a systematic review of community-based health interventions on depression for older adults with...
TRANSCRIPT

This article was downloaded by: [University of California Davis]On: 11 November 2014, At: 12:44Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Aging & Mental HealthPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/camh20
A systematic review of community-based healthinterventions on depression for older adults withheart diseaseChristina D. Kang-Yi a & Zvi D. Gellis ba Department of Psychiatry, Center for Mental Health Policy and Services Research ,University of Pennsylvania School of Medicine, 3535 Market Street , 3rd Floor,Philadelphia, PA 19104, USAb Hartford Geriatric Social Work Faculty Scholar, Center for Mental Health & Aging,School of Social Policy and Practice, University of Pennsylvania, 3701 Locust Walk ,Philadelphia, PA 19104, USAPublished online: 12 Feb 2010.
To cite this article: Christina D. Kang-Yi & Zvi D. Gellis (2010) A systematic review of community-based healthinterventions on depression for older adults with heart disease, Aging & Mental Health, 14:1, 1-19, DOI:10.1080/13607860903421003
To link to this article: http://dx.doi.org/10.1080/13607860903421003
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose ofthe Content. Any opinions and views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be reliedupon and should be independently verified with primary sources of information. Taylor and Francis shallnot be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and otherliabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Aging & Mental HealthVol. 14, No. 1, January 2010, 1–19
A systematic review of community-based health interventions on depression for older adults
with heart disease
Christina D. Kang-Yia* and Zvi D. Gellisb
aDepartment of Psychiatry, Center for Mental Health Policy and Services Research, University of Pennsylvania School ofMedicine, 3535 Market Street, 3rd Floor, Philadelphia, PA 19104, USA; bHartford Geriatric Social Work Faculty Scholar,Center for Mental Health & Aging, School of Social Policy and Practice, University of Pennsylvania, 3701 Locust Walk,
Philadelphia, PA 19104, USA
(Received 11 May 2009; final version received 24 September 2009)
Purpose: This systematic review examined the effectiveness of community-based heart-health interventions ondepression outcomes among homebound elderly (64 years and older) with heart disease.Design and Methods: A comprehensive literature search and meta analysis was performed to evaluate randomizedcontrolled trials examining outpatient or home-based interventions. Methodological quality was assessed bystandard criteria developed by the Cochrane Collaborative Initiative.Results: Fifteen studies met our inclusion criteria and all measured depression outcomes. Studies differed in scopeand methodological rigor and sample sizes varied widely. Problems in treatment fidelity and masking of groupassignment were noted. Great variability was found in depression outcomes due to the differences inmethodology and intervention. Five studies reported significant treatment effect on depression; three of thoseemployed home-based interventions and two were outpatient-clinic interventions. Ten studies were included inthe meta analysis and the effect sizes (ESs) ranged from �0.39 (in favor of control group) to 0.65 (in favor oftreatment group). The mean weighted ES was 0.11 and six studies showed positive ESs.Implications: Mixed evidence for community-based heart disease interventions on depression outcomes wasfound. Future research should include sub-analysis of ESs of interventions on depression outcomes by differentdemographic characteristics of the study sample, common depression outcome measures, and different follow-upperiods.
Keywords: heart disease; community-based interventions; homebound elderly; depression
Introduction
Heart disease affects an estimated 38.1 million olderadults (60 years and older) in the United States andconsumes an estimated total $475.3 billion dollars indirect and indirect health care expenditures (AmericanHeart Association, 2009; National Heart Lung andBlood Institute, 2007). It is the most common primarydiagnosis and the leading cause of death amongmedically ill homebound elderly patients (Centers forDisease Control and Prevention, 2005). The WorldHealth Organization’s (WHO) global burden of diseasestudy ranks depression second only to heart disease inburden (impact on disability-adjusted life years; WHO,2008). Depression is common and widespread amongmedically ill noninstitutionalized elderly where theprevalence rates are 13.5% for major depression(Bruce et al., 2002) and 16 to 37% for subthresholddepressive syndromes (Freedland et al., 2003; Gellis,2010; Rudisch & Nemeroff, 2003). Depression may bean independent risk factor for the onset of heart diseasesuggesting that patients are at high risk for negativeoutcomes (Nemeroff, Musselman, & Evans, 1998).
People with heart disease who are depressedhave an increased risk of death after a heart attackcompared to those who are not depressed(Frasure-Smith, Lesperance, & Talajic, 1995).
Hypertension, hypoglycemia, and coronary artery
disease can be worsened through depression (VanHout et al., 2004). Heart disease is often associatedwith increased fatigue, greater levels of chronic phys-
ical illness, increased disability, decreased psychologi-cal well-being, decreased life satisfaction and increased
healthcare costs among older adults (Glassman &Shapiro, 1998; Martin, Bishop, Poon, & Johnson,
2006; Penninx et al. 2001). Depression may alsojeopardize adherence to treatment regimens includingneeded medication.
Treatment for depression in conjunction with
heart disease may help people manage both diseases,thus enhancing survival and quality of life. Therefore,
there is a need for effective community-based inter-ventions among older adults with heart diseasecomorbid with depression (Gellis & Bruce, 2009).
Intervention research for heart disease has focusedon drug therapies, electric equipment therapies,
and community-based multidisciplinary team interven-tions as potential strategies for improving outcomes
in these patients. These multidisciplinary approachesmay also have a positive impact on the complexinteraction between medical, psychosocial, and behav-
ioral factors confronting homebound elderly with heartdisease.
*Corresponding author. Email: [email protected]
ISSN 1360–7863 print/ISSN 1364–6915 online
� 2010 Taylor & Francis
DOI: 10.1080/13607860903421003
http://www.informaworld.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

Caring for community-dwelling medically ill olderadults with complex needs continues to be a challengefor health care systems. In recent years,community-based care has been promoted in healthpolicies as it offers the prospect of substantialcost-savings as well as improved health outcomes(Johri, Beland, & Bergman, 2003). Currently, commu-nity care of heart disease is delivered in several ways.Large health care organizations commonly use nursecase managers in outpatient clinics to provide heartdisease management programs. Medically ill home-bound elderly may receive home health care visits ortelehealthcare using technology as a means of moni-toring and educating individuals regarding chronicmedical conditions for improved health outcomes.
This meta analysis examines the quality and effec-tiveness of community-based health care interventionson depression outcomes among non-institutionalizedolder adults diagnosed with heart disease. To ourknowledge, this is the first review that delineates a setof criteria for interpreting the validity, generalizability,and reliability of the research among selected studies ofoutpatient and home-based health care interventions aspotentially successful patient management approachesfor heart disease and depression.
Methods
A systematic review and meta analysis of the literatureon community-based healthcare interventions for olderadults diagnosed with heart disease was conducted to(1) identify the type of interventions used in nonin-stitutionalized settings and (2) determine the effective-ness of these interventions on depression outcomes.Two reviewers examined studies to determine theirselection for inclusion in the review and then assessedthe methodological quality of selected studies. Themethodology for this review was guided by theCochrane Collaboration Handbook for SystematicReviews of Interventions (Higgins & Green, 2006).
Search strategy
We conducted searches on the following electronicdatabases: Ageline, PubMed, PsycInfo, Medline,ClinialTrial.gov, Central Register of Controlled Trial,and CINAHL. Relevant treatment trials were searchedusing the following keywords: heart disease or heartfailure, and geri*, elder*, depress*, depression, ordepressive symptom. We reviewed studies ofcommunity-based health care interventions offered inthe home or in outpatient-clinic settings for olderadults diagnosed with heart disease. The search waslimited to studies published from 1998 to 2008 andclassified as randomized controlled trials investigatingan effect of an intervention. We also limited theparticipants’ mean age to 64 years or older due to thehigh prevalence rates of heart disease and depression inthe elderly population in the US.
A home-based intervention was defined as treat-ment that took place at the individuals’ home and mayinclude education, counseling, exercise program, videoand/or internet-based care, or telehealth care. Anoutpatient-clinic intervention was defined as treatmentthat occurred in an outpatient healthcare setting suchas a cardiac rehabilitation or prevention clinic. If anintervention involved more than one care setting, forexample, a disease management program held at aclinic with self-management activities at home, thestudy was classified as a combined home and outpa-tient clinic-based intervention.
Two reviewers screened abstracts and full papers,and extracted data on intervention type (home-basedvs. outpatient clinic-based), sample size, participants,intervention descriptions, methodological attributes,standardized outcome measures, and key findings foreach study. After selecting papers that met the inclu-sion criteria, the reviewers assessed methodologicalquality of the interventions by independently reviewingthe full papers.
Review of methodological quality
The review criteria of methodological quality included:(a) use of random allocation methods; (b) poweranalysis conducted; (c) measures used to preventperformance and detection bias; (d) explanation oftreatment protocol provided; (e) intent-to-treat analy-sis conducted; (f) description of interventionist train-ing; and (g) explanation of measures used to collectdata on treatment fidelity. These criteria are recom-mended by the Cochrane Collaboration Review ofRandomized Controlled Trials (Higgins & Green,2006). The definitions of criteria are explained indetail elsewhere (Gellis & Kenaley, 2008). The includedstudies were graded based on the Gellis and Kenaley’s(2008) methodological quality rating scale with a rangefrom 1 to 10.
Meta analysis
Meta analysis was performed to estimate effect sizes(ESs) for mean differences in depression outcomesbetween treatment and control groups. Effect size wascalculated as standardized mean difference (Hedges) atthe most current follow-up assessment with 95%confidence intervals (CIs) between treatment andcontrol group (Hedges, 1981). Fifteen studies wereincluded in the meta analysis. However, five studieswere excluded due to missing information on meansand standard deviations of depression outcomes fortreatment and control groups.
