a comparative immunohistochemical study
TRANSCRIPT
Tumor Markers in the Human Ovaryand Its Neoplasms
A Comparative Immunohistochemical Study
ETIENNE J. NOUWEN, PhD,PATRICIA G. HENDRIX, MS,
SIMONNE DAUWE,MARLENE W. EERDEKENS, MD, and
MARC E. DE BROE, MD, PhD
The incidence and histologic characteristics ofthe ex-pression of placental alkaline phosphatase (PLAP) inovarian tumors was compared with that of five othertumor antigens. Three monoclonal antibodies wereused for the specific localization of PLAP. PLAP waspresent in some sex cord cells of the 13-16-week fetalovary, probably germ cells. In normal ovaries, all anti-gens except carcinoembryonic antigen (CEA) werefrequently found in inclusion cysts; the germinal epi-thelium was positive only for cancer antigen 125 (CA125). The frequency and extent ofPLAP expression in
AN INTERESTING application of hybridoma tech-nology as a tool in cancer research consists in theproduction of specific monoclonal antibodies againsttumor specific substances called "tumor markers"and the use of these antibodies in tumor immuno-scintigraphy and immunotherapy of metastatic dis-ease. For this purpose, a marker substance should beexpressed in sufficient amounts by malignant cellsonly and preferably by all malignant cells in a tumor,including its metastases, and it should be located onthe cell surface. Unfortunately, several studies haverevealed that malignant tumors are often very hetero-geneous in the expression of tumor-associatedantigens.' 5 This problem might be significantly re-duced, however, by the combined use ofmonoclonalantibodies against different markers, provided thattheir histologic distribution is at least partially differ-ent. Immunohistology is a useful tool for investigatingthose features.
Using monoclonal antibodies, we have compared
From the Department ofNephrology and Hypertension,University Hospital Antwerp, Edegem, Belgium
nonmucinous carcinomas was higher than observedfor CA 19-9 and CEA, but was lower than for CA 125and human milk fat globule antigen. Serous tumorshad the highest PLAP expression, followed by endo-metrioid and poorly differentiated adenocarcinomas,and some other tumors. PLAP was predominantlymembranous; its histologic distribution was in generalheterogeneous. Different antibodies to PLAP gave dif-ferent staining intensities in some tumors, but thestaining patterns were always qualitatively identical.(AmJ Pathol 1987, 126:230-242)
on adjacent sections the histochemical distribution ofsix tumor-associated antigens that are more or less ofinterest in ovarian cancer. Different types of malig-nant and benign ovarian tumors and the normal adultand fetal ovary and reproductive tract were studied.
Supported by grants from the Fonds voor Kankeronder-zoek van de Algemene Spaar- en Lijfrentekas, NationaleLoterij - FGWO (Grant No. 9.0005.84), the National Pro-gram for Reinforcement of the Scientific Research(PREST/UIA 04) and a research grant from the Universityof Antwerp.Accepted for publication August 27, 1986.Address reprint requests to Marc E. De Broe, MD, PhD,Department of Nephrology and Hypertension, University
Hospital Antwerp, Wilrijkstraat 10, B-2520 Edegem, Bel-gium.
230
TUMOR MARKERS IN THE OVARY 231
Placental alkaline phosphatase (PLAP; EC 3.1.3.1.) isfrequently expressed by malignant ovarian neo-plasms.4'6'7 It is essential to use monoclonal antibod-ies for its specific localization, because all othermethods suffer from interference with other nontu-mor specific isoenzymes of alkaline phosphatasepresent in these tissues. HMFG 1 and HMFG 2 aremonoclonal antibodies directed against human milkfat globule membrane components and have beenused for tumor immunoscintigraphy and radioim-munotherapy of ovarian cancer.8 The other tumor-associated antigens investigated were cancer antigen125 (CA 125),9 10 CA 19-9,11 which is identical to sia-losyl-Lewisa, 12,13 and carcinoembryonic antigen(CEA).
Materials and MethodsMaterials
3-Amino-9-ethylcarbazole, poly-L-lysine (molec-ular weight >300,000), nitroblue tetrazolium, andtrypsin (Type Ills, 11,700 units/mg) were obtainedfrom Sigma Chemical Co., St. Louis, Missouri; bio-tinylated horse anti-mouse immunoglobulin serum,avidin, and biotinylated horseradish peroxidase wereobtained from Vector Laboratories, Inc., Burlin-game, California; L-p-bromotetramisole was ob-tained from Janssen Chimica, Beerse, Belgium; 5-bromo-4-chloro-3-indoxylphosphate-p-toluidine saltwas obtained from Serva Feinbiochemica GmbH,Heidelberg, Federal Republic ofGermany; low-melt-ing-point (49 C) paraffin was obtained from BDHChemicals Ltd., Poole, United Kingdom.
Tissues
The study comprises 54 malignant, 6 borderline,and 31 benign ovarian tumors; 23 normal ovaries (ageranging from 17 to 74 years); 7 normal oviducts; and 2normal endometrium samples. All tissues were surgi-cal biopsies. Fetal tissues between 11 and 16 weeks ofgestation were obtained from intact fetuses after pros-taglandin-induced expulsion. They included 4 fetalovaries, oviducts, and uteri (13,14,14, and 16 weeks ofgestation) and 2 fetal testes (1 1 and 14 weeks ofgesta-tion). The samples were processed for histologic ex-amination within 2 hours after receipt. Prior to fixa-tion, the tissues were cut into 1.5-mm-thick slices.
Immunohistochemical Localization of PLAP, CA125, HMFG, CA 19-9 and CEA
The immunohistochemical staining procedures forCA 125, HMFG, CA 19-9, and CEA are the same asdescribed previously for PLAP.4 Briefly, the tissueswere fixed for 1.5 hours in buffered 4% formaldehyde
(0.1 M sodium cacodylate buffer, pH 7.4, containing1% CaCl2) and were embedded in Paraplast or in low-melting-point paraffin. Adjacent 4-,u sections weremounted on poly-L-lysine-coated slides (0.1 mg/ml),treated with trypsin; and binding of the monoclonalantibodies was revealed by an indirect avidin -biotin - peroxidase method. Staining for peroxidasewas performed with 3-amino-9-ethyl carbazole. Forthe localization of PLAP, three specific monoclonalantibodies were used: 17E3'4 and E6'5 culture super-natant diluted 1/50, and purified H 1 7E2'6 diluted1/3000. The other monoclonal antibodies were OC125 for CA i25,9 ascitic fluid diluted 1/3000; HMFG1 and HMFG 2 for HMFG,17 culture supernatantsdiluted 1/50; 1116 NS 19-9 for CA 19-9,1" culturesupernatant diluted 1/20; purified antibody to CEAfrom Hybritech (Lot No. 360791) diluted 1/100,000.The sections were counterstained with methyl greenand were mounted in glycerin-gelatin.No difference could be found between tissues em-
bedded in Paraplast or in low-melting-point paraffin.Treatment with trypsin yielded significantly strongerand more consistent staining with each of the eightmonoclonal antibodies. Negative control stainingwas performed on adjacent sections with a monoclo-nal antibody ofirrelevant specificity or normal mouseserum. Full-term placenta, a colon carcinoma, amammary carcinoma, and an ovarian carcinoma,processed in identical ways, were used as positivecontrols for PLAP, CEA, HMFG, and CA 125 stain-ing, respectively.
