a randomized trial of rigid gas permeable contact lenses to reduce progression of children’s...
TRANSCRIPT
A Randomized Trial of Rigid Gas PermeableContact Lenses to Reduce Progression of
Children’s Myopia
JOANNE KATZ, SCD, OLIVER D. SCHEIN, MD, MPH, BRIAN LEVY, OD, MSC,TOM CRUISCULLO, BS, SEANG-MEI SAW, MBBS, MPH, PHD,
UMA RAJAN, MBBS, MPH, FAMS, TAT-KEONG CHAN, FRCOPH, FRCS,CHONG YEW KHOO, FRCSOPH, FRACS, FAMS, AND SEK-JIN CHEW, FRCOPH, FAMS, PHD
● PURPOSE: To test whether rigid gas permeable (RGP)contact lens wear can reduced the rate of myopia pro-gression in school age children.● DESIGN: Randomized clinical trial.● METHODS:
Setting: Single clinical center.Study Population: Both eyes of 428 Singaporean
children.Inclusion Criteria: 6 through 12 years of age with
myopia between �1 and �4 diopters, astigmatism < 2diopters, no prior contact lens wear, no other ocularpathologies.
Intervention: Spectacle or RGP lens correction formyopia. After a 3-month adaptation period, 383 childrenwere followed, and 298 (78%) remained after 24months.
Outcome measures: Cycloplegic subjective refraction,keratometry, and axial length measured at 12 and 24months.● RESULTS: Children who adapted to contact lenses worethem for a median of 7 hours per day, but no more than40% wore them at least 8 hours per day, 7 days per week.Spectacles were worn for a median of 15 hours per day atthe time of the 24-month follow-up. There was an
increase in the spherical equivalent of �1.33 and �1.28diopters (P � .64), and axial length increased by 0.84and 0.79 mm (P � .38) over 2 years among childrenrandomized to contact lenses and spectacles, respectively.Adjustment for baseline differences between the groupsand for hours per day of contact lens wear did not alterthese findings.● CONCLUSIONS: Rigid gas permeable lenses did not slowthe rate of myopia progression, even among children whoused them regularly and consistently. It is unlikely thatthis intervention holds promise as a method by which toslow the rate of progression of myopia in children. (AmJ Ophthalmol 2003;136:82–90. © 2003 by Elsevier Inc.All rights reserved.)
M YOPIA IS A MAJOR CONCERN FOR ETHNIC CHI-
nese among whom the prevalence is very highand appears to have increased rapidly over a few
generations.1–9 The economic burden of myopia is great,with expenditures on spectacles and contact lenses esti-mated at $ 2 billion annually in the United States alone.10
The use of refractive surgery to correct myopia has alsoincreased considerably ever since lasers have been ap-proved for this purpose.11,12 Severe myopia has also beenincreasing in ethnic Chinese,2 and this has led to aconcern about its ophthalmic consequences such as myo-pic macular degeneration, retinal holes, tears and detach-ments, lattice degeneration, cataract, and glaucoma.13–15
It has been postulated that rigid contact lenses couldslow the progression of myopia in children.16–18 Severalpotential mechanisms have been offered, including im-proved retinal image quality with contact lens wear;flattening of the cornea, producing a temporary slowing ofmyopia progression; or an overcorrection for myopia whenfitting contact lenses. Several studies have examined thisissue, but each has had methodological problems. Stone19
enrolled 124 unmatched, nonrandomized spectacle wearers
Accepted for publication Jan 9, 2003.InternetAdvance publication at ajo.com Feb 13, 2003.From the Department of International Health, Johns Hopkins
Bloomberg School of Public Health, Baltimore, Maryland (J.K.); DanaCenter for Preventive Ophthalmology, Wilmer Eye Institute, JohnsHopkins School of Medicine, Baltimore, Maryland (J.K., O.D.S.);Bausch and Lomb, Rochester, New York (B.L., T.C.); Department ofCommunity, Occupational and Family Medicine, National University ofSingapore, Singapore (S.M.S.); School Health Services, Singapore(U.R.), and Singapore Eye Research Institute, Singapore (T.K.C.,C.Y.K., S.J.C.).
The study was conducted at the Singapore Eye Research Institute,Singapore.
Inquiries to Joanne Katz, ScD, the Johns Hopkins Bloomberg School ofPublic Health, 615 N. Wolfe St., Room W5009, Baltimore, MD 21205-2103; fax: (410) 955-2029; e-mail: [email protected]
© 2003 BY ELSEVIER INC. ALL RIGHTS RESERVED.82 0002-9394/03/$30.00doi:10.1016/S0002-9394(03)00106-5

and 244 contact lens wearers, but only 28 controls and 22contacts lens patients remained after 5 years of follow-up.Kelly and co-workers20 did not randomize their patients,and they did not provide information about baselinecomparability. Grosvenor and colleagues enrolled 100contact lens wearers and 39 nonrandomized controls. Thefollow-up was 56% among contact lens wearers and 51%among controls after 3 years.21,22 These studies all showedhigher rates of myopia progression among controls thanamong contact lens wearers, only some of which could beexplained by flattening of the cornea due to the contactlens wear. Andreo23 retrospectively analyzed 37 contactlens wearers and 19 spectacle wearers followed for 1 yearand found no difference in myopia progression between thetwo groups. These studies were done in Caucasian popu-lations, where the prevalence and rate of myopia progres-sion was lower than in ethnic Chinese populations.