Results
As shown in Figure 1, the search strategy initiallyyielded 59 articles. Forty-four studies were excludeddue to the following reasons: (a) a non-randomized
2 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
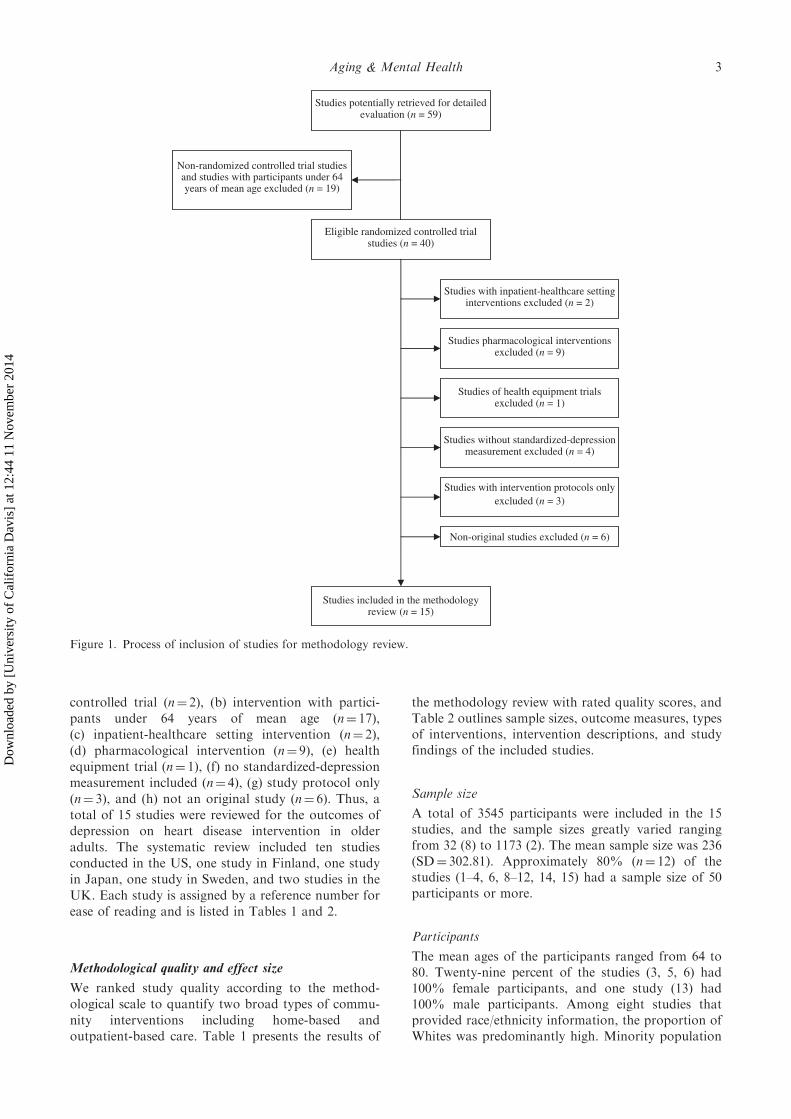
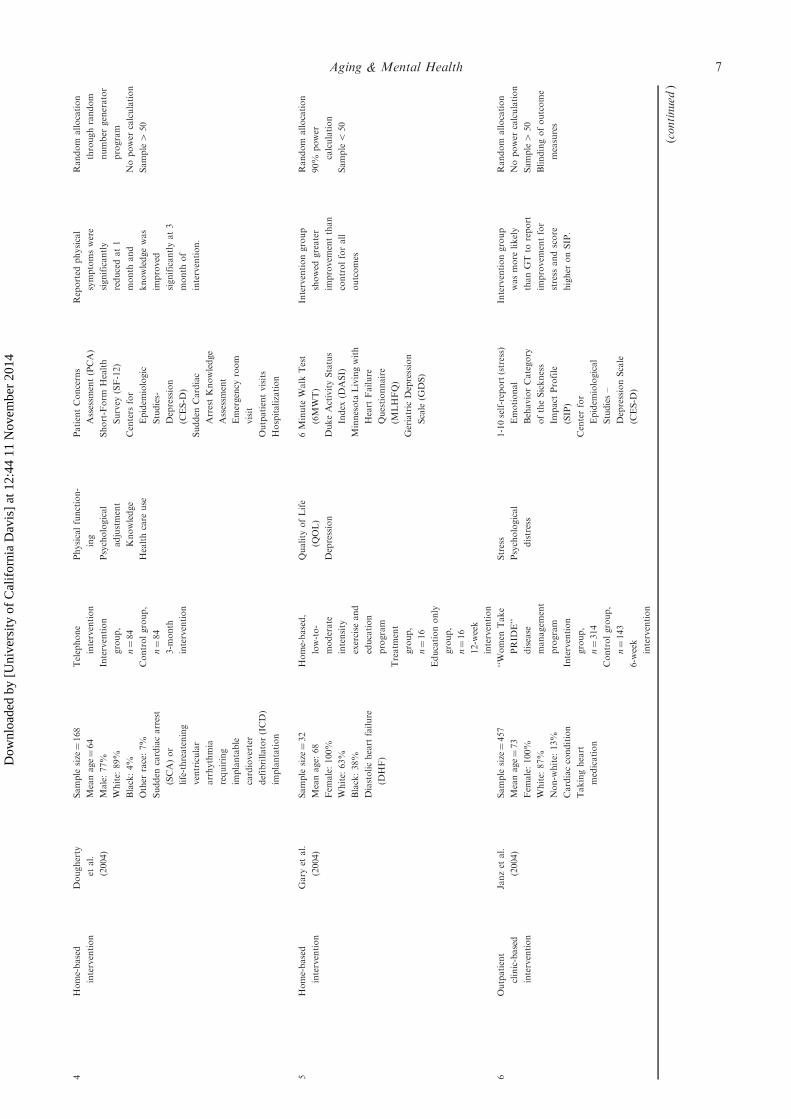
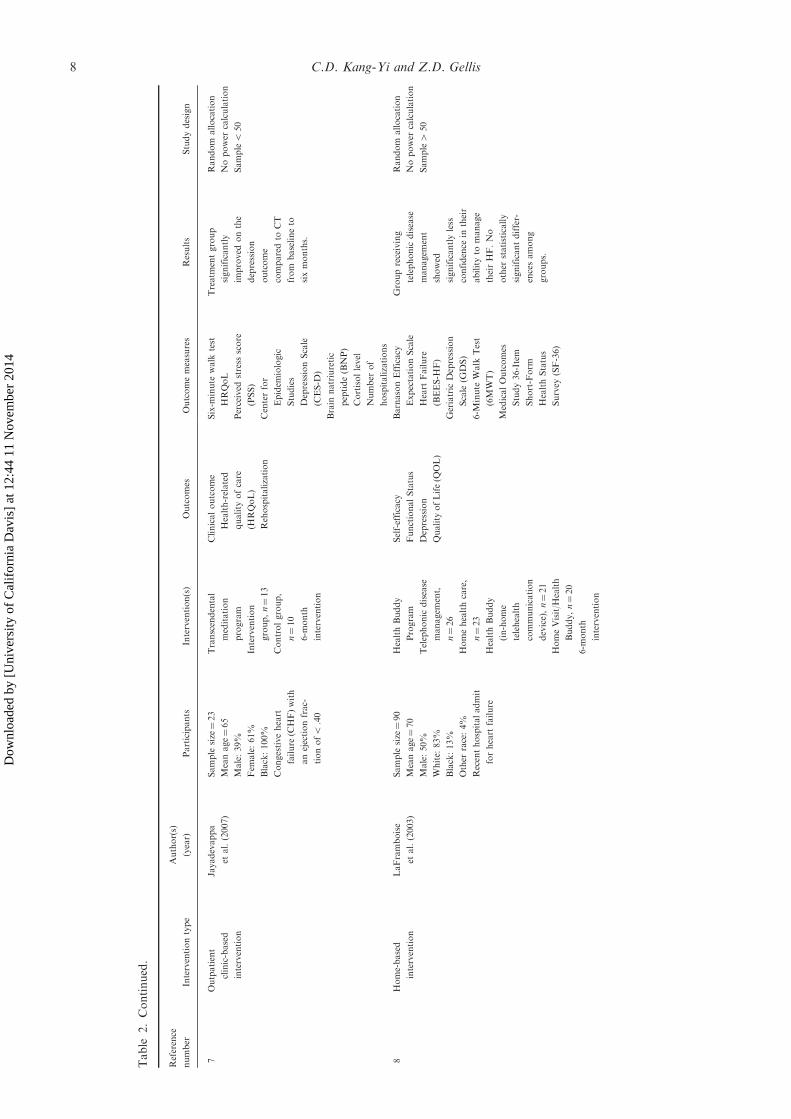
controlled trial (n¼ 2), (b) intervention with partici-pants under 64 years of mean age (n¼ 17),(c) inpatient-healthcare setting intervention (n¼ 2),(d) pharmacological intervention (n¼ 9), (e) healthequipment trial (n¼ 1), (f) no standardized-depressionmeasurement included (n¼ 4), (g) study protocol only(n¼ 3), and (h) not an original study (n¼ 6). Thus, atotal of 15 studies were reviewed for the outcomes ofdepression on heart disease intervention in olderadults. The systematic review included ten studiesconducted in the US, one study in Finland, one studyin Japan, one study in Sweden, and two studies in theUK. Each study is assigned by a reference number forease of reading and is listed in Tables 1 and 2.
