a cognitive/behavioral group intervention for weight loss in patients treated with atypical...
TRANSCRIPT
www.elsevier.com/locate/schres
Schizophrenia Research
A cognitive/behavioral group intervention for weight loss in
patients treated with atypical antipsychotics
Mary Weber a,*, Kathleen Wyne b
a School of Nursing, The University of Texas at Arlington, 411 S. Nedderman Dr. Box 19407 Arlington, TX 76019-0407, United Statesb Division of Endocrinology and Metabolism, Department of Internal Medicine, University of Texas Southwestern Medical Center at Dallas,
United States
Received 8 July 2005; received in revised form 9 January 2006; accepted 17 January 2006
Available online 28 February 2006
Abstract
Obesity and diabetes have caused problems for individuals with schizophrenia long before atypical antipsychotic agents.
The prevalence of obesity, insulin resistance, impaired glucose tolerance, type 2 diabetes mellitus, dyslipidemia, and the
Metabolic Syndrome has increased in people with schizophrenia as compared to the general population. Risk reduction studies
for persons with obesity, diabetes, and cardiovascular disease indicate that cognitive/behavioral interventions that promote
motivation and provide strategies to overcome the barriers in adherence to diet and activity modification are effective
interventions for weight management and risk reduction. In the landmark multi-center randomized-controlled trial study, the
Diabetes Prevention Project (DPP), a cognitive/behavioral intervention, was more successful in producing weight loss and
preventing diabetes than the drugs metformin, troglitazone or placebo. This pilot study examined the effectiveness of a
cognitive/behavioral group intervention, modified after the DPP program, in individuals with schizophrenia or schizoaffective
disorder taking atypical antipsychotics in a large urban public mental health system. Outcome measures included body weight,
body mass index, waist–hip ratios, and fasting glucose levels. Both groups demonstrated elevated fasting glucose levels and
were obese with a mean BMI of 33. The group that received the cognitive/behavioral group intervention lost more weight than
the treatment as usual group. The CB group participants lost an average of 5.4lb or 2.9% of body weight, and those in the
control group lost 1.3lb or 0.6% body weight. The range of weight loss for the treatment group was from 1 to 20lb. This pilot
study has demonstrated that weight loss is possible with cognitive/behavioral interventions in a population with a psychotic
disorder.
D 2006 Elsevier B.V. All rights reserved.
Keywords: Cognitive/behavioral intervention; Weight loss; Atypical antipsychotics; Schizophrenia
0920-9964/$ - see front matter D 2006 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2006.01.008
* Corresponding author. Tel.: +1 817 272 2776; fax: +1 817 272
5006.
E-mail address: [email protected] (M. Weber).
1. Introduction
Weight gain is a serious health concern for
individuals with schizophrenia. It increases their mor-
83 (2006) 95–101

M. Weber, K. Wyne / Schizophrenia Research 83 (2006) 95–10196
bidity and serves as an additional reason for non-
adherence with pharmacologic treatment (Green et al.,
2000; Perkins, 2002; Weiden et al., 1996). It is
estimated that 40% to 60% of persons with schizo-
phrenia are obese as compared to 20% prevalence in the
general US adult population (Green et al., 2000). Thus,
it is not surprising that the prevalence of insulin
resistance, impaired glucose tolerance, type 2 diabetes
mellitus, and the MS has increased in people with
schizophrenia as compared to the general population
(Henderson et al., 2000). The recent introduction of
new pharmacologic therapies for the treatment of
schizophrenia, which are commonly referred to as the
datypical antipsychoticsT has been correlated with a
further increase in the prevalence of excess body
weight and type 2 diabetes in this population (Allison
and Casey, 2001; Allison et al., 1999). In one of the few
descriptive studies examining the health of those with
schizophrenia, Brown and colleagues reported in
1999 that on average, individuals with schizophrenia
eat a diet high in fat, smoke heavily, and get very little
exercise. In addition to obesity, individuals with
schizophrenia appear to have increased visceral fat,
regardless of drug treatment, which is highly correlated
with insulin resistance and risk of diabetes (Thakore
et al., 2002).
