a tool to audit care of mothers in the community
TRANSCRIPT

11Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
A tool to audit care of mothers in the community
Reena Jairus, Indarjit Walia
Correspondence at :
Reena JairusAssistant Nursing SuperintendentCMCH, Ludhiana
Abstract : 'Maternal cards' in the community health care setup are a principal source of information inwhich the documentation of maternal care is an essential part. Maternal Care covers the antenatal and postnatalcare of women with pregnancy, problems during pregnancy, care during puerperium and family planning.Antenatal care is one of the "four pillars" of safe motherhood, as formulated by the Maternal Health and SafeMotherhood Program, Division of Family Health of the World Health Organization. Home visits by community-based health workers can help to reduce neonatal mortality by ensuring identification of pregnant women, andby ensuring optimal maternal health through both antenatal and postnatal care visits to their homes. Theinformation for the mothers, their age, education and the health status and the care provided by the FemaleMultipurpose Health Workers and nursing students to the mothers is documented on the maternal cards in thefamily folders. The audit is the major tool to evaluate the quality of care. It was felt that there is need for theevaluation of documented care and a tool is required hence an Audit tool is developed to audit the documentedcare. There are 81 items to evaluate care of mothers. Content validity was checked by giving the tool to experts,construct validity by application of Principal component analysis and reliability by Cronbach's alpha. Thevalue of Cronbach's alpha was .95 which showed that tool is reliable. The developed tool shall evaluate thefamily folders maintained by health workers and nursing students. This tool will help in improving the qualityof documentation.
Key words :Audit tool, Maternal care in the community.
Introduction
Mothers are important components offamily as the health of children depends uponthe health of the mother so the mothers areto be provided the best care right from theadolescent period. Mothers need timely accessto skilled care during pregnancy, child birth,and postpar tum period. Immediate andeffective care during and after labor can makea significant difference between the life anddeath of both the mother and the new born

12Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
as the complications are unpredictable andrapidly become life threatening. Timeliness ordegree to which care is provided at the mostbeneficial or necessary time is a keycomponent of quality health care along witheffectiveness.1,2
A maternal health record shows theextent of the health problems’, needs andother factors that affect mothers’ health. Whathas been done for the mothers is documentedin the maternal cards and further what is tobe done is also written. It also indicates theplans for future visits in order to meet theneeds. Record serves as a guide for evaluationof care provided by the workers. Whenrecords are made they help to continue thecare and also help to identify the high riskmothers.3 Audit is a kind of review and is amajor tool used to evaluate the quality of care.4
An audit is the systemic review of records forthe purpose of evaluation of thedocumentation. Nursing audit is theassessment of quality of nursing care anduses the record as an aid in evaluating thequality care. It is useful to identify areas ofstrength and weakness for further planning.A nursing audit is two types. First, aretrospective audit which refers to an in depthassessment of the quality after the provisionof the care and the record is the source ofdata. The second is the concurrent audit whichrefers to evaluation when client is still gettingcare.5
The records are the primary source forgetting the information related to the mothers.These are the legal records and the evidenceof the basis on which decisions were made.6
To see the quality of care and thedocumentation auditing is required in thecommunity to improve the care. C B Jorvelldeveloped an audit instrument that measuresthe extent to which patient records describeimportant aspects of nursing care.7
Improving documentation is an urgentissue. Poor documentation is an indicationthat further investigation is needed to judgewhether or not the given care is less thanoptimal. Evaluating the care throughdocumentation improves the care as well asthe documentation. Looking into the need forevaluation of the care of mothers, theinvestigator felt the need to develop an audittool.
With the ongoing emphasis in resourcemanagement cost control, efficiency in clientcare, quality improvement and accountability,the health workers are required to provide careand do effective documentation at the sametime.3 Maternal health records are the meansof providing information about health ofmothers. These records are practical andindispensable aid to the health personnel forgiving best possible proper care to mothers.The health worker before she goes to thefamily will read the record and get knowledgeabout their health and she will not be treatedas a stranger because this will help her tocreate good personal rapport.8
Objective
The objective of the present study wasto develop an audit tool for documented carefor mothers by the health workers and thenursing students.

13Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
Methodology
Present study used the methodologicalapproach. The study was conducted in oneof the nongovernmental hospital of Panjabwhere it has three health centers and they areproviding services to the rural and urbanpopulation. The health centers where thestudy was conducted the Health Care isprovided by the Female Multipurpose HealthWorkers and nursing students through homevisits. The nursing students are posted fortheir field experience in these centers and theywork under supervision. Center is providingcare for mothers, children and for generalpopulation. These centers work under thedepartment of social and preventive medicine.All the records, reports and registers belongto community medicine department but theyare maintained by Female Multipurpose HealthWorkers and nursing students posted in theareas. The reports and records, which aregenerally used by these centers, are sent tothe SPM department on monthly, quarterlyand yearly basis.
Family folder is maintained for eachfamily which gives description aboutsocioeconomic status of the family whichfurther describes about type of house, animalkept, sanitation and water supply, mechanicalprofession and economical status. It alsodescribes about the house no., area, familyfolder no., workers name, religion, descriptionabout all the family members, family planningstatus and immunization status whether it iscomplete or partial. The folders are enclosedwith many other cards like eligible couples’cards, maternity cards, preschool cards andindividual cards etc.
The total family folders in the one UrbanFamily Welfare center were 3189, in the otherurban health center the total family folderswere 2080 and whereas in the Rural healthcenter the total family folders were 2100.
Audit tool is developed by literaturereview, identifying items, discussion withpeers and determining items. There wasgeneration of item pool and their organization;suggestions were incorporated about theformat of tool. The tool can record all theabove information for five eligible couples andfive mothers. The tool is divided into two parts.
Part-I was to record the identificationas house no, folder no, area, name of the headof the family, date of making the folder, totalfamily members, family income, religion, typeof family, year of making the folder.
Part II is further divided into five partsand 196 items. The par ts are related topreparation of eligible couple card,assessment and care of antenatal mothers,information related to abortions, assessmentand care of mother during delivery and postnatal period.
Content validity of the tool was done infour rounds by peers, five rounds amongexper ts from the field of nursing andcommunity medicine. Further, five times thetool was field tested for feasibility, contentvalidity and the consumption of time.
Cronbach’s alpha was applied to checkreliability of the audit tool after its field test on100 maternal records.. This resulted indeletion of 100 items from differentcomponents of maternal care and retentionof reliable 96 items.
14Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
Thereafter the audit tool was field testedon 2000 sample records. On the datacollected, once again the Cronback’s alphawas applied and principal component analysiswas done. This resulted in deletion of 15 moreitems from maternal care. Total 81 items areleft in final Audit tool. The reliability of the toolis found to be .995 which shows that all itemsof this tool are consistent and showundimentionality. Factor analysis of tool afterVarimax rotation method indicated that totalseven factors.
Results
For construct validity of the tool factoranalysis is applied which divides the tool in to
seven parts according to the factors generatedthrough factor analysis. These parts were aspreparation of eligible couple card, antenatalmother, abortion, and post natal mother. Theitems of the tool are organized under the sameheads as they were prepared after analysis.Other 15 items which were related toidentification on folders, intra natal mother andfew items related to postnatal mother weredeleted but they are also important and canbe included in the tool.