Methodological quality and effect size
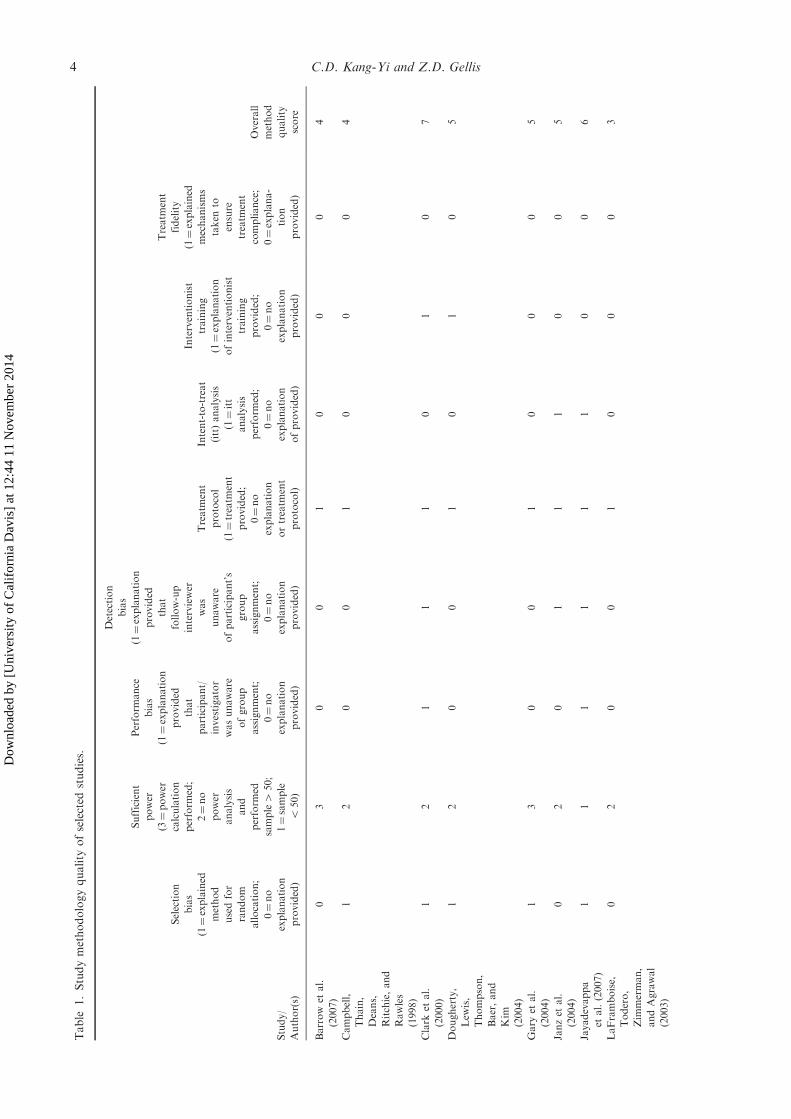
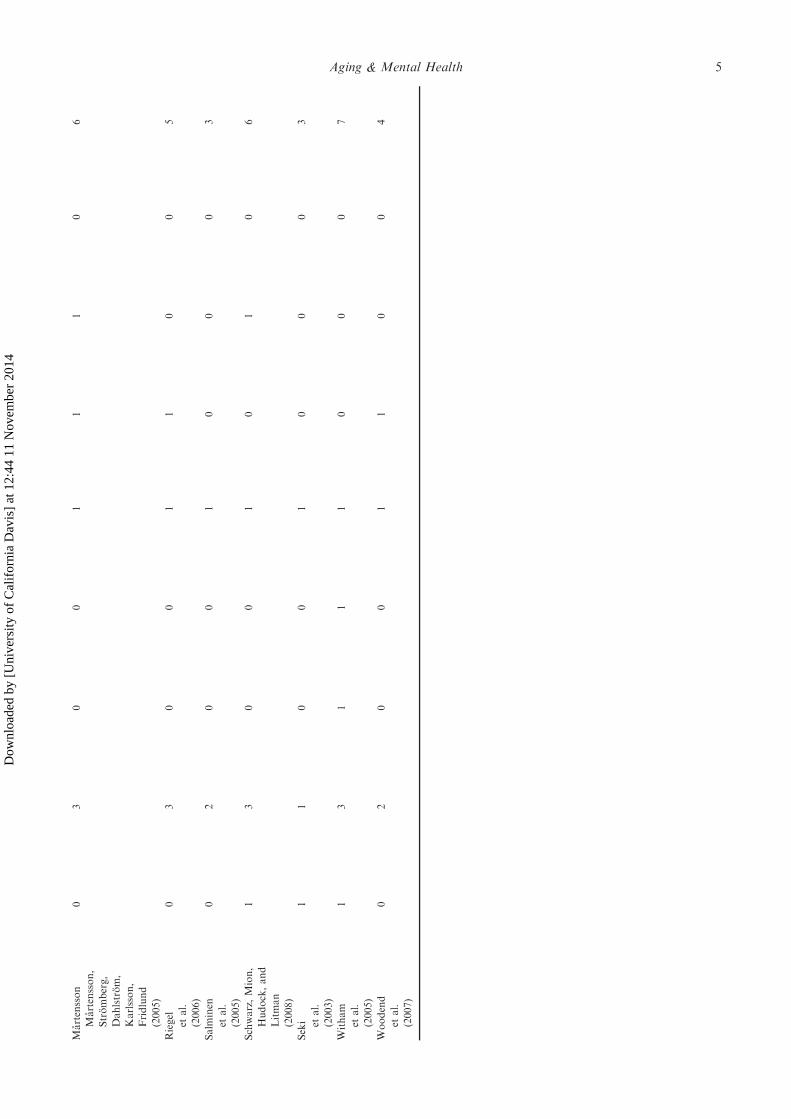
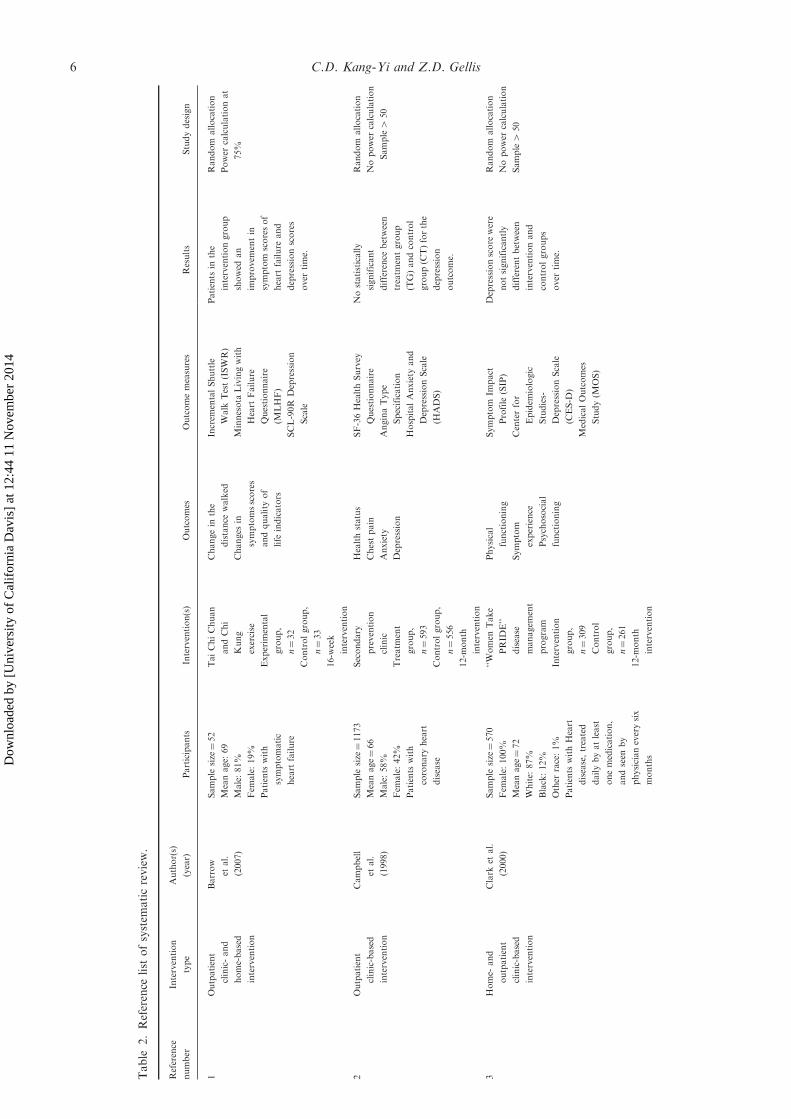
We ranked study quality according to the method-ological scale to quantify two broad types of commu-nity interventions including home-based andoutpatient-based care. Table 1 presents the results of
the methodology review with rated quality scores, andTable 2 outlines sample sizes, outcome measures, typesof interventions, intervention descriptions, and studyfindings of the included studies.
Sample size
A total of 3545 participants were included in the 15studies, and the sample sizes greatly varied rangingfrom 32 (8) to 1173 (2). The mean sample size was 236(SD¼ 302.81). Approximately 80% (n¼ 12) of thestudies (1–4, 6, 8–12, 14, 15) had a sample size of 50participants or more.
Participants
The mean ages of the participants ranged from 64 to80. Twenty-nine percent of the studies (3, 5, 6) had100% female participants, and one study (13) had100% male participants. Among eight studies thatprovided race/ethnicity information, the proportion ofWhites was predominantly high. Minority population
Studies potentially retrieved for detailedevaluation (n = 59)
Non-randomized controlled trial studiesand studies with participants under 64years of mean age excluded (n = 19)
Eligible randomized controlled trialstudies (n = 40)
Studies with inpatient-healthcare settinginterventions excluded (n = 2)
Studies pharmacological interventionsexcluded (n = 9)
Studies of health equipment trialsexcluded (n = 1)
Studies without standardized-depressionmeasurement excluded (n = 4)
Studies with intervention protocols onlyexcluded (n = 3)
Non-original studies excluded (n = 6)
Studies included in the methodologyreview (n = 15)
Figure 1. Process of inclusion of studies for methodology review.
Aging & Mental Health 3
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
Table
1.Studymethodologyquality
ofselected
studies.
Study/
Author(s)
Selection
bias
(1¼explained
method
usedfor
random
allocation;
0¼no
explanation
provided)
Sufficient
power
(3¼power
calculation
perform
ed;
2¼no
power
analysis
and
perform
ed
sample4
50;
1¼sample
550)
Perform
ance
bias
(1¼explanation
provided
that
participant/
investigator
wasunaware
ofgroup
assignment;
0¼no
explanation
provided)
Detection
bias
(1¼explanation
provided
that
follow-up
interviewer
was
unaware
ofparticipant’s
group
assignment;
0¼no
explanation
provided)
Treatm
ent
protocol
(1¼treatm
ent
provided;
0¼no
explanation
ortreatm
ent
protocol)
Intent-to-treat
(itt)analysis
(1¼itt
analysis
perform
ed;
0¼no
explanation
ofprovided)
Interventionist
training
(1¼explanation
ofinterventionist
training
provided;
0¼no
explanation
provided)
Treatm
ent
fidelity
(1¼explained
mechanisms
taken
to
ensure
treatm
ent
compliance;
0¼explana-
tion
provided)
Overall
method
quality
score
Barrow
etal.
(2007)
03
00
10
00
4
Campbell,
Thain,
Deans,
Ritchie,and
Rawles
(1998)
12
00
10
00
4
Clark
etal.
(2000)
12
11
10
10
7
Dougherty,
Lew
is,
Thompson,
Baer,and
Kim
(2004)
12
00
10
10
5
Gary
etal.
(2004)
13
00
10
00
5
Janzet
al.
(2004)
02
01
11
00
5
Jayadevappa
etal.(2007)
11
11
11
00
6
LaFramboise,
Todero,
Zim
merman,
andAgrawal
(2003)
02
00
10
00
3
4 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
Martensson
Martensson,
Stromberg,
Dahlstrom,
Karlsson,
Fridlund
(2005)
03
00
11
10
6
Riegel
etal.
(2006)
03
00
11
00
5
Salm
inen
etal.
(2005)
02
00
10
00
3
Schwarz,Mion,
Hudock,and
Litman
(2008)
13
00
10
10
6
Seki etal.
(2003)
11
00
10
00
3
Witham
etal.
(2005)
13
11
10
00
7
Woodend
etal.
(2007)
02
00
11
00
4
Aging & Mental Health 5
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
Table
2.Reference
list
ofsystem
aticreview.
Reference
number
Intervention
type
Author(s)
(year)
Participants
Intervention(s)
Outcomes
Outcomemeasures
Results
Studydesign
1Outpatient
clinic-and
home-based
intervention
Barrow
etal.
(2007)
Sample
size¼52
Meanage:
69
Male:81%
Fem
ale:19%
Patients
with
symptomatic
heart
failure
TaiChiChuan
andChi
Kung
exercise
Experim
ental
group,
n¼32
Controlgroup,
n¼33
16-w
eek
intervention
Changein
the
distance
walked
Changes
in
symptomsscores
andquality
of
life
indicators
Increm
entalShuttle
Walk
Test(ISWR)
Minnesota
Livingwith
Heart
Failure
Questionnaire
(MLHF)
SCL-90R
Depression
Scale
Patients
inthe
interventiongroup
showed
an
improvem
entin
symptom
scoresof
heart
failure
and
depressionscores
over
time.
Random
allocation
Power
calculationat
75%
2Outpatient
clinic-based
intervention
Campbell
etal.
(1998)
Sample
size¼1173
Meanage¼66
Male:58%
Fem
ale:42%
Patients
with
coronary
heart
disease
Secondary
prevention
clinic
Treatm
ent
group,
n¼593
Controlgroup,
n¼556
12-m
onth
intervention
Healthstatus
Chestpain
Anxiety
Depression
SF-36HealthSurvey
Questionnaire
AnginaType
Specification
HospitalAnxiety
and
DepressionScale
(HADS)
Nostatistically
significant
difference
between
treatm
entgroup
(TG)andcontrol
group(C
T)forthe
depression
outcome.
Random
allocation
Nopower
calculation
Sample4
50
3Home-
and
outpatient
clinic-based
intervention
Clark
etal.