Conclusions on the immunohistochemical stainingintensities for PLAP, obtained with the monoclonalantibodies 1 7E3, E6, and H 1 7E2, are based on at leasttwo separate staining experiments in which the threeantibodies were used on adjacent sections.
Histochemical Localization of Nonspecific AlkalinePhosphatase (NSAP)
Paraffin sections adjacent to those for the immuno-histochemical demonstration of PLAP were used tolocalize NSAP with 5-bromo-4-chloro-3-indoxyl-phosphate-p-toluidine salt as the substrate and nitroblue tetrazolium as the capturing agent. 18 Histochem-ical inhibition studies were performed as describedpreviously'9 by adding 1 mM L-p-bromotetramisole20to the incubation mixture. The sections were coun-terstained with methyl green and mounted inglycerin -gelatin.
Routine Histology
Adjacent sections were stained either with Carazzi'shematoxylin and eosin or with Masson's trichrome.
Vol. 126 * No. 2

232 NOUWEN ET AL
Results
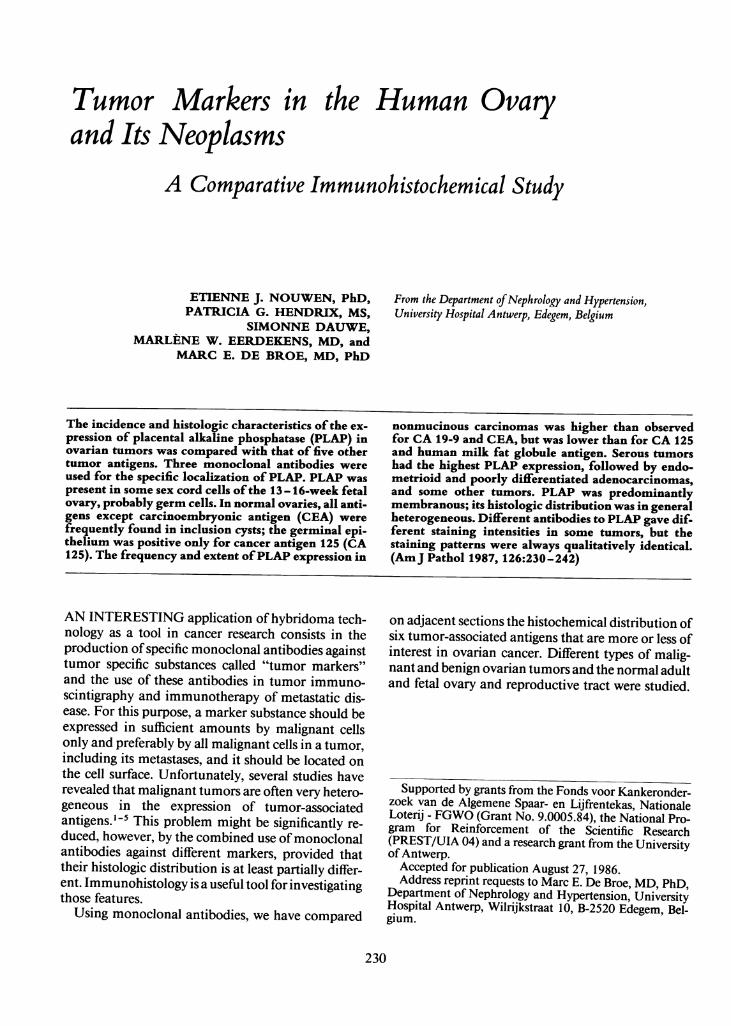
In the fetal ovaries of 13 - 16 weeks' gestation, thesurface epithelium was negative for all antigens. Incontrast, strong PLAP staining was found, irrespec-tive ofthe monoclonal antibody used, in a substantialnumber ofcells localized in the cortical sex cords. Thenumber ofpositive cells decreased from the peripheryto the center of the organ (Figure 1B). Staining forNSAP was stronger, and almost all sex cord cells werepositive (Figure 1A). L-p-Bromotetramisole nearlyabolished NSAP staining, except for a weak stainingin some cells, the number and position of which wasidentical to that of the PLAP immunohistochemi-cally positive cells. A few sex cord cells contained CA19-9 staining. No staining for CA 125, HMFG 1,HMFG 2, or CEA could be observed. In comparison,Figure 2A and B illustrates the distribution ofNSAPand PLAP, respectively, in a 14-week fetal testis.PLAP staining was found in a limited number of tu-bular cells with either of the three monoclonal anti-bodies. More tubular cells were positive for NSAP,and NSAP staining was also seen intracellularly in
some interstitial cells. The number of PLAP-express-ing cells in the fetal testis is significantly smaller thanin the ovary of comparable age.
Positive NSAP staining on the apical plasma mem-brane of the epithelial cells lining the 13- 14-weekfetal oviduct and uterus was abolished in the presenceof L-p-bromotetramisole. PLAP immunostainingwas absent. The oviduct was positive for CA 125 andHMFG 1 and 2; scarce staining was also found forCA19-9. The fetal uterus was positive only forHMFG 1.PLAP was found on the apical plasma membrane ofthe 11 - 16-week chorionic trophoblast, but only a fewof the villi showed positive staining. All other fetaltissues were negative for PLAP.