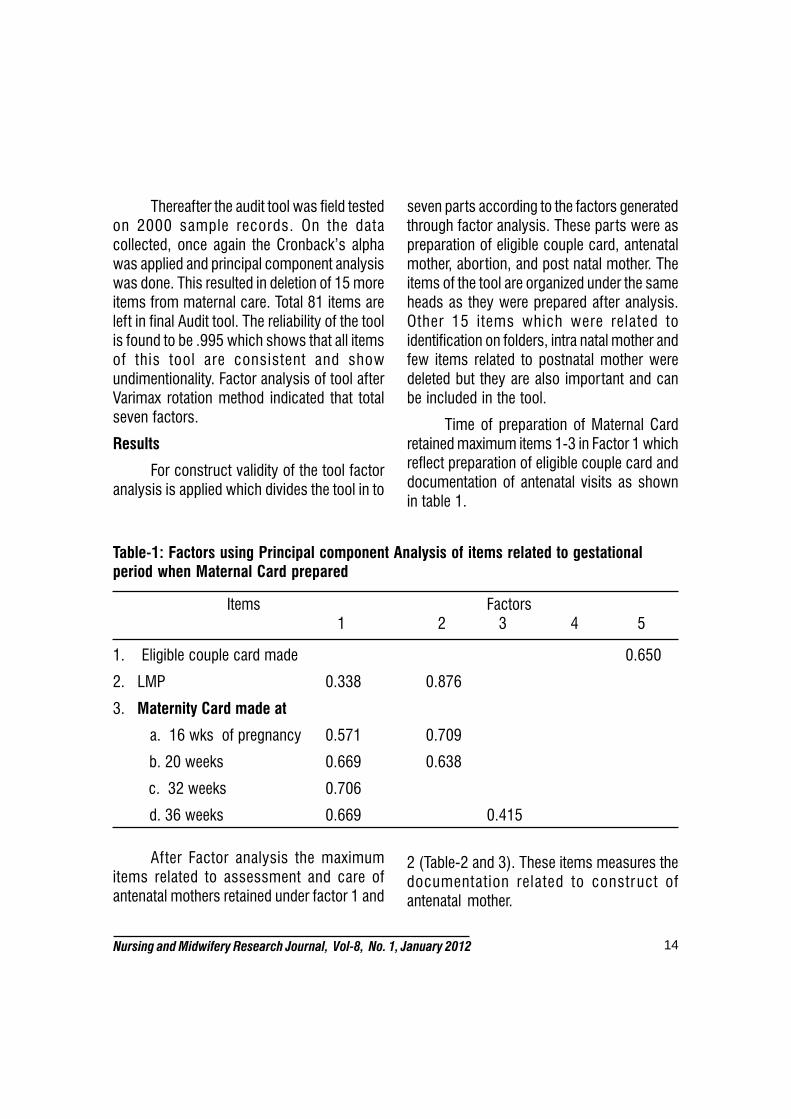
Time of preparation of Maternal Cardretained maximum items 1-3 in Factor 1 whichreflect preparation of eligible couple card anddocumentation of antenatal visits as shownin table 1.
Table-1: Factors using Principal component Analysis of items related to gestationalperiod when Maternal Card prepared
Items Factors 1 2 3 4 5
1. Eligible couple card made 0.650
2. LMP 0.338 0.876
3. Maternity Card made at
a. 16 wks of pregnancy 0.571 0.709
b. 20 weeks 0.669 0.638
c. 32 weeks 0.706
d. 36 weeks 0.669 0.415
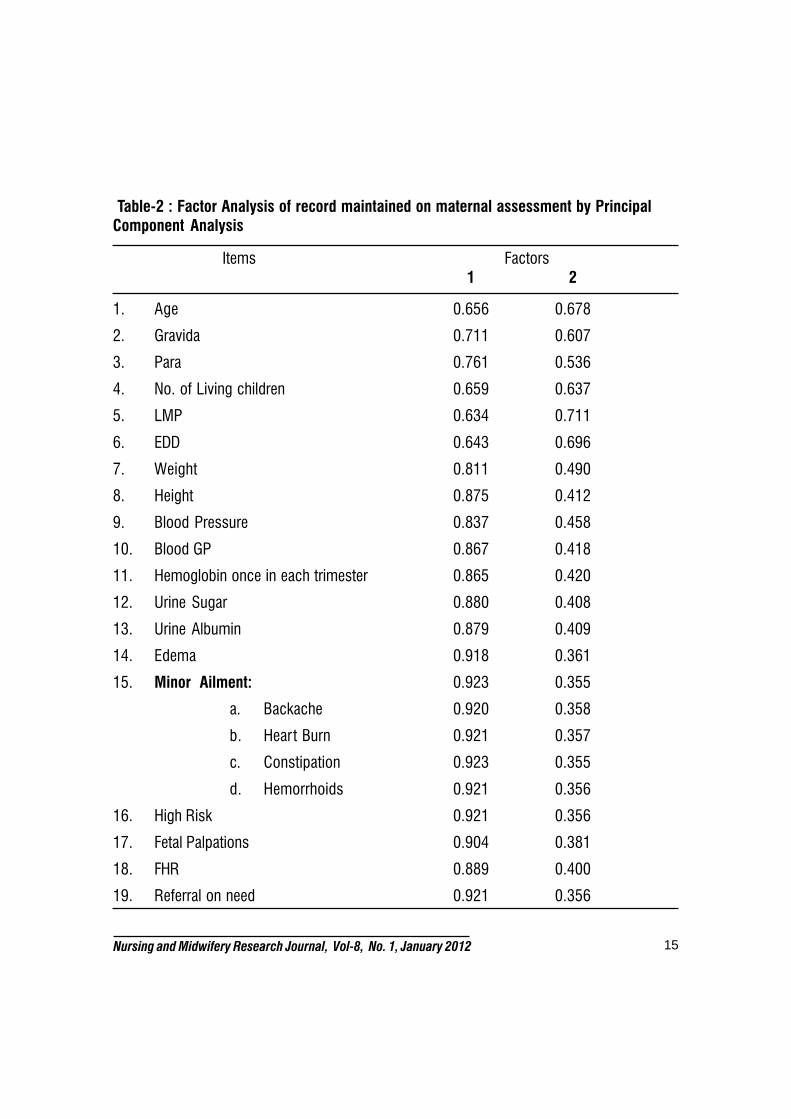
After Factor analysis the maximumitems related to assessment and care ofantenatal mothers retained under factor 1 and
2 (Table-2 and 3). These items measures thedocumentation related to construct ofantenatal mother.
15Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
Table-2 : Factor Analysis of record maintained on maternal assessment by Principal
Component Analysis
Items Factors1 2
1. Age 0.656 0.678
2. Gravida 0.711 0.607
3. Para 0.761 0.536
4. No. of Living children 0.659 0.637
5. LMP 0.634 0.711
