a girl with loose anagen hair syndrome and uncombable, spun-glass hair
TRANSCRIPT
Pediatric Dermatology
Vol. 22 No. 3 230–233, 2005
230
From the National Capital Consortium Dermatology ResidencyProgram, the Uniformed Services University department of dermatologyand the Johns Hopkins University department of dermatology.
Address correspondence to Leonard Sperling, M.D., Departmentof Dermatology, Uniformed Services University, 4301 Jones BridgeRoad, Bethesda, MD 20814, or email: [email protected].
Blackwell Publishing, Ltd.
A Girl with Loose Anagen Hair Syndrome and Uncombable, Spun-glass Hair
Abigail J. Lee, MC, USA,* Kimberly L. Maino, MC, USNR,† Bernard Cohen, M.D.,‡ and Leonard Sperling, MC, USA§
*
Uniformed Services University of the Health Sciences,
†
Department of Dermatology, National Naval Medical Center, Bethesda,
‡
Department of Dermatology, Johns Hopkins University, Baltimore, and
§
Department of Dermatology, Uniformed Services University, Bethesda, Maryland
Abstract:
A 4-year-old girl presented with a 2-year history of scalp hairthat had an odd texture, was difficult to manage, tended to “stick out” from thescalp, and was irregular in length. A hair pull test revealed that hairs couldbe easily and painlessly extracted. Light