell, PhD, MSW New York State Psychiatric Institute
Columbia University Department of Psychiatry
Addiction Treatment Technology Summit | Chicago, IL
August 27, 2014

Study Team 2
Ned Nunes, MD Lead Investigator
Aimee Campbell, PhD Co-Investigator
Traci Rieckmann, PhD Co-investigator, Project Manager Western States Node
Dennis McCarty, PhD Co-investigator
Frankie Kropp, MA Project Manager, Ohio Valley Node
Brenda Wood Site PI, City/County, Rapid City, SD
Steve Gilbert Site PI, NARA, Portland, OR
Jennifer Lima, MPH Node Coordinator
Primary Objective 3
To evaluate the acceptability of an interactive, web-based version of the Community
Reinforcement Approach (CRA) with urban American Indian/Alaska Natives (AI/AN)
Study Process
Initial discussions with the CTN AI/AN Special Interest Group and collaborators
Contact with CTN-affiliated treatment programs and initial meetings of interest
Protocol fine-tuning; pre-implementation training and feedback; Portland Area IHS IRB
Post-study sharing of results; interpretation of findings; data checks with program staff and partners
4
Overview and Design
Urban AI/AN clients (N=40)
2 Treatment Program Sites
OR: Native American Rehabilitation Association (NARA)
SD: City/County Alcohol and Drug Programs (CCADP)
Pre/post Design (baseline and 1-wk FU)
8 weeks of TES treatment
32 Core TES Modules
No contingency management
5
Therapeutic Education System 6
Community Reinforcement Approach
Budney & Higgins, 1998; Hunt & Azrin, 1973; Smith, Meyers, & Miller, 2001
TES comparable to clinician-delivered CRA; enhances outcomes
Bickel et al., 2008; Chaple et al., 2013; Christensen et al., 2014; Marsch et al., 2014
Examples: Core TES Modules
Conducting a Functional Analysis
Effective Problem Solving
Drug Refusal Skills Training
Managing Negative Thinking
Steps for Giving Constructive Criticism
Giving and Receiving Compliments
Communication Skills
Sharing Feelings
HIV and AIDS
Drug Use, HIV and Hepatitis
Increasing Self-Confidence in Decision-Making
How to Express Oneself in an Assertive Manner
7
Eligibility
Inclusion Criteria
18 years or older
Enrolled in treatment program
Within first 30 days of treatment
Self-identify as American Indian or Alaska Native
Planned treatment episode of 8 weeks or more
Exclusion Criteria
Insufficient ability to provide informed consent
Insufficient ability to use English to participate meaningfully in TES
8
Outcomes: Acceptability
Quantitative Proportion that agreed to participate Number of modules completed Seven acceptability indicators (mean score of < 6 on a 10
point scale would be considered necessary to adapt) 1) interest 2) usefulness 3) New information 4) satisfaction 5) relevance 6) likeability 7) ease of understanding
Qualitative (Participant Interviews & Staff Focus Groups)
9
Participant Characteristics (N=40)
Mean age 37.5 yrs (SD=10.9)
48% were female
Primary substance: alcohol (78%); meth (10%); opioids (8%); marijuana (5%)
25% reported < high school education; 57.5% high school or equivalent; and 17.5% > high school
35% full or regular part-time work
55% accessed the internet in the prior month (42.5% at least once per day)
73% lived on a reservation at some point in their lives
48% are familiar with their native language
10
Acceptability: Quantitative
68 clients approached; 47 brief screens; 41 baselines
40 enrolled (59% of those approached)
37 participants completed at least one module
Mean number of modules = 18.6 (SD=9.2)
Mean acceptability ratings (scale 0-10)
Usefulness 8.54 (SD=1.9)
Satisfaction 8.49 (SD=1.9)
Relevance 8.39 (SD=2.2)
Interesting 8.33 (SD=2.1)
New information 8.26 (SD=2.2)
Likability 8.22 (SD=2.2)
Understanding 7.43 (SD=3.5)
11
Acceptability: Quantitative
Highest rated modules
#30 Drug Use, HIV and Hepatitis (M=9.39, SD=1.2)
#32 Triggers for Risky Drug Use (M=9.25, SD=1.4)
#29 Sexual Transmission of HIV/STIs (M=9.25, SD=1.4)
Lowest rated modules
#4 Self-Management Planning (M=7.76, SD=1.8)
#9 Coping with Thoughts about Using (M=7.81, SD=2.0)
#2 Functional Analysis (M=7.84, SD=1.6)
12
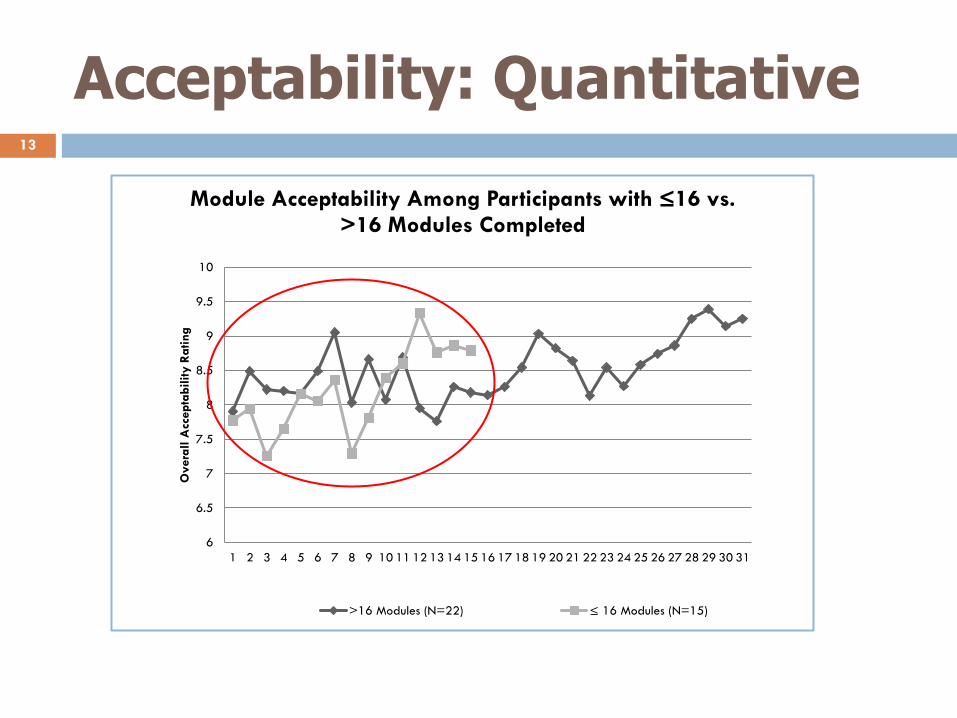
Acceptability: Quantitative 13
6
6.5
7
7.5
8
8.5
9
9.5
10
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31
Overa
ll A
ccepta
bility R
ating
Module Acceptability Among Participants with ≤16 vs. >16 Modules Completed
>16 Modules (N=22) ≤ 16 Modules (N=15)

