a clinical investigation of painful hiv-associated sensory...
TRANSCRIPT
1
A Clinical Investigation of Painful HIV-Associated Sensory Neuropathy
Thesis presented for the degree of
Doctor Of Medicine
Imperial College London
Dr Tudor Joseph Colin Phillips
The Pain Group, Section of Anaesthetics, Pain Medicine and Intensive
Care, Chelsea and Westminster Hospital Campus, London.
Supervisor: Professor ASC Rice
June 2013
2
Acknowledgements
I would first like to thank my supervisor, Andrew Rice for his encouragement to get involved
in the world of pain research, and his subsequent patience and guidance. As with many things
in life, small co-incidences can change your world; all of this would not have happened but
for the seating arrangement on a BA flight. I am thankful to whoever picked Andrew’s seat
for that flight.
Many thanks to the Derek Butler Trust who funded this research. It was a leap into the
unknown for them. Their enthusiasm for helping people living with HIV is inspiring.
Thanks to the Pain Lab guys who were (and are) a breath of fresh air after years in clinical
medicine. Talk of break-beats, Romanian gypsy music and photography were not normal in
hospital medicine. Many thanks to Tim who always had sensible advice and would often help
more than he needed to. Thanks also to Faruq for helping me to negotiate the red tape of a
clinical research project by always knowing which form I needed to fill in. I’d like to thank
Matt for his enthusiasm and help with the data entry; who along with Juan prepared the skin
biopsy slides. Bingo will never be the same again. Thanks Yohannes for getting me
enthusiastic again when I was loosing steam!
Many thanks to Amanda Williams for helping me understand what I was trying to achieve
when all I could see was an ocean of data. I’d like to thank Dave Bennett and Sarah Cox for
helping with the project and for the memories of the most interesting clinics I’ve ever been to.
Thanks to Jim for his hard work with the database. Jim was never rude to me once, despite
my incessant emails regarding the king of all unfathomably complicated quality of life
instruments. We all know which one that is.
Many thanks to all the participants who gave up their time and agreed to leave a bit of
themselves behind to test. Thanks to Dr Mark Nelson; his patients’ respect for him made my
recruitment life easy. Many thanks to the clinical and administrative staff at The St Stephens’
Centre who accepted me into their team.
Research has also given my future wife Amparo, and Blai – our beautiful baby boy who I
dedicate this thesis to. Thank you Amparo for being the best thing to happen to me and for
your love and support through about all the weekends and holidays I spent number crunching
for this. It would have been impossible without you.
It’s nearly done………..
3
Declaration and Author Contributions
All the work contained herein this thesis is mine, with the following exceptions.
Chapter 1:
Professor Andrew S. C. Rice (The Pain Research Group, Imperial College London),
Dr Catherine L. Cherry (Head of Neuropathy and Drug Toxicity Group, Monash
University, Melbourne, Australia) and Philippa Moss (PhD Student London Pain
Consortium Student, The Pain Research Group, Imperial College) edited and made
suggestions to the content of this chapter.
Chapter 2:
As part of the Systematic Review the following authors also conducted data quality
assessments: Dr Catherine L. Cherry, Dr Sarah Cox (Palliative Care Physician,
Chelsea and Westminster NHS Trust Hospital, London) and Professor Andrew S. C.
Rice who also acted as final arbitrator.
Chapter 3:
Dr Dave L. H. Bennett (Clinical Neurosciences Department, Oxford University) aided
with the protocol preparation, help preparing the Structure Neurological Examination
(SNE) and expertise in assessing participant electrophysiology data.
Dr Matthew R.D. Brown (NIHR Academic Clinical Fellow, The Pain Research Group
Imperial College) who collected 18 of the 36 healthy volunteer DFNS QST datasets,
and helped with data entry. Dr Matthew Brown and Dr Juan Ramirez Rozo (DPhil
Student, Clinical Neurosciences Dept Oxford University), prepared and stained the
skin biopsies I took, and determined intra-epidermal nerve fibre densities (IENFD).
Dr Amanda C. Williams (Clinical Health Psychology Department, University College
London) for help with selecting the Psychological Instruments for the protocol and for
help with the SPSS data analysis of these results.
4
James Perkins (PhD Student London Pain Consortium, The Bioinformatics Group,
University College London) for preparation and maintenance of the web-based data-
entry portal. James Perkins conducted the hierarchical cluster analysis of QST data.
Dr Yohannes Woldeamanuel (IASP Fellow, Imperial College) for conducting the
ROC analysis for the neuropathy screening tools and preparation of the QST data
scatter plots (Figures 3.1 and 3.2) as an alternative method to present the data in
Figure 3.3.
Copyright declaration:
The copyright of this thesis rests with the author and is made available under a
Creative Commons Attribution Non-Commercial No Derivatives licence. Researchers
are free to copy, distribute or transmit the thesis on the condition that they attribute it,
that they do not use it for commercial purposes and that they do not alter, transform or
build upon it. For any reuse or redistribution, researchers must make clear to others
the licence terms of this work’
5
Abstract
HIV-associated sensory polyneuropathy (HIV-SN) is a distal symmetrical
polyneuropathy that is a prevalent (approximately 40%), and often painful
complication of HIV infection. The introduction of combination antiretroviral
treatment (cART), transformed HIV infection from a high mortality condition
into a chronic disease. Despite this, and the phasing-out of neurotoxic
antiretroviral drugs, HIV-SN continues to be a significant morbidity
experienced in HIV infection. Consequently, the understanding, prevention and
management of HIV-SN is increasingly important.
A systematic review and meta-analysis was undertaken to examine the
evidence for the efficacy of pharmacological agents in the management of pain
in HIV-SN. Of 44 studies identified, 19 were randomized controlled trials, and
only 14 were of sufficient quality. Interventions demonstrating greater efficacy
than placebo included smoked cannabis and recombinant nerve growth factor
(rhNGF). However rhNGF is not clinically available and smoked cannabis
cannot be recommended as routine therapy.
A second study was undertaken to phenotype a cohort of HIV infected
participants with and without HIV-SN. This study examined demographic
factors, symptomatology, metabolic factors, sensory nerve dysfunction through
quantitative sensory testing (QST), and intra-epidermal nerve fibre density
(IENFD); quality of life, sleep dysfunction and psychological co-morbidity. A
novel triumvirate definition using QST, IENFD and a structured neurological
examination was used to define HIV-SN.
This study showed that patterns of sensory nerve dysfunction are
heterogeneous in HIV-SN; the most common feature being loss of sensory
function in mechanical and vibration detection modalities. Gain of function
sensory changes were infrequent, but were seen in a small sub-group
demonstrating wind-up phenomenon; this group demonstrated higher levels of
catastrophizing behaviours. Measures of quality of life were generally lower

6
than in other painful peripheral neuropathies. Sleep dysfunction was common
in HIV-SN. Participants with HIV-SN had elevated triglycerides (TRG),
providing further evidence for the role of dyslipidaemia in HIV-SN
pathogenesis.
7
Table of Contents
ACKNOWLEDGMENTS ............................................................................................................................... 2
DECLARATION AND AUTHOR CONTRIBUTIONS ........................................................................... 3
ABSTRACT ....................................................................................................................................................... 5
TABLE OF CONTENTS ................................................................................................................................ 7
TABLE OF FIGURES AND TABLES ...................................................................................................... 12
Figures ................................................................................................................. 12
Tables ................................................................................................................... 12
PUBLICATIONS ARISING FROM THIS WORK ................................................................................ 14
ABBREVIATIONS ....................................................................................................................................... 15
CHAPTER 1. INTRODUCTION TO PAINFUL HIV-ASSOCIATED SENSORY NEUROPATHY 18
PAIN AND HIV DISEASE ......................................................................................................................... 19
CLINICAL PRESENTATION OF HIV-SN ............................................................................................. 20
RISK FACTORS FOR HIV-SN .................................................................................................................. 21
Risk factors for HIV-SN in patients not exposed to anti-retrovirals .................... 21
Risk factors for HIV-SN in patients exposed to anti-retrovirals .......................... 21
The role of nucleoside reverse transcriptase inhibitors (NRTI)…...................21
cART era risk factors for HIV-SN........................................................................21
Emerging treatment associations with HIV-SN in era of cART ........................... 23
PUTATIVE MECHANISMS OF PATHOGENESIS IN HIV-SN DEVELOPMENT ..................... 24
Proposed pathogenesis of DSP ............................................................................ 24
Proposed pathogenesis of ATN ............................................................................ 25
CLINICAL ASSESSMENT OF HIV-SN .................................................................................................. 25
Clinical diagnosis ................................................................................................ 25
Clinical management ........................................................................................... 26
Remove the underlying cause ..............................................................................26
Provision of analgesia..........................................................................................27
SUMMARY AND CONCLUSION ............................................................................................................. 27
TABLES................................................................................................................ ..............................29
AIMS OF THESIS ........................................................................................................................................ 32
CHAPTER 2. PHARMACOLOGICAL TREATMENT OF PAINFUL HIV-ASSOCIATED SENSORY
NEUROPATHY .................................................................................................................................................. 34
8
INTRODUCTION ......................................................................................................................................... 35
METHODS ..................................................................................................................................................... 35
Eligibility of data sources and search strategy.................................................... 35
PRISMA (Preferred Reporting Items for Systematic reviews and
Meta-Analyses ......................................................................................................35
Search terms ......................................................................................................... 37
Study selection and risk of bias assessment ......................................................... 37
The modified Jadad scale.....................................................................................37
Data extraction..................................................................................................... 38
Statistical analysis............................................................................................... 38
Meta-analysis........................................................................................................38
Weighted average..................................................................................................39
Heterogeneity....................................................................................................... 40
Determination of Number Needed to Treat (NTT).............................................. 40
RESULTS ....................................................................................................................................................... 41
Acetyl-L-carnitine ................................................................................................ 42
Amitriptyline and Mexilitine ................................................................................ 42
Smoked Cannabis ................................................................................................. 43
Topical Capsaicin ................................................................................................ 44
Gabapentin ........................................................................................................... 45
Pregabalin ............................................................................................................ 45
Lamotrigine .......................................................................................................... 45
Recombinant Human Nerve Growth Factor ........................................................ 46
Prosaptide and Peptide T ..................................................................................... 47
DISCUSSION ................................................................................................................................................. 47
Summary ............................................................................................................... 51
FIGURES AND TABLES ............................................................................................................................ 53
CHAPTER 3. PATTERNS OF SENSORY, PSYCHOLOGICAL AND METABOLIC DYSFUNCTION
IN HIV POSITIVE PATIENTS WITH AND WITHOUT HIV-ASSOCIATED SENSORY
NEUROPATHY .................................................................................................................................................. 57
INTRODUCTION ......................................................................................................................................... 58
METHODS ..................................................................................................................................................... 59
Study design and participants .............................................................................. 59
Quantitative sensory testing (QST) ...................................................................... 60
9
QST equipment...........................................................................................61
Thermal threshold detection.......................................................................62
Mechanical detection threshold..............................................................,,..62
Mechanical pain threshold....................................................................,,,...62
Mechanical pain sensitivity and dynamic mechanical allodynia................62
Vibration detection threshold......................................................................62
Pressure pain threshold...............................................................................62
QST data analysis.......................................................................................62
Heat suprathreshold nociceptive testing.....................................................63
Hierarchical cluster analysis.......................................................................63
Structured neurological examination (SNE) ........................................................ 64
Intra-epidermal nerve fibre testing (IENFD) ....................................................... 64
Clinical electrophysiological testing ................................................................... 65
Neuropathy screen and severity tools .................................................................. 66
The Brief Peripheral Neuropathy Screen (BPNS).....................................66
The Toronto Clinical Scoring System (TCSS)..........................................67
The Utah Early Neuropathy Scale (UENS)...............................................67
Pain, sleep disturbance, quality of life and psychological co-morbidity
measures ............................................................................................................... 68
7-day Pain diary..........................................................................................68
Brief Pain Inventory (BPI) 7-item pain interference sub-scale…………..68
SF-36 instrument…....................................................................................68
Pain Anxiety Symptom Scale-20 (PASS-20)…………….........................69
Amended Depression Anxiety Positive-Outlook instrument (DAPOS)….69
The Pain Catastrophizing Scale (PCS)…....................................................69
Insomnia Severity Index (ISI)….................................................................70
Case definition of HIV-SN .................................................................................... 70
Sample size calculation ........................................................................................ 72
RESULTS ....................................................................................................................................................... 73
Participants .......................................................................................................... 73
Demographics ...................................................................................................... 73
Quantitative Sensory Testing healthy participants .............................................. 74
Anti-retroviral therapy history ............................................................................. 74
Quantitative Sensory Testing Results.................................................................. 75
10
Distribution of mean QST z-scores across groups ...................................... 75
Frequency of individual QST measure abnormalities: loss and gain of
function ......................................................................................................... 76
Patterns of loss and gain of sensory function ............................................... 76
Suprathreshold heat testing .......................................................................... 77
Hierarchical cluster analysis of QST data .................................................... 77
Intra-epidermal nerve fibre densities (IENFD) ................................................... 78
Electrophysiological testing ................................................................................. 79
Pain and reported symptoms ................................................................................ 79
Psychological co-morbidity, sleep disturbance and quality of life ...................... 80
Pain interference and health related quality of life......................................80
Sleep dysfunction...........................................................................................80
Depression, Anxiety and Catastrophizing......................................................81
Plasma lipid profiles, random glucose, BMI and waist circumference...............81
Peripheral neuropathy screening and severity instruments: BPNS, UENS and
TCSS.....................................................................................................................82
Testing the triumvirate definition and the consequences of using different HIV-SN
definitions …........................................................................................................82
DISCUSSION ................................................................................................................................................. 83
Quantitative Sensory Testing ............................................................................... 83
Intra-epidermal nerve fibre densities ................................................................... 86
Metabolic factors ................................................................................................. 87
Psychological co-morbidity and sleep disturbance ............................................. 87
Diagnostic tools ................................................................................................... 89
Epidemiological studies ....................................................................................... 90
Summary ............................................................................................................... 90
Study limitations...................................................................................................91
Further post-hoc exploration of using different HIV-SN definitions on
QST results............................................................................................................92
FIGURES AND TABLES..............................................................................................................................95
CHAPTER 4. SUMMARY ............................................................................................................................ 117
REFERENCES ................................................................................................................................................. 123
SUPPLEMENTAL DOCUMENTS ............................................................................................................. 141
11
SUPPLEMENTAL DOCUMENT 1: THE MODIFIED JADAD SCALE ...................................... 141
SUPPLEMENTAL DOCUMENT 2: PINS HIV STUDY CRF ........................................................ 144
SUPPLEMENTAL DOCUMENT 3: QST HEAT SUPRATHREHOLD
PROTOCOL ................................................................................................................................................ 153
SUPPLEMENTAL DOCUMENT 4: QST DATA CRF ...................................................................... 155
SUPPLEMENTAL DOCUMENT 5: STRUCTURED NEUROLOGICAL
EXAMINATION (SNE).................................................................................................. .......................... 156
12
Table of Figures and Tables
Figures
Figure 2.1. PRISMA flow diagram of included randomised controlled trials..... 53
Figure 3.1. Scatter plot of z scores of QST parameters in the Healthy control, HIV-No
SN and HIV-SN groups. ....................................................................................... 95
Figure 3.2.a. Scatter plot of z scores of QST parameters in the Healthy control, HIV-
No SN and HIV-SN groups .................................................................................. 96
Figure 3.2.b. Scatter plot of z scores for mechanical QST parameters in the Healthy
control, HIV-No SN and HIV-SN groups ............................................................. 97
Figure 3.2.c. Scatter plot of z scores for mechanical QST parameters in the Healthy
control, HIV-No SN and HIV-SN groups ............................................................. 98
Figure 3.2.d. Scatter plot of z scores for mechanical QST parameters in the Healthy
control, HIV-No SN and HIV-SN groups ............................................................. 99
Figure 3.3. Comparison of mean QST z-scores (SD) of the HIV-SN, No-HIV-SN and
Healthy control groups. .................................................................................... 100
Figure 3.4. Loss and Gain of sensory function: A comparison of the frequency of QST
abnormalities in participants in the Healthy control, HIV-No SN and HIV-SN groups
which have QST values outside the 95% CI of the DFNS reference database. 101
Figure 3.5. Pain intensity response curves for suprathreshold heat stimuli in Healthy
control subjects, HIV-No SN group and HIV-SN group. .................................. 102
Figure 3.6. Hierarchical cluster analysis of participants’ peripheral neuropathy and
pain status defined by participants QST data .................................................... 103
Figure 3.7. Two representative skin biopsy samples of HIV infected participants.104
Tables
Table 1.1. Summary of clinical studies examining associated factors and the
development of HIV-SN pre-cART introduction .................................................. 29
Table 1.2. Summary of clinical studies examining associated factors and the
development of HIV-SN following introduction of cART (2004 to 09). ............... 30
Table 1.3. Summary of clinical studies examining associated factors and the
development of HIV-SN following introduction of cART (2009 to 11) ................ 31
Table 2.1. Studies excluded from the systematic review. ..................................... 54
13
Table 2.2. Characteristics and results of included studies .................................. 55
Table 2.3. Summary of RCTs which demonstrated treatment superior to placebo, for
which Relative Risk and Number Needed to Treat values could be calculated. .. 56
Table 3.1. Comparison of participants’ demographics, characteristics and co-
morbidities between HIV-No SN and HIV-SN groups enrolled in the study. .... 105
Table 3.2. Comparison of antiretroviral drug therapy use between HIV-No SN and
HIV-SN groups. .................................................................................................. 106
Table 3.3. Mean values of QST parameters after z-score transformation for the three
groups. Dynamic mechanical allodynia (DMA) and paradoxical heat sensations
(PHS) are presented as mean number of events. ............................................... 107
Table 3.4. Frequency of different patterns of sensory loss and gain in the HIV-SN
group. ................................................................................................................. 108
Table 3.5. Correlation of IENFD and individual thermal and mechanical QST
parameters ........................................................................................................ 109
Table 3.6. Comparison of participant reported symptoms between HIV-SN and HIV-
No SN groups ....................................................................................................... 10
Table 3.7. Psychological and Sleep instruments questionnaire returned and completed
per group. ........................................................................................................... 111
Table 3.8. Summary of Sleep and Psychological instruments results comparing HIV-
No SN and painful HIV-SN. ............................................................................... 112
Table 3.9. Comparison of metabolic factors: random plasma lipid profiles, glucose,
BMI, waist-hip ratio and statin use for HIV-No SN and HIV-SN groups. ......... 113
Table 3.10. Comparison of using different combinations of the triumvirate criteria for
the diagnosis of HIV-SN..................................................................................... 114
Table 3.11. Comparisons of using original PINS study criteria, Brief Peripheral
Neuropathy Screen (BPNS) and the Structured Neurological Examination (SNE)
as HIV-SN criteria for QST z-score results; ……………………………………………....115
Table 3.12. Comparisons of using symptoms of paraesthesia and/or numbness,
and the presence of pain alone as HIV-SN criteria for QST z-score results.
respectfully…………………………………………………………………………..….116
14
Publications arising from this work
Abstracts
A Meta-analysis of Randomised Controlled Clinical Trials Assessing the
Effectiveness of Pharmacological Interventions for Painful HIV-
Associated Sensory Neuropathy. Tudor J. C. Phillips, Catherine L.
Cherry, Sarah Cox, Sarah Marshall, Andrew S. C. Rice
Abstract and poster presentation IASP 13th World Congress on Pain,
Montreal, Canada. September 2010.
Sensory Profiles and Epidermal Innervation in Patients with HIV-
Associated Sensory Neuropathy. Matthew R. D. Brown, Tudor J. C.
Phillips, Juan D. Ramirez, James R. Perkins, Christine Orengo,
Yohannes W. Woldeamanuel, Sarah Cox, Istvan Bodi, Christoph Maier,
Elena Krumova, David L. H. Bennett, Andrew S. C. Rice.
Abstract and poster presentation NeupSIG World Congress, Toronto
Canada. May 2013.
Assessment of the Utility of Clinical Instruments for Diagnosing HIV-
associated Sensory Neuropathy. Yohannes W. Woldeamanuel, Tudor J.
C. Phillips, Matthew R. D. Brown, Juan D. Ramirez, James R. Perkins,
Christine Orengo, Sarah Cox, David L. H. Bennett, Andrew S. C. Rice.
Abstract and poster presentation NeupSIG World Congress, Toronto
Canada. May 2013
Original Papers
Phillips, T. J. C., Cherry, C. L. , Cox, S. , Marshall, S. J. , et al. (2010)
Pharmacological treatment of painful HIV-associated sensory
neuropathy: a systematic review and meta-analysis of randomised
controlled trials. PloS one. [Online] 5 (12), e14433.
15
Abbreviations
AIDS Acquired Immunodeficiency Syndrome
ARV Anti-Retroviral agent
AUC Area Under the Curve
ATN Antiretroviral Toxic Neuropathy
BMI Body Mass Index
BPNS Brief Peripheral Neuropathy Screen
BPI Brief Pain Inventory
cART combination Anti-Retroviral Therapy
CDT Cold Detection Threshold
CIDP Chronic Inflammatory Demyelinating Polyradiculopathy
CPT Cold Pain Threshold
CRF Clinical Record File
DAPOS Depression Anxiety Positive-Outlook Scale
ddC 2',3'-dideoxycytidine (Zalcitabine)
ddI 2',3'-dideoxyinosine (Didanosine)
DDS Descriptor Differential Scale
DMA Dynamic Mechanical Allodynia
dNRTI 2',3'-dideoxy moiety containing class of NRTI drug
DSM-IV Diagnostic and Statistical Manual of Mental Disorders
DSP Distal Sensory Polyneuropathy
d4T 2',3'-didehydro-2',3'-dideoxythymidine (Stavudine)
16
EFNS European Federation of Neurological Societies
HDL High Density Lipoprotein
HIV Human Immunodeficiency Virus
HIV-No SN HIV infection with No HIV-Associated Sensory Neuropathy
HIV-SN HIV-Associated Sensory Neuropathy
HPT Heat Pain Threshold
IENFD Intra-Epidermal Nerve Fibre Density
ISI Insomnia Severity Index
ITT Intention-To-Treat
LDL Low Density Lipoprotein
MDT Mechanical Detection Threshold
MPT Mechanical Pain Threshold
MPS Mechanical Pain Sensitivity
NCS Nerve Conduction Studies
NICE National Institute for Health and Care Excellence
NNRTI Non-Nucleoside Reverse Transcriptase Inhibitor
NNT Number Needed to Treat
NPRS Numerical Pain Rating Scale
NRES National Research Ethics Service
NRS Numerical Rating Scale
NRTI Nucleoside Reverse Transcriptase Inhibitor
OCT Optimal Cutting Temperature compound
PASS-20 Short Version of the Pain Anxiety Symptoms Scale

17
PCS Pain Catastrophizing Scale
PEP Post Exposure Prophylaxis
PHS Paradoxical Heat Sensation
PI Protease Inhibitor
PP Per Protocol population
PPT Pressure Pain Threshold
PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses
QST Quantitative Sensory Testing
RCT Randomised Controlled Trial
rhNGF recombinant human Nerve Growth Factor
ROC Receiver Operating Characteristic
RR Relative Risk
SD Standard Deviation
SF-36 Short Form (36) Health Survey
SN Sensory Neuropathy
SNE Structured Neurological Examination
TCSS Toronto Clinical Neuropathy Score
TNF-α Tumour Necrosis Factor α
TRG Triglycerides
TSL Thermal Sensory Limen
UENS Utah Early Neuropathy Scale
18
Chapter 1
Introduction to Painful HIV-Associated Sensory Neuropathy
19
Introduction to Painful HIV-Associated Sensory Neuropathy Pain and HIV disease
Pain associated with HIV disease is common and multifactorial (Cox & Rice, 2008)
with different causes possible at different stages of the disease. A frequent cause of
pain, at all stages of the disease, is neuropathic pain associated with a symmetrical
sensory polyneuropathy; HIV associated sensory neuropathies (HIV-SN) attributable
to HIV itself and to some HIV treatments (Verma, 2001).
HIV-SN is common. Prior to the availability of antiretroviral drugs, estimates of HIV-
SN prevalence varied from <2% if those with very early HIV disease (R. Barohn et
al., 1993) to 35% among hospitalized patients with AIDS (So, Holtzman, Abrams, &
Olney, 1988). When ambulatory HIV patients (all stages of disease) were surveyed,
around 13% were found to have HIV-SN (Woolley, Faragher, Ugoni, & Spelman,
1993). The prevalence of HIV-SN attributable to the virus itself increases with
advancing HIV disease (Childs et al., 1999).
The introduction of combination antiretroviral therapy (cART) in the mid 1990s has
dramatically reduced the morbidity and mortality associated with HIV among patients
who have access to treatment (Mocroft et al., 2003). Life expectancy with HIV in
well-resourced countries is now estimated to be up to two-thirds of the general
population (Collaboration., 2008; Lohse et al., 2007). While the incidence of most
neurological complications of HIV has fallen with the introduction of effective
therapy, rates of HIV-SN have been rising since the first effective antiretroviral drugs
were developed (Bacellar et al., 1994). It is now clear that some HIV treatments,
notably particular nucleoside reverse transcriptase inhibitors (NRTI) – stavudine
(d4T), didanosine (ddI) and zalcitabine (ddC) – are potentially neurotoxic (Keswani,
Pardo, Cherry, Hoke, & Mcarthur, 2002; Moyle & Sadler, 1998). Recent estimates of
HIV-SN prevalence among cohorts with access to cART range from 20% to >50%
(Konchalard, K. Wangphonpattanasiri, 2007; Wright et al., 2008). Importantly, the
available evidence suggests that HIV-SN prevalence remains high among cART-
treated patients, even in countries where known neurotoxic antiretroviral drugs such
as stavudine are no longer commonly used (Smyth et al., 2007). In less well-resourced
centres, use of stavudine, an inexpensive and effective antiretroviral, in first-line HIV
20
treatment remains common despite high rates of toxicity (Joint United Nations
Programme on HIV/AIDS, 2013).
Current estimates of global HIV prevalence stand at 33 million, with 2.5 million new
infections each year and more patients gaining access to cART (Joint United Nations
Programme on HIV/AIDS, 2013). With high rates of HIV-SN now reported globally,
and up to 90% of affected patients experiencing potentially debilitating neuropathic
pain, HIV-SN represent a large, and potentially worsening, source of world morbidity.
Therefore, there is an urgent need to understand better the pathogenesis of HIV-SN,
identify risk factors, develop effective preventative strategies and improve symptom
control among existing sufferers.
Clinical Presentation of HIV-SN
The clinical presentation of HIV-SN is similar regardless of whether the syndrome is
caused by HIV itself (often termed Distal Sensory Polyneuropathy – DSP) or by
toxicity from antiretroviral drugs (Antiretroviral Toxic Neuropathy – ATN). In many
cases, DSP and ATN may co-exist and indeed there may be a level of
interdependence in their aetiologies.
Patients with HIV-SN typically present with the classical distal bilateral sensory
symptoms of an axonal length dependant polyneuropathy, in a “sock and glove”
distribution with the feet being first affected. Symptom onset is variable; with some
data suggesting ATN may be more likely to be sudden in onset and rapidly
progressive, and DSP more insidious (D. Cornblath & McArthur, 1988; Justin C
McArthur, Brew, & Nath, 2005).
Quantitative sensory testing of patients with HIV-SN reveals a loss of thermo-
sensation characteristic of a loss of C- fibres (Bouhassira, Attal, Willer, & Brasseur,
1999; Martin, Solders, Sönnerborg, & Hansson, 2003). This “die back” pattern of
degeneration of C fibres has been confirmed by analysis of epidermal innervation in
skin biopsies. Profound motor weakness is a relatively infrequent feature of HIV-SN,
and if present, is usually a late finding restricted to the intrinsic muscles of the feet
(D. Cornblath & McArthur, 1988). Indeed, its presence should prompt a search for an
alternative diagnosis such as Chronic Inflammatory Demyelinating Polyradiculopathy
(CIDP).
21
Risk Factors For HIV-SN
Risk factors for HIV-SN in patients not exposed to antiretroviral drug
Studies examining rates and risk factors for HIV-SN among AVR–naive patients
typically found that the prevalence of HIV-SN increases with disease progression (see
Table 1.1). Precise associations with HIV-SN vary among the available studies, but
have included lower CD4 T-cell count, higher viral load or surrogate markers of
disease progression, such as Mycobacterium avium infection.
Risk factors for SN among patients exposed to antiretroviral drugs
The role of nucleoside reverse transcriptase inhibitors (NRTI)
Despite the association between HIV-SN and advanced HIV disease in patients not
receiving antiretroviral therapy, the introduction of effective HIV treatment has not
been associated with the predicted fall in HIV-SN prevalence. Indeed, where data are
available before and after the introduction of cART, the prevalence of HIV-SN has
risen, probably due ATN (Bacellar et al., 1994; Smyth et al., 2007).
The potential neurotoxicity of particular NRTI and the development ATN was
observed in early clinical trials, where SN was a dose limiting toxicity for the NRTIs
d4T, ddI and ddC (Moyle & Sadler, 1998; Yarchoan et al., 1988). The profound
neurotoxicity of d4T, the dNRTI most widely used today, was highlighted in a study
of Post Exposure Prophylaxis (PEP) where healthy, HIV uninfected men were offered
28 days of antiretroviral therapy as prophylaxis following a possible HIV exposure.
Six percent of HIV negative adults developed symptoms consistent with neuropathy
within 28 days of d4T-containing PEP (Winston, McAllister, Amin, Cooper, & Carr,
2005). In HIV infected individuals on long-term cART, ATN has been observed to
occur as long as one year after commencement of therapy including a dNRTI
(Lichtenstein et al., 2005). In the clinical situation, the temporal association between
dNRTI exposure and the onset of neuropathy symptoms is typically the sole feature
that suggests a diagnosis of ATN rather than DSP.
cART-Era risk factors for HIV-SN
Whilst exposure to dNRTIs, high viral load and low CD4 counts have been previously
established in the pre-cART era as risk factors (see Table 1.1), in the cART era this
has become less clear (see Table 2.2).
22
One study has suggested that the use of dNRTI may be protective against SN after a
year of use (Lichtenstein et al., 2005). This paradox might be explained by the
observation that individuals susceptible to ATN will often become symptomatic
within a few months of dNRTI exposure. Thus, ATN susceptible individuals may be
switched to alternative ARV when they develop neuropathy symptoms, leaving only
those who are at intrinsically low risk for ATN on dNRTI therapy after a year.
The neurotoxic potential of dNRTI is clear but in recent years there has been a
growing interest in other factors that may place HIV patients at risk for neuropathy.
This is important for at least two reasons:
1. Although ddC, the most profoundly neurotoxic NRTI (A. Berger et al., 1993),
is not longer in clinical use, d4T remains a common component of first-line
HIV treatment in many low and middle-income countries, largely for
economic reasons. Understanding which patients are at highest risk for ATN if
treated with d4T would allow rational prioritization of the highest risk
individuals for access to more expensive alternatives.
2. As set out above, rates of HIV-SN remain high even in high-income country
centres where use of dNRTI has largely ceased. More work is needed to
understand why particular patients are developing HIV-SN despite effective
HIV treatment with cART not known to be neurotoxic so that preventative
strategies and pathogenesis based therapies can be developed (Smyth et al.,
2007).
Increasing age is associated with HIV-SN risk in almost every published cohort, both
before and after the introduction of cART (see Tables 1.1-1.3). This is consistent with
the known vulnerability of the ageing peripheral nervous system to most types of
polyneuropathy, including diabetic and toxin-induced neuropathies.
Height is an HIV-SN risk factors (Affandi et al., 2008; C L Cherry et al., 2006, 2009;
Morgello et al., 2004; Pettersen et al., 2006; Antonia L Wadley, Cherry, Price, &
Kamerman, 2011; Watters et al., 2004) as it is for other polyneuropathies (Cheng et
al., 2006). Rates of HIV-SN were associated with age and height in Australian,
Indonesian and Malaysian patients prescribed stavudine. Using cut off values of
170cm and 40 years, the authors showed that the rate of stavudine-associated

23
neuropathy was 20% in younger, shorter patients compared with 66% of older, taller
patients (C L Cherry et al., 2009). It was suggested that these simple criteria could be
used to determine who should be given priority access to less neurotoxic but more
expensive ARVs in resource poor settings.
Demographic and clinical features, other than age, in untreated HIV patients have not
been consistently associated with SN risk among patients on cART (Table 1.2). For
example, neither viral load nor CD4 T-cell counts are independently associated with
SN risk among treated patients (Morgello et al., 2004; Smyth et al., 2007). In contrast,
evidence of advanced HIV infection prior to initiation of therapy may still be
relevant, with nadir CD4 count and a history of an AIDS defining illness associating
with SN risks in some cohorts. As more studies are performed in a range of settings,
new risk factors for HIV-SN are also emerging. For example, race may be an
important determinant of the individual’s HIV-SN risk (Jessica Robinson-Papp,
Gonzalez-Duarte, Simpson, Rivera-Mindt, & Morgello, 2009).
Host genotype has been associated with SN risk among dNRTI-exposed patients by
several groups. Consistent with putative pathogenic mechanisms of HIV-SN,
associations include mitochondrial haplogroups (Hulgan et al., 2005) and genes
associated with inflammation (Affandi et al., 2008; Catherine L Cherry et al., 2008).
Associations with haemochromatosis gene polymorphisms are also reported
(Kallianpur et al., 2006).
Emerging treatment associations with HIV-SN in the era of cART
Despite a reduction in the use of dNRTI in well-resourced settings, the available data
suggest that the expected decline in HIV-SN prevalence has not occurred. For
example, repeated cross sectional surveys of an ambulatory Australian HIV
population showed that SN prevalence rose from 14% in 1993 (pre-cART) to 44% in
2001 (era of frequent use of dNRTI). Despite a change to mostly dNRTI sparing
cART regimens, and a reduction in the proportion of patients who had ever been
exposed to dNRTI, the prevalence of HIV-SN remained unchanged at 42% in 2006
(Smyth et al., 2007). This and other recent studies suggest that risk factors other than
dNRTI exposure are important. Exposure to certain protease inhibitors, especially
indinavir, is associated with SN risk (Lichtenstein et al., 2005; Pettersen et al., 2006;
Smyth et al., 2007). This is supported by in vitro studies using cultured rodent dorsal
24
root ganglia DRGs from rats expressing the human chemokine receptors required for
HIV cell entry demonstrate indinavir-associated neurotoxicity from indinavir
exposure (Pettersen et al., 2006). Whether this is a class effect of PI or is isolated to
indinavir has yet to be fully explored.
Putative mechanisms of pathogenesis in HIV-SN development
The exact mechanism/s by which HIV-SN develops continues to be subject of debate.
It also remains unclear whether or not DSP and ATN may share some degree of
interaction and/or synergy in their pathophysiology (Bhangoo, Ripsch, Buchanan,
Miller, & White, 2009; Wallace, Blackbeard, Pheby, et al., 2007).
Proposed pathogenesis of DSP
Direct infection of neurons by HIV rarely, if ever, occurs; consequently hypotheses of
HIV-SN have focused on neuronal toxicity of HIV secreted proteins and the immune
dysregulation seen in HIV disease.
The HIV viral envelope glycoprotein gp120 is required to interact with both CD4
receptors and with the chemokine receptors CXCR4 or CCR5 in order to enter
immune cells and replicate. Gp120 shed from HIV virions is thought to interact with
neuronally expressed CCR5 and/or CXCR4 to induced the neuronal apoptosis which
is characteristic of HIV dementia (Kaul, Garden, & Lipton, 2001; Kaul & Lipton,
1999; Kirsh et al., 1990). There is now a reasonable body of evidence to suggest that a
similar pathological mechanism exists for HIV-SN (Bhangoo et al., 2009; Maratou et
al., 2009; Melli, Keswani, Fischer, Chen, & Höke, 2006; Oh et al., 2001). GP120
induces a TNF-α mediated apoptosis and axonal degeneration in sensory neurones
both directly and indirectly via the stimulation of Schwann cells and macrophages
that results in the aberrant release of neurotoxins (Kaul & Lipton, 1999; Keswani et
al., 2003; Melli et al., 2006). Chemokines have been shown to play a key role in the
pathophysiology of neuropathic pain in the context of multiple diseases (White, Jung,
& Miller, 2007). TNF-α 1031*2 was independently associated with an increased risk
of HIV-SN in both, a population of predominately European descent and an
Indonesian population (Affandi et al., 2008). In contrast a cytokine polymorphism of
the proinflammatory IL-12β cytokine was associated with increased risk of
developing HIV-SN but this was not replicated in an Indonesian population. A recent
large epidemiological study in a South African population has further established the
25
role of inflammatory response and HIV-SN development by identifying the
importance of a IL-4 inflammatory cytokine polymorphism (IL-4 590*T) as a risk
factor for the development of HIV-SN (A L Wadley et al., 2013).
Proposed pathogenesis of ATN
dNRTIs have been shown to be neurotoxic to sensory neurones and result in features
reflecting neuropathic pain in animal models (Bhangoo et al., 2009; Chen & Levine,
2007; Joseph, Chen, Khasar, & Levine, 2004; Joseph & Levine, 2004, 2006; Wallace,
Blackbeard, Segerdahl, et al., 2007a): both chemokine-induced and mitochondrial
toxicity have been implicated in this pathology. There is also some evidence of
indinavir mediated neurotoxicity of sensory neurones (Pettersen et al., 2006).
Recently established animal models of both stavudine (Wenlong Huang et al., 2013)
and indinavir mediated neurotoxicity (W Huang, Pheby, & Rice, 2013) will be
important in further elucidating the pathogenesis of ARV mediated neurotoxicity.
Clinical assessment of HIV-SN
HIV-SN is primarily a clinical diagnosis and the general principles of assessing any
patient with peripheral neuropathic pain should be followed (Cruccu et al., 2010;
Haanpää et al., 2009). Use of diagnostic tests to investigate primary sensory neurone
morphology or function (such as quantification of epidermal nerve fibre density,
thermal threshold testing or nerve conduction studies) may be helpful (Bouhassira et
al., 1999; Griffin, McArthur, & Polydefkis, 2001; Lauria et al., 2005, 2010; Martin et
al., 2003; Rolke et al., 2006), but such testing is not always available outside
specialist centres. Importantly, normal nerve conduction studies do not necessarily
exclude the diagnosis of HIV-SN, as they primarily survey the function of large
diameter afferent nerve fibres. Such testing is most often indicated when atypical
features (such as motor involvement) necessitate the exclusion of alternative
diagnoses, such as a demyelinating polyneuropathy (Keswani et al., 2002).
Clinical diagnosis of HIV-SN
HIV-SN is typically a small fibre, sensory neuropathy. Common symptoms are often
accompanied by neuropathic signs such as reduced or absent ankle reflexes,
diminished vibration sense and altered sensitivity to light tactile or thermal stimuli.
In a patient with HIV infection, a diagnosis of HIV-SN is supported by symptoms and
signs that are largely symmetrical and distal in nature, and the absence of significant
26
motor involvement. Investigating a temporal association between symptom onset and
exposure to potentially neurotoxic ARV is the only method available to assess
whether ATN is perhaps contributing to a case of HIV-SN (Keswani et al., 2002).
Screening tools for the diagnosis of HIV-SN in research context have been described,
including the widely used AIDS Clinical Trials Group Brief Peripheral Neuropathy
Screen (BPNS). This tool is based on a directed symptom questionnaire and limited
clinical examination. It takes only minutes to administer and requires no specialized
equipment. Importantly, this tool has been validated against objective measures
including both thermal threshold testing and epidermal nerve fibre density (Catherine
L Cherry, Wesselingh, Lal, & McArthur, 2005). However, while these features make
the BPNS a useful research tool (for example, in studies examining risk factors
associated with HIV-SN) it cannot replace a careful clinical assessment of the HIV
infected patient presenting with neuropathic symptoms or signs.
A critical part of the clinical assessment of HIV-SN is to exclude alternative
diagnoses that may explain the patient’s symptoms – looking particularly for
reversible causes of peripheral neuropathy. This includes a careful drug history
(including ARV exposures, use of isoniazid or cytotoxic chemotherapy, use of large
doses of vitamins that may be neurotoxic, such as pyridoxine (Gdynia et al., 2008),
and alcohol/recreational drug use) and the exclusion of metabolic disturbances such as
diabetes, thyroid dysfunction or vitamin B12 deficiency. Treatment of any other
contributing condition (or removal of a contributing toxin) is important, including in
patients where HIV-SN is thought to be present. Exclusion of non-neuropathy causes
of pain such as arthropathy or plantar fascitis is also important.
Clinical management of HIV-SN
The clinical management of HIV-SN is primarily directed towards minimising the
progression of pathology and managing the patient’s symptoms.
Remove the underlying cause
When HIV-SN develops in a patient naive to antiretroviral therapy, symptomatic
improvement may be observed with commencement of (non-neurotoxic) cART to
control HIV replication. However, this situation is uncommon today in well-
27
resourced settings, with DSP being a disease of advanced HIV and earlier
commencement of cART recommended in current treatment guidelines.
When HIV-SN develops in a patient who is on treatment with known neurotoxic ARV
(again, an uncommon situation in well-resourced settings today), a change to non-
neurotoxic agents may be required. However, this is a complex decision that only
those with expertise in the management of HIV disease should make. In early clinical
trials, immediate cessation of dNRTI therapy upon development of neuropathic
symptoms was associated with symptomatic improvement in around two thirds of
cases (Blum et al., 1996; Moore, Wong, Keruly, & McArthur, 2000; Pettersen et al.,
2006). Importantly, an initial worsening of symptoms, or “coasting”, commonly
occurs prior to any improvement and may continue for months (Moyle & Sadler,
1998). Following this, some improvement in neuropathic symptoms may be seen up
to a year after discontinuation of the causative agent. Beyond this time, further
improvement is unlikely.
As above, minimizing (or removing) any other potential peripheral nerve insults (e.g.
poorly controlled diabetes, vitamin B12 deficiency) is important to prevent any
additive or synergistic effect this might have on the continued progression of HIV-
SN.
Provision of analgesia
The pharmacological management of pain associated with HIV-SN is an area of
therapeutic need with few therapies being supported by robust evidence. Until the
systematic review presented in Chapter 2 was prepared, there were no systematic
reviews or meta-analysis of evidence for the efficacy of pharmacological agents in
treating pain in HIV-SN.
Summary and conclusions
Sensory neuropathy is a frequent complication of HIV and some HIV treatments.
With an estimated 33 million people living with HIV, more people gaining access to
antiretroviral therapy every day, and HIV-SN prevalence ranging from 20% to >50%
in cART treated cohorts, the burden of HIV-SN pain is a problem of enormous global
importance. No routinely available therapy has been unequivocally shown to be
effective for treating HIV-SN pain. There is an urgent need to understand better the
28
pathogenesis of HIV-SN, develop strategies to prevent new cases of this debilitating
condition and find effective treatments to control the symptoms associated with
existing cases of HIV-SN.
29
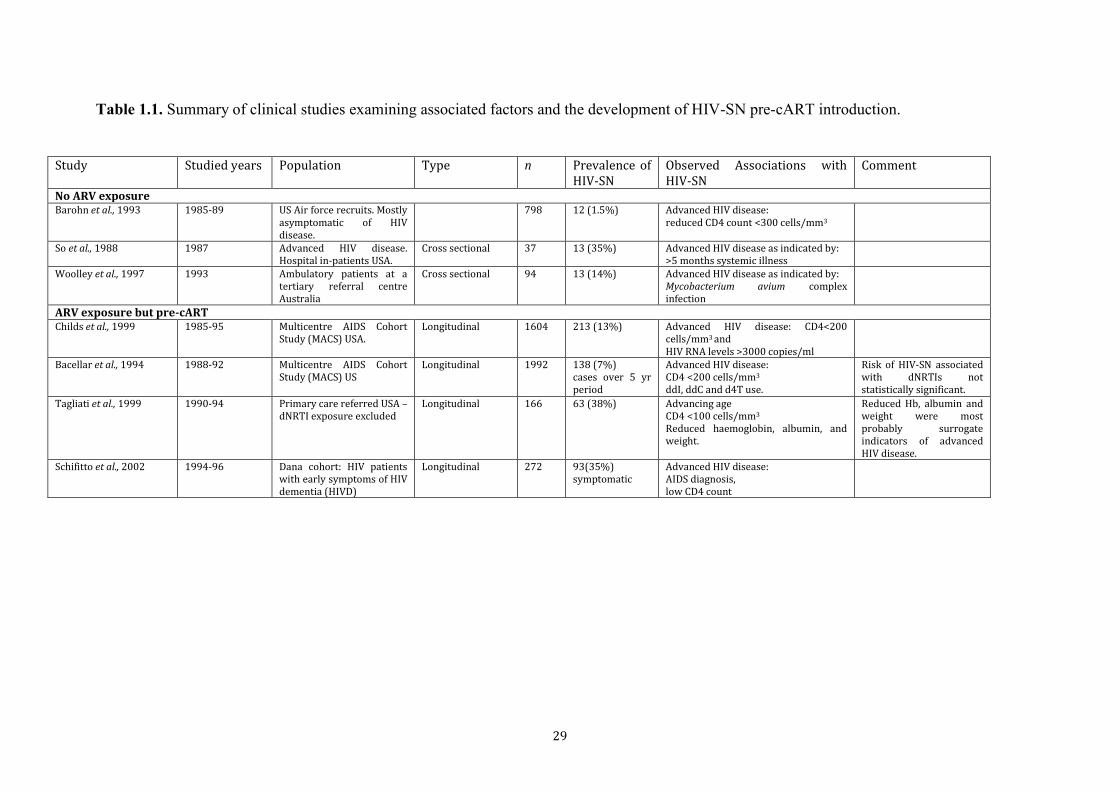
Table 1.1. Summary of clinical studies examining associated factors and the development of HIV-SN pre-cART introduction.