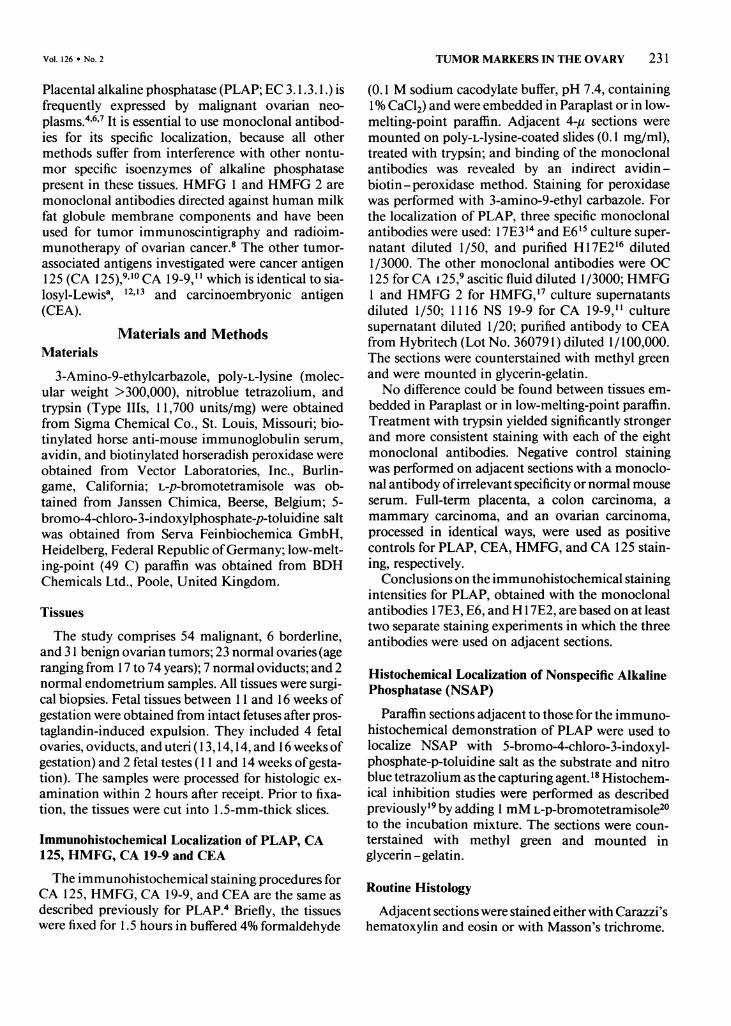
In 23 adult normal ovaries, relicts of the surfaceepithelium, present in 75% of them were sometimes(47%) positively stained for CA 125 (Figure 3A).HMFG was present only in 1 case; the other antigenswere always absent. Local invaginations (Figure 3Cand D) and proliferations (Figure 3B) ofthe germinalepithelium, present in 8 (35%) and 5 (22%) ovaries,respectively, were frequently positive for CA 125(83% and 90%, respectively). Germinal inclusion
2 EFigure 1-Fourteen-week fetal ovary. A-NSAP staining (arrows indicate primary oocytes). B-PLAP staining in some sex cord cells, probablyoogonia (antibody 17E3). The surface epithelium is negative for NSAP and PLAP. (A and B, adjacent sections, X21 0) Figure 2- Fourteen-week fetaltestis. A- NSAP staining (arrows indicate intracellular NSAP staining in some interstitial cells). B- PLAP staining in some tubular cells (antibodyH17E2). (A and B, X210)
AJP * February 1987

TUMOR MARKERS IN THE OVARY 233
cysts were sometimes positive for NSAP (8/16 [50%]),PLAP (10/23 [44%], Figure 4B), HMFG 1 (7/19[37%]), HMFG 2 (9/16 [56%]), and CA 19-9 (14/21[67%], Figure 4C). They were nearly always positivefor CA 125 (14/15 [93%], Figure 4A). In contrast,CEA was absent in all of 15 inclusion cysts. Expres-sion of the different antigens in these cysts was inde-pendant. Some NSAP-containing inclusion cystswere negative for PLAP. Staining for PLAP, HMFG1, CA 125, and CA 19-9 was localized on the apicalplasma membrane of the epithelial cells and in thecontent of the inclusion cysts. Staining for HMFG 2was also cytoplasmic. The lining epithelium was ingeneral homogeneous in the expression of themarkers (Figure 4A and B), but a pronounced cellularheterogeneity was also observed occasionally (eg, Fig-ure 4C). Primary and growing follicles, observed in 6premenopausal ovaries, were frequently positive onlyfor CA 19-9 (Figure 5A and B). The zona pellucida ofmature vesicular follicles found in two ovaries wasalso positive (Figure 5C). All other constituents ofnormal pre- and postmenopausal ovaries were nega-tive for all antigens. The normal adult peritoneal me-sothelium was positively stained only for CA 125.
In the normal tubal epithelium, the distribution ofthe different markers was roughly similar to thatfound in the borderline and malignant serous tumors,although CA 125 was more heterogenously distrib-uted (grading, 2-4). The immunohistochemicalgrading was 2 - 3 for PLAP,2 -4 forHMFG 1,3 -4 forHMFG 2, and 1-2 forCA 19-9; CEA was absent. Oneof 7 samples was negative for PLAP, and anotherlacked CA 19-9 staining. Normal endometrial glandswere uniformly stained for CA 125, HMFG 1, andHMFG 2 and scarcely for CA 19-9. PLAP and CEAstaining were absent.Table 1 shows the histopathologic tumor identifi-
cation and grade, the histochemical grading forNSAP, and the immunohistochemical grading forPLAP (using the antibodies 17E3, E6, and HI 7E2),CA 125, HMFG 1 and 2, CEA, and CA 19-9 for themalignant tumors. NSAP staining in the tumoralstroma and small blood vessels was omitted in thehistochemical grading. Table 2 summarizes the re-sults for the borderline and benign ovarian tumors.
In the group ofbenign tumors, PLAP and CEA hadthe lowest frequency of positivity (26% for both),PLAP being present in some serous tumors and cysts,CEA being present in some mucinous tumors andteratomas. CA 125, HMFG 1 and 2, and CA 19-9positive staining occurred with a frequency ofapprox-imately 60% in all common types of benign tumors.Figure 7 illustrates the staining pattern for HMFG 2in a dermoid cyst.
