a controlled study of visual symptoms and eye strain factors in chronic headache
TRANSCRIPT

A Controlled Study of Visual Symptoms and Eye Strain Factors in Chronic Headache
Arnaud J.P. Vincent, M.Sc., Egilius L.H. Spierings, M.D., Ph.D. and Harley B. Messinger, M.D., Ph.D.
The Headache Research Foundation and John R. Graham Headache Centre, The Faulkner Hospital; and Department ofNeurology, Tufts University School of Medicine, Boston, Massachusetts.
Reprint requests to: Dr. E..L.H. Spierings, Director, The Headache Research Foundation, The Faulkner Hospital, Allandale atCentre Street, Boston, MA 02130, U.S.A.
Accepted for Publication: March 31, 1989.
SYNOPSIS
In a questionnaire survey we determined the prevalence of visual symptoms and eye strain factors in a group of chronicheadache sufferers as compared with age- and sex-matched controls. The visual symptoms studied were those not specificfor headache, i.e., sensitivity to light and blurred vision. Sensitivity to light in the absence of headache was reported by 27.8%of controls and 44.7% of headache sufferers (p<0.05). The latter figure increased to 71.3% when headache was actuallypresent (p<0.001). Blurred vision occurred in 13.5% of controls and 7.4% of headache sufferers (not significant). In thepresence of headache, the latter figure increased to 44.7% (p< 0.01).
Of the eye strain factors studied, bright light was reported to precipitate headache in 29.3% and to aggravate it in 73.4%.For reading, these figures were 16.0% and 55.3%, respectively; for working at the computer screen, 14.5% and 31.3%; and forwatching television, 6.4% and 27.7%. We conclude that visual symptoms are more common in chronic headache and eyestrain factors more important than is generally recognized.
(Headache 29:523-527, 1989)
INTRODUCTION
The visual symptoms which occur in relation to headache can be divided into specific and non-specific. The specific visual symptomsare those generally looked upon as aura symptoms of migraine. They represent the scintillating scotoma, also known as teichopsia orfortification spectra, as wall as its many variants. Characteristic features of these symptoms are the zigzag pattern, flickering brightnessand a particular pattern of development or "march."
The non-specific visual symptoms of headache are sensitivity to light, or photophobia, and blurred vision. These symptoms areneither specific for headache nor for any particular headache condition. The sensitivity to light can range from light being uncomfortableto the eyes, to light actually aggravating or precipitating headache.
In terms of aggravating or precipitating headache, light can also be looked upon as an eye strain factor. In this regard it can becompared with strenuous activities of the eyes such as in reading, working at the computer screen and watching television.
In the present study we determined the prevalence of the non-specific visual symptoms of headache in a group of chronic headachesufferers as compared with age- and sex-matched controls. As sensitivity to light is generally considered in the context of "sensitivity ofthe sensory organs," we also looked at sensitivity to noise and smell. Finally, we determined the prevalence of light as an eye strainfactor and compared it with reading, working at the computer screen and watching television.
METHODS
For the collection of data we developed a questionnaire which included the following items:
1. Age and sex;
2. Headache occurrence, age of onset of headache and present frequency, duration, laterality and intensity of headache;
3. Aggravation of headache by physical activity and whether headaches interfere with or prevent intended activities;
4. Association of headache with nausea, vomiting, sensitivity to light, noise and smell, and the occurrence of the sensitivities whenno headache is present;
5. Intensity of headache, nausea and the above mentioned sensitivities expressed on a visual analogue scale with no headache,nausea or sensitivity on one end of the scale and worst headache, nausea and sensitivity possible on the other;1
6. Occurrence of blurred vision with and without headache as well as a history of serious visual impairment or eye disease;
7. Precipitation or aggravation of headache by bright light, reading, working at the computer screen and watching television;
8. Occurrence of headache in parents, siblings and children.
The headache-related questions ware based, to as great an extent as possible, on the classification criteria of the InternationalHeadache Society.2
For data collection, patients attending the John R. Graham Headache Centre at Faulkner Hospital as well as the persons accompanyingthem and patients attending the Faulkner-Sagoff Centre for Mammography were used. The latter two groups were included in order toestablish a control group for which the criterion was either no headaches at all or a frequency of headaches of less than once per month. Thequestionnaires were filled out under the direct supervision of the first author who was also available for questions, but in answeringrespondents' questions special care was taken that the answers were not biased.
