a comparison of lisinopril and nifedipine in the treatment of mild to moderate hypertension
TRANSCRIPT
Eur J Clin Pharmacol (1994) 46:487-489
l BQssae eJle@ © Springer-Verlag 1994
Originals
A comparison of lisinopril and nifedipine in the treatment of mild to moderate hypertension
A muiticentre study
B. Rogstad
Medical Department, Buskerud Central Hospital, N-3004 Drammen, Norway
Received: 20 October 1993/Accepted in revised form: 10 May 1994
Abstract. Lisinopril has been compared with slow-re- lease nifedipine in a 16-week double-blind, randomized, parallel-group study involving 102 patients with mild to modera te hypertension. Sitting systolic and diastolic blood pressures were reduced 6 and 5 m m H g more by lisinopril than by nifedipine over 12 weeks mono- therapy.
After 12 weeks a greater proport ion of patients taking lisinopril was controlled (sitting diastolic blood pressure below 95 m m Hg) than in those taking nifedipine. As a re- sult, 17 % of those taking lisinopril and 38 % of those tak- ing nifedipine required additional therapy with hydro- chlorothiazide. The addition of hydrochlorothiazide re- suited in similar response rates in the lisinopril and nife- dipine groups (89 % and 75 % respectively).
The rate of reporting of adverse events considered to be drug-related and the rate of withdrawals were similar for both treatments. Cough was more often repor ted with lisinopril and headache, sweating, and hot flushes with nifedipine.
We conclude that once-daily t i trated doses of lisinopril produced bet ter control of blood pressure than twice- daily t i trated doses of nifedipine.
Key words: Lisinopril, Nifedipine, Hypertension; multi- centre study
In previous studies lisinopril in dosages of 10-80 mg once daily has been compared with nifedipine in dosages of 20- 80 mg daily in mild to severe [1] and mild to modera te [2, 3] hypertension. In two studies they were equally effec- tive [1, 2]. However, in a large-scale study [3], lisinopriI re- duced systolic and diastolic blood pressures significantly more than nifedipine. Lisinopril was bet ter tolerated than nifedipine in all three studies [1-3].
The aim of this study was to compare the antihyper- tensive effects and tolerability of lisinopril (titrated f rom 20-40 mg once daily) with nifedipine (titrated f rom 20- 40 mg twice daily) in patients with mild to modera te
hypertension, and to evaluate the effect of adding hydro- chlorothiazide 25 mg daily in patients inadequately con- trolled by either drug alone.
Patients and methods
We recruited men and women aged 18-70 y with mild to moderate essential hypertension (sitting diastolic pressure 95-115 mmHg). Patients who were already taking antihypertensive drugs disconti- nued treatment at least 4 weeks before entry. Patients with any of the following characteristics were excluded: secondary or malignant hypertension, myocardial infarction within the last three months, angina pectoris, heart failure, aortic outflow obstruction, renal, he- patic, or blood disorders, diabetes mellitus requiring insulin or oral medication, women likely to become pregnant during the course of the study (including those taking oral contraceptives), known hyper- sensitivity or contraindication to an ACE inhibitor or calcium anta- gonist, and poorly compliant patients. No other drugs known to af- fect blood pressure were permitted. All the patients gave informed consent to take part. The study was approved by the regional Ethics Committee and conducted according to the guidelines of the Decla- ration of Helsinki.
Procedure
This study was carried out in 14 centres in Norway, each enrolling 1- 15 patients. Sitting systolic and diastolic (phase V) blood pressures were measured to the nearest 2 mmHg with a sphygmomanometer after 5 rain rest. Each visit included three measurements and the mean of the last two measurements was recorded. Blood pressure and heart rate were assessed during the placebo run-in phase and after 2, 4, 8, 12, and 16 weeks of active treatment. Blood pressure control was considered achieved if the diastolic blood pressure was below 95 mmHg.
Blood samples were collected for routine haematological and biochemical tests after the placebo run-in period and after 12 and 16 weeks of active treatment. At each visit the patients were asked to report any adverse or unusual events and they completed a symptom questionnaire at the end of the run-in period and after 2, 12, and 16 weeks of treatment. The opinion of the investigator was obtained regarding the relation of these events to the study medication.