In a recent epidemiological study, as little as a 5%
increase in body weight is correlated with a 200%
greater risk of developing this metabolic or insulin
resistance syndrome by middle age (Everson et al.,
1998). Thus, individuals with schizophrenia, already
overweight, significantly increase their chances of
significant co-morbidity with as little as a 5% weight
gain. Data to support prevention of weight gain and
appropriate choices of antipsychotic medications has
become a public health priority. Risk reduction
studies for persons with obesity, diabetes, and
cardiovascular disease indicate that cognitive/behav-
ioral interventions that promote motivation and
provide strategies to overcome the barriers in
adherence to diet and activity modification are
effective interventions for weight management and
risk reduction (Nawaz and Katz, 2001; Williamson
and Perrin, 1996).
In the landmark multi-center Diabetes Prevention
Project (DPP), a cognitive/behavioral lifestyle inter-
vention was more successful in producing weight loss
and preventing diabetes than the drug metformin
(Knowler et al., 2002). The group that received
troglitazone actually had the lowest diabetes incidence
in the first year but they only received the drug for the
first 9 months and this benefit was not sustained over
the three years of the trial (Knowler et al., 2005). The
intensive lifestyle intervention in the DPP was found
to decrease the incidence of diabetes by 58% in high-
risk populations. Further, the investigators found that
the randomized clinical data collected from 27 clinical
sites throughout the country, showed that intensive
cognitive/behavioral therapies that focused on modi-
fying diet and increasing activity were just as effective
for both men and women, in all age groups, and in all
ethnic groups.
Weight reduction studies in the population with
schizophrenia have been cited in the literature but
results are mixed and none have used a randomized-
control model. This pilot study examined the effective-
ness of a randomized-control group design cognitive/
behavioral group intervention based on the DPP
lifestyle intervention in those individuals who were
taking atypical antipsychotics for schizophrenia or
schizoaffective disorder in a large urban public mental
health clinic system. It was hypothesized that those
individuals completing the 16-week program would
demonstrate significantly different weight, body mass
index (BMI), waist–hip ratio (WHR), and fasting
glucose levels than those in the treatment as usual
(TAU) group.
2. Methods
2.1. Sample
A randomized, placebo-controlled design was
chosen for this pilot study to test the efficacy of this
group intervention. The sample was recruited over
approximately one month from over 900 patients per
month attending a large urban public mental health
clinic in Dallas. The PI used flyers in the clinic as
well as working with the case managers and medical
providers to recruit over 30 potential subjects. The
first seventeen subjects who qualified and were
interested in participating were randomized to the
16-week cognitive/behavioral (CB) group interven-
tion or treatment as usual (TAU) care. The inclusion
criteria included subjects diagnosed by the Diagnostic
M. Weber, K. Wyne / Schizophrenia Research 83 (2006) 95–101 97
Statistical Manual 4-TR (DSM) criteria for schizo-
phrenia or schizoaffective disorder, taking only one
oral atypical antipsychotic, between the ages of 18
and 65 years old, and have a BMI equal to or greater
than 25. Patients were excluded if they were acutely
psychotic, in need of immediate detoxification, or
alcohol dependent. The study consisted of 17 patients,
12 females and 5 males. There were 9 Afro-American
subjects, 3 Hispanic (English speaking), and 5 Cau-
