a dilated fetal stomach predicts a complicated postnatal course in cases of prenatally diagnosed...
TRANSCRIPT
American Journal of Obstetrics and Gynecology (2004) 190, 1326e30
www.elsevier.com/locate/ajog
A dilated fetal stomach predicts a complicated postnatalcourse in cases of prenatally diagnosed gastroschisis
Abimbola J. Aina-Mumuney, MD,a Anne C. Fischer, MD,b Karin J. Blakemore, MD,a
Jude P. Crino, MD,a Kathleen Costigan, MPH,a Kerry Swenson, MD,a
Christian A. Chisholm, MDa
Departments of Gynecology and Obstetricsa and Pediatric Surgery,b Johns Hopkins University School of Medicine,Baltimore, Md
Received for publication July 3, 2003; revised October 2, 2003; accepted November 4, 2003
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Objective: The purpose of this study was to determine whether dilation of the fetal stomach is
associated with increased perinatal complications in infants with prenatally diagnosed gastroschi-sis.Study design: From 34 newborn infants with gastroschisis who were delivered at our institution
over a 10-year period, 2 groups were analyzed on the basis of the presence or absence of a dilatedfetal stomach. Reactive versus nonreactive nonstress test results were recorded, when performed.Neonatal outcomes were compared.Results: Twenty-one fetuses had no evidence of gastric dilation. Thirteen fetuses had a dilated
fetal stomach that was identified by ultrasound scanning. Within this group there was a higherincidence of nonreactive nonstress tests (P=.01). Infants with a prenatally dilated stomachhad a higher incidence of volvulus and neonatal death, a significantly delayed time to full oral
feeds, and a longer hospitalization than those infants who did not have a prenatally dilated stom-ach (P%.05).Conclusion: Postnatal morbidity and mortality rates are increased in infants with gastroschisis
who have a prenatally dilated stomach. These fetuses, although not acidotic at delivery, alsohad a higher incidence of nonreactive nonstress test results.� 2004 Elsevier Inc. All rights reserved.
KEY WORDSGastroschisisDilated fetal stomach
VolvulusPostnatal morbidityNonstress test
–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
Gastroschisis is a rare congenital anomaly (in 0.6 to10 per 100,000 live births) that consists of a full-thick-ness abdominal wall defect that permits the protrusionof fetal bowel and other abdominal contents.1 Gastroin-testinal complications occur in approximately 40% ofbabies with gastroschisis.2 Some of these complications
Reprints not available from the authors.
0002-9378/$ - see front matter � 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.ajog.2003.11.003
occur early in fetal life (such as intestinal atresia); othercomplications develop in the perinatal period, with life-threatening consequences (such as volvulus and necro-tizing enterocolitis with potential short gut syndromeand fistulas).