The patients took placebo tablets for 2 weeks in a single-blind phase. At the end of the run-in period patients were assigned to a treatment group using a computer-generated random scheme. Dur-
488
ing the active treatment period the "double-dummy" technique was used to maintain double-blindness, i. e. patients taking lisinopril also took the same number of placebo tablets matching nifedipine each day and vice versa. Hydrochlorothiazide packs were labelled. The patients took either lisinopril 10 mg in the morning or nifedipine 20 mg twice daily. After 4 weeks, if the diastolic blood pressure was 95 mmHg or more the dosage was increased to lisinopri120 mg once daily or nifedipine 40 mg in the morning and 20 mg in the evening. After 8 weeks the dosages were further increased, if necessary, to lisinopri140 mg once daily or nifedipine 40 mg twice daily. If the dias- tolic pressure after 12 weeks remained at 95 mm Hg or more, hydro- chlorothiazide 25 mg once daily was added.
Patient compliance was assessed at each visit by counting the re- maining tablets in the packages.
Statistical analyses
Analysis of co-variance was used to compare the changes in blood pressures and heart rates at the end of the two-week run-in period with those observed after 12 weeks of both active treatments. The null hypothesis of no inter-treatment difference was tested using an F-ratio test, and the treatment effect was estimated using confidence intervals. The model included terms for centre, treatment, and pre- treatment value (covariate). Initially, a term to test for centre by treatment interaction was included in the model, but as this was found not to contribute substantially it was dropped.
Two analyses of the data were performed. Data were analysed for all patients who completed the study ("completed patients ana-
Table 1. Characteristics of the patients (mean and SD or range)
Lisinopril Nifedipine
Number 49 53
Male/female 29/20 33/20
Age (y) 49 (29-67) 51 (24-68)
Weight (kg) 82 (16) 82 (18)
Sitting blood pressure (mmng) 166/104 (17/6) 167/106 (16/6)
Sitting heart rate (beats. min -1) 73 (10) 76 (8)
lysis"). Patients who did not complete the study, but who had data from the run-in period and a subsequent visit, were also analysed ("last value analysis"). The latter analysis has been given primary emphasis, as it is designed to reduce bias compared with a "com- pleted patients analysis". The "per protocol" analysis was not per- formed because there were too many protocol deviators (25 lisino- pril and 31 nifedipine).
The proportions of patients controlled after 4, 12, and 16 weeks were compared using Fisher's exact test, based on a "last value ana- lysis".
The proportion of patients with adverse events leading to with- drawal and the proportion of patients with adverse events possibly related to treatment were compared using Fisher's exact test.
Results
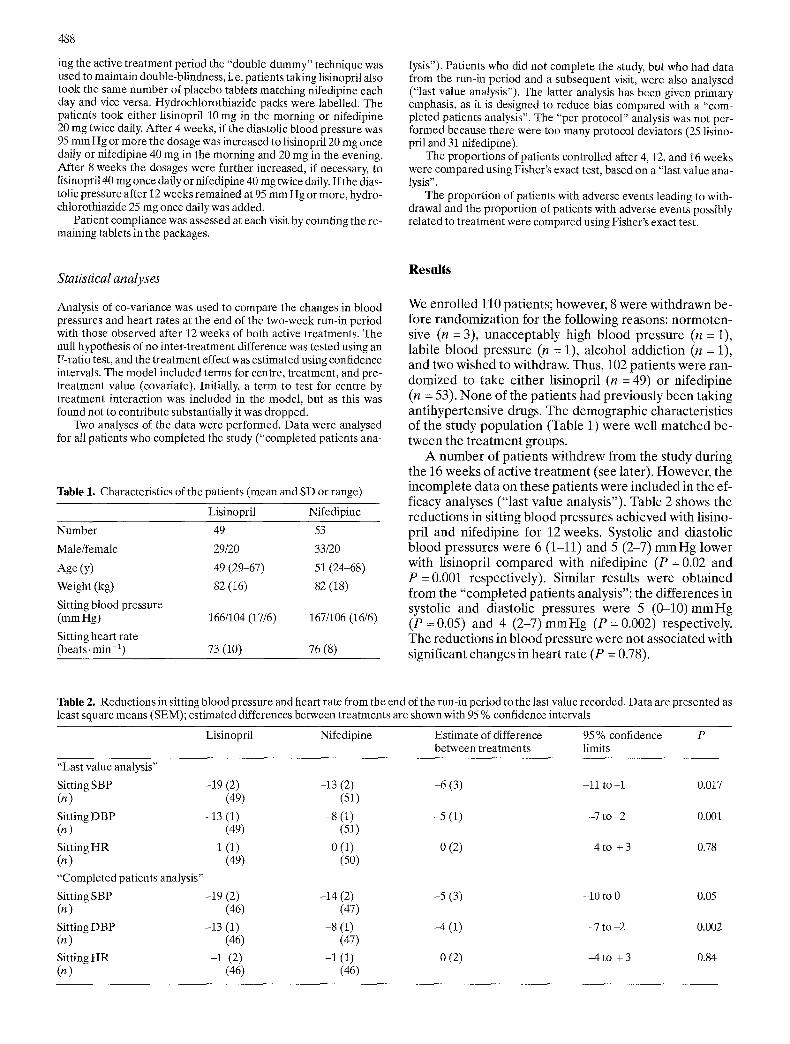