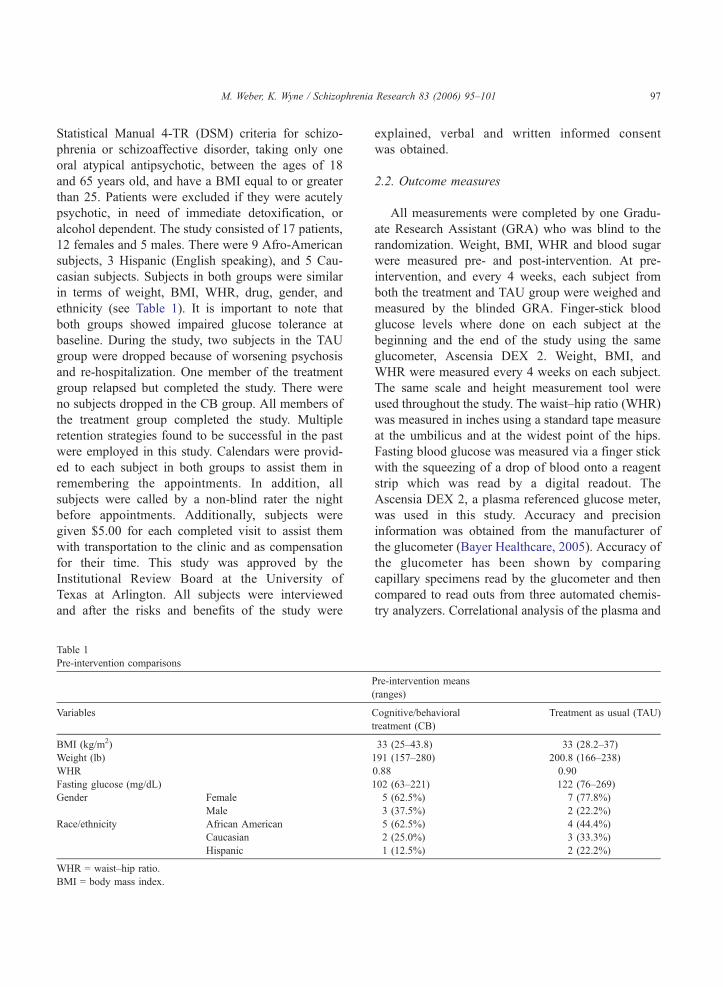
casian subjects. Subjects in both groups were similar
in terms of weight, BMI, WHR, drug, gender, and
ethnicity (see Table 1). It is important to note that
both groups showed impaired glucose tolerance at
baseline. During the study, two subjects in the TAU
group were dropped because of worsening psychosis
and re-hospitalization. One member of the treatment
group relapsed but completed the study. There were
no subjects dropped in the CB group. All members of
the treatment group completed the study. Multiple
retention strategies found to be successful in the past
were employed in this study. Calendars were provid-
ed to each subject in both groups to assist them in
remembering the appointments. In addition, all
subjects were called by a non-blind rater the night
before appointments. Additionally, subjects were
given $5.00 for each completed visit to assist them
with transportation to the clinic and as compensation
for their time. This study was approved by the
Institutional Review Board at the University of
Texas at Arlington. All subjects were interviewed
and after the risks and benefits of the study were
Table 1
Pre-intervention comparisons
Variables
BMI (kg/m2)
Weight (lb)
WHR
Fasting glucose (mg/dL)
Gender Female
Male
Race/ethnicity African American
Caucasian
Hispanic
WHR = waist–hip ratio.
BMI = body mass index.
explained, verbal and written informed consent
was obtained.
2.2. Outcome measures
All measurements were completed by one Gradu-
ate Research Assistant (GRA) who was blind to the
randomization. Weight, BMI, WHR and blood sugar
were measured pre- and post-intervention. At pre-
intervention, and every 4 weeks, each subject from
both the treatment and TAU group were weighed and
measured by the blinded GRA. Finger-stick blood
glucose levels where done on each subject at the
beginning and the end of the study using the same
glucometer, Ascensia DEX 2. Weight, BMI, and
WHR were measured every 4 weeks on each subject.
The same scale and height measurement tool were
used throughout the study. The waist–hip ratio (WHR)
was measured in inches using a standard tape measure
at the umbilicus and at the widest point of the hips.
Fasting blood glucose was measured via a finger stick
with the squeezing of a drop of blood onto a reagent
strip which was read by a digital readout. The
Ascensia DEX 2, a plasma referenced glucose meter,
was used in this study. Accuracy and precision
information was obtained from the manufacturer of
the glucometer (Bayer Healthcare, 2005). Accuracy of
the glucometer has been shown by comparing
capillary specimens read by the glucometer and then
compared to read outs from three automated chemis-
try analyzers. Correlational analysis of the plasma and
Pre-intervention means
(ranges)
Cognitive/behavioral
treatment (CB)
Treatment as usual (TAU)
33 (25–43.8) 33 (28.2–37)
191 (157–280) 200.8 (166–238)
0.88 0.90
102 (63–221) 122 (76–269)
5 (62.5%) 7 (77.8%)
3 (37.5%) 2 (22.2%)
5 (62.5%) 4 (44.4%)
2 (25.0%) 3 (33.3%)
1 (12.5%) 2 (22.2%)
M. Weber, K. Wyne / Schizophrenia Research 83 (2006) 95–10198
Ascensia DEX 2 readings produced a correlation
coefficient of r =0.98. Precision of the Ascensia DEX
2 was determined by testing whole blood pools
supplemented with glucose to obtain five glucose
levels. Precision results using test solutions ranged
from a standard deviation at 2.7 to 5.7 with a
confidence value (CV) of 1.5% to 3.5%. According
to the American Diabetic Association (ADA, 1996),
error of meters designed for self monitoring and point
of care testing of glucose should not exceed 5%. After
reviewing these values, the Ascensia DEX 2 was
determined to be an accurate and precise measurement
of glucose for this study.