Among the obstetric dilemmas in the treatment of thefetus with gastroschisis is the lack of reliable prognosticindicators of poor perinatal outcome that shouldprompt delivery. Although some investigators have
Aina-Mumuney et al 1327
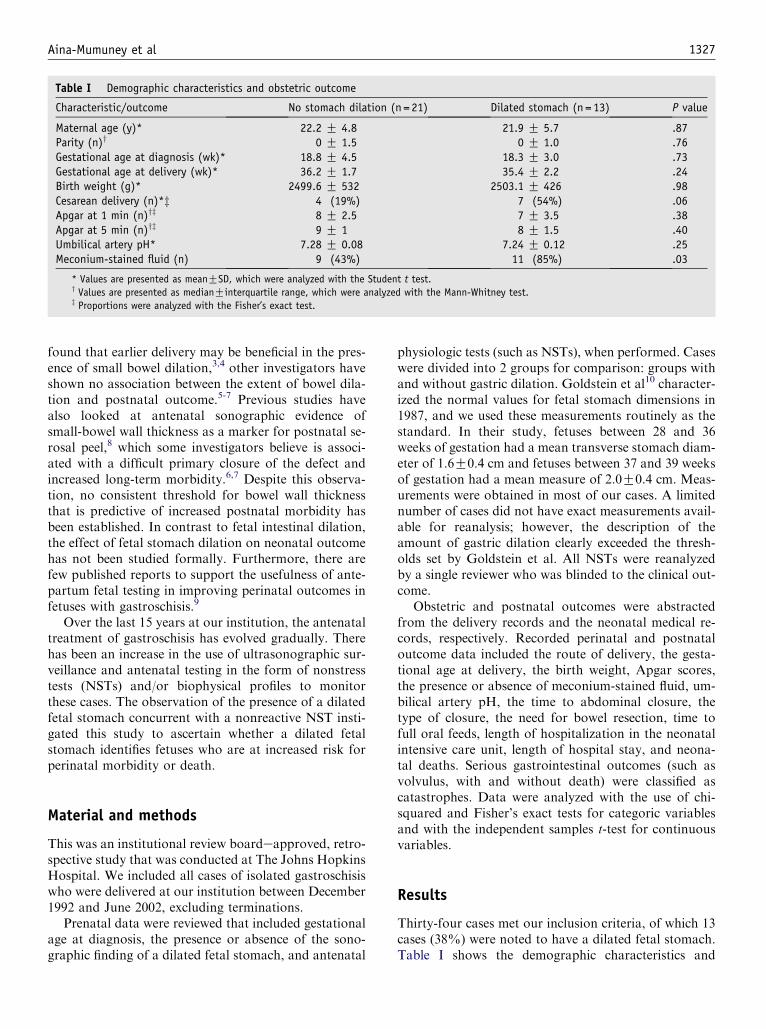
Table I Demographic characteristics and obstetric outcome
Characteristic/outcome No stomach dilation (n = 21) Dilated stomach (n = 13) P value
Maternal age (y)* 22.2 G 4.8 21.9 G 5.7 .87Parity (n)y 0 G 1.5 0 G 1.0 .76Gestational age at diagnosis (wk)* 18.8 G 4.5 18.3 G 3.0 .73Gestational age at delivery (wk)* 36.2 G 1.7 35.4 G 2.2 .24Birth weight (g)* 2499.6 G 532 2503.1 G 426 .98Cesarean delivery (n)*z 4 (19%) 7 (54%) .06Apgar at 1 min (n)yz 8 G 2.5 7 G 3.5 .38Apgar at 5 min (n)yz 9 G 1 8 G 1.5 .40Umbilical artery pH* 7.28 G 0.08 7.24 G 0.12 .25Meconium-stained fluid (n) 9 (43%) 11 (85%) .03
* Values are presented as meanGSD, which were analyzed with the Student t test.y Values are presented as medianGinterquartile range, which were analyzed with the Mann-Whitney test.z Proportions were analyzed with the Fisher’s exact test.
found that earlier delivery may be beneficial in the pres-ence of small bowel dilation,3,4 other investigators haveshown no association between the extent of bowel dila-tion and postnatal outcome.5-7 Previous studies havealso looked at antenatal sonographic evidence ofsmall-bowel wall thickness as a marker for postnatal se-rosal peel,8 which some investigators believe is associ-ated with a difficult primary closure of the defect andincreased long-term morbidity.6,7 Despite this observa-tion, no consistent threshold for bowel wall thicknessthat is predictive of increased postnatal morbidity hasbeen established. In contrast to fetal intestinal dilation,the effect of fetal stomach dilation on neonatal outcomehas not been studied formally. Furthermore, there arefew published reports to support the usefulness of ante-partum fetal testing in improving perinatal outcomes infetuses with gastroschisis.9
Over the last 15 years at our institution, the antenataltreatment of gastroschisis has evolved gradually. Therehas been an increase in the use of ultrasonographic sur-veillance and antenatal testing in the form of nonstresstests (NSTs) and/or biophysical profiles to monitorthese cases. The observation of the presence of a dilatedfetal stomach concurrent with a nonreactive NST insti-gated this study to ascertain whether a dilated fetalstomach identifies fetuses who are at increased risk forperinatal morbidity or death.
Material and methods
This was an institutional review boardeapproved, retro-spective study that was conducted at The Johns HopkinsHospital. We included all cases of isolated gastroschisiswho were delivered at our institution between December1992 and June 2002, excluding terminations.