microscopic examination of thehair demonstrated anagen hairs with a ruffled cuticle and distorted bulb aswell as an unusual undulation and grooving of the shafts. These findings areconsistent with both loose anagen and uncombable hair syndromes. Theoccurrence of both syndromes in the same patient seems unlikely, and wepropose that our patient has loose anagen hair syndrome with features
resembling uncombable hair syndrome.
Loose anagen hair syndrome (LAHS) is characterizedby easily extractable anagen hairs that lose the inner andouter root sheaths during removal (1). Patients withuncombable hair syndrome (UHS) have unruly, “spun-glass” hair with a triangular cross-sectional shape andprominent longitudinal grooves (2). In 1996 Boyer et al(3) reported an instance of LAHS mimicking uncombablehair. We wish to report another patient with findingssuggestive of both syndromes.
CASE REPORT
The parents of a 4-year-old girl complained that thechild’s hair had a peculiar texture and was difficult tocomb. Although her hair had been cut only once in her
life, it was short and irregular in length. Her parentsnoted a gradual worsening of the condition over the past2 years. Otherwise, the girl was in good health and wastaking no medication. There was no family history ofhair disorders. The parents denied having similar hairproblems when they were children.
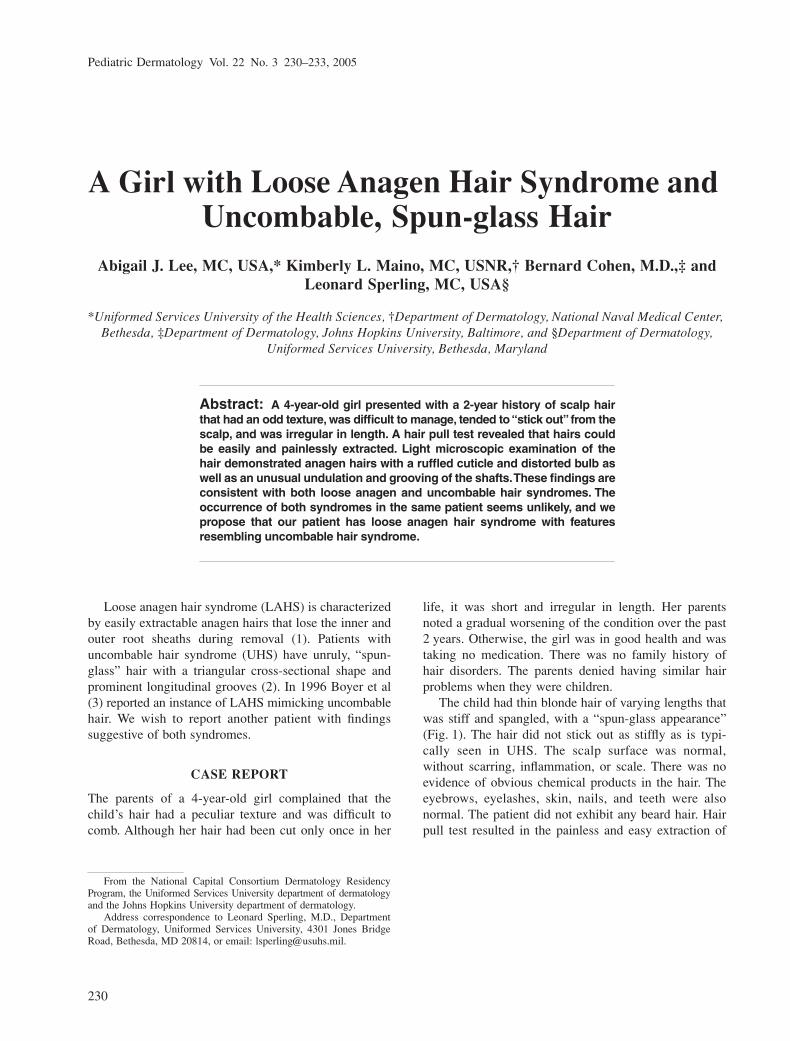
The child had thin blonde hair of varying lengths thatwas stiff and spangled, with a “spun-glass appearance”(Fig. 1). The hair did not stick out as stiffly as is typi-cally seen in UHS. The scalp surface was normal,without scarring, inflammation, or scale. There was noevidence of obvious chemical products in the hair. Theeyebrows, eyelashes, skin, nails, and teeth were alsonormal. The patient did not exhibit any beard hair. Hairpull test resulted in the painless and easy extraction of
Lee et al: Loose Anagen Hair Syndrome and Spun-glass Hair 231
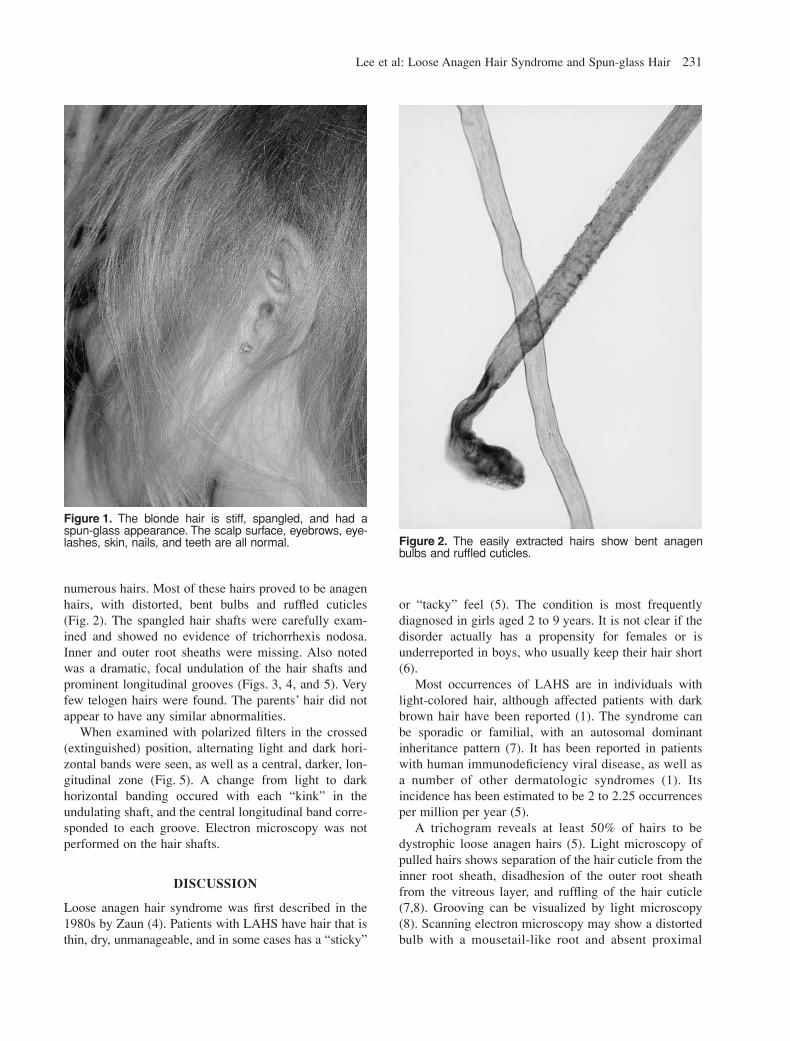
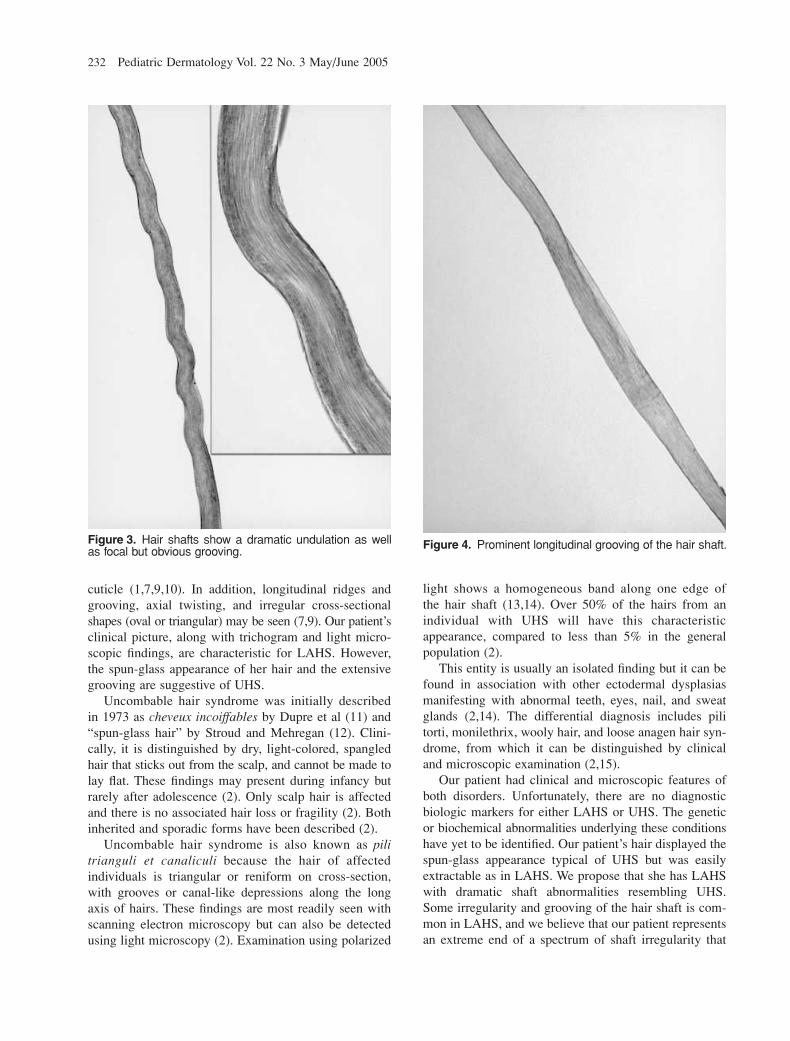
numerous hairs. Most of these hairs proved to be anagenhairs, with distorted, bent bulbs and ruffled cuticles(Fig. 2). The spangled hair shafts were carefully exam-ined and showed no evidence of trichorrhexis nodosa.Inner and outer root sheaths were missing. Also notedwas a dramatic, focal undulation of the hair shafts andprominent longitudinal grooves (Figs. 3, 4, and 5). Veryfew telogen hairs were found. The parents’ hair did notappear to have any similar abnormalities.