Each of the five borderline serous cystadenomascontained staining for PLAP, CA 125, HMFG 1 and2, and CA 19-9; only one was scarcely positive forCEA. An example ofthe comparative distribution ofthe different antigens is shown in Figure 6. The scarceCEA positivity in this tumor was restricted to cellsthat did not stain for PLAP.Among the malignant tumors, serous adenocarci-
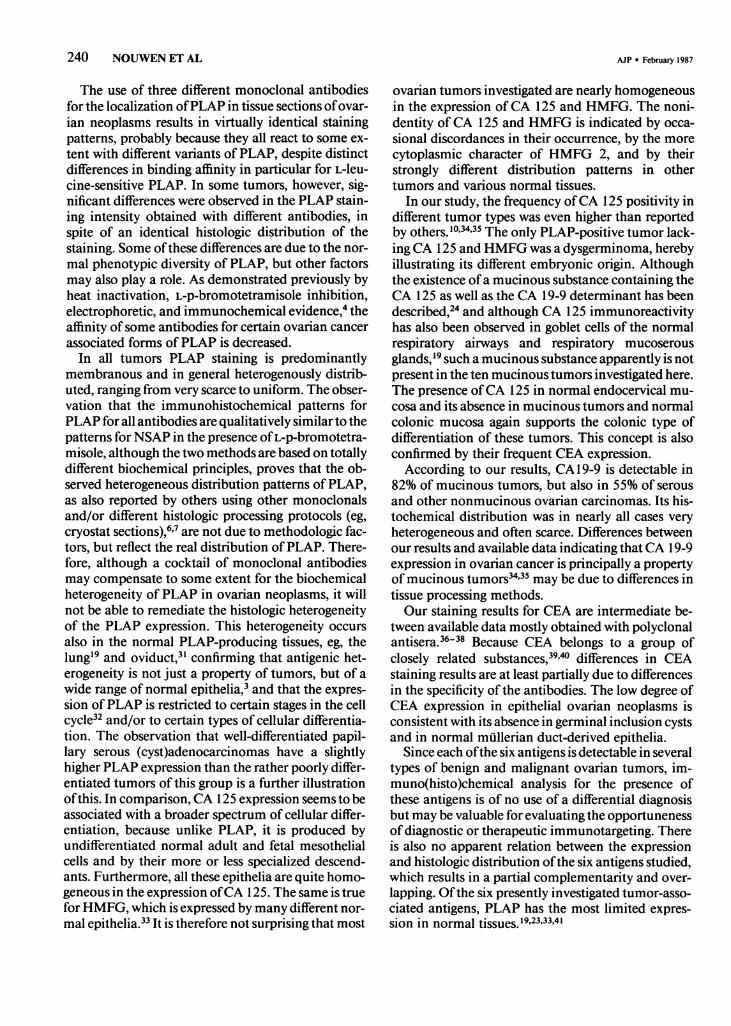
nomas had the highest incidence of PLAP-positivestaining (85%), followed by endometrioid and poorlydifferentiated adenocarcinomas (57%) and granulosacell tumors. Mucinous carcinomas and some otherless frequent tumor types were negative. However, inthe first group, only 35% ofthe tumors showed PLAPstaining in more than half of the cells. The overallfrequency of PLAP was 60%. PLAP expression inGrade 1 and Grade 1-2 papillary serous (cyst)adeno-carcinomas was comparable to that in borderlineserous tumors but was slightly higher than in Grade2 - 3 and Grade 3 serous adenocarcinomas. Compari-son ofPLAP staining patterns obtained with the threemonoclonal antibodies reveals that although the pat-terns were always qualitatively identical, differentstaining intensities were found with each ofthese anti-bodies in some tumors. The histochemical stainingpatterns for NSAP, obtained in the presence of L-p-bromotetramisole (a specific inhibitor for liver-bone-kidney type alkaline phosphatase), were more hetero-geneous than those obtained in the absence ofinhibitor and were similar to the immunohistochemi-cal patterns revealed by each ofthe anti-PLAP mono-clonal antibodies (Figure 11). Many tumors also con-tained a substantial number ofmalignant cells lackingNSAP staining. CEA was found in all different tumortypes, except in the granulosa-cell tumors, the clear-cell carcinomas, the dysgerminoma, and some otherrare types. It was predominantly localized on theplasma membranes, and staining was, in general,scarce. The overall frequency of CEA-positive stain-ing was 37%. CA 125, HMFG 1 and 2, and CA 19-9were present in all major tumor types, with an overallfrequency of 81%, 89%, 92%, and 60%, respectively.HMFG 1 had a slightly more heterogeneous expres-sion than HMFG 2. The latter was, in general, notonly membranous but also cytoplasmic. All antigenshad a different histologic distribution, both withinsingle and between different tumors. Some typicalexamples ofthe staining patterns are given in Figures8-12.
DiscussionThe use ofPLAP as a serologic marker for ovarian
cancer, compared with CA 125 and CEA, has been
Vol. 126 * No. 2

234 NOUWEN ET AL
..C...
:.4
AJP * February 1987
if
-44ik.
C.
-K
-.kQ.
I.il:
I14B4,1

Vol. 126 * No. 2 TUMOR MARKERS IN THE OVARY 235
Table 1 Histochemical Grading* for NSAP and Immunohistochemical Grading for PLAP, CA 125, HMFG 1, HMFG 2, CEA, and CA19-9 in Malignant Ovarian Tumors
No. Gradet Histopathology NASP PLAP CA125 HMFG 1 HMFG 2 CEA CA 199
1 Papillary serous cystadenocarcinoma1 Papillary serous cystadenocarcinoma1 Papillary serous cystadenocarcinoma1 Papillary serous cystadenocarcinoma1 Papillary serous cystadenocarcinoma1 Papillary serous cystadenocarcinoma1 Papillary serous cystadenocarcinoma1 Papillary serous cystadenocarcinoma
1-2 Papillary serous cystadenocarcinoma1-2 Papillary serous cystadenocarcinoma1-2 Papillary serous cystadenocarcinoma2-3 Papillary serous cystadenocarcinoma2-3 Papillary serous cystadenocarcinoma2-3 Papillary serous cystadenocarcinoma2-3 Papillary serous adenocarcinoma3 Papillary serous adenocarcinoma3 Papillary serous cystadenocarcinoma3 Papillary serous adenocarcinoma3 Papillary serous adenocarcinoma3 Tubulopapillary cystadenocarcinoma1 Mixed serous/mucinous cystadenocarcinoma1 Endometrioid carcinoma
1-2 Endometrioid carcinoma1-2 Endometrioid carcinoma2 Endometroid carcinoma3 Endometrioid carcinoma3 Endometrioid carcinoma3 Endometrioid carcinoma3 Adenocarcinoma3 Adenocarcinoma3 Adenocarcinoma3 Adenocarcinoma3 Adenocarcinoma3 Adenocarcinoma3 Adenocarcinoma1 Clear-cell carcinoma1 Clear-cell carcinoma1 Mucinous cystadenocarcinoma
1-2 Mucinous cystadenocarcinoma1-2 Mucinous cystadenocarcinoma2-3 Mucinous cystadenocarcinoma2 Granulosa-cell tumor3 Granulosa-cell tumor3 Granulosa-cell tumor
Monodermal teratoma struma ovarii/carcinoidEpidermoid carcinomaMixed homologous MUllerian sarcomaMixed heterologous MUllerian sarcoma
CarcinosarcomaSarcomaSarcomaSarcomaSarcoma
3 Dysgerminoma
4-a 4-a 3-a 3-a2-a 2-a 4-a 2-a2-a 2-a 4-a 3-am4-a 4-a 4-a 2-a2-a 2-ac 2-a 2-a3-ma 2-m 3-m 4-a3-a 3-a 4-a 3-a
0 0 4-a 2-a3-ma 3-m 4-m 4-ac4-ac 3-am 3-m 3-am3-a 2-a 4-m 4-a
0 0 4-am 3-a3-cg 0 4-am 2-ag3-m 3-m 3-m 4-ac2-m 2-m 4-mc 4-a1-a 1-a 4-ac 2-a2-m 1-am 4-mc 4-ac3-m 3-m 4-m 4-a2-ac 2-a 3-a 3-a3-mc 2-a 4-mc 2-a2-a 2-a 3-a 3-a2-am 2-a 4-a 3-ac3-am 3-m 4-m 3-a2-a 1-a 1-a 2-a3-am 2-a 4-ac 4-ac4-ma 0 2-ca 3-ag
0 0 0 2-m2-am 0 4-m 4-a1-ma 1-a 1-a 2-a3-m 2-c 4-m 3-ac3-am 3-am 3-ma 3-ag
0 0 4-am 3-ag0 0 2-a 3-mc
3-am 2-m 3-ma 4-ac3-m 0 4-m 4-mc
0 0 3-a 4-a0 0 1-a 3-a0 0 1-a 2-ac0 0 0 3-ac
3-a 0 0 00 0 0 0
2-am 1-m 3-a 4-ac2-ma 1-am 4-m 4-a
0 0 0 0
0 0 0 2-a3-am 2-a 4-ac 4-a3-m 3-m 4-m 4-am3-m 0 2-a 4-a2-mc 0 0 4-a
0 0 0 0
0 0 0 0
0 0 0 0
3-c 0 0 03-mc 3-m 0 0
4-a 2-a 3-a4-c 3-a 2-a3-a 0 03-c 0 2-a2-a 2-ca 3-ac4-ac 0 04-ac 0 1-a4-a 0 04-ac 1-a 03-am 0 04-mc 1-c 2-a4-ac 0 04-m 0 1-a4-ac 1-a 1-a4-mc 0 1-am3-m 0 04-ca 3-a 04-mc 1-mc 03-ac 0 2-a3-ac 3-c 1 -m3-ac 2-ca 03-ac 0 3-a3-m 0 3-ac2-a 3-a 2-a4-ca 0 03-mc 0 03-mc 0 04-ac 0 1--m2-a 0 04-mc 1-c 1-m4-ac 2-ca 2-a4-ac 1--m 04-c 0 2-a4-mc 0 1--m4-mc 0 1-mg4-m 0 2-a2-a 0 03-a 3-a 2-a3-ac 0 1-c2-ca 3-a 2-ca
0 4-ac 4-m3-ac 0 2-m4-ac 0 1--m
o 0 0
2-a 0 1-a4-ac 2-c 04-mc 3-m 3-m3-cm 0 1-a2-ac 0 0