Prenatal data were reviewed that included gestationalage at diagnosis, the presence or absence of the sono-graphic finding of a dilated fetal stomach, and antenatal
physiologic tests (such as NSTs), when performed. Caseswere divided into 2 groups for comparison: groups withand without gastric dilation. Goldstein et al10 character-ized the normal values for fetal stomach dimensions in1987, and we used these measurements routinely as thestandard. In their study, fetuses between 28 and 36weeks of gestation had a mean transverse stomach diam-eter of 1.6G0.4 cm and fetuses between 37 and 39 weeksof gestation had a mean measure of 2.0G0.4 cm. Meas-urements were obtained in most of our cases. A limitednumber of cases did not have exact measurements avail-able for reanalysis; however, the description of theamount of gastric dilation clearly exceeded the thresh-olds set by Goldstein et al. All NSTs were reanalyzedby a single reviewer who was blinded to the clinical out-come.
Obstetric and postnatal outcomes were abstractedfrom the delivery records and the neonatal medical re-cords, respectively. Recorded perinatal and postnataloutcome data included the route of delivery, the gesta-tional age at delivery, the birth weight, Apgar scores,the presence or absence of meconium-stained fluid, um-bilical artery pH, the time to abdominal closure, thetype of closure, the need for bowel resection, time tofull oral feeds, length of hospitalization in the neonatalintensive care unit, length of hospital stay, and neona-tal deaths. Serious gastrointestinal outcomes (such asvolvulus, with and without death) were classified ascatastrophes. Data were analyzed with the use of chi-squared and Fisher’s exact tests for categoric variablesand with the independent samples t-test for continuousvariables.
Results
Thirty-four cases met our inclusion criteria, of which 13cases (38%) were noted to have a dilated fetal stomach.Table I shows the demographic characteristics and
1328 Aina-Mumuney et al
obstetric outcomes of the 2 groups. The gestational ageat diagnosis of gastroschisis and at delivery was similarin both groups, as were birth weight, Apgar scores, andumbilical artery pH. The presence of meconium-stainedamniotic fluid was the only parameter with a statisticallysignificant difference between the 2 groups, which waspresent in 85% of the fetuses with a dilated stomach ver-sus 43% of the fetuses without gastric dilation.
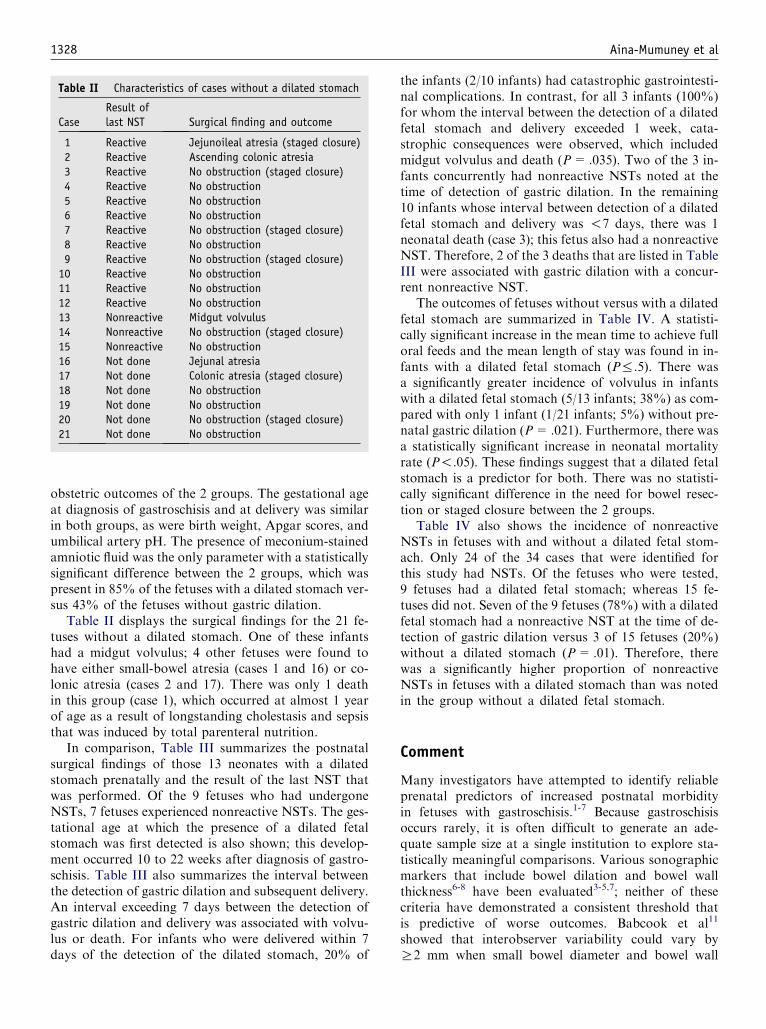
Table II displays the surgical findings for the 21 fe-tuses without a dilated stomach. One of these infantshad a midgut volvulus; 4 other fetuses were found tohave either small-bowel atresia (cases 1 and 16) or co-lonic atresia (cases 2 and 17). There was only 1 deathin this group (case 1), which occurred at almost 1 yearof age as a result of longstanding cholestasis and sepsisthat was induced by total parenteral nutrition.