2.3. Treatment intervention
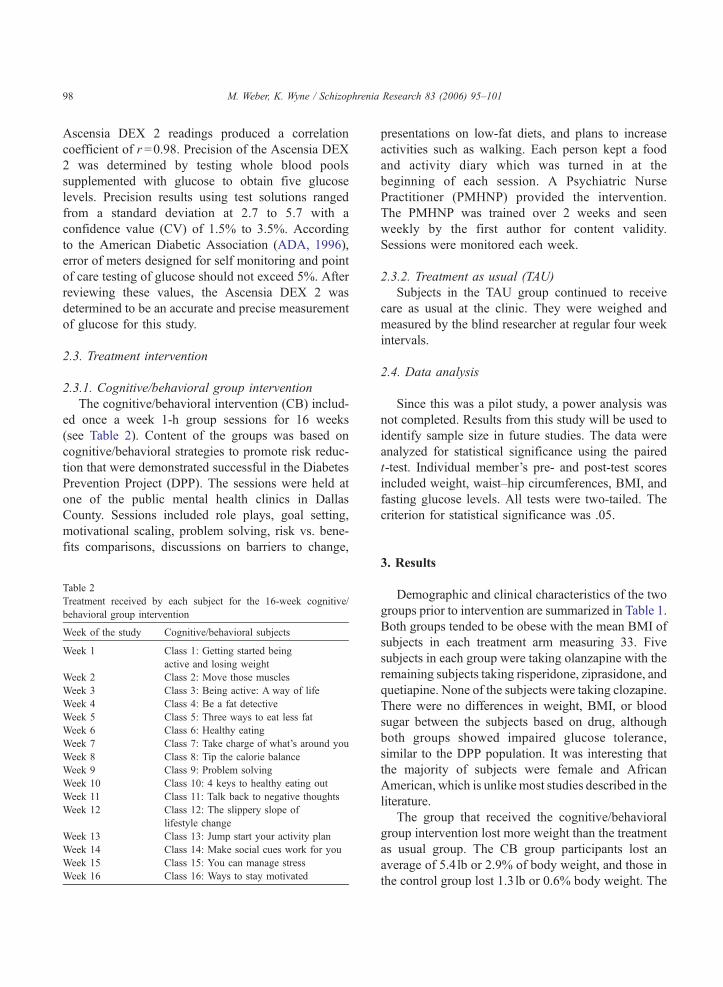
2.3.1. Cognitive/behavioral group intervention
The cognitive/behavioral intervention (CB) includ-
ed once a week 1-h group sessions for 16 weeks
(see Table 2). Content of the groups was based on
cognitive/behavioral strategies to promote risk reduc-
tion that were demonstrated successful in the Diabetes
Prevention Project (DPP). The sessions were held at
one of the public mental health clinics in Dallas
County. Sessions included role plays, goal setting,
motivational scaling, problem solving, risk vs. bene-
fits comparisons, discussions on barriers to change,
Table 2
Treatment received by each subject for the 16-week cognitive/
behavioral group intervention
Week of the study Cognitive/behavioral subjects
Week 1 Class 1: Getting started being
active and losing weight
Week 2 Class 2: Move those muscles
Week 3 Class 3: Being active: A way of life
Week 4 Class 4: Be a fat detective
Week 5 Class 5: Three ways to eat less fat
Week 6 Class 6: Healthy eating
Week 7 Class 7: Take charge of what’s around you
Week 8 Class 8: Tip the calorie balance
Week 9 Class 9: Problem solving
Week 10 Class 10: 4 keys to healthy eating out
Week 11 Class 11: Talk back to negative thoughts
Week 12 Class 12: The slippery slope of
lifestyle change
Week 13 Class 13: Jump start your activity plan
Week 14 Class 14: Make social cues work for you
Week 15 Class 15: You can manage stress
Week 16 Class 16: Ways to stay motivated
presentations on low-fat diets, and plans to increase
activities such as walking. Each person kept a food
and activity diary which was turned in at the
beginning of each session. A Psychiatric Nurse
Practitioner (PMHNP) provided the intervention.