0 0 0
0 0 0
1-m 0 02-c 0 0
0 0 1--m
*Number indicates histologic distribution (% positive cells): 1, scarce (<5%); 2, focal (5- <50%); 3, predominant (50-<90%); 4, uniform (90-100%). Lettercode indicates cellular localization: c, diffuse cytoplasmic; g, intracellular granules; a, apical plasma membrane; m, plasma membranes.
tGrades: 1, well-differentiated; 2, moderately well differentiated; 3, poorly differentiated.
23456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Figure 3-Normal postmenopausal ovaries. A-CA 125 staining in normal germinal epithelium. B-CA 125 staining in local proliferations of thegerminal epithelium. C and D-CA 125 staining in invaginations of the germinal epithelium. (A, X262; B, X164; C, X210; D, X164) Figure 4-Normalpostmenopausal ovaries. A-CA 125 staining in a germinal inclusion cyst. B- PLAP staining in the same cyst. C-CA 19-9 staining in a germinalinclusion cyst. (A and B, X210; C, X131) Figure 5-Normal premenopausal ovaries. A-CA 19-9 staining in primary follicles. B-CA 19-9staining in zona pellucida of a mature vesicular follicle. (A, X164; B, X265)

236 NOUWEN ET AL
Table 2- Histochemical Staining for NSAP and Immunohistochemical Staining for PLAP, CA 125, HMFG 1, HMFG 2, CEA, and CA19-9 in Borderline and Benign Ovarian Tumors
No. positive for
Histopathology N NSAP PLAP CAl 25 HMFG1 HMFG2 CEA CA 19-9
Borderline tumors(Papillary) serous cystadenoma 5 5 5 5 5 5 1 5Mucinous cystadenoma 1 0 0 0 1 1 0 0
Benign tumorsSerous cystadenofibroma 4 4 3 3 3 3 0 1Serous/mucinous cystadenoma 1 1 1 1 1 1 1 1Serous cyst 5 3 3 4 4 3 1 3Endometriosis 4 2 1 3 3 2 0 3Fibroma 1 0 0 0 0 0 0 0Mucinous cystadenoma 5 0 0 0 4 4 3 4Dermoid cyst 5 1 0 3 4 5 1 3Immature teratoma 1 1 0 1 1 1 1 1Cystic teratoma 3 1 0 2 2 2 1 3
Granulosa lutein cyst 2 0 0 0 0 0 0 0
documented previously.4'2123 In this paper the ex-
pression ofPLAP in the major histologic types ofma-lignant and benign ovarian tumors and in differentfetal tissues, including the male and female gonads, isdescribed with the use of three different monoclonalantibodies and is compared with that of five othermarkers which are ofsome interest in ovarian cancer.
All antigens studied except CEA are more or lessfrequently found in normal ovaries, but their expres-sion is always very limited, and their distribution pat-terns are not identical. Positive CA 125 staining innormal ovaries is in contrast to available data,'0'24 butis probably related to the presence of this antigen inthe normal peritoneal and pleural'9 mesothelium.PLAP can be considered as a real oncofetal marker
for the ovary because it is the only one ofthe six sub-stances investigated having a significant expression inthe 13 - 16-week fetal ovary, and the ovary is the onlyfemale fetal organ expressing PLAP, apart from thechorion. It is difficult to determine on morphologicgrounds whether the PLAP-positive cells are somaticsex cord cells and/or germ cells, more in particular,oogonia. The clearly recognizable large primary oo-
cytes and the mesenchymal cells are negative. Like-wise, in the fetal testis, the PLAP-expressing tubularcells might be germ cells and/or primitive Sertoli cells.However, the expression ofPLAP by the dysgermin-oma and the observations that seminomas and em-
bryonic carcinomas25'26 and primary intracranialgerm cell tumors27 also express PLAP frequently, sug-gest that the PLAP-expressing cells in the fetal ovaryand testis are probably germ cells. Moreover, the
greater tendency of peripherally localized fetal ovar-ian cells to express PLAP parallels the mitotic activityofthe germ cells, which decreases from the peripherytoward the center ofthe organ, suggesting that PLAPexpression is a property ofthe less differentiated germcells. The absence ofPLAP in primary oocytes and inthe ovum of primary, growing, and mature vesicularadult follicles is also consistent with this.On the other hand, approximately 90% of the ma-
lignant ovarian tumors that develop in adults do notoriginate from germ cells, but instead are thought toarize from modified peritoneal mesothelial cells cov-ering the surface ofthe ovary or lining germinal inclu-sion cysts.28'29 Nevertheless, several of these tumortypes express PLAP frequently, as also reported byothers.67 Although neither the adult nor the fetalovarian surface epithelium produce PLAP, its fre-quent expression by germinal inclusion cysts indi-cates that this epithelium has a strong potentiality toproduce PLAP under certain conditions. The expres-
sion of the other tumor-associated antigens in ger-
minal inclusion cysts adds further evidence in favor ofthe germinal epithelial origin of ovarian carcinomas.On the other hand, only a few normal epithelia pro-
duce PLAP in varying amounts, ie, the glandular en-
docervical epithelium,30 the tubal epithelium,3' andthe respiratory epithelium. 19 The former two are em-
bryonically related to the ovarian surface epithelium,because they develop from the mullerian duct. Thisrelationship is also reflected by the observations thatbenign, borderline, and malignant ovarian tumorswith a clearly recognizable serous, ie, tubal, differen-
Figure 6-Borderline papillary serous cystadenoma (Tumor 55). A-PLAP staining (antibody 17E3). B-HMFG 2 staining. C-HMFG 1staining. D-CA 19-9 staining. E-PLAP staining (antibody E6). F-CEA staining. G-CA 125 staining. (A-D, adjacent sections, X131;E - G, adjacent sections, X21 0) Figure7-Dermoid cyst (Tumor 81). HMFG 2 staining in sebaceous gland and stratum germinativum of epidermislike innersurface epithelium. (X105)
AJP * February 1987

TUMOR MARKERS IN THE OVARY 237
-:57* h-s
tX.i jXl.X
..