6. EDD 0.643 0.696
7. Weight 0.811 0.490
8. Height 0.875 0.412
9. Blood Pressure 0.837 0.458
10. Blood GP 0.867 0.418
11. Hemoglobin once in each trimester 0.865 0.420
12. Urine Sugar 0.880 0.408
13. Urine Albumin 0.879 0.409
14. Edema 0.918 0.361
15. Minor Ailment: 0.923 0.355
a. Backache 0.920 0.358
b. Heart Burn 0.921 0.357
c. Constipation 0.923 0.355
d. Hemorrhoids 0.921 0.356
16. High Risk 0.921 0.356
17. Fetal Palpations 0.904 0.381
18. FHR 0.889 0.400
19. Referral on need 0.921 0.356
16Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
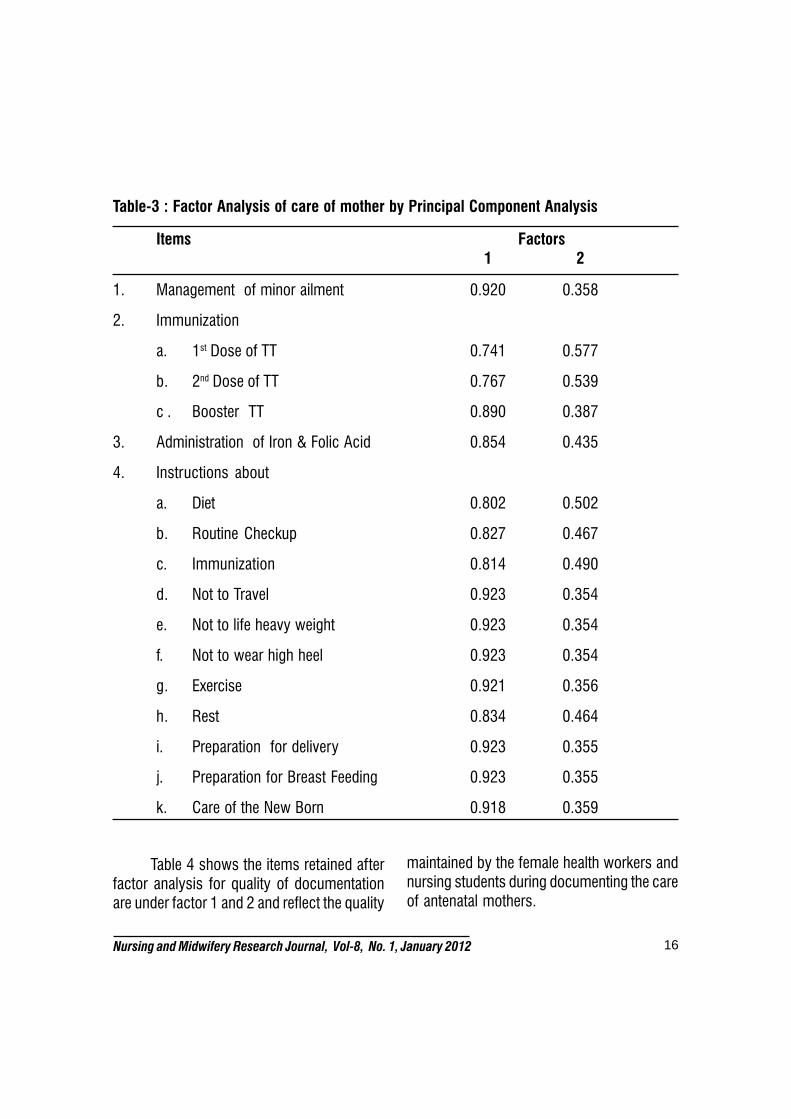
Table-3 : Factor Analysis of care of mother by Principal Component Analysis
Items Factors1 2
1. Management of minor ailment 0.920 0.358
2. Immunization
a. 1st Dose of TT 0.741 0.577
b. 2nd Dose of TT 0.767 0.539
c . Booster TT 0.890 0.387
3. Administration of Iron & Folic Acid 0.854 0.435
4. Instructions about
a. Diet 0.802 0.502
b. Routine Checkup 0.827 0.467
c. Immunization 0.814 0.490
d. Not to Travel 0.923 0.354
e. Not to life heavy weight 0.923 0.354
f. Not to wear high heel 0.923 0.354