The PMHNP was trained over 2 weeks and seen
weekly by the first author for content validity.
Sessions were monitored each week.
2.3.2. Treatment as usual (TAU)
Subjects in the TAU group continued to receive
care as usual at the clinic. They were weighed and
measured by the blind researcher at regular four week
intervals.
2.4. Data analysis
Since this was a pilot study, a power analysis was
not completed. Results from this study will be used to
identify sample size in future studies. The data were
analyzed for statistical significance using the paired
t-test. Individual member’s pre- and post-test scores
included weight, waist–hip circumferences, BMI, and
fasting glucose levels. All tests were two-tailed. The
criterion for statistical significance was .05.
3. Results
Demographic and clinical characteristics of the two
groups prior to intervention are summarized in Table 1.
Both groups tended to be obese with the mean BMI of
subjects in each treatment arm measuring 33. Five
subjects in each group were taking olanzapine with the
remaining subjects taking risperidone, ziprasidone, and
quetiapine. None of the subjects were taking clozapine.
There were no differences in weight, BMI, or blood
sugar between the subjects based on drug, although
both groups showed impaired glucose tolerance,
similar to the DPP population. It was interesting that
the majority of subjects were female and African
American, which is unlike most studies described in the
literature.
The group that received the cognitive/behavioral
group intervention lost more weight than the treatment
as usual group. The CB group participants lost an
average of 5.4lb or 2.9% of body weight, and those in
the control group lost 1.3 lb or 0.6% body weight. The
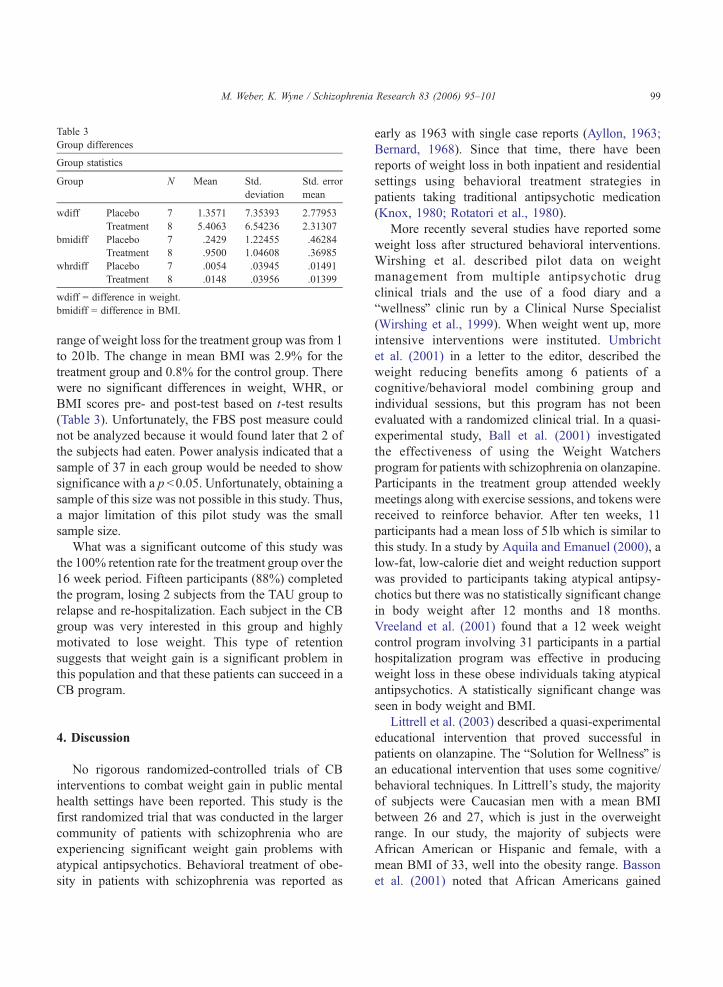
Table 3
Group differences
Group statistics
Group N Mean Std.
deviation
Std. error
mean
wdiff Placebo 7 1.3571 7.35393 2.77953
Treatment 8 5.4063 6.54236 2.31307
bmidiff Placebo 7 .2429 1.22455 .46284
Treatment 8 .9500 1.04608 .36985
whrdiff Placebo 7 � .0054 .03945 .01491
Treatment 8 .0148 .03956 .01399
wdiff = difference in weight.
bmidiff = difference in BMI.