(2000)
Sample
size¼570
Fem
ale:100%
Meanage¼72
White:
87%
Black:12%
Other
race:1%
Patients
withHeart
disease,treated
dailybyatleast
onemedication,
andseen
by
physicianeverysix
months
‘‘Women
Take
PRID
E’’
disease
managem
ent
program
Intervention
group,
n¼309
Control
group,
n¼261
12-m
onth
intervention
Physical
functioning
Symptom
experience
Psychosocial
functioning
Symptom
Impact
Profile
(SIP)
Centerfor
Epidem
iologic
Studies-
DepressionScale
(CES-D
)
MedicalOutcomes
Study(M
OS)
Depressionscore
were
notsignificantly
differentbetween
interventionand
controlgroups
over
time.
Random
allocation
Nopower
calculation
Sample4
50
6 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
4Home-based
intervention
Dougherty
etal.
(2004)
Sample
size¼168
Meanage¼64
Male:77%
White:
89%
Black:4%
Other
race:7%
Sudden
cardiacarrest
(SCA)or
life-threatening
ventricular
arrhythmia
requiring
implantable
cardioverter
defibrillator(ICD)
implantation
Telephone
intervention
Intervention
group,
n¼84
Controlgroup,
n¼84
3-m
onth
intervention
Physicalfunction-
ing
Psychological
adjustment
Knowledge
Healthcare
use
PatientConcerns
Assessm
ent(PCA)
Short-Form
Health
Survey
(SF-12)
Centers
for
Epidem
iologic
Studies-
Depression
(CES-D
)
Sudden
Cardiac
ArrestKnowledge
Assessm
ent
Emergency
room
visit
Outpatientvisits
Hospitalization
Reported
physical
symptomswere
significantly
reducedat1
month
and
knowledgewas
improved
significantlyat3
month
of
intervention.
Random
allocation
throughrandom
number
generator
program
Nopower
calculation
Sample4
50
5Home-based
intervention
Gary
etal.
(2004)
Sample
size¼32
Meanage:
68
Fem
ale:100%
White:
63%
Black:38%
Diastolicheart
failure
(DHF)
Home-based,
low-to-
moderate
intensity
exercise
and
education
program
Treatm
ent
group,
n¼16
Educationonly
group,
n¼16
12-w
eek
intervention
Quality
ofLife
(QOL)
Depression
6Minute
Walk
Test
(6MWT)
DukeActivityStatus
Index
(DASI)
Minnesota
Livingwith
Heart
Failure
Questionnaire
(MLHFQ)
Geriatric
Depression
Scale
(GDS)
Interventiongroup
showed
greater
improvem
entthan
controlforall
outcomes
Random
allocation
90%
power
calculation
Sample5
50
6Outpatient
clinic-based
intervention
Janzet
al.
(2004)
Sample
size¼457
Meanage¼73
Fem
ale:100%
White:
87%
Non-w
hite:
13%
Cardiaccondition
Takingheart
medication
‘‘Women
Take
PRID
E’’
disease
managem
ent
program
Intervention
group,
n¼314
Controlgroup,
n¼143
6-w
eek
intervention
Stress
Psychological
distress
1-10self-report(stress)
Emotional
BehaviorCategory
oftheSickness
Impact
Profile
(SIP)
Centerfor
Epidem
iological
Studies–
DepressionScale
(CES-D
)
Interventiongroup
wasmore
likely
thanGTto
report
improvem
entfor
stress
andscore
higher
onSIP.
Random
allocation
Nopower
calculation
Sample4
50
Blindingofoutcome
measures
(continued
)
Aging & Mental Health 7
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
Table
2.Continued.
Reference
number
Interventiontype
Author(s)
(year)
Participants
Intervention(s)
Outcomes
Outcomemeasures
Results
Studydesign
7Outpatient
clinic-based
intervention
Jayadevappa
etal.(2007)
Sample
size¼23
Meanage¼65
Male:39%
Fem
ale:61%
Black:100%
Congestiveheart
failure
(CHF)with
anejectionfrac-
tionof5
.40
Transcendental
meditation
program
Intervention
group,n¼13
Controlgroup,
n¼10
6-m
onth
intervention
Clinicaloutcome
Health-related
quality
ofcare
(HRQoL)
Rehospitalization
Six-m
inute
walk
test
HRQoL
Perceived
stress
score
(PSS)
Centerfor
Epidem
iologic
Studies
DepressionScale
(CES-D
)
Brain
natriuretic
peptide(BNP)
Cortisollevel
Number
of
hospitalizations
Treatm
entgroup
significantly
improved
onthe
depression
outcome
comparedto
CT
from
baselineto
sixmonths.
Random
allocation
Nopower
calculation
Sample5
50
8Home-based
intervention
LaFramboise
etal.(2003)
Sample
size¼90
Meanage¼70
Male:50%
White:
83%
Black:13%
Other
race:4%
Recenthospitaladmit
forheart
failure
HealthBuddy
Program
Telephonic
disease
managem
ent,
n¼26
Homehealthcare,
n¼23
HealthBuddy
(in-home
telehealth
communication
device),n¼21
HomeVisit/H
ealth
Buddy,n¼20
6-m
onth
intervention
Self-efficacy
FunctionalStatus
Depression
Quality
ofLife(Q
OL)
BarnasonEfficacy
ExpectationScale
Heart
Failure
(BEES-H
F)
Geriatric
Depression
Scale
(GDS)
6-M
inute
Walk
Test
(6MWT)
MedicalOutcomes
Study36-Item
Short-Form
HealthStatus
Survey
(SF-36)
Groupreceiving
telephonic
disease
managem
ent
showed
significantlyless
confidence
intheir
abilityto
manage
theirHF.No
other
statistically
significantdiffer-
encesamong
groups.
Random
allocation
Nopower
calculation
Sample4
50
8 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

9Home-based
intervention
Martensson
etal.(2005)
Sample
size¼153
Meanage¼79
Male:54%
Fem
ale:46%
Patients
withheart
failure
inprimary
healthcare
Nurse-led
intervention
aim
edat
improvingself-
managem
entof
heart
failure
Treatm
entgroup,
n¼78
Usualcare
group,
n¼75
Meanage:79years
12-m
onth
intervention
Health-relatedquality
oflife
Depression
MedicalOutcomes
Study36-Item
Short-Form
HealthStatus
Survey
(SF-36)
ZungSelf-Rating
DepressionScale
(SDS)
Interventiongroup
wassignificantly
bettermaintaining
HRQOLand
experience
of
depressionto
a
greaterextentthan
thecontrolgroup.
Random
allocation
80%
power
calculation
Sample4
50
10
Home-based
intervention
Riegel
etal.
(2006)
Sample
size¼134
Meanage¼72
Male:46%
Fem
ale:54%
Hispanic:100%
Chronic
heart
failure
(HF)
AtHomewith
Heart
Failure
telephonecase
managem
ent
Treatm
entgroup,
n¼69
Controlgroup,
n¼65
6-m
onth
intervention
Hospitalization
Quality
ofLife(Q
OL)
Depression
Minnesota
Living
withHeartFailure
Questionnaire
(MLHFQ)
EQ-5D
PatientHealth
Questionnaire,
9-item
measure
of
depressionseverity
Nostatistically
significant
differences
betweenTG
and
CTgroupsforany
oftheoutcomes.
Random
allocation
80%
power
calculation
Sample4
50
11
Outpatient
clinic-based
intervention
Salm
inen
etal.(2005)
Sample
size¼279
Meanage¼74
Male:47%
Fem
ale:53%
Adults
Heart
disease
Livingin
community
Depressivesymptoms
Health
advocacy,
counselingand
activationpro-
gram
Intervention
group,n¼116
Controlgroup,
n¼106
16-m
onth
intervention
Depression
ZungSelf-rating
DepressionScale
(SDS)
Overall,no
statistically
significant
difference
between
TG
andCT
groupsfor
depression.
However,among
male
participants
withdepression,
Intervention
outperform
edCT;
depressed
women
inTG
andCT
groupsshowed
improvem
ent.
Random
allocation
Nopower
calculation
Sample4
50
(continued
)
Aging & Mental Health 9
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

Table
2.Continued.
Reference
number
Intervention
type
Author(s)
(year)
Participants
Intervention(s)
Outcomes
Outcomemeasures
Results
Studydesign
12
Home-based
intervention
Schwartz
etal.
(2008)
Sample
size¼102
Meanage¼78
Male:48%
Fem
ale:52%
White:
81%
Non-W
hite:
19%
Homecare
receiver
withhart
failure
(HF)andcare-
giver
dyads
Telem
onitoring
intervention
Telem
onitoring
group,
n¼51
Controlgroup,
n¼51
90-day
intervention
Hospital
readmission
Emergency
departmentvisit
Costsofcare
Functionalstatus
Depressive
symptoms
Quality
oflife
Caregiver
mastery
Medicalrecord
review
after
90days’
postdiscahrge
ActivitiesofDaily
Livings(A
DLs)
Independent
ActivitiesofDaily
Living(IADLs)
Centerfor
Epidem
iological
Studies
DepressionScale
(CES-D
)
Minnesota
Living
withHF
questionnaire
(MLWHF)
Philadelphia
Geriatric
CenterCaregiving
AppraisalScale
(PGCCAS)
Nosignificanteffect
oftelemonitoring
interventionwas
found.
Random
allocation
80%
power
calculation
13
Outpatient
clinic-based
intervention
Sekiet
al.
(2003)
Sample
size¼38
Meanage¼70
Male:100%
Coronary
artery
disease
(CAD)
Post
majorcoronary
event
Phase
IIcardiac
rehabiliation
program
Intervention
group,
n¼20
Controlgroup,
n¼18
6-m
onth
intervention
Quality
ofLife
(QOL)
Depression
Anxiety
MedicalOutcome
StudyShort-Form
(SF-36)
Stait-TraitAnxiety
Inventory
Questionnaire(STAI)
ZungSelf-Rating
DepressionScale
(SDS)
Interventiongroup
improved
significantlyfor
QOLandanxiety
butnotfor
depression;CT
showed
no
significant
improvem
entfor
anyoftheout-
comes.
Random
allocation
Nopower
calculation
Sample5
50
Blindingofoutcome
measures
10 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

14
Outpatient
clinic-and
home-based
intervention
Witham
etal.
(2005)
Sample
size¼82
Meanage¼80
Male:83%
Fem
ale:17%
Chronic
heart
failure
Seatedexercise
program
Intervention
group,
n¼41
Controlgroup,
n¼41
6-m
onth
intervention
Quality
ofLife
(QOL)
Anxiety
Depression
6Minute
Walk
Test
(6MWT)
Guyattchronic
heart
failure
questionnaire
HospitalAnxiety
and
DepressionScale
(HADS)
Philadelphia
Geriatric
Morale
Scale
Functional
Lim
itations
Profile
Treatm
entgroup
showed
significant
improvem
entin
physicalactivity;
nosignificant
difference
inQOL
betweenTG
and
CT
Random
allocation
Power
at90%
Blindingofoutcome
measures
15
Home-based
intervention
Woodend
etal.