g. Exercise 0.921 0.356
h. Rest 0.834 0.464
i. Preparation for delivery 0.923 0.355
j. Preparation for Breast Feeding 0.923 0.355
k. Care of the New Born 0.918 0.359
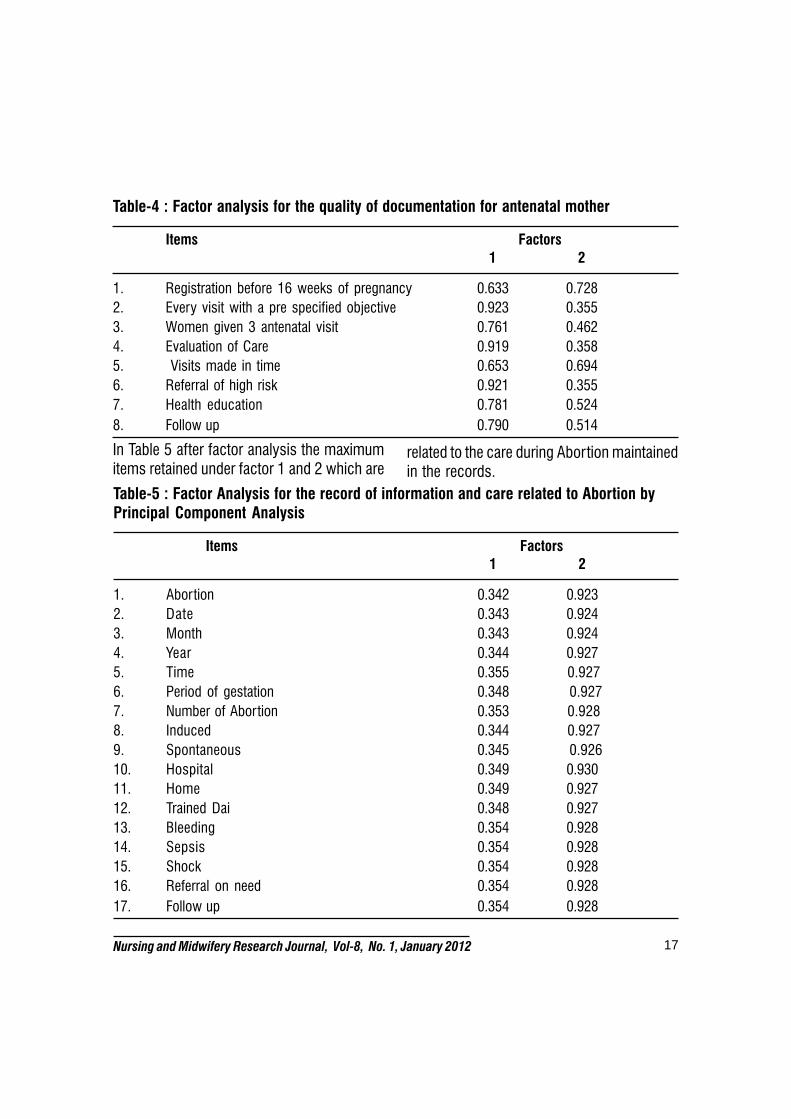
Table 4 shows the items retained afterfactor analysis for quality of documentationare under factor 1 and 2 and reflect the quality
maintained by the female health workers andnursing students during documenting the careof antenatal mothers.
17Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
Table-4 : Factor analysis for the quality of documentation for antenatal mother
Items Factors
1 2
1. Registration before 16 weeks of pregnancy 0.633 0.728
2. Every visit with a pre specified objective 0.923 0.355
3. Women given 3 antenatal visit 0.761 0.462
4. Evaluation of Care 0.919 0.358
5. Visits made in time 0.653 0.694
6. Referral of high risk 0.921 0.355
7. Health education 0.781 0.524
8. Follow up 0.790 0.514
In Table 5 after factor analysis the maximumitems retained under factor 1 and 2 which are
related to the care during Abortion maintainedin the records.