Study Studied years Population Type n Prevalence of HIV-SN
Observed Associations with HIV-SN
Comment
No ARV exposure Barohn et al., 1993 1985-89 US Air force recruits. Mostly
asymptomatic of HIV disease.
798 12 (1.5%) Advanced HIV disease: reduced CD4 count <300 cells/mm3
So et al., 1988 1987 Advanced HIV disease. Hospital in-patients USA.
Cross sectional 37 13 (35%) Advanced HIV disease as indicated by: >5 months systemic illness
Woolley et al., 1997 1993 Ambulatory patients at a tertiary referral centre Australia
Cross sectional 94 13 (14%) Advanced HIV disease as indicated by: Mycobacterium avium complex infection
ARV exposure but pre-cART Childs et al., 1999 1985-95 Multicentre AIDS Cohort
Study (MACS) USA. Longitudinal 1604 213 (13%) Advanced HIV disease: CD4<200
cells/mm3 and
HIV RNA levels >3000 copies/ml
Bacellar et al., 1994 1988-92 Multicentre AIDS Cohort Study (MACS) US
Longitudinal 1992 138 (7%) cases over 5 yr period
Advanced HIV disease: CD4 <200 cells/mm3 ddI, ddC and d4T use.
Risk of HIV-SN associated with dNRTIs not statistically significant.
Tagliati et al., 1999 1990-94 Primary care referred USA – dNRTI exposure excluded
Longitudinal 166 63 (38%) Advancing age CD4 <100 cells/mm3
Reduced haemoglobin, albumin, and weight.
Reduced Hb, albumin and weight were most probably surrogate indicators of advanced HIV disease.
Schifitto et al., 2002 1994-96 Dana cohort: HIV patients with early symptoms of HIV dementia (HIVD)
Longitudinal 272 93(35%) symptomatic
Advanced HIV disease: AIDS diagnosis, low CD4 count
30
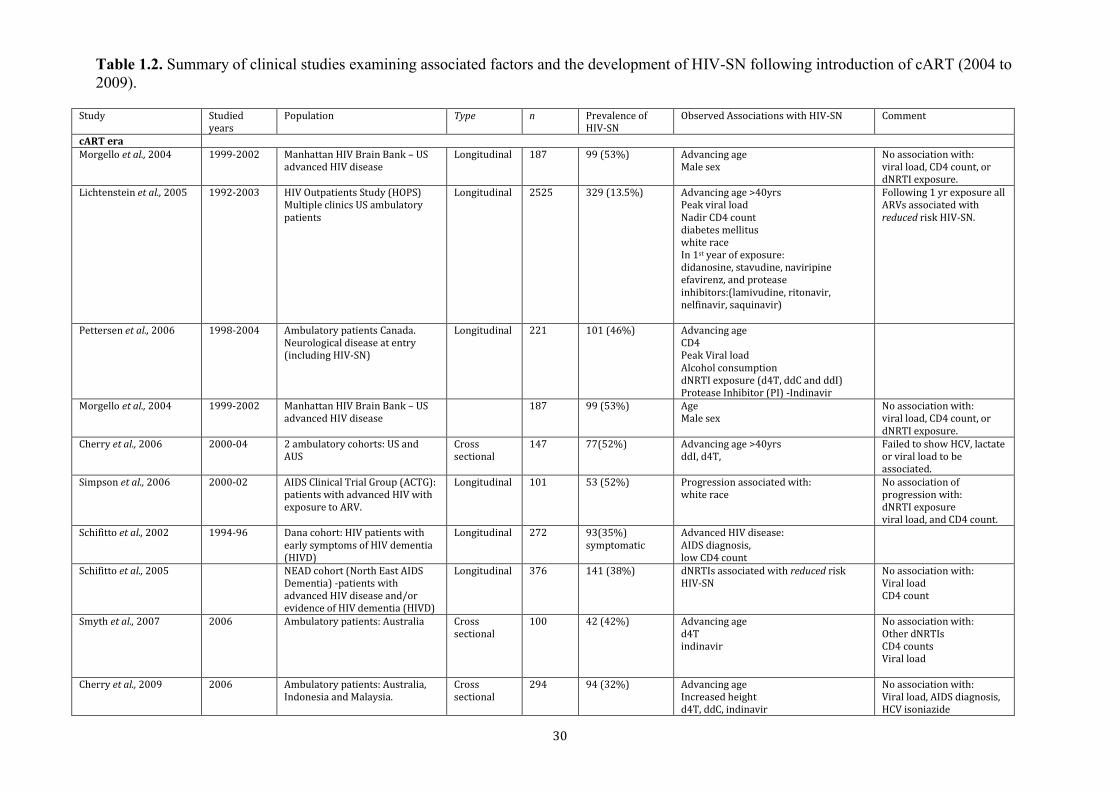
Table 1.2. Summary of clinical studies examining associated factors and the development of HIV-SN following introduction of cART (2004 to 2009).
Study Studied years
Population Type n Prevalence of HIV-SN
Observed Associations with HIV-SN Comment
cART era Morgello et al., 2004 1999-2002 Manhattan HIV Brain Bank – US
advanced HIV disease Longitudinal 187 99 (53%) Advancing age
Male sex No association with: viral load, CD4 count, or dNRTI exposure.
Lichtenstein et al., 2005 1992-2003 HIV Outpatients Study (HOPS) Multiple clinics US ambulatory patients
Longitudinal 2525 329 (13.5%) Advancing age >40yrs Peak viral load Nadir CD4 count diabetes mellitus white race In 1st year of exposure: didanosine, stavudine, naviripine efavirenz, and protease inhibitors:(lamivudine, ritonavir, nelfinavir, saquinavir)
Following 1 yr exposure all ARVs associated with reduced risk HIV-SN.
Pettersen et al., 2006 1998-2004 Ambulatory patients Canada. Neurological disease at entry (including HIV-SN)
Longitudinal 221 101 (46%) Advancing age CD4 Peak Viral load Alcohol consumption dNRTI exposure (d4T, ddC and ddI) Protease Inhibitor (PI) -Indinavir
Morgello et al., 2004 1999-2002 Manhattan HIV Brain Bank – US advanced HIV disease
187 99 (53%) Age Male sex
No association with: viral load, CD4 count, or dNRTI exposure.
Cherry et al., 2006 2000-04 2 ambulatory cohorts: US and AUS
Cross sectional
147 77(52%) Advancing age >40yrs ddI, d4T,
Failed to show HCV, lactate or viral load to be associated.
Simpson et al., 2006 2000-02 AIDS Clinical Trial Group (ACTG): patients with advanced HIV with exposure to ARV.
Longitudinal 101 53 (52%) Progression associated with: white race
No association of progression with: dNRTI exposure viral load, and CD4 count.
Schifitto et al., 2002 1994-96 Dana cohort: HIV patients with early symptoms of HIV dementia (HIVD)
Longitudinal 272 93(35%) symptomatic
Advanced HIV disease: AIDS diagnosis, low CD4 count
Schifitto et al., 2005 NEAD cohort (North East AIDS Dementia) -patients with advanced HIV disease and/or evidence of HIV dementia (HIVD)
Longitudinal 376 141 (38%) dNRTIs associated with reduced risk HIV-SN
No association with: Viral load CD4 count
Smyth et al., 2007 2006 Ambulatory patients: Australia Cross sectional
100 42 (42%) Advancing age d4T indinavir
No association with: Other dNRTIs CD4 counts Viral load
Cherry et al., 2009 2006 Ambulatory patients: Australia, Indonesia and Malaysia.
Cross sectional
294 94 (32%) Advancing age Increased height d4T, ddC, indinavir
No association with: Viral load, AIDS diagnosis, HCV isoniazide
31
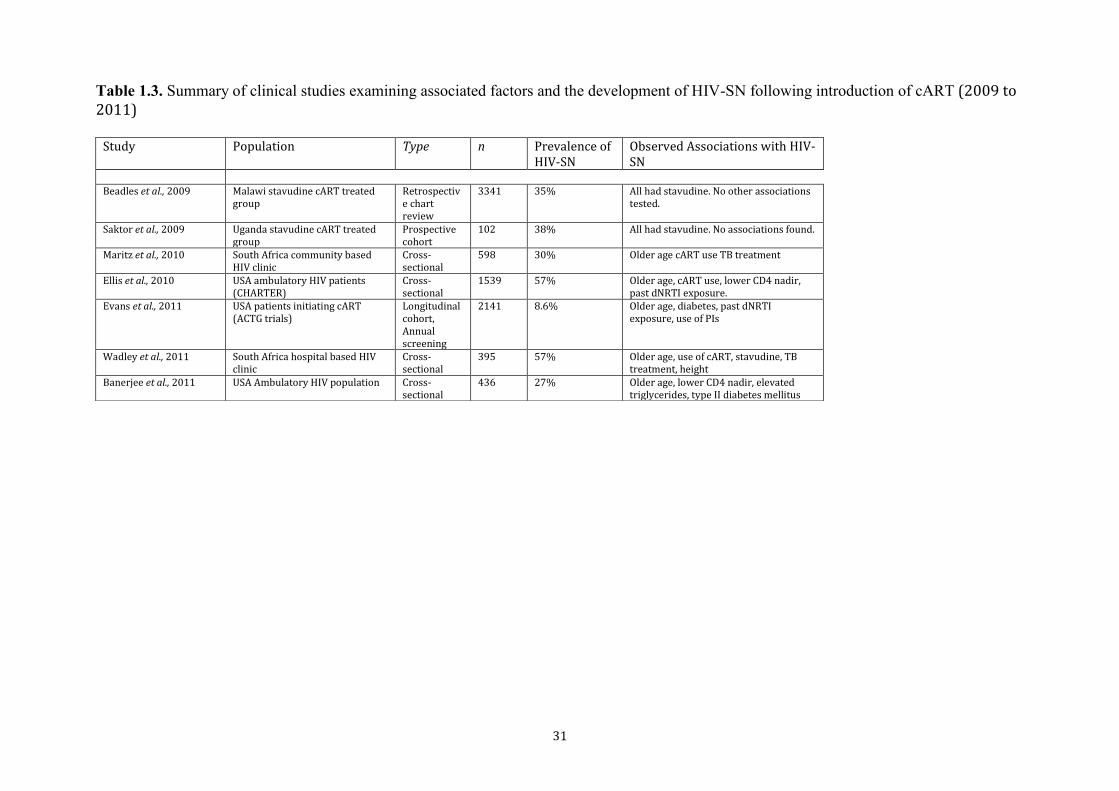
Table 1.3. Summary of clinical studies examining associated factors and the development of HIV-SN following introduction of cART (2009 to 2011)
Study Population Type n Prevalence of HIV-SN
Observed Associations with HIV-SN
Beadles et al., 2009 Malawi stavudine cART treated
group Retrospective chart review
3341 35% All had stavudine. No other associations tested.
Saktor et al., 2009 Uganda stavudine cART treated group
Prospective cohort
102 38% All had stavudine. No associations found.
Maritz et al., 2010 South Africa community based HIV clinic
Cross-sectional
598 30% Older age cART use TB treatment
Ellis et al., 2010 USA ambulatory HIV patients (CHARTER)
Cross-sectional
1539 57% Older age, cART use, lower CD4 nadir, past dNRTI exposure.
Evans et al., 2011 USA patients initiating cART (ACTG trials)
Longitudinal cohort, Annual screening
2141 8.6% Older age, diabetes, past dNRTI exposure, use of PIs
Wadley et al., 2011 South Africa hospital based HIV clinic
Cross-sectional
395 57% Older age, use of cART, stavudine, TB treatment, height
Banerjee et al., 2011 USA Ambulatory HIV population Cross-sectional
436 27% Older age, lower CD4 nadir, elevated triglycerides, type II diabetes mellitus
32
Aims of the thesis
Many of the important risk factors for the development of HIV-SN identified in the
pre-cART era were related to poor HIV virus suppression (nadir CD4 counts, high
viral loads and AIDS) and its treatment with earlier neurotoxic ARV agents (e.g. ‘d’
NRTI agents). It was therefore anticipated, with good reason that the prevalence of
HIV-SN would fall significantly with the introduction of effective HIV management
with cART in the mid-1990s. However despite both the improved HIV virus control
and crucially the phasing out of neurotoxic dNRTI drugs, especially in well-resourced
countries, the prevalence of HIV-SN in both high and low resource HIV populations
has remained consistently at around 40%. This suggests strongly that drug induced
neurotoxicity may not be a major aetiological factor for HIV-SN in the cART-era
(Catherine Louise Cherry, Wadley, & Kamerman, 2012; Ellis et al., 2010; Smyth et
al., 2007).
Current estimates of global HIV prevalence stand at 33 million, with 2.5 million new
infections each year and more patients gaining access to cART (Joint United Nations
Programme on HIV/AIDS, 2013). With high rates of HIV-SN now reported globally,
and with between 40 to 90% of affected patients experiencing potentially debilitating
neuropathic pain, HIV-SN represent a large, and potentially worsening, source of
world morbidity.
There is an urgent need to better understand the pathogenesis of HIV-SN, identify risk
factors, develop effective preventative strategies and improve symptom control
among existing sufferers. In Chapter 2 this thesis will explore the current evidence
base for the treatment of pain in HIV-SN by means of a systematic review and meta-
analysis of available randomised controlled trials of pharmacological agents used in
the treatment of painful HIV-SN. This work is important, as it will aid decision
making by clinicians treating painful HIV-SN and will potentially direct future
clinical efficacy trials by identifying any paucity in the literature that might need to be
addressed.
Chapter 3 of this thesis will explore in great detail the nature of the phenotype
associated with HIV-SN, with a view to gain a better understanding of the
relationships between pain symptomatology, sensory nerve dysfunction, intra-
epidermal nerve fibre density, health related quality of life, psychological co-
33
morbidity and sleep disturbance. In addition to collecting detailed medical and drug
histories, this phenotyping study will employ a battery of techniques:
Quantitative Sensory Testing (QST) using the established DFNS protocol.
Patient self-reporting instruments to exam the characteristics and existence of
psychological, health-related quality of life and sleep disturbance co-
morbidity.
Intra-epidermal sensory nerve fibre densities (IENFD) through the taking of
small skin biopsies.
This study is the first time a single cohort of HIV infected individuals have been
extensively phenotyped in this manner. Whilst there have been a number of small
detailed QST studies of HIV-SN in the pre-cART era (Bouhassira et al., 1999; Martin
et al., 2003), this study will be important as it will explore if the phenotype of HIV-
SN has changed in parallel with the change in risk factors that has occurred in the
transition from pre-cART to cART eras. The potential identification of phenotypically
distinct sub-groups, particularly with QST measures, is important as there has been
some limited evidence to suggest that such sub-groups might have a differential
response to analgesic drug therapy (D M Simpson, Scott, & Freeman, 2010).
Useful comparisons between different QST studies have been limited by the lack of
an established common QST protocol, however by using the DFNS QST protocol the
work that results from this study will be comparable to other neuropathic pain states
aiding both the study of HIV-SN and neuropathic pain per se.
There is also a need for easy to use, robust screening tools for the identification of
HIV-SN that can be translated for use into resource poor settings. Part of the
phenotyping study examined the efficacy of a number of neuropathy screening tools
(and their constituent components), some of which have not been previously validated
in the context of HIV-SN. This study will hopefully form the basis for future work
directed at producing a composite screening tool for use in resource poor settings.
As part of this study it is hoped that a blood and tissue bank for highly phenotyped
individuals with HIV-SN would be established, which would inform future work
exploring genetic risk factors for the development of HIV-SN and painful HIV-SN.
34
Chapter 2
Pharmacological treatment of painful HIV-associated sensory neuropathy

35
Pharmacological treatment of painful HIV-associated sensory neuropathy: a systematic review and meta-analysis of randomised controlled trials. Introduction
Evidence-based guidelines for the pharmacological management of neuropathic pain
tend to focus on a “blanket” approach of recommending therapies across the spectrum
of neuropathic pain, irrespective of the underlying condition (Finnerup, Sindrup, &
Jensen, 2010; RH, Dworkin et al., 2007). NICE guidance for the management of
neuropathic pain in “non-specialist settings” have adopted this approach (Tan, Barry,
Reken, Baker, & Guideline Development Group, 2010). This may not be appropriate
for HIV-SN for three main reasons. Firstly, neuropathic pain is a heterogeneous
phenomenon, both within and across underlying conditions, and evidence obtained
from the study of an analgesic in one condition cannot necessarily be applied to
another (Baron, Tölle, Gockel, Brosz, & Freynhagen, 2009; Scholz et al., 2009).
Secondly, in high, middle and low income countries the pain associated with HIV-SN
will usually be managed outside of specialist pain management clinics, so appropriate,
disease specific guidance may be required. Finally, there are a number of randomised
controlled trials (RCTs) conducted in HIV-SN, which were not identified in the NICE
guidance. Therefore, I have conducted a systematic review and meta-analysis to
elucidate the evidence base for pharmacological management of neuropathic pain in
HIV-SN.
Methods
Eligibility, data sources and search strategy
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses)
Systematic reviews and meta-analysis are important tools for the summary of
evidence accurately and reliably. They help to keep clinicians up to date, gather
together and summarise related research for patients and carers; provide a resource for
the development of clinical practice guidelines; provide summaries of previous
research to identify paucity of evidence for both researchers and funders wishing to
support new research. However, prior to the development of QUOROM, and
subsequently PRISMA, there had been much criticism of the reporting of systematic
reviews and meta-analysis; in particular poor literature searches, poor evaluation of
36
the quality of RCTs and the poor synthesis of results (Mulrow, 1987; Sacks, Berrier,
Reitman, Ancona-Berk, & Chalmers, 1987).
The QUOROM (QUality Of Reporting Of Meta-analyses) Statement, published in
1999 (Moher et al., 1999), was conceived as a guidance for authors reporting meta-
analysis of randomized trials. The QUOROM statement was developed by an
international group of thirty clinical epidemiologists, clinicians, statisticians, editors
and experienced researchers. The original QUOROM statement was subsequently
updated in 2009 to address conceptual advances in outcome level assessment (detailed
evaluation of the reliability and validity of the data for each important outcome by
determining the methods used to assess them in each individual study), and risk of
bias relevant to systematic review and meta-analysis. This updated statement
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) was
published in 2009 and comprises of a 27 item check-list and a flow-diagram
pertaining to the content of a systematic review and meta-analysis, which includes the
title, abstract, methods, results, discussion and funding. The flow diagram is four-
phased and depicts the flow of information through the different phases of a
systematic review and helps to display information about the number of records
identified in the literature searches, the number of studies included and excluded, and
the reasons for exclusions in a clear manner.
The PRISMA statement is not a quality assessment instrument for medical
intervention RCTs.
In accordance with PRISMA (Liberati et al., 2009), I sought to identify RCTs that
included patients with painful HIV-SN and reported at least one clinically relevant
pain outcome measure.
A systematic search, without language restrictions, was conducted on 20 June 2008,
and a follow-up search on 22 February 2010, with the following databases: Medline
(from 1966 to date searched), The Cochrane central register of controlled trials
(Cochrane Library 2010, Issue 2), www.clinicaltrials.gov (a US registry of clinical
trials) and www.controlled-trials.com (a meta-registry of controlled trials). By
searching registries of clinical trials it was hoped to reduce the risk of missing
‘negative’ results from unpublished trials, as this is a potential source of publication-
bias in systematic review and meta-analysis reporting.
37
Search terms
Search and Boolean logic terms used were: {“HIV” or “AIDS”} and {“pain” or
“painful”} and {“neuropathy” or “neuropathic”}, and {“treatment” or “trial” or
“random” or “randomised” or “double-blinded”}. Further trials were identified by
hand searching the reference lists of identified trials and review articles, relevant
NICE guidelines and Health Technology Assessment reports.
Study selection and risk of bias assessment
I excluded animal studies, reviews, letters, abstract-only trials, open-label trials, and
trials that were not randomised. The identified RCTs then underwent independent
quality assessment by me and another three reviewers (C. L. Cherry, S. Cox and A. S.
C. Rice) using the 7-point modified “Jadad” scoring system.
The modified Jadad scale
The Jadad assessment scale, also known as the Oxford quality scoring system, was
developed as a method to systematically assess the quality of medical intervention
RCTs (Jadad et al., 1996). The Jadad scale is a widely used RCT quality instrument in
the medical literature (Haynes, 2005).
The Jadad scale assesses three areas of an RCT that have potential to ‘bias’ its
conclusions from a ‘true’ result: randomisation, blinding and participant withdrawals/
drop-outs (the fate of all participants is known).
The Jadad scale was modified by the supervisor of this thesis (A.S.C.Rice) in
collaboration with the original authors of the Jadad scale to include an assessment of
adequate powering of an RCT. This scale is called the modified Jadad scale (A. Rice,
Lever, & Zarnegar, 2008).
The modified Jadad scale asks reviewers to answer the following for each RCT:
1. Was the study described as randomised (this includes the use of words
such as randomly, random, and randomisation)?
2. Was the study described as double blind?
3. Was there a description of withdrawals and drop-outs?
4. Was there a description of a power calculation?
38
A ‘yes’ answer to each of the above questions receives one point. Questions 1, 2 and
4 receive an extra point each if the methods used for each is appropriate. A point is
deducted from 1, 2 or 4 if the method is inappropriate or its description is unclear. A
maximum score is seven points (Supplemental Document 1: The Modified Jadad
Score).
RCTs with a score of less than five points and studies that enrolled fewer than five
HIV-SN patients were excluded from the systematic review. Scoring discrepancies
between reviewers were resolved through discussion and consensus.
Data extraction
I extracted the data from eligible RCTs. Data extracted included: year of publication;
study design and duration; study sample population and characteristics; withdrawals;
interventions; doses; pain and non-pain related primary and secondary outcome
measures; and adverse events.
Where possible, dichotomous pain improvement outcome data were extracted from
RCTs that reported efficacy superior to placebo. Intention to treat (ITT) responder
rates for 30% and 50% pain relief were sought for the longest follow-up period
reported in each study. If required, authors were contacted for missing or unreported
data.
RCTs in which the primary pain outcome of a studied intervention did not show
efficacy greater than placebo in the intention to treat population, were not included in
a subsequent meta-analysis.
Statistical analysis
For each intervention the extracted dichotomous outcomes were used to calculate
numbers needed to treat (NNT) by me and another reviewer (A. S. C. Rice), with 95%
confidence intervals for 30% and 50% pain improvement responders.
Meta-analysis
In the context of medical RCTs, meta-analysis are methods that focus on combining
results from different studies in order to obtain a quantified synthesis which increases
the power of statistical analysis by using pooled results.
39
There are three main parts to a meta-analysis:
1. Production of a pooled estimate and confidence interval for the treatment
effect after combining all the studies.
2. To test if the treatment effects seen are statistically significant or not (i.e. does
the treatment effect differ from no effect more than would be expected by
chance?)
3. To test heterogeneity of the effects outcome between the included studies (i.e.
does the effect vary across the studies more than would be expected by
chance?)
To combine the results of more than one study a summary statistic needs to be
calculated for each. This determines the treatment effect seen in each individual trail.
This treatment effect then needs to be weighted according to the importance of each
trial. In the context of RCTs this is most often the size of the trail.
Weighted average
There are two statistical models of meta-analysis:
1. Fixed effect model:
The fixed effect model provides a weighted average of a series of study effects. The
model assumes that all included studies investigate the same population, use the same
variable and outcome definitions, etc. This assumption is typically unrealistic as
RCTs are often prone to several sources of heterogeneity; e.g. treatment effects may
differ according to population studies, drug dosage, study conditions, etc .
2. Random effects model:
A common model used to synthesize heterogeneous research is the random effects
model of meta-analysis. This is simply the weighted average of the effect sizes of a
group of studies. The weight that is applied in this process of weighted averaging with
a random effects meta-analysis is achieved in two steps:
Weight = 1/√ variance of the trial estimate
1/√Standard Error (SE) of the trial
40
This ‘weighting’ is then used to multiple by the effects difference seen in each trial to
give the weighted average, which can then be used to pool with other studies.
Heterogeneity
Ideally, those studies whose results are being combined in the meta-analysis should
all be conducted in the same way and to the same protocol: study heterogeneity is a
term used to indicate that this ideal is not fully met. There are several sources of
heterogeneity. Clinical heterogeneity can be the result of different treatment protocols
or different study populations being used. Measuring study heterogeneity is
important, as it indicates where it might not be valid to pool the results of different
studies.
Identifying statistical heterogeneity requires testing the null hypothesis that the
different trials all have the same treatment effect in the population. The test looks at
the differences between observed treatment effects for the trials and the pooled
treatment effect estimate. By using the Chi-squared test with degrees of freedom (df)
and a ‘p’ value, heterogeneity can be estimated. When there are few studies, the test is
not very good at detecting heterogeneity if it is present. For this reason, a p value of
less than 0.10 is often used to indicate heterogeneity rather than the conventional cut
point of p = 0.05. A useful way to identify heterogeneity without having to use
statistical tables to look up p values is to compare the chi-square statistic with its
degrees of freedom. If the statistic is bigger than its degrees of freedom then there is
evidence of heterogeneity (The Cochrane Collaborators Open learning material).
I originally planned to assess heterogeneity as described above, however, as only
three studies were used in the meta-analysis, this was felt to be inappropriate by the
supervisor of this thesis, for reasons outlined above. Similarly, a sensitivity analysis
was not performed, as there were insufficient data. All calculations were undertaken
using Microsoft Excel 2007
Determination of Number Needed to Treat (NNT)
The NNT is a useful way of expressing the results of a medical intervention trial as it
indicates the number of patients that would have to be treated in order for one to have
benefit. To calculate NNT dichotomous outcome measures need to be available. For
41
this systematic review/meta-analysis I used the dichotomous outcome measure of >
30% or 50% improvement on a pain VAS for a given treatment and its placebo.
NNT is the inverse of the Absolute Risk Reduction (ARR).
The ARR = Placebo event rate – Treatment event rate.
NNT=1/ARR
Results
I identified 44 potentially relevant articles (Figure 2.1). Twenty-five articles were
excluded after screening identified these as being a review article, letter, open-label
study, case report or other non-RCT study. The remaining 19 RCTs were retrieved
and independently reviewed by me and other three reviewers (C. L. Cherry, S. Cox
and A. S. C. Rice). Four articles were excluded at this stage by scoring <5 out of 7-
points with the modified Jadad score. A further RCT was excluded as having <5 HIV-
SN patients enrolled. Details of these excluded RCTs, and therefore of interventions
that must be regarded as not having been adequately tested, are shown in Table 2.1.
The remaining 14 RCTs were retained for further analysis (Table 2.2). Of the 14 trials
retained for further analysis, 13 were of a parallel group design and one a cross-over
design. All were placebo controlled with one using “active” placebo (David M
Simpson, Brown, & Tobias, 2008). Data extraction was for the longest follow-up
period reported by the article. In most cases this was to the end of the treatment phase,
except for a study of a topical 8% capsaicin (David M Simpson, Brown, et al., 2008)
that reported data for 12 weeks after a single treatment application.
In two studies (Paice et al., 2000 and Hahn et al., 2004) no reference to ITT analysis
was made. In one of these RCTs studying topical capsaicin 0.075% efficacy (Paice et
al., 2000) no primary outcome data were published, as it was reported that no
superiority to placebo was seen. In a study of lamotrigine efficacy (D M Simpson et
al., 2003) only a per protocol (PP) population data analysis was undertaken. This was
reported to show no superiority over placebo; however no primary outcome data were
reported.
Of the four trials that reported superiority of an intervention over placebo, three
reported dichotomous pain outcome measures. Where possible I used responder rate
42
data for ≥30% and ≥50% improvement in pain as measured using Visual Analogue
Scale (VAS) or Numerical Pain Rating Scale (NPRS). These data were requested
from the authors if they had not been reported.
Acetyl –L-carnitine
Whilst acetyl-L-carnitine has been the subject of six articles (Chiechio, Copani,
Gereau, & Nicoletti, 2007; Hart et al., 2004; Herzmann, Johnson, & Youle, 2005;
Osio et al., 2006; Scarpini, Sacilotto, Baron, Cusini, & Scarlato, 1997; M Youle &
Osio, 2007) in the treatment of painful HIV-SN, only one was an RCT (M Youle &
Osio, 2007) and eligible for inclusion. This was a parallel group trial of acetyl-L-
carnitine (1000mg/day) and placebo intramuscular injections. In this RCT acetyl-L-
carnitine, in an analysis of the PP population, showed a modest superiority to placebo.
However an analysis of the ITT population did not show superiority to placebo: mean
change in VAS (0-10cm)(SD) from baseline to the end of week 2: acetyl-L-carnitine -
1.32 (1.84); placebo -0.61 (1.55) p=0.07. Consequently we undertook no further
analysis of this trial.
Amitriptyline and Mexilitine
Two trials (Shlay et al., 1998 and Kieburtz et al., 1998) that were included studied the
efficacy of amitriptyline. Both trials compared amitriptyline to placebo and another
intervention. One RCT (Shlay et al., 1998) examined efficacy of amitriptyline as part
of a trial also assessing acupuncture treatment. However despite being described as a
parallel group, placebo controlled RCT, its design was complex. Consequently the
results of this trial are difficult to evaluate. In particular bias may have been
introduced because of unconventional randomisation procedures and because true
placebo controls were not used. Specifically, patients were allowed to ‘opt-out’ of
being randomised to the amitriptyline arms of the trial based on personal preference.
In addition, many participants included in the analysis of amitriptyline efficacy, had
also received acupuncture or sham acupuncture, further complicating analysis.
Ignoring the methodological concerns, amitriptyline demonstrated no superiority to
placebo in the primary outcome measure. The mean change in Gracely pain scores
from baseline to week 14 was -0.26 with amitriptyline (maximum dose 75mg/day)
and -0.30 with placebo. The difference between amitriptyline and placebo was: 0.00
95%CI(-0.18 to 0.19) p=0.99.

43
The second trial (Kieburtz et al., 1998) compared amitriptyline, mexilitine and
placebo. This trial was terminated early following an interim review of results. It was
deemed by the trial monitoring board that further enrolment into the study was
unlikely to detect significant differences in either amitriptyline or mexilitine arms
compared to placebo. No superiority was reported in reducing mean Gracely pain
scores (SD) from baseline to the end of treatment week 8 for: amitriptyline (maximum
dose 100mg/day) -0.31 (0.31); mexilitine -0.23 (0.41); compared to placebo -0.20
(0.30).
Smoked Cannabis
The original literature search found four articles related to cannabinoid use and
painful HIV-SN. Only two were RCTs (Abrams et al., 2007; Ellis et al., 2009). The
excluded articles included one clinical survey (Woolridge et al., 2005) and one review
article (Beaulieu & Ware, 2007).
One of these included articles (Ellis et al., 2009) was a cross-over study that
compared the efficacy of smoked cannabis (maximum tolerated dose 1 to 8% ∆-9-
tetrahydrocannabinol q.d.s.) to placebo cigarettes in reducing subjects pain measured
using the Descriptor Differential Scale (DDS). The DDS is a ratio scale (0 to 20)
containing 24 words describing pain intensity and unpleasantness. Smoked cannabis
was reported to be superior to placebo in reducing DDS from baseline to end of
treatment day five in the PP population. The median difference between cannabis and
placebo was -3.3 out of 20; p=0.016. No data were reported for the ITT analysis,
however the authors stated that the PP analysis was similar to the ITT analysis with
p=0.02. VAS data not reported by the authors, but was supplied on request, relating
to cannabis and placebo subjects who reported a ≥30% (18/34 and 7/34 respectively)
and ≥50% (13/34 and 4/34 respectively) improvement in pain intensity.
This trial reported a high proportion of inadvertent unblinding amongst subjects
following dose titration with smoked cannabis cigarettes in the treatment arms, but
not with placebo cigarettes.
A second study (Abrams et al., 2007) compared smoked cannabis (3.56% ∆-9-
tetrahydrocannabinol t.d.s.) to placebo cigarettes in a parallel group RCT. Smoked
cannabis was shown to be superior to placebo in reducing pain from baseline to end of
treatment day 5 in the ITT analysis: cannabis -34% (IQR -71 to -16), placebo -17%
44
(IQR -29 to 8) p=0.03. More subjects reported ≥30% VAS improvement with
smoked cannabis compared to the placebo: 13/27 and 6/27 respectively.
Inclusion into the study required subjects to have had previous exposure to cannabis,
with current users asked to discontinue prior to the study. Of note no attempt was
made to assess unintentional unblinding during the course of the study, which may
have been high due to subjects’ previous experience with smoked cannabis.
Using the ITT analysis dichotomous VAS data from both trials, an NNT for smoked
cannabis was calculated as 3.38 95%CI (2.19 to 7.50) (Table 2.3)
Topical Capsaicin
Four trials (D. B. Clifford et al., 2012; Paice et al., 2000; David M Simpson,
Estanislao, Brown, & Sampson, 2008 and D. Clifford, Simpson, Brown, Moyle, &
Brew, 2010) were found that assessed topical capsaicin efficacy in painful HIV-SN.
Two reports were excluded from further analysis; one was an open-label study (David
M Simpson, Brown, et al., 2008) and the other has been reported in abstract form only
(D. Clifford et al., 2010). Of the included trials, one (Paice et al., 2000) examined the
efficacy of topical capsaicin 0.075% cream in a parallel group RCT. The authors
stated that no superiority of capsaicin 0.075% over placebo in mean improvement in a
numeric rating score (NRS) (0-10) was seen, however only graphical data were
presented.
A second study (David M Simpson, Brown, et al., 2008) examined topical capsaicin
8%. Patients received either the 8% patch or an active placebo (capsaicin 0.04%) in a
single application lasting either 30, 60 or 90 minutes. Following this single
application patients were followed-up for 12 weeks. Capsaicin 8% was found to be
superior to placebo in the percentage reduction of the NPRS (SD) from baseline to
week 2 to 12: 8% capsaicin: -22.8 (30.6); compared to placebo: -10.7 (30.8),
(p=0.0026). The study also reported responder rates as percentage of patients
measured on the NPRS who experienced ≥30% mean reduction in pain: capsaicin 8%:
76/225; placebo (capsaicin 0.04%): 15/82; p=0.0092. It is not possible to calculate an
NNT that is strictly comparable to those calculated for other studies included in this
review since the placebo control used here was not pharmacologically inactive.
However, as an informative exercise using these data, and presuming that the control
45
capsaicin 0.04% is a true placebo, an NNT of 6.46 95%CI(3.86-19.69) was calculated
for treatment with capsaicin 8% patch.
Gabapentin
Only one retrieved report related to treatment of painful HIV-SN with gabapentin was
an RCT. Four additional articles were excluded. Two were letters (Newshan, 1998;
Vadivelu & Berger, 1999) one an abstract (Gatti, Antonella, Jann, Stefano, & Sandro,
1998), and one a case series (La Spina, Porazzi, Maggiolo, Bottura, & Suter, 2001).
The included study (Hahn et al., 2004) compared gabapentin (titrated to a maximum
of 2400mg/day) to placebo in a parallel group RCT. At the longest treatment period
assessed, no difference in efficacy was reported between gabapentin and placebo
groups for the primary outcome measure, median change in VAS (0-100mm) baseline
to end of week 4: gabapentin: - 44.1, placebo: -29.8. No indication of variance or p
value was documented.
It is noteworthy that this trial demonstrated an unusual placebo response. The placebo
subjects’ pain VAS baseline remained unchanged for the first two weeks, after which
a stronger placebo response followed to week 4. This unusual placebo response may
have contributed to the apparent superiority of gabapentin over placebo at week 2,
which was not evident at week 4.
Pregabalin
One large multi-centre RCT (D M Simpson, Schifitto, et al., 2010)[50] examined the
efficacy of pregabalin, titrated over 2 weeks to a maximum tolerated dose up to
1200mg/day, in a multicentre, 14 week parallel group, placebo controlled RCT. No
superiority of pregabalin over placebo in the primary pain outcome measure was
reported: mean change in NPRS baseline to end of week 14: pregabalin -2.88; placebo
-2.63, p=0.39.
Lamotrigine
Three trials assessing the efficacy of lamotrigine in painful HIV-SN were identified
(Silver, Blum, Grainger, Hammer, & Quessy, 2007; D M Simpson et al., 2000 and D
M Simpson et al., 2003). One trial (Silver et al., 2007), enrolled only one painful
HIV-SN patient (to the placebo control group) and was therefore excluded from
further analysis. The included lamotrigine trials (D M Simpson et al., 2000) and (D M
46
Simpson et al., 2003) were both conducted by the same group; with (D M Simpson et
al., 2000) being smaller and preceding (D M Simpson et al., 2003). The smaller study
(D M Simpson et al., 2000) did demonstrate some efficacy superior to placebo when
the primary outcome for the PP population was analysed. However in the ITT
analysis with ‘last value carried forward’ (LVCF), lamotrigine was not superior to
placebo: improvement in mean Gracely pain score (SE): lamotrigine: – 0.242
(0.009); placebo: -0.183 (0.087); (p=0.65). The large number of dropouts in the
lamotrigine group (n= 11 of 20) compared to placebo (n=3 of 22) suggest a narrow
therapeutic index and make interpretation of the trial results difficult.
Similarly the larger trial (D M Simpson et al., 2003), where participants were
stratified according to previous exposure to neurotoxic ARVs, did not demonstrate a
superiority of lamotrigine over placebo for the primary outcome measure (mean
improvement in Gracely pain score) in the total cohort or in either stratum. However
lamotrigine did show superiority to placebo in the neurotoxic ARV-exposed stratum
in a secondary outcome measure, mean improvement in VAS (0-100mm) baseline to
end of treatment: lamotrigine: -27.1; compared to placebo: -9.0; p=0.003.
For each stratum the number of responders (≥30% improvement in VAS) were
calculated from the published data. For the neurotoxic ARV stratum: lamotrigine
36/62, placebo 7/30 (p=0.02) and for no exposure to neurotoxic ART: lamotrigine
46/88, placebo 21/47. As an informative exercise using these data the NNT for
lamotrigine was calculated for each stratum, and for the overall trial. Subjects with
exposure to neurotoxic ARVs: 2.88 95%CI(1.84 to 6.57); no exposure to neurotoxic
ARVs: 13.17 95%CI(3.96 to -9.95) and for the unstratified population: 6.09
95%CI(3.51 to 23.08)(Not included in Table 2.3 as no superiority of lamotrigine over
placebo was demonstrated for any primary endpoint).
Recombinant human Nerve Growth Factor (rhNGF)
One RCT (J C McArthur et al., 2000) examined the efficacy of subcutaneous
recombinant human Nerve Growth Factor (rhNGF) in the treatment of painful HIV-
SN. This study assessed two doses (0.1 and 0.3μg/kg) given twice weekly compared
with placebo for 18 weeks. rhNGF was superior to placebo for the primary outcome
measure in the ITT analysis; median change of the Gracely pain score from baseline
47
to end of week 18: rhNGF 0.1μg/kg: -0.18 (-0.10 to -0.25) p=0.05, 0.3μg/kg: -0.21 (-
0.14 to -0.29) p=0.04, and placebo: 0.06 (+0.01 to -0.14)
No significant dose effect was reported and no differential effect was seen based on
baseline stratification of subjects according to neurotoxic ARV drug exposure. As
rhNGF was reported to be associated with myalgia, there may have been inadvertent
breaking of the blinding.
Dichotomous data were requested from the authors however we were unable to
calculate RR and NNT values for rhNGF from the data provided.
Prosaptide and Peptide –T
Two trials (Evans et al., 2007; D M Simpson et al., 1996) examined the efficacy of
the novel agents in placebo controlled parallel group RCTs. One (Evans et al., 2007)
reported the use of subcutaneous prosaptide (maximum dose of 16mg/day) over 6
treatment weeks and did not report efficacy superior to placebo in the primary
outcome measure; mean change in Gracely pain score baseline to week 6. The study
was terminated after a planned interim futility analysis. Another trial (D M Simpson
et al., 1996) studied efficacy of intranasal peptide T (maximum dose 6mg/day), over
12 treatment weeks, but reported no superiority over placebo in the primary outcome
measure; mean change in a modified Gracely pain score baseline to end of week 12.
Discussion
This systematic review found that RCT evidence of analgesic efficacy superior to
placebo in the context of HIV-SN pain exists only for smoked cannabis, rhNGF and
high dose (8%) topical capsaicin. Several other agents have been examined in high
quality RCTs and found to be no more effective than placebo for managing HIV-SN
pain in the doses used, specifically acetyl-L carnitine (1g/day), amitriptyline
(100mg/day), topical capsaicin 0.075%, gabapentin (2.4g/day), mexilitine
(600mg/day), peptide –T (6mg/day), pregabalin (1200mg/day), lamotrigine
(600mg/day) and prosaptide (16mg/day). Therefore, there is evidence that both of the
first line therapies (pregabalin and amitriptyline) recommended in the NICE guidance
for non-specialist management of neuropathic pain show no superiority to placebo in
the management of pain in HIV-SN (Tan et al., 2010).
48
Of the pharmacological interventions shown to be effective for HIV-SN in RCTs,
only topical capsaicin 8% is currently approved for marketing for neuropathic pain
indications. In Europe 8% capsaicin has been approved for the treatment of peripheral
neuropathic pain in non-diabetic adults, whilst the U.S. Food and Drug
Administration (FDA) has approved its use only for the indication of post herpetic
neuralgia. However, it should also be borne in mind that we located a preliminary
report (conference abstract only and therefore excluded from the systematic review)
of another parallel group RCT which included 494 patients with HIV-SN in which
topical 8% capsaicin was compared to 0.04% topical capsaicin (D. Clifford et al.,
2010). No analgesic superiority of 8% capsaicin over 0.04% was demonstrated.
rhNGF therapy is not currently clinically available and both legal and mental health
issues preclude routine recommendation of long term smoked cannabis for pain
management (A. S. C. Rice, 2008).
This systematic review represents a comprehensive review of the literature relating to
the pharmacological management of painful HIV-SN. It used a predefined protocol
for the initial literature search, data extraction and analysis. There was also strict
adherence to inclusion quality criteria as assessed by four independent reviewers
using the modified Jadad score, a tool that assesses each study for potential bias as
well as evaluating study power.
This systematic review was limited by the paucity of high quality RCTs examining
pharmacological treatment of painful HIV-SN. Additionally the heterogeneity of the
included studies design and size made evaluation and comparison of trials difficult. In
particular, use of the Gracely pain scale (GPS) in five of the 14 included RCTs made
evaluation and inter-study comparison complicated. The GPS is a log unit pain
outcome measure that is not a frequently used measure outside trials of HIV-SN. In a
recent consensus statement regarding core chronic pain outcome measures (Dworkin,
Katz, & Gitlin, 2005) it was not one of the recommended pain scales. Several of the
studies utilising the Gracely pain score also included more validated secondary pain
outcome measures such as either a VAS score or a NPRS. These were used here in
preference to the Gracely pain score in the calculation of NNT and RR.
The Jadad tool has been validated and used widely to identify common and major
sources of experimental bias in RCTs identified in systematic reviews. Nevertheless,
whilst the use of the modified Jadad score improves the probability that only high
49
quality RCTs were included in the systematic review, its use may conceivably have
biased our systematic review in favour of more recently tested agents. The RCTs
associated with these agents now routinely report the information required by the
modified Jadad tool, because of the nature of the evolution of RCT methodology over
the past few years.
Both of the RCTs that examined the efficacy of smoked cannabis, were of high
quality, however the apparent marked superiority of smoked cannabis to placebo
cigarettes should be tempered by the high proportion of potential unblinding
measured in (Ellis et al., 2009) (92% correctly guessing treatment allocation after
treatment cross-over), and its lack of measurement in (Abrams et al., 2007) despite
participants having all had previous experience of smoked cannabis. In a similar
manner, the RCT investigating recombinant human NGF demonstrated a high degree
of unblinding related to injection site myalgia, which when accounted for in a
separate analysis reported a more attenuated treatment-related difference which
consequently lost statistical significance.
Lamotrigine was the subject of two high quality RCTs. Both failed to show
superiority over placebo in the primary pain outcome measure, improvement in the
GPS in the ITT population. However, in the larger of the two RCTs, analysis of a
secondary pain outcome measure, mean improvement in VAS, did demonstrate
efficacy superior to placebo in the subpopulation of subjects who had been previously
exposed to neurotoxic ARTs. If this stratum alone is examined an NNT of 2.88 is
calculated.
Most of the included RCTs did not stratify subjects with painful HIV-SN according to
their exposure to neurotoxic ARTs. This stratification was instrumental in
demonstrating an efficacy of lamotrigine in neurotoxic ART exposed painful HIV-SN
subjects. It is possible to speculate that a similar strategy of stratifying other RCTs
might have elucidated other agents with sub-group efficacy, despite lack of observed
analgesic efficacy in an unstratified painful HIV-SN subject population. Additionally,
the included RCTs were not uniform in their approach to the use of concomitant
analgesics; whilst most allowed continued use of drugs at stable doses, two elected to
stop them (Evans et al., 2007; Hahn et al., 2004). The use of such concomitant
analgesics, and also the inclusion of participants with previously failed therapies, may
conceivably have influenced the outcomes of these RCTs.