(2007)
Sample
size¼249
Meanage¼66
Male:75%
Fem
ale:25%
Cardiacdisease
Telehome
monitoring
Heart
failure
groupwith
telehome
intervention,
n¼62
Hearfailure
groupwith
usualcare,
n¼59
Anginagroup
withtele-
home
intervention,
n¼62
Anginagroup
withusual
care,n¼66
3-m
onth
intervention
Readmission,
healthcare
resourceuse,
morbidity,and
quality
oflife
Minnesota
Living
withHeart
Failure
(LiH
Fe)
forHF
patients
MedicalOutcomes
StudyShort
Form
36(SF36)for
QOLandmental
healthassessm
ent
Telem
onitoring
significantly
improved
quality
oflife
and
functionalstatus
inpatients
with
HF.
Random
allocation
Nopower
calculation
Sample4
50
Aging & Mental Health 11
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

ranged from 11% to 38%. Jayadevappa et al.’s (2007)study had 100% African Americans, and Riegel,Carson, Glaser, and Romero (2006) study had 100%Hispanics.
Outcome measures
The most common measure administered to assessdepression severity was the Center for EpidemiologicStudies – Depression Scale (CES-D), followed by theZung Self-Rating Depression Scale (SDS) and theGeriatric Depression Scale (GDS). Approximately33% of the studies (3, 4, 6, 7, 12) used CES-D, 20%of the studies (9, 11, 13) used SDS, and 13% of thestudies (5, 8) used GDS. Other standardized depressionmeasures included the Hospital Anxiety andDepression Scale (HADS), the SCL-90R DepressionScale, and the Patient Health Questionnaire 9-itemmeasure of depression severity. Woodened et al. (2007)assessed mental health status using the MedicalOutcomes Study Short Form 36 (SF36).
Intervention modalities
Home-based and outpatient clinic-based interventionswere the major inclusion criterion for this review.About 47% of the studies (4, 5, 8, 9, 10, 12, 15) usedhome-based interventions, and 33% of the studies(2, 6, 7, 11, 13) used outpatient clinic-based interven-tions. Three studies (1, 3, 14) carried out interventionsthat occurred in combination at the outpatient clinicand in the patient’s home. Regarding the specificintervention components, four studies (1, 5, 13, 14)used a typical exercise protocol: three studies used awalking program, one study used Tai Chi Chuan andChi Kung exercise, and one study used a cardiacrehabilitation program. Six studies (4, 8, 9, 10, 12, 15)used telehealth interventions. Three of these studiesused self-disease management interventions including aprogram named Women Take PRIDE (3, 6) and anurse-led program (9). Other interventions includedTranscendental Meditation program (TM) for stressreduction (7) and a secondary prevention clinic (2). Allstudies provided detailed descriptions of theinterventions.
Study quality rating scale
As shown in Table 1, using Gellis and Kenaley’s (2008)study quality rating scale, we assessed the overallquality of methodology used in the reviewed studies.The average score of the overall methodology qualitywas 4.7 ranging from 3 to 7. About 60% (n¼ 15) of thestudies (3, 4, 5, 6, 7, 9, 10, 12, 14) received scores abovethe average. Jayadevappa et al.’s (2007) study thatcompared Transcendental Medication (TM) with usualcare and Martensson, Stromberg, Dahlstrom,Karlsson, and Fridlund’s (2005) study that comparedself-disease management with usual care received the
highest score. None of the included studies met thecriteria of performance bias and treatment fidelity.
Depression treatment outcomes and effect sizes ofinterventions
Overall, sample participants reported mild depressionsymptom levels at baseline. Table 3 shows thecomparisons of intervention effect on depression out-comes between treatment and control groups of thereviewed studies. Three home-based intervention stu-dies (5, 9, 15) and two outpatient clinic-based inter-vention studies (7, 11) found the treatment groups tobe significantly superior to the control groups.Salminen et al.’s study (2005) showed the longesttreatment effect (16 months) followed by Gary et al.’s(2004) exercise program and Jayadevappa et al.’s(2007) Transcendental Meditation program (6months). Barrow et al. (2007) compared the effect ofan exercise intervention to medical supervision anddrug treatment as usual care and found a significantdecrease in depression scores in the treatment group at4-month follow-up. However, their study found nooverall difference in depression outcomes betweentreatment and control groups. Salminen, Isoaho,Vahlberg, Ojanlatva, and Kivela, (2005) tested ahealth advocacy intervention to usual care, and con-ducted four different types of comparisons including(a) treatment group vs. control group for all men,(b) treatment group vs. control group for all women,(c) treatment group vs. control group for men withZSDS� 45, and (d) treatment group vs. control groupfor women with ZSDS� 45. The authors foundsignificant within-group differences in ZSDS scoresover time for both treatment and control groupsamong women with ZSDS� 45. Treatment group wassignificantly superior to control group among menwith ZSDS� 45 at 16-month follow-up.
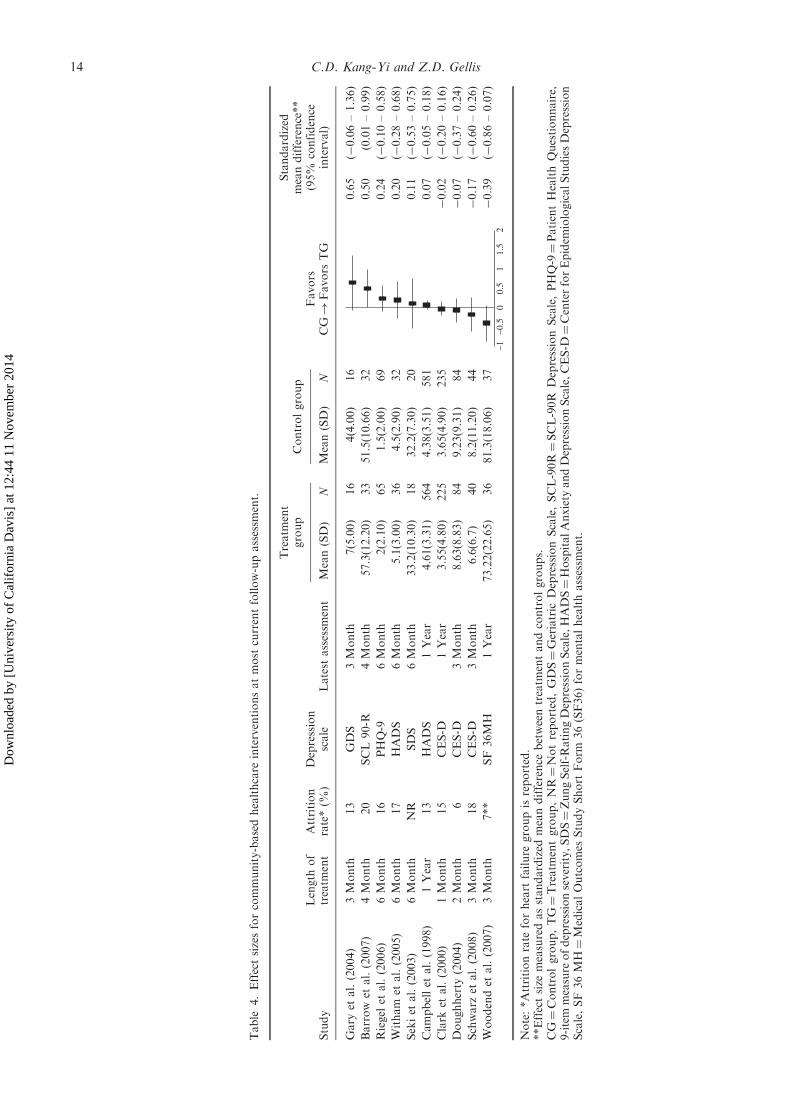
The mean weighted effect size (ES) of the interven-tions from the meta analysis was 0.11 (Table 4). Therange of ESs was from� 0.39 (in favor of controlgroup) to 0.65 (in favor of treatment group), and sixstudies showed positive ESs. Studies with positive ESshad longer treatment periods with the final assessmentat the end of treatment. The length of treatment forthese studies (1, 2, 5, 10, 13, 14) ranged from 12 to 52weeks. The studies with negative ESs (3, 4, 12, 15) hadrelatively shorter treatment periods, but had follow-upperiods up to 11 months. Exercise interventionsshowed higher ESs that favored treatment groupsand all telehealth care interventions showed negativeESs that favored control groups except for one study.We examined the depression outcome measures chosenby the investigators and found that studies using theGeriatric Depression Scale showed the largest positiveES (ES¼ 0.65, CI¼�0.11 to 1.41) followed by theSymptom Checklist 90-R (ES¼ 0.50, CI¼ 0.01 to0.99), Patient Health Questionnaire-9 (ES¼ 0.24,CI¼�0.10 to 0.58), Hospital Anxiety and
12 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

Depression Scale (ES¼ 0.20, CI¼�0.23 to 0.64), andSelf-Rating Depression Scale (ES¼ 0.11, CI¼�0.53 to0.75). Interventions that used the Center forEpidemiologic Studies – Depression Scale and SF-36Mental Health Scale had negative ESs favoring controlgroups. Studies with larger ESs had relatively smallersample sizes. The top three studies with the largest ESshad sample sizes ranging from 32 to 65. Attrition ratesof the studies included in the meta analysis rangedfrom 6% to 28%. Average attrition rates of the studieswith positive ESs and negative ESs were 15.8% and13.0%, respectively. The mean age, the gender mix,and the racial mix of study samples were notsignificantly different between the interventions withpositive ESs and negative ESs (Table 4).
Discussion
Based on the inclusion criteria, we selected andreviewed 15 studies of community-based health inter-ventions for older adults with heart disease andexamined intervention impact on depression outcomes.The interventions show wide variations in terms ofsample size, treatment protocol, and length of inter-vention, outcomes, and methodological quality. Whilesample sizes varied widely, outpatient clinic-based
interventions had relatively larger sample sizes com-pared to home-based interventions. Specifichome-based and/or outpatient clinic-based interven-tions include self care, exercise, rehabilitation, tele-health care, and prevention. The intervention periodacross studies also greatly differ ranging from 1 to 16months. The selected studies used seven differentdepression outcome measures including the: CES-D,GDS, SDS, HADS, the SCL-90R Depression Scale,the Patient Health Questionnaire, and SF 36Short-Form mental health scale.
The reviewed studies appear to lack rigorousmethodological approaches required for the validityand generalizability of the study findings. The averagescore of overall methodological quality was 4.7 out of apossible score of 10. Quality problems include lack ofsufficient power, detection bias, lack of intent-to-treatanalysis, lack of interventionist training, and notreatment fidelity reported. Less than 30% of thestudies met these criteria. In clinical trials, selectionbias, performance bias, detection bias, and attritionbias are all related to internal validity (Juni, Altman, &Egger, 2001), and 70% of the selected studies reviewedhave a serious internal validity problem based on theirpublished report.
Among the studies showing positive ESs, 67% ofstudies were home-based interventions or home- and
Table 3. Intervention effect on depression outcomes: treatment vs. control group comparisons.