.r. .t .:,. ; x;
: ..... a..* - . i:X:i... ., s-;
,i! [@ filil,.... * .. 1,.,.; 2 ;. gi.,li.,''*; ' .I. .i-^X. ;s P *. .;
'-},:.'
Vol. 126 * No. 2
I.. ., I.' ... j"- I " -, ;m: .,." 0 -,,&a

AV
~ ~ 8
9 B

TUMOR MARKERS IN THE OVARY 239
B
Figure 11-Moderately well differentiated granulosa cell tumor (Tumor 42). A-NSAP staining. B-NSAP staining in the presence of 1 mML-p-bromotetramisole. C-PLAP staining (antibody 17E3). (A-C, adjacent sections, X105) Figure 12-Dysgerminoma (Tumor 54). A-NSAPstaining in the presence of 1 mM L-p-bromotetramisole. B-PLAP staining (antibody 17E3). (arrows indicate dotlike staining distribution on the cellsurface). (A and B, X265; inset, B, X550)
tiation have the highest tendency to express PLAP,and that the distribution patterns of the six presentlyinvestigated markers in this category of tumors are
similar to their patterns in the normal adult oviduct.The absence of PLAP in mucinous ovarian tumorscontrasts with its expression in endocervical gobletcells.6'30 It supports, however, the concept that vir-tually all malignant mucinous ovarian tumors are ofthe colonic, instead ofthe endocervical, type.28'29 Theabsence of PLAP in the normal endometrial glandu-lar epithelium has also been demonstrated previously
by heat-inactivation experiments," but the fact thatendometrial glandulocystic hyperplasia is frequentlyassociated with PLAP expression (unpublished ob-servations) again illustrates that also this mullerianepithelium possesses, like the ovarian surface epithe-lium, the capability to express PLAP under certainconditions. As a result, the expression of PLAP bydifferent ovarian constituents after malignant trans-formation has a double embryonic basis, ie, a ger-minal-mullerian epithelial origin and probably also agerm cell origin.
Figure 8-Moderately well to poorly differentiated papillary serous adenocarcinoma (Tumor 15). A-PLAP staining (antibody 17E3). B-HMFG 2staining. C-HMFG 1 staining. (A- C, adjacent sections, X 105) Figure 9-Poorly differentiated adenocarcinoma (Tumor 30). A-Homogeneouscytoplasmic HMFG 2 staining. B-CA 19-9 staining in isolated or clustered cells. (A and B, adjacent sections, X131) Figure 10-Well-differentiatedendometrioid carcinoma (Tumor 22). A-PLAP staining (antibody 17E3). B-HMFG 1 staining. C-CA 19-9 staining. (A-C, adjacent sections,X105)
Vol. 126 * No. 2
.
I
;
240 NOUWEN ET AL
The use of three different monoclonal antibodiesfor the localization ofPLAP in tissue sections ofovar-ian neoplasms results in virtually identical stainingpatterns, probably because they all react to some ex-tent with different variants of PLAP, despite distinctdifferences in binding affinity in particular for L-leu-cine-sensitive PLAP. In some tumors, however, sig-nificant differences were observed in the PLAP stain-ing intensity obtained with different antibodies, inspite of an identical histologic distribution of thestaining. Some ofthese differences are due to the nor-mal phenotypic diversity of PLAP, but other factorsmay also play a role. As demonstrated previously byheat inactivation, L-p-bromotetramisole inhibition,electrophoretic, and immunochemical evidence,4 theaffinity ofsome antibodies for certain ovarian cancerassociated forms ofPLAP is decreased.
In all tumors PLAP staining is predominantlymembranous and in general heterogenously distrib-uted, ranging from very scarce to uniform. The obser-vation that the immunohistochemical patterns forPLAP for all antibodies are qualitatively similar to thepatterns for NSAP in the presence ofL-p-bromotetra-misole, although the two methods are based on totallydifferent biochemical principles, proves that the ob-served heterogeneous distribution patterns ofPLAP,as also reported by others using other monoclonalsand/or different histologic processing protocols (eg,cryostat sections),6'7 are not due to methodologic fac-tors, but reflect the real distribution ofPLAP. There-fore, although a cocktail of monoclonal antibodiesmay compensate to some extent for the biochemicalheterogeneity of PLAP in ovarian neoplasms, it willnot be able to remediate the histologic heterogeneityof the PLAP expression. This heterogeneity occursalso in the normal PLAP-producing tissues, eg, thelung'9 and oviduct,3' confirming that antigenic het-erogeneity is not just a property of tumors, but of awide range of normal epithelia,3 and that the expres-sion ofPLAP is restricted to certain stages in the cellcycle32 and/or to certain types of cellular differentia-tion. The observation that well-differentiated papil-lary serous (cyst)adenocarcinomas have a slightlyhigher PLAP expression than the rather poorly differ-entiated tumors of this group is a further illustrationofthis. In comparison, CA 125 expression seems to beassociated with a broader spectrum of cellular differ-entiation, because unlike PLAP, it is produced byundifferentiated normal adult and fetal mesothelialcells and by their more or less specialized descend-ants. Furthermore, all these epithelia are quite homo-geneous in the expression ofCA 125. The same is truefor HMFG, which is expressed by many different nor-mal epithelia.33 It is therefore not surprising that most
ovarian tumors investigated are nearly homogeneousin the expression ofCA 125 and HMFG. The noni-dentity of CA 125 and HMFG is indicated by occa-sional discordances in their occurrence, by the morecytoplasmic character of HMFG 2, and by theirstrongly different distribution patterns in othertumors and various normal tissues.