A more recent controlled, but not randomized, studyundertaken among school children in Singapore foundthat there was a slower rate of progression among contactlens wearers compared with spectacle wearers.24 This studyalso concluded that the difference in progression could notbe explained by changes in corneal curvature. However,the study enrolled 105 children in the contact lens group,was not randomized, and the dropout rate was 47% amongcontact lens wearers over a 3-year period. There were alsodifferences in the baseline severity of myopia between thespectacle and contact lens groups. For this reason, wedecided to undertake a larger, randomized trial of the valueof rigid gas permeable lenses in reducing progression ofmyopia in Singaporean school-age children. A prospective,randomized trial with a similar aim but slightly differentdesign is currently underway in the United States.25 TheContact Lens and Myopia Study (CLAMP) randomizespre-adolescent children to rigid gas permeable or softcontact lenses after an adaptation period and follows themfor 3 years. However, the results of this trial are not yetavailable.
DESIGN
THE STUDY WAS A CLINICAL TRIAL, WHERE CHILDREN
were randomized to use either rigid gas permeable contactlenses or spectacle correction for treatment of myopia.Patients were randomized prior to adaptation to contactlens wear.
METHODS
● SETTING: Children were enrolled and all examinationswere conducted at the Myopia Clinic of the Singapore EyeResearch Institute.
● POPULATION: The population for this study was se-lected because of the high rates of myopia progressionobserved in Singaporean children.3,9 Participants wererecruited through the Refraction Clinics of the SchoolHealth Services and through newspaper advertisements,and any child who met the eligibility criteria couldparticipate in the trial. Eligible children were those ofChinese ethnicity, between the ages of 6 and 12, withmyopia between �1.0 and �4.0 diopters of sphere, astig-matism of �2 diopters, no prior history of contact lenswear, who did not have any other ocular or medicalpathologies, and who provided informed consent.26–29
Eligible patients were randomized to one of the twotreatment arms using a randomization schedule of blocksize 6, generated from random number tables in Baltimoreand placed in sealed envelopes with sequential patientnumbers. Randomization allocation was checked severaltimes during the study against the master list and patientidentifiers. Neither patients nor clinical observers weremasked to treatment group.
The projected sample size for randomization was 150 ineach group and was based on a mean change in refractiveerror of 0.7 diopters per year in the spectacle group, 80%power to detect a 0.2-diopter lower rate of progression peryear in the contact lens group, a type I error of 5%, and adropout rate of approximately 30% in the contact lensgroup over 2 years of follow-up. Because it was likely thatthere would be more dropouts among contact lens thanamong spectacle wearers during the adaptation period, ahigher number of patients were recruited to ensure at least150 children in the contact lens group following adapta-tion and 100 remaining in the trial at 24 months.
The study conformed to the Helsinki guidelines. Thetrial was approved by the Ethics Committee of the Singa-pore National Eye Center, and by Bausch and Lomb,which sponsored the trial and provided the contact lenses.After explaining the study to parents and children, writteninformed consent was obtained from parents and verbalassent from children.
● INTERVENTION: Children were randomized to receiverigid gas permeable contact lenses (Asian Design Lens,Bausch and Lomb, Rochester, New York, USA) or spec-tacles to correct their refractive error. The contact lensconsisted of a front and back junctionless aspheric designwith an overall diameter of 9.2 mm. Base curves availablefor the lenses ranged from 7.3 mm to 8.4 mm in 0.1-mmsteps. The lenses were fit to achieve central alignment withlight mid peripheral bearing. Apical bearing seen withfluoroscein evaluation was not allowed. The lens was fit tomove smoothly 1 to 2 mm after each blink and centeredover the cornea with full pupil capture. An automatedover-refraction was performed with trial lenses, a fullcycloplegic refraction prescription minus 0.5 diopters wasprovided, and the visual acuity was verified with the triallenses. Children assigned to spectacle correction were
CONTACT LENSES AND MYOPIAVOL. 136, NO. 1 83

refracted (cyclopleged) by the study personnel and re-ceived new spectacles if their current prescription did notconform to the refractive error measured in the study.
● MAIN OUTCOME MEASURES: The principal outcomewas the change in refractive error measured by subjectivecycloplegic refraction from postadaptation through 2 yearsof follow-up. Secondary outcomes were the change inkeratometry (autokeratometry) and total axial length (A-Scan ultrasonography) over the same time period.
Refractive error was obtained using both automatedrefraction (Nidek ARK 900, Nidek Co., Tokyo, Japan) andsubjective refraction (using autorefraction as the startingpoint for refining the refraction) 30 minutes after the thirddrop of 1% cyclogyl ophthalmic solution was instilled.Total axial length was measured by placing the probe inthe center of the patient’s cornea without applanation.Additional readings were taken until the SD was 0.12 mmor below.