InterventionStudy
Number
Months
BS 1 2 3 4 5 6 7 12 16
Self-disease management vs. UC 6 ns ns ns3 ns ns
Secondary prevention clinic vs. generalist practitionerclinic as UC
2 ns
Cardiac rehabilitation vs. UC in outpatient clinic 13 nsNurse-led education and counseling vs. unspecified UCNo depression 9 ns ns nsMild depression 9 ns ns nsModerate/severe depression 9 ns þ ns
Transcendental Meditation vs. health education as UC 7 ns þ þ
Exercise vs. unspecified UC 14 ns* nsExercise vs. education as UC 5 þ ns þ
Exercise vs. medical supervision and drug treatment asUC
1 ns
Telehealth care vs. unspecified UC 12 ns ns15 þ þ ns10 ns ns ns
Telehealth care vs. education as UC 4 ns nsHealth advocacy, counseling, and activation program
vs. unspecified UCMen with ZSDS� 45 vs. UC 11 þ
Women with ZSDS� 45 vs. UC 11 nsTelephonic vs.Home visit vs.Health Buddy vs.Home visit/Health Buddy 8 ns ns
Notes: Studies reported assessment periods in weeks were recalculated to months. BS¼Baseline; UC¼ usual care; ns¼ nosignificant difference between treatment and control groups; þ¼ treatment group is superior to control group on outcomes.*While this study reports significant percentage-mean-score change between treatment and control groups at 3-month follow-upassessment, it is noted as ‘‘ns’’ as the study reports no significant mean score change between the two groups.
Aging & Mental Health 13
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
Table
4.Effectsizesforcommunity-basedhealthcare
interventionsatmost
currentfollow-upassessm
ent.
Study
Length
of
treatm
ent
Attrition
rate*(%
)Depression
scale
Latest
assessm
ent
Treatm
ent
group
Controlgroup
Favors
CG!
Favors
TG
Standardized
meandifference**
(95%
confidence
interval)
Mean(SD)
NMean(SD)
N
Gary
etal.(2004)
3Month
13
GDS
3Month
7(5.00)
16
4(4.00)
16
–1–0
.50
0.5
11.
52
0.65
(�0.06–1.36)
Barrow
etal.(2007)
4Month
20
SCL90-R
4Month
57.3(12.20)
33
51.5(10.66)
32
0.50
(0.01–0.99)
Riegel
etal.(2006)
6Month
16
PHQ-9
6Month
2(2.10)
65
1.5(2.00)
69
0.24
(�0.10–0.58)
Witham
etal.(2005)
6Month
17
HADS
6Month
5.1(3.00)
36
4.5(2.90)
32
0.20
(�0.28–0.68)
Sekiet
al.(2003)
6Month
NR
SDS
6Month
33.2(10.30)
18
32.2(7.30)
20
0.11
(�0.53–0.75)
Campbellet
al.(1998)
1Year
13
HADS
1Year
4.61(3.31)
564
4.38(3.51)
581
0.07
(�0.05–0.18)
Clark
etal.(2000)
1Month
15
CES-D
1Year
3.55(4.80)
225
3.65(4.90)
235
�0.02
(�0.20–0.16)
Doughherty
(2004)
2Month
6CES-D
3Month
8.63(8.83)
84
9.23(9.31)
84
�0.07
(�0.37–0.24)
Schwarz
etal.(2008)
3Month
18
CES-D
3Month
6.6(6.7)
40
8.2(11.20)
44
�0.17
(�0.60–0.26)
Woodendet
al.(2007)
3Month
7**
SF36MH
1Year
73.22(22.65)
36
81.3(18.06)
37
�0.39
(�0.86–0.07)
Note:*Attritionrate
forheart
failure
groupisreported.
**Effectsize
measuredasstandardized
meandifference
betweentreatm
entandcontrolgroups.
CG¼Controlgroup,TG¼Treatm
entgroup,NR¼Notreported,GDS¼Geriatric
DepressionScale,SCL-90R¼SCL-90R
DepressionScale,PHQ-9¼PatientHealthQuestionnaire,
9-item
measure
ofdepressionseverity,SDS¼ZungSelf-RatingDepressionScale,HADS¼HospitalAnxiety
andDepressionScale,CES-D¼CenterforEpidem
iologicalStudiesDepression
Scale,SF36MH¼MedicalOutcomes
StudyShort
Form
36(SF36)formentalhealthassessm
ent.
14 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

outpatient-based interventions for older adults withheart disease. Based on these findings, home-basedinterventions may be considered as one strategy inreducing depressive symptoms in older adults withheart disease. In these patients, depression is not onlyhighly prevalent, but also characterized by symptoms(e.g. anhedonia and suicidal ideation) and condition(such as comorbid cardiovascular pulmonary diseases,cognitive impairment, and functional disability) asso-ciated with negative outcomes. Mobility limitationsalong with other disabilities are significant predictorsof depressive symptoms. Consequently, loneliness andisolation are likely to contribute to increased depres-sive symptoms. Home-based interventions can reducesocial isolation and eliminate barriers to transporta-tion, as well as meeting older adults’ care preference. Inaddition, home-based interventions may be more costeffective than outpatient clinic-based interventions.However, any general conclusions drawn from thesedata are mitigated by the limited number of rando-mized controlled studies and the varying quality andmethodological limitations of the selected studies.
Effect sizes were larger for studies with a longertreatment period than those with a shorter treatmentperiod. Nonetheless, drawing a conclusion of theassociation between length of treatment and depressionoutcome is difficult as the analysis included only themost current assessment outcomes. Higher attritionrate may inflate the treatment effect. The attrition rateof studies with positive ESs was 2.8% higher than thatof studies with negative ESs. Nonetheless, this analysisdid not lend itself to determine the influence ofattrition rates on treatment effect. Further study thatexamines if there is attrition influence on the treatmenteffect will provide more definite information. Mostinterventions included in the meta analysis recruitedparticipants with mild depression symptoms. Thus, thestudies with positive effect sizes may be, in fact,underpowered since it is difficult to demonstrate atreatment effect for those patients with mild depression(Zarit & Femia, 2008).
The studies reviewed in this article describedinterventions specifically for heart-disease manage-ment interventions and not for depression care.However, many of the components utilized in heartdisease interventions (e.g. exercise, chronic-diseasemanagement strategies, and education) are also appliedin depression care interventions. Education andchronic-disease management may reduce depressionby teaching patients how to change lifestyle andregulate symptoms (Martensson et al., 2005). TaiChi, Chi Kung, and Transcendental Meditationtechniques are designed for physical and cognitiverelaxation (Barrow et al., 2007; Jayadevappa et al.,2007), and these interventions have the potential toreduce patients’ depressive symptoms. For exerciseinterventions, attending regular programs may leadolder adults to become more active and less depressed(Gary & Lee, 2007). Group affiliations or socialsupport created through an intervention may also
play a key factor in lowering depression severity (Gary
& Lee, 2007).PRIDE, a well-known heart-disease management
program, was not associated with significant reduction
of depression. Clark et al. (2000) reported that theintentional shifts in PRIDE to emphasize physical
activity may be the reason why they did not find
significant treatment effects on depression symptoms.
Janz et al.’s (2004) study on PRIDE also showed no
significant results on depression outcomes but did findan effect on stress reduction. The authors suggest that
one of the reasons for negative findings were likely due
to the lack of sensitivity of the measurements chosen
(CES-D).Older adults with heart disease clearly have differ-
ent care management needs than younger patients.
Older adults are more likely to have lower
physical-functioning capacity than younger cohorts,
or they may be homebound due to debilitating chronicmedical conditions. More importantly, older adults are
at high risk of suffering from depression. High rates of
depression are well documented among medically ill
elderly and those confined to their homes by medical
illness and disability. Their homebound status is abarrier for access to depression care. Left untreated,
depression leads to exacerbation of medical conditions,
deterioration in functioning, and increased health
costs.It is possible to view interventions in a sample with
low levels of depressive symptoms as of the prevention
program type. In that regard, one might observe
differences over longer periods of time, with symptoms
remaining low in the treatment condition and rising in
the control condition from baseline points (Zarit &Femia, 2008). Thus, longer observation phases may be
needed to observe a treatment effect (Mittelman, Roth,
Coon, & Haley, 2004; Zarit & Femia, 2008).Psychosocial heart disease intervention studies
excluded from this review focused on quality-of-lifeimprovement and measured anxiety and/or distress
levels. These studies were also excluded because
depression outcomes were not assessed, they were not
randomized controlled trials, and the sample wasyounger than 64 years of age. The main
components of these psychosocial interventions
included education and counseling (e.g., Jaarsma et
al., 2000; Ramachandran et al., 2007). Some of the
quality-of-life interventions included an exercisecomponent as well. Since most community-based
interventions included exercise, education, and
self-management, the strength of each component
used in the intervention may have resulted in variabil-ity on depression outcomes. Identifying which compo-
nent of the intervention has a direct effect on
depression may contribute to more effective and
efficient care for older adults with heart disease.
Furthermore, evidence-based treatments for depres-sion such as cognitive behavioral therapy, interper-
sonal psychotherapy, or problem solving therapy can
Aging & Mental Health 15
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

be easily integrated into heart disease interventions formedically ill elderly and be evaluated for effectiveness.
Conclusion
The strengths of this meta analytic review include theuse of a broad search strategy and standardizedinclusion and study evaluation criteria. One limitationis that quasi-experimental studies were not consideredeven when experimental designs offer more support forthe association of a causal relationship. Implementingand evaluating a randomized field trial is inherentlydifficult in ‘‘real world’’ home and community-basedsettings. The contribution of lower levels of evidenceshould not be overlooked especially when improvingaccess and quality of care for depressed medically illolder adults is critical. Another limitation is that themeta analysis was conducted using all availableoutcome data at the most current assessment. Thisexcluded other assessment outcomes during thefollow-up period.
Upon examination of the methodological quality ofthe studies and the meta analysis, we address impor-tant implications. First, depression outcome researchon community-health interventions for medically illolder adults with heart disease is needed to providefurther evidence of intervention effects on depression.Second, future intervention studies should conductmore rigorous trials that investigate its effects ondepression over longer time periods with morediversified samples of older adults with heart disease.Third, reports of randomized trial studies for heartdisease management should consider using thewell-known Consolidated Standards of ReportingTrials (CONSORT). Finally, since heart disease is acommon diagnosis in older persons and highlyassociated with depression, systematic review ofcommunity-health interventions for older adults withheart disease should be routinely conducted. In addi-tion, a larger number of studies should be included inthe systematic review and meta analysis. Interventionswith quasi experimental design could be considered aspart of inclusion criteria. Finally, future meta analysisshould consider including sub-group analyses by dif-ferent demographic characteristics of the study sample,common depression outcome measures, and assess-ment stages. This may lead to limiting the greatvariability in methodology and interventions and toprovide better understanding of the evidence. With theevidence based on sound methodological trials, clin-icians will be more knowledgeable about effectiveinterventions for community-dwelling older adultswith heart disease and depression.
References
American Heart Association (2009). Heart disease and
stroke statistics 2009 Update: A report from theAmerican Heart Association Statistics Committee and
Stroke Statistics Subcommittee. Retrieved February
25, 2009, from http://circ.ahajournals.org/cgi/reprint/
CIRCULATIONAHA.108.191261\Appels, A., Elderen, T., Bar, F., Pol, G., Erdman, R.,
Assman, M., et al. (2006). Effects of a behavioural
intervention on quality of life and related variables in
angioplasty patients: Results of the exhaustion interven-
tion trial. Journal of psychosomatic Research, 61, 1–7.Barrow, D.E., Bedford, A., Ives, G., O’Toole, L., &
Channer, K.S. (2007). An evaluation of the effects of Tai
Chi Chuan and Chi Kung training in patients with
symptomatic heart failure: A randomized controlled pilot
study. Postgraduate Medical Journal, 83, 717–721.