The answers were entered into a personal computer using the SPSS data-entry module. The SPSS statistical modules were used foranalysis of variance (F test), cross tabulations (Chi-Square test) and paired and unpaired comparisons (t-test). For age-and sex-matching anddata checking, the EXCEL spreadsheet was employed. A program designed by one of the authors (H.B.M.) was used for the Fisher's Exacttest.
In total 260 persons filled out the questionnaire in a way adequate for data entry and analysis. Of these 65 denied having headaches andan additional 30 indicated they had headaches less than once per month. To form the control group these two groups were combined,generating a population consisting of 47 males and 48 females with an average age of 45.3 years. The remaining 165 persons constituted theheadache group, consisting of 48 males and 117 females with an average age of 38.0 years.
In matching the two groups by age and sex, we first removed all the 15-year-olds as outliers because there were ten of them at thatextreme value in the female headache group. Then random scores were assigned to the remaining cases by multiplying age by a uniformzero-to-one random variable. A random selection with an age bias was achieved by removing cases starting with the lowest scores. This wasdone incrementally until the age mean for the headache females had been sufficiently increased. At that point, 94 cases remained in thatgroup after which a simple random sample was taken to get 50 cases. The result was a mean age of 41.2 years compared with 48 controlfemales with a mean age of 42.2 years.
The age mean for the control males, initially 48.5 years, was reduced by the same random-score method. The ultimate age mean was 45.3years for 42 cases to compare with 44 headache males with a mean age of 41.3. Analysis of variance revealed the remaining age and sexdifferences between the groups not to be significant with the lowest p-value being 0.223.
RESULTS