In our study, the frequency ofCA 125 positivity indifferent tumor types was even higher than reportedby others. 10'34'35 The only PLAP-positive tumor lack-ing CA 125 and HMFG was a dysgerminoma, herebyillustrating its different embryonic origin. Althoughthe existence ofa mucinous substance containing theCA 125 as well as the CA 19-9 determinant has beendescribed,24 and although CA 125 immunoreactivityhas also been observed in goblet cells of the normalrespiratory airways and respiratory mucoserousglands,'9 such a mucinous substance apparently is notpresent in the ten mucinous tumors investigated here.The presence ofCA 125 in normal endocervical mu-cosa and its absence in mucinous tumors and normalcolonic mucosa again supports the colonic type ofdifferentiation of these tumors. This concept is alsoconfirmed by their frequent CEA expression.According to our results, CA 19-9 is detectable in
82% of mucinous tumors, but also in 55% of serousand other nonmucinous ovarian carcinomas. Its his-tochemical distribution was in nearly all cases veryheterogeneous and often scarce. Differences betweenour results and available data indicating that CA 19-9expression in ovarian cancer is principally a propertyof mucinous tumors34'35 may be due to differences intissue processing methods.Our staining results for CEA are intermediate be-
tween available data mostly obtained with polyclonalantisera.36-38 Because CEA belongs to a group ofclosely related substances,3940 differences in CEAstaining results are at least partially due to differencesin the specificity of the antibodies. The low degree ofCEA expression in epithelial ovarian neoplasms isconsistent with its absence in germinal inclusion cystsand in normal mullerian duct-derived epithelia.
Since each ofthe six antigens is detectable in severaltypes of benign and malignant ovarian tumors, im-muno(histo)chemical analysis for the presence ofthese antigens is of no use of a differential diagnosisbut may be valuable for evaluating the opportunenessof diagnostic or therapeutic immunotargeting. Thereis also no apparent relation between the expressionand histologic distribution ofthe six antigens studied,which results in a partial complementarity and over-lapping. Ofthe six presently investigated tumor-asso-ciated antigens, PLAP has the most limited expres-sion in normal tissues. 19,23,33,41
AJP * February 1987

Vol. 126 * No. 2 TUMOR MARKERS IN THE OVARY 241
In conclusion, because a substantial number ofovarian carcinomas contain an important number ofPLAP-expressing malignant cells, because PLAP ispredominantly localized on the surface of these cellsand because most normal tissues are negative, PLAPmay be useful as a tumor marker for ovarian cancer.The frequent expression of PLAP by ovarian neo-plasms has a double embryonic basis, ie, a mullerianepithelial and probably a germ-cell one. Differentmonoclonal antibodies against PLAP are unable toovercome the histologic heterogeneity of the PLAPexpression. This should be taken into account whenone is planning PLAP-targeted immunotherapy ofovarian cancer; and, in view of the observation thatthe expression ofthe presently investigated markers islargely independent, combination of anti-PLAPmonoclonals with antibodies against other specificmarkers should be considered.
References1. Hockey MS, Stokes HJ, Woodhouse CS, Macdonald F,
Fielding JW, Ford CH: Carcinoembryonic antigen(CEA) expression and heterogeneity in primary andautologous metastatic gastric tumours demonstratedby a monoclonal antibody. Br J Cancer 1984, 49:129 -133
2. Hernandez E, Rosenheim NB, Bhagavan BS, ParmleyTH: Tumor heterogeneity and histopathology in epi-thelial ovarian cancer. Obstet Gynecol 1984, 63:330-334
3. Edwards PAW: Heterogenous expression of cell-sur-face antigens in normal epithelia and their tumours,revealed by monoclonal antibodies. Br J Cancer 1985,51:149- 160
4. Nouwen EJ, Pollet DE, Schelstraete JB, EerdekensMW, Hansch C, Van de Voorde A, De Broe ME:Human placental alkaline phosphatase in benign andmalignant ovarian neoplasia. Cancer Res 1985,45:892-902
5. Miller FR: Intratumor imunologic heterogeneity.Cancer Metast Rev 1982, 1:319-334
6. Sunderland CA, Davies JO, Stirrat GM: Immunohisto-logy of normal and ovarian cancer tissue with a mono-clonal antibody to placental alkaline phosphatase.Cancer Res 1984, 44:4496 -4502
7. McDicken IW, McLaughlin PJ, Tromans PM, LuesleyDM, Johnson PM: Detection ofplacental-type alkalinephosphatase in ovarian cancer. Br J Cancer 1985,52:59-64
8. Epenetos AA, Mather S, Granowska M, Nimmon CC,Hawkins LR, Britton KE, Shepherd J, Taylor-Papadi-mitriou J, Durbin H, Malpas JS: Targeting of iodine-123-labelled tumour-associated monoclonal antibod-ies to ovarian, breast, and gastrointestinal tumours.Lancet 1982, 2:999 - 1004
9. Bast RC, Feeney M, Lazarus H, Nadler LM, ColvinRB, Knapp RC: Reactivity of a monoclonal antibodywith human ovarian carcinoma. Am Soc Clin Invest1981, 68:1331 - 1336
10. Kabawat SE, Bast RC, Welch WR, Knapp RC, ColvinRB: Immunopathologic characterization of a mono-clonal antibody that recognizes common surface anti-gens of human ovarian tumors of serous, endome-
trioid, and clear cell types. Am J Clin Pathol 1983,79:98-104
11. Koprowski H, Steplewski Z, Mitchell K, Herlyn M,Herlyn D, Fuhrer P: Colorectal carcinoma antigens de-tected by hybridoma antibodies. Somatic Cell Genet1979, 5:957-972
12. Magnani JL, Nilsson B, Brockhaus M, Zopf D, Ste-plewski Z, Koprowski H, Ginsburg V: A monoclonalantibody-defined antigen associated with gastrointesti-nal cancer is a ganglioside containing sialylated lacto-N-fucopentaose II. J Biol Chem 1982, 257:365-369
13. Falk KE, Karlsson KA, Larson G, Thurin J, BlaszczykM, Steplewski Z, Koprowski H: Mass spectrometry ofahuman tumor glycolipid antigen being defined bymouse monoclonal antibody NS- 19-9. BiochemBiophys Res Commun 1983, 100:383- 391
14. Hendrix PG, Nouwen EJ, Briers TW, Martens E, PolletDE, De Broe ME: Biochemical and immunochemicalanalysis ofthe molecular heterogeneity ofplacental al-kaline phosphatase from tumor cells. (Manuscript inpreparation)