Bruce, M.L., McAvay, G.J., Raue, P.J., Brown, E.L.,
Meyers, B.S., Keohane, D.J., et al. (2002). Major depres-
sion in elderly home health care patients. The American
Journal of Psychiatry, 159, 1367–1374.Campbell, N.C., Thain, J., Deans, G., Ritchie, L.D., &
Rawles, J.M. (1998). Secondary prevention in coronary
heart disease: Baseline survey of provision in general
practice. British Medical Journal, 316, 1430–1437.Centers for Disease Control and Prevention (2005).
National Center for Health Statistics, National Home
and Hospital Survey 2005: Table 94. Retrieved February
25, 2009, from http://www.cdc.gov/nchs/data/hus/
hus05.pdf#094
Clark, N.M., Janz, N.K., Dodge, J.A., Schork, A., Fingerlin,
T.E., Wheeler, J.R.C., et al. (2000). Changes in functional
health status of older women with heart disease:
Evaluation of a program based on self-regulation.
Journal of Gerontology, 55B(2), S117–S126.Dougherty, C.M., Lewis, F.M., Thompson, E.A., Baer, J.D.,
& Kim, W. (2004). Short-term efficacy of a telephone
intervention by expert nurses after an implantable
cardioverter defibrillator. PACE, 27, 1594–1602.Frasure-Smith, N., Lesperance, F., & Talajic, M. (1995).
The impact of negative emotions on prognosis following
myocardial infarction: Is it more than depression? Health
Psychology, 14(5), 388–398.Frasure-Smith, N., Lesperance, F., & Talajic, M. (in press).
Depression and 18-month prognosis after myocardial
infarction. Circulation, 91(4), 999–1005.Freedland, K.E., Rich, M., Skala, J., Carney, R.M., Davila-
Roman, V., & Jaffe, A.S. (2003). Prevalence of depression
in hospitalized patients with congestive heart failure.
Psychosomatic Medicine, 65, 119–128.Gary, R., & Lee, S. (2007). Physical function and quality of
life in older women with diastolic heart failure: Effects of a
progressive walking program on sleep patterns. Progress in
Cardiovascular Nursing, 22, 72–80.Gary, R.A., Sueta, C.A., Dougherty, M., Rosenberg, B.,
Cheek, D., Preisser, J., et al. (2004). Home-based exercise
improves functional performance and quality of life in
women with diastolic heart failure. Heart & Lung, 33,
210–218.
Gellis, Z.D. (2010). Depression screening in medically ill
homecare elderly. Best Practices in Mental Health: An
International Journal, 6(1), 1–16.Gellis, Z.D., & Kenaley, B. (2008). Problem-solving therapy
for depression in adults: A systematic review. Research on
Social Work Practice, 18(2), 117–131.
Gellis, Z.D., & Bruce, M.L. (2009). Problem solving therapy
for subthreshold depression in home healthcare patients
with cardiovascular disease. American Journal of Geriatric
Psychiatry. DOI: 10.1097/JGP.0b013e3181b21442 (pub-
lished ahead of print).
16 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
Glassman, A.H., & Shapiro, P.A. (1998). Depression and the
course of coronary artery disease. American Journal of
Psychiatry, 155, 4–11.Hedges, L.V. (1981). Distribution theory for Glass’s estima-
tor of effect size and related estimators. Journal of
Educational Statistics, 6, 106–128.Higgins, J.P.T. & Green, S. (Eds). Cochrane Handbook for
Systematic Reviews of Interventions Version 5.0.1.
[Updated September 2006]. The Cochrane Collaboration,
2008. Retrieved February 25, 2009, from www.cochrane-
handbook.org
Jaarsma, T., Halfens, R., Tan, F., Abu-Saad, H., Dracup, K.,
Diederiks, J., et al. (2000). Self-care and quality of life in
patients with advanced heart failure: The effect of a
supportive educational intervention. Heart & Lung, 29(5),
319–330.Janz, N.K., Dodge, J.A., Janevic, M.R., Lin, X.,
Donaldson, A.E., & Clark, N.M. (2004).
Understanding and reducing stress and psychological
distress in older women with heart disease. Journal of
Women & Aging, 16(3/4), 19–38.Jayadevappa, R., Johnson, J.C., Bloom, B.S., Nidich, S.,
Desai, S., Chhatre, S., et al. (2007). Effectiveness of
transcendental meditation on functional capacity and
quality of life of African Americans with congestive
heart failure: A randomized control study. Ethnic &
Disease, 17(1), 72–77.
Johri, M., Beland, F., & Bergman, H. (2003). International
experiments in integrated care for the elderly: A synthesis
of evidence. International Journal of Geriatric Psychiatry,
18, 222–235.Juni, P., Altman, D.G., & Egger, M. (2002). Assessing the
quality of randomized controlled trials. In M. Egger,
G.D. Smith, & D.G. Altman (Eds.), Systematic Reviews in
Health Care Mata-Analysis in Context (pp. 87–108).
London: BMJ Publishing Group.LaFramboise, L.M., Todero, C.M., Zimmerman, L., &
Agrawal, S. (2003). Comparison of Health Buddy with
traditional approaches to heart failure management.
Family & Community Health, 26(4), 275–288.
Martensson, J., Stromberg, A., Dahlstrom, U., Karlsson,
J.E., & Fridlund, B. (2005). Patients with heart failure in
primary health care: Effects of a nurse-led intervention on
health-related quality of life and depression. The European
Journal of Heart Failure, 7, 393–403.Martin, P., Bishop, A., Poon, L., & Johnson, M.A. (2006).
Influence of personality and health behaviors on fatigue in
late and very late life. The Journals of Gerontology: Series
B, 61, P161–P166.Mittelman, M.S., Roth, D.L., Coon, D.W., & Haley, W.E.
(2004). Sustained benefit of supportive intervention for
depressive symptoms in caregivers of patients with
Alzheimer’s disease. American Journal of Psychiatry,
161(5), 850–856.
Moncher, F.J., & Prinz, R.J. (1991). Treatment fidelity in
outcome studies. Clinical Psychology, 11, 247–266.National Heart Lung and Blood Institute (2007). National
Heart Lung and Blood Institute Fact Book, Fiscal Year
2007. Retrieved on February 28, 2009 from http://
www.nhlbi.gov/about/factbook/FactBookFinal.pdf
Nemeroff, C.B., Musselman, D.L., & Evans, D.L. (1998).
Depression and cardiac disease. Depression and Anxiety,
8(Suppl 1), 71–78.Penninx, B., Beekman, A., Honig, A., Deeg, D.,
Schoevers, R., Van Eijk, J., et al. (2001). Depression
and cardiac mortality: Results from a community-based
longitudinal study. Archives of General Psychiatry, 58,221–227.
Riegel, B., Carson, B., Glaser, D., & Romero, T. (2006).Randomized controlled trial of telephone case manage-
ment in Hispanics of Mexican origin with heart failure.
Journal of Cardiac Failure, 12(3), 211–219.Rudisch, B., & Nemeroff, C.B. (2003). Epidemiology of
comorbid coronary artery disease and depression.Biological Psychiatry, 54, 227–240.
Salminen, M., Isoaho, R., Vahlberg, T., Ojanlatva, A., &Kivela, S. (2005). Effects of a health advocacy, counseling,
and activation programme on depressive symptoms in
older coronary heart disease patients. International Journalof Geriatric Psychiatry, 20, 552–558.
Schwarz, KA., Mion, L.C., Hudock, D., & Litman, G.(Winter 2008). Telemonitoring of heart failure patients and
their caregivers: A pilot randomized controlled trial.
Progress in Cardiovascular Nursing, 23(1), 18–26.Seki, E., Watanabe, Y., Sunayama, S., Iwama, Y.,
Shimada, K., Kawawkami, K., et al. (2003). Effects ofphase III cardiac rehabilitation programs on
health-related quality of life in elderly patients with
coronary artery disease. Circulation Journal, 67, 73–77.Van Hout, H., Beekman, A., De Beurs, E., Comijs, H., Van
Marwijk, H., & De Hann, M. (2004). Anxiety and the riskof death in older men and women. British Journal of
Psychiatry, 185, 399–404.Witham, M.D., Gray, J.M., Argo, I.S., Johnston, D.W.,
Struthers, A.D., & McMurdo, M.E.T. (2005). Effect of a
seated exercise program to improve physical functionand health status in frail patients� 70 years of age with
heart failure. The American Journal of Cardiology, 95,
1120–1124.Woodened, A.K., Sherrard, H., Fraser, M., Stuewe, L.,
Cheung, T., & Struthers, C. (2007). Telehome monitoringin patients with cardiac disease who are at high risk of
remission. Heart & Lung, 37, 36–45.World Health Organization (2008). The Global Burden of
Disease: 2004 update. Geneva: WHO Press 2008.Zarit, S.H., & Femia, E.E. (2008). A future for family care
and dementia intervention research? Challenges and
strategies. Aging & Mental Health, 12(1), 5–13.
Appendix I. Reference list of other studies found
through literature search
Aimonino, N., Tibaldi, V., Barale, S., Bardelli, B., Pilon, S.,Marchetto, C., et al. (2007). Depressive symptoms and
quality of life in elderly patients with exacerbation of
chronic obstructive pulmonary disease or cardiac heartfailure: Preliminary data of a randomized controlled trial.
Archives of Gerontology and Geriatrics, Supplement, 1,
7–12.Bari, M.D., Pahor, M., Franse, L.V., Shorr, R.I., Wan, J.Y.,
Ferrucci, L., et al. (2001). Dementia and disabilityoutcomes in large hypertension trials: Lessons learned
from the systolic hypertension in the elderly program
(SHEP) trial. American Journal of Epidemiology, 153(1),72–78.
Blumenthal, J.A., Sherwood, A., Babyak, M.A., Watkins,L.L., Waugh, R., Georgiades, A., et al. (2005). Effects of
exercise and stress management training on markers of
Aging & Mental Health 17
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014
cardiovascular risk in patients with ischemic heart disease.
Journal of the American Medical Association, 293(13),
1626–1634.Davidson, P., Digiacomo, M., Zecchin, R., Clarke, M.,
Paul, G., Lamb, K., et al. (2008). A cardiac rehabilita-
tion program to improve psychosocial outcomes of
women with heart disease. Journal of Women’s Health,
17(1), 123–134.ENRICH Investigators (2000). Enhancing recovery in
coronary heart disease patients (ENRICHD): Study
design and methods. American Heart Journal, 139, 1–9.ENRICH Investigators (2003). Effects of treating depression
and low perceived social support on clinical events after
myocardial infarction. Journal of the American Medical
Association, 289(23), 3106–3116.
Evangelista, L.S., Doering, L.V., Lennie, T., Moser, D.K.,
Hamilton, M.A., Fonarow, G.C., et al. (2005). Usefulness
of a home-based exercise program for overweight and
obese patients with advanced heart failure. The American
Journal of Cardiology, 97, 886–890.Fletcher, A.E., Bulpitt, C.J., Thijs, L., Toumilehto, J.,
Antikainen, R., Bossini, A., et al. (2001). Quality of life
on randomized treatment for isolated systolic hyperten-
sion: Results from the Syst-Eur Trial. Journal of
Hypertension, 20, 2069–2079.