Children were dispensed contact lenses or spectaclesbased on the refraction obtained during the preadaptationexamination. A 3-month period was provided to allowchildren to adapt to wearing the contact lenses or specta-cles before the start of the trial. Children returned for anexamination every 3 months to undergo a slit-lamp exam-ination for detection of any adverse events, and thecontact lens fit was evaluated at these visits. Children wereasked to wear their contact lenses for 4 hours prior to theocular examination. Cycloplegic refractions were obtainedat 6-month intervals following the end of the adaptationperiod. Cycloplegic autorefraction and keratometry wereperformed within 2 hours of lens removal. Children couldalso come to the clinic at any time if they believed therewere any adverse events or concerns. Spectacles andcontact lenses were replaced annually for all participants.If the visual acuity at any of the three monthly visits fellbelow 20/40, then the study team replaced the contactlenses or spectacles. The total follow-up period was 24months or five 6-month visits in which cycloplegic refrac-tive errors were measured.
Two measures of adherence were taken at each fol-low-up visit, one from children and one from parents. Eachwas asked how many hours per day the contact lenses orspectacles were worn and the number of days per week.The agreement between children and parents was almost100%, so the parent data for compliance measures wereselected for analysis. Adherence was defined as use ofcontact lenses (if assigned to this group) or spectacle use (ifassigned to spectacle wear) for at least 8 hours per day, 7days per week as reported at each scheduled visit.
Statistical analysis included comparability of baselinecharacteristics in the two treatment groups, a comparisonof those who completed the study and those who droppedout for various reasons, and a comparison of the mainoutcomes by treatment group. The mean changes inspherical equivalent refraction, keratometry, and total
axial length were compared using t tests, and the propor-tion of eyes with changes in these variables above certaincutoff points was compared between treatment groupsusing chi-square tests. The analysis was done for right andleft eyes separately with comparable results. The analysispresented here only uses data from right eyes. A multivar-iate linear model was used to estimate the difference in thechange in refractive errors from baseline through 24months between the two treatment groups, adjusted forcharacteristics that were different at baseline.
RESULTS
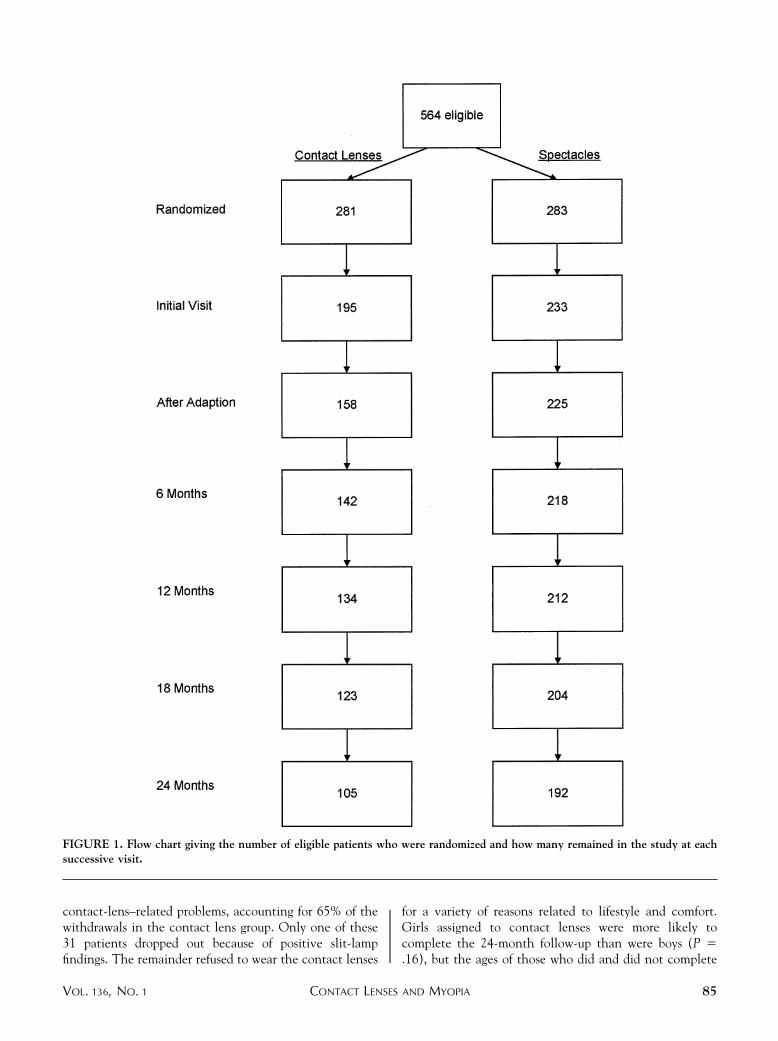
AS SHOWN IN FIGURE 1, A TOTAL OF 564 ELIGIBLE PATIENTS
were randomized to contact lenses (281) or spectacles(283). Because of initial problems with the supply ofcontact lenses for the trial, a lag time existed betweenrandomization and the initial preadaptation visit. Hence,195 patients completed the initial visit in the contact lensgroup and 233 in the spectacle group (Figure 1). Of theseparticipants, 158 in the contact lens group and 225 in thespectacle group completed the adaptation phase. Theproportion of patients remaining in the trial declined witheach successive visit. After 24 months, 105 patientsremained in the contact lens group and 192 in thespectacle group.