Acceptability: Qualitative (n=26)
Theme 1: TES information was relevant to overall to addiction treatment and recovery (n=21).
“Oh, I think it’s very appropriate for any culture actually just because it deals with the problems that are here and now, you know?”
“The information that it provided, I shared it with other recovering Natives and it was really informative to them.”
“It just kind of went through, it like it took you like step by step, how to overcome your, you know, your urge or triggers to, to use.”
14

Acceptability: Qualitative
Theme 2: Although the information itself was relevant, the presentation could be more culturally congruent (n=16).
“For what I’m doing personally right now, I think it’s relevant to me. But when you say culture, I think of sweat lodges, I think of ceremonies, I think of powwows, I think of drumming and singing, I think of speaking […] our language. I think about educating […] our children and ourselves culturally. Culturally, I don’t see it.”
“It’s straight […] college type information, exam type stuff. For Native people, I would make it a little more comfortable or a little more spiritual with the speaking.”
“…Maybe they’ll put it off because they’re thinking it’s another way the White man’s trying to tell you how to do things, but if it’s about Natives, maybe we’ll accept it more and use more of it and take it as a tool…”
15

Participant Adaptation Suggestions
Insert humor, Native words or slang, and storytelling
Use Native actors in videos and for voice over
Remove content that might be counter to Native culture
Use references to/depictions of the natural world
Incorporate Native spirituality, especially as it relates to effective coping (e.g., prayer, sweats, drumming)
Include videos that are relevant to AI/AN experience (e.g., returning to the reservation to visit family and being confronted with alcohol and drug use)
16
Staff Feedback
Synergy with treatment-as-usual
Empowering for clients
Clients face challenges making it into program
Computer-assisted modality did not appear to be an issue – even among older clients
Presentation was too academic
Increase cultural representation – better reflect the lives and issues facing urban AI/AN
17
Conclusions
Findings suggest core TES content is acceptable among a diverse urban AI/AN sample
Clinical staff were enthusiastic and interested in ways TES could be integrated within standard care
Targeted adaptation could address concerns related to cultural representation and relevance
Although TES was not culturally tailored to a specific racial or ethnic group, adaptation to enhance relative advantage and compatibility (Rogers, 2003) could enhance program adoption
18
Acknowledgements
Manuscript Co-authors: Michelle Moore, Roz Ringor-
Carty, Eva Turrigiano, Frankie Kropp, Traci Rieckmann, Gloria Miele, Edward Nunes
Participants
Clinical and administrative staff at the treatment programs
Local research teams
Kamilla Venner (Athabascan); Duane Mackey (Santee Sioux) (deceased)
Clinical Trials Network AI/AN Special Interest Group
19