M. Weber, K. Wyne / Schizophrenia Research 83 (2006) 95–101 99
range of weight loss for the treatment group was from 1
to 20lb. The change in mean BMI was 2.9% for the
treatment group and 0.8% for the control group. There
were no significant differences in weight, WHR, or
BMI scores pre- and post-test based on t-test results
(Table 3). Unfortunately, the FBS post measure could
not be analyzed because it would found later that 2 of
the subjects had eaten. Power analysis indicated that a
sample of 37 in each group would be needed to show
significance with a p b0.05. Unfortunately, obtaining a
sample of this size was not possible in this study. Thus,
a major limitation of this pilot study was the small
sample size.
What was a significant outcome of this study was
the 100% retention rate for the treatment group over the
16 week period. Fifteen participants (88%) completed
the program, losing 2 subjects from the TAU group to
relapse and re-hospitalization. Each subject in the CB
group was very interested in this group and highly
motivated to lose weight. This type of retention
suggests that weight gain is a significant problem in
this population and that these patients can succeed in a
CB program.
4. Discussion
No rigorous randomized-controlled trials of CB
interventions to combat weight gain in public mental
health settings have been reported. This study is the
first randomized trial that was conducted in the larger
community of patients with schizophrenia who are
experiencing significant weight gain problems with
atypical antipsychotics. Behavioral treatment of obe-
sity in patients with schizophrenia was reported as
early as 1963 with single case reports (Ayllon, 1963;
Bernard, 1968). Since that time, there have been
reports of weight loss in both inpatient and residential
settings using behavioral treatment strategies in
patients taking traditional antipsychotic medication
(Knox, 1980; Rotatori et al., 1980).
More recently several studies have reported some
weight loss after structured behavioral interventions.
Wirshing et al. described pilot data on weight
management from multiple antipsychotic drug
clinical trials and the use of a food diary and a
bwellnessQ clinic run by a Clinical Nurse Specialist
(Wirshing et al., 1999). When weight went up, more
intensive interventions were instituted. Umbricht
et al. (2001) in a letter to the editor, described the
weight reducing benefits among 6 patients of a
cognitive/behavioral model combining group and
individual sessions, but this program has not been
evaluated with a randomized clinical trial. In a quasi-
experimental study, Ball et al. (2001) investigated
the effectiveness of using the Weight Watchers
program for patients with schizophrenia on olanzapine.
Participants in the treatment group attended weekly
meetings along with exercise sessions, and tokens were
received to reinforce behavior. After ten weeks, 11
participants had a mean loss of 5lb which is similar to
this study. In a study by Aquila and Emanuel (2000), a
low-fat, low-calorie diet and weight reduction support
was provided to participants taking atypical antipsy-
chotics but there was no statistically significant change
in body weight after 12 months and 18 months.
Vreeland et al. (2001) found that a 12 week weight
control program involving 31 participants in a partial
hospitalization program was effective in producing
weight loss in these obese individuals taking atypical
antipsychotics. A statistically significant change was
seen in body weight and BMI.
Littrell et al. (2003) described a quasi-experimental
educational intervention that proved successful in
patients on olanzapine. The bSolution for WellnessQ isan educational intervention that uses some cognitive/
behavioral techniques. In Littrell’s study, the majority
of subjects were Caucasian men with a mean BMI
between 26 and 27, which is just in the overweight
range. In our study, the majority of subjects were
African American or Hispanic and female, with a
mean BMI of 33, well into the obesity range. Basson
et al. (2001) noted that African Americans gained

M. Weber, K. Wyne / Schizophrenia Research 83 (2006) 95–101100
more weight with the atypical antipsychotics, and we
found that many Caucasian men in our clinics did not
meet the inclusion criteria of a BMI of 25 or greater,
thus demonstrating the significant problem of weight
gain in the African American and Hispanic population
with schizophrenia in this large urban public mental
health system.