At the initial preadaptation visit, the age distribution,mean age (8.3 years), axial length (24.3 mm), astigmatism(�0.4 diopters), and prior spectacle wear (85%) werecomparable, but mean keratometry was 44.1 mm and 43.6mm in the contact and spectacle groups, respectively (P �.001). Mean subjective spherical equivalent was �2.56and �2.39 diopters in the contact lens and spectaclegroups (P � .02). The proportion of girls in the contactlens group was higher than in the spectacle group (56% vs41%, P � .002). At the end of the adaptation phase (thebaseline for change in refractive error over the subsequent24 months), the mean age and age distribution, history ofprior spectacle wear, axial length, and astigmatism werecomparable in the two groups and similar to the initial visitvalues (Table 1). The keratometric readings remainedslightly higher in the contact lens than in the spectaclegroup (P � .01), and the children assigned to contactlenses remained more myopic by 0.2 diopters than didthose in the spectacle group (P � .02). The genderimbalance remained the same, with 55% and 41% girls inthe contact lens and spectacle groups, respectively (P �.006).
Among the 158 assigned to contact lenses at the start ofthe postadaptation phase, 53 patients did not complete the24-month examination. Forty-eight patients withdrewfrom the study and 5 remained in the study but did notcomplete the 24-month examination and were considered“censored” from the study. Of the 48 patients who with-drew, 31 dropped out prior to 24 months owing to
AMERICAN JOURNAL OF OPHTHALMOLOGY84 JULY 2003
contact-lens–related problems, accounting for 65% of thewithdrawals in the contact lens group. Only one of these31 patients dropped out because of positive slit-lampfindings. The remainder refused to wear the contact lenses
for a variety of reasons related to lifestyle and comfort.Girls assigned to contact lenses were more likely tocomplete the 24-month follow-up than were boys (P �.16), but the ages of those who did and did not complete
FIGURE 1. Flow chart giving the number of eligible patients who were randomized and how many remained in the study at eachsuccessive visit.
CONTACT LENSES AND MYOPIAVOL. 136, NO. 1 85
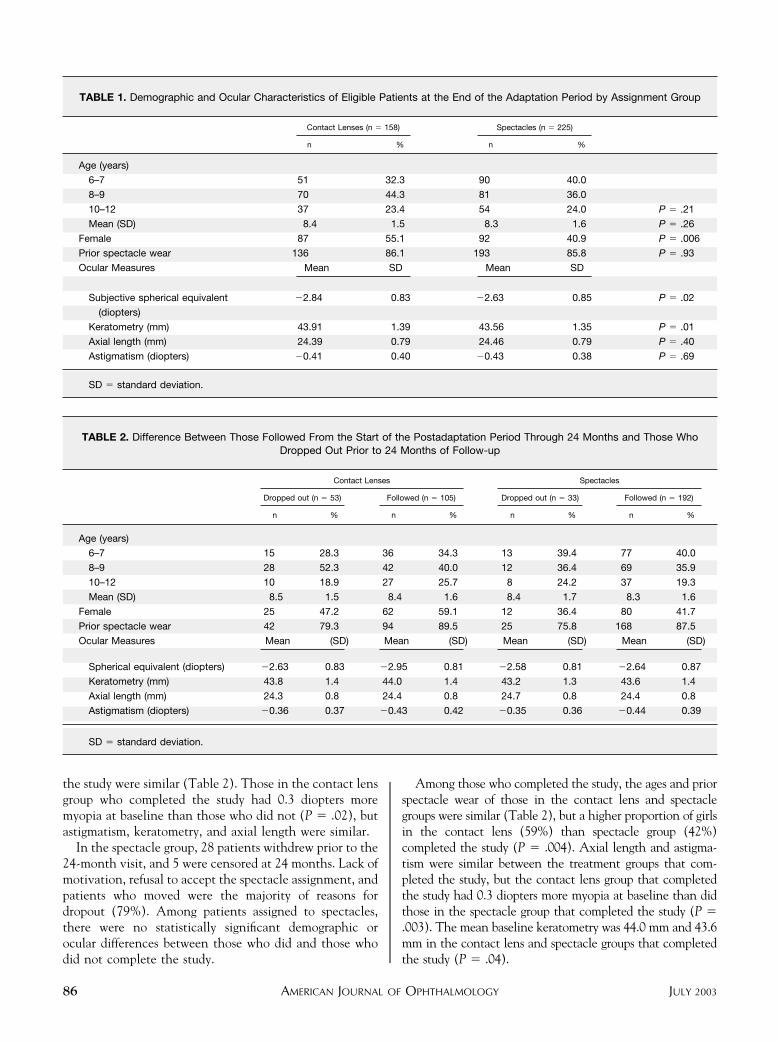
the study were similar (Table 2). Those in the contact lensgroup who completed the study had 0.3 diopters moremyopia at baseline than those who did not (P � .02), butastigmatism, keratometry, and axial length were similar.
In the spectacle group, 28 patients withdrew prior to the24-month visit, and 5 were censored at 24 months. Lack ofmotivation, refusal to accept the spectacle assignment, andpatients who moved were the majority of reasons fordropout (79%). Among patients assigned to spectacles,there were no statistically significant demographic orocular differences between those who did and those whodid not complete the study.
Among those who completed the study, the ages and priorspectacle wear of those in the contact lens and spectaclegroups were similar (Table 2), but a higher proportion of girlsin the contact lens (59%) than spectacle group (42%)completed the study (P � .004). Axial length and astigma-tism were similar between the treatment groups that com-pleted the study, but the contact lens group that completedthe study had 0.3 diopters more myopia at baseline than didthose in the spectacle group that completed the study (P �.003). The mean baseline keratometry was 44.0 mm and 43.6mm in the contact lens and spectacle groups that completedthe study (P � .04).