Frasure-Smith, N., Lesperance, F., Gravel, G., Masson, A.,
Juneau, M., & Bourassa, M.G. (2002). Long-term
survival differences among low-anxious, high-anxious
and repressive copers enrolled in the Montreal heart
attack readjustment trial. Psychosomatic Medicine, 64,
571–579.Frasure-Smith, N., Lesperance, F., & Talajic, M. (1995).
The impact of negative emotions on prognosis following
myocardial infarction: Is it more than depression? Health
Psychology, 14(5), 388–398.Gary, R. (2006). Exercise self-efficacy in older women with
diastolic heart failure: Results from a walking program
and education intervention. Journal of Gerontological
Nursing, 32(7), 31–39.Gary, R., & Lee, S. (2007). Physical function and quality of
life in older women with diastolic heart failure: Effects of a
progressive walking program on sleep patterns. Progress in
Cardiovascular Nursing, 22, 72–80.
Glassman, A.H., O’Connor, C.M., Califf, R.M.,
Swedberg, K., Schwartz, P., Bigger, J.T., et al. (2008).
Sertraline treatment of major depression in patients
with acute MI or unstable angina. Journal of American
Medical Association, 288(6), 701–709.Greenwald, B.S., Kramer-Ginsberg, E., Krishnan, K.R.R.,
Hu, J., Ashtari, M., Wu, H., et al. (2001). A controlled
study of MRI signal Hypertensities in older depressed
patients with and without hypertension. Journal of
American Geriatrics Society, 49, 1218–1225.Hamm, L.F., Kavanagh, T., Campbell, R.B., Mertens, D.J.,
Beyene, J., Kennedy, J., et al. (2004). Timeline for peak
improvements during 52 weeks of outpatient cardiac
rehabilitation. Journal of Cardiopulmonary Rehabilitation,
24, 374–382.Jaarsma, T., Halfens, R., Tan, F., Abu-Saad, H.,
Dracup., K., Diederiks, J., et al. (2000). Self-care and
quality of life in patients with advanced heart failure:
The effect of a supportive educational intervention.
Heart & Lung, 29(5), 319–330.Jerant, A., Kravitz, R., Moore-Hill, M., & Franks, P. (2008).
Depressive symptoms moderated the effect of chronic
illness self-management training on self-efficacy. Medical
Care, 46(5), 523–531.Jiang, W., O’Connor, C., Silva, S.G., Kuchibhatla, M.,
Cuffe, M.S., Callwood, D.D., et al. (2008). Safety and
efficacy of sertraline for depression in patients with CHF
(SADHART-CHF): A randomized, double-blind, pla-
cebo-controlled trial of sertraline for major depression
with congestive heart failure. American Heart Journal, 156,
437–444.Jolly, K., Lip, G.Y.H., Sandercock, J., Greenfield, S.M.,
Raftery, J.P., Mant, J., et al. (2003). Home-based versus
hospital-based cardiac rehabilitation after myocardial
infarction or revascularization: Design and rationale of
the Birmingham Rehabilitation Uptake Maximisation
Study (BRUM): A randomized controlled trail.
Cardiovascular Disorders, 3(10), 1–11.
Karlsson, M.R., Edstrom-Plu¡¡ss, C., Held, C.,
Henriksson, P., Billing, E., & Wallen, N.H. (2007).
Effects of expanded cardiac rehabilitation on psycho-
social status in coronary artery disease with focus on
type D characteristics. Journal of Behavioral Medicine,
30, 253–261.Koertge, J., Janszky, I., Sundin, O., Blom, M.,
Georgiades, A., Laszlo, K.D., et al. (2007). Effects of
a stress management program in vital exhaustion and
depression in women with coronary heart disease: A
randomized controlled intervention study. Journal of
Internal Medicine, 263, 281–293.Kohn, C., Petrucci, R., Baessler, C., Soto, D., &
Movsowitz, C. (2000). The effect of psychological
intervention on patients’ long-term adjustment to the
ICD: A prospective . study. PACE, 23(Part I), 450–456.Koukouvou, G., Kouidi, E., Lacovides, A., Konstantinidou,
E., Kaprinis, G., & Deligiannis, A. (2004). Quality of life,
psychological and physiological changes following exercise
training in patients with chronic heart failure. Journal of
Rehabilitation Medicine, 36(1), 36–41.
Krishnan, K.R., Doraiswamy, P.M., & Clary, C.M. (2001).
Clinical and treatment response characteristics of late-life
depression associated with vascular disease: A pooled
analysis of two multicenter trials with sertraline. Progress
in Neuro-Psychopharmacology and Biological Psychiatry,
25, 347–361.Kulcu, D.G., Kurtais, Y., Tur, B.S., Gulec, G., & Seckin, B.
(2007). The effect of cardiac rehabilitation on
quality of life, anxiety and depression in patients
with congestive heart failure: A randomized controlled
trial, short-tern results. Europa Medicophysica, 43(4),
489–497.Lacey, E.A., Musgrave, R.J., Freeman, J.V., Tod, A.M., &
Scott, P. (2004). Psychological morbidity after myocardial
infarction in an area of deprivation in the UK: Evaluation
of a self-help package. European Journal of Cardiovascular
Nursing, 3, 219–224.
Luskin, F., Reitz, M., Newell, K., Quinn, T.G., &
Haskell, W. (2002). A controlled pilot study of stress
management training of elderly patients with congestive
heart failure. Preventive Cardiology, 5, 168–176.
Marchionni, N., Fattirolli, F., Fumagalli, S., Oldridge, N.,
Lungo, F., Bonechi, F., et al. (2000). Determinants of
exercise tolerance after acute myocardial infarction in
older persons. Journal of the American Geriatrics Society,
48(2), 146–153.Mittag, O., China, C., Hoberg, E., Juers, E., Kolenda, K.,
Richardt, G., et al. (2006). Outcomes of cardiac
18 C.D. Kang-Yi and Z.D. Gellis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014

rehabilitation with versus without a follow-up intervention
rendered by telephone (Luebeck follow-up trial): Overall
and gender-specific effects. International Journal of
Rehabilitation Research, 29(4), 295–302.Nuyen, J., Spreeuwenberg, P.M., Beekman, A.T.F.,
Groenewegen, P.P., Bos, G.A.M., & Schellevis, F.G.
(2007). Cerebrovascular risk factors and subsequent
depression in older general practice patients. Journal of
Affective Disorders, 99, 73–81.Oslin, D.W., Ten Have, T.R., Streim, J.E., Datto, C.J.,
Weintraub, D., DiFilippo, S., et al. (2003). Probing the
safety of medications in the frail elderly: Evidence from a
randomized clinical trial of sertraline and venlafaxine in
depressed nursing home residents. Journal of Clinical
Psychiatry, 64(8), 875–882.Peter-Klimm, F., Muller-Tasch, T., Shellberg, D., Gensichen,
J., Muth, C., Herzog, W., et al. (2007). Rationale, design
and conduct of a randomized controlled trial evaluating a
primary care-based complex interventions to improve the
quality of life of heart failure patients: HICMan
(Heidelberg Integrated Case Management).
Cardiovascular Disorders, 7(25), 1471–2261.
Peters, R., Beckett, N., Nunes,M., Fletcher, A., Forette, F., &
Bulpitt, C. (2006). A substudy protocol of the hypertension
in the very elderly trial assessing cognitive decline and
dementia incidence (HYVET-COG). Drugs Aging, 23(1),
83–92.Ramachandran, K., Husain, N., Muikhuri, R., Seth, S.,
Vij, A., Kumar, M., et al. (2007). Impact of a
comprehensive telephone-based disease management pro-
gramme on quality-of-life in patients with heart failure.
The National Medical Journal of India, 20(2), 67–73.Riegel, B., Carlson, B., Glaser, D., & Romero, T. (2003).
Changes over 6-month in health-related quality of life in a
matched sample of Hispanics and non-Hispanics with
heart failure. Quality of Life Research, 12, 689–698.Santos, F.S., & Velasco, I.T. (2005). Clinical features of
elderly patients submitted to coronary artery bypass graft.
Gerontology, 51(4), 234–241.Schneiderman, N., Saab, P.G., Catellier, D.J., Powell, L.H.,
Debusk, R.F., Williams, R.B., et al. (2004). Psychosocial
treatment within sex by ethnicity subgruops in the
enhancing recovery in coronary heart disease clinical
trial. Psychosomatic Medicine, 66, 476–483.
Sheikh, J.I., Cassidy, E.L., Doraiswamy, P.M., Salomon,R.M., Hornig, M., Holland, P.J., et al. (2004). Efficacy,
safety, and tolerability of sertraline in patients with late-life depression and comorbid mental illness. Journal ofAmerican Geriatrics Society, 52, 86–92.
Shuldham, C.M., Fleming, S., & Goodman, H. (2002). The
impact of pre-operative education on recovery followingcoronary artery bypass surgery. European Heart Journal,23, 666–674.
Sneed, N.V., Paul, S., Michel, Y., VanBakel, A., &Hendrix, G. (2001). Evaluation of 3 quality of lifemeasurement tools in patients with chronic heart failure.
Heart & Lung, 30, 332–340.Southard, B.H., Southard, D.R., & Nuckolls, J. (2003).Clinical trial of an internet-based case managementsystem for secondary prevention of heart disease. Journal
of Cardiopulmonary Rehabilitation, 23, 341–348.Swenson, J.R., O’Connor, C.M., Barton, D., Van Zyl, L.T.,Swedberg, K., Forman, L.M, et al. (2003). Influence of
depression and effect of treatment with sertraline onquality of life after hospitalization for acute coronarysyndrome. American Journal of Cardiology, 92(1),
1271–1276.Wakefield, B.J., Bylund, C.L., Holman, J.E., Ray, A.,Scherubel, M., Kienzle, M.G., et al. (2008).
Nurse and patient communication profiles in ahome-based telehealth intervention for heart failuremanagement. Patient Education and Counseling, 71,285–292.
Witham, M.D., Argo, I.S., Johnston, D.W., Struthers, A.D.,& McMurdo, M.E.T. (2007). Long-term follow-up of veryolder heart failure patients enrolled in a trial exercise
training. American Journal of geriatric cardiology, 16(4),423–248.
Woodened, A.K., Sherrard, H., Fraser, M., Stuewe, L.,
Cheung, T., & Struthers, C. (2007). Telehome monitoringin patients with cardiac disease who are at high risk ofremission. Heart & Lung, 37, 36–45.
Zwisler, A., Soja, A., Rasmussen, S., Frederiksen, M.,Abadini, S., Appel, J., et al. (2008). Hospital-basedcomprehensive cardiac rehabilitation versus usual careamong patients with congestive heart failure, ischemic
heart disease, or high risk of ischemic heart disease:12-Month results of a randomized clinical trial. Preventionand Rehabilitation, 155, 1106–1113.
Aging & Mental Health 19
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a D
avis
] at
12:
44 1
1 N
ovem
ber
2014