It was very interesting that both groups did not show
weight gain, which would be expected in this popula-
tion, especially with the trend in this population to
continue to gain weight each month. Perhaps even a
simple intervention of bweighing-inQ may prove to
have some benefit. It is clear that although not
statistically significant, weight loss of any kind for this
population has clinical significance and thus is an
important finding. We attribute our lack of statistical
significance to several factors besides the sample size
itself. Unfortunately t-tests with such small means are
not powerful enough to pick up individual differences
in weight loss or changes in waist–hip ratios, as
evidenced by our power analysis. In addition, there
are multiple factors involved in weight loss treatment,
including issues such as motivation, money, transpor-
tation, and availability of healthy foods and activity.
The subjects felt their biggest obstacles to weight loss
were a high crime rate, lack of transportation options,
and low income. Transportation and availability of
healthy foods or activities became significant
obstacles. Fast foods are the most common diet of this
population, and we had to develop creative tools in
helping them to choose the bleast harmfulQ of options.Strategies employed included getting sample menus
from restaurants to discuss, going on walks around the
clinic and local parks, using pedometers and exercise
videos, teaching weight lifting exercises utilizing soup
cans, and discussing types of frozen meals that fit into a
low-calorie diet. It was also interesting that subjects
bforgotQ that they ate the morning of the study and
revealed it later in the day. Obtaining accurate measures
is a challenge in this population.
The Diabetes Prevention Project, which focused on
the prevention of diabetes in individuals with impaired
glucose, was used as a model for this study. It is
noteworthy that both TAU group and treatment group
had evidence of impaired glucose tolerance prior to the
beginning of this study, although only two subjects had
a diagnosis of type 2 diabetes. Impaired glucose
tolerance is a significant and unfortunately a growing
problem in this population with schizophrenia. This
study reinforces the importance of intensive lifestyle
interventions which may also prove to reduce the
incidence of diabetes in this high-risk population.
It is also possible that if the intervention period had
been longer than 16 weeks then more weight loss may
have occurred. Further randomized-controlled trials
with larger samples sizes and longer treatment periods
are planned to learn the best ways to combat this
growing health crisis. The power analysis from this
pilot trial indicates that a sample size of at least 37
would be needed in each group to show statistically
significant weight loss over 16 weeks. We plan to
continue to develop strategies to facilitate weight loss
and to prevent further weight gain in patients treated
with the atypical antipsychotics. We plan to focus on
the population of women with schizophrenia who are
already at highest risk of developing diabetes and
cardiovascular diseases, especially, those who are
Hispanic and African American (Ford et al., 2002;
Meigs, 2003). We hope this research will support
clinicians in providing the highest quality of care to
these individuals who can best benefit from the most
efficacious treatments for their illness
Obesity and its consequences pose a serious health
threat to those with schizophrenia, especially if they are
taking atypical antipsychotics. Cognitive/behavioral
interventions have proven successful in the prevention
of weight gain and diabetes in non-pyschiatric pop-
ulations. This pilot study has demonstrated that weight
loss is possible with cognitive/behavioral interventions
in a population with a psychotic disorder.
References
Allison, D., Casey, D., 2001. Antipsychotic-induced weight gain: a
review of the literature. Journal of Clinical Psychiatry 62 (suppl
7), 22–31.
Allison, D., Mentore, J., Heo, M., Chandler, L., Cappelleri, J.,
Infante, M., Weiden, P., 1999. Antipsychotic-induced weight
gain: a comprehensive research synthesis. American Journal of
Psychiatry 156, 1686–1696.
American Diabetes Association,, 1996. Self-monitoring of blood
glucose. Diabetes Care 19 (supp 1), 62–66.
Aquila, R., Emanuel, M., 2000. Interventions for weight gain in
adults treated with novel antipsychotics. Primary Care Com-
panion to the Journal of Clinical Psychiatry 11, 181–182.
Ayllon, T., 1963. Intensive treatment of psychotic behavior by
stimulus satiation and food reinforcement. Behavior Research
and Therapy 21, 53–61.

M. Weber, K. Wyne / Schizophrenia Research 83 (2006) 95–101 101
Ball, M.P., Coons, V.B., Buchanan, R.W., 2001. A program for
treating olanzapine-related weight gain. Psychiatric Services 52,
967–969.
Basson, B., Kinon, B., Taylor, C., 2001. Factors influencing acute
weight change in patients with schizophrenia treated with
olanzapine, haloperidol, or risperidone. Journal of Clinical
Psychiatry 62, 231–238.