TABLE 1. Demographic and Ocular Characteristics of Eligible Patients at the End of the Adaptation Period by Assignment Group
Contact Lenses (n � 158) Spectacles (n � 225)
n % n %
Age (years)
6–7 51 32.3 90 40.0
8–9 70 44.3 81 36.0
10–12 37 23.4 54 24.0 P � .21
Mean (SD) 8.4 1.5 8.3 1.6 P � .26
Female 87 55.1 92 40.9 P � .006
Prior spectacle wear 136 86.1 193 85.8 P � .93
Ocular Measures Mean SD Mean SD
Subjective spherical equivalent
(diopters)
�2.84 0.83 �2.63 0.85 P � .02
Keratometry (mm) 43.91 1.39 43.56 1.35 P � .01
Axial length (mm) 24.39 0.79 24.46 0.79 P � .40
Astigmatism (diopters) �0.41 0.40 �0.43 0.38 P � .69
SD � standard deviation.
TABLE 2. Difference Between Those Followed From the Start of the Postadaptation Period Through 24 Months and Those WhoDropped Out Prior to 24 Months of Follow-up
Contact Lenses Spectacles
Dropped out (n � 53) Followed (n � 105) Dropped out (n � 33) Followed (n � 192)
n % n % n % n %
Age (years)
6–7 15 28.3 36 34.3 13 39.4 77 40.0
8–9 28 52.3 42 40.0 12 36.4 69 35.9
10–12 10 18.9 27 25.7 8 24.2 37 19.3
Mean (SD) 8.5 1.5 8.4 1.6 8.4 1.7 8.3 1.6
Female 25 47.2 62 59.1 12 36.4 80 41.7
Prior spectacle wear 42 79.3 94 89.5 25 75.8 168 87.5
Ocular Measures Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Spherical equivalent (diopters) �2.63 0.83 �2.95 0.81 �2.58 0.81 �2.64 0.87
Keratometry (mm) 43.8 1.4 44.0 1.4 43.2 1.3 43.6 1.4
Axial length (mm) 24.3 0.8 24.4 0.8 24.7 0.8 24.4 0.8
Astigmatism (diopters) �0.36 0.37 �0.43 0.42 �0.35 0.36 �0.44 0.39
SD � standard deviation.
AMERICAN JOURNAL OF OPHTHALMOLOGY86 JULY 2003

The median hours per day that contact lenses were wornif they were being used daily varied from 5.7 hours at the18-month visit to 7.1 hours at the 6- and 12-month visits.In contrast, spectacles were worn for a median of 12 hoursper day at the 6-month visit and 15 hours per day by the24-month visit. Using the definition of “adherence” aswearing either contact lenses or spectacles for at least 8hours per day, 7 days per week, 39.8% and 91.1% ofchildren were adherent at the 6-month visit in the contactlens and spectacle groups, respectively. The adherencewith contact lens wear declined over time, reaching 31.5%at the 24-month visit, while adherence with spectaclesincreased to 98.4%.
The increase in spherical equivalent for subjectiverefraction was approximately �0.6 diopters per year forsubjective cycloplegic refraction (Table 3). No differenceexisted between the two treatment groups with respect tothe change in refraction from the start of the trial through1 and 2 years of follow-up. Similarly, no difference wasseen in the distribution of change in refractive error over24 months (P � .35). Twenty-four percent of eyes in thecontact lens group had an increase of 2 or more diopters,whereas 16% of eyes in the spectacle group increased bythat amount or more over 2 years (P � .11). A similarincrease occurred in total axial length in both the specta-cle and contact lens groups over the course of the study, aswould be expected with a similar increase in severity ofmyopia over the same time period (Table 3). A flatteningof the cornea occurred, as measured by keratometry, in thecontact-lens–wearing group, but the difference betweenthe spectacle and contact lens groups was statisticallysignificant only at 12 months of follow-up.