When examined with polarized filters in the crossed(extinguished) position, alternating light and dark hori-zontal bands were seen, as well as a central, darker, lon-gitudinal zone (Fig. 5). A change from light to darkhorizontal banding occured with each “kink” in theundulating shaft, and the central longitudinal band corre-sponded to each groove. Electron microscopy was notperformed on the hair shafts.
DISCUSSION
Loose anagen hair syndrome was first described in the1980s by Zaun (4). Patients with LAHS have hair that isthin, dry, unmanageable, and in some cases has a “sticky”
or “tacky” feel (5). The condition is most frequentlydiagnosed in girls aged 2 to 9 years. It is not clear if thedisorder actually has a propensity for females or isunderreported in boys, who usually keep their hair short(6).
Most occurrences of LAHS are in individuals withlight-colored hair, although affected patients with darkbrown hair have been reported (1). The syndrome canbe sporadic or familial, with an autosomal dominantinheritance pattern (7). It has been reported in patientswith human immunodeficiency viral disease, as well asa number of other dermatologic syndromes (1). Itsincidence has been estimated to be 2 to 2.25 occurrencesper million per year (5).
A trichogram reveals at least 50% of hairs to bedystrophic loose anagen hairs (5). Light microscopy ofpulled hairs shows separation of the hair cuticle from theinner root sheath, disadhesion of the outer root sheathfrom the vitreous layer, and ruffling of the hair cuticle(7,8). Grooving can be visualized by light microscopy(8). Scanning electron microscopy may show a distortedbulb with a mousetail-like root and absent proximal
Figure 1. The blonde hair is stiff, spangled, and had aspun-glass appearance. The scalp surface, eyebrows, eye-lashes, skin, nails, and teeth are all normal. Figure 2. The easily extracted hairs show bent anagen
bulbs and ruffled cuticles.
232
Pediatric Dermatology Vol. 22 No. 3 May/June 2005
cuticle (1,7,9,10). In addition, longitudinal ridges andgrooving, axial twisting, and irregular cross-sectionalshapes (oval or triangular) may be seen (7,9). Our patient’sclinical picture, along with trichogram and light micro-scopic findings, are characteristic for LAHS. However,the spun-glass appearance of her hair and the extensivegrooving are suggestive of UHS.
Uncombable hair syndrome was initially describedin 1973 as
cheveux incoiffables
by Dupre et al (11) and“spun-glass hair” by Stroud and Mehregan (12). Clini-cally, it is distinguished by dry, light-colored, spangledhair that sticks out from the scalp, and cannot be made tolay flat. These findings may present during infancy butrarely after adolescence (2). Only scalp hair is affectedand there is no associated hair loss or fragility (2). Bothinherited and sporadic forms have been described (2).
Uncombable hair syndrome is also known as
pilitrianguli et canaliculi
because the hair of affectedindividuals is triangular or reniform on cross-section,with grooves or canal-like depressions along the longaxis of hairs. These findings are most readily seen withscanning electron microscopy but can also be detectedusing light microscopy (2). Examination using polarized
light shows a homogeneous band along one edge ofthe hair shaft (13,14). Over 50% of the hairs from anindividual with UHS will have this characteristicappearance, compared to less than 5% in the generalpopulation (2).
This entity is usually an isolated finding but it can befound in association with other ectodermal dysplasiasmanifesting with abnormal teeth, eyes, nail, and sweatglands (2,14). The differential diagnosis includes pilitorti, monilethrix, wooly hair, and loose anagen hair syn-drome, from which it can be distinguished by clinicaland microscopic examination (2,15).
Our patient had clinical and microscopic features ofboth disorders. Unfortunately, there are no diagnosticbiologic markers for either LAHS or UHS. The geneticor biochemical abnormalities underlying these conditionshave yet to be identified. Our patient’s hair displayed thespun-glass appearance typical of UHS but was easilyextractable as in LAHS. We propose that she has LAHSwith dramatic shaft abnormalities resembling UHS.Some irregularity and grooving of the hair shaft is com-mon in LAHS, and we believe that our patient representsan extreme end of a spectrum of shaft irregularity that
Figure 3. Hair shafts show a dramatic undulation as wellas focal but obvious grooving. Figure 4. Prominent longitudinal grooving of the hair shaft.