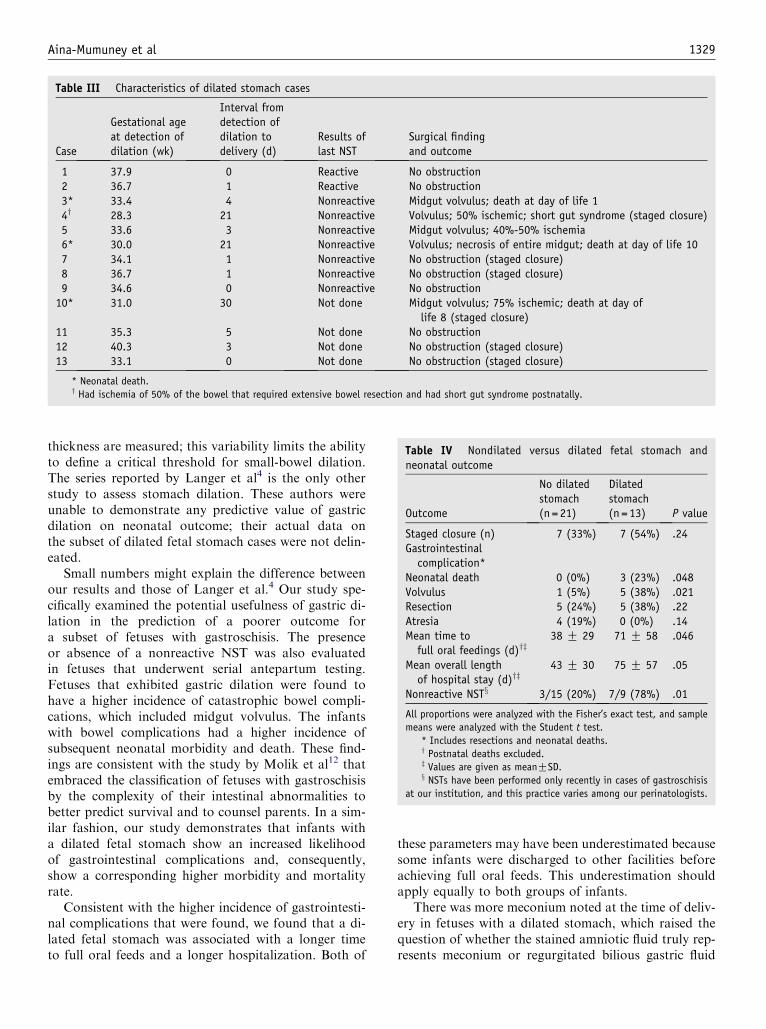
In comparison, Table III summarizes the postnatalsurgical findings of those 13 neonates with a dilatedstomach prenatally and the result of the last NST thatwas performed. Of the 9 fetuses who had undergoneNSTs, 7 fetuses experienced nonreactive NSTs. The ges-tational age at which the presence of a dilated fetalstomach was first detected is also shown; this develop-ment occurred 10 to 22 weeks after diagnosis of gastro-schisis. Table III also summarizes the interval betweenthe detection of gastric dilation and subsequent delivery.An interval exceeding 7 days between the detection ofgastric dilation and delivery was associated with volvu-lus or death. For infants who were delivered within 7days of the detection of the dilated stomach, 20% of
Table II Characteristics of cases without a dilated stomach
CaseResult oflast NST Surgical finding and outcome
1 Reactive Jejunoileal atresia (staged closure)2 Reactive Ascending colonic atresia3 Reactive No obstruction (staged closure)4 Reactive No obstruction5 Reactive No obstruction6 Reactive No obstruction7 Reactive No obstruction (staged closure)8 Reactive No obstruction9 Reactive No obstruction (staged closure)10 Reactive No obstruction11 Reactive No obstruction12 Reactive No obstruction13 Nonreactive Midgut volvulus14 Nonreactive No obstruction (staged closure)15 Nonreactive No obstruction16 Not done Jejunal atresia17 Not done Colonic atresia (staged closure)18 Not done No obstruction19 Not done No obstruction20 Not done No obstruction (staged closure)21 Not done No obstruction
the infants (2/10 infants) had catastrophic gastrointesti-nal complications. In contrast, for all 3 infants (100%)for whom the interval between the detection of a dilatedfetal stomach and delivery exceeded 1 week, cata-strophic consequences were observed, which includedmidgut volvulus and death (P=.035). Two of the 3 in-fants concurrently had nonreactive NSTs noted at thetime of detection of gastric dilation. In the remaining10 infants whose interval between detection of a dilatedfetal stomach and delivery was !7 days, there was 1neonatal death (case 3); this fetus also had a nonreactiveNST. Therefore, 2 of the 3 deaths that are listed in TableIII were associated with gastric dilation with a concur-rent nonreactive NST.
The outcomes of fetuses without versus with a dilatedfetal stomach are summarized in Table IV. A statisti-cally significant increase in the mean time to achieve fulloral feeds and the mean length of stay was found in in-fants with a dilated fetal stomach (P%.5). There wasa significantly greater incidence of volvulus in infantswith a dilated fetal stomach (5/13 infants; 38%) as com-pared with only 1 infant (1/21 infants; 5%) without pre-natal gastric dilation (P=.021). Furthermore, there wasa statistically significant increase in neonatal mortalityrate (P!.05). These findings suggest that a dilated fetalstomach is a predictor for both. There was no statisti-cally significant difference in the need for bowel resec-tion or staged closure between the 2 groups.