50
Gabapentin and pregabalin were the subject of two high quality RCTs in which
neither agent was shown to be superior to placebo. This contrasts with the efficacy of
these agents demonstrated in other peripheral neuropathic pain conditions (Finnerup
et al., 2010; Hempenstall, Nurmikko, Johnson, A’Hern, & Rice, 2005; RH, Dworkin
et al., 2007; Tan et al., 2010). However the gabapentin study was small, with only 30
patients randomised (Hahn et al., 2004). This finding may therefore represent a ‘failed
trial’ rather than a true lack of efficacy.
Amitriptyline efficacy was examined in two large RCTs. The evaluation of one study
(Shlay et al., 1998) was made difficult by a complicated study design that may have
not been truly randomised or placebo controlled. However the finding that
amitriptyline did not display superior analgesic efficacy than placebo in the context of
HIV-SN is supported by a similar finding a second, higher quality RCT (Kieburtz et
al., 1998). Again, this finding directly contrasts with evidence of efficacy for tricyclic
antidepressants in a range of other peripheral neuropathic pain conditions (Finnerup et
al., 2010; Hempenstall et al., 2005; RH, Dworkin et al., 2007; Tan et al., 2010).
Capsaicin 0.075% cream was the subject of a small RCT enrolling only 26 subjects.
The authors stated that capsaicin 0.075% did not demonstrate statistically significant
superiority to placebo in the primary pain outcome measure. However, outcome data
were published only in a graphical representation of mean current pain scores from
baseline to the end of treatment. From this graph there does appear to be a trend for
capsaicin to be superior to placebo at this final time point measured at week 4.
However a high drop-out rate in both arms resulted in only 6/11 patients remaining in
the capsaicin group, and only 8/15 in the placebo group. It is therefore difficult to
determine from this study if capsaicin 0.075% was indeed without efficacy. This has
two implications: the first being that capsaicin 0.075% might have some degree of
clinically relevant efficacy in painful HIV-SN; and secondly, if capsaicin 0.075% is
indeed efficacious, then the use of a similar concentration (capsaicin 0.04%) as an
active placebo in the large capsaicin 8% patch RCT would change the design of this
study from a placebo controlled to a superiority approach.
In the treatment of painful HIV-SN, the lack of efficacy compared with placebo of
many agents with proven efficacy in other forms of neuropathic pain has implications
in the understanding of neuropathic pain in general. These findings further support the
hypothesis that neuropathic pain cannot be considered as a single symptom with a
51
single pathogenesis (Baron et al., 2009; Scholz et al., 2009). A more mechanistic
approach to the treatment of specific types of neuropathic pain is therefore warranted
as has been established in trigeminal neuralgia and post herpetic neuralgia. Equally,
caution should be exercised in the use of neuropathic pain treatment algorithms that
do not consider these potential mechanistic differences, as their rationale may be
fundamentally flawed.
The absence of studies examining the efficacy of opioid use in painful HIV-SN is
notable and mandates additional research. Opioids have shown efficacy in other
neuropathic pain conditions (Finnerup et al., 2010; Hempenstall et al., 2005; RH,
Dworkin et al., 2007). Furthermore, the efficacy of duloxetine in diabetic neuropathy,
a condition that has similarities to HIV-SN, may suggest that it is worth investigating
(Tan et al., 2010). In addition, the efficacy of cannabis in HIV-SN would suggest that
cannabinoids with an appropriate therapeutic index when delivered by a mechanism
other than smoking might be worthy of investigation (A. S. C. Rice, 2008).
Summary
On the basis of current published evidence, topical capsaicin 8%, smoked cannabis
and Nerve Growth Factor have evidence of efficacy in pain associated with HIV-SN.
However the apparent efficacy of capsaicin is contentious, as a larger RCT, reported
in abstract form only at the time of this systematic review, suggested this treatment is
not superior to placebo (D. Clifford et al., 2010). Some commonly recommended
analgesics, including opioids, have not been formally studied for the management of
painful HIV-SN.
The current evidence base available for the treatment of painful HIV-SN is at odds
with the recommendations made by NICE for neuropathic pain management in the
non-specialist situation. This indicates the potential dangers of extrapolating efficacy
from one neuropathic pain condition to another where efficacy has not been directly
assessed. In particular amitriptyline, pregabalin, and gabapentin have been
demonstrated to have no superiority to placebo in the treatment of painful HIV-SN.
With an estimated 33 million people living with HIV and more gaining access to
ARV every day, the management of HIV-SN associated neuropathic pain is a problem
of major global significance. There is an urgent need for the development of effective;
evidence based analgesic strategies for this common condition. On-going evaluation
52
of both novel analgesics and existing untested strategies for HIV-SN is a clear
research priority.
Update Search
On December 15th 2013 follow-up literature search limited to Medline (from 1966 to
date searched) was conducted using the same search terms used for the above
systematic review.
Only two additional RCTs were identified as being potentially relevant to the above
systematic review.
One was a high quality RCT that had been previously only reported in abstract form,
but mentioned in the systematic review discussion (D. B. Clifford et al., 2012). This
RCT was a high quality active placebo controlled with n=332 painful HIV-SN
participants for capsaicin 8% patch for either 30 or 60min and n=162 painful HIV-SN
who received active placebo (0.04% capsaicin patch). The treatment group showed no
statistically significant superiority to placebo at any time point from week 2 to week
12 for the primary outcome Numeric Pain Rating Scale score or for the secondary
outcome measure of Patients Impression of Change at week 12.
A second RCT of capsaicin 8% patch was identified comparing capsaicin with three
topical anaesthetic preparations (Webster, Peppin, Murphy, Tobias, & Vanhove,
2012). This RCT included n=117 participants with neuropathic pain, however only
one participant with painful HIV-SN was entered; this RCT would therefore not be
suitable for inclusion in the above systematic review.
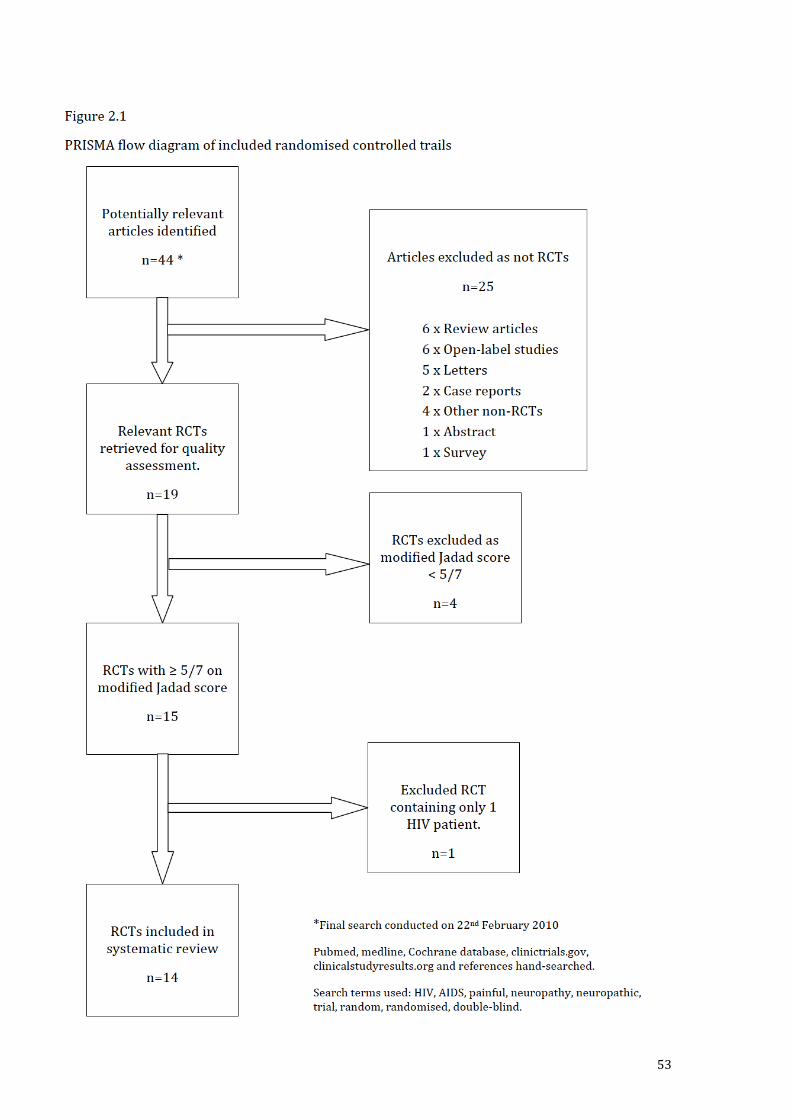
53
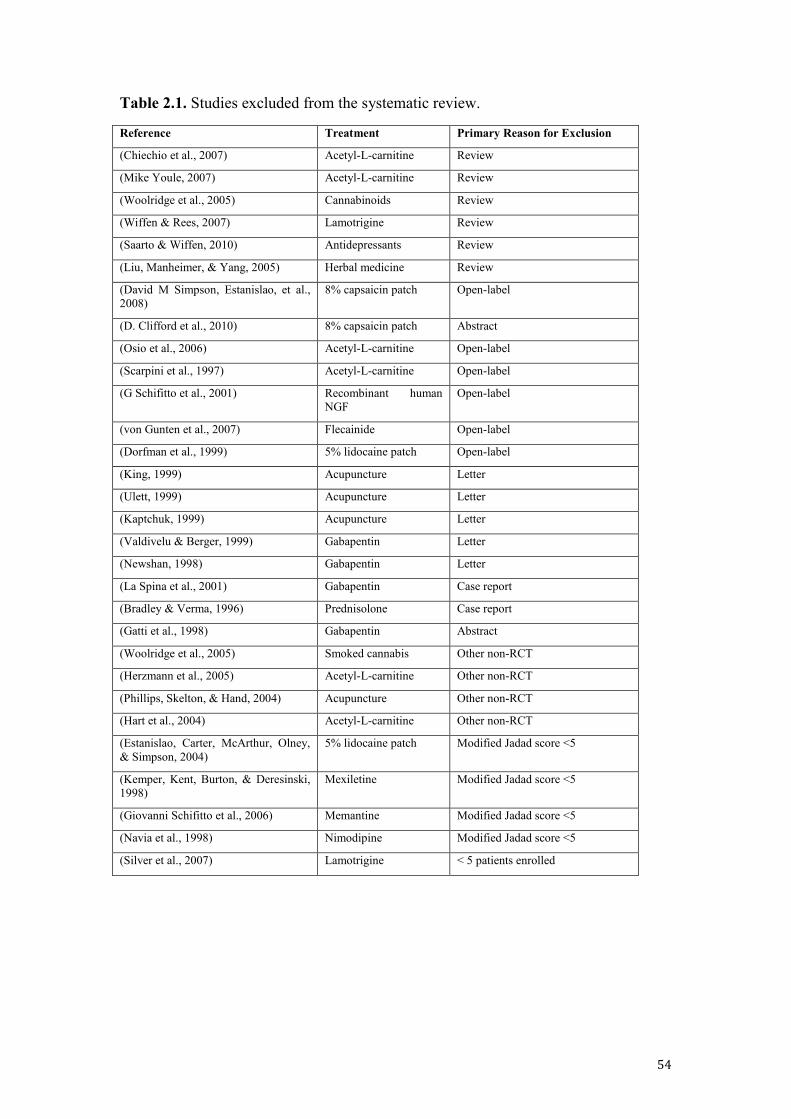
54
Table 2.1. Studies excluded from the systematic review.
Reference Treatment Primary Reason for Exclusion
(Chiechio et al., 2007) Acetyl-L-carnitine Review
(Mike Youle, 2007) Acetyl-L-carnitine Review
(Woolridge et al., 2005) Cannabinoids Review
(Wiffen & Rees, 2007) Lamotrigine Review
(Saarto & Wiffen, 2010) Antidepressants Review
(Liu, Manheimer, & Yang, 2005) Herbal medicine Review
(David M Simpson, Estanislao, et al., 2008)
8% capsaicin patch Open-label
(D. Clifford et al., 2010) 8% capsaicin patch Abstract
(Osio et al., 2006) Acetyl-L-carnitine Open-label
(Scarpini et al., 1997) Acetyl-L-carnitine Open-label
(G Schifitto et al., 2001) Recombinant human NGF
Open-label
(von Gunten et al., 2007) Flecainide Open-label
(Dorfman et al., 1999) 5% lidocaine patch Open-label
(King, 1999) Acupuncture Letter
(Ulett, 1999) Acupuncture Letter
(Kaptchuk, 1999) Acupuncture Letter
(Valdivelu & Berger, 1999) Gabapentin Letter
(Newshan, 1998) Gabapentin Letter
(La Spina et al., 2001) Gabapentin Case report
(Bradley & Verma, 1996) Prednisolone Case report
(Gatti et al., 1998) Gabapentin Abstract
(Woolridge et al., 2005) Smoked cannabis Other non-RCT
(Herzmann et al., 2005) Acetyl-L-carnitine Other non-RCT
(Phillips, Skelton, & Hand, 2004) Acupuncture Other non-RCT
(Hart et al., 2004) Acetyl-L-carnitine Other non-RCT
(Estanislao, Carter, McArthur, Olney, & Simpson, 2004)
5% lidocaine patch Modified Jadad score <5
(Kemper, Kent, Burton, & Deresinski, 1998)
Mexiletine Modified Jadad score <5
(Giovanni Schifitto et al., 2006) Memantine Modified Jadad score <5
(Navia et al., 1998) Nimodipine Modified Jadad score <5
(Silver et al., 2007) Lamotrigine < 5 patients enrolled
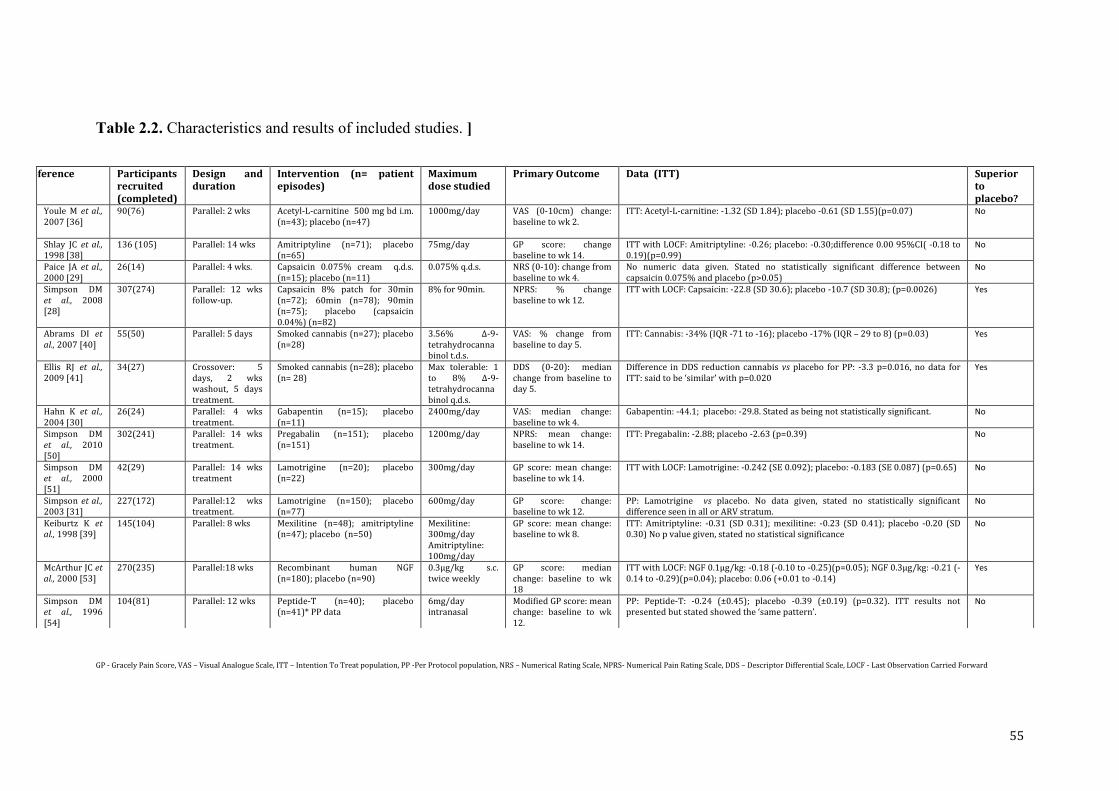
55
Table 2.2. Characteristics and results of included studies. ]
GP - Gracely Pain Score, VAS – Visual Analogue Scale, ITT – Intention To Treat population, PP -Per Protocol population, NRS – Numerical Rating Scale, NPRS- Numerical Pain Rating Scale, DDS – Descriptor Differential Scale, LOCF - Last Observation Carried Forward
Reference Participants recruited (completed)
Design and duration
Intervention (n= patient episodes)
Maximum dose studied
Primary Outcome Data (ITT) Superior to placebo?
Youle M et al., 2007 [36]
90(76) Parallel: 2 wks Acetyl-L-carnitine 500 mg bd i.m. (n=43); placebo (n=47)
1000mg/day VAS (0-10cm) change: baseline to wk 2.
ITT: Acetyl-L-carnitine: -1.32 (SD 1.84); placebo -0.61 (SD 1.55)(p=0.07) No
Shlay JC et al., 1998 [38]
136 (105) Parallel: 14 wks Amitriptyline (n=71); placebo (n=65)
75mg/day GP score: change baseline to wk 14.
ITT with LOCF: Amitriptyline: -0.26; placebo: -0.30;difference 0.00 95%CI( -0.18 to 0.19)(p=0.99)
No
Paice JA et al., 2000 [29]
26(14) Parallel: 4 wks. Capsaicin 0.075% cream q.d.s. (n=15); placebo (n=11)
0.075% q.d.s. NRS (0-10): change from baseline to wk 4.
No numeric data given. Stated no statistically significant difference between capsaicin 0.075% and placebo (p>0.05)
No
Simpson DM et al., 2008 [28]
307(274) Parallel: 12 wks follow-up.
Capsaicin 8% patch for 30min (n=72); 60min (n=78); 90min (n=75); placebo (capsaicin 0.04%) (n=82)
8% for 90min. NPRS: % change baseline to wk 12.
ITT with LOCF: Capsaicin: -22.8 (SD 30.6); placebo -10.7 (SD 30.8); (p=0.0026) Yes
Abrams DI et al., 2007 [40]
55(50) Parallel: 5 days Smoked cannabis (n=27); placebo (n=28)
3.56% ∆-9- tetrahydrocannabinol t.d.s.
VAS: % change from baseline to day 5.
ITT: Cannabis: -34% (IQR -71 to -16); placebo -17% (IQR – 29 to 8) (p=0.03) Yes
Ellis RJ et al., 2009 [41]
34(27) Crossover: 5 days, 2 wks washout, 5 days treatment.
Smoked cannabis (n=28); placebo (n= 28)
Max tolerable: 1 to 8% ∆-9- tetrahydrocannabinol q.d.s.
DDS (0-20): median change from baseline to day 5.
Difference in DDS reduction cannabis vs placebo for PP: -3.3 p=0.016, no data for ITT: said to be ‘similar’ with p=0.020
Yes
Hahn K et al., 2004 [30]
26(24) Parallel: 4 wks treatment.
Gabapentin (n=15); placebo (n=11)
2400mg/day VAS: median change: baseline to wk 4.
Gabapentin: -44.1; placebo: -29.8. Stated as being not statistically significant. No
Simpson DM et al., 2010 [50]
302(241) Parallel: 14 wks treatment.
Pregabalin (n=151); placebo (n=151)
1200mg/day NPRS: mean change: baseline to wk 14.
ITT: Pregabalin: -2.88; placebo -2.63 (p=0.39) No
Simpson DM et al., 2000 [51]
42(29) Parallel: 14 wks treatment
Lamotrigine (n=20); placebo (n=22)
300mg/day GP score: mean change: baseline to wk 14.
ITT with LOCF: Lamotrigine: -0.242 (SE 0.092); placebo: -0.183 (SE 0.087) (p=0.65) No
Simpson et al., 2003 [31]
227(172) Parallel:12 wks treatment.
Lamotrigine (n=150); placebo (n=77)
600mg/day GP score: change: baseline to wk 12.
PP: Lamotrigine vs placebo. No data given, stated no statistically significant difference seen in all or ARV stratum.
No
Keiburtz K et al., 1998 [39]
145(104) Parallel: 8 wks Mexilitine (n=48); amitriptyline (n=47); placebo (n=50)
Mexilitine: 300mg/day Amitriptyline: 100mg/day
GP score: mean change: baseline to wk 8.
ITT: Amitriptyline: -0.31 (SD 0.31); mexilitine: -0.23 (SD 0.41); placebo -0.20 (SD 0.30) No p value given, stated no statistical significance
No
McArthur JC et al., 2000 [53]
270(235) Parallel:18 wks Recombinant human NGF (n=180); placebo (n=90)
0.3μg/kg s.c. twice weekly
GP score: median change: baseline to wk 18
ITT with LOCF: NGF 0.1μg/kg: -0.18 (-0.10 to -0.25)(p=0.05); NGF 0.3μg/kg: -0.21 (-0.14 to -0.29)(p=0.04); placebo: 0.06 (+0.01 to -0.14)
Yes
Simpson DM et al., 1996 [54]
104(81) Parallel: 12 wks Peptide-T (n=40); placebo (n=41)* PP data
6mg/day intranasal
Modified GP score: mean change: baseline to wk 12.
PP: Peptide-T: -0.24 (±0.45); placebo -0.39 (±0.19) (p=0.32). ITT results not presented but stated showed the ‘same pattern’.
No
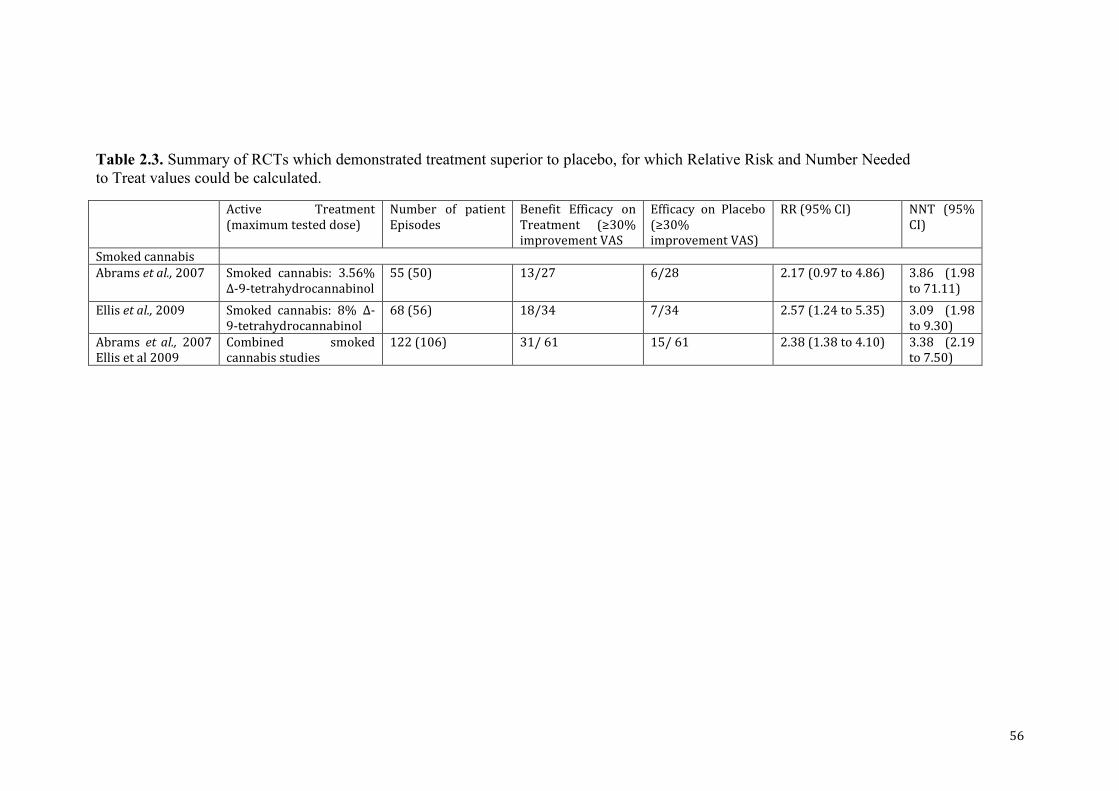
56
Table 2.3. Summary of RCTs which demonstrated treatment superior to placebo, for which Relative Risk and Number Needed to Treat values could be calculated.
Active Treatment (maximum tested dose)
Number of patient Episodes
Benefit Efficacy on Treatment (≥30% improvement VAS
Efficacy on Placebo (≥30% improvement VAS)
RR (95% CI) NNT (95% CI)
Smoked cannabis Abrams et al., 2007 Smoked cannabis: 3.56%
∆-9-tetrahydrocannabinol 55 (50) 13/27 6/28 2.17 (0.97 to 4.86) 3.86 (1.98
to 71.11)
Ellis et al., 2009 Smoked cannabis: 8% ∆-9-tetrahydrocannabinol
68 (56) 18/34 7/34 2.57 (1.24 to 5.35) 3.09 (1.98 to 9.30)
Abrams et al., 2007 Ellis et al 2009
Combined smoked cannabis studies
122 (106) 31/ 61 15/ 61 2.38 (1.38 to 4.10) 3.38 (2.19 to 7.50)
57
Chapter 3
Patterns of sensory, psychological and metabolic dysfunction in HIV positive patients with and without HIV-associated peripheral neuropathy.
58
Patterns of sensory, psychological, and metabolic dysfunction in HIV positive patients with and without HIV-associated peripheral neuropathy.
Introduction.
Established risk factors associated with the development of HIV-SN include advancing
age, height, lower nadir CD4 counts, high viral titres, and exposure to the neurotoxic
‘d’ NRTI class of antiretroviral agents. Crucially, despite the phasing out of neurotoxic
dNRTI drugs, especially in well-resourced countries, the prevalence of HIV-SN has
remained consistently at around 40%, suggesting that drug induced neurotoxicity may
not be a major aetiological factor for HIV-SN in the cART-era (Catherine Louise
Cherry et al., 2012; Ellis et al., 2010; Smyth et al., 2007). More recent cART-era
population and genetic association studies have identified additional patient related risk
factors such as ethnicity, elevated plasma triglycerides (Banerjee et al., 2011), the
expression of genes involved in the peripheral inflammatory response and those
affecting mitochondrial function (Kamerman, Wadley, & Cherry, 2012). Whilst there
have been several epidemiological studies documenting the prevalence and risk factors
for HIV-SN in the current cART era; profiling studies directed at describing in detail
the HIV-SN phenotype are lacking. Specifically, factors which are crucial to
understanding the nature of HIV-SN, such as the relationships between sensory nerve
dysfunction, symptomatology, clinical signs, patient quality of life, psychological co-
morbidity and sleep disturbance in HIV-SN are required.
There have been few studies that have attempted to describe in detail the HIV-SN
phenotype in the cART era (Bouhassira et al., 1999; Martin et al., 2003).
I have therefore conducted detailed profiling of a cohort of HIV positive patients, with
and without HIV-SN, using a battery of techniques directed at understanding the nature
and pattern of sensory nerve dysfunction in HIV-SN and its relationship to
symptomatology, psychological and circadian rhythm disruption.
59
Methods.
Study design and participants
The Pain In Neuropathy Study - HIV (PINS-HIV) was an observational single cohort
cross-sectional study conducted at Chelsea and Westminster Hospital NHS Trust
London. The study protocol was assessed and approved by a local ethics committee
(Riverside Research Ethics Committee; NRES number: 09/H0706/24). Subjects
participated in the study after giving written informed consent.
Participants were recruited between July 7th 2009 and January 25th 2011 from
ambulatory HIV infected patients attending the St Stephen’s Centre, Chelsea and
Westminster Hospital NHS Trust London. In order to reflect the population treated at
one of Europe’s major HIV centres, the inclusion criteria were as inclusive as possible.
Eligible persons were all HIV infected adults (≥18 yrs of age) irrespective of
concurrent or previous ARV treatment, or the presence of symptoms of a peripheral
neuropathy. Exclusion criteria included pregnancy, co-incident major psychiatric
disorders (DSM-IV), poor or no English language skills, pain ≥4/10 on a numerical
rating scale (NRS) from a cause other than a peripheral neuropathy at recruitment,
patients with central nervous system lesions, subjects with insufficient mental capacity
to obtain informed consent from or complete the study questionnaires. Skin biopsies
were not conducted on anticoagulated patients, or who had any other contra-indication
to skin biopsy.
The study design consisted of a single clinical assessment appointment, at the end of
which participants were given a questionnaire pack to complete and return to the study
centre by post.
During the clinical assessment appointment participants had detailed medical and drug
histories taken by a study investigator recording: gender, age, ethnicity, past medical
history, date of HIV diagnosis, presence of a family history of neuropathy, presence of
other potential causes of neuropathy (hypothyroidism, diabetes, alcohol abuse, vitamin
B12 deficiency, isoniazid and chemotherapy drug exposure); smoking and alcohol
consumption assessed using UK Department of Health method (Hedges, 1996).
60
Following this, basic clinical parameters were measured for each participant: weight,
height and lying/standing blood pressures. Participants then underwent a Structured
Neurological Examination (SNE), a detailed Quantitative Sensory Testing (QST)
assessment and skin biopsy sampling as described below. Each participant had 30mls
of blood drawn and stored for future genotype studies.
Following the clinical assessment appointment the study investigator collected further
drug, laboratory and clinical investigation data from the clinical records. The following
clinical data was collected: detailed ARV drug histories; nerve conduction study data;
the most recent routine haematological and biochemical tests: HIV-viral load, CD4+
counts, plasma electrolytes, liver function enzymes, vitamin B12, thyroid function,
blood glucose, plasma lipid profiles, and Hepatitis B, Hepatitis C and Syphilis serology
(Supplemental Document 1: PINS-HIV CRF).
Quantitative sensory testing (QST)
Sensory profiles were measured using the German Research Network on Neuropathic
Pain (DFNS) QST protocol. Measurements were performed bilaterally in the S1
dermatome at the dorsum of feet. The DFNS has developed and validated a
comprehensive QST battery which uses standardised equipment, paradigms and verbal
instructions as described (Rolke, 2006; Rolke et al., 2006). This method has been used
in multiple investigations of different neuropathic pain conditions to phenotypically
characterise patterns of sensory nerve dysfunction (Gierthmühlen et al., 2012;
Konopka et al., 2012; Maier et al., 2010).
The DFNS QST protocol assesses the functional characteristics of both small and large
afferent fibres by recording responses to 13 thermal and mechanical stimuli. These are
described elsewhere in detail and have not been duplicated here (Rolke, 2006; Rolke et
al., 2006). In brief, the DFNS QST battery test the following modalities in the order:
cold detection threshold (CDT), warm detection threshold (WDT), thermal sensory
limen (TSL), the presence of paradoxical heat sensations (PHS), cold pain threshold
(CPT), heat pain threshold (HPT), mechanical detection threshold (MDT), mechanical
pain threshold (MPT), a stimulus response function for pinprick sensitivity (MPS:
mechanical pain sensitivity), allodynia (DMA: dynamic mechanical allodynia), wind-
up ratio (WUR), vibration detection threshold (VDT), and blunt pressure pain
61
threshold (PPT).
Me and the other QST operator (M. R. D. Brown) underwent a formal course of
instruction in conducting the DFNS QST protocol at Mannheim University using
healthy volunteers. On return to the UK investigation centre, for quality control
purposes each investigator was required to produce QST data sets for 18 healthy
volunteer controls which were age and sex matched to DFNS requirements: equal
number of male and female participants. Healthy volunteers were recruited through
local departmental advertisement targeting students and employees of Imperial College
London. Inclusion as healthy volunteer data required participants to have responses to
vibration, warm and cold threshold detection, within the normal standardised DFNS
values. Potential participants were excluded if they presented with a neurological,
vascular or psychiatric disorder or a chronic pain condition; diabetes mellitus; or were
taking medication with potential central or peripheral nervous system effects, this
included benzodiazepines, triptanes or cortisone preparations.
The healthy volunteer control data were subsequently analysed and critiqued by the
DFNS to provide quality assurances for the study centre and QST investigators.
Additionally normative data for suprathreshold heat testing (as outlined below) were
collected from each healthy control subject after the completion of the DFNS QST
protocol.
QST equipment
DFNS specification compliant QST equipment was used in the study as described
below.
Thermal threshold detection
Sensory and nociceptive thermal thresholds were determined using a SOMEDIC
MSA100 thermal stimulator (SOMEDIC AB, Hörby, Sweden) using a fluid cooled
Peltier element thermode measuring 25 x 50mm. Base line temperature 320C; ramped
stimuli at 10Cs-1 using method of limits. Threshold values of cold detection (CDT) and
warm detection (WDT) were first determined in triplicate. A thermal sensory limen of
alternating warm and cold stimuli determined the presence of paradoxical heat
sensations to cold stimuli (PHS).
62
Mechanical detection threshold
MDT was assessed using a standardized set of modified von Frey filaments (Optihair2-
Set, Marstock Nervtest, Schreisheim, Germany) exerting forces between 0.25 and 512
mN. The contact area of the von Frey hairs with the skin was a rounded tip (0.5 mm in
diameter) to avoid sharp edges that would cause nociceptor activation.
Mechanical pain threshold
MPT was assessed using custom-made weighted pinprick stimuli with fixed stimulus
intensities (8, 16, 32, 64, 128, 256, 512 mN; flat contact area of 0.25 mm diameter;
The PinPrick, MRC Systems GmbH, Heidelberg, Germany).
Mechanical pain sensitivity and dynamic mechanical allodynia
A stimulus-response function for MPS was determined using the same weighted
pinprick stimuli as for mechanical pain threshold. Additionally, pain in response to
light touch (DMA) was tested by light stroking with a cotton wisp (3 mN), a cotton
wool tip fixed to an elastic strip (100 mN), and a brush (200–400 mN).
Vibration detection threshold
VDT was assessed with a Rydel–Seiffert tuning fork (128/64 Hz, 8/8 scale;
Model:AB-125A, A. Barthelmes & Co. GmbH, Tuttlingen, Germany) applied at
suprathreshold vibration intensity over the subjects medial malleolus until the
participant indicated the sensation of vibration had ceased.
Pressure pain threshold
PPT was assessed by using a pressure gauge device (FDN200, Wagner Instruments,
Greenwich, CT, USA) with a probe area of 1 cm2 that exerts pressure up to 2000 kPa.
QST data analysis
QST data entry was into an Excel-based (Excel 2007, Microsoft USA) data analysis
system (EQUISTA, Casquar GmbH Germany) provided by the DFNS. This system
allowed entry of basic patient demographics and QST data. EQUISTA performed z-
score transformations of raw QST data values by comparing against normative
reference data published by the DFNS (n=180 subjects, bilateral assessment of 560 test
63
areas; Magerl et al., 2010). The DFNS normative reference data is age, gender and
anatomical test site matched. The mathematical transformation of QST data to z-scores
has been described elsewhere in detail (Rolke, 2006)
Heat suprathreshold nociceptive testing
The DFNS protocol is largely threshold based, but includes a stimulus response
function for detection of dynamic mechanical allodynia. However, it does not include
such a function for thermal stimuli. This was considered necessary by the supervisor of
this thesis (A. S. C. Rice) on the basis of his clinical observations from employing
QST for routine clinical diagnosis of HIV-SN for several years. This includes HPT,
and sometimes WDT, often being above the range the maximum temperature (> 500C)
in the DFNS protocol and that hyperpathia is reported once threshold was reached.
Therefore, after completion of the standard DFNS QST protocol, we conducted an
additional bespoke heat suprathreshold testing protocol designed in collaboration with
Prof Didier Bouhassira. Participants were subjected to 14 suprathreshold heat stimuli
of 2s duration each in a temperature range between 440C and 520C, at 20C intervals
(Supplemental Document 3: Heat Suprathreshold Protocol). During each stimulus,
patients recorded pain experienced using an electronic visual analogue scale (eVAS)
transducer (SENSEbox™ 450-010, SOMEDIC AB, Sweden). The anchors used were
0mm - ‘No Pain’ and 100mm - ‘Maximum pain imaginable’. The protocol ensured that
each temperature was tested twice, in a fixed, but random order to prevent participants
anticipating stimulus temperatures. All the patient responses for QST were recorded in
the QST CRF (Supplemental Document 4: QST CRF).
Hierarchical cluster analysis
The extent to which specific groups of participants with similar QST profiles also
associate according to other measures was tested using hierarchical cluster analysis.
DAISY function of R (version 2.1.2; R Foundation for Statistical Computing, Vienna,
Austria; http://www.r-project.org/) was used to calculate a distance matrix based on
Gower’s general dissimilarity coefficient. Binary variables were treated as asymmetric.
Ward’s method was applied to perform a hierarchical cluster analysis on the distance
matrix. In the resulting dendrogram, an arbitrary separation threshold was set so that
the resulting clusters would not include fewer than 10% of the total participants.
64
Structured Neurological Examination (SNE) A comprehensive structured upper and lower limb neurological examination was
devised to detect clinical signs of a peripheral neuropathy. The examination was
performed on each patient and included assessment of: light touch and pin-prick
sensation, joint position proprioception, vibration perception, deep-tendon reflexes,
muscle wasting and motor power (Supplemental Document 5: Structured Neurological
Examination).
Sympathetic nervous system function was examined by testing for the presence of
orthostatic hypotension, as assessed by measuring lying and standing blood pressure in
accordance with established protocols (The Consensus Committee of the American
Autonomic Society and the American Academy of Neurology, 1996). Lying and
standing blood pressures were each measured in triplicate using a non-invasive blood
pressure measuring system (Patient Transport Monitor HP M1275A, Hewlett-Packard,
USA). Lying blood pressures were measured first, following which the subject was
asked to stand for a timed three minutes after which standing blood pressures were
measured. Orthostatic hypotension was determined to be present in subjects in whom
either at least a 20mmHg reduction in systolic or a 10mmHg reduction in diastolic
blood pressure was observed.
Intra-epidermal nerve fibre density testing (IENFD) The determination of IENFD in skin biopsies is a validated and sensitive diagnostic
tool for the assessment of small fibre neuropathies including HIV-SN (Griffin et al.,
2001; Lauria et al., 2005, 2010; M. Polydefkis et al., 2002; Michael Polydefkis, 2006).
Punch biopsies of skin were taken immediately after the completion of QST. Biopsies
were taken in accordance with the consensus document produced by the European
Federation of Neurological Societies/ Peripheral Nerve Society Guideline (Lauria et
al., 2005, 2010) on the utilization of skin biopsies in the diagnosis of peripheral
neuropathies. Following the local infiltration of tissues with 1% lidocaine and under
sterile conditions, skin biopsies were taken from a site 10cm proximal to the lateral
malleolus with a disposable 3mm punch biopsy circular blade (Stiefel Laboratories
Inc/ GSK Plc NC, USA).
65
The freshly harvested biopsies were fixed for 12 to 24 hours in 2% paraformaldehyde/
lysine/ periodate (PLP) fixative at 4°C and rinsed with 0.08% Sorensen’s phosphate
buffer. Samples underwent cryoprotection with 15% and then 30% sucrose solutions
for 24 hours each. Samples were then embedded in OCT (Fisher Scientific UK Ltd),
snap-frozen by submersion in liquid nitrogen and stored at -20oC. Each biopsy was cut
into 50μm sections using a sliding microtome. Immunohistochemistry for PGP 9.5
(Ultraclone Ltd, Isle of White, UK; dilution 1:15000) was performed on sections using
the immunoperoxidase method. Sections from each patient were processed in two
separate staining runs to eliminate the risk of tissue loss and to ensure staining quality.
All sections were allocated an individual code and three sections per subject were
selected randomly to undergo analysis of IENFD using random sequences generated
by http://www.random.org/.
IENFD was assessed using a double bright-field microscope at 40× magnification
using established counting rules (Lauria et al., 2005, 2010). The two IENFD assessors
(M. R. D. Brown and J. D. Ramirez) underwent instruction and technical validation in
IENFD assessment at a clinical diagnostic laboratory run by Dr I. Bodi. The study
biopsy samples were coded, so that the assessors were unaware of the participant’s
neuropathy status. For the study materials, each assessor independently determined
IENFD values on three biopsy sections for each participant; the resulting mean value
was used. Inter-observer Pearson’s product-moment correlation co-efficacies were
determined for all the samples between the two microscopists; in addition intra-
observer reliability scores were also determined for 20 of these study sample selected
randomly (http://www.random.org/).
In accordance with previously published data, IENFD values below 7.63 fibre/mm
were considered to be abnormal (Bakkers et al., 2009). This value has been shown to
be associated with a specificity of 90% and sensitivity of 82.8% for the diagnosis of
small fibre neuropathies (Devigili et al., 2008).
Clinical Electrophysiology testing
Electrophysiological data were extracted where available from the electronic hospital
record of participants who had had lower limb electrophysiology clinical tests as part

66
of their routine medical care. This clinical data was evaluated for peripheral
neuropathies by an experienced neurologist (D. L. H. Bennett) who was blinded to the
peripheral neuropathy status of the participants evaluated.
Neuropathy Screening and Severity Tools
The Brief Peripheral Neuropathy Screen (BPNS)
The Brief Peripheral Neuropathy Screening tool was developed to detect HIV-SN and
has been used in several studies of HIV-SN (Affandi et al., 2008; C L Cherry et al.,
2009; Catherine L Cherry et al., 2008, 2005; Wright et al., 2008). The BPNS was
designed to be utilised by non-specialist medical personnel for the detection of HIV-
SN and consists of a set of questions relating to patient reported symptoms of a
peripheral neuropathy and a brief examination of the distal lower limb vibration
perception and deep tendon reflexes. The sensitivity and specificity of the BPNS has
been measured on several occasions, most notably by Simpson et. al, 2006 in a group
of 101 subjects: sensitivity 73% and specificity of 68% (D M Simpson et al., 2006).
The subjective elicited symptoms questions ask patients to report (i) the presence of
pain, aching, burning in the feet and/or legs and (ii) the presence of ‘pins and needles’
and numbness in feet and/or legs. Symptom severity is scored on an 11-point Likert
scale 0 (absent) to 10 (severe). The total response is then graded Grade 0 (score 0),
Grade 1 (score 1 -3), Grade 2 (score 4 – 6), Grade 3 (score 7-10).
The lower limb examination consists of vibration perception evaluation using a 128 Hz
tuning fork maximally struck and placed on the top of the distal inter-phalangeal (DIP)
joint on one great toe. The time for a patient to lose vibration perception is graded:
Grade 0 - >10 sec, Grade 1 - felt for 6 -10 sec, Grade 2 - felt for 5 sec or less, Grade 3 -
no perception of vibration. Ankle reflexes are assessed relative to knee reflexes and
graded: Grade 0 - absent, Grade 1 - hypoactive, Grade 2 - normal, Grade 4 - clonus.
Subjects are considered to have HIV-SN if they have at least one symptom and either
reduced or absent vibration sensation or ankle reflexes using the BPNS as revised by
Simpson et al 2006 (D M Simpson et al., 2006).
67
The Toronto Clinical Scoring System (TCSS)
The TCSS was developed as a screening tool for diabetic peripheral neuropathy (B. a
Perkins, Olaleye, Zinman, & Bril, 2001). Subsequent studies validated its utility in
reflecting diabetic neuropathy severity, its correlation with clinical
electrophysiological measures and microscopic morphological changes in peripheral
nerve biopsies (Bril & Perkins, 2002) . The TCSS utilises a simplified neurological
examination assessing peripheral sensory perception, deep tendon reflexes, and the
presence of neuropathy symptoms.
Sensory testing is performed on the first toe for: pinprick sensation using a Neurotip™
(Owen Mumford, Oxford U.K.); temperature discrimination (warm and cool water
filled test tubes); light touch 10g monofilament and vibration with a maximally struck
128Hz tuning fork; position and rated as normal or abnormal, 0 or 1 point respectively.
Scores range from 0 to a maximum of 19.
Deep tendon reflexes scores are graded as loss - 2, reduced -1 and normal - 0 for each
side. The presence of each following neuropathy symptom scores 1 point: pain,
numbness, tingling and weakness in the feet; the presence of similar upper limb
symptoms and the presence of unsteadiness on ambulation.
The Utah Early Neuropathy Scale (UENS)
The UENS is a physical examination scale developed specifically for the detection of
early, sensory predominant, diabetic polyneuropathy (Singleton et al., 2008). The
UENS emphasis is on the severity and spatial distribution of pin sharp sensation loss in
the lower limb. The scale was developed and validated in a population with early
diabetic peripheral neuropathy.
The UENS assesses sharp sensation in the lower leg relative to an unaffected portion of
skin. A Neurotip™ pin (Owen Mumford, Oxford U.K.) is applied to the dorsum of the
first toe and, working centripetally in 2cm increments, the subject is asked at each
application if they feel “any sharpness” and if they do “is it as sharp as they would
expect?” This is performed on both lower limbs. The lower limbs are divided into 6
regions for testing; 2 points are scored for each region in which the subject fails to feel
68
any sharpness. This is conducted and scored on both lower limbs. One additional point
is scored for each additional region in which the pin feels less sharp than expected.
Vibration is tested using a 128Hz tuning fork maximally struck and applied to the
dorsum of the great toe at the interphalangeal joint.
The UENS has also been correlated with data from electrophysiological and QST
testing (Singleton et al., 2008). Moreover, the UENS has recently been used in a small
HIV-SN population, where it was shown to correlate with autonomic dysfunction
measures (quantitative sudomotor axon reflex testing) and pain severity, but it was not
validated in the diagnosis of HIV-SN (Boger et al., 2012).