Lee et al: Loose Anagen Hair Syndrome and Spun-glass Hair 233
can be found in LAHS. Easily extractable anagen hairshave not been described in UHS, and we feel that thisfinding is incompatible with a diagnosis of UHS. Theclosely set undulations seen in Fig. 5 are not the moregradual bending and twisting found in kinky-hairedindividuals. Our patient’s undulations are not typical ofmost patients with LAHS. However, they probably helpaccount for the unmanageable, spangled appearance ofthe hair.
Examination with polarized light showed light anddark horizontal banding alternating with each undula-tion, a finding that, to our knowledge, has not beendescribed in either LAHS or UHS. The bending is
closely set and more regular in trichothiodystrophy thanin patients with kinky hair. The pattern of banding in tri-chothiodystrophy is not the result of bending, but a con-tinuous change in the orientation of keratin filamentswithin the hair shaft (16).
REFERENCES
1. Li V, Baden H, Kvedar J. Loose anagen syndrome andloose anagen hair. Dermatol Clin 1996;14:747–751.
2. Hicks J. Uncombable hair (
chevaeux incoiffables, pilitrianguli et canaliculi
) syndrome: brief review and role ofscanning electron microscopy in diagnosis. UltrastrucPathol 2001;25:99–103.
3. Boyer J, Cobb M, Sperling L, et al. LAHS mimicking theuncombable hair syndrome. Cutis 1996;57:111–112.
4. Zaun H. Differential diagnosis of alopecia in children. In:Happle R, Grosshans E, eds. Pediatric dermatology: advancesin diagnosis and treatment. Berlin: Springer-Verlag, 1987:164–165.
5. Chapalain V, Winter H, Langbein L, et al. Is the looseanagen syndrome a keratin disorder? Arch Dermatol2002;138:501–506.
6. Tosti A. Loose anagen hair syndrome and loose anagenhair. Arch Dermatol 2002;138:521–522.
7. Baden H, Kvedar J, Magro C. Loose anagen hair as causeof hereditary hair loss in children. Arch Dermatol1992;128:1349–1353.
8. O’Donnell B, Sperling L, James W. Loose anagen hairsyndrome. Int J Dermatol 1992;31(2):107–109.
9. Price V, Gummer C. Loose anagen syndrome. J Am AcadDermatol 1989;20:249–256.
10. Tosti A, Peluso A, Misciali C, et al. Loose anagen hair.Arch Dermatol 1997;133:1089–1093.
11. Dupre A, Rochiccioli P, Bonafe JL. “Cheveux incoiffable”anomalie congenitale des cheveux. Bull Soc Franc DermatolSyphil 1973;80:111–112.
12. Stround JD, Mehregan AW. “Spun-glass” hair: a clinico-pathologic study of an unusual hair defect. In: Brown, AC,ed. First human hair symposium. New York: MedcomPress, 1973:103–107.
13. Dupre A, Bonafe JL. Etude en lumiere polarisee des dys-plasies pilaires. Essai d’actualisation de la nomenclature.Ann Dermatol Venereol 1978;105:921–930.
14. Shelley WB, Shelley ED. Uncombable hair syndrome:observations on response to biotin and occurrence insiblings with ectodermal dysplasia. J Am Acad Dermatol1985;13:97–102.
15. McCullum N, Sperling L, Vidmar D. The uncombable hairsyndrome. Cutis 1990;46:479–483.
16. Sperling LC, DiGiovanna JJ. “Curly” wood and tiger tails:An explanation for light and dark banding with polariza-tion in trichothiodystrophy. Arch Dermatol 2003;139:1189–92.
Figure 5. With routine light microscopy, the shaft has auniform color (top/center). When examined with polarizedfilters in the crossed (extinguished) position, alternatinglight and dark horizontal bands are seen (right side/lowpower). The light and dark horizontal bands correspond tothe “kinks” in the undulating shaft (left side/high power).