Table IV also shows the incidence of nonreactiveNSTs in fetuses with and without a dilated fetal stom-ach. Only 24 of the 34 cases that were identified forthis study had NSTs. Of the fetuses who were tested,9 fetuses had a dilated fetal stomach; whereas 15 fe-tuses did not. Seven of the 9 fetuses (78%) with a dilatedfetal stomach had a nonreactive NST at the time of de-tection of gastric dilation versus 3 of 15 fetuses (20%)without a dilated stomach (P=.01). Therefore, therewas a significantly higher proportion of nonreactiveNSTs in fetuses with a dilated stomach than was notedin the group without a dilated fetal stomach.
Comment
Many investigators have attempted to identify reliableprenatal predictors of increased postnatal morbidityin fetuses with gastroschisis.1-7 Because gastroschisisoccurs rarely, it is often difficult to generate an ade-quate sample size at a single institution to explore sta-tistically meaningful comparisons. Various sonographicmarkers that include bowel dilation and bowel wallthickness6-8 have been evaluated3-5,7; neither of thesecriteria have demonstrated a consistent threshold thatis predictive of worse outcomes. Babcook et al11
showed that interobserver variability could vary byR2 mm when small bowel diameter and bowel wall
Aina-Mumuney et al 1329
Table III Characteristics of dilated stomach cases
Case
Gestational ageat detection ofdilation (wk)
Interval fromdetection ofdilation todelivery (d)
Results oflast NST
Surgical findingand outcome
1 37.9 0 Reactive No obstruction2 36.7 1 Reactive No obstruction3* 33.4 4 Nonreactive Midgut volvulus; death at day of life 14y 28.3 21 Nonreactive Volvulus; 50% ischemic; short gut syndrome (staged closure)5 33.6 3 Nonreactive Midgut volvulus; 40%-50% ischemia6* 30.0 21 Nonreactive Volvulus; necrosis of entire midgut; death at day of life 107 34.1 1 Nonreactive No obstruction (staged closure)8 36.7 1 Nonreactive No obstruction (staged closure)9 34.6 0 Nonreactive No obstruction10* 31.0 30 Not done Midgut volvulus; 75% ischemic; death at day of
life 8 (staged closure)11 35.3 5 Not done No obstruction12 40.3 3 Not done No obstruction (staged closure)13 33.1 0 Not done No obstruction (staged closure)
* Neonatal death.y Had ischemia of 50% of the bowel that required extensive bowel resection and had short gut syndrome postnatally.