Pain, sleep disturbance, quality of life and psychological co-morbidity measures
Participants were given a questionnaire pack to complete and return to the
investigation centre following their clinical assessment appointment.
7-day Pain diary
Patients were also asked to keep a pain diary for seven days, recording pain at 8am and
8pm daily on an 11-point Likert scale with 0 being ‘no pain’ and 10 the ‘worst pain
imaginable’.
Brief Pain Inventory (BPI) 7-item pain interference sub-scale
Pain related interference in activities of daily living was assessed using the 7-item Pain
Interference Sub-scale of the Brief Pain Inventory (BPI-PIS; Cleeland & Ryan, 1994).
The BPI-PIS assesses pain interference within 7 domains: general activity, walking,
work, relationships, mood, life enjoyment and sleep which participants score on a 11
point Likert scale ranging from 0 to 10. The composite score was calculated as the sum
of the 7 interference items.
SF-36 instrument
The short-form 36 questions (SF-36) is an established instrument used for the
assessment of health-related quality of life (Ware & Sherbourne, 1992). Participants
complete a questionnaire consisting of 36 questions. As per convention, SF-36
69
responses were regrouped, into 8 domains of physical functioning: physical
functioning, role - physical, bodily pain, general health, vitality, social functioning,
role - emotional, and mental health. SF-36 scores range from 0 to 100: representing
extreme dysfunction/ symptom severity to optimal function respectively.
Pain Anxiety Symptom Scale-20 (PASS-20)
Pain-related anxiety was assessed with the Pain Anxiety Symptom Scale-20 (PASS-20;
L. McCracken & Dhingra, 2002) which is a shortened version of PASS (M. L.
McCracken, Zayfert, & Gross, 1992). It is comprised of 20 questions assessing four
facets of pain-related anxiety: fearfulness of pain, cognitive anxiety, escape/avoidance,
and physiological anxiety. Each subscale score ranges from 0 ‘no interference’ to 25
‘maximum interference’. Additionally summation of the sub-scales provides a general
measure of pain related anxiety.
Amended Depression Anxiety Positive-Outlook instrument (DAPOS)
We used the depression and anxiety sub-scales of the Depression Anxiety Positive-
Outlook (DAPOS) instrument (Pincus, Williams, Vogel, & Field, 2004). The DAPOS
instrument was designed to measure mood in pain populations, and consists of 3
subscales. The subscale for depression (DAPOS-D) contains 5 items with scores
ranging from 5 to 25, indicating normal mood to severe depression. The subscale for
anxiety (DAPOS-A) contains 3 items, which ranges from 3 to 15 (no anxiety to
maximal anxiety).
The Pain Catastrophizing Scale (PCS)
Pain Catastrophizing Scale assesses the cognitive process by which pain is seen as an
extreme threat and from which the patient suffers exaggerated negative consequences
(Osman et al., 1997). The PCS questionnaire consists of 13 statements of descriptions
of pain experiences. Respondents are asked to indicate whether they agree with these
statements by using a 5-point rating scale scored from 0 (not at all) to 4 (always). A
high total score indicates a high level of pain catastrophizing. The instrument
comprises three dimensions: rumination, magnification and helplessness. Rumination
70
refers to the patients’ inability to apart the pain from his mind; magnification expresses
the exaggerated cognitions of pain as a threat and hopelessness is the estimation that
the patient cannot do anything to influence in his pain.
Insomnia Severity Index (ISI)
To assess the prevalence of sleep dysfunction we used the Insomnia Severity Index
(ISI; Bastien, Vallières, & Morin, 2001). The ISI was specifically designed to assess
insomnia and is a brief self-report instrument, which measures a patient’s perception,
subjective symptoms and consequences of their insomnia. Its content corresponds, in
part, to the diagnostic criteria of insomnia. The ISI comprises of seven items assessing
the severity of sleep-onset and sleep maintenance difficulties, satisfaction with sleep
patterns, interference with daily functioning, noticeability of impairment due to sleep
dysfunction and the degree of distress experienced by the patient.
Case definition of HIV-SN for PINS-HIV; rationale and implications for the study.
There is no gold standard test for the presence of HIV-SN (Brew, 2003; Catherine L
Cherry et al., 2005). This lack of gold standard for HIV-SN and other predominately
small fibre neuropathies, has been identified as a factor hindering the progress in
understanding HIV-SN (Evans et al., 2008) and small fibre neuropathy
pathophysiologies per se (Devigili et al., 2008).
The most frequently employed neuropathy screening instruments used to assess the
presence of HIV-SN, were the Total Neuropathy Score (TNS) and Brief Peripheral
Neuropathy Screen (BPNS) (Catherine L Cherry et al., 2008; Maritz et al., 2010; J
Robinson-Papp et al., 2010; D M Simpson et al., 2006; Smyth et al., 2007). These
instruments were conceived for use in larger epidemiological studies and are designed
to be brief and require little specialist equipment or training to use. These screening
tools focus predominately on large sensory nerve fibre function, such as vibration
sensation and deep tendon reflexes. Consequently these scales may be less sensitive to
the small fibre dysfunction characteristics of HIV-SN (Boger et al., 2012) which have
been hypothesized to be important in the early pathogenesis of HIV-SN (Catherine L
Cherry et al., 2005; D. R. Cornblath et al., 1999) which is an area of interest in the
PINS-HIV study. The use of these established screening instruments would potentially
71
lead to an over representation of participants with later, established HIV-SN and fail to
diagnose early HIV-SN.
Other diagnostic tests such as nerve conduction studies, (R. J. Barohn et al., 1996; P.
Y. Chavanet et al., 1988; P. Chavanet et al., 1989; Fuller, Jacobs, & Guiloff, 1991;
Husstedt et al., 2000; Jakobsen, Smith, Gaub, Helweg-Larsen, & Trojaborg, 1989;
Malessa et al., 1996; T. Smith, Jakobsen, Gaub, Helweg-Larsen, & Trojaborg, 1988)
QST testing, (Bouhassira et al., 1999; Huengsberg, Winer, Ross, & Shahmanesh, 1998;
Tagliati, Grinnell, Godbold, & Simpson, 1999; Winer et al., 1992) and IENFD
quantification (D N Herrmann, Griffin, Hauer, Cornblath, & McArthur, 1999; Holland
et al., 1997; McCarthy et al., 1995; Pittenger et al., 2004; M. Polydefkis et al., 2002;
Michael Polydefkis et al., 2004) may be abnormal in the context of HIV-SN. However,
normal results to these tests occur frequently in patients with clinically apparent HIV-
SN (M. Polydefkis et al., 2002; Tagliati et al., 1999; Winer et al., 1992). Similarly,
some subclinical abnormalities, not necessarily indicative of neuropathy
pathophysiology are also described in these tests (R. J. Barohn et al., 1996; Bouhassira
et al., 1999; P. Y. Chavanet et al., 1988; P. Chavanet et al., 1989; Fuller et al., 1991;
David N Herrmann et al., 2004; Huengsberg et al., 1998; Husstedt et al., 2000;
Jakobsen et al., 1989; Malessa et al., 1996; T. Smith et al., 1988; Tagliati et al., 1999).
As no single testing paradigm could be identified that would have an acceptable
reliability, sensitivity and specificity for the aims of the PINS-HIV study, a novel
composite definition was constructed in discussion with the collaborating neurologist.
The PINS-HIV study used a definition of HIV-SN requiring ≥2 out of the following
triumvirate:
Clinical signs of distal neuropathy on the Structured Neurological Exam (SNE).
≥2 abnormal QST findings using DFNS protocol.
Intra-epidermal-nerve-fibre-density of ≤7.63 fibres/mm on skin biopsy examination.
Such a composite definition has been previously proposed for use in the study of other
small fibre neuropathies, but has not been used in studies of HIV-SN (Devigili et al.,
2008).
72
By using three different test modalities and requiring more than one ‘positive’ finding
for defining HIV-SN, it was hoped to negate many of the shortcomings of the
individual tests if used in isolation.
A limitation of using this method is that there is potential for a circular argument for
some of the outcome measures of interest in the study, which partly rely on the
diagnostic tests used in the case definition. To explore this potential problem a post-
hoc analysis of altering the case definition was planned to investigate the impact on
individual participant neuropathy diagnosis designation (Table 3.10). A further
exploration of using different definitions of HIV-SN on the QST results has also been
conducted post-hoc below (Table 3.11, 3.12 and Figures 3.2.a,b,c and d).
Sample Size Calculation
At the time of the study there were few data available regarding the diagnostic value
for HIV-SN for each of the two primary measurements of interest (QST and IENFD)
on which to base a sample size calculation. Nevertheless, such a calculation in relation
to these measures has been performed in order to guide study conduct (t test for power
calculation, Sigma v 3.5, Systat Software Inc).
For QST the ΔWDT data for HIV positive patients versus healthy controls from Martin
et al were used (Martin et al., 2003). This calculation revealed a minimum sample size
of 11 was required per group for a power > 0.8 (Power 0.828; Difference in Means 4.3;
Standard Deviation 3.3; α 0.05).
For IENFD data for patients with small fibre neuropathies verses healthy controls from
Nebuchennykh et al were used (Nebuchennykh, Løseth, Lindal, & Mellgren, 2009).
This calculation revealed a minimum sample size of 16 was required per group for a
power > 0.8 (Power 0.816; Difference in Means 4.7; Standard Deviation 4.5; α 0.05).
However, because of the uncertain assumptions inherent in such calculations a
minimum group size of 25 was used.
73
Results
Participants
Between July 7th 2009 and January 25th 2011 66 volunteers who were living with HIV
were recruited to participate in the study. They were all receiving routine clinical care
for their HIV disease as ambulatory patients attending the St Stephen’s Centre out
patients department, Chelsea and Westminster Hospital NHS Foundation Trust,
London, United Kingdom
All 66 participants attended the clinical assessment appointment. Two participants (one
from the HIV-SN and the other from the HIV-No SN group) produced only partial
QST datasets (missing thermal parameters) due an isolated equipment problem that
was resolved. These subjects were excluded from the subsequent thermal parameter
QST data analysis.
IENFD were determined on 57 participants out of the total 66; 6 participants did not
consent to a skin biopsy (4 from the HIV-No SN and 2 from the HIV-SN group), one
participant from the HIV-SN group was anticoagulated with warfarin and so a skin
biopsy was contra-indicated. Two samples (one from each group) were of insufficient
quality to allow IENFD determination. Participants with missing IENFD data were not
included in the IENFD data analysis.
Demographics
Participant demographic data are presented in Table 3.1. The groups were evenly
matched in terms of demographic and related clinical factors. The majority of
participants were white (86.4%), male (86.4%) and middle aged (mean 49.23 yrs SD
8.78), broadly reflecting the patient population of the highly resourced United
Kingdom recruitment centre in the current cART era (personal communication Dr
Marta Boffito and Dr David Asboe). Using the triumvirate criteria for HIV-SN
diagnosis the study group was divided into ‘HIV-SN’ and ‘HIV-No SN’ groups.
Twenty-eight (42.4%) of participants were determined to have HIV-SN and 38
(57.6%) to have HIV-No SN. Twenty-one (75.0%) of the 28 HIV-SN patients
complained of a painful peripheral neuropathy. No statistically significant difference
74
was seen between the HIV-SN and HIV-No SN groups for sex, ethnicity, height, or
weight. There was also no difference between the groups in terms of age, height and
years since HIV diagnosis.
There was also no difference between the two groups for the frequency of co-
morbidities which might potentially affect the peripheral neuropathy status of
participants; diabetes, hepatitis B and C, syphilis or exposure to chemotherapy agents.
Quantitative Sensory Testing healthy control participants
Healthy control data was collected to meet the DFNS group’s requirements for
investigation centre quality assurance, and to provide normal values for suprathreshold
heat responses. To fulfil DFNS requirements 36 healthy controls were recruited with a
mean age of 34.60 yrs of age (SD 9.45) of which 21 (58.3%) were male. These
participants underwent the DFNS QST protocol after which the additional
suprathreshold heat testing was conducted on each.
Anti-retroviral therapy history
ARV therapy histories of the participants are presented in Table 3.2. Only 2
participants (3%) had no previous exposure to ARVs; both were in the HIV-No SN
group. The majority had previous ARV exposure and were all still currently receiving
cART (n=64, 97%). No statistical difference was observed between the two groups for
either, individual agents or classes of agents in relation to exposure or mean years
exposed. There was also no difference between the two groups for the total number of
‘drug years’ a patient received a class of agent for, or the maximum number of
consecutive years of exposure to a given drug class (data not shown).
There was no difference between the two groups for exposure to NRTI agents.
Between 52% and 71% of participants had been exposed at some point to neurotoxic
“dNRTIs” and the average exposure was about 12 years. This was independent to the
duration of time since HIV diagnosis. The groups were also matched for exposure to
the potentially neurotoxic protease inhibitor indinavir (Catherine Louise Cherry et al.,
2012; Ellis et al., 2010; Pettersen et al., 2006; Smyth et al., 2007) with 13-32 % of
subjects having been exposed to the drug for an average of about 13 years.
75
Quantitative Sensory Testing results
Distribution of mean QST z-scores across groups
Mean z-score values for HIV-No SN and HIV-SN groups (Figure 3.1, Figure 3.3 and
Table 3.3) showed a loss of sensory function for all three thermal sensory QST
parameters CDT, WDT, and TSL compared to DFNS values, indicating a degree of
thermal detection hypothesia (p<0.05 Kruskal-Wallis, Dunn’s post-hoc; HIV-No SN
and HIV-SN and HC groups). This general shift across all thermal parameters towards
hypothesia was largest in the HIV-SN group. A similar shift in thermal nociceptive
parameters was not seen, with only HPT demonstrating a shift in mean z–scores
towards loss of function. Mean z-scores for CPT were similar to DFNS control values
in both groups.
Mechanical detection parameters also showed a shift of the group mean towards loss of
function in the HIV groups; again, the largest difference was observed in the HIV-SN
group (see Figures 3.1 and 3.3 and Table 3.3). This was particularly marked in the
HIV-SN group for MDT and VDT mean values compared to the HIV-No SN, HC and
DFNS control values (p<0.05 Kruskal-Wallis, Dunn’s post-hoc). MDT and VDT were
the only QST parameters that showed a mean group value outside of the DFNS defined
normal range.
Whilst the difference in mean WUR was small in the HIV-SN compared to the other
groups it had a large SD value (1.66) suggestive of a high degree of heterogeneity for
this parameter within the HIV-SN group. This heterogeneity was evident in the scatter
plot of WUR for HIV-SN, where a small group of 4 HIV-SN participants (14.3%)
number showed high (gain of function) z-scores for WUR (p <0.05 Chi squared test of
association compared to HIV-No SN group).
Mean healthy control QST participant data closely matched that expected by DFNS
control values for 12 of the 13 DFNS QST parameters (see Table 3.3). This is
indicated by the fact that the z-transformed QST mean values in the healthy control
group are all close to zero, with standard deviations of near to one or less. Healthy
control MPS values showed a slight shift in mean values, with 5 (13.9%) participants
more than expected showing abnormal values compared to DFNS healthy control data.
76
Frequency of individual QST measure abnormalities: loss and gain of sensory function.
The frequency of abnormal QST values in each group are shown in Figure 3.4 and
Table 3.3. The majority of abnormal parameters were loss of sensory function in any of
the QST parameters with 34.2% and 85.7% in the HIV-No SN and HIV-SN groups
respectively. A smaller number of participants in the HIV-No SN and HIV-SN group
showed gain of function in any parameter: 26.3% and 28.6% respectively. – but this
was similar to the Healthy control groups at 30.6%, there was no statistical difference
between all three groups.
The most frequent sensory abnormalities seen in the HIV-SN group were loss of MDT
and VDT both of which were independently absent in 50% of the HIV-SN subjects,
with 32.14% demonstrating the loss of both. In contrast, the healthy control and HIV-
No SN group showed a loss of MDT in only 5.6% and 5.3%, and VDT in 5.6% and
10.5% respectively.
Within the thermal sensory parameters the HIV-SN participants showed a loss of CDT
function (28.6%) compared to HIV-No SN group (5.3%), most frequently followed by
WDT and TSL (14.3%, 2.6% in both HIV groups). Loss of HPT was the most frequent
abnormal thermal nociceptor parameter in the HIV-SN group (32.1%) and in the HIV-
No SN group (7.9%). No participants in either HIV group displayed abnormalities of
CPT. The presence of PHS was considered a loss of thermal discrimination and
therefore a loss of sensory function (Rolke, 2006). PHS phenomena were observed in
7.9% and 14.3% of the HIV-No SN and HIV-SN groups respectively.
The presence of gain of function in QST parameters was rare across all groups, but was
seen most frequently in the mechanical WUR parameter, with 14.3% of HIV-SN
patients demonstrating it, compared to only 5.3% and 5.6% of the healthy control and
HIV-No SN groups respectively (p<0.05 Chi squared test of association against HIV-
No SN group). No participants in any of the groups were found to have DMA.
Patterns of loss and gain of sensory function
We utilized the DFNS coding system (Maier et al., 2010) to display combinations of
sensory dysfunction in HIV-SN (Table 3.4). Accordingly, a value for a QST parameter
77
within the normal DFNS reference range was designated ‘0’; the presence of thermal
hypoesthesia (i.e. loss of WDT or CDT) was designated as L1; and the presence of
hypoesthesia to mechanical modalities (i.e. loss of MDT or VDT) was designated L2.
Gain of sensory function to thermal modalities was designated G1 and gain of sensory
function to mechanical modalities designated as G2. When both thermal and
mechanical abnormalities were present they were designated as L3 and G3
respectively.
HIV-SN abnormal QST parameters were dominated by loss of sensory function. The
majority of HIV-SN participants (85.7%) had at least one abnormality on QST testing,
and had, at a minimum, the loss of one sensory parameter. Different combinations of
sensory loss and gain did occur across the HIV-SN group, however the majority
involved just sensory loss (L1+L2+L3: 78.6%). Indeed, the most frequent combination
was the loss of at least one thermal and one mechanical QST parameter in 42.9% of
participants (L3G0). HIV-No SN participants demonstrated loss or gain of thermal
modalities in isolation (L1 or G1; see Table 3.4). The second most frequent
combination was loss of just mechanical sensory modalities (L2G0: 21.4%).
Suprathreshold heat testing
Figure 3.5 displays the cumulative mean pain VAS responses to suprathreshold heat
stimuli from 48oC to 52oC for the three groups: healthy controls, HIV-No SN and HIV-
SN groups. Health control patients had an earlier take off in pain VAS responses – i.e.
this occurred at lower temperatures, however at higher suprathreshold temperatures
there was little difference in the VAS responses elicited from all the three groups
tested. No statistically significant difference was seen between the three groups, or in
the painful HIV-SN subgroup of HIV-SN (not shown) for pain response at any
suprathreshold temperature.
Hierarchical cluster analysis of QST data
The results of hierarchical cluster analysis of individual participant’s DFNS QST data
did show a tendency for HIV-SN patients to cluster according to neuropathy and pain
status (see Figure 3.6). A distinct cluster of 25 subjects, containing 20 (71.4%) of the
HIV-SN participants, of whom the majority (80%) complained of pain symptoms, was
78
observed. No other discernible clusters were found relating to any other participant
outcome measures examined using hierarchical cluster analysis of QST data (Figure
3.6).
Intra Epidermal Fibre Densities (IENFD)
A total of 57 skin punch biopsy samples were available for IENFD measurement from
the 66 participants (see above for details). Figure 3.7 shows representative images of
two participants, one with normal fibre counts (Figure 3.7A) and the other with
reduced IENFD counts (Figure 3.7B).
The associated intra-observer correlation co-efficients for 20 randomly selected
samples for quality assurance exercise was 0.88 (J. D. Ramirez) and 0.89 (M. R. D.
Brown), both of which are high. A high inter-observer Pearson’s product-moment
correlation co-efficient of 0.93 was determined between the two microscopists for all
study samples (n=55).
The median values of IENFD for HIV-No SN group was 9.2 fibres/mm (range 1.7 -
14.4 fibres/mm) compared to 6.3 fibres/mm (range 0.7 - 12.4 fibres/mm) for the HIV-
SN group (p<0.001). In accordance with previously published literature, an IENFD
value of < 7.63 fibres/mm was taken as being abnormal (Lauria et al., 2005); this was
seen in 8 subjects (21.1%) of the HIV-No SN and in 17 subjects (60.7%) of the HIV-
SN group (p<0.05) with an associated sensitivity and specificity of detecting HIV-SN
in isolation of 61% and 79% respectively.
Table 3.5 shows Pearson’s correlation coefficients for individual QST parameters and
IENFD. Little correlation between the measured QST parameters and IEFND can be
seen.
As would be expected, IENFD was inversely correlated to the severity of the
peripheral neuropathy as measured by the TCSS instrument (r=-0.343, 95%CI -0.56 to
-0.88; p<0.01).
79
Electrophysiological testing
Suitable lower limb electrophysiology clinical studies were available for 18 (27.3%) of
the 66 HIV positive participants; 5 subjects (13.2%) in the HIV-No SN group and 13
subjects (46.4%) in the HIV-SN group. Within the HIV-SN group, nine of the thirteen
participants (64.3%) were diagnostic of an axonal peripheral neuropathy in comparison
to only one in the HIV-No SN group.
Pain and patient reported symptoms
Results of the structured patient symptom and medical history interview, and 7-day
pain diary are presented in Table 3.6.
More patients reported experiencing pain in their hands and/or feet in the HIV-SN
compared to HIV-No SN (75% vs 28.95% respectively; p<0.001). The mean 7-day
pain score for patients experiencing pain was also greater in the HIV-SN group (5.65,
SD 1.76) compared to the HIV-No SN group (2.8, SD 2.34; p<0.001). The mean
number of years from HIV diagnosis and the mean duration of pain were similar in the
two groups. Although there was no difference between groups in the reporting of ‘pins
and needles’, the reporting of ‘numbness’ in feet and/or hands was more frequent in
the HIV-SN group (75%) compared to the HIV-No SN group (36.8%; p<0.05).
More participants with HIV-SN compared to those without HIV-SN, reported suffering
from symptoms of postural hypotension (50% vs 24.6% respectively; p <0.01),
however participants’ reported symptoms of orthostatic hypotension correlated to
measured orthostatic hypotension in only 33.3% of HIV-No SN and 7.1% of HIV-SN
participants. No difference was seen in measured orthostatic hypotension between the
two groups (14.8% vs 18.4% for HIV-SN and HIV-No SN groups respectively;
p=0.702).
Patients reported symptoms of urinary dysfunction more commonly in the HIV-SN
group (42.9%) compared to participants in the HIV-No SN (15.8%; p<0.05). The
frequency of participants reporting erectile dysfunction and nocturnal diarrhoea were
similar for both groups respectively (Table 3.6)
80
Psychological co-morbidity, sleep disturbance and health related quality of life.
The return of questionnaires and completion of individual scores within each group are
shown in Table 3.7. Of the 66 participants, 57 (86.3%) returned completed
questionnaire booklets to the test centre for analysis. Results from the psychological
and insomnia instrument battery are presented in Table 3.8.
Pain interference and health related quality of life
As expected the Brief Pain Interference (BPI) subscale mean total score was
significantly higher in the painful HIV-SN group (46.11, SD 13.69) compared to the
HIV-No SN group (15.20, SD 16.22; p<0.001; see Table 3.8). The high scores present
in the painful HIV-SN group indicate that participants’ pain has an important
detrimental impact on their day to day living and their quality of life.
The SF-36 data further emphasises this point, showing participants with painful HIV-
SN displayed significantly more morbidity when compared to the HIV-No SN group
across all of the domains of the SF-36 (Table 3.8). In particular HIV-SN patient’s
physical functioning (RP), perceptions of their physical selves (RP), general vitality
(VT) and social functioning (SF) were dramatically poorer in the participants in the
painful HIV-SN group compared to patients in the HIV-No SN group.
Sleep dysfunction
Analysis of data from the self-report ISI instrument indicated that both groups suffered
from mild sub-clinical insomnia. However, at the group level there was no independent
effect of HIV-SN in this regard. Nevertheless, at the individual level, more participants
in the painful HIV-SN group reported degrees of sleep disturbance equating to clinical
insomnia (ISI ≥15): 13 participants (68.4%), with 7 (36.8% overall) of these suffering
severe insomnia (ISI ≥ 22). In contrast, 7 participants (22.6%, p <0.001) of the HIV-
No SN group suffered from clinical insomnia, and 3 participants (9.7% overall, p
<0.001) with severe insomnia (Table 3.8).
81
Depression, Anxiety and Catastrophizing
Participants with painful HIV-SN were more depressed (11.21, SD 4.22 vs 8.38, SD
4.10, p<0.05) and anxious (4.47 SD 2.97 vs 5.45 SD 2.89, p<0.05) as measured with
the DAPOS instrument, than those in the HIV-No SN group (see Table 3.8).
Overall, there was no difference between the groups with regards to the total PASS-20
scores (see Table 3.8). However, differences were evident in some domains of the
PASS-20. The HIV-SN group reported more features of cognitive impairment in
response to pain compared to the HIV-No SN group (PASS-20 cognitive sub-scale -
mean 8.45, SD 5.28 vs 14.95, SD 5.64 respectively; p < 0.001). There was more
psychological anxiety and fear as measured with the PASS subscales in the painful
HIV-SN group compared to the HIV-No SN group: physiological anxiety (9.21 SD
7.54 vs 4.83 SD 6.45 respectively; p < 0.05) and fear (11.79, SD 6.75 vs 6.97, SD 7.11
respectively: p < 0.05).
Catastrophizing as measured using the PCS instrument revealed a significant
difference in PCS total scores between the groups (see Table 3.8; 14.3, SD 11.81 in the
HIV-No SN group compared to 23.74, SD 12.64 in the painful HIV-SN group;
p=0.009). This difference was mostly attributable to a difference in the PCS
helplessness sub-scale (6.03, SD 5.52 in the HIV-No SN group compared to 11.16, SD
6.13 in the HIV-SN group; p=0.004). No statistically significant differences were seen
in the other PCS sub-scores for rumination or magnification.
Plasma lipid profiles, random glucose, BMI and waist-hip circumference ratios.
A higher mean triglyceride plasma (TRG) concentration was measured in the HIV-SN
group compared to the than the HIV-No SN group (see Table 3.9; 2.18mmol/l, SD 1.09
vs 1.61mmol/l, SD 0.77 respectively; p <0.05). There was no significant difference
between the two groups in statin drug use. Despite this difference in TRG
concentrations we did not find a correlation between the severity of neuropathy (using
the TCSS instrument) and plasma TRG concentrations (rs = -0.155 (-0.514 to 0.250); p
= 0.439). No significant differences were found between the two groups for other
plasma lipids, BMI or waist-hip circumference ratios, although all were the upper-end
of normal (see Table 3.9).
82
Peripheral neuropathy screening and severity instruments: BPNS, UENS and TCSS.
Mean scores were determined and ROC plots were generated for each of the three
neuropathy screening instruments examined in the study. Optimal cut-off values for the
diagnosis of HIV-SN in the study population were determined from these plots, giving
equal weight for sensitivity and specificity.
Using the standard BPNS scoring method (D M Simpson et al., 2006), which adds
weight to the loss of deep tendon reflexes and vibration perception, the BPNS
instrument shows a specificity and sensitivity in the detection of HIV-SN of 75% and
79% respectively (p<0.001).For the ROC analysis the numerical component of the
BPNS was used in its raw form, weighting sensitivity and specificity equally. A cut-off
value of 19 was determined as optimal which was associated with a sensitivity and
specificity of 76%.
The mean TCSS values in the HIV-SN were higher when compared to those in the
HIV-No SN group (9.26, SD 3.28 vs 3.36, SD 3.65 respectively; p<0.001). ROC
analysis found a value of 8 provided the best accuracy in HIV-SN detection;
sensitivity/ specificity 81%.
The UENS median values were also significantly higher in the HIV-SN group when
compared to the HIV-No SN group (11.26, SD 5.66 vs 3.64, SD 2.98 respectively;
p<0.001). Following a ROC analysis a cut-off value of 7 was selected as providing the
best accuracy in our study population. This provides a sensitivity and specificity of
84% in detection of HIV-SN.
Using the ROC plots for each instrument, AUC was used as a measure of accuracy;
with a smaller AUC equating to greater accuracy. The instrument found to have the
greatest accuracy was the UENS (AUC 0.91), followed by TCSS (AUC 0.86) and then
the BPNS (AUC 0.69).
Testing the HIV-SN triumvirate definition and the consequences of using
different HIV-SN definitions.
As this study’s case definition of HIV-SN used a triumvirate utilising QST, IENFD
and a Structured Neurological Examination (SNE), we tested the consequences of
83
using different combinations of the triumvirate on the HIV-SN designation of
participants in the study (see Table 3.10). Removal of QST and IENFD individually
from the triumvirate resulted in sensitivity and specificity of 71%, 100% and 79%,
100% respectively when compared to using the full triumvirate diagnosis. Not using
QST in the diagnosis resulted in 8 participants (12.1%) having a different diagnosis;
not using IENFD results in a change in 6 subject’s diagnosis (9.1%) and removal of
SNE resulted in the largest number of diagnosis changes at 17 (25.8%).
The criteria most effective in isolation is SNE - with a sensitivity and specificity of
1.00 and 0.740 respectively, followed by QST, (0.786 sensitivity, 0.816 specificity)
and IENFD (0.607 sensitivity, 0.790 specificity).
Discussion
Quantitative Sensory Testing
To our knowledge, this is the first detailed profiling of the HIV-SN phenotype in a
cART era population. This study has shown that the pattern of sensory nerve
dysfunction that occurs in HIV-SN is profoundly heterogeneous. Across sensory and
nociceptive mechanical and thermal modalities, the predominant picture was that of
loss of sensory function; 86% of HIV-SN participants were observed to have a loss of
function of at least one sensory modality. However the degree to which individual
modalities were affected across the HIV-SN group did not correlate to either the
symptoms experienced (including pain) or the severity of neuropathy. Equally, no
single sensory QST parameter was found to have a useful diagnostic utility for HIV-
SN diagnosis in isolation.
Unexpectedly it was the large fibre mediated modalities of MDT and VDT (both
mediated by larger myelinated Aβ fibres) which were most frequently lost in HIV-SN
(see Table 3.4; loss of 50% for each modality). Moreover 32% of HIV-SN participants
demonstrated a loss of both MDT and VDT modalities together. HIV-SN has often
been described to be a predominately small fibre neuropathy, i.e. affecting mostly
small unmyelinated C and Aδ sensory fibres. Therefore, it would be expected that this
would be reflected in QST testing as more in a loss of thermal detection thresholds
(CDT and WDT) and an elevation in the heat pain threshold (HPT), as these modalities
84
are mediated by the smaller unmyelinated sensory fibres. Whilst these modalities are
indeed affected on a group level (see Figures 3.2-3.3 and Table 3.3), HIV-SN mean
CDT and WDT showed a significant reduction in function compared to both the HIV-
No SN and DFNS values. Individually only a smaller number of HIV-SN participants
showed a large enough loss in function of these modalities to be considered as
‘abnormal’ by the DFNS definitions used. As mechanical QST parameters are more
often affected in HIV-SN, the inclusion of thermal QST parameters as part of
diagnostic testing for HIV-SN would appear to not be necessary. This has significant
resource implications, as the equipment involved in such thermal testing is, to date,
expensive and not easily portable. Consequently the use of QST outside of well-
resourced research centres has been limited. VDT can be tested with an appropriate
128Hz tuning fork and MDT with von Frey filaments, both of which are relatively
inexpensive and do not require specialist training to use.
Whilst the diagnostic limitations of electrophysiological methods for small fibre
neuropathies is well know, this study shows the limitations of QST for the diagnosis of
HIV-SN. Forteen per cent of participants determined to have HIV-SN by the
multimodal definition used in this study did not demonstrate dysfunction of any of the
QST modalities measured. This is broadly similar to an earlier DFNS study examining
the QST phenotype of painful polyneuropathies (HIV- SN participants), which found
17% of subjects that did not present QST abnormalities (Maier et al., 2010).
An observation in routine clinical QST testing by the supervisor of this thesis (A.S.C.
Rice) was that patients with HIV-SN appeared to express higher pain on the routine
testing of heat pain thresholds (HPT). The heat suprathreshold testing protocol was
designed to detect the presence of thermal hyperpathia in HIV-SN participants. No
statistically significant difference was seen between the three groups (Healthy
volunteers, HIV-No SN and HIV-SN) at any of the temperatures tested. The HC and
HIV-No SN groups did have early takes offs of the VAS/ temperature stimulus
response curves (see Figure 3.5), but at higher temperatures little difference was seen
between the groups. A similar finding was seen in an earlier study, which employed an
analogous heat suprathreshold protocol during the pre cART era (Bouhassira et al.,
1999).
85
This current study found no evidence of gain of function features of neuropathic pain
for dynamic mechanical allodynia (DMA) or static mechanical hyperalgesia (MPS),
but did find a small group (14%) of HIV-SN participants who demonstrated high wind-
up ratios (WUR) to pin-prick stimuli (discussed below). In contrast, the group of
Bouhassira demonstrated mechanical hyperalgesia in HIV-SN (Bouhassira et al.,
1999), however, the current study did not replicate this finding. There are two potential
reasons for this: firstly the DFNS QST protocol tests for mechanical hyperalgesia uses
a method that is different to Bouhassira’s group; secondly, and more fundamentally,
the HIV-SN participants examined in Bouhassira’s study were from the pre-cART era.
It has been demonstrated that different risk factors for the development of HIV-SN
operated in the pre-cART era to present day (e.g. CD4 counts, d NRTI drug exposure;
Catherine Louise Cherry et al., 2012), consequently the HIV-SN phenotype might be
substantially different now in the c-ART era.
Simpson and collaborators found a raised pin-prick punctate hyperalgesia present in
13% of HIV-SN participants screened for a large pregabalin efficacy RCT (D M
Simpson, Scott, et al., 2010). This study measured the pain response to a single (non-
standardised) strength pin-prick stimulus to measure pin-prick hyperalgesia. In
contrast, the DFNS protocol uses a stimulus pain response curve to different
(standardised strength) pin-prick stimuli, consequently comparing the two measures is
difficult. However one of the tests used in the DFNS QST protocol does exam the pain
response to a single strength pin-prick applied multiple times to exam for the presence
of wind-up phenomenon; and whilst not strictly the same, this is perhaps a more
comparable test to the one used by Simpson and collaborators. Interestingly the current
study’s sub-group of raised WUR in 14% subjects (n=4) in painful HIV-SN
participants, is of similar proportion to the pin-prick hyperalgesia sub-group seen in
Simpson and collaborators’ work (13%) and therefore the raised WUR sub-group
might represent the same pin-prick hyperalgesia sub-group seen in the Simpson and
collaborators’ study. The pin-prick hyperalgesia group of the Simpson and
collaborators’ study is important as this group demonstrated a greater therapeutic
response to pregabalin. Future studies would need to determine if these two findings
indeed represent the same sub-group, as it would potentially have important
mechanistic and therapeutic implications for HIV-SN and neuropathic pain per se.
86
As higher levels of catastrophization have been previously shown to correlate with the
presence of wind-up phenomenon (Vase et al., 2011), a post-hoc analysis of
catastrophization was undertaken for this high wind-up sub-group. It was found that
this sub-group of participants demonstrated higher levels of catastrophization (PCS
total=26.0 (IQR 22.5 - 31.5) vs the other participants, PCS total=2.0 (IQR 0 - 22.0); p
< 0.05; Mann Whitney Rank Sum Test). A correlation between raised wind-up
phenomena and catastophising traits has previously been seen in a study of an upper-
limb amputees with phantom limb pain, but this is, to our knowledge, the first time this
has been shown in a painful peripheral neuropathy population. This is additionally
interesting as it shows that wind-up and catastrophizing are associated in two very
different forms of neuropathic pain, perhaps showing a common mechanism of
interaction between spinal pain processing (wind-up) and higher centres
(catastrophizing) in different types of neuropathic pain.
The hierarchical cluster dendrogram of QST data (Figure 3.6) shows that the majority
of the participants divide at a high level broadly into HIV-SN and HIV-No SN: 71% of
all HIV-SN participants are contained within a cluster of 25 subjects. The hierarchical
cluster analysis shows that HIV-SN neuropathy participants tend to cluster together.
Interestingly participants with HIV-SN but no pain (n=7) were more evenly distributed
and did not appear to associate with the HIV-SN dominant cluster or each other. This
suggests that non-painful HIV-SN perhaps have different QST characteristics to
painful HIV-SN. Whilst its difficult to say that this is a robust finding as the study was
not powered primarily for such a hierarchical cluster analysis, the differences between
painful and non-painful HIV-SN seen here suggest that this should be investigated by
future larger studies.
Intra-epidermal nerve fibre densities
Mean IENFD counts were significantly lower in the HIV-SN group (9.2 fibres/mm vs
6.3fibres/mm), and the severity of neuropathy was inversely correlated to IENFD.
However the diagnostic utility of IENFD counts <7.63 fibres/mm can only be
considered moderate at best with a sensitivity and specificity of 61% and 79% in
isolation of detecting HIV-SN (Table 3.10). Consistent with several other studies, no
convincing correlation was found between IENFD and sensory nerve fibre dysfunction
87
for individual QST parameters (Table 3.5), even in the small fibre modalities of CDT,
WDT, HPT, MPT and PPT (Cruccu et al., 2010).
Metabolic factors
This study found significantly higher random plasma TRG concentrations in the HIV-
SN group compared to the HIV-No SN group. Whilst no correlation was identified
between TRG concentrations and the neuropathy severity, this finding further
underlines the emerging understanding in the literature that dyslipidaemia is important
in the development of HIV-SN (Ances et al., 2009; Banerjee et al., 2011) as well as
diabetic peripheral neuropathy (Vincent, Hinder, Pop-busui, & Feldman, 2009; Wiggin
et al., 2009). In this study there was no difference in statin use between the two groups,
however, an important future question is if more effective or earlier suppression of
raised TRGs might reduce the risk or delay the progression of HIV-SN development.
The role of other metabolic factors in this study is less clear, as no differences were
seen in BMI, random plasma glucose, waist-hip circumferences or other plasma lipids
between the HIV-SN and HIV-No SN groups.
Psychological co-morbidity and sleep disturbance
Participants with painful HIV-SN show significant interference from pain on the BPI
instrument and had significantly reduced quality of life compared to participants
without neuropathy across most of the domains of the SF-36. The largest differences
seen between the two groups were in domains of physical functioning (PF) and social
functioning (SF); indicating that painful HIV-SN profoundly interferes with everyday
tasks, social interaction and relationships. This is comparable to changes seen in other
painful peripheral neuropathies, however, HIV-SN appear to have lower mean scores
across all domains implying greater disability (Poliakov & Toth, 2011). Compared to
other painful peripheral neuropathies, a difference was seen in participants perception
of general health (GH; HIV-SN= 26.58, SD 19.8 vs HIV-No SN=50.3, SD 10.7) This
low general health perception has been previously identified as characteristic of
individuals with HIV infection (Drewes, Gusy, & Rüden, 2013), but appears to be
further reduced by HIV-SN. Interestingly bodily pain (BP) perception values were very
comparable to other painful peripheral neuropathies that did not include HIV-SN, this
is despite HIV-SN participants having a higher mean VAS (HIV-SN=5.65, SD 1.76 vs
HIV-No SN=4.6, SD 2.4) to that study.
88
Pain related anxiety symptoms measured using the PASS-20 were similar across most
domains to that previously seen in a recent study using the same instrument comparing
lower back pain (LBP) and post-herpetic neuralgia (PHN) patients (Daniel et al.,
2008). However HIV-SN patients would appear to be less likely to have
escape/avoidance behaviour in response to pain than either PHN or LBP patients.
Whilst depression and anxiety symptoms were more common in the HIV-SN group, a
greater difference was seen in catastrophizing behaviours in the HIV-SN compared to
those who did not suffer with a painful neuropathy. The majority of this difference was
seen in the PCS helplessness domain. This may well be a reflection of the relatively
low levels of less escape/avoidance behaviour seen in HIV-SN compared to other pain
states (Daniel et al., 2008; Poliakov & Toth, 2011).
There have been numerous sleep laboratory and self report studies examining insomnia
in HIV infected individuals (Reid & Dwyer, 2005). However the current significance
of insomnia in HIV-infection is unclear, as its reported prevalence ranges from the
same as the general population (D. Perkins et al., 1995) to 73% of HIV infected
individuals (Rubinstein & Selwyn, 1998). Early pre-cART era studies suggested that
CD4 count (Brown, Mitler, & Atkinson, 1991), cognitive impairment (Rubinstein &
Selwyn, 1998) and ARV therapy (Nokes & Kendrew, 2001) were important risk
factors for insomnia in HIV positive patients. More recent studies continue to
demonstrate insomnia in HIV positive individuals, but do not correlate as convincingly
with earlier risk factors (Cruess et al., 2003; Lee, Portillo, & Miramontes, 2001). Few
studies have discussed the role of pain or neuropathy in HIV-associated insomnia. In
the present study we have shown a large difference in the incidence of insomnia
between the patients with HIV-SN (68%) and those without (23%; p < 0.001). As it is
established that other forms of neuropathic pain have a high co-incidence of insomnia
(Langley, Van Litsenburg, Cappelleri, & Carroll, 2013), the role neuropathic pain and
insomnia in HIV-SN would appear to be a useful area to explore in future studies.
The PINS-HIV study demonstrates that the presence of painful HIV-SN has a marked
impact on individuals’ quality of life as measured by the SF-36, DAPOS, ISI and BPI.
In particular participants with painful HIV-SN have reduced vitality, social
functioning, emotional functioning.
89
If time had allowed I would have liked to have performed a more detailed analysis of
the psychological outcomes to see if there was indeed any clustering of certain
psychological attributes or dysfunction that could be corresponded to severity of pain
or neuropathy. The presence of high catastrophising scores (PCS) within the high
WUR group supports the idea that perhaps testing for high WUR groups through the
use of simple psychological testing is possible. It is clear that further exploration of
this area would be useful.
Diagnostic tools
The use of a robust composite HIV-SN definition is useful for research purposes, but
would prove too time consuming and require expensive diagnostic equipment for
routine use in most clinical practices. This is especially so in poorly resourced settings.
Part of the objectives of this study was to investigate the utility of neuropathy
screening tools that might be useful in such situations. Therefore in this study the
BPNS, TCSS and the UENS were compared.
The BPNS has been used as the screening tool for several HIV-SN studies (C L Cherry
et al., 2009; Catherine L Cherry et al., 2008; Smyth et al., 2007; Antonia L Wadley et
al., 2011). Whilst its utility is clear, we found that both, the TCSS and the UENS were
superior in the diagnosis of HIV-SN in our population in a head-to-head comparison
against this study’s triumvirate diagnostic criteria. The UENS has been used in a
proportion of one study of HIV-SN where it showed correlation with measures of
cutaneous autonomic function and pain (Boger et al., 2012). This current study is, to
our knowledge, the first validation of the UENS and TCSS in HIV-SN diagnosis.
The original validation study for the UENS did not suggest a cut-off score for
determining the presence of a peripheral neuropathy (Singleton et al., 2008). However,
in the present study, giving equal weight to sensitivity and specificity, a cut off value
of 7 was selected. In that studies population it is associated with a sensitivity and
specificity of 84%. The utility of the UENS was superior to both the TCSS (79%) and
the BPNS (76%) in detecting HIV-SN when tested against the triumvirate multimodal
scoring system. The utility of the BPNS as determined in this population is similar to
that seen in previous larger studies (D M Simpson et al., 2006) and underlines that this
90
relatively small study population behaved as expected, and also that the triumvirate
definition used as a gold standard in the study was a valid one.
Epidemiological studies
Using the triumvirate criteria definition for HIV-SN, in this study, HIV-SN showed a
prevalence of 43% with 75% of these participants suffering with a painful neuropathy.
This is very similar to that seen in recent large epidemiological studies of HIV
populations in both well and poor resourced countries (Catherine Louise Cherry et al.,
2012). In the cART era HIV-SN prevalence is consistently found to be approximately
40% in many different HIV populations (Wenlong Huang et al., 2013; Kamerman,
Moss, et al., 2012; Maratou et al., 2009; Wallace, Blackbeard, Pheby, et al., 2007;
Wallace, Blackbeard, Segerdahl, et al., 2007b). This reinforces the face validity of the
triumvirate criteria used in this work and makes it likely that this study’s findings
would be applicable to larger HIV populations and in different settings. However, this
study did not find important some of the well-established risk factors for the
development of HIV-SN in the cART era in this study population. In particular, no
significant difference or correlation with HIV-SN severity was seen between the HIV-
SN and HIV-No SN group for height and age. The reasons for these are probably two-
fold: Firstly, the study reflects the studied population, which is generally white, middle
aged, male and tall and therefore, it would be difficult for this study to elucidate risk
factors that have been found in much more heterogeneous epidemiological studies.
Secondly, the current study was powered as a detailed phenotyping study and was not
large enough to elucidate these risk factors compared to substantially larger
epidemiological studies (C L Cherry et al., 2009; Ellis et al., 2010; Maritz et al., 2010;
Smyth et al., 2007; Wright et al., 2008).
Summary
This study has demonstrated that the sensory nerve dysfunction that occurs in HIV-SN
is heterogenic as measured with QST. The most frequent changes seen in QST where
loss of function in the large fibre parameters of mechanical and vibration detection.