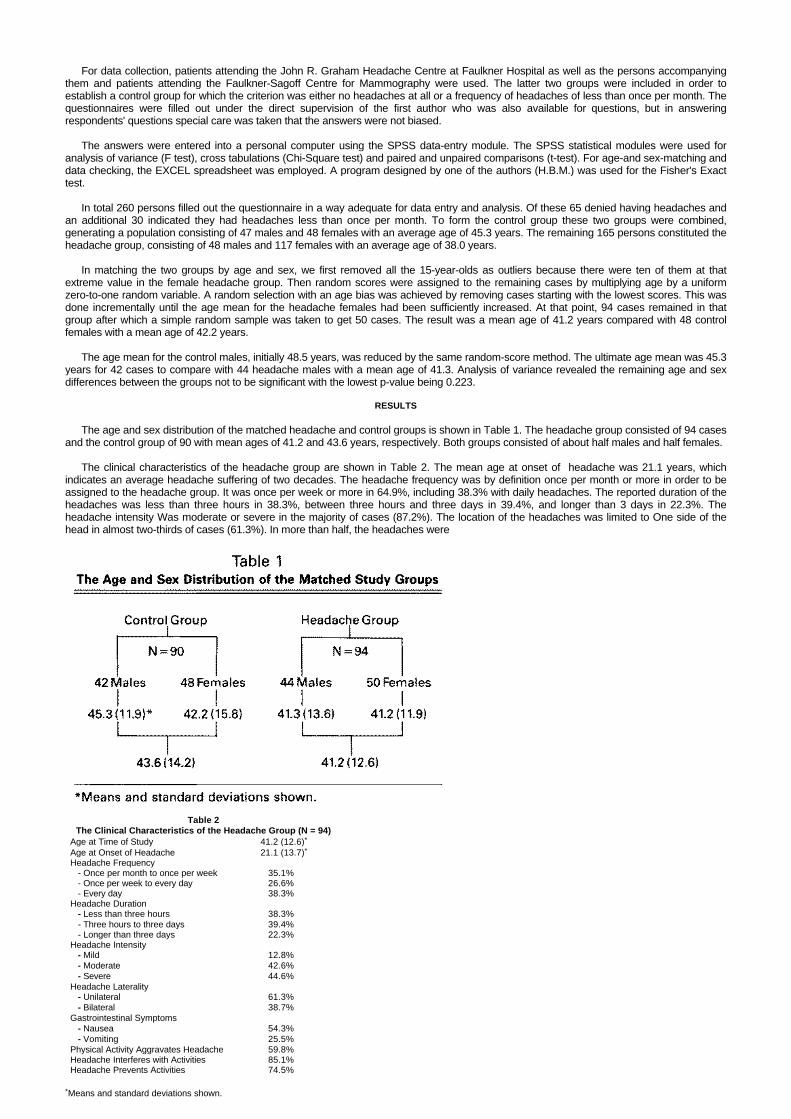
The age and sex distribution of the matched headache and control groups is shown in Table 1. The headache group consisted of 94 casesand the control group of 90 with mean ages of 41.2 and 43.6 years, respectively. Both groups consisted of about half males and half females.
The clinical characteristics of the headache group are shown in Table 2. The mean age at onset of headache was 21.1 years, whichindicates an average headache suffering of two decades. The headache frequency was by definition once per month or more in order to beassigned to the headache group. It was once per week or more in 64.9%, including 38.3% with daily headaches. The reported duration of theheadaches was less than three hours in 38.3%, between three hours and three days in 39.4%, and longer than 3 days in 22.3%. Theheadache intensity Was moderate or severe in the majority of cases (87.2%). The location of the headaches was limited to One side of thehead in almost two-thirds of cases (61.3%). In more than half, the headaches were
Table 2The Clinical Characteristics of the Headache Group (N = 94)
Age at Time of Study 41.2 (12.6)*
Age at Onset of Headache 21.1 (13.7)*Headache Frequency - Once per month to once per week 35.1% - Once per week to every day 26.6% - Every day 38.3%Headache Duration - Less than three hours 38.3% - Three hours to three days 39.4% - Longer than three days 22.3%Headache Intensity - Mild 12.8% - Moderate 42.6% - Severe 44.6%Headache Laterality - Unilateral 61.3% - Bilateral 38.7%Gastrointestinal Symptoms - Nausea 54.3% - Vomiting 25.5%Physical Activity Aggravates Headache 59.8%Headache Interferes with Activities 85.1%Headache Prevents Activities 74.5%
*Means and standard deviations shown.
associated with nausea (54.3%) and in one-fourth, with vomiting (25.5%). The headaches were aggravated by physicalactivity in 59.8% of cases; they interfered with activities in 85.1% and prevented activities in 74.5%.