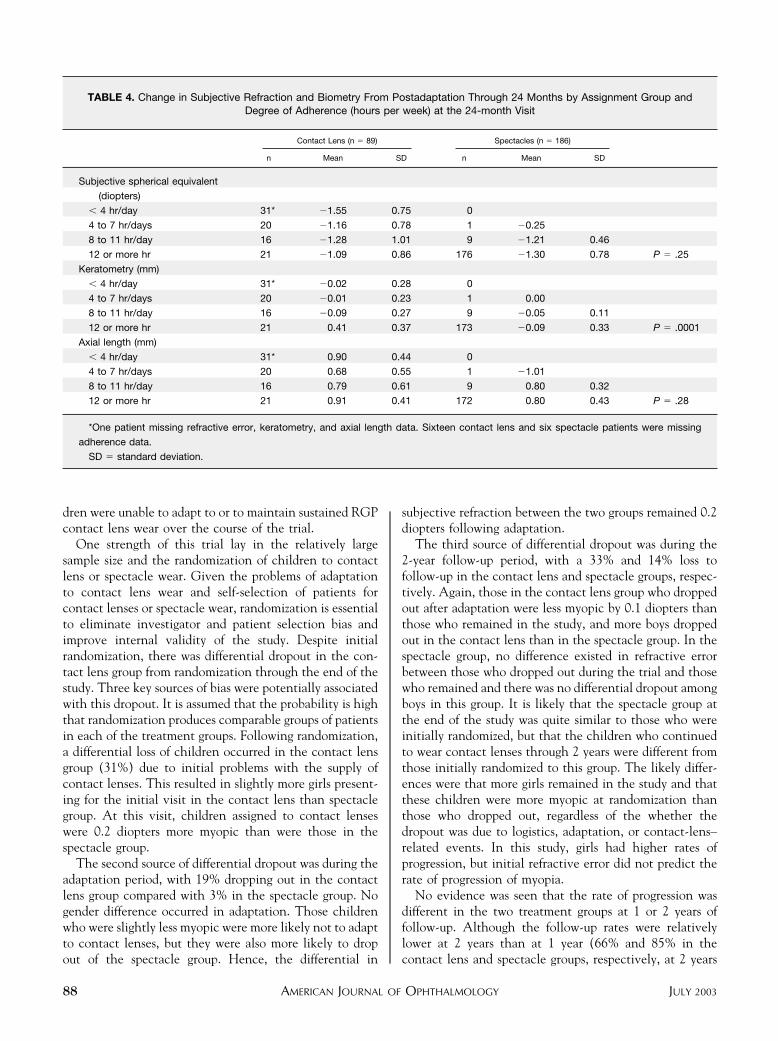
Among children who wore their contact lenses for 12 ormore hours per day at the 24-month visit, no differenceexisted in the change in refractive error, compared with allchildren in the spectacle group or among children whowore their spectacles for a similar amount of time per day
as the contact lens wearers (Table 4). No evidence wasseen of decreasing myopia progression with increasingcontact lens wear. Among children who wore contactlenses for 12 or more hours per day, there was a differencein the keratometry between the contact lens and spectaclegroups, but no difference in total axial length.
A multivariate model to predict the change in sphericalequivalent from baseline through 24 months was fit withtreatment group, age, gender, subjective refractive error,and keratometry at baseline as explanatory variables.These variables were selected because they were differentat baseline between those in the spectacle and contact lensgroups (subjective spherical equivalent and keratometry),or because they were predictive of myopia progression over2 years of follow-up in bivariate models (progression ofmyopia decreased with increasing age and more progres-sion among girls than boys). The adjusted difference in thechange in refractive error from baseline through 24 monthsbetween the two groups (�0.033 diopters, 95% confidenceinterval [CI] from �0.204, 0.138) was slightly less than theunadjusted difference of �0.047 diopters. None of thesedifferences was statistically significantly different fromzero. Predictors that remained statistically significant inthe multivariate model were age and gender.
DISCUSSION
BASED ON THIS RANDOMIZED 2-YEAR TRIAL, NO EVIDENCE
was found that rigid gas permeable (RGP) lenses reducedthe progression of myopia in preadolescent school childrenin Singapore. Among the children with 12 or more hoursper day of contact lens wear, there was a slight, but notstatistically significant difference of 0.2 diopters betweenthe rate of progression in the contact lenses compared tothe spectacle group, but a substantial proportion of chil-
TABLE 3. Changes in Refraction and Biometry at 1 and 2 Years of Follow-up by Assignment Group (Change Equals Follow-upMinus Immediate Postadaptation Measurements)
Contact Lenses Spectacles
n Mean SD n Mean SD
Change in subjective spherical
equivalent (diopters)
0 to 12 months 120 �0.65 0.55 186 �0.63 0.49 P � .74
0 to 24 months 97 �1.33 0.84 188 �1.28 0.78 P � .64
Change in keratometry (mm)
0 to 12 months 120 �0.08 0.33 183 �0.002 0.20 P � .006
0 to 24 months 97 �0.13 0.33 185 �0.07 0.33 P � .20
Change in axial length (mm)
0 to 12 months 118 0.35 0.41 183 0.33 0.40 P � .65
0 to 24 months 97 0.84 0.47 184 0.79 0.45 P � .38
SD � standard deviation.
CONTACT LENSES AND MYOPIAVOL. 136, NO. 1 87
dren were unable to adapt to or to maintain sustained RGPcontact lens wear over the course of the trial.
One strength of this trial lay in the relatively largesample size and the randomization of children to contactlens or spectacle wear. Given the problems of adaptationto contact lens wear and self-selection of patients forcontact lenses or spectacle wear, randomization is essentialto eliminate investigator and patient selection bias andimprove internal validity of the study. Despite initialrandomization, there was differential dropout in the con-tact lens group from randomization through the end of thestudy. Three key sources of bias were potentially associatedwith this dropout. It is assumed that the probability is highthat randomization produces comparable groups of patientsin each of the treatment groups. Following randomization,a differential loss of children occurred in the contact lensgroup (31%) due to initial problems with the supply ofcontact lenses. This resulted in slightly more girls present-ing for the initial visit in the contact lens than spectaclegroup. At this visit, children assigned to contact lenseswere 0.2 diopters more myopic than were those in thespectacle group.
The second source of differential dropout was during theadaptation period, with 19% dropping out in the contactlens group compared with 3% in the spectacle group. Nogender difference occurred in adaptation. Those childrenwho were slightly less myopic were more likely not to adaptto contact lenses, but they were also more likely to dropout of the spectacle group. Hence, the differential in
subjective refraction between the two groups remained 0.2diopters following adaptation.