This further emphasises the large sensory nerve fibre involvement that occurs in HIV-
SN despite it frequently being considered a small fibre neuropathy in the literature. The
diagnostic utility and limitation of QST, IENFD and clinical examination in isolation
91
has been demonstrated. This study has validated the use of UENS and TCSS in the
diagnosis of HIV-SN both of which were found to be superior in HIV-SN diagnosis in
this study population. This study also further supported the growing evidence that lipid
dyslipidaemia is an important factor in the development of HIV-SN. Moreover, painful
HIV-SN also appears to have a greater negative impact on quality of life when
compared to other painful polyneuropathies, post-herpetic neuralgia and lower back
pain.
Future work should determine the triumvirate diagnostic criteria’s validity and utility
in other HIV populations. Detailed examination of individual components of
diagnostic tools should be investigated as there is an urgent need to produce a simple
and robust diagnostic tool for both large epidemiological studies in low resource
environments and for the use in future therapeutic efficacy trials.
Study limitations
A potential criticism of the study is that after the start of study recruitment, the joint
EFNS/ PNS guidelines on the use of skin biopsies for the diagnosis of small fibre
neuropathies was updated (Cruccu et al., 2010) to recommend the use of sex and age
matched healthy control data (Bakkers et al., 2009). However, Nebuchennykh and
collaborators identified that the method used in determining IENFD cut-off values is
very important to the IENFD test’s final sensitivity and specificity (Nebuchennykh et
al., 2009). In this study, comparisons were made using less than fifth-percentile values,
a ROC analysis or using fifth-percentile of age and decade matched normal values (z-
scores) as “cut-off” values as recommended by the EFNS/PNS 2010 guidelines. Age
and sex adjusted cut-off values produced the best specificity (98%) but resulted in
much poorer sensitivity (31%); using a ROC analysis with a higher “cut-off” value of
10.3 fibres/mm produced improved sensitivity (78%) but resulted in a poorer
specificity (64%). The lower “cut-off” value of 7.63 fibres/mm proposed by Devigili
and collaborators (Devigili et al., 2008) is associated with a specificity of 90% and a
sensitivity of 80% and represents a compromise between the z-score and ROC methods
of Nebuchennykh and collaborators’ study.
My opinion was that the use of age and sex matched “cut-offs” would improve
specificity from 90 to 98%, but sensitivity would be excessively reduced to
92
approximately 30% and this was not acceptable for the aims of the current study.
Consequently, 7.63 fibres/mm continued to be used as the cut-off value in the
triumvirate HIV-SN definition.
To explore the impact of using the newer guidelines on IENFD use a post-hoc analysis
of using the EFNS/PNS 2010 guideline age and sex matched values was performed
using the recommended normative values (Bakkers et al., 2009) in conjunction with
this study’s diagnostic triumvirate. This analysis demonstrated no change in the
participants originally allocated to HIV-No SN group, however five participants
(7.6%) previously allocated to HIV-SN group were now allocated to HIV-No SN. This
was felt to be acceptable as the difference is proportional to that which would be
expected using this more conservative definition of HIV-SN. Additionally, 3 of the 5
(60%) participants who’s diagnosis was altered by the re-analysis to HIV-No SN
complained of a painful peripheral neuropathy, confirming that the diagnosis of HIV-
SN was indeed the correct one for these participants.
A further potential limitation of the study is that several items of the multimodal
triumvirate definition for HIV-SN are compared and contrasted between the HIV-No
SN group and the HIV-SN group. There is therefore potential for a circular argument
relating to the QST and IENFD findings of this study; however this is minimal, as a
post-hoc re-analysis using different combinations of the triumvirate (Table 3.10) shows
that the neuropathy diagnosis of individual participants was not dramatically altered by
the removal of individual items from the definition. Removal of QST resulted in 12%
of the study participants having an altered diagnosis, and IENFD only 9%. The single
most important factor of the definition was found to be the SNE which when removed
from the definition altered the diagnosis of 26% of the participants.
Further post-hoc exploration of using different HIV-SN definitions on QST results
A post-hoc exploration of the impact of the HIV-SN case definition on one of the main
outcome measures of the study, QST evaluation was undertaken.
Three additional different case definitions were used:
1. Using the BPNS definition of HIV-SN alone to determine neuropathy status.
2. Using the Structured Neurological Examination (SNE) alone to determine neuropathy
status.
93
3. Using only the reported symptoms of paraesthesia and/or numbness to determine
neuropathy status.
BPNS
The BPNS was chosen for further exploration, as it is a well-established screening tool
for HIV-SN that has been used in many previous studies of HIV-SN. Using the BPNS
to determine HIV-SN status resulted in similar proportions to that when using PINS-
HIV criteria: n=37 for HIV-No SN and n=29 for HIV-SN (Table 3.11 and Figure
3.2.b). However there are larger differences in individual neuropathy allocations: eight
individual allocations are changed from HIV-No SN to HIV-SN, and seven from HIV-
SN to HIV-No SN. The mean z score values are similar for HIV-SN and HIV-No SN
however the proportion of individuals demonstrating loss and gain of sensory function
on QST is different. Interestingly the high WUR ‘cluster’ seen with the PINS criteria is
larger using the BPNS (five/six with BPNS versus four participants with PINS). The
high WUR cluster also appears more separated from the lower WUR HIV-SN group.
Whilst the overall conclusions regarding QST changes seen in HIV-SN would be
similar
The finding that using the BPNS as a HIV-SN criteria produces similar results, and
demonstrates a similar interesting feature of a cluster of HIV-SN participants with
raised WUR is supportive of the findings seen in the PINS study, as it demonstrates
that this novel high WUR is not a result of the new HIV-SN definition used.
Structured Neurological Examination (SNE)
The use of the SNE tended to ‘over’ diagnose HIV-SN in comparison to the PINS
criteria, with ten more subjects being allocated to HIV-SN compared to PINS; n=38
for HIV-SN and n=28 for HIV-No SN. The allocation of individuals with HIV-SN
however resulted in a smaller cluster of high WUR in the HIV-SN.
Paraesthesia and numbness symptoms
Using self reported symptoms of peripheral neuropathy (paraesthesia and /or numbness
symptoms) tended to over diagnose HIV-SN compared to using the PINS criteria.
HIV-SN n=43 and HIV-No SN n=23. Despite a larger group of HIV-SN the high
WUR remained similar with four participants present.
94
Pain
Using pain as the definition of HIV-SN interestingly produced identical proportions of
patients allocated to HIV-SN and HIV-No SN; however seven participants were
reallocated from HIV-SN to No SN and seven from HIV-No SN to HIV-SN so the
situation is not identical. Once again similar mean z score values were seen and a
similar high WUR cluster in HIV-SN group
The overall QST findings for each of the different criteria tested are similar to using
the PINS criteria: i.e. a ‘loss’ of sensory function dominated picture, with the most
affected modalities being MDT and VDT in the HIV-SN groups (Table 3.11 and 3.12).
More affected by the changes of definition however is the detail of the number of
individuals who show loss and gain in areas of interest such as WUR. The relatively
small number of participants in the PINS-HIV study probably heightens this sensitivity
to the definition of HIV-SN.
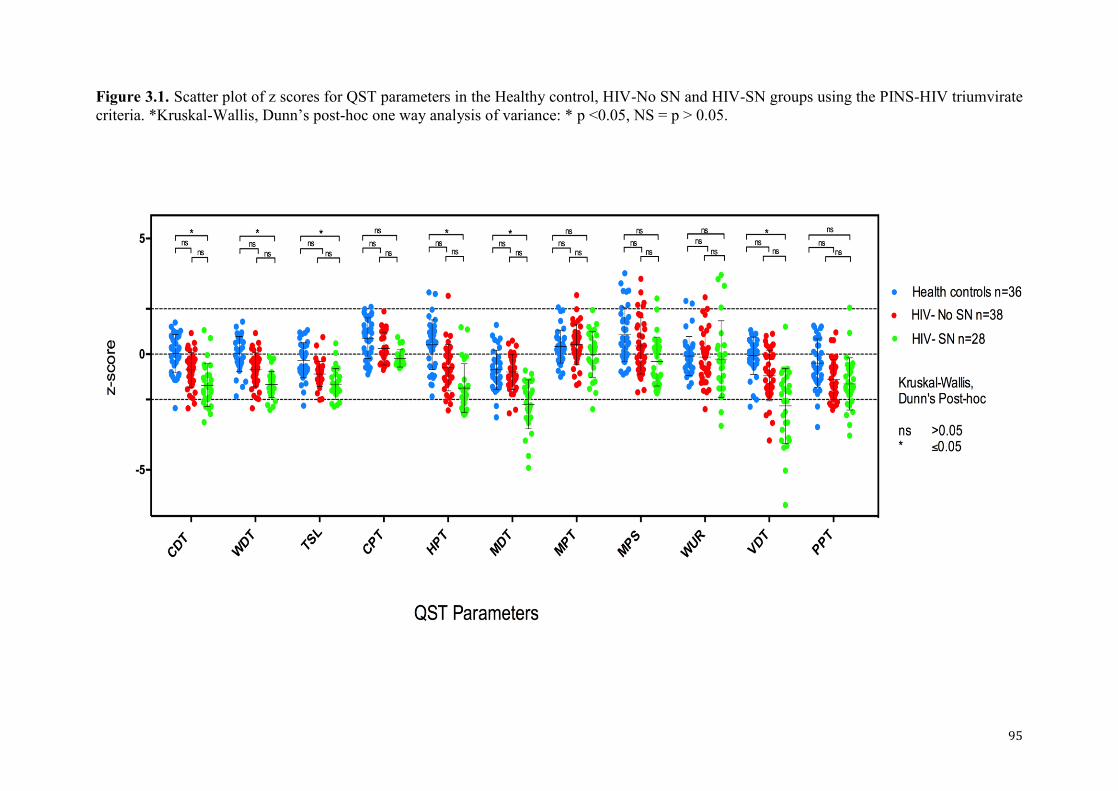
95
Figure 3.1. Scatter plot of z scores for QST parameters in the Healthy control, HIV-No SN and HIV-SN groups using the PINS-HIV triumvirate criteria. *Kruskal-Wallis, Dunn’s post-hoc one way analysis of variance: * p <0.05, NS = p > 0.05.
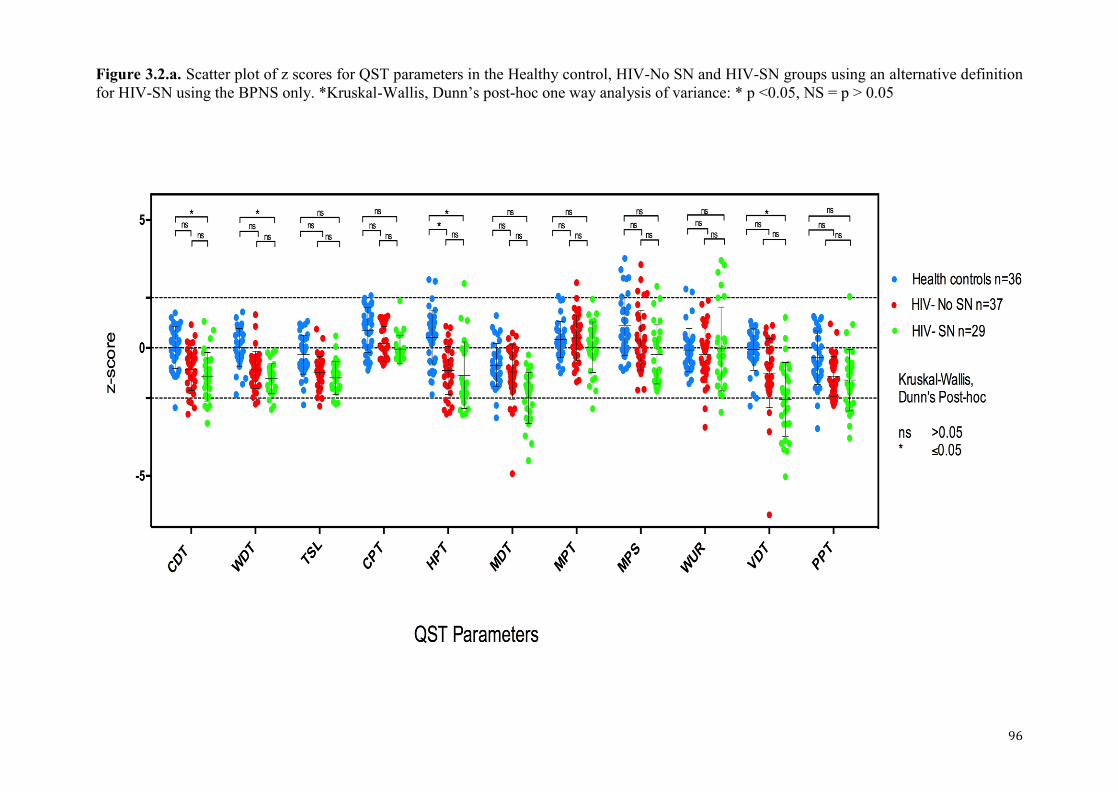
96
Figure 3.2.a. Scatter plot of z scores for QST parameters in the Healthy control, HIV-No SN and HIV-SN groups using an alternative definition for HIV-SN using the BPNS only. *Kruskal-Wallis, Dunn’s post-hoc one way analysis of variance: * p <0.05, NS = p > 0.05
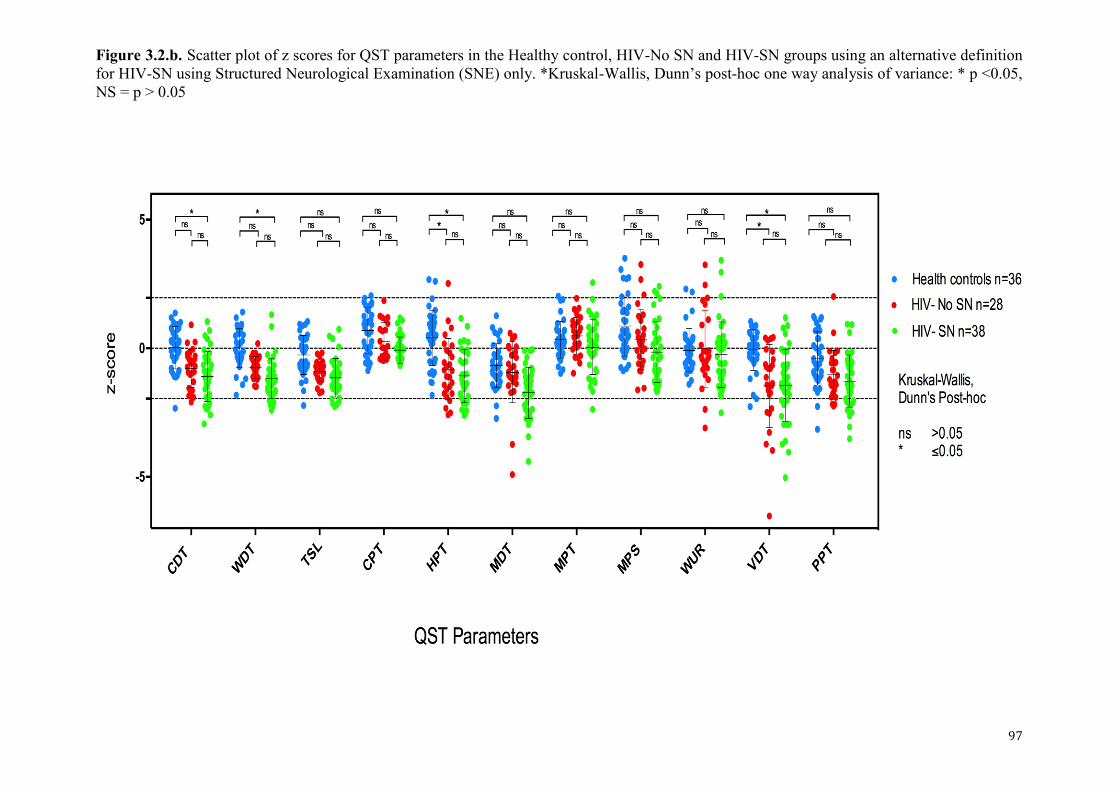
97
Figure 3.2.b. Scatter plot of z scores for QST parameters in the Healthy control, HIV-No SN and HIV-SN groups using an alternative definition for HIV-SN using Structured Neurological Examination (SNE) only. *Kruskal-Wallis, Dunn’s post-hoc one way analysis of variance: * p <0.05, NS = p > 0.05
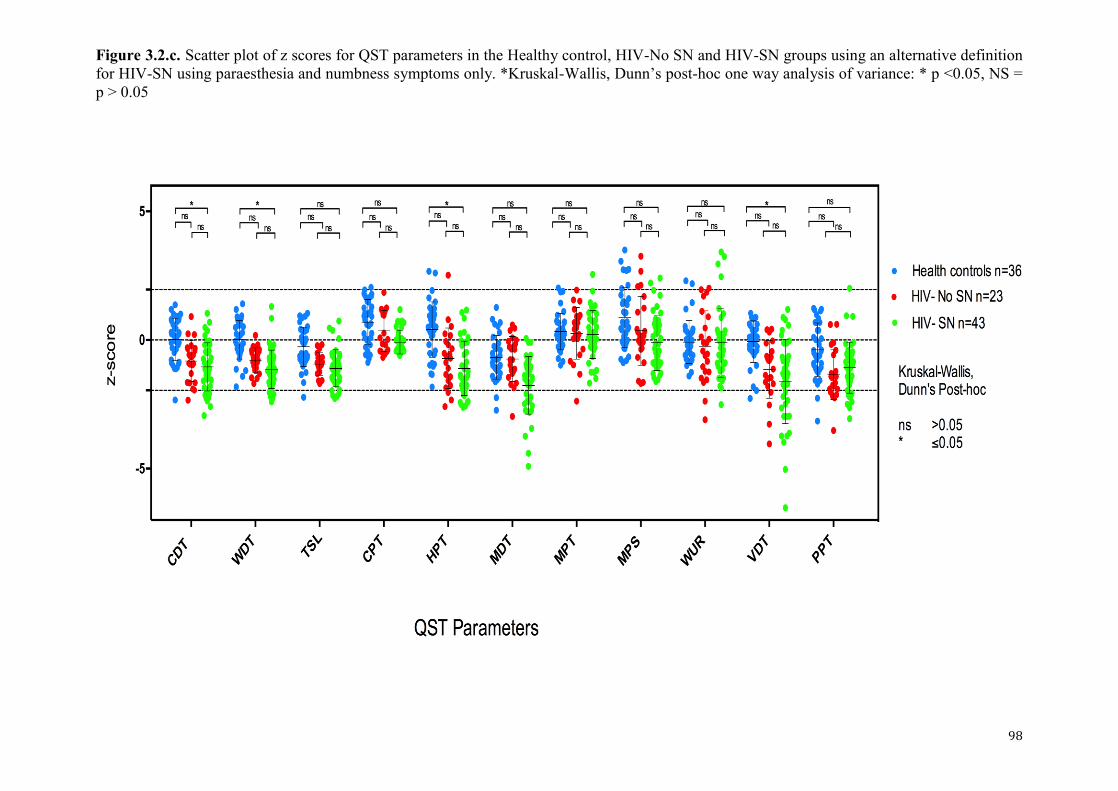
98
Figure 3.2.c. Scatter plot of z scores for QST parameters in the Healthy control, HIV-No SN and HIV-SN groups using an alternative definition for HIV-SN using paraesthesia and numbness symptoms only. *Kruskal-Wallis, Dunn’s post-hoc one way analysis of variance: * p <0.05, NS = p > 0.05
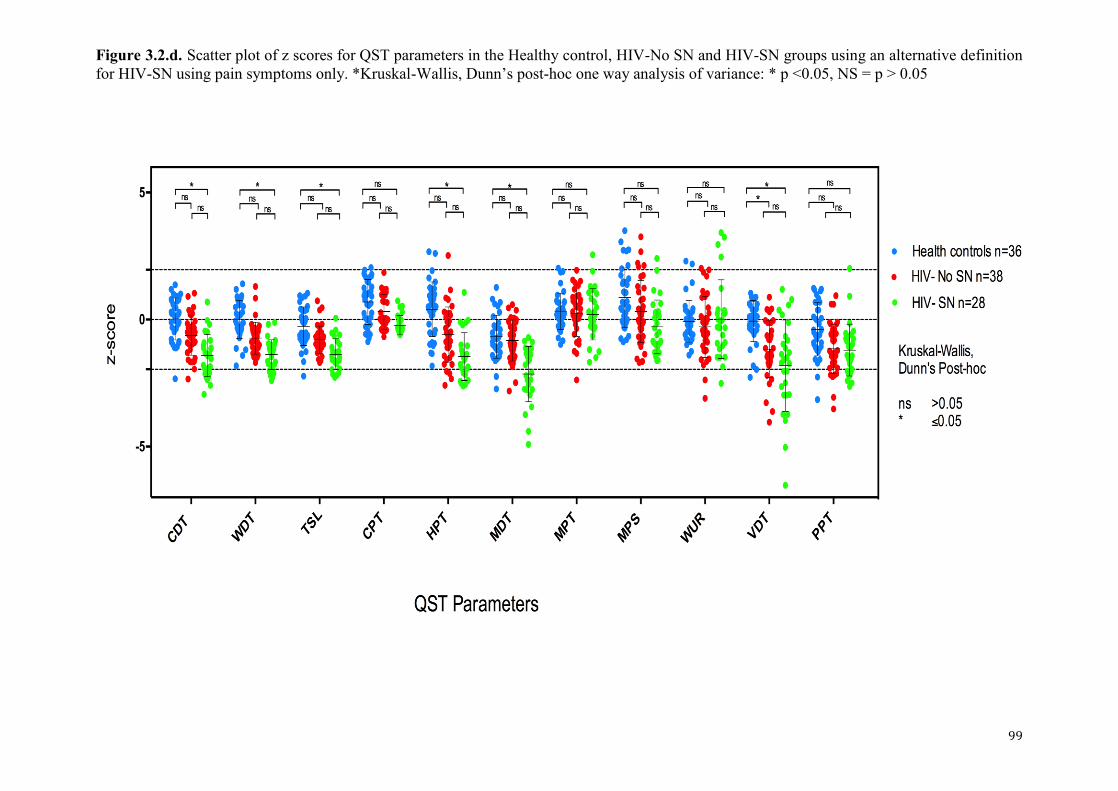
99
Figure 3.2.d. Scatter plot of z scores for QST parameters in the Healthy control, HIV-No SN and HIV-SN groups using an alternative definition for HIV-SN using pain symptoms only. *Kruskal-Wallis, Dunn’s post-hoc one way analysis of variance: * p <0.05, NS = p > 0.05
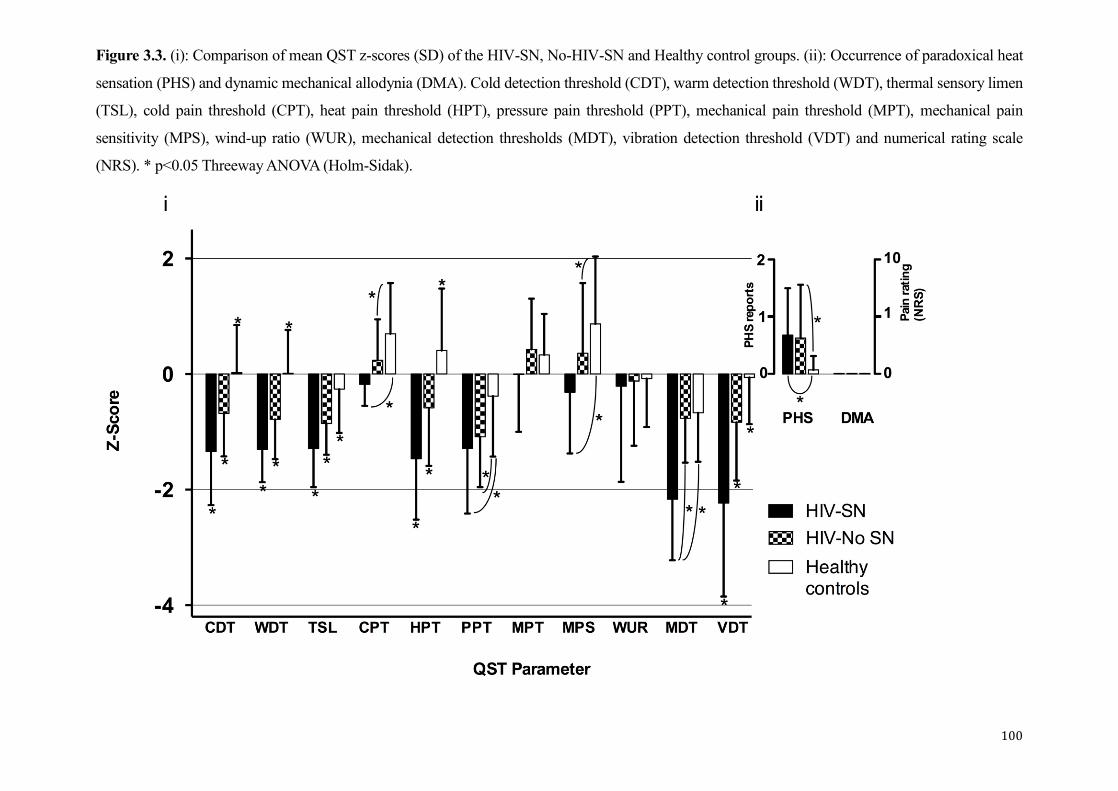
100
Figure 3.3. (i): Comparison of mean QST z-scores (SD) of the HIV-SN, No-HIV-SN and Healthy control groups. (ii): Occurrence of paradoxical heat
sensation (PHS) and dynamic mechanical allodynia (DMA). Cold detection threshold (CDT), warm detection threshold (WDT), thermal sensory limen
(TSL), cold pain threshold (CPT), heat pain threshold (HPT), pressure pain threshold (PPT), mechanical pain threshold (MPT), mechanical pain
sensitivity (MPS), wind-up ratio (WUR), mechanical detection thresholds (MDT), vibration detection threshold (VDT) and numerical rating scale
(NRS). * p<0.05 Threeway ANOVA (Holm-Sidak).
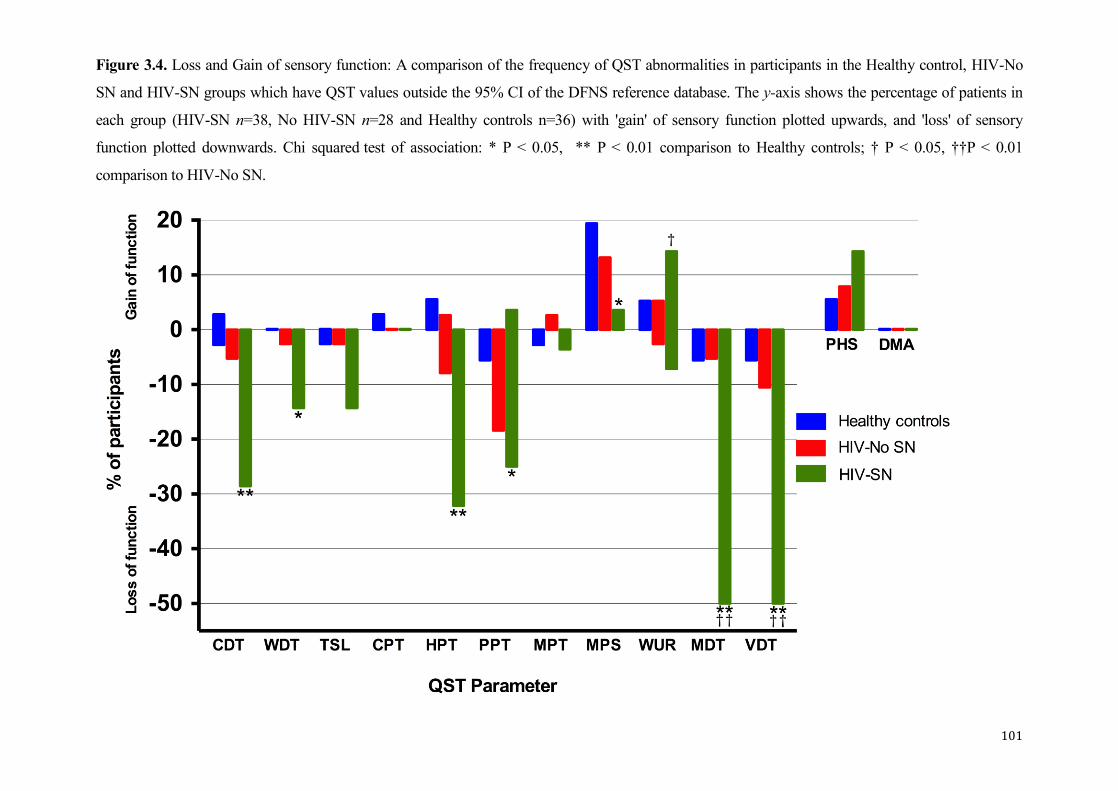
101
Figure 3.4. Loss and Gain of sensory function: A comparison of the frequency of QST abnormalities in participants in the Healthy control, HIV-No
SN and HIV-SN groups which have QST values outside the 95% CI of the DFNS reference database. The y-axis shows the percentage of patients in
each group (HIV-SN n=38, No HIV-SN n=28 and Healthy controls n=36) with 'gain' of sensory function plotted upwards, and 'loss' of sensory
function plotted downwards. Chi squared test of association: * P < 0.05, ** P < 0.01 comparison to Healthy controls; † P < 0.05, ††P < 0.01
comparison to HIV-No SN.
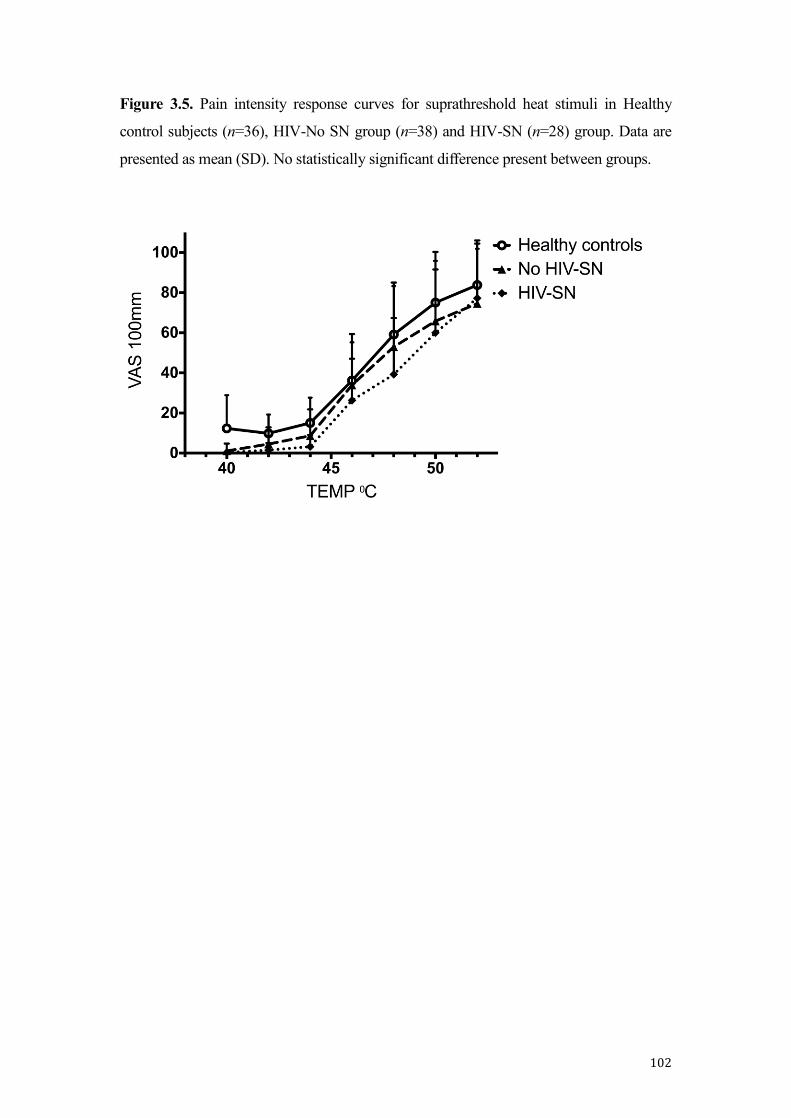
102
Figure 3.5. Pain intensity response curves for suprathreshold heat stimuli in Healthy
control subjects (n=36), HIV-No SN group (n=38) and HIV-SN (n=28) group. Data are
presented as mean (SD). No statistically significant difference present between groups.
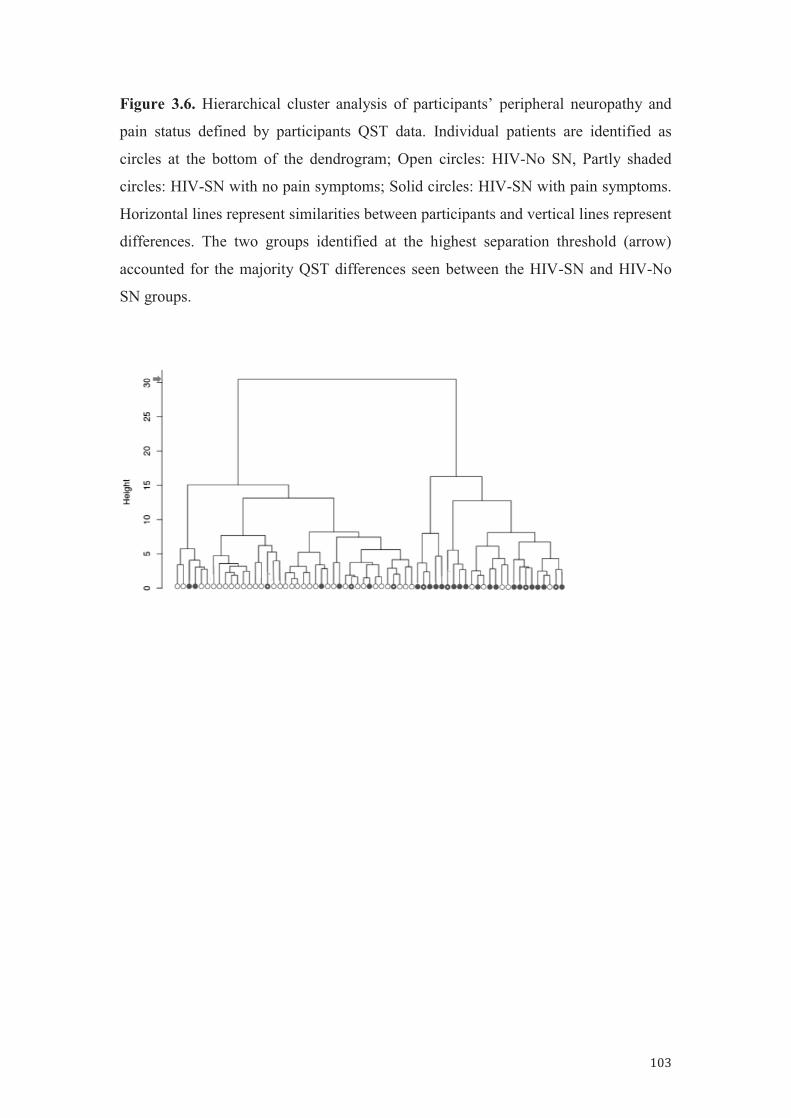
103
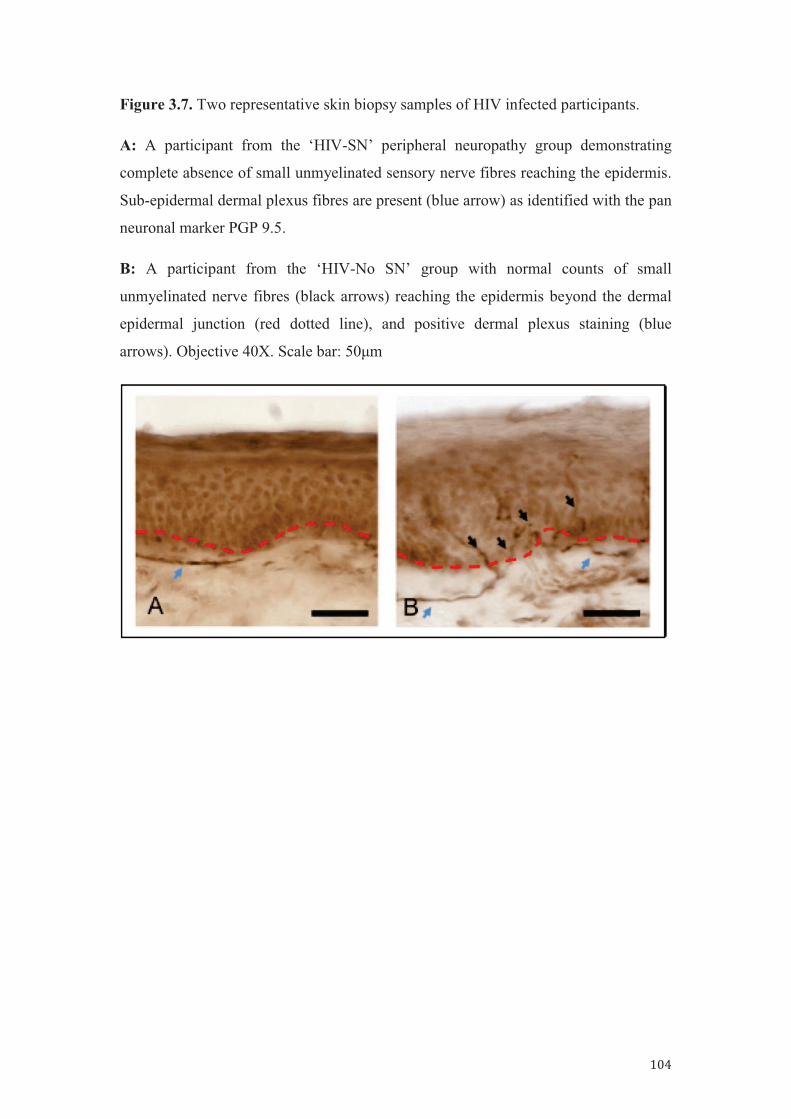
104
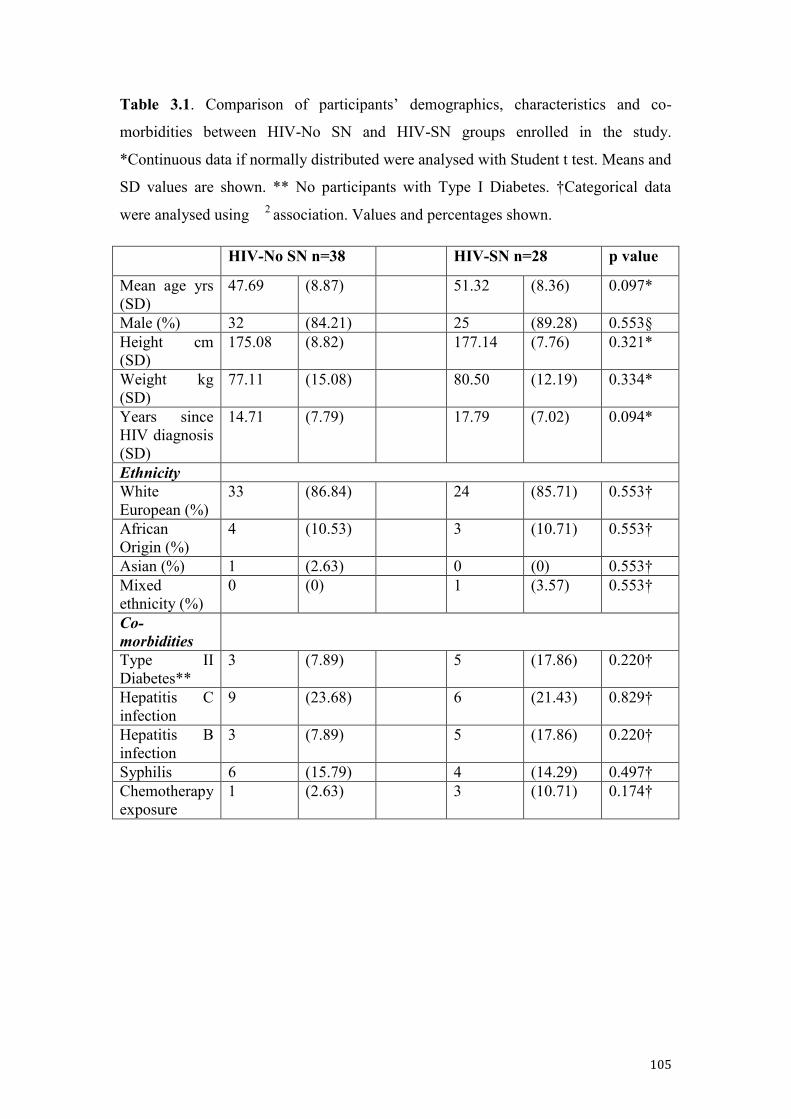
105
Table 3.1. Comparison of participants’ demographics, characteristics and co-
morbidities between HIV-No SN and HIV-SN groups enrolled in the study.
*Continuous data if normally distributed were analysed with Student t test. Means and
SD values are shown. ** No participants with Type I Diabetes. †Categorical data
were analysed using 2 association. Values and percentages shown.
HIV-No SN n=38 HIV-SN n=28 p value
Mean age yrs (SD)
47.69 (8.87) 51.32 (8.36) 0.097*
Male (%) 32 (84.21) 25 (89.28) 0.553§ Height cm (SD)
175.08 (8.82) 177.14 (7.76) 0.321*
Weight kg (SD)
77.11 (15.08) 80.50 (12.19) 0.334*
Years since HIV diagnosis (SD)
14.71 (7.79) 17.79 (7.02) 0.094*
Ethnicity White European (%)
33 (86.84) 24 (85.71) 0.553†
African Origin (%)
4 (10.53) 3 (10.71) 0.553†
Asian (%) 1 (2.63) 0 (0) 0.553† Mixed ethnicity (%)
0 (0) 1 (3.57) 0.553†
Co-morbidities
Type II Diabetes**
3 (7.89) 5 (17.86) 0.220†
Hepatitis C infection
9 (23.68) 6 (21.43) 0.829†
Hepatitis B infection
3 (7.89) 5 (17.86) 0.220†
Syphilis 6 (15.79) 4 (14.29) 0.497† Chemotherapy exposure
1 (2.63) 3 (10.71) 0.174†
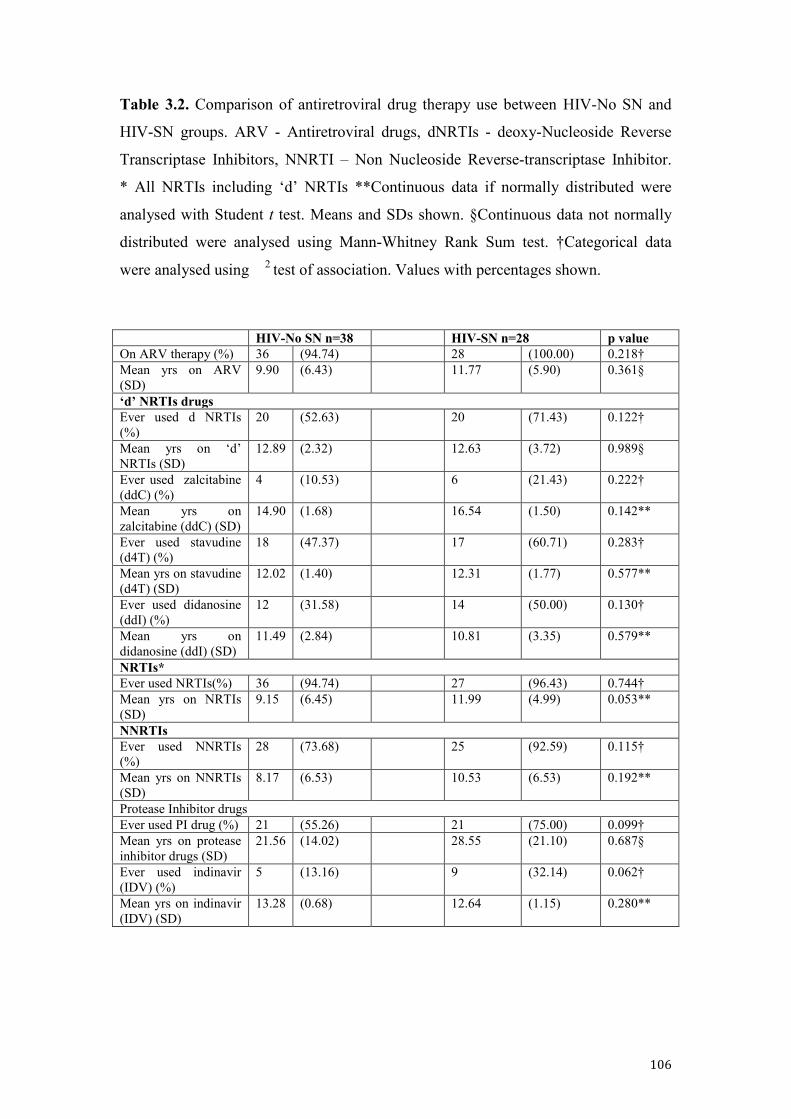
106
Table 3.2. Comparison of antiretroviral drug therapy use between HIV-No SN and
HIV-SN groups. ARV - Antiretroviral drugs, dNRTIs - deoxy-Nucleoside Reverse
Transcriptase Inhibitors, NNRTI – Non Nucleoside Reverse-transcriptase Inhibitor.
* All NRTIs including ‘d’ NRTIs **Continuous data if normally distributed were
analysed with Student t test. Means and SDs shown. §Continuous data not normally
distributed were analysed using Mann-Whitney Rank Sum test. †Categorical data
were analysed using 2 test of association. Values with percentages shown.