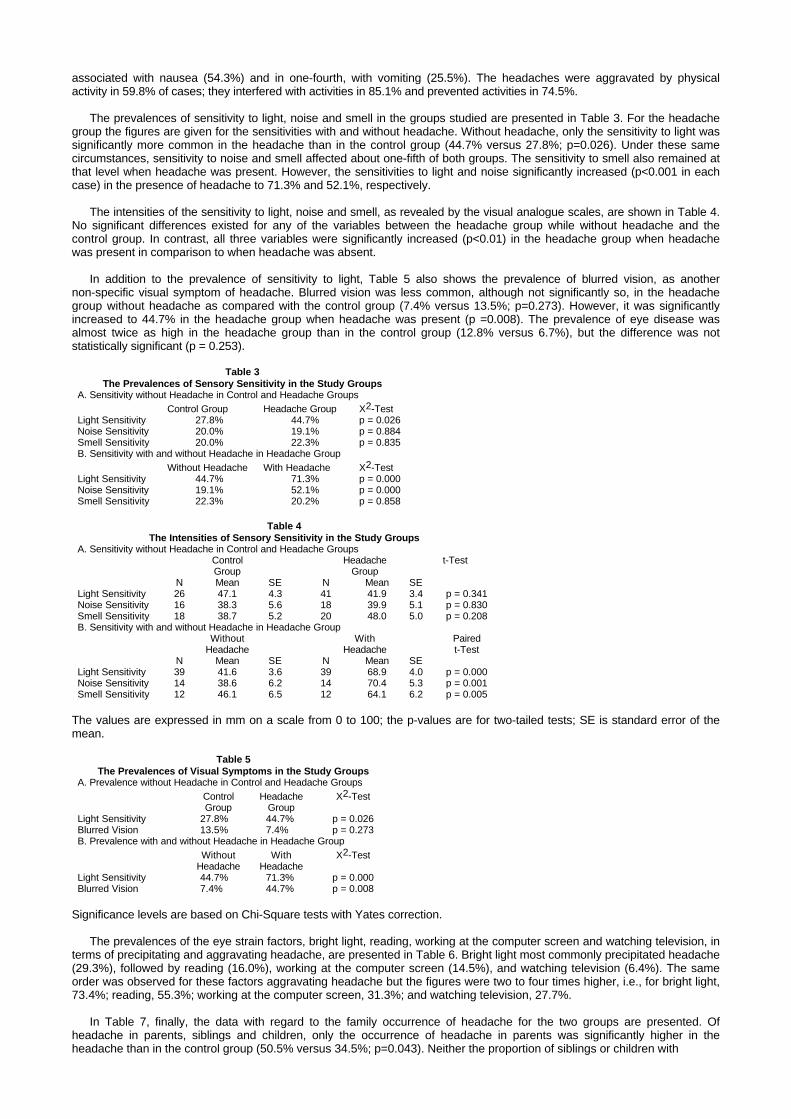
The prevalences of sensitivity to light, noise and smell in the groups studied are presented in Table 3. For the headachegroup the figures are given for the sensitivities with and without headache. Without headache, only the sensitivity to light wassignificantly more common in the headache than in the control group (44.7% versus 27.8%; p=0.026). Under these samecircumstances, sensitivity to noise and smell affected about one-fifth of both groups. The sensitivity to smell also remained atthat level when headache was present. However, the sensitivities to light and noise significantly increased (p<0.001 in eachcase) in the presence of headache to 71.3% and 52.1%, respectively.
The intensities of the sensitivity to light, noise and smell, as revealed by the visual analogue scales, are shown in Table 4.No significant differences existed for any of the variables between the headache group while without headache and thecontrol group. In contrast, all three variables were significantly increased (p<0.01) in the headache group when headachewas present in comparison to when headache was absent.
In addition to the prevalence of sensitivity to light, Table 5 also shows the prevalence of blurred vision, as anothernon-specific visual symptom of headache. Blurred vision was less common, although not significantly so, in the headachegroup without headache as compared with the control group (7.4% versus 13.5%; p=0.273). However, it was significantlyincreased to 44.7% in the headache group when headache was present (p =0.008). The prevalence of eye disease wasalmost twice as high in the headache group than in the control group (12.8% versus 6.7%), but the difference was notstatistically significant (p = 0.253).
Table 3The Prevalences of Sensory Sensitivity in the Study Groups
A. Sensitivity without Headache in Control and Headache GroupsControl Group Headache Group X2-Test
Light Sensitivity 27.8% 44.7% p = 0.026Noise Sensitivity 20.0% 19.1% p = 0.884Smell Sensitivity 20.0% 22.3% p = 0.835B. Sensitivity with and without Headache in Headache Group
Without Headache With Headache X2-TestLight Sensitivity 44.7% 71.3% p = 0.000Noise Sensitivity 19.1% 52.1% p = 0.000Smell Sensitivity 22.3% 20.2% p = 0.858
Table 4The Intensities of Sensory Sensitivity in the Study Groups
A. Sensitivity without Headache in Control and Headache GroupsControl Headache t-TestGroup Group
N Mean SE N Mean SELight Sensitivity 26 47.1 4.3 41 41.9 3.4 p = 0.341Noise Sensitivity 16 38.3 5.6 18 39.9 5.1 p = 0.830Smell Sensitivity 18 38.7 5.2 20 48.0 5.0 p = 0.208B. Sensitivity with and without Headache in Headache Group
Without With PairedHeadache Headache t-Test
N Mean SE N Mean SELight Sensitivity 39 41.6 3.6 39 68.9 4.0 p = 0.000Noise Sensitivity 14 38.6 6.2 14 70.4 5.3 p = 0.001Smell Sensitivity 12 46.1 6.5 12 64.1 6.2 p = 0.005
The values are expressed in mm on a scale from 0 to 100; the p-values are for two-tailed tests; SE is standard error of themean.