15. De Groote G, De Waele P, Van de Voorde A, De BroeME, Fiers W: Use of monoclonal antibodies to detecthuman placental alkaline phosphatase. Clin Chem1983, 29:115-119
16. Travers PJ, Bodmer WF: Preparation and characterisa-tion of monoclonal antibodies against placental alka-line phosphatase and other trophoblast associated de-terminants. Int J Cancer 1984, 33:633 - 641
17. Taylor-Papadimitriou J, Peterson JA, Arklie J, Bur-chell J, Ceriani RL, Bodmer WF: Monoclonal antibod-ies to epithelium-specific components of the humanmilk fat globule membrane: Production and reactionwith cells in culture. Int J Cancer 1981, 28:17-21
18. Gossrau R: Azoindoxylverfahren zum hydrolasen-nachweis: IV. Zur eignung verschiedener diazolium-salze. Histochemie 1978, 57:323-342
19. Nouwen EJ, Pollet DE, Eerdekens MW, Hendrix PG,Briers TW, De Broe ME: Immunohistochemical locali-zation of placental alkaline phosphatase, carcinoem-bryonic antigen and cancer antigen 125 in normal andneoplastic human lung. Cancer Res 1986, 46:866 - 876
20. Van Belle H, De Broe ME, Wieme J: L-p-bromotetra-misole, a new reagent for use in measuring placental orintestinal isoenzymes of alkaline phosphatase inhuman serum. Clin Chem 1977, 23:454-459
21. Eerdekens MW, Nouwen EJ, Pollet DE, Briers TW, DeBroe ME: Human placental alkaline phosphatase andcancer antigen 125 in sera of patients with benign andmalignant diseases. Clin Chem 1985, 31:687 - 690
22. Pollet DE, Nouwen EJ, Schelstraete JB, Renard J,Van de Voorde A, DeBroe ME: Enzyme-antigen im-munoassay to human placental alkaline phosphatase inserum and tissue extracs, and its application as a tumormarker. Clin Chem 1985, 31:41-45
23. De Broe ME, Nouwen EJ, Pollet DE, Eerdekens MW,Briers TW, Hendrix PG: Human placental alkalinephosphatase as a tumour marker. Adv Clin Enzymol1986, 3:39-52
24. Bast RC, Knapp RC: CA 125 antigen for diagnosis andmonitoring of epithelial ovarian carcinoma. Proceed-ings of the international meeting on Monoclonal Anti-bodies in Oncology: Clinical Applications. Nantes,June 1984. Edited by JF Chatal, M Douis. NouvellesEditions Medicales Franqaises, 1984, pp 35-38
25. Paiva J, Damjanov I, Lange PH, Harris H: Immuno-histochemical localization of placental-like alkalinephosphatase in testis and germ-cell tumors usingmonoclonal antibodies. Am J Pathol 1983, 111:156 -165
26. Epenetos AA, Travers P, Gatter KC, Oliver RDT,Mason DY, Bodmer WF: An immunohistological

242 NOUWEN ET AL AJP * February 1987
study of testicular germ cell tumours using two differ-ent monoclonal antibodies against placental alkalinephosphatase. Br J Cancer 1984, 49:11 - 15
27. Shinoda J, Miwa Y, Sakai N, Yamada H, Shima H,Kato K, Takahashi M, Shimokawa K: Immunohisto-chemical study of placental alkaline phosphatase inprimary intracranial germ-cell tumors. J Neurosurg1985, 63:733-739
28. Dallenbach-Hellweg G: On the histogenesis and mor-phology of ovarian carcinomas. J Cancer Res ClinOncol 1984, 107:71-80
29. Russell P: Common epithelial tumours ofthe ovary: Anew look. Pathology 1984, 17:555 - 557
30. Goldstein DJ, Blasco L, Harris H: Placental alkalinephosphatase in nonmalignant human cervix. Proc NatlAcad Sci USA 1980, 77:4226-4228
31. Van de Voorde A, Serreyn R, De Boever J, De Waele P,Vandekerckhove D, Fiers W: The occurrence ofhuman placental alkaline phosphatase (PLAP) in ex-tracts of normal, benign, and malign tissues of the fe-male genital tract. Tumour Biol 1985, 6:545-553
32. Fishman WH: Oncotrophoblast gene expression: Pla-cental alkaline phosphatase. Adv Cancer Res (In press)
33. Arklie J, Taylor-Papadimitriou J, Bodmer W, Egan M,Millis R: Differentiation antigens expressed by epithe-lial cells in the lactating breast are also detectable inbreast cancers. Int J Cancer 1981, 28:23-29
34. Kremer M, Chatal JF, Curtet C, Douillard JY: Theimmunohistochemical reactivity of monoclonal anti-bodies with tissue sections of human ovarian tumors,Proceedings of the Eleventh Annual Meeting of theInternational Society for Oncodevelopmental Biologyand Medicine, Stockholm, Sweden, September 1983
35. Kremer M: Diagnostic immunohistochimique des tu-meurs ovariennes avec 1' anticorps monoclonal OC125,24 pp 39-41
36. Van Nagell JR, Donaldson ES, Gay EC, Sharkey RM,Rayburn P, Goldenberg DM: Carcinoembryonic anti-gen in ovarian epithelial cystadenocarcinomas: Theprognostic value oftumor and serial plasma determina-tions. Cancer 1978, 41:2335 - 2340
37. Heald J, Buckley CH, Fox H: An immunohistochemi-
cal study of the distribution ofcarcinoembryonic anti-gen in epithelial tumours of the ovary. J Clin Pathol1979, 32:918-926
38. Malkin A, Kellen JA, Lickrish GM, Bush RS: Carcin-oembryonic antigen (CEA) and othertumor markers inovarian and cervical cancer. Cancer 1978, 42:1452-1456
39. Kuroki M, Koga Y, Matsuoka Y: Monoclonal antibod-ies to carcinoembryonic antigen: a systematic analysisof antibody specificities by using related normal anti-gens and evidence for allotypic determinants on carcin-oembryonic antigen. J Immunol 1984, 133:2090-2097
40. Yachi A, Imai K, Fujita H, Moriya Y, Tanda M, EndoT, Tsujisaki M, Kawaharada M: Immunohistochemi-cal distribution of the antigenic determinants detectedby monoclonal antibodes to carcinoembryonic anti-gen. J Immunol 1984, 132:1998-2004
41. Atkinson BF, Ernst CS, Herlyn M, Steplewski Z, SearsHF, Koprowski H: Gastrointestinal cancer associatedantigen in immunoperoxidase assay. Cancer Res 1982,42:4820-4823
AcknowledgmentsWe wish to thank Dr. Andre Van de Voorde (Depart-
ment of Molecular Biology, State University ofGhent, Bel-gium) for providing us the monoclonal antibody E6, Dr.Robert C. Bast (Department ofMedicine, Duke UniversityMedical Center, Durham, NC) for the batch of antibodyOC 125, Dr. Hilary Koprowski (The Wistar Institute, Phila-delphia, Pa) for the batch ofmonoclonal antibody 1116 NS19-9, Dr. Joyce Taylor-Papadimitriou (Imperial CancerResearch Fund, London, UK) for the batches of antibodyHMFG 1 and HMFG 2, and Drs. P. J. Den Houwdyker, J.Renard, L. Delbeke, P. Buytaert, F. Uytenbroeck, I. DeWever, and J. Claeys for providing some ofthe biopsy speci-mens. The technical assistance of R. Marynissen was grate-fully acknowledged.