Table-5 : Factor Analysis for the record of information and care related to Abortion byPrincipal Component Analysis
Items Factors
1 2
1. Abortion 0.342 0.923
2. Date 0.343 0.924
3. Month 0.343 0.924
4. Year 0.344 0.927
5. Time 0.355 0.927
6. Period of gestation 0.348 0.927
7. Number of Abortion 0.353 0.928
8. Induced 0.344 0.927
9. Spontaneous 0.345 0.926
10. Hospital 0.349 0.930
11. Home 0.349 0.927
12. Trained Dai 0.348 0.927
13. Bleeding 0.354 0.928
14. Sepsis 0.354 0.928
15. Shock 0.354 0.928
16. Referral on need 0.354 0.928
17. Follow up 0.354 0.928
18Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
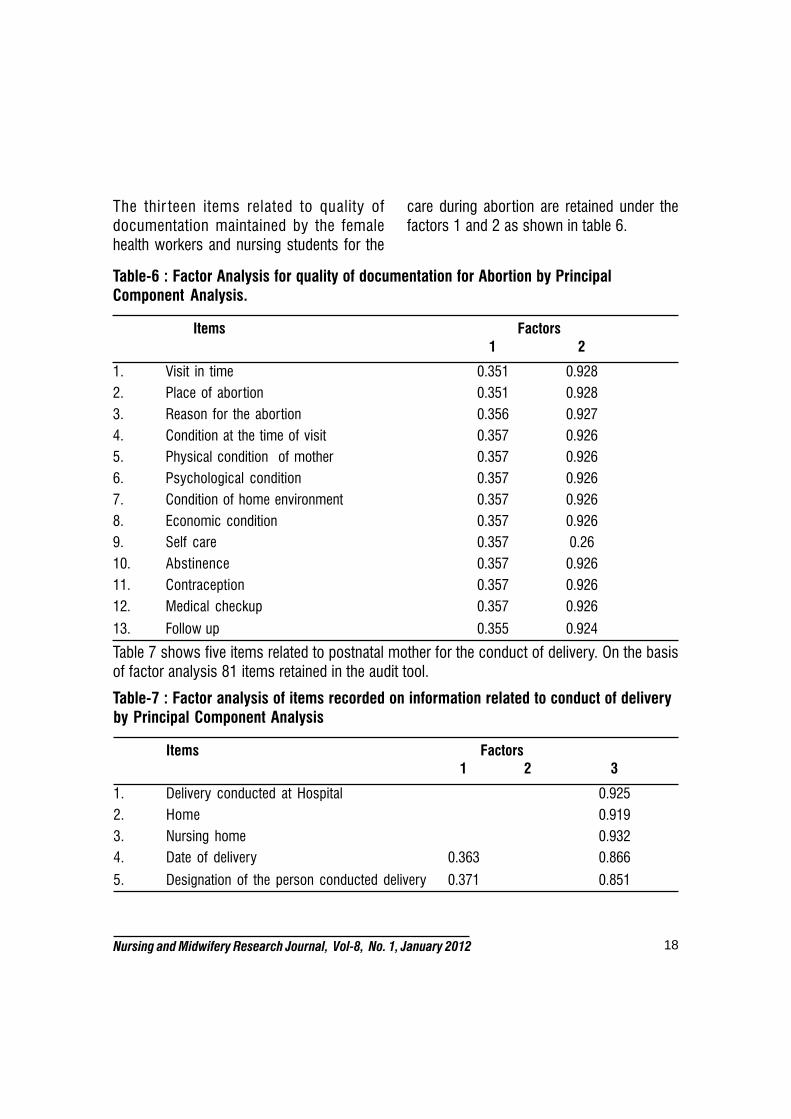
The thir teen items related to quality ofdocumentation maintained by the femalehealth workers and nursing students for the
care during abortion are retained under thefactors 1 and 2 as shown in table 6.
Table-6 : Factor Analysis for quality of documentation for Abortion by Principal
Component Analysis.
Items Factors
1 2
1. Visit in time 0.351 0.928
2. Place of abortion 0.351 0.928
3. Reason for the abortion 0.356 0.927
4. Condition at the time of visit 0.357 0.926
5. Physical condition of mother 0.357 0.926
6. Psychological condition 0.357 0.926
7. Condition of home environment 0.357 0.926
8. Economic condition 0.357 0.926
9. Self care 0.357 0.26
10. Abstinence 0.357 0.926
11. Contraception 0.357 0.926
12. Medical checkup 0.357 0.926
13. Follow up 0.355 0.924
Table 7 shows five items related to postnatal mother for the conduct of delivery. On the basisof factor analysis 81 items retained in the audit tool.
Table-7 : Factor analysis of items recorded on information related to conduct of deliveryby Principal Component Analysis
Items Factors
1 2 3
1. Delivery conducted at Hospital 0.925
2. Home 0.919
3. Nursing home 0.932
4. Date of delivery 0.363 0.866
5. Designation of the person conducted delivery 0.371 0.851

19Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
Discussion
The aim of present study was to developan audit tool for care of mothers. The care isdocumented related to mothers duringpregnancy, intranatal period, for abortion andpost natal period. Audit tool is developed toaudit care for mothers.