Table 5The Prevalences of Visual Symptoms in the Study Groups
A. Prevalence without Headache in Control and Headache GroupsControl Headache X2-TestGroup Group
Light Sensitivity 27.8% 44.7% p = 0.026Blurred Vision 13.5% 7.4% p = 0.273B. Prevalence with and without Headache in Headache Group
Without With X2-TestHeadache Headache
Light Sensitivity 44.7% 71.3% p = 0.000Blurred Vision 7.4% 44.7% p = 0.008
Significance levels are based on Chi-Square tests with Yates correction.
The prevalences of the eye strain factors, bright light, reading, working at the computer screen and watching television, interms of precipitating and aggravating headache, are presented in Table 6. Bright light most commonly precipitated headache(29.3%), followed by reading (16.0%), working at the computer screen (14.5%), and watching television (6.4%). The sameorder was observed for these factors aggravating headache but the figures were two to four times higher, i.e., for bright light,73.4%; reading, 55.3%; working at the computer screen, 31.3%; and watching television, 27.7%.
In Table 7, finally, the data with regard to the family occurrence of headache for the two groups are presented. Ofheadache in parents, siblings and children, only the occurrence of headache in parents was significantly higher in theheadache than in the control group (50.5% versus 34.5%; p=0.043). Neither the proportion of siblings or children with
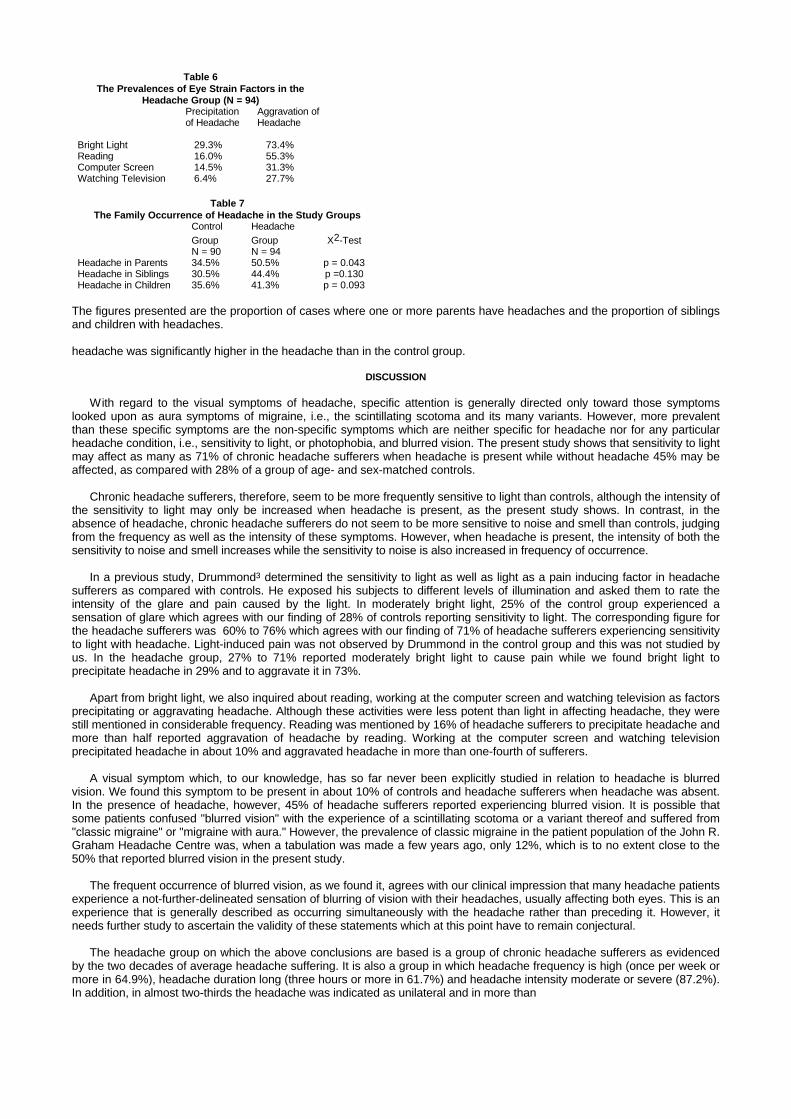
Table 6The Prevalences of Eye Strain Factors in the
Headache Group (N = 94)Precipitation Aggravation ofof Headache Headache
Bright Light 29.3% 73.4%Reading 16.0% 55.3%Computer Screen 14.5% 31.3%Watching Television 6.4% 27.7%
Table 7The Family Occurrence of Headache in the Study Groups
Control HeadacheGroup Group X2-TestN = 90 N = 94
Headache in Parents 34.5% 50.5% p = 0.043Headache in Siblings 30.5% 44.4% p =0.130Headache in Children 35.6% 41.3% p = 0.093
The figures presented are the proportion of cases where one or more parents have headaches and the proportion of siblingsand children with headaches.
headache was significantly higher in the headache than in the control group.
DISCUSSION