The third source of differential dropout was during the2-year follow-up period, with a 33% and 14% loss tofollow-up in the contact lens and spectacle groups, respec-tively. Again, those in the contact lens group who droppedout after adaptation were less myopic by 0.1 diopters thanthose who remained in the study, and more boys droppedout in the contact lens than in the spectacle group. In thespectacle group, no difference existed in refractive errorbetween those who dropped out during the trial and thosewho remained and there was no differential dropout amongboys in this group. It is likely that the spectacle group atthe end of the study was quite similar to those who wereinitially randomized, but that the children who continuedto wear contact lenses through 2 years were different fromthose initially randomized to this group. The likely differ-ences were that more girls remained in the study and thatthese children were more myopic at randomization thanthose who dropped out, regardless of the whether thedropout was due to logistics, adaptation, or contact-lens–related events. In this study, girls had higher rates ofprogression, but initial refractive error did not predict therate of progression of myopia.
No evidence was seen that the rate of progression wasdifferent in the two treatment groups at 1 or 2 years offollow-up. Although the follow-up rates were relativelylower at 2 years than at 1 year (66% and 85% in thecontact lens and spectacle groups, respectively, at 2 years
TABLE 4. Change in Subjective Refraction and Biometry From Postadaptation Through 24 Months by Assignment Group andDegree of Adherence (hours per week) at the 24-month Visit
Contact Lens (n � 89) Spectacles (n � 186)
n Mean SD n Mean SD
Subjective spherical equivalent
(diopters)
� 4 hr/day 31* �1.55 0.75 0
4 to 7 hr/days 20 �1.16 0.78 1 �0.25
8 to 11 hr/day 16 �1.28 1.01 9 �1.21 0.46
12 or more hr 21 �1.09 0.86 176 �1.30 0.78 P � .25
Keratometry (mm)
� 4 hr/day 31* �0.02 0.28 0
4 to 7 hr/days 20 �0.01 0.23 1 0.00
8 to 11 hr/day 16 �0.09 0.27 9 �0.05 0.11
12 or more hr 21 0.41 0.37 173 �0.09 0.33 P � .0001
Axial length (mm)
� 4 hr/day 31* 0.90 0.44 0
4 to 7 hr/days 20 0.68 0.55 1 �1.01
8 to 11 hr/day 16 0.79 0.61 9 0.80 0.32
12 or more hr 21 0.91 0.41 172 0.80 0.43 P � .28
*One patient missing refractive error, keratometry, and axial length data. Sixteen contact lens and six spectacle patients were missing
adherence data.
SD � standard deviation.
AMERICAN JOURNAL OF OPHTHALMOLOGY88 JULY 2003

vs 85% and 94% at 1 year), the rate of progression was�0.65 diopters and �0.63 diopters in the contact lens andspectacle groups at 1 year. Hence, even with a relativelyhigh follow-up rate and less differential loss at 1 year offollow-up, there was no evidence of an impact of contactlens wear on myopia progression. This consistency fromthe first to the second year of follow-up adds strength tothe evidence supporting the no-treatment effect. Therewas also no pattern of decreasing progression with increas-ing daily hours of contact lens wear during the study,further evidence of a lack of a dose response to treatment.Finally, despite the slight difference in initial refractiveerror and gender distribution associated with differentialdropout, after adjusting for all factors that were differentbetween the two treatment groups at baseline, or thatmight predict myopia progression, there was still no differ-ence in progression between the contact lens and spectaclewearers.
In this study, children were randomized prior to adap-tation to contact lens wear. A design where all eligiblechildren were provided contact lenses and only those whocould adapt to lens wear would be eligible for randomiza-tion would not have been practical or logistically feasible.Such children would not have agreed to be randomized tospectacles following successful adaptation to contactlenses. In this sense, the current design allowed for an“effectiveness” analysis in which children who could adaptto contact lenses were compared with children who couldwear spectacles, resulting in less internal, but greaterexternal, validity. The CLAMP study now underway in theUnited States, has resolved this problem by randomizingafter adaptation, but the “control” group subjects areassigned to soft contact lenses, thus removing the problemof refusal to enter the control group after successfuladaptation to contact lenses.25 Investigators found that78.4% were able to adapt to RGP contact lens wearfollowing adaptation, comparable to the 81% in ourpopulation. Dropout rates from that study25 have not yetbeen reported, so they cannot be compared to our findings.Because of the control group, the CLAMP trial will answera slightly different question; that of whether RGP lensesrather than soft contact lenses can reduce the rate ofmyopia progression.
Despite the adaptation period in our trial, a higherdropout rate occurred in the contact lens than the spec-tacle group during the 2 years following the adaptationperiod, with the excess dropout being associated withcontact lens wear problems. Among those contact lenswearers who remained in the trial, at least 35% wore thecontact lenses for fewer than 4 hours per day. Hence,contact lens wear for this age group of school children wasnot easy to maintain over long periods of time, except in arelatively small group of patients.
In summary, the rate of myopia progression was about0.65 diopters per year among this group of Singaporeanchildren. The use of RGP lenses did not slow the rate of
myopia progression, and there was only a slightly lowerprogression rate among children who tolerated the contactlenses well and used them regularly and consistently.Adaptation to contact lenses and continued contact lenswear in this age group of children was relatively high. It isunlikely that this intervention holds promise as a methodby which to slow the rate of progression of myopia in suchchildren.