HIV-No SN n=38 HIV-SN n=28 p value On ARV therapy (%) 36 (94.74) 28 (100.00) 0.218† Mean yrs on ARV (SD)
9.90 (6.43) 11.77 (5.90) 0.361§
‘d’ NRTIs drugs Ever used d NRTIs (%)
20 (52.63) 20 (71.43) 0.122†
Mean yrs on ‘d’ NRTIs (SD)
12.89 (2.32) 12.63 (3.72) 0.989§
Ever used zalcitabine (ddC) (%)
4 (10.53) 6 (21.43) 0.222†
Mean yrs on zalcitabine (ddC) (SD)
14.90 (1.68) 16.54 (1.50) 0.142**
Ever used stavudine (d4T) (%)
18 (47.37) 17 (60.71) 0.283†
Mean yrs on stavudine (d4T) (SD)
12.02 (1.40) 12.31 (1.77) 0.577**
Ever used didanosine (ddI) (%)
12 (31.58) 14 (50.00) 0.130†
Mean yrs on didanosine (ddI) (SD)
11.49 (2.84) 10.81 (3.35) 0.579**
NRTIs* Ever used NRTIs(%) 36 (94.74) 27 (96.43) 0.744† Mean yrs on NRTIs (SD)
9.15 (6.45) 11.99 (4.99) 0.053**
NNRTIs Ever used NNRTIs (%)
28 (73.68) 25 (92.59) 0.115†
Mean yrs on NNRTIs (SD)
8.17 (6.53) 10.53 (6.53) 0.192**
Protease Inhibitor drugs Ever used PI drug (%) 21 (55.26) 21 (75.00) 0.099† Mean yrs on protease inhibitor drugs (SD)
21.56 (14.02) 28.55 (21.10) 0.687§
Ever used indinavir (IDV) (%)
5 (13.16) 9 (32.14) 0.062†
Mean yrs on indinavir (IDV) (SD)
13.28 (0.68) 12.64 (1.15) 0.280**
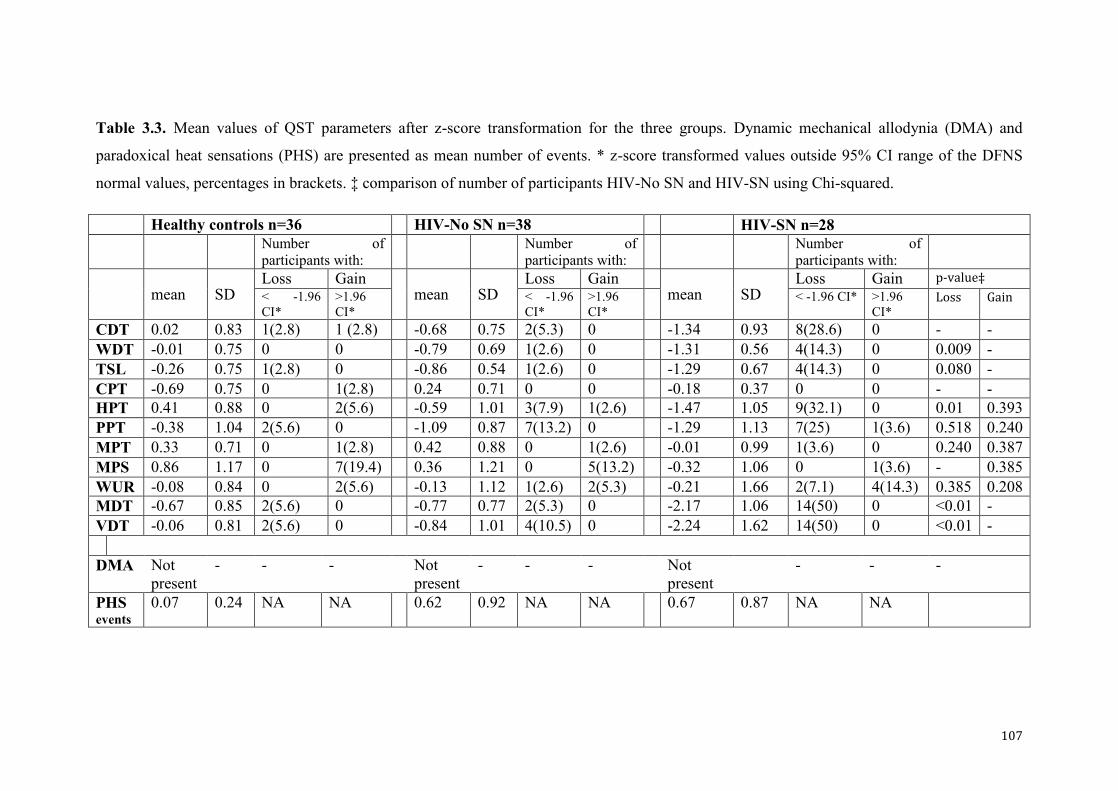
107
Table 3.3. Mean values of QST parameters after z-score transformation for the three groups. Dynamic mechanical allodynia (DMA) and
paradoxical heat sensations (PHS) are presented as mean number of events. * z-score transformed values outside 95% CI range of the DFNS
normal values, percentages in brackets. ‡ comparison of number of participants HIV-No SN and HIV-SN using Chi-squared.
Healthy controls n=36 HIV-No SN n=38 HIV-SN n=28 Number of
participants with: Number of
participants with: Number of
participants with:
mean SD
Loss Gain mean SD
Loss Gain mean SD
Loss Gain p-value‡ < -1.96 CI*
>1.96 CI*
< -1.96 CI*
>1.96 CI*
< -1.96 CI* >1.96 CI*
Loss Gain
CDT 0.02 0.83 1(2.8) 1 (2.8) -0.68 0.75 2(5.3) 0 -1.34 0.93 8(28.6) 0 - - WDT -0.01 0.75 0 0 -0.79 0.69 1(2.6) 0 -1.31 0.56 4(14.3) 0 0.009 - TSL -0.26 0.75 1(2.8) 0 -0.86 0.54 1(2.6) 0 -1.29 0.67 4(14.3) 0 0.080 - CPT -0.69 0.75 0 1(2.8) 0.24 0.71 0 0 -0.18 0.37 0 0 - - HPT 0.41 0.88 0 2(5.6) -0.59 1.01 3(7.9) 1(2.6) -1.47 1.05 9(32.1) 0 0.01 0.393 PPT -0.38 1.04 2(5.6) 0 -1.09 0.87 7(13.2) 0 -1.29 1.13 7(25) 1(3.6) 0.518 0.240 MPT 0.33 0.71 0 1(2.8) 0.42 0.88 0 1(2.6) -0.01 0.99 1(3.6) 0 0.240 0.387 MPS 0.86 1.17 0 7(19.4) 0.36 1.21 0 5(13.2) -0.32 1.06 0 1(3.6) - 0.385 WUR -0.08 0.84 0 2(5.6) -0.13 1.12 1(2.6) 2(5.3) -0.21 1.66 2(7.1) 4(14.3) 0.385 0.208 MDT -0.67 0.85 2(5.6) 0 -0.77 0.77 2(5.3) 0 -2.17 1.06 14(50) 0 <0.01 - VDT -0.06 0.81 2(5.6) 0 -0.84 1.01 4(10.5) 0 -2.24 1.62 14(50) 0 <0.01 - DMA Not
present - - - Not
present - - - Not
present - - -
PHS events
0.07 0.24 NA NA 0.62 0.92 NA NA 0.67 0.87 NA NA
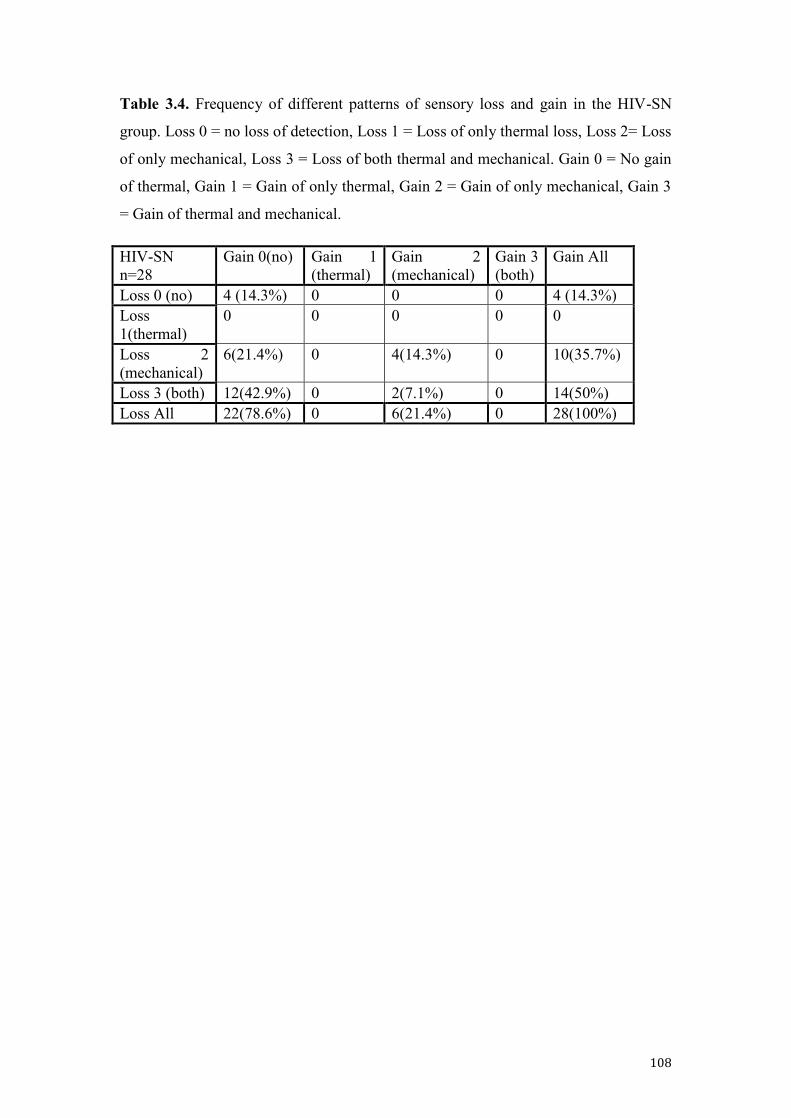
108
Table 3.4. Frequency of different patterns of sensory loss and gain in the HIV-SN
group. Loss 0 = no loss of detection, Loss 1 = Loss of only thermal loss, Loss 2= Loss
of only mechanical, Loss 3 = Loss of both thermal and mechanical. Gain 0 = No gain
of thermal, Gain 1 = Gain of only thermal, Gain 2 = Gain of only mechanical, Gain 3
= Gain of thermal and mechanical.
HIV-SN n=28
Gain 0(no) Gain 1 (thermal)
Gain 2 (mechanical)
Gain 3 (both)
Gain All
Loss 0 (no) 4 (14.3%) 0 0 0 4 (14.3%) Loss 1(thermal)
0 0 0 0 0
Loss 2 (mechanical)
6(21.4%) 0 4(14.3%) 0 10(35.7%)
Loss 3 (both) 12(42.9%) 0 2(7.1%) 0 14(50%) Loss All 22(78.6%) 0 6(21.4%) 0 28(100%)
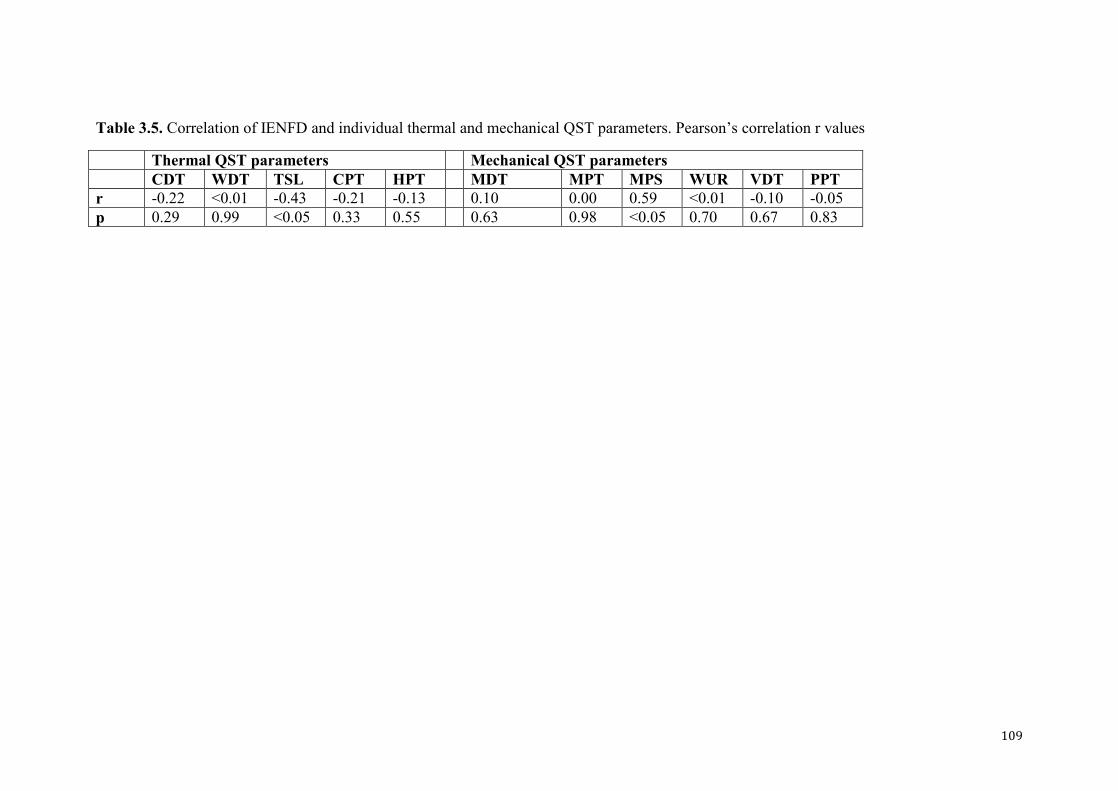
109
Table 3.5. Correlation of IENFD and individual thermal and mechanical QST parameters. Pearson’s correlation r values
Thermal QST parameters Mechanical QST parameters CDT WDT TSL CPT HPT MDT MPT MPS WUR VDT PPT r -0.22 <0.01 -0.43 -0.21 -0.13 0.10 0.00 0.59 <0.01 -0.10 -0.05 p 0.29 0.99 <0.05 0.33 0.55 0.63 0.98 <0.05 0.70 0.67 0.83
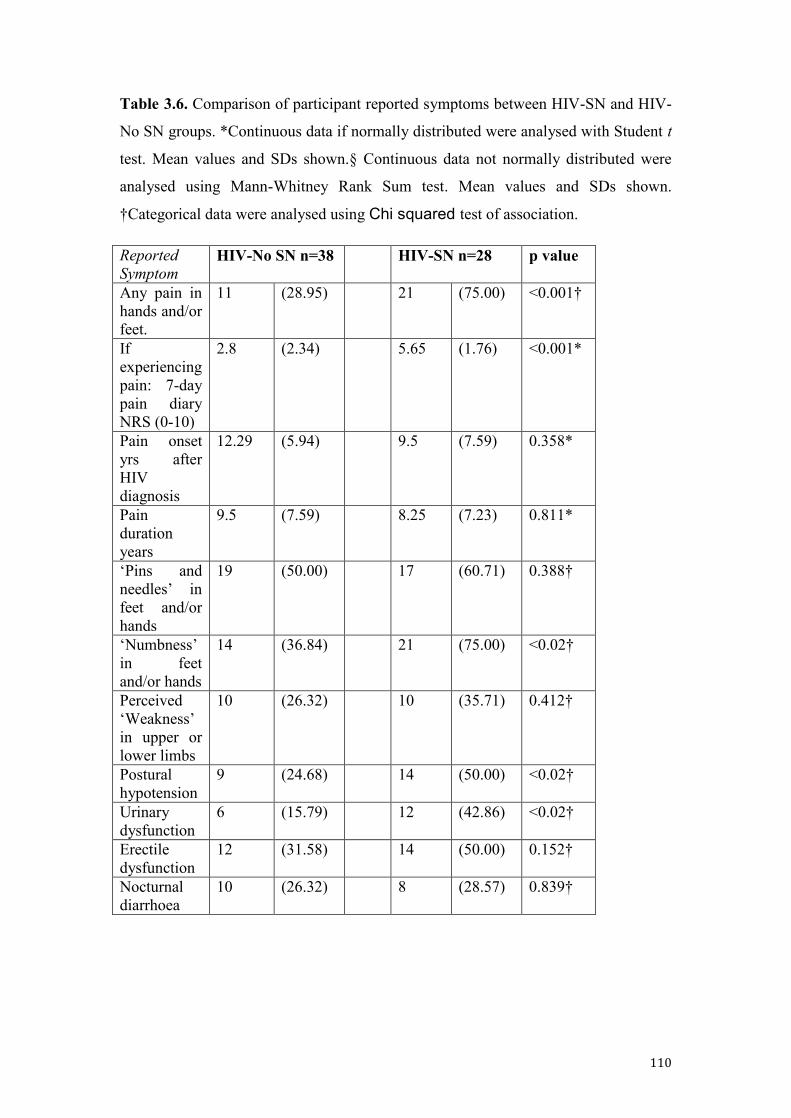
110
Table 3.6. Comparison of participant reported symptoms between HIV-SN and HIV-
No SN groups. *Continuous data if normally distributed were analysed with Student t
test. Mean values and SDs shown.§ Continuous data not normally distributed were
analysed using Mann-Whitney Rank Sum test. Mean values and SDs shown.
†Categorical data were analysed using Chi squared test of association.
Reported Symptom
HIV-No SN n=38 HIV-SN n=28 p value
Any pain in hands and/or feet.
11 (28.95) 21 (75.00) <0.001†
If experiencing pain: 7-day pain diary NRS (0-10)
2.8 (2.34) 5.65 (1.76) <0.001*
Pain onset yrs after HIV diagnosis
12.29 (5.94) 9.5 (7.59) 0.358*
Pain duration years
9.5 (7.59) 8.25 (7.23) 0.811*
‘Pins and needles’ in feet and/or hands
19 (50.00) 17 (60.71) 0.388†
‘Numbness’ in feet and/or hands
14 (36.84) 21 (75.00) <0.02†
Perceived ‘Weakness’ in upper or lower limbs
10 (26.32) 10 (35.71) 0.412†
Postural hypotension
9 (24.68) 14 (50.00) <0.02†
Urinary dysfunction
6 (15.79) 12 (42.86) <0.02†
Erectile dysfunction
12 (31.58) 14 (50.00) 0.152†
Nocturnal diarrhoea
10 (26.32) 8 (28.57) 0.839†
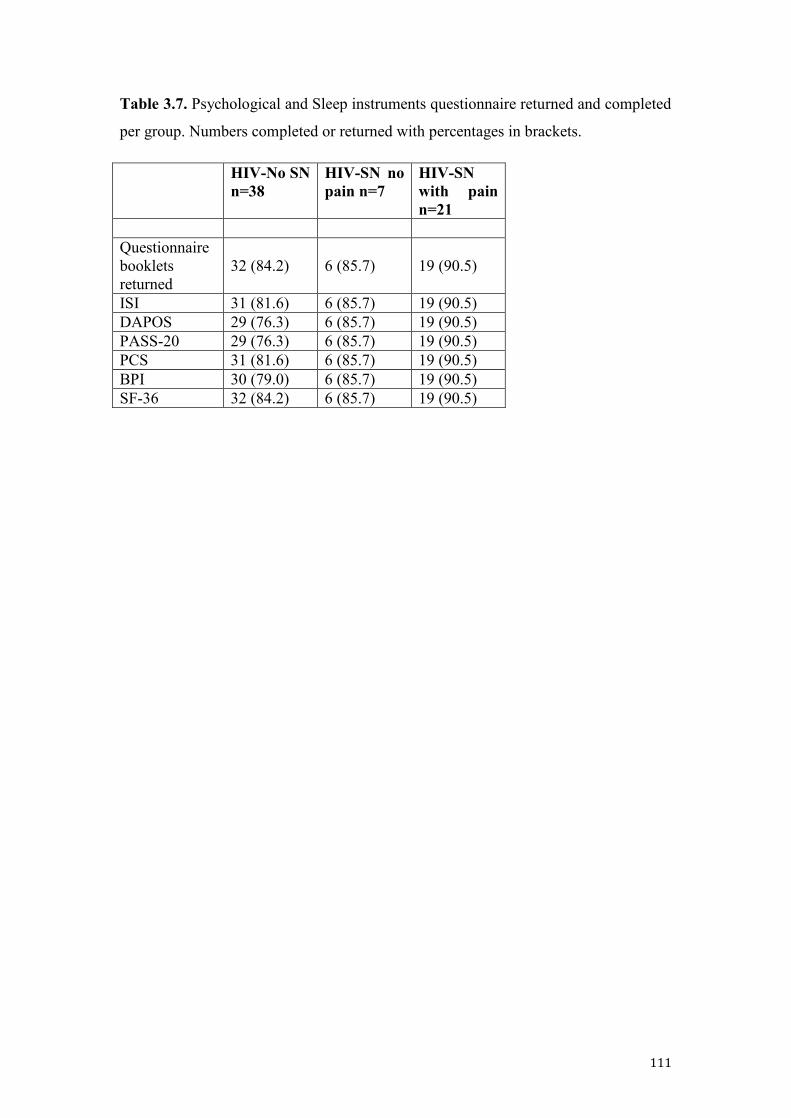
111
Table 3.7. Psychological and Sleep instruments questionnaire returned and completed
per group. Numbers completed or returned with percentages in brackets.
HIV-No SN n=38
HIV-SN no pain n=7
HIV-SN with pain n=21
Questionnaire booklets returned
32 (84.2)
6 (85.7)
19 (90.5)
ISI 31 (81.6) 6 (85.7) 19 (90.5) DAPOS 29 (76.3) 6 (85.7) 19 (90.5) PASS-20 29 (76.3) 6 (85.7) 19 (90.5) PCS 31 (81.6) 6 (85.7) 19 (90.5) BPI 30 (79.0) 6 (85.7) 19 (90.5) SF-36 32 (84.2) 6 (85.7) 19 (90.5)
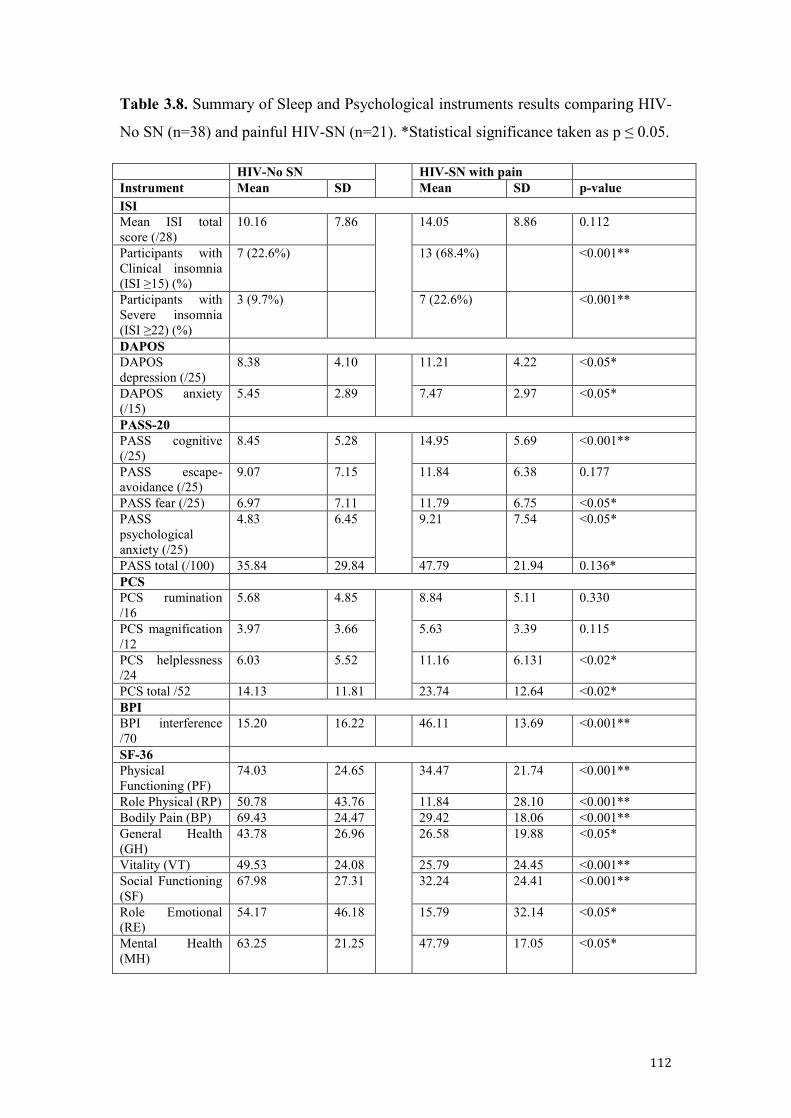
112
Table 3.8. Summary of Sleep and Psychological instruments results comparing HIV-
No SN (n=38) and painful HIV-SN (n=21). *Statistical significance taken as p ≤ 0.05.
HIV-No SN HIV-SN with pain Instrument Mean SD Mean SD p-value ISI Mean ISI total score (/28)
10.16 7.86 14.05 8.86 0.112
Participants with Clinical insomnia (ISI ≥15) (%)
7 (22.6%) 13 (68.4%) <0.001**
Participants with Severe insomnia (ISI ≥22) (%)
3 (9.7%) 7 (22.6%) <0.001**
DAPOS DAPOS depression (/25)
8.38 4.10 11.21 4.22 <0.05*
DAPOS anxiety (/15)
5.45 2.89 7.47 2.97 <0.05*
PASS-20 PASS cognitive (/25)
8.45 5.28 14.95 5.69 <0.001**
PASS escape-avoidance (/25)
9.07 7.15 11.84 6.38 0.177
PASS fear (/25) 6.97 7.11 11.79 6.75 <0.05* PASS psychological anxiety (/25)
4.83 6.45 9.21 7.54 <0.05*
PASS total (/100) 35.84 29.84 47.79 21.94 0.136* PCS PCS rumination /16
5.68 4.85 8.84 5.11 0.330
PCS magnification /12
3.97 3.66 5.63 3.39 0.115
PCS helplessness /24
6.03 5.52 11.16 6.131 <0.02*
PCS total /52 14.13 11.81 23.74 12.64 <0.02* BPI BPI interference /70
15.20 16.22 46.11 13.69 <0.001**
SF-36 Physical Functioning (PF)
74.03 24.65 34.47 21.74 <0.001**
Role Physical (RP) 50.78 43.76 11.84 28.10 <0.001** Bodily Pain (BP) 69.43 24.47 29.42 18.06 <0.001** General Health (GH)
43.78 26.96 26.58 19.88 <0.05*
Vitality (VT) 49.53 24.08 25.79 24.45 <0.001** Social Functioning (SF)
67.98 27.31 32.24 24.41 <0.001**
Role Emotional (RE)
54.17 46.18 15.79 32.14 <0.05*
Mental Health (MH)
63.25 21.25 47.79 17.05 <0.05*
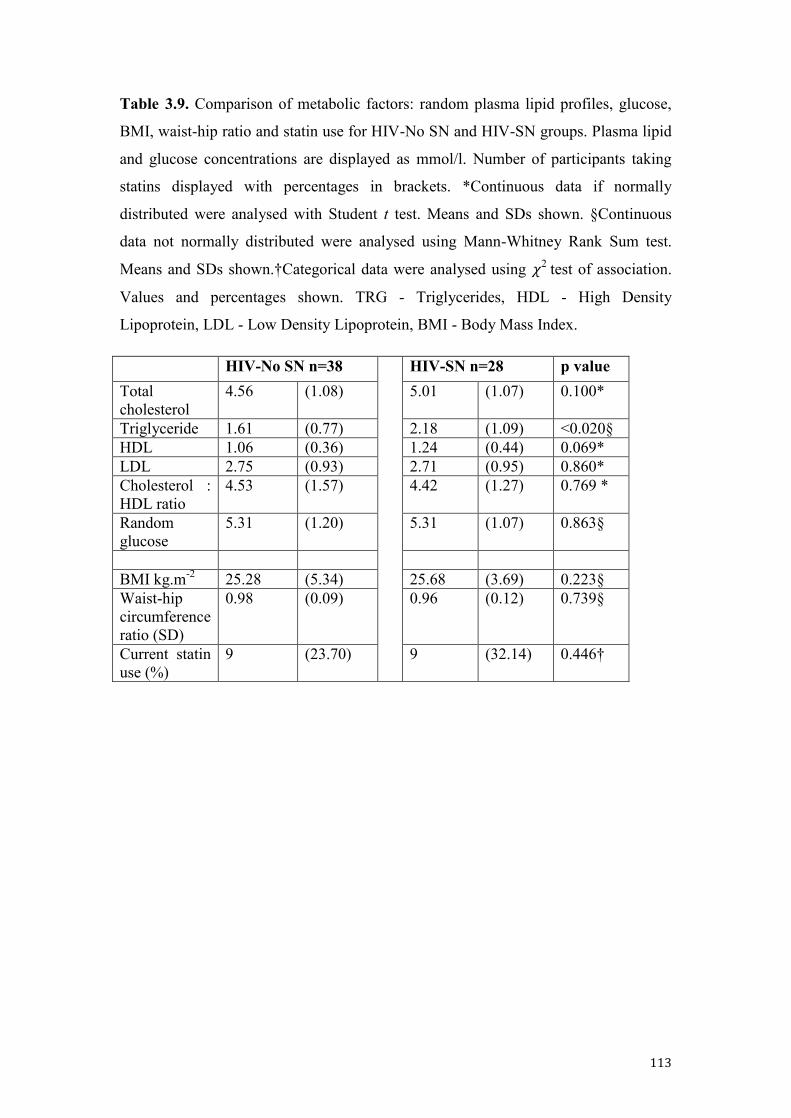
113
Table 3.9. Comparison of metabolic factors: random plasma lipid profiles, glucose,
BMI, waist-hip ratio and statin use for HIV-No SN and HIV-SN groups. Plasma lipid
and glucose concentrations are displayed as mmol/l. Number of participants taking
statins displayed with percentages in brackets. *Continuous data if normally
distributed were analysed with Student t test. Means and SDs shown. §Continuous
data not normally distributed were analysed using Mann-Whitney Rank Sum test.
Means and SDs shown.†Categorical data were analysed using 𝜒2 test of association.
Values and percentages shown. TRG - Triglycerides, HDL - High Density
Lipoprotein, LDL - Low Density Lipoprotein, BMI - Body Mass Index.
HIV-No SN n=38 HIV-SN n=28 p value Total cholesterol
4.56 (1.08) 5.01 (1.07) 0.100*
Triglyceride 1.61 (0.77) 2.18 (1.09) <0.020§ HDL 1.06 (0.36) 1.24 (0.44) 0.069* LDL 2.75 (0.93) 2.71 (0.95) 0.860* Cholesterol : HDL ratio
4.53 (1.57) 4.42 (1.27) 0.769 *
Random glucose
5.31 (1.20) 5.31 (1.07) 0.863§
BMI kg.m-2 25.28 (5.34) 25.68 (3.69) 0.223§ Waist-hip circumference ratio (SD)
0.98 (0.09) 0.96 (0.12) 0.739§
Current statin use (%)
9 (23.70) 9 (32.14) 0.446†
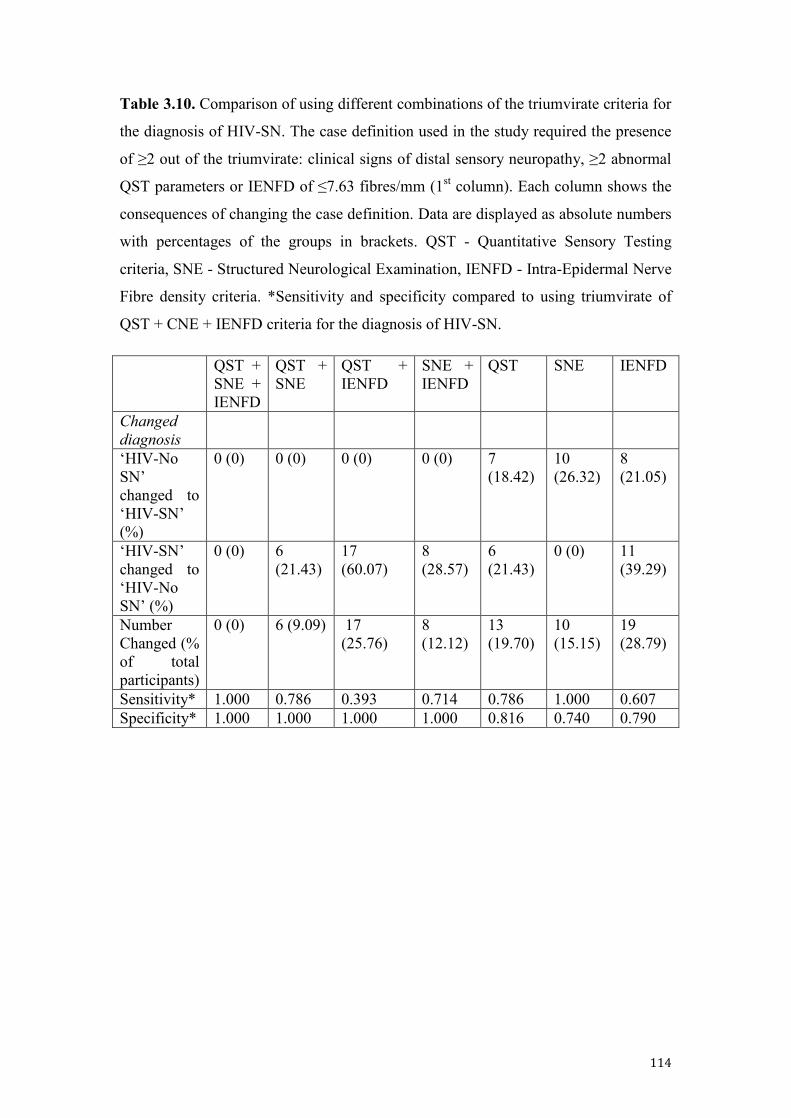
114
Table 3.10. Comparison of using different combinations of the triumvirate criteria for
the diagnosis of HIV-SN. The case definition used in the study required the presence
of ≥2 out of the triumvirate: clinical signs of distal sensory neuropathy, ≥2 abnormal
QST parameters or IENFD of ≤7.63 fibres/mm (1st column). Each column shows the
consequences of changing the case definition. Data are displayed as absolute numbers
with percentages of the groups in brackets. QST - Quantitative Sensory Testing
criteria, SNE - Structured Neurological Examination, IENFD - Intra-Epidermal Nerve
Fibre density criteria. *Sensitivity and specificity compared to using triumvirate of
QST + CNE + IENFD criteria for the diagnosis of HIV-SN.
QST + SNE + IENFD
QST + SNE
QST + IENFD
SNE + IENFD
QST SNE IENFD
Changed diagnosis
‘HIV-No SN’ changed to ‘HIV-SN’ (%)
0 (0) 0 (0) 0 (0) 0 (0) 7 (18.42)
10 (26.32)
8 (21.05)
‘HIV-SN’ changed to ‘HIV-No SN’ (%)
0 (0) 6 (21.43)
17 (60.07)
8 (28.57)
6 (21.43)
0 (0) 11 (39.29)
Number Changed (% of total participants)
0 (0) 6 (9.09) 17 (25.76)
8 (12.12)
13 (19.70)
10 (15.15)
19 (28.79)
Sensitivity* 1.000 0.786 0.393 0.714 0.786 1.000 0.607 Specificity* 1.000 1.000 1.000 1.000 0.816 0.740 0.790

115
Table 3.11. Comparisons of using original PINS study criteria, Brief Peripheral
Neuropathy Screen (BPNS) and the Structured Neurological Examination (SNE)
as HIV-SN criteria for QST z-score results; mean values (SD),‘Loss’ and ‘Gain’ of
function: number of participant z scores ≤ -1.96, and ≥ 1.96 respectfully.
Original PINS criteria
CDT WDT TSL CPT HPT MDT MPT MPS WUR VDT PPT PHS DMA
HIV-No SN n=38
Mean (SD)
-0.68 (0.75)
-0.79 (0.69)
-0.86 (0.54)
0.24 (0.71)
-0.59 (1.01)
-0.77 (0.77)
0.42 (0.88)
0.36 (1.21)
-0.13 (1.12)
-0.84 (1.01)
-1.09 (0.87)
0.62 (0.92)
0
Loss 2 1 1 0 3 2 0 0 1 4 7 0 0
Gain 0 0 0 0 1 0 1 5 2 0 0 0 0
HIV-SN n=28 Mean (SD)
-1.34 (0.93)
-1.31 (0.56)
-1.29 (0.67)
-0.18 (0.37)
-1.47 (1.05)
-2.17 (1.06)
-0.01 (0.99)
-0.32 (1.06)
-0.21 (1.66)
-2.24 (1.62)
-1.29 (1.13)
0.67 (0.87)
0
Loss 8 4 4 0 9 14 1 0 2 14 7 0 0
Gain 0 0 0 0 0 0 0 1 4 0 1 0 0
BPNS as criteria CDT WDT TSL CPT HPT MDT MPT MPS WUR VDT PPT PHS DMA
HIV-No SN n=37
Mean (SD)
-0.84 (0.82)
-0.85 (0.73)
-0.95 (0.62)
0.17 (0.68)
-0.88 (0.94)
-0.94 (1.06)
0.39 (0.90)
-0.26 (1.17)
-0.26 (1.09)
-0.98 (1.35)
-1.11 (0.79)
0.57 (0.84)
0
Loss 4 2 2 0 6 4 0 0 2 3 4 0 0
Gain 0 0 0 0 0 0 1 5 0 0 0 4 0
HIV-SN n=29
Mean (SD)
-0.84 (0.78)
-0.85 (0.89)
-0.9 (1.00)
0.16 (0.98)
-0.87 (1.14)
-0.94 (1.22)
0.39 (0.67)
0.30 (1.03)
0.26 (1.27)
-0.98 (0.69)
-1.12 (0.88)
0.57 (0.95)
0
Loss 4 3 3 0 6 12 1 0 1 15 9 0 0
Gain 0 0 0 0 1 0 0 1 5 0 1 5 0
Structured Neurological Exam (SNE) as criteria CDT WDT TSL CPT HPT MDT MPT MPS WUR VDT PPT PHS DMA
HIV-No SN n=28
Mean (SD)
-0.78 (0.75)
-0.76 (0.43)
-0.90 (0.41)
-0.26 (0.73)
-0.82 (1.19)
-0.94 (1.19)
0.48 (0.72)
0.35 (1.17)
-0.02 (1.50)
-1.46 (1.61)
-1.03 (0.94)
0.54 (0.78)
0
Loss 1 0 0 0 4 2 0 0 2 7 3 0 0
Gain 0 0 0 0 1 0 0 3 2 0 1 2 0
HIV-SN n=38
Mean (SD)
-1.09 (0.75)
-1.19 (0.43)
-1.14 (0.41)
-0.07 (0.73)
-1.08 (1.19)
-1.73 (1.19)
0.04 (1.19)
-0.15 (0.71)
-0.25 (1.17)
-1.44 (1.50)
-1.28 (1.61)
0.77 (0.95)
0
Loss 7 5 5 0 8 14 1 0 1 11 10 0 0
Gain 0 0 0 0 0 0 1 1 1 0 0 6 0
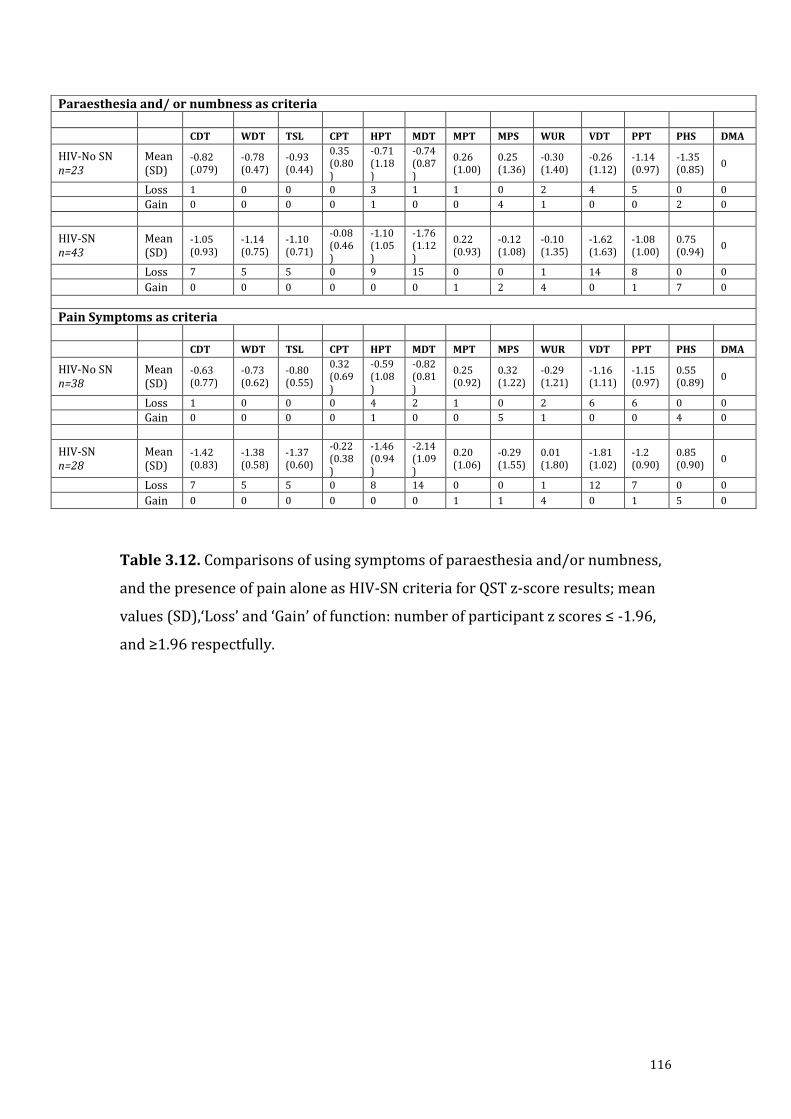
116
Table 3.12. Comparisons of using symptoms of paraesthesia and/or numbness,
and the presence of pain alone as HIV-SN criteria for QST z-score results; mean
values (SD),‘Loss’ and ‘Gain’ of function: number of participant z scores ≤ -1.96,
and ≥1.96 respectfully.
Paraesthesia and/ or numbness as criteria
CDT WDT TSL CPT HPT MDT MPT MPS WUR VDT PPT PHS DMA
HIV-No SN n=23
Mean (SD)
-0.82 (.079)
-0.78 (0.47)
-0.93 (0.44)
0.35 (0.80)
-0.71 (1.18)
-0.74 (0.87)
0.26 (1.00)
0.25 (1.36)
-0.30 (1.40)
-0.26 (1.12)
-1.14 (0.97)
-1.35 (0.85)
0
Loss 1 0 0 0 3 1 1 0 2 4 5 0 0
Gain 0 0 0 0 1 0 0 4 1 0 0 2 0
HIV-SN n=43
Mean (SD)
-1.05 (0.93)
-1.14 (0.75)
-1.10 (0.71)
-0.08 (0.46)
-1.10 (1.05)
-1.76 (1.12)
0.22 (0.93)
-0.12 (1.08)
-0.10 (1.35)
-1.62 (1.63)
-1.08 (1.00)
0.75 (0.94)
0
Loss 7 5 5 0 9 15 0 0 1 14 8 0 0
Gain 0 0 0 0 0 0 1 2 4 0 1 7 0
Pain Symptoms as criteria
CDT WDT TSL CPT HPT MDT MPT MPS WUR VDT PPT PHS DMA
HIV-No SN n=38
Mean (SD)
-0.63 (0.77)
-0.73 (0.62)
-0.80 (0.55)
0.32 (0.69)
-0.59 (1.08)
-0.82 (0.81)
0.25 (0.92)
0.32 (1.22)
-0.29 (1.21)
-1.16 (1.11)
-1.15 (0.97)
0.55 (0.89)
0
Loss 1 0 0 0 4 2 1 0 2 6 6 0 0
Gain 0 0 0 0 1 0 0 5 1 0 0 4 0
HIV-SN n=28
Mean(SD)
-1.42 (0.83)
-1.38 (0.58)
-1.37 (0.60)
-0.22 (0.38)
-1.46 (0.94)
-2.14 (1.09)
0.20 (1.06)
-0.29 (1.55)
0.01 (1.80)
-1.81 (1.02)
-1.2 (0.90)
0.85 (0.90)
0
Loss 7 5 5 0 8 14 0 0 1 12 7 0 0
Gain 0 0 0 0 0 0 1 1 4 0 1 5 0
117
Chapter 4
Summary
118
Summary
Chapter 2: Findings and implications of the systematic review of pharmacological
agents in the treatment of painful HIV-SN Chapter 2.
The systematic review and meta-analysis presented in Chapter 2 demonstrates that the
pharmacological management of the painful symptoms of HIV-SN is at present
unsatisfactory. There is currently no evidence of efficacy for many agents commonly
used to treat other neuropathic pain states in the treatment of painful HIV-SN:
amitriptyline, topical capsaicin (0.075%), gabapentin or lamotrigine all failed to show
efficacy greater than placebo in the doses tested in the included RCTs.