With regard to the visual symptoms of headache, specific attention is generally directed only toward those symptomslooked upon as aura symptoms of migraine, i.e., the scintillating scotoma and its many variants. However, more prevalentthan these specific symptoms are the non-specific symptoms which are neither specific for headache nor for any particularheadache condition, i.e., sensitivity to light, or photophobia, and blurred vision. The present study shows that sensitivity to lightmay affect as many as 71% of chronic headache sufferers when headache is present while without headache 45% may beaffected, as compared with 28% of a group of age- and sex-matched controls.
Chronic headache sufferers, therefore, seem to be more frequently sensitive to light than controls, although the intensity ofthe sensitivity to light may only be increased when headache is present, as the present study shows. In contrast, in theabsence of headache, chronic headache sufferers do not seem to be more sensitive to noise and smell than controls, judgingfrom the frequency as well as the intensity of these symptoms. However, when headache is present, the intensity of both thesensitivity to noise and smell increases while the sensitivity to noise is also increased in frequency of occurrence.
In a previous study, Drummond3 determined the sensitivity to light as well as light as a pain inducing factor in headachesufferers as compared with controls. He exposed his subjects to different levels of illumination and asked them to rate theintensity of the glare and pain caused by the light. In moderately bright light, 25% of the control group experienced asensation of glare which agrees with our finding of 28% of controls reporting sensitivity to light. The corresponding figure forthe headache sufferers was 60% to 76% which agrees with our finding of 71% of headache sufferers experiencing sensitivityto light with headache. Light-induced pain was not observed by Drummond in the control group and this was not studied byus. In the headache group, 27% to 71% reported moderately bright light to cause pain while we found bright light toprecipitate headache in 29% and to aggravate it in 73%.
Apart from bright light, we also inquired about reading, working at the computer screen and watching television as factorsprecipitating or aggravating headache. Although these activities were less potent than light in affecting headache, they werestill mentioned in considerable frequency. Reading was mentioned by 16% of headache sufferers to precipitate headache andmore than half reported aggravation of headache by reading. Working at the computer screen and watching televisionprecipitated headache in about 10% and aggravated headache in more than one-fourth of sufferers.