thickness are measured; this variability limits the abilityto define a critical threshold for small-bowel dilation.The series reported by Langer et al4 is the only otherstudy to assess stomach dilation. These authors wereunable to demonstrate any predictive value of gastricdilation on neonatal outcome; their actual data onthe subset of dilated fetal stomach cases were not delin-eated.
Small numbers might explain the difference betweenour results and those of Langer et al.4 Our study spe-cifically examined the potential usefulness of gastric di-lation in the prediction of a poorer outcome fora subset of fetuses with gastroschisis. The presenceor absence of a nonreactive NST was also evaluatedin fetuses that underwent serial antepartum testing.Fetuses that exhibited gastric dilation were found tohave a higher incidence of catastrophic bowel compli-cations, which included midgut volvulus. The infantswith bowel complications had a higher incidence ofsubsequent neonatal morbidity and death. These find-ings are consistent with the study by Molik et al12 thatembraced the classification of fetuses with gastroschisisby the complexity of their intestinal abnormalities tobetter predict survival and to counsel parents. In a sim-ilar fashion, our study demonstrates that infants witha dilated fetal stomach show an increased likelihoodof gastrointestinal complications and, consequently,show a corresponding higher morbidity and mortalityrate.
Consistent with the higher incidence of gastrointesti-nal complications that were found, we found that a di-lated fetal stomach was associated with a longer timeto full oral feeds and a longer hospitalization. Both of
these parameters may have been underestimated becausesome infants were discharged to other facilities beforeachieving full oral feeds. This underestimation shouldapply equally to both groups of infants.
There was more meconium noted at the time of deliv-ery in fetuses with a dilated stomach, which raised thequestion of whether the stained amniotic fluid truly rep-resents meconium or regurgitated bilious gastric fluid
Table IV Nondilated versus dilated fetal stomach andneonatal outcome
Outcome
No dilatedstomach(n = 21)
Dilatedstomach(n = 13) P value
Staged closure (n) 7 (33%) 7 (54%) .24Gastrointestinalcomplication*
Neonatal death 0 (0%) 3 (23%) .048Volvulus 1 (5%) 5 (38%) .021Resection 5 (24%) 5 (38%) .22Atresia 4 (19%) 0 (0%) .14Mean time tofull oral feedings (d)yz
38 G 29 71 G 58 .046
Mean overall lengthof hospital stay (d)yz
43 G 30 75 G 57 .05
Nonreactive NSTx 3/15 (20%) 7/9 (78%) .01
All proportions were analyzed with the Fisher’s exact test, and sample
means were analyzed with the Student t test.
* Includes resections and neonatal deaths.y Postnatal deaths excluded.z Values are given as meanGSD.x NSTs have been performed only recently in cases of gastroschisis
at our institution, and this practice varies among our perinatologists.

1330 Aina-Mumuney et al
from the dilated stomach. If an obstruction to intestinalcontinuity exists (such as in cases of atresia or acutelywith volvulus), then intestinal fluid is expected to accu-mulate, and an increase in bilious staining would beexpected.