The conclusion of the systematic review is that only recombinant human NGF (a
commercially unavailable agent) and smoked cannabis are better than placebo in the
management of pain in HIV-SN. An NNT for smoked cannabis was calculated as 3.38
with a 95% CI (2.19 – 7.50). This apparent efficacy should be tempered by the high
proportion of inadvertent unblinding that occurred in at least one trial (92% of
participants correctly guessing treatment allocation) (Ellis et al., 2009), and the
potential for this to have occurred in the other included cannabis RCT, where
previous recreational exposure to cannabis was an inclusion criteria for participants.
Limitations of this study and future work
The systematic review used the modified Jadad scale to assess the quality of RCTs
entered into it. The Jadad scale has been previously criticised as being over-simplistic,
showing low consistency between different raters (Hartling et al., 2009) and it places
too much emphasis on blinding (V. W. Berger, 2006). Furthermore, it does not take
into account allocation concealment.
Quality scales and resulting scores are not an appropriate way to appraise clinical
trials. They tend to combine assessments of aspects of the quality of reporting with
aspects of trial conduct, and to assign weights to different items in ways that are often
difficult to justify (J. P. T. Higgins et al., 2011). If I was repeat the systematic review
I would use the Cochrane Collaborations Risk of Bias Tool (CCRNT) for the above
reasons (J. Higgins & Altman, 2008). Whilst no assessment tool is infallible, the
119
CCRNT has taken into consideration advances in the understanding risk of bias in
RCT and appears to be currently the most complete instrument available.
The systematic review in Chapter 2 also underlines the need for disease specific
analgesic efficacy RCTs, as guidelines drawn up to treat neuropathic pain per se,
based on RCTs for other conditions, do not reflect the response of HIV-SN to
conventional analgesics or neuropathic pain adjuvants.
Cannabinoids have been extensively investigated and whilst useful in certain
neuropathic pain states, their use is limited by the significant psychotropic effects of
cannabinoid compounds (A. S. C. Rice, 2008). A notable exception is multiple
sclerosis (MS) where cannabinoids have been shown to be useful in the treatment of
MS associated spasticity and pain in at least a subset of patients (P. F. Smith, 2007).
The apparent efficacy of smoked cannabis in the treatment of pain in HIV-SN would
suggest that the use of cannabis extracts and synthetic compounds would be worthy of
further investigation.
Unfortunately it is unlikely if there will be further work using recombinant NGF in
the treatment of painful HIV-SN. Recombinant NGF is commercially unavailable
after it proved disappointing in the treatment of painful diabetic neuropathy at Phase
III trials and was so abandoned by the pharmaceutical company investigating it
(Apfel, 2002).
Whilst high dose 8% capsaicin patches initially showed promise in the treatment of
pain associated with HIV-SN, a subsequently published larger RCT showed no
superiority of high dose capsaicin patches to placebo (D. B. Clifford et al., 2012).
If painful HIV-SN was an occasional complication of a rare condition, painful HIV-
SN might remain an academic oddity. However as argued in Chapter 1, HIV-SN
represents probably the largest cause of pain morbidity worldwide, potentially
affecting more than a third of the 34 million persons infected with HIV. The
conclusions of the systematic review underline the urgent need to seek out novel
agents to treat this pain.
The systematic review was hampered by the paucity of good quality RCTs
particularly for older neuropathic pain adjuvant drugs which are off-patent. Modern
high quality RCTs suitable to assess the efficacy of pharmacological agents, are
120
complex and expensive to conduct. Unfortunately, the majority of these high quality
RCTs are currently conducted by pharmaceutical companies who have the financial
and logistical resources to undertake them. Consequently, this biases newer, on-patent
agents where there is a financial incentive to find efficacy. It has been suggested that
it should be the role of governmental research agencies, such as the National Institute
of Health Research (NIHR) in both the US and UK to fund modern RCTs examining
older agents against placebo, each other (head-to-head) and in combination therapies
in a clinically meaningful way.
New evidence related to the use of high dose capsaicin patches has been published
whilst this thesis was in preparation (D. B. Clifford et al., 2012). As suggested in an
abstract assessed in the systematic review, the outcome of these trials demonstrates
that high dose capsaicin patch is not superior to placebo in the treatment of painful
HIV-SN. A new systematic review should be conducted and this high dose capsaicin
study included formally assessed and integrated into the systematic review.
Chapter 3: Patterns of sensory, psychological and metabolic dysfunction in HIV
positive patients with and without HIV-associated peripheral neuropathy.
Findings, implications and future work
One of the key findings of the phenotyping study is that the sensory dysfunction seen
in HIV-SN is heterogeneous. Comparing the HIV-SN population to the HIV-No SN
group the most profound difference is that of sensory loss across all modalities
measured. Most frequently, this was seen in the large fibre modalities of MDT and
VDT. Whilst differences were seen in small fibre function the picture across the
group was quite mixed, with no discernable patterns evident. This highlights the fact
that HIV-SN is not a pure small fibre neuropathy (as it has been widely considered)
and potentially opens a new line of research in the mechanisms underlying HIV-SN.
Moreover, this finding would support the use of MDT and VDT in low resource
settings in preference to expensive thermal parameter QST equipment. In addition, the
absence of gain of function phenomena is consistent with QST studies of other painful
peripheral neuropathies. Nevertheless, a small sub-group with wind-up phenomenon
was seen in 14% of the HIV-SN group patients (n=4) – whilst this is a small number,
it is a comparable proportion of HIV-SN participants seen to have mechanical
hyperalgesia in previous studies. However, as this thesis used the standardised DFNS
121
protocol, it is difficult to draw direct conclusions with this specific study (D M
Simpson, Schifitto, et al., 2010). A future phenotyping study should actively look for
this phenomenon, especially as the sub-group seen in the pregabalin RCT work of
Simpson and collaborators in 2010 had a differential response to analgesics. The
presence of high levels of catastrophising in this high WUR is another interesting
phenomenon as would be useful to explore further.
This thesis showed that patients with HIV-SN had significantly higher triglyceride
levels than patients without HIV-SN. This is a finding that further supports recent
work in both HIV-SN and Diabetic neuropathy which suggests lipid dysfunction is an
important factor in the development of painful peripheral neuropathies(Banerjee et al.,
2011; Vincent et al., 2009; Wiggin et al., 2009). This opens an interesting question
about the role of lipid lowering agents such as statins to act as disease modifying
agents to prevent or slow the development of HIV-SN.
Strengths of this study
This comprehensive phenotyping of HIV-SN is important for the future development
of animal models.
Although the phenotyping study presented in Chapter 3 produced a wealth of
information, it will take a lot more time to fully explore its implications. Further
analysis of the diagnostic utility of individual components tested in this study should
be undertaken to yield a composite refined diagnostic protocol using the best of the
sensory testing, screening tools and specific symptom questioning to produce a robust
tool for screening and early detection of HIV-SN. This had been part of the original
aims of the thesis but could not be completed due to time restrictions. Colleagues who
intend to build on the work of this thesis have already started this work.
As part of this thesis a blood and tissue bank has been established. This is an
important resource as these tissue samples have extensive phenotyping information
associated with them. The hope is that this will be potentially useful in future genetic
analysis studies examining painful HIV-SN.
Limitations of this study
122
One of the weaknesses of the phenotyping study was that the relatively small number
of HIV infected participants recruited (n=66) into the study meant that a useful
comparison between participants with non-painful (n=7) and painful HIV-SN (n=21)
was not possible to do with meaning full statistical significance. Another potential
consequence of small recruitment numbers was that many of the established risk
factors for the development of HIV-SN were not confirmed in this study – most
notably age and height. As argued in Chapter 3 some of this failure to see established
risk factors can be accounted for in the population. Compared to many larger
epidemiological studies, the population we recruited was quite homogeneous: male,
white, tall and middle aged. Unfortunately, the labour intensive nature of phenotyping
individuals over three to four hours each, meant that recruiting greater numbers was
not practical. A future phenotyping study could utilise the work here and use a smaller
number of components to reduce both participant and investigator work loads to allow
a greater number of individuals to be recruited.
The use of a composite definition for HIV-SN, using abnormal QST (2 or more
abnormal modalities), reduced IENFD (<7.63 fibres/mm) and a structured clinical
examination meant that comparing these measures between the two groups might risk
a circular argument. Reasons for this to be unlikely are outlined in the discussion of
Chapter 3, however if a more robust definition for HIV-SN can be produced as
described as above, future phenotyping studies might be free from this potential
criticism.
There is also a need for ease to use, robust screening tools for the identification of
HIV-SN that can be translated for use into resource poor settings. Part of the
phenotyping study examined the efficacy of a number of neuropathy screening tools
(and their constituent components), some of which have not been previously validated
in the context of HIV-SN. This study will hopefully form the basis for future work
directed at producing a composite screening tool for use in resource poor settings.
As part of this study a blood and tissue bank for each highly phenotyped individual
with HIV-SN was established; this valuable resource will inform future work
exploring genetic risk factors for the development of HIV-SN and painful HIV-SN.
123
REFERENCES
Abrams, D. I., Jay, C. A., Shade, S. B., Vizoso, H., Reda, H., Press, S., … Petersen, K. L. (2007). Cannabis in painful HIV-associated sensory neuropathy: a randomized placebo-controlled trial. Neurology, 68(7), 515–21. doi:10.1212/01.wnl.0000253187.66183.9c
Affandi, J. S., Price, P., Imran, D., Yunihastuti, E., Djauzi, S., & Cherry, C. L. (2008). Can we predict neuropathy risk before stavudine prescription in a resource-limited setting? AIDS research and human retroviruses, 24(10), 1281–4. doi:10.1089/aid.2008.0045
Ances, B. M., Vaida, F., Rosario, D., Marquie-Beck, J., Ellis, R. J., Simpson, D. M., … McCutchan, J. A. (2009). Role of metabolic syndrome components in HIV-associated sensory neuropathy. AIDS (London, England), 23(17), 2317–22. doi:10.1097/QAD.0b013e328332204e
Apfel, S. C. (2002). Nerve growth factor for the treatment of diabetic neuropathy: what went wrong, what went right, and what does the future hold? International review of neurobiology, 50, 393–413.
Bacellar, H., Muñoz, A., Miller, E., Cohen, B., Besley, D., Selnes, O., … McArthur, J. (1994). Temporal trends in the incidence of HIV-1-related neurologic diseases: Multicenter AIDS Cohort Study, 1985-1992. Neurology, 44(10), 1892–900.
Bakkers, M., Merkies, I. S. J., Lauria, G., Devigili, G., Penza, P., Lombardi, R., … Faber, C. G. (2009). Intraepidermal nerve fiber density and its application in sarcoidosis. Neurology, 73(14), 1142–8. doi:10.1212/WNL.0b013e3181bacf05
Banerjee, S., McCutchan, J. A., Ances, B. M., Deutsch, R., Riggs, P. K., Way, L., & Ellis, R. J. (2011). Hypertriglyceridemia in combination antiretroviral-treated HIV-positive individuals: potential impact on HIV sensory polyneuropathy. AIDS (London, England), 25(2), F1–6. doi:10.1097/QAD.0b013e328341dd68
Barohn, R., Gronseth, G., LeForce, B., McVey, A., McGuire, S., Butzin, C., & King, R. (1993). Peripheral nerve involvement in a large cohort of human immunodeficiency virus-infected individuals. Archives of neurology, 50, 167–171.
Barohn, R. J., Gronseth, G. S., Amato, a a, McGuire, S. a, McVey, a L., LeForce, B. R., & King, R. B. (1996). Cerebrospinal fluid and nerve conduction abnormalities in HIV positive individuals. Journal of the neurological sciences, 136(1-2), 81–5.
Baron, R., Tölle, T. R., Gockel, U., Brosz, M., & Freynhagen, R. (2009). A cross-sectional cohort survey in 2100 patients with painful diabetic neuropathy and postherpetic neuralgia: Differences in demographic data and sensory symptoms. Pain, 146(1-2), 34–40. doi:10.1016/j.pain.2009.06.001
124
Bastien, C. H., Vallières, a, & Morin, C. M. (2001). Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep medicine, 2(4), 297–307.
Beaulieu, P., & Ware, M. (2007). Reassessment of the role of cannabinoids in the management of pain. Current opinion in anaesthesiology, 20(5), 473–7. doi:10.1097/ACO.0b013e3282efd175
Berger, A., Arezzo, J., Schaumburg, H., Skowron, G., Merigan, T., Bozzette, S., … Soo, W. (1993). 2’,3'-dideoxycytidine (ddC) toxic neuropathy: a study of 52 patients. Neurology, 43(2), 358–62.
Berger, V. W. (2006). Is the Jadad score the proper evaluation of trials? The Journal of rheumatology, 33(8), 1710–1; author reply 1711–2.
Bhangoo, S., Ripsch, M., Buchanan, D., Miller, R., & White, F. (2009). Increased chemokine signaling in a model of HIV1-associated peripheral neuropathy. Mol Pain, 5:, 48.
Blum, A., Dal Pan, G., Feinberg, J., Raines, C., Mayjo, K., Cornblath, D., & McArthur, J. (1996). Low-dose zalcitabine-related toxic neuropathy: frequency, natural history, and risk factors. Neurology, 46(4), 999–1003.
Boger, M. S., Hulgan, T., Haas, D. W., Mitchell, V., Smith, a G., Singleton, J. R., & Peltier, a C. (2012). Measures of small-fiber neuropathy in HIV infection. Autonomic neuroscience : basic & clinical, 169(1), 56–61. doi:10.1016/j.autneu.2012.04.001
Bouhassira, D., Attal, N., Willer, J. C., & Brasseur, L. (1999). Painful and painless peripheral sensory neuropathies due to HIV infection: a comparison using quantitative sensory evaluation. Pain, 80(1-2), 265–72.
Bradley, W. G., & Verma, A. (1996). Painful vasculitic neuropathy in HIV-1 infection: relief of pain with prednisone therapy. Neurology, 47(6), 1446–51.
Brew, B. J. (2003). The peripheral nerve complications of human immunodeficiency virus (HIV) infection. Muscle & nerve, 28(5), 542–52. doi:10.1002/mus.10484
Bril, V., & Perkins, B. a. (2002). Validation of the Toronto Clinical Scoring System for diabetic polyneuropathy. Diabetes care, 25(11), 2048–52.
Brown, S., Mitler, M., & Atkinson, H. (1991). Correlation of subjective sleep com- plaints, absolute T-4 cell number and anxiety in HIV illness. Sleep Res, 20, 363.
Chavanet, P., Solary, E., Giroud, M., Waldner, A., Beuriat, P., Nordman, P., & Portier, H. (1989). Infraclinical neuropathies related to immunodeficiency virus infection associated with higher T-helper cell count. Journal of acquired immune deficiency syndromes, 2(6), 564–9.
125
Chavanet, P. Y., Giroud, M., Lancon, J. P., Borsotti, J. P., Waldner-Combernoux, A. C., Pillon, D., … Portier, H. (1988). Altered peripheral nerve conduction in HIV-patients. Cancer detection and prevention, 12(1-6), 249–55.
Chen, X., & Levine, J. D. (2007). Mechanically-evoked C-fiber activity in painful alcohol and AIDS therapy neuropathy in the rat. Molecular pain, 3, 5. doi:10.1186/1744-8069-3-5
Cheng, Y., Gregg, E., Kahn, H., Williams, D., De Rekeneire, N., & Narayan, K. (2006). Peripheral insensate neuropathy--a tall problem for US adults? Am J Epidemiol, 164(9), 873–80.
Cherry, C L, Affandi, J. S., Imran, D., Yunihastuti, E., Smyth, K., Vanar, S., … Price, P. (2009). Age and height predict neuropathy risk in patients with HIV prescribed stavudine. Neurology, 73(4), 315–20. doi:10.1212/WNL.0b013e3181af7a22
Cherry, C L, Skolasky, R. L., Lal, L., Creighton, J., Hauer, P., Raman, S. P., … McArthur, J. C. (2006). Antiretroviral use and other risks for HIV-associated neuropathies in an international cohort. Neurology, 66(6), 867–73. doi:10.1212/01.wnl.0000203336.12114.09
Cherry, Catherine L, Rosenow, A., Affandi, J. S., McArthur, J. C., Wesselingh, S. L., & Price, P. (2008). Cytokine genotype suggests a role for inflammation in nucleoside analog-associated sensory neuropathy (NRTI-SN) and predicts an individual’s NRTI-SN risk. AIDS research and human retroviruses, 24(2), 117–23. doi:10.1089/aid.2007.0168
Cherry, Catherine L, Wesselingh, S. L., Lal, L., & McArthur, J. C. (2005). Evaluation of a clinical screening tool for HIV-associated sensory neuropathies. Neurology, 65(11), 1778–81. doi:10.1212/01.wnl.0000187119.33075.41
Cherry, Catherine Louise, Wadley, A. L., & Kamerman, P. R. (2012). Painful HIV-associated sensory neuropathy: still a problem in the post-stavudine era? Future Virology, 2(6), 543–552.
Chiechio, S., Copani, A., Gereau, R. W., & Nicoletti, F. (2007). Acetyl-L-carnitine in neuropathic pain: experimental data. CNS drugs, 21 Suppl 1, 31–8; discussion 45–6.
Childs, E. a, Lyles, R. H., Selnes, O. a, Chen, B., Miller, E. N., Cohen, B. a, … McArthur, J. C. (1999). Plasma viral load and CD4 lymphocytes predict HIV-associated dementia and sensory neuropathy. Neurology, 52(3), 607–13.
Cleeland, C. S., & Ryan, K. M. (1994). Pain assessment global use of the Brief Pain Inventory. Annals of the Academy of Medicine, Singapore, 23(2), 129 –38.
Clifford, D. B., Simpson, D. M., Brown, S., Moyle, G., Brew, B. J., Conway, B., … Vanhove, G. F. (2012). A randomized, double-blind, controlled study of NGX-4010, a capsaicin 8% dermal patch, for the treatment of painful HIV-associated
126
distal sensory polyneuropathy. Journal of acquired immune deficiency syndromes (1999), 59(2), 126–33. doi:10.1097/QAI.0b013e31823e31f7
Clifford, D., Simpson, D., Brown, S., Moyle, G., & Brew, B. (2010). A multicenter, randomized, double-blind, controlled study of NGX-4010 (Qutenza), a high concentration capsaicin patch for the treatment of HIV-Associated distal sensory neuropathy. 17th Conference on Retroviruses and Opportunistic Infections, Abstract 4.
Collaboration., A. T. C. (2008). Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Lancet, 372(9635), 293–9.
Cornblath, D., & McArthur, J. (1988). Predominantly sensory neuropathy in patients with AIDS and AIDS-related complex. Neurology, 38(5), 543–55.
Cornblath, D. R., Chaudhry, V., Carter, K., Lee, D., Seysedadr, M., Miernicki, M., & Joh, T. (1999). Total neuropathy score: validation and reliability study. Neurology, 53(8), 1660–4.
Cox, S., & Rice, A. S. C. (2008). HIV and AIDS. In P. Wilson, P. Watson, J. Haythornthwaite, & T. Jensen (Eds.), Text Book of Clinical Pain Management (2nd ed., pp. 352 –61). Taylor and Francis.
Cruccu, G., Sommer, C., Anand, P., Attal, N., Baron, R., Garcia-Larrea, L., … Treede, R.-D. (2010). EFNS guidelines on neuropathic pain assessment: revised 2009. European journal of neurology : the official journal of the European Federation of Neurological Societies, 17(8), 1010–8. doi:10.1111/j.1468-1331.2010.02969.x
Cruess, D., Antoni, M., Gonzalez, J., Fletcher, M., Klimas, N., Duran, R., … Schneiderman, N. (2003). Sleep disturbance mediates the association between psychological distress and immune status among HIV-positive men and women on combination antiretroviral therapy. J Psychosom Res, 54, 185–9.
Daniel, H. C., Narewska, J., Serpell, M., Hoggart, B., Johnson, R., & Rice, A. S. C. (2008). Comparison of psychological and physical function in neuropathic pain and nociceptive pain: implications for cognitive behavioral pain management programs. European journal of pain (London, England), 12(6), 731–41. doi:10.1016/j.ejpain.2007.11.006
Devigili, G., Tugnoli, V., Penza, P., Camozzi, F., Lombardi, R., Melli, G., … Lauria, G. (2008). The diagnostic criteria for small fibre neuropathy: from symptoms to neuropathology. Brain : a journal of neurology, 131(Pt 7), 1912–25. doi:10.1093/brain/awn093
Dorfman, D., Dalton, A., Khan, A., Markarian, Y., Scarano, A., Cansino, M., … Simpson, D. (1999). Treatment of painful distal sensory polyneuropathy in HIV-infected patients with a topical agent: results of an open-label trial of 5% lidocaine gel. AIDS (London, England), 13(12), 1589–90.
127
Drewes, J., Gusy, B., & Rüden, U. (2013). More Than 20 Years of Research into the Quality of Life of People with HIV and AIDS--A Descriptive Review of Study Characteristics and Methodological Approaches of Published Empirical Studies. J Int Assoc Provid AIDS Care, 12(1), 18–22.
Dworkin, R. H., Katz, J., & Gitlin, M. J. (2005). Placebo response in clinical trials of depression and its implications for research on chronic neuropathic pain. Neurology, 65(12 Suppl 4), S7–19.
Ellis, R. J., Rosario, D., Clifford, D. B., McArthur, J. C., Simpson, D., Alexander, T., … Grant, I. (2010). Continued high prevalence and adverse clinical impact of human immunodeficiency virus-associated sensory neuropathy in the era of combination antiretroviral therapy: the CHARTER Study. Archives of neurology, 67(5), 552–8. doi:10.1001/archneurol.2010.76
Ellis, R. J., Toperoff, W., Vaida, F., van den Brande, G., Gonzales, J., Gouaux, B., … Atkinson, J. H. (2009). Smoked medicinal cannabis for neuropathic pain in HIV: a randomized, crossover clinical trial. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology, 34(3), 672–80. doi:10.1038/npp.2008.120
Estanislao, L., Carter, K., McArthur, J., Olney, R., & Simpson, D. (2004). A randomized controlled trial of 5% lidocaine gel for HIV-associated distal symmetric polyneuropathy. Journal of acquired immune deficiency syndromes (1999), 37(5), 1584–6.
Evans, S. R., Clifford, D. B., Kitch, D. W., Goodkin, K., Schifitto, G., Mcarthur, J. C., & Simpson, D. M. (2008). Simplification of the Research Diagnosis of HIV-Associated Sensory Neuropathy. HIV Clinical Trials, 9(6), 434–439.
Evans, S. R., Simpson, D. M., Kitch, D. W., King, A., Clifford, D. B., Cohen, B. a, & McArthur, J. C. (2007). A randomized trial evaluating Prosaptide for HIV-associated sensory neuropathies: use of an electronic diary to record neuropathic pain. PloS one, 2(6), e551. doi:10.1371/journal.pone.0000551
Finnerup, N., Sindrup, S., & Jensen, T. (2010). The evidence for pharmacological treatment of neuropathic pain. Pain, (150), 573–581.
Fuller, G. N., Jacobs, J. M., & Guiloff, R. J. (1991). Subclinical peripheral nerve involvement in AIDS: an electrophysiological and pathological study. Journal of neurology, neurosurgery, and psychiatry, 54(4), 318–24.
Gatti, Antonella, Jann, Stefano, & Sandro. (1998). Treatment of Distal Symmetric Axonopathy in HIV Infected Patients. (Abstract) Neurology, 50:, A216.
Gdynia, H.-J., Müller, T., Sperfeld, A.-D., Kühnlein, P., Otto, M., Kassubek, J., & Ludolph, A. C. (2008). Severe sensorimotor neuropathy after intake of highest dosages of vitamin B6. Neuromuscular disorders : NMD, 18(2), 156–8. doi:10.1016/j.nmd.2007.09.009
128
Gierthmühlen, J., Maier, C., Baron, R., Tölle, T., Treede, R.-D., Birbaumer, N., … Westermann, A. (2012). Sensory signs in complex regional pain syndrome and peripheral nerve injury. Pain, 153(4), 765–74. doi:10.1016/j.pain.2011.11.009
Griffin, J. W., McArthur, J. C., & Polydefkis, M. (2001). Assessment of cutaneous innervation by skin biopsies. Current opinion in neurology, 14(5), 655–9.
Haanpää, M. L., Backonja, M.-M., Bennett, M. I., Bouhassira, D., Cruccu, G., Hansson, P. T., … Baron, R. (2009). Assessment of neuropathic pain in primary care. The American journal of medicine, 122(10 Suppl), S13–21. doi:10.1016/j.amjmed.2009.04.006
Hahn, K., Arendt, G., Braun, J. S., von Giesen, H.-J., Husstedt, I. W., Maschke, M., … Schielke, E. (2004). A placebo-controlled trial of gabapentin for painful HIV-associated sensory neuropathies. Journal of neurology, 251(10), 1260–6. doi:10.1007/s00415-004-0529-6
Hart, A. M., Wilson, A. D. H., Montovani, C., Smith, C., Johnson, M., Terenghi, G., & Youle, M. (2004). Acetyl-l-carnitine: a pathogenesis based treatment for HIV-associated antiretroviral toxic neuropathy. AIDS (London, England), 18(11), 1549–60.
Hartling, L., Ospina, M., Liang, Y., Dryden, D. M., Hooton, N., Krebs Seida, J., & Klassen, T. P. (2009). Risk of bias versus quality assessment of randomised controlled trials: cross sectional study. BMJ (Clinical research ed.), 339, b4012.
Haynes, R. B. (2005). Conducting systematic reviews. In R. B. Haynes, D. L. Sackett, P. Guyatt, & G. H. Tugwell (Eds.), Clinical Epidemiology (3rd ed., p. p. 31). Lippincott Williams & Wilkins.
Hedges, B. (1996). Health Survey for England 1994. London, HMOS. Retrieved October 22, 2008, from http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_4002768/
Hempenstall, K., Nurmikko, T. J., Johnson, R. W., A’Hern, R. P., & Rice, A. S. C. (2005). Analgesic therapy in postherpetic neuralgia: a quantitative systematic review. PLoS medicine, 2(7), e164. doi:10.1371/journal.pmed.0020164
Herrmann, D N, Griffin, J. W., Hauer, P., Cornblath, D. R., & McArthur, J. C. (1999). Epidermal nerve fiber density and sural nerve morphometry in peripheral neuropathies. Neurology, 53(8), 1634–40.
Herrmann, David N, McDermott, M. P., Henderson, D., Chen, L., Akowuah, K., & Schifitto, G. (2004). Epidermal nerve fiber density, axonal swellings and QST as predictors of HIV distal sensory neuropathy. Muscle & nerve, 29(3), 420–7. doi:10.1002/mus.10567
129
Herzmann, C., Johnson, M. A., & Youle, M. (2005). Long-term effect of acetyl-L-carnitine for antiretroviral toxic neuropathy. HIV clinical trials, 6(6), 344–50. doi:10.1310/CH1N-YBNU-G3CU-JBXR
Higgins, J., & Altman, D. (2008). Assessing risk of bias in included studies. In J. Higgins & S. Green (Eds.), Cochrane handbook for systematic reviews of interventions. (pp. p.187–241). Wiley.
Higgins, J. P. T., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., … Sterne, J. A. C. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ (Clinical research ed.), 343, d5928.
Holland, N. R., Stocks, A., Hauer, P., Cornblath, D. R., Griffin, J. W., & McArthur, J. C. (1997). Intraepidermal nerve fiber density in patients with painful sensory neuropathy. Neurology, 48(3), 708–11.
Huang, W, Pheby, T., & Rice, A. (2013). A clinically relevant rodent model of HIV antiretroviral drug (indinavir) induced peripheral sensory neuropathy. Program of the 4th International Congress on Neuropathic Pain, (Program No. A-484-0002-00458.).
Huang, Wenlong, Calvo, M., Karu, K., Olausen, H. R., Bathgate, G., Okuse, K., … Rice, A. S. C. (2013). A clinically relevant rodent model of the HIV antiretroviral drug stavudine induced painful peripheral neuropathy. Pain, 154(4), 560–75. doi:10.1016/j.pain.2012.12.023
Huengsberg, M., Winer, J. B., Ross, J. D., & Shahmanesh, M. (1998). Thermosensory threshold: a sensitive test of HIV associated peripheral neuropathy? Journal of neurovirology, 4(4), 433–7.
Hulgan, T., Haas, D. W., Haines, J. L., Ritchie, M. D., Robbins, G. K., Shafer, R. W., … Canter, J. a. (2005). Mitochondrial haplogroups and peripheral neuropathy during antiretroviral therapy: an adult AIDS clinical trials group study. AIDS (London, England), 19(13), 1341–9.
Husstedt, I. W., Evers, S., Reichelt, D., Grotemeyer, K. H., Kammer-Suhr, B., Böckenholt, S., & Heese, C. (2000). Screening for HIV-associated distal-symmetric polyneuropathy in CDC-classification stages 1, 2, and 3. Acta neurologica Scandinavica, 101(3), 183–7.
Jadad, a R., Moore, R. a, Carroll, D., Jenkinson, C., Reynolds, D. J., Gavaghan, D. J., & McQuay, H. J. (1996). Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled clinical trials, 17(1), 1–12.
Jakobsen, J., Smith, T., Gaub, J., Helweg-Larsen, S., & Trojaborg, W. (1989). Progressive neurological dysfunction during latent HIV infection. BMJ (Clinical research ed.), 299(6693), 225–8.
130
Joint United Nations Programme on HIV/AIDS. (2013). Global Report 2012: Unaids Report on the Global AIDS Epidemic (2012th ed.). Joint United Nations Programme on HIV/AIDS.
Joseph, E. K., Chen, X., Khasar, S. G., & Levine, J. D. (2004). Novel mechanism of enhanced nociception in a model of AIDS therapy-induced painful peripheral neuropathy in the rat. Pain, 107(1-2), 147–58.
Joseph, E. K., & Levine, J. D. (2004). Caspase signalling in neuropathic and inflammatory pain in the rat. The European journal of neuroscience, 20(11), 2896–902. doi:10.1111/j.1460-9568.2004.03750.x
Joseph, E. K., & Levine, J. D. (2006). Mitochondrial electron transport in models of neuropathic and inflammatory pain. Pain, 121(1-2), 105–14. doi:10.1016/j.pain.2005.12.010
Kallianpur, A., Hulgan, T., Tebas, P., Canter, J., Mulligan, K., Haas, D., … Study, A. C. T. G. 384 and A. (2006). Hemochromatosis gene polymorphisms, mitochondrial haplogroups, and peripheral lipoatrophy during antiretroviral therapy. AIDS, 197(6), 858–66.
Kamerman, P. R., Moss, P. J., Weber, J., Wallace, V. C. J., Rice, A. S. C., & Huang, W. (2012). Pathogenesis of HIV-associated sensory neuropathy: evidence from in vivo and in vitro experimental models. Journal of the peripheral nervous system : JPNS, 17(1), 19–31. doi:10.1111/j.1529-8027.2012.00373.x
Kamerman, P. R., Wadley, A. L., & Cherry, C. L. (2012). HIV-associated sensory neuropathy: risk factors and genetics. Current pain and headache reports, 16(3), 226–36. doi:10.1007/s11916-012-0257-z
Kaptchuk, T. J. (1999). Acupuncture and amitriptyline for HIV-related peripheral neuropathic pain. JAMA : the journal of the American Medical Association, 281(14), 1270; author reply 1271–2.
Kaul, M., Garden, G. A., & Lipton, S. A. (2001). Pathways to neuronal injury and apoptosis in HIV-associated dementia. Nature, 410(6831), 988–94. doi:10.1038/35073667
Kaul, M., & Lipton, S. A. (1999). Chemokines and activated macrophages in HIV gp120-induced neuronal apoptosis. Proceedings of the National Academy of Sciences of the United States of America, 96(14), 8212–6.
Kemper, C. A., Kent, G., Burton, S., & Deresinski, S. C. (1998). Mexiletine for HIV-infected patients with painful peripheral neuropathy: a double-blind, placebo-controlled, crossover treatment trial. Journal of acquired immune deficiency syndromes and human retrovirology : official publication of the International Retrovirology Association, 19(4), 367–72.
Keswani, S. C., Pardo, C. A., Cherry, C. L., Hoke, A., & Mcarthur, J. C. (2002). HIV-associated sensory neuropathies. Aids, (April), 2105–2117.
131
Keswani, S. C., Polley, M., Pardo, C. a, Griffin, J. W., McArthur, J. C., & Hoke, A. (2003). Schwann cell chemokine receptors mediate HIV-1 gp120 toxicity to sensory neurons. Annals of neurology, 54(3), 287–96. doi:10.1002/ana.10645
Kieburtz, K., Simpson, D., Yiannoutsos, C., Max, M. B., Hall, C. D., Ellis, R. J., … Cohen, B. (1998). A randomized trial of amitriptyline and mexiletine for painful neuropathy in HIV infection. AIDS Clinical Trial Group 242 Protocol Team. Neurology, 51(6), 1682–8.
King, S. A. (1999). Acupuncture and amitriptyline for HIV-related peripheral neuropathic pain. JAMA : the journal of the American Medical Association, 281(14), 1271–2.
Kirsh, R., Hart, T., Ellens, H., Miller, J., Petteway, S. J., Lambert, D., … Bugelski, P. (1990). Morphometric analysis of recombinant soluble CD4-mediated release of the envelope glycoprotein gp120 from HIV-1. AIDS Res Hum Retroviruses, 6(10), 1209–12.
Konchalard, K. Wangphonpattanasiri, K. (2007). Clinical and electrophysiologic evaluation of peripheral neuropathy in a group of HIV-infected patients in Thailand. J Med Assoc Thai, 90, 774–781.
Konopka, K.-H., Harbers, M., Houghton, A., Kortekaas, R., van Vliet, A., Timmerman, W., … van Wijhe, M. (2012). Bilateral sensory abnormalities in patients with unilateral neuropathic pain; a quantitative sensory testing (QST) study. PloS one, 7(5), e37524. doi:10.1371/journal.pone.0037524
La Spina, I., Porazzi, D., Maggiolo, F., Bottura, P., & Suter, F. (2001). Gabapentin in painful HIV-related neuropathy: a report of 19 patients, preliminary observations. European journal of neurology : the official journal of the European Federation of Neurological Societies, 8(1), 71–5.
Langley, P., Van Litsenburg, C., Cappelleri, J., & Carroll, D. (2013). The burden associated with neuropathic pain in Western Europe. J Med Econ., 16(1), 85–95.
Lauria, G., Cornblath, D. R., Johansson, O., McArthur, J. C., Mellgren, S. I., Nolano, M., … Sommer, C. (2005). EFNS guidelines on the use of skin biopsy in the diagnosis of peripheral neuropathy. European journal of neurology : the official journal of the European Federation of Neurological Societies, 12(10), 747–58. doi:10.1111/j.1468-1331.2005.01260.x
Lauria, G., Hsieh, S. T., Johansson, O., Kennedy, W. R., Leger, J. M., Mellgren, S. I., … Valls-Solé, J. (2010). European Federation of Neurological Societies/Peripheral Nerve Society Guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Ner. European journal of neurology : the official journal of the European Federation of Neurological Societies, 17(7), 903–12, e44–9. doi:10.1111/j.1468-1331.2010.03023.x
132
Lee, K., Portillo, C., & Miramontes, H. (2001). The influence of sleep and activity patterns on fatigue in women with HIV/AIDS. J Assoc Nurses AIDS Care, 12(suppl), 19–27.
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. a, … Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS medicine, 6(7), e1000100. doi:10.1371/journal.pmed.1000100
Lichtenstein, K. a, Armon, C., Baron, A., Moorman, A. C., Wood, K. C., & Holmberg, S. D. (2005). Modification of the incidence of drug-associated symmetrical peripheral neuropathy by host and disease factors in the HIV outpatient study cohort. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 40(1), 148–57. doi:10.1086/426076
Liu, J. P., Manheimer, E., & Yang, M. (2005). Herbal medicines for treating HIV infection and AIDS. Cochrane database of systematic reviews (Online), (3), CD003937. doi:10.1002/14651858.CD003937.pub2
Lohse, N., Hansen, A., Pedersen, G., Kronborg, G., Gerstoft, J., Sørensen, H., … Obel, N. (2007). Survival of persons with and without HIV infection in Denmark, 1995-2005. Annals of internal medicine, 146(2), 87–95.
Magerl, W., Krumova, E. K., Baron, R., Tölle, T., Treede, R.-D., & Maier, C. (2010). Reference data for quantitative sensory testing (QST): Refined stratification for age and a novel method for statistical comparison of group data. Pain, 151(3), 598–605. doi:10.1016/j.pain.2010.07.026
Maier, C., Baron, R., Tölle, T. R., Binder, a, Birbaumer, N., Birklein, F., … Treede, R.-D. (2010). Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain, 150(3), 439–50. doi:10.1016/j.pain.2010.05.002
Malessa, R., Agelink, M., Himmelmann, M., Kloss, T., Mertins, L., & Brockmeyer, N. H. (1996). Nerve conduction changes in asymptomatic HIV-1 seropositive individuals in the absence of other risk factors for neuropathy. Electromyography and clinical neurophysiology, 36(1), 3–8.
Maratou, K., Wallace, V. C. J., Hasnie, F. S., Okuse, K., Hosseini, R., Jina, N., … Rice, A. S. C. (2009). Comparison of dorsal root ganglion gene expression in rat models of traumatic and HIV-associated neuropathic pain. European journal of pain (London, England), 13(4), 387–98. doi:10.1016/j.ejpain.2008.05.011
Maritz, J., Benatar, M., Dave, J. a, Harrison, T. B., Badri, M., Levitt, N. S., & Heckmann, J. M. (2010). HIV neuropathy in South Africans: frequency, characteristics, and risk factors. Muscle & nerve, 41(5), 599–606. doi:10.1002/mus.21535
133
Martin, C., Solders, G., Sönnerborg, A., & Hansson, P. (2003). Painful and non-painful neuropathy in HIV-infected patients: an analysis of somatosensory nerve function. European journal of pain (London, England), 7(1), 23–31.
McArthur, J C, Yiannoutsos, C., Simpson, D. M., Adornato, B. T., Singer, E. J., Hollander, H., … Karalnik, I. J. (2000). A phase II trial of nerve growth factor for sensory neuropathy associated with HIV infection. AIDS Clinical Trials Group Team 291. Neurology, 54(5), 1080–8.
McArthur, Justin C, Brew, B. J., & Nath, A. (2005). Neurological complications of HIV infection. Lancet neurology, 4(9), 543–55. doi:10.1016/S1474-4422(05)70165-4
McCarthy, B. G., Hsieh, S.-T., Stocks, a., Hauer, P., Macko, C., Cornblath, D. R., … McArthur, J. C. (1995). Cutaneous innervation in sensory neuropathies: Evaluation by skin biopsy. Neurology, 45(10), 1848–1855. doi:10.1212/WNL.45.10.1848
McCracken, L., & Dhingra, L. (2002). A short version of the Pain Anxiety Symptoms Scale (PASS-20): Preliminary development and validity. Pain Research & Management, 7(1), 45–50.
McCracken, M. L., Zayfert, C., & Gross, R. T. (1992). The Pain Anxiety Symptoms Scale: development and validation of a sclae to measure fear of pain. Pain, 50(1), 66–73.
Melli, G., Keswani, S. C., Fischer, A., Chen, W., & Höke, A. (2006). Spatially distinct and functionally independent mechanisms of axonal degeneration in a model of HIV-associated sensory neuropathy. Brain : a journal of neurology, 129(Pt 5), 1330–8. doi:10.1093/brain/awl058
Mocroft, A., Ledergerbe, B., Katlama, C., Kirk, O., Reiss, P., D’Arminio, … Group., ; EuroSIDA study. (2003). Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet, 362(9377), 22–9.
Moher, D., Cook, D. J., Eastwood, S., Olkin, I., Rennie, D., & Stroup, D. F. (1999). Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet, 354(9193), 1896–900.
Moore, R. D., Wong, W. M., Keruly, J. C., & McArthur, J. C. (2000). Incidence of neuropathy in HIV-infected patients on monotherapy versus those on combination therapy with didanosine, stavudine and hydroxyurea. AIDS (London, England), 14(3), 273–8.
Morgello, S., Estanislao, L., Simpson, D., Geraci, A., DiRocco, A., Gerits, P., … Sharp, V. (2004). HIV-associated distal sensory polyneuropathy in the era of highly active antiretroviral therapy: the Manhattan HIV Brain Bank. Archives of neurology, 61(4), 546–51. doi:10.1001/archneur.61.4.546
134
Moyle, G., & Sadler, M. (1998). Peripheral neuropathy with nucleoside antiretrovirals: risk factors, incidence and management. Drug Saf, 19:, 1892–900.
Mulrow, C. D. (1987). The medical review article: state of the science. Annals of internal medicine, 106(3), 485–8.
Navia, B. A., Dafni, U., Simpson, D., Tucker, T., Singer, E., McArthur, J. C., … Lipton, S. A. (1998). A phase I/II trial of nimodipine for HIV-related neurologic complications. Neurology, 51(1), 221–8.
Nebuchennykh, M., Løseth, S., Lindal, S., & Mellgren, S. I. (2009). The value of skin biopsy with recording of intraepidermal nerve fiber density and quantitative sensory testing in the assessment of small fiber involvement in patients with different causes of polyneuropathy. Journal of neurology, 256(7), 1067–75. doi:10.1007/s00415-009-5065-y
Newshan, G. (1998). HIV neuropathy treated with gabapentin. AIDS (London, England), 12(2), 219–21.
Nokes, K., & Kendrew, J. (2001). Correlates of sleep quality in persons with HIV disease. J Assoc Nurses AIDS Care, 12, 17–22.
Oh, S. B., Tran, P. B., Gillard, S. E., Hurley, R. W., Hammond, D. L., & Miller, R. J. (2001). Chemokines and glycoprotein120 produce pain hypersensitivity by directly exciting primary nociceptive neurons. The Journal of neuroscience : the official journal of the Society for Neuroscience, 21(14), 5027–35.
Osio, M., Muscia, F., Zampini, L., Nascimbene, C., Mailland, E., Cargnel, A., & Mariani, C. (2006). Acetyl-l-carnitine in the treatment of painful antiretroviral toxic neuropathy in human immunodeficiency virus patients: an open label study. Journal of the peripheral nervous system : JPNS, 11(1), 72–6. doi:10.1111/j.1085-9489.2006.00066.x
Osman, a, Barrios, F. X., Kopper, B. a, Hauptmann, W., Jones, J., & O’Neill, E. (1997). Factor structure, reliability, and validity of the Pain Catastrophizing Scale. Journal of behavioral medicine, 20(6), 589–605.
Paice, J. A., Ferrans, C. E., Lashley, F. R., Shott, S., Vizgirda, V., & Pitrak, D. (2000). Topical capsaicin in the management of HIV-associated peripheral neuropathy. Journal of pain and symptom management, 19(1), 45–52.
Perkins, B. a, Olaleye, D., Zinman, B., & Bril, V. (2001). Simple screening tests for peripheral neuropathy in the diabetes clinic. Diabetes care, 24(2), 250–6.
Perkins, D., Leserman, J., Stern, R., Baum, R., Liao, D., Golden, R., & DL., E. (1995). Somatic symptoms and HIV infection: relationship to depressive symptoms and indicators of HIV disease. Am J Psychiatry, 152, 1776–81.
135
Pettersen, J. a, Jones, G., Worthington, C., Krentz, H. B., Keppler, O. T., Hoke, A., … Power, C. (2006). Sensory neuropathy in human immunodeficiency virus/acquired immunodeficiency syndrome patients: protease inhibitor-mediated neurotoxicity. Annals of neurology, 59(5), 816–24. doi:10.1002/ana.20816
Phillips, K. D., Skelton, W. D., & Hand, G. A. (2004). Effect of acupuncture administered in a group setting on pain and subjective peripheral neuropathy in persons with human immunodeficiency virus disease. Journal of alternative and complementary medicine (New York, N.Y.), 10(3), 449–55. doi:10.1089/1075553041323678
Pincus, T., Williams, A. C. D. C., Vogel, S., & Field, A. (2004). The development and testing of the depression, anxiety, and positive outlook scale (DAPOS). Pain, 109(1-2), 181–8. doi:10.1016/j.pain.2004.02.004
Pittenger, G. L., Ray, M., Burcus, N. I., McNulty, P., Basta, B., & Vinik, A. I. (2004). Intraepidermal nerve fibers are indicators of small-fiber neuropathy in both diabetic and nondiabetic patients. Diabetes care, 27(8), 1974–9.
Poliakov, I., & Toth, C. (2011). The impact of pain in patients with polyneuropathy. European journal of pain (London, England), 15(10), 1015–22. doi:10.1016/j.ejpain.2011.04.013
Polydefkis, M., Yiannoutsos, C. T., Cohen, B. a., Hollander, H., Schifitto, G., Clifford, D. B., … McArthur, J. C. (2002). Reduced intraepidermal nerve fiber density in HIV-associated sensory neuropathy. Neurology, 58(1), 115–119. doi:10.1212/WNL.58.1.115
Polydefkis, Michael. (2006). Skin biopsy findings predict development of symptomatic neuropathy in patients with HIV. Nature clinical practice. Neurology, 2(12), 650–1. doi:10.1038/ncpneuro0353
Polydefkis, Michael, Hauer, P., Sheth, S., Sirdofsky, M., Griffin, J. W., & McArthur, J. C. (2004). The time course of epidermal nerve fibre regeneration: studies in normal controls and in people with diabetes, with and without neuropathy. Brain : a journal of neurology, 127(Pt 7), 1606–15. doi:10.1093/brain/awh175
Reid, S., & Dwyer, J. (2005). Insomnia in HIV infection: a systematic review of prevalence, correlates, and management. Psychosomatic medicine, 67(2), 260–9. doi:10.1097/01.psy.0000151771.46127.df
RH, Dworkin, R., O’Connor, A., Backonja, M., Farrar, J., Finnerup, N., Jensen, T., … Wallace, M. (2007). Pharmacologic management of neuropathic pain: evidence-based recommendations. Pain, 132(3), 237–51.