A visual symptom which, to our knowledge, has so far never been explicitly studied in relation to headache is blurredvision. We found this symptom to be present in about 10% of controls and headache sufferers when headache was absent.In the presence of headache, however, 45% of headache sufferers reported experiencing blurred vision. It is possible thatsome patients confused "blurred vision" with the experience of a scintillating scotoma or a variant thereof and suffered from"classic migraine" or "migraine with aura." However, the prevalence of classic migraine in the patient population of the John R.Graham Headache Centre was, when a tabulation was made a few years ago, only 12%, which is to no extent close to the50% that reported blurred vision in the present study.
The frequent occurrence of blurred vision, as we found it, agrees with our clinical impression that many headache patientsexperience a not-further-delineated sensation of blurring of vision with their headaches, usually affecting both eyes. This is anexperience that is generally described as occurring simultaneously with the headache rather than preceding it. However, itneeds further study to ascertain the validity of these statements which at this point have to remain conjectural.
The headache group on which the above conclusions are based is a group of chronic headache sufferers as evidencedby the two decades of average headache suffering. It is also a group in which headache frequency is high (once per week ormore in 64.9%), headache duration long (three hours or more in 61.7%) and headache intensity moderate or severe (87.2%).In addition, in almost two-thirds the headache was indicated as unilateral and in more than
half associated with nausea. These are important facts related to the possible generality of the resultsreported herein.
Acknowledgements: We would like to thank Dr. Norman L. Sadowsky, Director of the Faulkner-SagoffCentre, for allowing us to include his patients as controls in the study, and Mrs. Malina Zarskar Spierings,M.A. for editorial assistance in the preparation of the manuscript.
REFERENCES
1. Price DD, McGrath PA, Rafii A, Buckingham B: The validation of visual analogue scales as ratio scalemeasures for chronic and experimental pain. Pain 17:45-56, 1983.
2. International Headache Society: Classification and diagnostic criteria for headache disorders, cranialneuralgias and facial pain. Cephalalgia 8 (suppl 7): 1-96, 1988.
3. Drummond PD: A quantitative assessment of photophobia in migraine and tension headache.Headache 26:465-469, 1986.
Book Review
Title: Handbook of Chronic Pain ManagementEdited by: C. David TollisonWilliams and Wilkins, 1989
Price: $87.95
This is a well written, extremely comprehensive text book on the management of chronic pain. Thecomprehensive nature is accomplished by the use of 81 authors connected in various ways to the pain field.The list includes physicians from many different specialties such as Internal Medicine, Neurology,Neurosurgery, Anaesthesia, Physiatry, Psychiatry, Orthopaedics; and many others . . . Dentists,Psychologists, Chiropractors, as well as Physiologists, Pharmacologists and Engineers. Each explains his orher craft and its applicability to pain management. The chapters are in general, well written, and have readilyidentifiable sub-sections that make the material very readable. Many authors make use of well organizedcharts and diagrams to complement their text. In general the chapters offer many up-to-date references andthe index, like the text itself, is comprehensive.
The chapter on psychopharmacological agents in the treatment of pain syndromes is particularly excellentin its presentation of data and practical aspects.
The first section of the book is titled "Foundations." The chapter on Anatomy here is quite slim, and doesnot make use of the more current concepts. Diagrams are not used to illustrate the pathways. I felt that thiswas a weakness. Likewise I felt that a more intense description of biochemical aspects of pain should havebeen included in the "Foundations" section.
The chapter on headache is very well written. Obviously it would not meet the demands of someonespecialized in that field, but would serve as a good introduction to other readers.
A few inconsistencies are noted from chapter to chapter. I believe this is an unavoidable occurrence when81 authors contribute to one textbook and do not significantly detract from the quality of this work.
Overall, in view of the comprehensive nature of this text and its many excellent chapters, I would highlyrecommend "The Handbook of Chronic Pain Management" to anyone with an interest in the field.
Warren C. Goldstein, M.D.Next Book Review