We enrol led 110 patients; however, 8 were wi thdrawn be- fore randomiza t ion for the following reasons: no rmoten- sive (n = 3), unacceptably high b lood pressure (n = 1), labile b lood pressure (n = 1), alcohol addict ion (n = 1), and two wished to withdraw. Thus, 102 patients were ran- domized to take ei ther lisinopril (n = 49) or nifedipine (n = 53). N o n e of the patients had previously been taking ant ihypertensive drugs. The demographic characteristics of the study popula t ion (Table 1) were well ma tched be- tween the t rea tment groups.
A n u m b e r of patients wi thdrew f rom the study during the 16 weeks of active t rea tment (see later). However , the incomplete data on these pat ients were included in the ef- ficacy analyses ("last value analysis"). Table 2 shows the reduct ions in sitting b lood pressures achieved with lisino- pril and nifedipine for 12 weeks. Systolic and diastolic b lood pressures were 6 (1-11) and 5 (2-7) m m H g lower with lisinopril c o m p a r e d with nifedipine (P = 0.02 and P = 0.001 respectively). Similar results were obta ined f rom the "comple ted patients analysis": the differences in systolic and diastolic pressures were 5 ( 0 - 1 0 ) m m H g (P =0.05) and 4 ( 2 - 7 ) m m H g (P = 0.002) respectively. The reduct ions in b lood pressure were not associated with significant changes in heart rate (P = 0.78).
Table 2. Reductions in sitting blood pressure and heart rate from the end of the run-in period to the last value recorded. Data are presented as least square means (SEM); estimated differences between treatments are shown with 95 % confidence intervals
Lisinopril Nifedipine Estimate of difference 95 % confidence P between treatments limits
"Last value analysis"
Sitting SBP -19 (2) (n) (49)
Sitting DBP -13 (1) (n) (49)
Sitting HR -1 (1) (n) (49)
"Completed patients analysis"
Sitting SBP -19 (2) (n) (46)
Sitting DBP -13 (1) (n) (46)
Sitting HR -1 (2) (n) (46)
-13 (2) -6 (3) -11 to -1 (51)
-8 (1) -5 (1) -7 to -2 (51)
0 (1) 0 (2) -4 to + 3 (50)
-14 (2) -5 (3) -10 to 0 (47)
-8 (1) -4 (1) -7 to -2 (47)
-1 (1) 0 (2) -4 to + 3 (46)
0.017
0.001
0.78
0.05
0.002
0.84

489
Table 3. Adverse events possibly related to treatment reported in more than one patient; Patient number (n) included all events re- ported
Lisinopril (n = 19) Nifedipine (n = 23) Run-in phase (n : 4)
Cough (9) Flushes/hot sweats (7) Headache (2) Pain in throat (4) Headache (6) Dizziness (3) Peripheral oedema (3) Disturbed sleep (2) Cold extremities (2) Nausea (2) Cough (2) Mouth discomfort (2) Dizziness (2)
Fatigue (2) Feeling of warmth (2) Itching (2) Palpitation (2) Tiredness (2)
After the initial 4 weeks of randomized treatment, diastolic pressure fell below 95 m m H g in 60 % of those taking lisinopril and in 47 % of those taking nifedipine (NS). After 12 weeks 17 % of those taking lisinopril and 38 % of those taking nifedipine required additional hydro- chlorothiazide (P = 0.04). After 16 weeks 89 % of those taking lisinopril and 75 % of those taking nifedipine were responders (P = 0.1).