Rice, A., Lever, I., & Zarnegar, R. (2008). Cannabinoids and analgesia, with special reference to neuropathic pain. In H. McQuay, E. E, Kalso, & R. Moore (Eds.), Systematic reviews and meta-analyses in pain (pp. p. 233–46). IASP Press, Seattle.
136
Rice, A. S. C. (2008). Should cannabinoids be used as analgesics for neuropathic pain? Nature clinical practice. Neurology, 4(12), 654–5. doi:10.1038/ncpneuro0949
Robinson-Papp, J, Morgello, S., Vaida, F., Fitzsimons, C., Simpson, D. M., Elliott, K. J., … Ellis, R. (2010). Association of self-reported painful symptoms with clinical and neurophysiologic signs in HIV-associated sensory neuropathy. Pain, 151(3), 732–736. doi:10.1016/j.pain.2010.08.045
Robinson-Papp, Jessica, Gonzalez-Duarte, A., Simpson, D. M., Rivera-Mindt, M., & Morgello, S. (2009). The roles of ethnicity and antiretrovirals in HIV-associated polyneuropathy: a pilot study. Journal of acquired immune deficiency syndromes (1999), 51(5), 569–73. doi:10.1097/QAI.0b013e3181adcefa
Rolke, R. (2006). Quantitative sensory testing : a comprehensive protocol for clinical trials. European Journal of Pain, 10, 77–88. doi:10.1016/j.ejpain.2005.02.003
Rolke, R., Baron, R., Maier, C., Tölle, T. R., Treede, R.-D., Beyer, a, … Wasserka, B. (2006). Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain, 123(3), 231–43. doi:10.1016/j.pain.2006.01.041
Rubinstein, M., & Selwyn, P. (1998). High prevalence of insomnia in an outpatient population with HIV infection. J Acquir Immun Defic Syndr Human Retrovirol, 19, 260–265.
Saarto, T., & Wiffen, P. J. (2010). Antidepressants for neuropathic pain: a Cochrane review. Journal of neurology, neurosurgery, and psychiatry, 81(12), 1372–3. doi:10.1136/jnnp.2008.144964
Sacks, H. S., Berrier, J., Reitman, D., Ancona-Berk, V. A., & Chalmers, T. C. (1987). Meta-analyses of randomized controlled trials. The New England journal of medicine, 316(8), 450–5. doi:10.1056/NEJM198702193160806
Scarpini, E., Sacilotto, G., Baron, P., Cusini, M., & Scarlato, G. (1997). Effect of acetyl-L-carnitine in the treatment of painful peripheral neuropathies in HIV+ patients. Journal of the peripheral nervous system : JPNS, 2(3), 250–2.
Schifitto, G, Yiannoutsos, C., Simpson, D. M., Adornato, B. T., Singer, E. J., Hollander, H., … McArthur, J. C. (2001). Long-term treatment with recombinant nerve growth factor for HIV-associated sensory neuropathy. Neurology, 57(7), 1313–6.
Schifitto, Giovanni, Yiannoutsos, C. T., Simpson, D. M., Marra, C. M., Singer, E. J., Kolson, D. L., … Navia, B. (2006). A placebo-controlled study of memantine for the treatment of human immunodeficiency virus-associated sensory neuropathy. Journal of neurovirology, 12(4), 328–31. doi:10.1080/13550280600873835
137
Scholz, J., Mannion, R. J., Hord, D. E., Griffin, R. S., Rawal, B., Zheng, H., … Woolf, C. J. (2009). A novel tool for the assessment of pain: validation in low back pain. PLoS medicine, 6(4), e1000047. doi:10.1371/journal.pmed.1000047
Shlay, J. C., Chaloner, K., Max, M. B., Flaws, B., Reichelderfer, P., Wentworth, D., … Cohn, D. L. (1998). Acupuncture and amitriptyline for pain due to HIV-related peripheral neuropathy: a randomized controlled trial. Terry Beirn Community Programs for Clinical Research on AIDS. JAMA : the journal of the American Medical Association, 280(18), 1590–5.
Silver, M., Blum, D., Grainger, J., Hammer, A. E., & Quessy, S. (2007). Double-blind, placebo-controlled trial of lamotrigine in combination with other medications for neuropathic pain. Journal of pain and symptom management, 34(4), 446–54. doi:10.1016/j.jpainsymman.2006.12.015
Simpson, D M, Dorfman, D., Olney, R. K., McKinley, G., Dobkin, J., So, Y., … Friedman, B. (1996). Peptide T in the treatment of painful distal neuropathy associated with AIDS: results of a placebo-controlled trial. The Peptide T Neuropathy Study Group. Neurology, 47(5), 1254–9.
Simpson, D M, Kitch, D., Evans, S. R., McArthur, J. C., Asmuth, D. M., Cohen, B., … Clifford, D. B. (2006). HIV neuropathy natural history cohort study: assessment measures and risk factors. Neurology, 66(11), 1679–87. doi:10.1212/01.wnl.0000218303.48113.5d
Simpson, D M, McArthur, J. C., Olney, R., Clifford, D., So, Y., Ross, D., … Hammer, A. E. (2003). Lamotrigine for HIV-associated painful sensory neuropathies: a placebo-controlled trial. Neurology, 60(9), 1508–14.
Simpson, D M, Olney, R., McArthur, J. C., Khan, A., Godbold, J., & Ebel-Frommer, K. (2000). A placebo-controlled trial of lamotrigine for painful HIV-associated neuropathy. Neurology, 54(11), 2115–9.
Simpson, D M, Schifitto, G., Clifford, D. B., Murphy, T. K., Durso-De Cruz, E., Glue, P., … Freeman, R. (2010). Pregabalin for painful HIV neuropathy: a randomized, double-blind, placebo-controlled trial. Neurology, 74(5), 413–20. doi:10.1212/WNL.0b013e3181ccc6ef
Simpson, D M, Scott, G. N., & Freeman, R. (2010). Pregabalin for painful HIV neuropathy.
Simpson, David M, Brown, S., & Tobias, J. (2008). Controlled trial of high-concentration capsaicin patch for treatment of painful HIV neuropathy. Neurology, 70(24), 2305–13. doi:10.1212/01.wnl.0000314647.35825.9c
Simpson, David M, Estanislao, L., Brown, S. J., & Sampson, J. (2008). An open-label pilot study of high-concentration capsaicin patch in painful HIV neuropathy. Journal of pain and symptom management, 35(3), 299–306. doi:10.1016/j.jpainsymman.2007.04.015
138
Singleton, J. R., Bixby, B., Russell, J. W., Feldman, E. L., Peltier, A., Goldstein, J., … Smith, a G. (2008). The Utah Early Neuropathy Scale: a sensitive clinical scale for early sensory predominant neuropathy. Journal of the peripheral nervous system : JPNS, 13(3), 218–27. doi:10.1111/j.1529-8027.2008.00180.x
Smith, P. F. (2007). Symptomatic treatment of multiple sclerosis using cannabinoids: recent advances. Expert review of neurotherapeutics, 7(9), 1157–63. doi:10.1586/14737175.7.9.1157
Smith, T., Jakobsen, J., Gaub, J., Helweg-Larsen, S., & Trojaborg, W. (1988). Clinical and electrophysiological studies of human immunodeficiency virus-seropositive men without AIDS. Annals of neurology, 23(3), 295–7. doi:10.1002/ana.410230313
Smyth, K., Affandi, J. S., McArthur, J. C., Bowtell-Harris, C., Mijch, a M., Watson, K., … Cherry, C. L. (2007). Prevalence of and risk factors for HIV-associated neuropathy in Melbourne, Australia 1993-2006. HIV medicine, 8(6), 367–73. doi:10.1111/j.1468-1293.2007.00478.x
So, Y., Holtzman, D., Abrams, D., & Olney, R. (1988). Peripheral neuropathy associated with acquired immunodeficiency syndrome. Prevalence and clinical features from a population-based survey. Arch Neurol, 45(9), 945–8.
Tagliati, M., Grinnell, J., Godbold, J., & Simpson, D. M. (1999). Peripheral nerve function in HIV infection: clinical, electrophysiologic, and laboratory findings. Archives of neurology, 56(1), 84–9.
Tan, T., Barry, P., Reken, S., Baker, M., & Guideline Development Group. (2010). Pharmacological management of neuropathic pain in non-specialist settings: summary of NICE guidance. BMJ, 340, :c1079. doi: 10.1136/bmj.c1079.
The Consensus Committee of the American Autonomic Society and the American Academy of Neurology. (1996). Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. Journal of the neurological sciences, 144(1-2), 218–9.
Ulett, G. A. (1999). Acupuncture and amitriptyline for HIV-related peripheral neuropathic pain. JAMA : the journal of the American Medical Association, 281(14), 1270–1; author reply 1271–2.
Vadivelu, N., & Berger, J. (1999). Neuropathic pain after anti-HIV gene therapy successfully treated with gabapentin. Journal of pain and symptom management, 17(3), 155–6.
Valdivelu, N., & Berger, J. (1999). Neuropathic pain after anti-HIV gene therapy successfully treated with gabapentin. J Pain Symptom Manage., 17(3), 155–6.
Vase, L., Nikolajsen, L., Christensen, B., Egsgaard, L. L., Arendt-Nielsen, L., Svensson, P., & Staehelin Jensen, T. (2011). Cognitive-emotional sensitization
139
contributes to wind-up-like pain in phantom limb pain patients. Pain, 152(1), 157–62. doi:10.1016/j.pain.2010.10.013
Verma, A. (2001). Epidemiology and clinical features of HIV-1 associated neuropathies. J Peripher Nerv Syst., 6, 8–13.
Vincent, A. M., Hinder, L. M., Pop-busui, R., & Feldman, E. L. (2009). 2009 PNS PLENARY LECTURE AND REVIEW Hyperlipidemia : a new therapeutic target for diabetic neuropathy, 267, 257–267.
Von Gunten, C. F., Eappen, S., Cleary, J. F., Taylor, S. G., Moots, P., Regevik, N., … Cella, D. (2007). Flecainide for the treatment of chronic neuropathic pain: a Phase II trial. Palliative medicine, 21(8), 667–72. doi:10.1177/0269216307083031
Wadley, A L, Kamerman, P. R., Chew, C. S. N., Lombard, Z., Cherry, C. L., & Price, P. (2013). A polymorphism in IL4 may associate with sensory neuropathy in African HIV patients. Molecular immunology, 55(3-4), 197–9. doi:10.1016/j.molimm.2013.02.002
Wadley, Antonia L, Cherry, C. L., Price, P., & Kamerman, P. R. (2011). HIV neuropathy risk factors and symptom characterization in stavudine-exposed South Africans. Journal of pain and symptom management, 41(4), 700–6. doi:10.1016/j.jpainsymman.2010.07.006
Wallace, V. C. J., Blackbeard, J., Pheby, T., Segerdahl, A. R., Davies, M., Hasnie, F., … Rice, A. S. C. (2007). Pharmacological, behavioural and mechanistic analysis of HIV-1 gp120 induced painful neuropathy. Pain, 133(1-3), 47–63. doi:10.1016/j.pain.2007.02.015
Wallace, V. C. J., Blackbeard, J., Segerdahl, A. R., Hasnie, F., Pheby, T., McMahon, S. B., & Rice, A. S. C. (2007a). Characterization of rodent models of HIV-gp120 and anti-retroviral-associated neuropathic pain. Brain : a journal of neurology, 130(Pt 10), 2688–702. doi:10.1093/brain/awm195
Wallace, V. C. J., Blackbeard, J., Segerdahl, A. R., Hasnie, F., Pheby, T., McMahon, S. B., & Rice, A. S. C. (2007b). Characterization of rodent models of HIV-gp120 and anti-retroviral-associated neuropathic pain. Brain : a journal of neurology, 130(Pt 10), 2688–702. doi:10.1093/brain/awm195
Ware, J. E., & Sherbourne, C. D. (1992). The MOS 36-Item Short Form Health Survey (SF-36). Medical Care, 30(6), 473–483.
Watters, M. R., Poff, P. W., Shiramizu, B. T., Holck, P. S., Fast, K. M. S., Shikuma, C. M., & Valcour, V. G. (2004). Symptomatic distal sensory polyneuropathy in HIV after age 50. Neurology, 62(8), 1378–83.
Webster, L. R., Peppin, J. F., Murphy, F. T., Tobias, J. K., & Vanhove, G. F. (2012). Tolerability of NGX-4010, a capsaicin 8% patch, in conjunction with three
140
topical anesthetic formulations for the treatment of neuropathic pain. Journal of pain research, 5, 7–13. doi:10.2147/JPR.S25272
White, F. A., Jung, H., & Miller, R. J. (2007). Chemokines and the pathophysiology of neuropathic pain. Proceedings of the National Academy of Sciences of the United States of America, 104(51), 20151–8. doi:10.1073/pnas.0709250104
Wiffen, P. J., & Rees, J. (2007). Lamotrigine for acute and chronic pain. Cochrane database of systematic reviews (Online), (2), CD006044. doi:10.1002/14651858.CD006044.pub2
Wiggin, T. D., Sullivan, K. A., Pop-busui, R., Amato, A., Sima, A. A. F., & Feldman, E. L. (2009). Elevated Triglycerides Correlate With Progression of Diabteic Neuropathy. Diabetes, 58(July), 1634–1640. doi:10.2337/db08-1771.T.D.W.
Winer, J. B., Bang, B., Clarke, J. R., Knox, K., Cook, T. J., Gompels, M., … Harris, J. W. (1992). A study of neuropathy in HIV infection. The Quarterly journal of medicine, 83(302), 473–88.
Winston, a, McAllister, J., Amin, J., Cooper, D. a, & Carr, a. (2005). The use of a triple nucleoside-nucleotide regimen for nonoccupational HIV post-exposure prophylaxis. HIV medicine, 6(3), 191–7. doi:10.1111/j.1468-1293.2005.00288.x
Woolley, I., Faragher, M., Ugoni, A., & Spelman, D. (1993). An analysis of factors associated with HIV-related peripheral neuropathy. Neurological Infections and Epidemiology, 1997:, 33–7.
Woolridge, E., Barton, S., Samuel, J., Osorio, J., Dougherty, A., & Holdcroft, A. (2005). Cannabis Use in HIV for Pain and Other Medical Symptoms. Journal of Pain and Symptom Management, 29(4), 358–367. doi:10.1016/j.jpainsymman.2004.07.011
Wright, E., Brew, B., Arayawichanont, a, Robertson, K., Samintharapanya, K., Kongsaengdao, S., … Wesselingh, S. (2008). Neurologic disorders are prevalent in HIV-positive outpatients in the Asia-Pacific region. Neurology, 71(1), 50–6. doi:10.1212/01.wnl.0000316390.17248.65
Yarchoan, R., Perno, C., Thomas, R., Klecker, R., Allain, J., Wills, R., … McNeely, M. (1988). Phase I studies of 2’,3'-dideoxycytidine in severe human immunodeficiency virus infection as a single agent and alternating with zidovudine (AZT). Lancet, 1(8577), 76–81.
Youle, M, & Osio, M. (2007). A double-blind, parallel-group, placebo-controlled, multicentre study of acetyl L-carnitine in the symptomatic treatment of antiretroviral toxic neuropathy in patients with HIV-1 infection. HIV medicine, 8(4), 241–50. doi:10.1111/j.1468-1293.2007.00467.x
Youle, Mike. (2007). Acetyl-L-carnitine in HIV-associated antiretroviral toxic neuropathy. CNS drugs, 21 Suppl 1, 25–30; discussion 45–6.
141
SUPLEMMENTAL DOCUMENTS
Supplemental Document 1:
Instrument To Measure The Likelihood Of Bias And Insufficient Statistical “Power” In Pain Research Reports (modified Jadad scale)
This is not the same as being asked to review a paper. It should not take more than 10 minutes to score a report and there are no right or wrong answers.
Please read the article and try to answer the following questions (see attached instructions):
1. Was the study described as randomised (this includes the use of words such as randomly, random, and randomisation)?
2. Was the study described as double blind? 3. Was there a description of withdrawals and dropouts? 4. Was there a description of a power calculation?
Scoring the items:
Either give a score of 1 point for each “yes” or 0 points for each “no”. There are no in-between marks.
Give 1 additional point if: For question 1, the method is to generate the sequence of
randomisation was described and it was appropriate
(table of random numbers, computer generated, etc).
And/or: If for question 2 the method of double blinding was described
and it was appropriate (identical placebo, active placebo,
dummy etc).
And/or: If for question 4 the method and assumptions for power calculation was described and it was appropriate and the number of patients who were randomised and
142
analysed on an intention to treat basis was in concordance with this calculation.
Deduct 1 point if:- For question 1, the study was described as randomised the
method of randomisation was inappropriate (patients were allocated
alternately, or according to date of birth, hospital number, etc) or the description was unclear.
And/or For question 2, the study was described as double blind but the
method of blinding was inappropriate (e.g., comparison of tablet vs. injection with no double dummy) or the description unclear.
And/or: If for question 4 the method and assumptions for power calculation was described and it was inappropriate or the number of patients who were randomised and analysed on an intention to treat basis did not reached the level required by the power calculation.
Guidelines for Assessment
1. Randomization A method used to generate the sequence of randomization will be regarded as appropriate if it allowed each study participant to have the same chance of receiving each intervention and the investigators could not predict which treatment was next. Methods of allocation using date of birth, date of admission, hospital numbers, or alternation should not be regarded as appropriate.
2. Double blinding
A study must be regarded as double blind if the word “double blind” is used. The method will be regarded as appropriate if it is stated that neither the person doing the assessments nor the study participant could identify the intervention being assessed, or if in the absence of such a statement the use of active placebos, identical placebos, or dummies is mentioned.
143
3. Withdrawals and dropouts Participants who were included in the study but did not complete the observation period or who were not included in the analysis must be described. The number and the reasons for withdrawal in each group must be stated. If there were no withdrawals, it should be stated in the article. If there is no statement on withdrawals, this item must be given no points.
4. Power calculations
The method for calculating the statistical power must be described and the assumptions regarding effect size, the alpha value (min. 0.05) and the power level (min. 0.8). The group sizes in the intention to treat analysis must be a minimum of that indicted by the power calculation.
Reference List
(1) Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ et al. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Controlled Clinical Trials 1996; 17(1):1-12.
(2) Rice ASC, Lever IJ, Zarnegar R. Cannabinoids and analgesia, with special reference to neuropathic pain. In: McQuay HJ, Kalso E, Moore RA, editors. Systematic reviews and meta-analyses in pain. Seattle: IASP Press; 2008. p. 233–46.
144
145
146
147
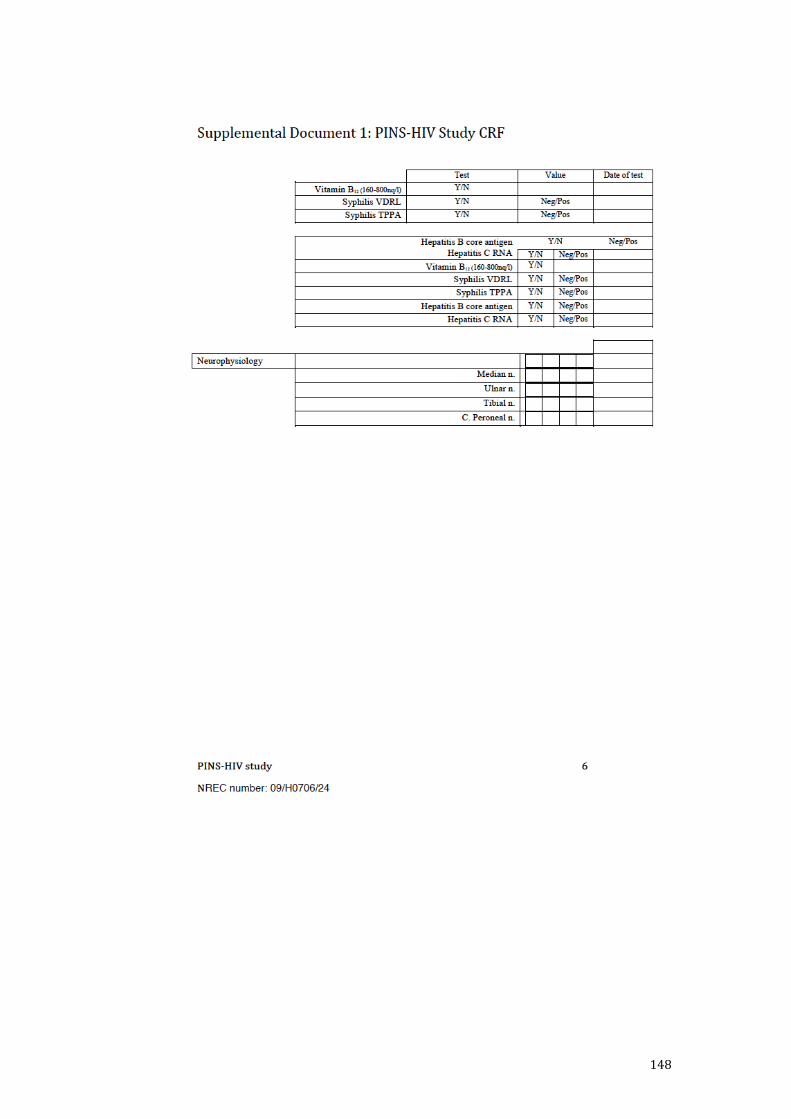
148
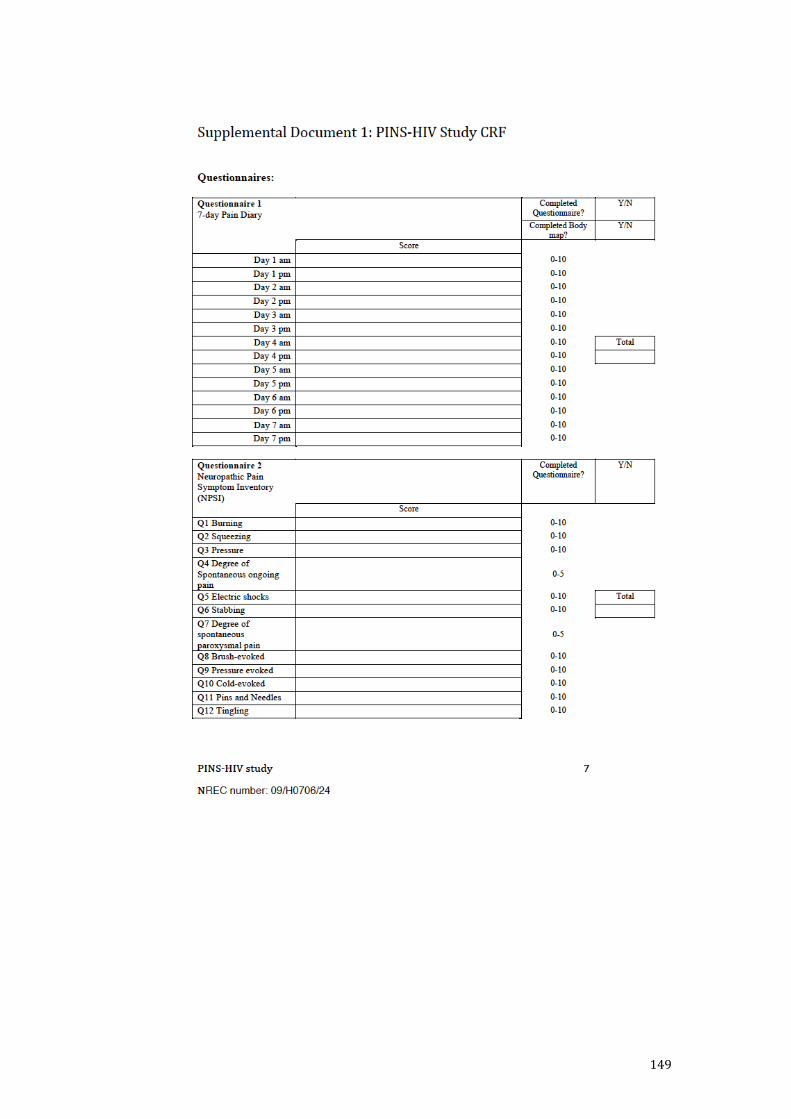
149
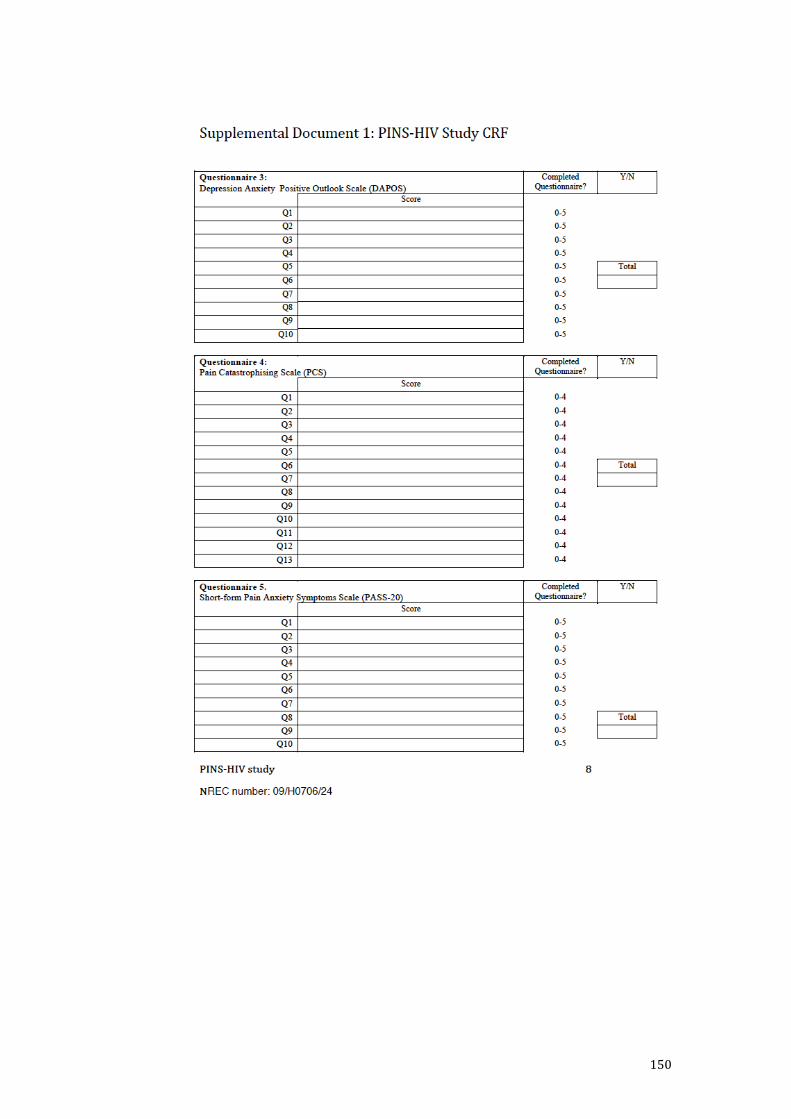
150
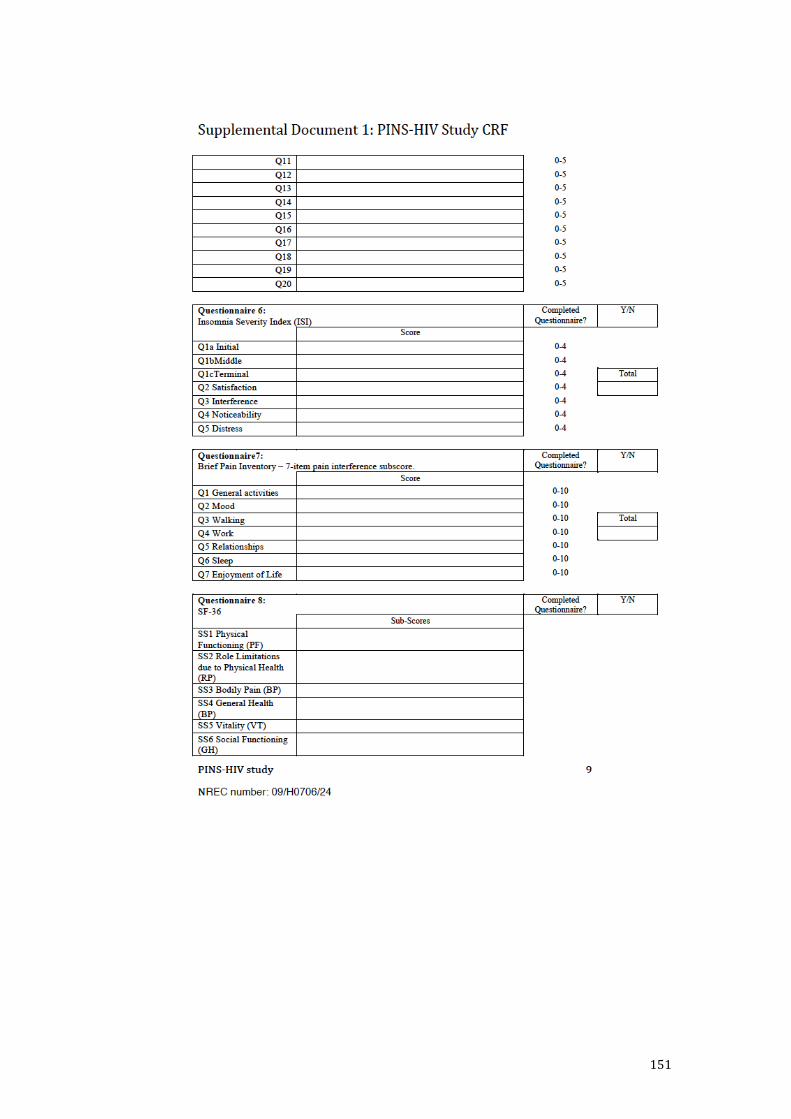
151
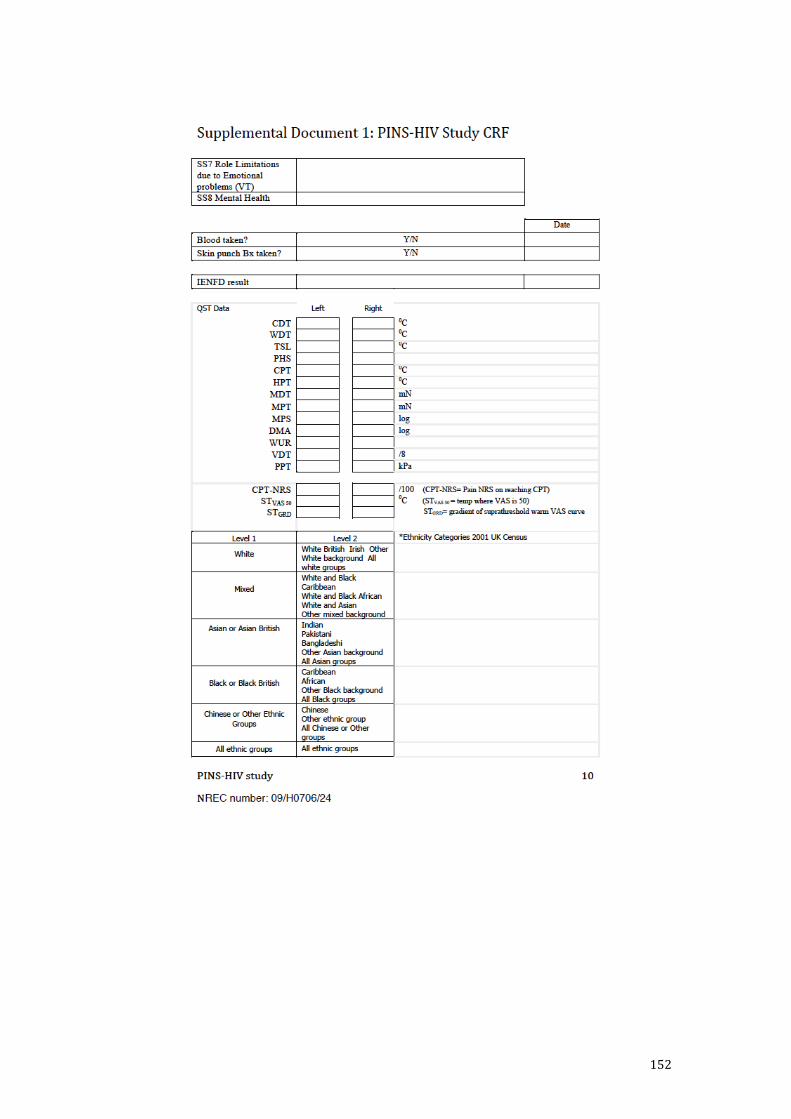
152
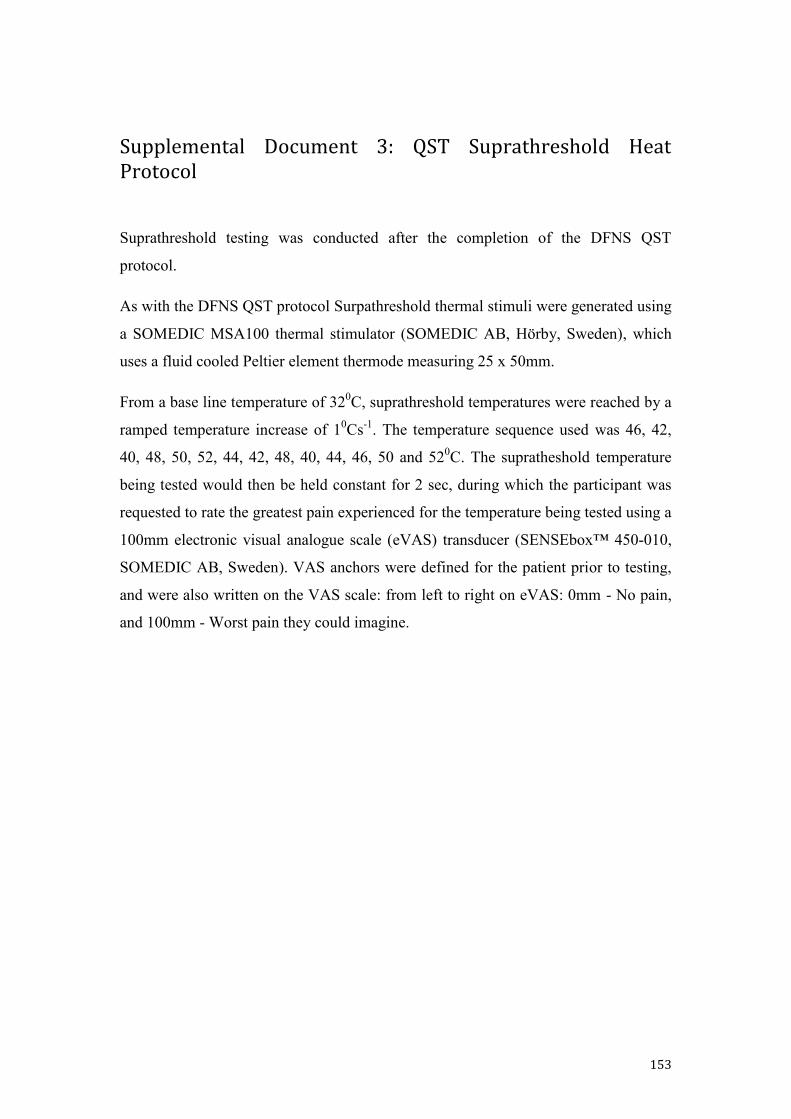
153
Supplemental Document 3: QST Suprathreshold Heat Protocol
Suprathreshold testing was conducted after the completion of the DFNS QST
protocol.
As with the DFNS QST protocol Surpathreshold thermal stimuli were generated using
a SOMEDIC MSA100 thermal stimulator (SOMEDIC AB, Hörby, Sweden), which
uses a fluid cooled Peltier element thermode measuring 25 x 50mm.
From a base line temperature of 320C, suprathreshold temperatures were reached by a
ramped temperature increase of 10Cs-1. The temperature sequence used was 46, 42,
40, 48, 50, 52, 44, 42, 48, 40, 44, 46, 50 and 520C. The supratheshold temperature
being tested would then be held constant for 2 sec, during which the participant was
requested to rate the greatest pain experienced for the temperature being tested using a
100mm electronic visual analogue scale (eVAS) transducer (SENSEbox™ 450-010,
SOMEDIC AB, Sweden). VAS anchors were defined for the patient prior to testing,
and were also written on the VAS scale: from left to right on eVAS: 0mm - No pain,
and 100mm - Worst pain they could imagine.
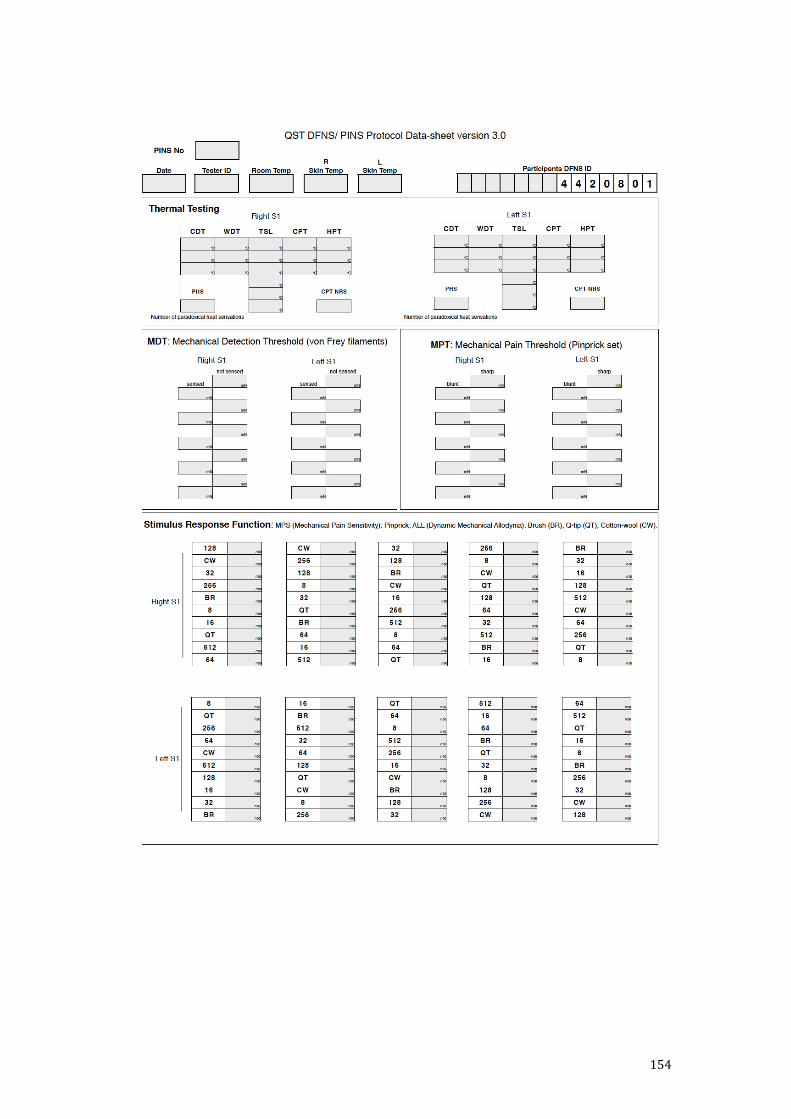
154
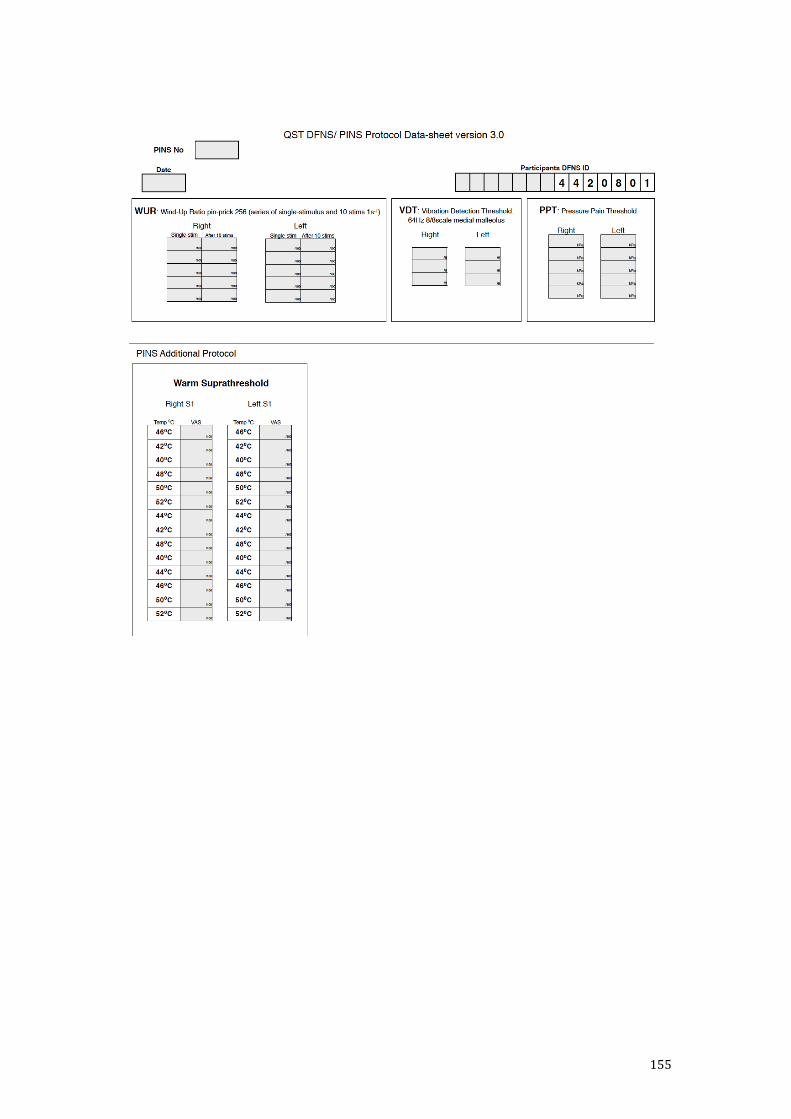
155
156
Supplemental Document 5: Structured Neurological Examination (SNE)
The structured neurological examination of the upper and lower limb was designed by an experienced neurologist (DB), to exam in detail, clinical neurological signs which might be present in a peripheral neuropathy.
Upper and Lower Limb Examination
Inspection
The presence of any muscle wasting is noted, with special attention given to the First Dorsal Interosseous muscle in the upper limb and Extensor Digitorium Brevis in the lower limb. The presence of ulcerations and deformities is also noted.
Motor
Motor strength is assessed using the expanded MRC grading system (see below table for details) for shoulder abduction, elbow flexion/ extension and wrist extension in the upper limb. In the lower limb Hip flexion, Knee extension and Extensor Hallucis Longus power are assessed.
Sensory
Joint position proprioception – The subject’s index finger at the level of the distal-interphalangeal joint is placed in the ‘up’ and ‘down’ position, with the examiner explaining to the subject the position the joint is in when the subject’s eyes are open. The procedure is repeated with the subject’s eyes closed for 3 different joint positions. If the subject fails to recognize 3 out of 3 positions, the examiner repeats the examination on the next proximal joint and so on, until a level is reached where the subject demonstrates normal joint proprioception. This level is then recorded.
Vibration perception – the examiner applies a maximally struck 128Hz tuning fork to the distal inter-phalangeal joint of the subject’s index finger in the upper limb, and the distal interphalangeal joint in the first toe in the lower limb. The examiner asks the subject to indicate if they can feel the vibration. If they are able to detect vibration, the examiner asks if it feels the same as when applied to the subject’s sternum. If the subject indicates that it does not feel the same, the assessment is repeated at the next most proximal joint until the subject indicates that the vibration sensation felt is the same when applied distally as when applied to the sternum. This level is then recorded.
Light touch – The examiner touches the palmer aspect of fingers 1 to 5 with a cotton wisp and asks the subject to point to the finger being touched with their eyes closed. The light touch stimulus is demonstrated first to the subject on their sternum with their eyes open.
Pin-prick perception – The examiner uses a Neurotip™ pin (Owen Mumford, Oxford U.K.) asking the subject to identify if the blunt or sharp part of the Neurotip pin is

157
being applied to the palmer aspect of the subjects index fingers. If the subject is not successful on 3 out of 3 applications, the examiner would repeat the assessment at the next most proximal joint. The level at which normal pin-prick sensation is recorded. The pin-prick examination is demonstrated first to the subject on their sternum with their eyes open
Temperature perception - The examiner uses cold and warm water filled test tubes, asking the subject to indicate if the test tube applied is warm or cold when applied to first the subjects palmer aspect of their finger tips with their eyes are closed. If the subject is unable to correctly identify the temperature, the assessment is repeated at the next most proximal joint. The examiner first demonstrates the test on the subjects sternum with their eyes open.
Reflexes
Using a standard 40 cm ‘Queen Square’ style reflex hammer. Reflexes assessed: biceps, triceps and brachioradialis in the upper limb; patella, Achilles’ and plantar in the lower limb. The examiner records if the reflex was normal, absent, brisk or only present with a reinforcement maneuver. Plantar reflexes are recorded as up or down.