REFERENCES
1. Lin LL, Chen CJ, Hung PT, et al. Nation-wide survey ofmyopia among school children in Taiwan, 1986. ActaOphthalmol Suppl 1988;185:29–33.
2. Lin LL, Shih YF, Tsai CB, et al. Epidemiologic study ofocular refraction among schoolchildren in Taiwan in 1995.Optom Vis Sci 1999;76:275–281.
3. Zhan MZ, Saw SM, Hong RZ, et al. Refractive errors inSingapore and Ziamen, China—a comparative study inschool children aged 6 to 7 years. Optom Vis Sci 2000;77:302–308.
4. Au Eong KG, Tay TH, Lim MK. Race, culture and myopia in110,236 young Singaporean males. Singapore Med J 1993;34:29–32.
5. Edwards MH. The development of myopia in Hong Kongchildren between the ages of 7 and 12 years: a five-yearlongitudinal study. Ophthalmic Physiol Opt 1999;19:286–294.
6. Wu MM, Edwards MH. The effect of having myopic parents:an analysis of myopia in three generations. Optom Vis Sci1999;76:387–392.
7. Chew SJ, Chia SC, Lee LK. The pattern of myopia in youngSingaporean men. Singapore Med J 1988;29:201–211.
8. Chow YC, Dhillon B, Chew PT, et al. Refractive errors inSingapore medical students. Singapore Med J 1990;31:472–473.
9. Rajan U, Tan FT, Chan TK, et al. Increasing prevalence ofmyopia in Singapore school children: In: Chew SJ, Wein-traub J, editors. Proceedings of the Fifth International Con-ference on Myopia, Toronto, Canada, June 22–24, 1994.New York: Myopia International Research Foundation,1995, 41–46.
10. National Advisory Eye Council (US). Vision Research: anational plan, 1983–1987. US Department of Health andHuman Services, Public Health Service, National Institutesof Health, 1983 (NIH Publication No. 83-2469).
11. Mandelbaum S, de Luise VP, Driebe W, Groden LR, McLeodSD, Sher NA, Talamo JH, Katz J. Refractive Errors PreferredPractice Pattern. San Francisco: American Academy ofOphthalmology, 1997.
12. American Academy of Ophthalmology. Excimer lazer pho-torefractive keratectomy (PRK) for myopia and astigmatism.Ophthalmology 1999;106:422–437.
13. Celorio JM, Pruett RC. Prevalence of lattice degenerationand its relation to axial length in severe myopia. Am JOphthalmol 1991;111:20–23.
14. Sorensen KE, Baggesen K. Retinal detachment followingintracapsular cataract extraction. Acta Ophthalmol 1990;68:549–553.
15. Saw SM, Katz J, Schein OD, Chew SJ, Chan TK. Epidemi-ology of myopia. Epidemiol Rev 1996;18:175–187.
16. Jessen GN. Contact lenses as a therapeutic device. Am JOptom Arch Am Acad Optom 1964;41:429–435.
CONTACT LENSES AND MYOPIAVOL. 136, NO. 1 89

17. Morrison RJ. The use of contact lenses in adolescent myopicpatients. Am J Optom 1960;37:165–168.
18. Stone J. Contact lens wear in the young myope. Br J PhysiolOpt 1973;28:90–134.
19. Stone J. The possible influence of contact lenses on myopia.Br J Physiol Opt 1976;31:89–114.
20. Kelly T, Chatfield C, Tustin G. Clinical assessment of thearrest of myopia. Br J Ophthalmol 1975;59:529–538.
21. Grosvenor T, Perrigin J, Perrigin D, Quintero S. Use ofsilicone-acrylate contact lenses for the control of myopia.Results after two years of lens wear. Optom Vis Sci 1989;66:41–47.
22. Perrigin J, Perrigin D, Quintero S, Grosvenor T. Silicone-acrylate contact lenses for myopia control: 3-year results.Optom Vis Sci 1990;67:764–769.
23. Andreo LK. Long-term effects of hydrophilic contact lenseson myopia. Ann Ophthalmol 1990;22:224–229.
24. Khoo CY, Chong J, Rajan U. A 3-year study on the effect of
RGP contact lenses on myopic children. Singapore Med J1999;40:230–237.
25. The Contact Lens And Myopia Progression (CLAMP)study: design and baseline data. Optom Vis Sci 2001;78:223–233.
26. Saw SM, Nieto JF, Katz J, Chew SJ. Estimating the magni-tude of close-up work in school-age children: a comparison ofquestionnaire and diary instruments. Ophthalmic Epidemiol1999;6:291–301.
27. Saw SM, Nieto JF, Katz J, Chew SJ. Distance, lighting, andparental beliefs: understanding near work in epidemiologicstudies of myopia. Optom Vis Sci 1999;76:355–362.
28. Saw SM, Nieto JF, Katz J, Schein OD, Levy B, Chew SJ.Factors related to the progression of myopia in Singaporeanchildren. Optom Vis Sci 2000;77:549–554.
29. Saw SM, Nieto JF, Katz J, Schein OD, Levy B, Chew SK.Familial clustering and myopia progression in Singapore schoolchildren. Ophthalmic Epidemiol 2001;8:227–236.
AMERICAN JOURNAL OF OPHTHALMOLOGY90 JULY 2003