Bayer Healthcare (2005, February 24). Ascensia DEX 2 diabetics
care system. Retrieved February 24, 2005 from http://
www.bayercarediabetes.com/prodServ/custService/pdf/dex2_
eng.pdf.
Bernard, J., 1968. Rapid treatment of gross obesity by operant
techniques. Psychological Reports 23, 663–666.
Everson, S., Goldberg, D.E., Helmrich, S., Lakka, T., Lynch, J.,
Kaplan, G., Solonen, J., 1998. Weight gain and the risk of
developing insulin resistance syndromes. Diabetes Care 21,
1637–1643.
Ford, E., Giles, W., Dietz, W., 2002. Prevalence of the metabolic
syndrome among US adults: findings from the third National
Health and Nutrition Examination Survey. Journal of the
American Medical Association 287, 356–359.
Green, A., Patel, J., Goisman, R., Allison, D., Blackburn, G., 2000.
Weight gain from novel antipsychotic drugs: need for action.
General Hospital Psychiatry 22, 224–235.
Henderson, D., Cagliero, E., Gray, C., Nasrallah, R., Hayden, D.,
Schoenfeld, D., Goff, Donald, 2000. Clozapine, diabetes melli-
tus, weight gain, and lipid abnormalities: a five-year naturalistic
study. American Journal of Psychiatry 157, 975–981.
Knowler, W., Barrett-Connor, E., Fowler, S., Hamman, R., Lachin,
J., Walker, E., Nathan, D., 2002. Reduction in the incidence of
Type 2 diabetes with lifestyle intervention or metformin. The
New England Journal of Medicine 346, 393–403.
Knowler, W.C., Hamman, R.F., Edelstein, S.L., Barrett-Connor, E.,
Ehrmann, D.A., Walker, E.A., Fowler, S.E., Nathan, D.M.,
Kahn, S.E.Diabetes Prevention Program Research Group, 2005.
Prevention of type 2 diabetes with troglitazone in the Diabetes
Prevention Program. Diabetes 54 (4), 1150–1156 (Apr).
Knox, J., 1980. A study of weight reducing diets in psychiatric in-
patients. British Journal of Psychiatry 136, 287–289.
Littrell, K., Hilligoss, N., Kirshner, C., Petty, R., Johnson, C., 2003.
Journal of Nursing Scholarship 35, 237–241.
Meigs, J., 2003. Epidemiology of the insulin resistance syndrome.
Current Diabetes Reports 3, 73–79.
Nawaz, H., Katz, D., 2001. American College of Preventive
Medicine Practice Policy Statement: weight management
counseling of overweight adults. American Journal of Preven-
tive Medicine 21, 73–78.
Rotatori, A., Fox, R., Wicks, A., 1980. Weight loss with psychiatric
residents in a behavioral self-control program. Psychological
Reports 46, 483–486.
Perkins, D., 2002. Predictors of noncompliance in patients with
schizophrenia. Journal of Clinical Psychiatry 63, 1121–1128.
Thakore, J., Mann, J., Vlahos, I., Martin, A., Reznek, R., 2002.
Increased visceral fat distribution in drug-naı̈ve and drug-fee
patients with schizophrenia. International Journal of Obesity and
Related Metabolic Disorders 26, 137–141.
Umbricht, D., Flury, H., Bridler, R., 2001. Cognitive behavior
therapy for weight gain. American Journal of Psychiatry 158,
971.
Vreeland, B., Minsky, S., Menza, M., Rigassio Radler, D.,
Roemheld-Hamm, B., Stern, R., 2001. A program for managing
weight gain associated with atypical antipsychotics. Psychiatric
Services 54, 1155–1157.
Weiden, P., Aquila, R., Standard, J., 1996. Atypical antipsychotic
drugs and long-term outcome in schizophrenia. Journal of
Clinical Psychiatry 57 (suppl 11), 53–60.
Williamson, D., Perrin, L., 1996. Behavioral therapy for obesity.
Endocrinology and Metabolism Clinics of North America 25,
943–953.
Wirshing, D., Wirshing, W., Kysar, L., Berisford, M., Goldstein, D.,
Pashdag, J., Mintz, J., Marder, S., 1999. Novel antipsychotics:
comparison of weight gain liabilities. Journal of Clinical
Psychiatry 60, 358–363.