The internal consistency and reliabilityof the tool was measured by Cronbach’salpha. The estimated Cronbach’s alpha >0.70is considered statistically significant andindicates a substantial internal consistency ofscale in simple items. High Cronbach’s alphaof 0.995 highlights a homogeneity of all itsitems and all items measured the underlyingconstruct of mother. This was supported withthe study where Socio-Economic Status Scalewas developed and cronbach’s alpha was0.81.10 The widely-accepted social sciencecut-off is that alpha should be .70 or higherfor a set of items to be considered a scale,but some use .75 or .80 while others are aslenient as .60.11
To check the eligibility data for factoranalysis minimum sample size should be totalno of items multiplied by 10 and for thepresent study there 96 items and the samplesize was 2000 so the data was eligible forfactor analysis.9
Principal component Factor analysiswas used to compute the construct validity.Total seven factors were identified. This wascompared with a study where the tool wasdeveloped and for Bir th preparedness and
total 10 factors were identified.12 First factorretained maximum number of items whichreflect “Assessment and Care of AntenatalMother”. Factor 2 retained items which reflect“Assessment and Care of Abortion”. Factor 3retained 4 items which reflect “Postnatal care”.Factor 4 retained only 2 items which reflect“Eligible Couple card made”. Item 4, whichwas ‘folder no’ has value <.3 which wasdeleted. If this was deleted it did not lose theinformation as on the first page of the audit‘Folder no’ is to be written. Factor 5 retained1 item. Factor 6 retained item no: 6 and 7which had value <3 and were related to“Eligible couple card made” deleted. Factor 7retained 1 item ‘HIV’ which was discardedbecause as a useful factor it should have atleast 3 items loading significantly on thatcomponent.
The item of ‘HIV’ which was under theeligible couple card made and was deletedbecause it was not very useful item as it wasnot documented in the folders and may bebecause of the social stigma people do nottell about it or the nursing students and thehealth workers are not asking about it.
A valid and reliable tool developed toevaluate the quality of nursing care anddocumentation of nursing care provided tomother and the tool can also be used tocompare the quality of documentation of twoinstitutes. The tool can be used by theteachers and administrators in order toevaluate the care provided to mother bynursing students and health workers.
20Nursing and Midwifery Research Journal, Vol-8, No. 1, January 2012
References
1. Choudhury Nuzhat and Ahmed Syed M.Maternal care practices among the ultra poorhousehold in rural Bangladesh: a qualitativeexploratory study.BMC Pregnancy and Childbirth2011,11:15.
2. Edson W, Burkhalter B., Mc Law BinnnsA., timeliness of care for eclampsia and pre-eclampsia in benin. International Journal ofGynecology and Obstetrics 2007;97:209-214.
3. Shah P.M, Selwyn B.J, Shah K, Kumar V.Evaluation of the home based maternal record: aWHO collaborative study. Bull World Health Organ1993;71(5):535-5 40.
4. James Chris. Have you got a record?Nursing times 1895; 88(14): 26 – 28.
5. Tobin Melen M, Yoder Wise Pat S, HullPeggy K. The process of staff development. 2nd
Ed. Mosby Company, London. 1979.
6. Johnson G. Reviewing audit;barriers &facilitating factors for effective clinical audit. JQuality in health care 2000; 9:23-36.
7. Bjorvell C. Development of an auditinstrument for the nursing care plan in the patientrecord. J quality in health care 2000;9;6-13.
8. Bryn D. Daire, Jenifer R. Billings &Richard K Ryland. Evaluation of Nursing ProcessDocumentation. Journal of Advance Nursing.1994; 19 (5): 960.
9. Bandana. Development of audit tool: Amethodological sudy for auditing the familyFolders. Nursing and Midwifery research Journal2009;4:166-175.
10. Pebma Monika, Saini Kumari Sushma,Walia Indarjit. Development of Socio-EconomicStatus Scale for community residing in DaduMajra Colony. Nursing & Midwifery researchJournal 2010;6(1):119-136.
11. www2.chass.ncsu.edu/garson/pa765/standard.htm
12. Varinder Kaur. Development of Bir thPreparedness tool (BPT)- A tool to assessmother’s preparedness for delivery, postnatal andnew born care. Nursing and Midwifery Journal2009;5:45-58.