Adverse events possibly related to treatment (Table 3) were reported by 39 % patients on lisinopril and 43 % on nifedipine (P = 0.07). Adverse events possibly related to t reatment which led to withdrawal were reported in two patients taking lisinopril and in three patients taking nife- dipine. A further three patients on lisinopril and two on nifedipine withdrew during the randomized part of the study for reasons other than adverse events. Headache, flushes, and hot sweats were more frequently reported by patients on nifedipine and cough by patients on lisinopril.
The laboratory variables remained unchanged.
Discussion
We have shown that lisinopril 10.40 mg once daily had a small but significantly larger effect on sitting blood pres- sure than nifedipine 20-40 mg twice daily over 12 weeks. This supports the previous finding of a large-scale study of 828 patients [3]. In another comparison [2] of fixed doses
of lisinopril (20 mg once daily) and nifedipine (20 mg twice daily), the two drugs were equally effective. The divergent result in that study might have been caused by the fixed dosage regimens.
Although the reduction in mean blood pressure is an important parameter of antihypertensive efficacy, the re- sponse rate to treatment is also important, as this indicates the likelihood of success. After 12 weeks a greater propor- tion of patients were controlled by once-daily lisinopril than by twice-daily nifedipine, as also reported in another study [3]. However, because of a large number of protocol violators in the presenting study, this result must be inter- preted with caution.
The adverse effects reported were largely those recog- nised to be associated with dihydropyridines and AC E in- hibitors. In contrast to other studies [1-3] we did not find a significant difference in tolerability between lisinopril and nifedipine.
Acknowledgements. I greatly acknowledge the help from the other centre (see Appendix) and thank Tore Ekeli and Henning Slinning from Zeneca, Norway, for assistance in the administration and co-or- dination of the study.
Appendix I
The following colleagues took part in the study: Dr. H. Bergrem, Dr. E. Bjering, Dr. L. Brodschj¢ll, Dr. O. Bharstad, Dr. D. Dyrbekk, Dr. A.Hauge, Dr. J.O.Lindeb¢, Dr. A.Lislerud, Dr. T.Meling, Dr. F. Moe, Dr. L. M. Nagy, Dr. E. Saltvedt, Dr. A. C. Sellgren, Dr. R Sir- nes, Dr. T. Stavnar, Dr. K. Valnes, Dr. T. Wessel-Aas, Dr. A. Woie.
References
1. M~arlin C, Baglivo H, Boeijinga JK, Breckenridge AM, Clement D, Johnston GD, Klein W, Kramer R, Luccioni R, Meurer KA, Richardson PJ, Rosenthal J, Six R, Witzgall H (1987) Com- parative trial of lisinopril and nifedipine in mild to severe essential hypertension. J Cardiovasc Pharmacol 9 [Suppl 3]: $48-$52
2. Witchitz S, Serradimigni A (1989) Lisinopril versus slow-release nifedipine in the treatment of mild to moderate hypertension: a multicentre study. J Human Hypertens 3 [Suppl 1]: 29-33
3. Os I, Bratland B, Dahlcf D, Gisholt K, Syvertsen JO, Tretli S (1991) Lisinopril or nifedipine in essential hypertension? A Nor- wegian multicenter study on efficacy, tolerability and quality of life in 828 patients. J Hypertens 9:1097-1104