Another point of interest is the association betweennonreactive NSTs and a dilated fetal stomach. Despitethe increase in nonreactive NSTs that was noted in fe-tuses with a dilated stomach, no significant differencewas observed in Apgar scores or umbilical artery pHat delivery in this group, excluding fetal acidosis asthe cause of the nonreactivity of the fetal heart ratepattern. As gastric dilation develops, one can postulatethat increased vagal tone from gastric distension pro-duces a decrease in long-term variability of the fetalheart rate. This, as opposed to fetal hypoxemia or ac-idosis, may account for the frequent number of nonre-active NSTs that are observed in those fetuses withgastric dilation. This group of fetuses did have a higherincidence of poorer outcomes, but these appear to berelated to gastrointestinal complications and not peri-natal asphyxia.
Our study is limited by a small sample size. Although34 fetuses represents a relatively large case series of pre-natally diagnosed gastroschisis, less than one half ofthem exhibited the finding of interest, a dilated fetalstomach. The overall survival rate in our study was91%, which is comparable to other studies2,12; however,it is worth noting that the survival rate of fetuses witha dilated fetal stomach was 77% versus 100% in fetuseswithout a dilated stomach (P=.048). Fetuses with thisfinding, when delivered promptly, had greater survival,fewer gastrointestinal catastrophes, and a shorter hospi-talization.
In conclusion, our study indicates that the ultrasono-graphic finding of a dilated fetal stomach can help iden-tify those fetuses who are most at risk for increasedpostnatal morbidity and death. The presence of a dilatedfetal stomach may warrant an increase in the frequency
of antenatal surveillance and may warrant expeditiousdelivery to optimize postnatal outcome.
References
1. Rinehart BK, Terrone DA, Isler CM, Larmon JE, Perry KG,
Roberts WE. Modern obstetric management and outcome of
infants with gastroschisis. Obstet Gynecol 1999;94:112-6.
2. Durfee SM, Downard CD, Benson CB, Wilson JM. Postnatal
outcome of fetuses with the prenatal diagnosis of gastroschisis.
J Ultrasound Med 2002;21:269-74.
3. Pryde PG, Bardicef M, Treadwell MC, Klein M, Isada NB, Evans
MI. Gastroschisis: Can antenatal ultrasound predict infant out-
comes? Obstet Gynecol 1994;84:505-10.
4. Langer JC, Khanna J, Caco C, Dykes EH, Nicolaides KH.
Prenatal diagnosis of gastroschisis: Development of objective
sonographic criteria for predicting outcome. Obstet Gynecol
1993;81:53-6.
5. Alsulyman OM, Monteiro H, Ouzounian JG, Barton L, Songster
GS, Kovacs BW. Clinical significance of prenatal ultrasonographic
intestinal dilatation in fetuses with gastroschisis. Am J Obstet
Gynecol 1996;175:982-4.
6. Lenke RR, Persute WH, Nemes J. Ultrasonographic assessment of
intestinal damage in fetuses with gastroschisis: Is it of clinical
value? Am J Obstet Gynecol 1990;163:995-8.
7. Sipes SL, Weiner CP, Williamson RA, Pringle KC, Kimura K.
Fetal gastroschisis complicated by bowel dilatation: An indication
for imminent delivery? Fetal Diagn Ther 1990;5:100-3.
8. Tibboel D, Vermey-Keers C, Kluck P, Gaillard JP, Koppenberg J,
Molenaar JC. The natural history of gastroschisis during fetal life:
development of the fibrous coating on the bowel loops. Teratology
1986;33:267-72.
9. Ingamells S, Saunders NJ, Burge D. Gastroschisis and reduced
fetal heart-rate variability. Lancet 1995;345:1024-5.
10. Goldstein I, Reece EA, Yarko S, Wan M, Green JLJ, Hobbins JC.
Growth of the fetal stomach in normal pregnancies. Obstet
Gynecol 1987;70:641-4.
11. Babcook CJ, Hedrick MH, Goldstein RB, Callen PW, Harrison
MR, Adzick NS, et al. Gastroschisis: Can sonography of the fetal
bowel accurately predict postnatal outcome? J Ultrasound Med
1994;13:701-6.
12. Molik KA, Gingalewski CA, West KW, Rescorla FJ, Scherer LR
III, Engum SA, et al. Gastroschisis: a plea for risk categorization.
J Pediatr Surg 2001;36:51-5.